Back to Journals » Patient Related Outcome Measures » Volume 14
Impact of Belimumab on Patient-Reported Outcomes in Systemic Lupus Erythematosus: Insights from Clinical Trials and Real-World Evidence
Authors Gomez A ![]() , Enman Y, Parodis I
, Enman Y, Parodis I ![]()
Received 10 November 2022
Accepted for publication 11 January 2023
Published 19 January 2023 Volume 2023:14 Pages 1—13
DOI https://doi.org/10.2147/PROM.S369584
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Robert Howland
Alvaro Gomez,1 Yvonne Enman,1 Ioannis Parodis1,2
1Division of Rheumatology, Department of Medicine Solna, Karolinska Institutet and Karolinska University Hospital, Stockholm, Sweden; 2Department of Rheumatology, Faculty of Medicine and Health, Örebro University, Örebro, Sweden
Correspondence: Ioannis Parodis, Division of Rheumatology, Karolinska University Hospital Solna, SE-171 76, Stockholm, Sweden, Tel +46722321322, Email [email protected]
Abstract: Systemic lupus erythematosus (SLE) is a chronic, autoimmune disease, characterised by a relapsing-remitting pattern of inflammatory activity, with each relapse contributing to irreversible end-organ damage with detrimental effects on patients’ course, adding up to morbidity burden and shortening life-length. Along with several other demographic, socioeconomic, and life-style factors, high inflammatory activity and accrued organ damage have been coupled with adverse health-related quality of life (HRQoL) within physical, mental, and psychosocial aspects. The management of SLE has improved substantially during the last decades, owing to a technological explosion that has advanced drug development towards more targeted options. Being the first drug to be approved for SLE in more than half a century and the first in history biological agent for SLE, the introduction in 2011 of the monoclonal antibody belimumab that specifically binds to the soluble counterpart of B cell activating factor (BAFF) was a breakthrough in SLE drug development. The efficacy and favourable safety profile of belimumab has been demonstrated across several clinical trials and observational studies. Herein, we reviewed the literature and provide a summary on the effects of belimumab on SLE patients’ HRQoL based on 23 studies. Belimumab has been shown to induce clinically important improvements in physical aspects of HRQoL and in fatigue, the latter being a common and major complaint within the SLE population. People with SLE overall benefit more from belimumab within physical compared with mental aspects of HRQoL. However, despite improvements of clinical and immunological features upon therapy with belimumab, HRQoL perception remains unsatisfactory for a substantial percentage of the patients. Finally, our review made apparent an urgent need for optimisation of the use of patient-reported outcome measures, both in research and clinical practice.
Keywords: systemic lupus erythematosus, health-related quality of life, fatigue, patient-reported outcomes, belimumab, monoclonal antibodies
Introduction
Systemic lupus erythematosus (SLE) is a complex, chronic, autoimmune disease that is characterised by a relapsing-remitting pattern of inflammatory activity, with each relapse contributing to irreversible end-organ damage.1 Such damage has detrimental effects on SLE patients’ course, adding up to morbidity burden and shortening life-length.2,3 Along with several other demographic, socioeconomic, and life-style factors, high inflammatory activity and accrued organ damage have been coupled with adverse health-related quality of life (HRQoL) within physical, mental, and psychosocial aspects.4,5
The management of SLE has improved substantially during the last decades as a result of technological advances that have propelled drug development towards more targeted options, such as biological agents.6 Owing to the central role of B cells in SLE pathogenesis,7 several compounds that target the B cell compartment have been investigated as candidate treatments of SLE.8 Belimumab is one of those compounds; it is a fully human IgG1-λ monoclonal antibody that specifically binds to the soluble form of B cell activating factor belonging to the TNF family (BAFF; also known as B lymphocyte stimulator, BLyS). Being the first biological agent to be licensed for treating SLE and the first drug to be approved for SLE in more than half a century in 2011, the introduction of belimumab indicated a breakthrough in SLE drug development.
Belimumab was approved in 2011 for the treatment of adult patients with active SLE after two pivotal Phase III randomised clinical trials (RCTs), ie, the BLISS-52 and BLISS-76 trials.9,10 The initial licence for belimumab was for its intravenous (IV) administration at a dose of 10 mg/kg every second week for four weeks, and every fourth week thereafter. Later, the subcutaneous (SC) administration at a weekly dose of 200 mg was added as an alternative option.11 Belimumab has also received approval for use in paediatric SLE,12 and since recently in lupus nephritis (LN).13
The efficacy and favourable safety profile of belimumab has been demonstrated across several clinical trials and observational studies.9–24 Safety signals reported in the literature mainly comprise infusion reactions and non-severe infections.9,10,15,21,22,25 Data from two RCTs10,26 raised concerns about an increased risk for psychiatric events, including severe depression and suicidal ideation, but a systematic review and meta-analysis of 11 RCTs did not corroborate this risk.27 Overall, belimumab has a satisfactory safety profile, also during long-term usage.21,22
A previous review summarised the impact of belimumab on patient-reported outcomes based on results from the phase III belimumab RCTs,28 and we recently reviewed the effect of different biological agents on SLE patients’ HRQoL, focusing on methodological approaches for reporting HRQoL outcomes.29 We herein reviewed the literature and provide a summary on the effects of belimumab on SLE patients’ HRQoL based on RCTs and real-world evidence, aiming to highlight clinical implications.
Methods
We searched the MEDLINE and EMBASE databases from database inception until March 2022. To increase sensitivity, a two-block search was conducted including the search terms “systemic lupus erythematosus” and “belimumab”. The search strategy can be found as Supplementary Material. Interventional studies, including RCTs and their respective open-label extension studies and post-hoc analyses, quasi-experimental studies, cohort studies, and cross-sectional studies, were deemed eligible. Studies in languages other than English, Spanish, or Swedish (languages spoken by the authors) were excluded.
The patient perspective was obtained through contributions from a patient research partner (YE) at the level of study design and conduct.
Results
We identified 23 eligible articles of studies that comprised patients with SLE who were treated with belimumab (Figure 1). Table 1 summarises the characteristics of studies that were deemed eligible for analysis, while Table 2 details the effectiveness of belimumab in terms of HRQoL in the different studies. The most common instruments used to measure HRQoL were generic, particularly the Medical Outcomes Study Short Form 36 (SF-36) health survey,30 the EuroQol 5-Dimension health questionnaire (EQ-5D),31 and the Functional Assessment of Chronic Illness Therapy – Fatigue (FACIT-F) scale, the latter to specifically assess fatigue.32
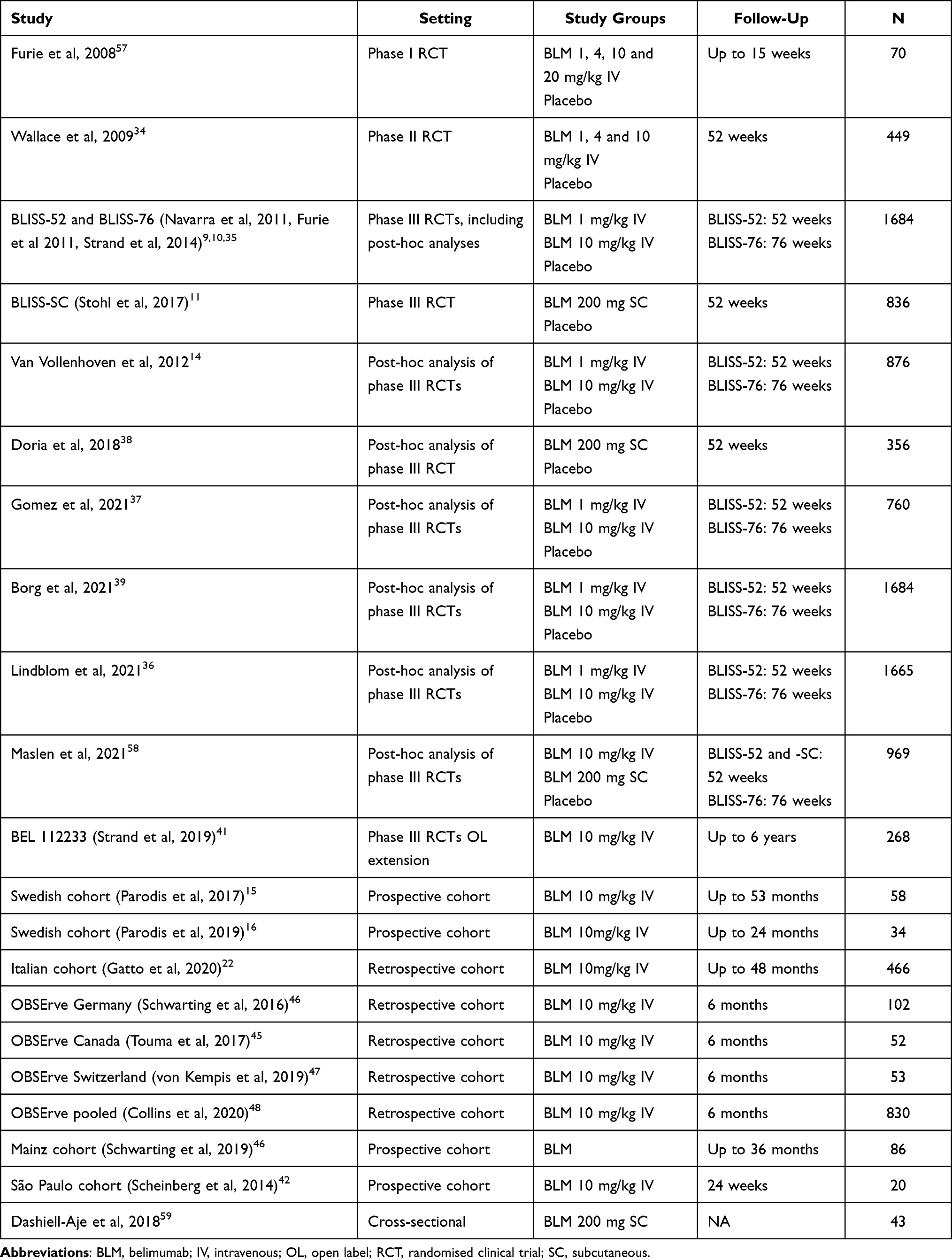 |
Table 1 Characteristics of Eligible Studies on Belimumab in Patients with Systemic Lupus Erythematosus |
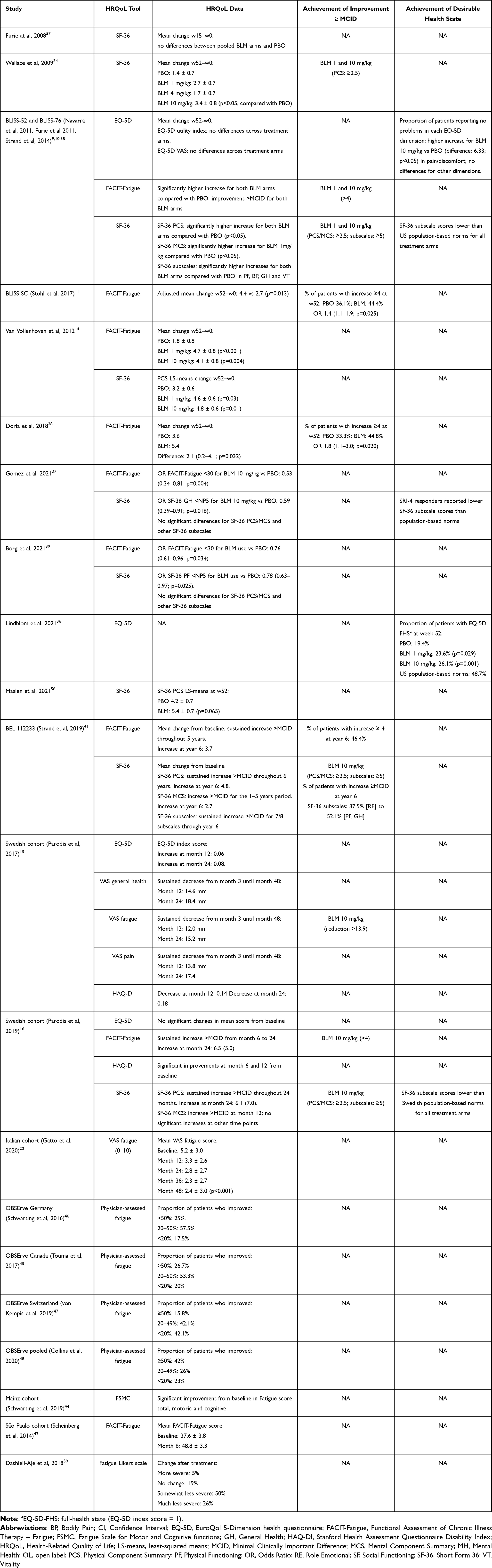 |
Table 2 Impact of Belimumab on SLE Patient’s HRQoL |
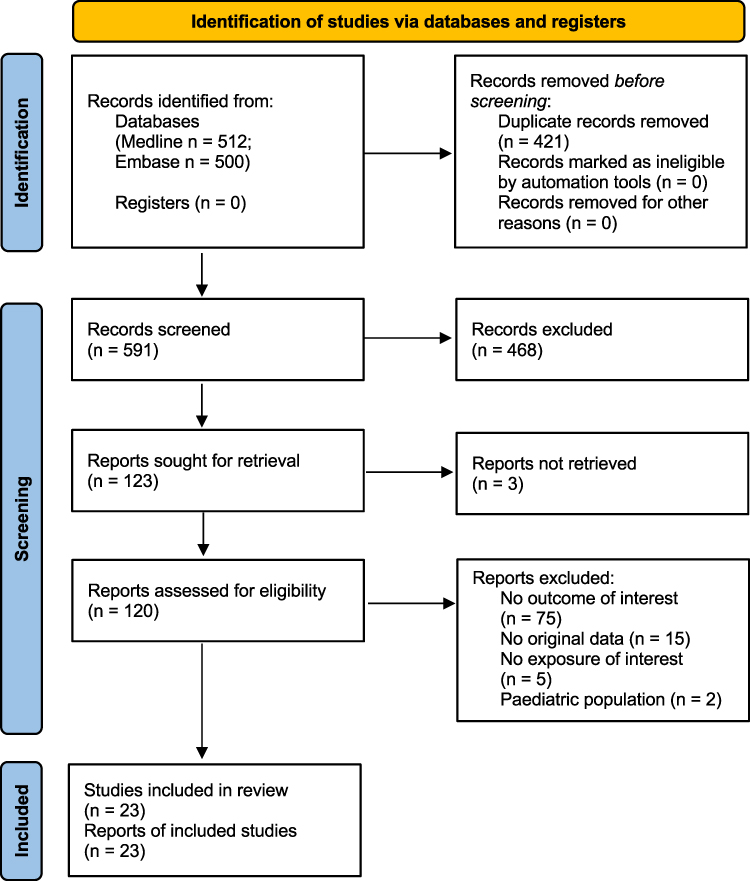 |
Figure 1 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram. Adapted from Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71, Open Access. |
The SF-36 health survey is a 36-item questionnaire that assesses self-perception of HRQoL over the past four weeks. Patient responses are computed and summarised into eight subscales that denote distinct HRQoL aspects, ie, physical functioning (PF), role physical (RP), bodily pain (BP), general health (GH), social functioning (SF), vitality (VT), role emotional (RE), and mental health (MH). Additionally, scores from these subscales are weighted and summarised into the physical component summary (PCS) and the mental component summary (MCS). Higher scores in SF-36 subscales and component summaries denote better HRQoL.
EQ-5D consists of a visual analogue scale (VAS) that captures overall health status, and a descriptive system that comprises five questions, each representing a distinct health dimension. Patient responses to these questions are summarised into a health profile, and an index score; the latter score is calculated based on population-specific valuation sets and ranges from less than 0 to 1. An EQ-5D index score of 1 represents the desired perception of health status, and is termed full health state (FHS).33
FACIT-F is a 13-item survey that evaluates fatigue over the past seven days.32 Patient responses are transformed into a score that ranges from 0 (maximal fatigue) to 52 (minimal fatigue).
Phase II RCT of Belimumab
In the phase II RCT of belimumab, SLE patients with moderate disease activity were randomly allocated to IV infusions of three doses of verum drug or placebo. The trial did not meet its primary efficacy endpoint; however, belimumab induced greater clinical benefits than placebo in seropositive patients and in patients who received prednisone >7.5 mg/day at baseline. Patients who received belimumab 10 mg/kg self-reported improvements in SF-36 PCS scores, which exceeded those considered clinically important and were greater than those reported by patients who received placebo (3.4 ± 0.8 versus 1.4 ± 0.7; P < 0.05); no such differences between belimumab and placebo were noted for the lower belimumab doses.34
Pivotal Phase III RCTs of Belimumab: BLISS-52 and BLISS-76
In the two pivotal phase III RCTs of belimumab, patients with SLE received IV infusions of belimumab at a dose 1 mg/kg or 10 mg/kg, or placebo. The BLISS-52 and BLISS-76 trials had similar design but differed in the length of follow-up (52-week follow-up in BLISS-52 and 76-week follow-up in BLISS-76). Both trials met the primary efficacy endpoint, ie, attainment of SLE Responder Index 4 (SRI-4) at week 52, as well as key secondary endpoints such as lower frequencies of severe flares and reductions in glucocorticoid doses n belimumab-treated patients versus placebo-receivers.9,10
A post-hoc analysis these trials investigated HRQoL outcomes in belimumab-treated patients compared with placebo-receivers,35 and reported greater improvements in SF-36 PCS at week 52 in both belimumab arms compared with patients who received placebo, and greater improvements in SF-36 MCS in patients who received IV belimumab 1 mg/kg compared with placebo-receivers. Regarding SF-36 subscales, belimumab induced greater improvements in PF, BP, and GH. However, despite the documented improvements, HRQoL at week 52 was poorer than that of age- and sex-matched US population-based norms. Mean changes in EQ-5D utility index scores or VAS scores did not differ across treatment arms. Lastly, improvements in FACIT-F and SF-36 VT scores were greater in both belimumab arms compared with patients who received placebo and exceeded minimal clinically important differences (MCIDs).
In subsequent post-hoc analyses, the proportion of patients who reported EQ-5D full health state at week 52 was greater in belimumab-treated patients compared with placebo-receivers, as well as in SRI-4 responders compared with non-responders.36 Moreover, greater proportions of patients in the belimumab 10 mg/kg arm versus placebo reported “no problems” at week 52 regarding mobility (odds ratio, OR: 1.32; 95% confidence interval, CI: 1.00–1.74; P = 0.049), self-care (OR: 1.46; 95% CI: 1.02–2.10; P = 0.038), and pain/discomfort (OR: 1.51; 95% CI: 1.14–1.99; P = 0.004).
Another post-hoc analysis that focused on the SLE patients who attained the primary efficacy endpoint of the trials (SRI-4) showed that use of IV belimumab 10 mg/kg was independently associated with a lower probability of adverse self-reported SF-36 PF (OR: 0.59; 95% CI: 0.39–0.91; P = 0.016) and FACIT-F scores <30 (OR: 0.53; 95% CI: 0.34–0.81; P = 0.004) at week 52.37 It is however worth nothing that self-reported scores were worse than those derived from age- and sex-matched norms in all SF-36 subscales. Adverse SF-36 outcome was defined in line with research in rheumatoid arthritis38 as scores ≤ the normative 5th percentile in an age- and sex-matched US population-based sample, while adverse FACIT-F outcome was defined as scores <30.32 The benefit from belimumab use regarding prevention of both adverse physical HRQoL outcome and severe fatigue was later corroborated in a post-hoc analysis that included the entire study population from the BLISS-52 and BLISS-76 trials.39 Lastly, analyses in the subgroup of patients with positive anti-dsDNA levels and/or low complement levels at baseline reported greater improvements in HRQoL and fatigue in belimumab-treated patients compared with placebo-receivers.14,40
Open-Label Extension Phases
A subset of patients who completed the BLISS-76 trial continued in an open-label extension study, in which they continued to receive belimumab (belimumab/belimumab arm; n = 177), or switched to belimumab (placebo/belimumab arm; n = 91). These patients were followed for up to 6 years. In this study, patients reported sustained improvements in SF-36 PCS (mean change ± standard deviation, SD from baseline through year 6: 3.4 ± 8.6) and MCS (mean change ± SD from baseline through year 6: 2.5 ± 10.1), which were greater than MCIDs.41 Percentages of patients reporting increases in SF-36 subscale scores ≥MCID at the end of follow-up (year 6) were overall greater for the physical subscales of SF-36; they ranged from 37.5% (RE) to 52.1% (PF, BP, and GH). Despite improvements deemed clinically important, SF-36 scores were, again, considerably lower compared with reference normative values derived from the US general population. Moreover, patients reported sustained improvements in FACIT-F scores (mean change ± SD from baseline through year 6: 3.7 ± 11.8), which exceeded the MCID in comparisons over the first five years, but not at further assessments (year 6).
Subsequent RCTs
The BLISS-SC trial evaluated the efficacy and safety of weekly SC injections of belimumab 200 mg in patients with SLE.11 Patients who received belimumab self-reported improvements in FACIT-F scores at week 52 which were deemed clinically important and were statistically greater than those reported by placebo-receivers (mean increase: 4.4 versus 2.7; P = 0.01). Moreover, the percentage of patients who improved in FACIT-F at an extent that exceeded the MCID was greater among belimumab-treated patients than among placebo-receivers (44.4% versus 36.1%; P = 0.02). Three additional phase III RCTs of belimumab have been conducted, BLISS-Northeast Asia42 and EMBRACE43 for active SLE, yet excluding severe active renal SLE, and BLISS-LN13 for active LN, but no results on HRQoL have been reported from these trials.
Observational Studies
Efficacy and safety of belimumab have also been reported from several cohorts around the world. In a cohort of 20 patients from Brazil, improvements in FACIT-F scores from baseline (37.6 ± 3.8) through month 6 (48.8 ± 3.3) were documented.44 In a cohort of 58 patients from three tertiary referral centres in Sweden, SLE patients reported a sustained increase in EQ-5D index score over 24 months on treatment with belimumab, as well as decreases in 100-mm VAS pain (mean change from baseline to month 24: 17.3 mm; P < 0.001), VAS fatigue (mean change from baseline to month 24: 15.1 mm; P = 0.007), VAS general health (mean change from baseline to month 24: 18.4 mm; P < 0.001), and Stanford Health Assessment Questionnaire Disability Index (HAQ-DI; mean change from baseline to month 24: 0.18; P = 0.014).15 In a subsequent study of belimumab-treated patients from the Karolinska University Hospital in Stockholm, SLE patients reported early and continuous, gradual improvements in SF-36 PCS over time on belimumab therapy, which exceeded the MCID at the assessments of month 12 and 24; self-reports concerning SF-36 MCS yielded less consistent results, which improvements documented at month 12 only.45 Importantly, patients self-reported considerable HRQoL impairments over time within all SF-36 domains compared with an age- and sex-matched normative reference group, despite the documented improvements. Regarding fatigue, patients in that study self-reported sustained improvements that exceeded the MCID in FACIT-F scores, as well as in SF-36 VT subscale scores.45
In a study from Mainz in Germany, levels of antibodies against the NR2 subunit of the N-methyl-D-aspartate receptor (anti-NR2) were found to correlate with fatigue and were higher in patients with severe fatigue compared with SLE patients with moderate, mild, or no fatigue.46 In a subgroup of 68 belimumab-treated SLE patients who received treatment for at least 6 months, improvements in fatigue were documented and included improvements within subscales for motor and cognitive functions; those were accompanied by decreases in serum levels of anti-NR2 antibodies.46 In a study from Italy that comprised 466 belimumab-treated patients with SLE, sustained decreases in VAS fatigue scores were documented throughout a follow-up of up to 48 months, yielding a change from 5.2 ± 3.0 at baseline to 2.4 ± 3.0 at month 48 (P < 0.001).19
The observational programme “evaluation Of use of Belimumab in clinical practice Settings” (OBSErve) comprised a series of studies carried out in 6 different countries (Argentina, Canada, Germany, Spain, Switzerland, USA).47–49 In these studies, physician-assessed changes in fatigue at month 6 compared with baseline were reported. In the pooled OBSErve study population that comprised 372 patients with SLE, 23% of the patients experienced minimal or no improvement in fatigue (<20% improvement), whereas 44% experienced a ≥50% improvement.23
Discussion
We reviewed the literature in a systematic manner to gain insight in the impact of belimumab on HRQoL. Results from six studies suggest that belimumab induces clinically meaningful improvements in several aspects of HRQoL and fatigue; these results mainly are based on assessments using the SF-36 and FACIT-F scales. Importantly, the benefit from belimumab was greater within physical compared with mental aspects of HRQoL.41
Several studies have shown that belimumab exerts clinically important and sustained improvements on physical aspects of HRQoL. Two RCTs of belimumab demonstrated improvements induced by belimumab in the physical components of SF-36 that exceeded thresholds set to define minimal clinically important differences, and were greater than improvements seen in the placebo arm; importantly, these improvements were sustained in the open-label extension phases of these RCTs.35,41 Along the same lines, benefits from belimumab exceeded the MCID regarding SF-36 PCS, yet not SF-36 MCS, in a Swedish real-life clinical setting.45
Moreover, the positive effects of belimumab on fatigue have been consistently demonstrated in RCTs and cohort studies. In the RCTs of IV belimumab, use of both low-dose and high-dose belimumab was associated with clinically important improvements in fatigue, along with lower proportions of belimumab-treated patients reporting severe fatigue compared with placebo receivers.9,10,35,37,39 Similarly, in the RCT of SC belimumab, higher proportions of patients treated with belimumab experienced clinically important improvements in fatigue compared with patients who received placebo.11,40 Several cohorts of SLE patients exposed to belimumab therapy from South America, North America, and Europe have used various instruments to assess fatigue, eg, FACIT-F, Fatigue Scale for Motor and Cognitive functions (FSMC), patient-reported visual analogue scales, and physician-based reports 11,15,19,23,44–49 Despite the diversity across study populations and outcome measures, a consistent benefit from belimumab was noted regarding fatigue.
However, despite the documented improvements, results from the phase III RCTs of belimumab,35 their open-label extension phases,41 as well as real-life studies,45 consistently showed considerable HRQoL impairments in patients with SLE compared with age- and sex-matched population-based reference data, even after documented improvements in HRQoL over time on treatment, particularly within physical aspects of HRQoL. As shown in a study from our group, considerable impairments were also shown in the subgroup of SLE patients who had attained adequate response to therapy based on clinical and laboratory parameters; importantly, this was shown to be partially driven by a negative impact of established irreversible end-organ damage.37
In a post-hoc analysis of the BLISS-52 and BLISS-76 trials of belimumab from our group, approximately one-fourth of the SLE patients self-reported EQ-5D full health state (FHS) after a 52-week-long therapeutic intervention; FHS corresponds to the best possible health experience.36 Interestingly, EQ-5D FHS showed ability to distinguish SRI-4 responders from non-responders, as well as belimumab-treated patients from placebo receivers,36 lending support to the usefulness of EQ-5D FHS as a patient-reported outcome fitting the treat-to-target concept in SLE,50 and warranting analysis of its association with long-term outcomes, eg, organ damage accrual.
It is worth noting that the evidence on the impact of belimumab on HRQoL compiled in the present review derive solely from generic patient-reported outcome measures. The use of generic instruments for HRQoL assessment has advantages, such as allowing comparisons with other disease populations as well as with the general population. However, their main limitation is that generic instruments may not capture aspects of particular relevance for SLE patient populations. Disease-specific tools, eg, the LupusQoL51 and LupusPro,52 allow researchers and health-care providers to investigate such aspects that may be omitted in generic tools, including body image, intimate relationships, and sleep. Furthermore, disease-specific tools have been shown to be more responsive to changes compared with generic tools in certain contexts.53,54 We herein advocate the combination of generic and disease-specific HRQoL instruments in clinical trials and cohort studies, aiming to obtain a comprehensive understanding of the SLE patients’ HRQoL experience.5
Belimumab may exert its benefits in multiple ways, eg, through overall disease control and corticosteroid-sparing effects,55,56 or through favourable effects on symptoms such as fatigue, that constitutes a major patient complaint, the latter being shown to be the case irrespective of the impact of belimumab on physician-assessed disease activity.37,46 In this regard, the documentation of correlations between fatigue and levels of anti-NR2 antibodies was of particular interest, along with the observed reductions both in the degree of fatigue and anti-NR2 antibody levels upon belimumab therapy;46 together, these observations suggest that belimumab may exert favourable effects that specifically concern fatigue, along with the overall clinical benefit and benefit in HRQoL.
Concluding Remarks
Along with the well-documented clinical efficacy of belimumab in patients with SLE and an overall satisfactory safety profile, there is robust evidence that belimumab induces clinically meaningful improvements in HRQoL, especially within physical aspects of HRQoL and in fatigue. Despite improvements in clinical and immunological features upon therapy, HRQoL perception remains unsatisfactory for a substantial percentage of SLE patients. In this regard, individualised and multicomponent management comprising non-pharmacological interventions along with optimised pharmacotherapy should be considered towards better outcomes in this highly heterogeneous patient population. Finally, our review made apparent an urgent need for optimisation of the use of patient-reported outcome measures, eg, through consistent use of MCIDs and comprehensive reports of not only changes in perceptions but also attainment of desirable states. Such optimisation is desirable both in research and clinical practice.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grants from the Swedish Rheumatism Association (R-941095), King Gustaf V’s 80-year Foundation (FAI-2020-0741), Professor Nanna Svartz Foundation (2020-00368), Swedish Society of Medicine (SLS-974449), Ulla and Roland Gustafsson Foundation (2021–26), Nyckelfonden (OLL-974804), Region Stockholm (FoUI-955483), and Karolinska Institutet.
Disclosure
IP has received research funding and/or honoraria from Amgen, AstraZeneca, Aurinia Pharmaceuticals, Elli Lilly and Company, Gilead Sciences, GlaxoSmithKline, Janssen Pharmaceuticals, Novartis, Otsuka Pharmaceutical, and F. Hoffmann-La Roche AG. The other authors declare that they have no conflicts of interest in this work.
References
1. Kaul A, Gordon C, Crow MK, et al. Systemic lupus erythematosus. Nat Rev Dis Primers. 2016;2:16039. doi:10.1038/nrdp.2016.39
2. Nived O, Jonsen A, Bengtsson AA, Bengtsson C, Sturfelt G. High predictive value of the systemic lupus international collaborating clinics/American college of rheumatology damage index for survival in systemic lupus erythematosus. J Rheumatol. 2002;29:1398–1400.
3. Bernatsky S, Boivin JF, Joseph L, et al. Mortality in systemic lupus erythematosus. Arthritis Rheum. 2006;54:2550–2557. doi:10.1002/art.21955
4. Gomez A, Hani Butrus F, Johansson P, et al. Impact of overweight and obesity on patient-reported health-related quality of life in systemic lupus erythematosus. Rheumatology. 2021;60:1260–1272. doi:10.1093/rheumatology/keaa453
5. Parodis I, Studenic P. Patient-reported outcomes in systemic lupus erythematosus. can lupus patients take the driver’s seat in their disease monitoring? J Clin Med. 2022;11(2):340. doi:10.3390/jcm11020340
6. Fanouriakis A, Kostopoulou M, Alunno A, et al. 2019 update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann Rheum Dis. 2019;78:736–745. doi:10.1136/annrheumdis-2019-215089
7. Szelinski F, Lino AC, Dorner T. B cells in systemic lupus erythematosus. Curr Opin Rheumatol. 2022;34:125–132. doi:10.1097/BOR.0000000000000865
8. Parodis I, Stockfelt M, Sjowall C, Cell B. Therapy in systemic lupus erythematosus: from rationale to clinical practice. Front Med. 2020;7:316. doi:10.3389/fmed.2020.00316
9. Navarra SV, Guzman RM, Gallacher AE, et al. Efficacy and safety of belimumab in patients with active systemic lupus erythematosus: a randomised, placebo-controlled, Phase 3 trial. Lancet. 2011;377:721–731. doi:10.1016/S0140-6736(10)61354-2
10. Furie R, Petri M, Zamani O, et al. A Phase III, randomized, placebo-controlled study of belimumab, a monoclonal antibody that inhibits B lymphocyte stimulator, in patients with systemic lupus erythematosus. Arthritis Rheum. 2011;63:3918–3930. doi:10.1002/art.30613
11. Stohl W, Schwarting A, Okada M, et al. Efficacy and safety of subcutaneous belimumab in systemic lupus erythematosus: a fifty-two-week randomized, double-blind, placebo-controlled study. Arthritis Rheumatol. 2017;69:1016–1027. doi:10.1002/art.40049
12. Brunner HI, Abud-Mendoza C, Viola DO, et al. Paediatric Rheumatology International Trials and G; the Pediatric Rheumatology Collaborative Study, Safety and efficacy of intravenous belimumab in children with systemic lupus erythematosus: results from a randomised, placebo-controlled trial. Ann Rheum Dis. 2020;79:1340–1348. doi:10.1136/annrheumdis-2020-217101
13. Furie R, Rovin BH, Houssiau F, et al. Two-year, randomized, controlled trial of belimumab in lupus nephritis. NEJM. 2020;383:1117–1128. doi:10.1056/NEJMoa2001180
14. van Vollenhoven RF, Petri MA, Cervera R, et al. Belimumab in the treatment of systemic lupus erythematosus: high disease activity predictors of response. Ann Rheum Dis. 2012;71:1343–1349. doi:10.1136/annrheumdis-2011-200937
15. Parodis I, Sjowall C, Jonsen A, et al. Smoking and pre-existing organ damage reduce the efficacy of belimumab in systemic lupus erythematosus. Autoimmun Rev. 2017;16:343–351. doi:10.1016/j.autrev.2017.02.005
16. Parodis I, Gomez A, Frodlund M, et al. Smoking reduces the efficacy of belimumab in mucocutaneous lupus. Expert Opin Biol Ther. 2018;18:911–920. doi:10.1080/14712598.2018.1494719
17. Ramskold D, Parodis I, Lakshmikanth T, et al. B cell alterations during BAFF inhibition with belimumab in SLE. EBioMedicine. 2019;40:517–527. doi:10.1016/j.ebiom.2018.12.035
18. Parodis I, Åkerström E, Sjöwall C, et al. Autoantibody and cytokine profiles during treatment with belimumab in patients with systemic lupus erythematosus. Int J Mol Sci. 2020;21(10):3463. doi:10.3390/ijms21103463
19. Gatto M, Saccon F, Zen M, et al. Early disease and low baseline damage as predictors of response to belimumab in patients with systemic lupus erythematosus in a real-life setting. Arthritis Rheumatol. 2020;72:1314–1324. doi:10.1002/art.41253
20. Gatto M, Saccon F, Andreoli L, et al. Durable renal response and safety with add-on belimumab in patients with lupus nephritis in real-life setting (BeRLiSS-LN). Results from a large, nationwide, multicentric cohort. J Autoimmun. 2021;124:102729. doi:10.1016/j.jaut.2021.102729
21. Wallace DJ, Ginzler EM, Merrill JT, et al. Safety and efficacy of belimumab plus standard therapy for up to thirteen years in patients with systemic lupus erythematosus. Arthritis Rheumatol. 2019;71:1125–1134. doi:10.1002/art.40861
22. Tanaka Y, Bae SC, Bass D, et al. Long-term open-label continuation study of the safety and efficacy of belimumab for up to 7 years in patients with systemic lupus erythematosus from Japan and South Korea. RMD Open. 2021;7:07. doi:10.1136/rmdopen-2021-001629
23. Collins CE, Cortes-Hernandez J, Garcia MA, et al. Real-world effectiveness of belimumab in the treatment of systemic lupus erythematosus: pooled analysis of multi-country data from the OBSErve Studies. Rheumatol Ther. 2020;7:949–965. doi:10.1007/s40744-020-00243-2
24. Fanouriakis A, Adamichou C, Koutsoviti S, et al. Low disease activity-irrespective of serologic status at baseline-associated with reduction of corticosteroid dose and number of flares in patients with systemic lupus erythematosus treated with belimumab: a real-life observational study. Semin Arthritis Rheum. 2018;48:467–474. doi:10.1016/j.semarthrit.2018.02.014
25. Iaccarino L, Andreoli L, Bocci EB, et al. Clinical predictors of response and discontinuation of belimumab in patients with systemic lupus erythematosus in real life setting. Results of a large, multicentric, nationwide study. J Autoimmun. 2018;86:1–8. doi:10.1016/j.jaut.2017.09.004
26. Sheikh SZ, Scheinberg MA, Wei JCC, et al. Mortality and adverse events of special interest with intravenous belimumab for adults with active, autoantibody-positive systemic lupus erythematosus (BASE): a multicentre, double-blind, randomised, placebo-controlled, Phase 4 trial. Lancet Rheumatol. 2021;3:E122–E130. doi:10.1016/S2665-9913(20)30355-6
27. Xie W, Huang H, Zhan S, Zhang Z. Risk of psychiatric disorders and all-cause mortality with belimumab therapy in patients with systemic lupus erythematosus: a meta-analysis of randomised controlled trials. Lupus Sci Med. 2021;8(1):e000534. doi:10.1136/lupus-2021-000534
28. Bangert E, Wakani L, Merchant M, Strand V, Touma Z. Impact of belimumab on patient-reported outcomes in systemic lupus erythematosus: review of clinical studies. Patient Relat Outcome Meas. 2019;10:1–7. doi:10.2147/PROM.S134326
29. Gomez A, Parodis I. Do biological agents improve health-related quality of life in patients with systemic lupus erythematosus? Results from a systematic search of the literature. Autoimmun Rev. 2022;21(11):103188. doi:10.1016/j.autrev.2022.103188
30. Ware J, Sherbourne C, The MOS. 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med Care. 1992;30:473–483. doi:10.1097/00005650-199206000-00002
31. EuroQol Group. EuroQol--a new facility for the measurement of health-related quality of life. Health Policy. 1990;16:199–208. doi:10.1016/0168-8510(90)90421-9
32. Webster K, Cella D, Yost K. The functional assessment of chronic illness therapy (FACIT) Measurement System: properties, applications, and interpretation. Health Qual Life Outcomes. 2003;1:79. doi:10.1186/1477-7525-1-79
33. EuroQol Research Foundation. EQ-5D-3L user guide; 2018. Available from: https://euroqol.org/publications/user-guides.
34. Wallace DJ, Stohl W, Furie RA, et al. A Phase II, randomized, double-blind, placebo-controlled, dose-ranging study of belimumab in patients with active systemic lupus erythematosus. Arthritis Rheum. 2009;61:1168–1178. doi:10.1002/art.24699
35. Strand V, Levy RA, Cervera R, et al. Study, Improvements in health-related quality of life with belimumab, a B-lymphocyte stimulator-specific inhibitor, in patients with autoantibody-positive systemic lupus erythematosus from the randomised controlled BLISS trials. Ann Rheum Dis. 2014;73:838–844. doi:10.1136/annrheumdis-2012-202865
36. Lindblom J, Gomez A, Borg A, et al. EQ-5D-3L full health state discriminates between drug and placebo in clinical trials of systemic lupus erythematosus. Rheumatology. 2021;60:4703–4716. doi:10.1093/rheumatology/keab080
37. Gomez A, Qiu V, Cederlund A, et al. Adverse health-related quality of life outcome despite adequate clinical response to treatment in systemic lupus erythematosus. Front Med. 2021;8:651249. doi:10.3389/fmed.2021.651249
38. Druce KL, Jones GT, Macfarlane GJ, Basu N. Patients receiving anti-TNF therapies experience clinically important improvements in RA-related fatigue: results from the British Society for Rheumatology Biologics Register for Rheumatoid Arthritis. Rheumatology. 2015;54:964–971. doi:10.1093/rheumatology/keu390
39. Borg A, Gomez A, Cederlund A, et al. Contribution of abnormal BMI to adverse health-related quality of life outcomes after a 52-week therapy in patients with SLE. Rheumatology. 2021;60:4205–4217. doi:10.1093/rheumatology/keaa909
40. Doria A, Stohl W, Schwarting A, et al. Efficacy and safety of subcutaneous belimumab in anti-double-stranded DNA-positive, hypocomplementemic patients with systemic lupus erythematosus. Arthritis Rheumatol. 2018;70:1256–1264. doi:10.1002/art.40511
41. Strand V, Berry P, Lin X, Asukai Y, Punwaney R, Ramachandran S. Long-term impact of belimumab on health-related quality of life and fatigue in patients with systemic lupus erythematosus: six years of treatment. Arthritis Care Res. 2019;71:829–838. doi:10.1002/acr.23788
42. Zhang F, Bae SC, Bass D, et al. A pivotal phase III, randomised, placebo-controlled study of belimumab in patients with systemic lupus erythematosus located in China, Japan and South Korea. Ann Rheum Dis. 2018;77:355–363. doi:10.1136/annrheumdis-2017-211631
43. Ginzler E, Guedes Barbosa LS, D’Cruz D, et al. At the time of the, EMBRACE: phase 3/4, randomized, 52-week study of belimumab efficacy and safety in patients of black African Ancestry With Systemic Lupus Erythematosus. Arthritis Rheumatol. 2021;2021:24.
44. Scheinberg M, Golmia R. Real life experience on the effect of Belimumab in patients with active systemic lupus. Springerplus. 2014;3:758. doi:10.1186/2193-1801-3-758
45. Parodis I, Lopez Benavides AH, Zickert A, et al. The impact of belimumab and rituximab on health-related quality of life in patients with systemic lupus erythematosus. Arthritis Care Res. 2019;71:811–821. doi:10.1002/acr.23718
46. Schwarting A, Mockel T, Lutgendorf F, et al. Fatigue in SLE: diagnostic and pathogenic impact of anti-N-methyl-D-aspartate receptor (NMDAR) autoantibodies. Ann Rheum Dis. 2019;78:1226–1234. doi:10.1136/annrheumdis-2019-215098
47. Touma Z, Sayani A, Pineau CA, et al. Belimumab use, clinical outcomes and glucocorticoid reduction in patients with systemic lupus erythematosus receiving belimumab in clinical practice settings: results from the OBSErve Canada Study. Rheumatol Int. 2017;37:865–873. doi:10.1007/s00296-017-3682-9
48. Schwarting A, Schroeder JO, Alexander T, et al. First real-world insights into belimumab use and outcomes in routine clinical care of systemic lupus erythematosus in Germany: RESULTS FROM the OBSErve Germany Study. Rheumatol Ther. 2016;3:271–290. doi:10.1007/s40744-016-0047-x
49. von Kempis J, Duetsch S, Reuschling N, et al. Clinical outcomes in patients with systemic lupus erythematosus treated with belimumab in clinical practice settings: a retrospective analysis of results from the OBSErve study in Switzerland. Swiss Med Wkly. 2019;149:w20022.
50. van Vollenhoven RF, Mosca M, Bertsias G, et al. Treat-to-target in systemic lupus erythematosus: recommendations from an international task force. Ann Rheum Dis. 2014;73:958–967. doi:10.1136/annrheumdis-2013-205139
51. McElhone K, Abbott J, Shelmerdine J, et al. Development and validation of a disease-specific health-related quality of life measure, the LupusQol, for adults with systemic lupus erythematosus. Arthritis Rheum. 2007;57:972–979. doi:10.1002/art.22881
52. Jolly M, Pickard AS, Block JA, et al. Disease-specific patient reported outcome tools for systemic lupus erythematosus. Semin Arthritis Rheum. 2012;42:56–65. doi:10.1016/j.semarthrit.2011.12.005
53. Izadi Z, Gandrup J, Katz PP, Yazdany J. Patient-reported outcome measures for use in clinical trials of SLE: a review. Lupus Sci Med. 2018;5:e000279. doi:10.1136/lupus-2018-000279
54. Devilliers H, Amoura Z, Besancenot JF, et al. Responsiveness of the 36-item short form health survey and the lupus quality of life questionnaire in SLE. Rheumatology. 2015;54:940–949. doi:10.1093/rheumatology/keu410
55. Singh JA, Shah NP, Mudano AS. Belimumab for systemic lupus erythematosus. Cochrane Database Syst Rev. 2021;2:CD010668. doi:10.1002/14651858.CD010668.pub2
56. Levy RA, Gonzalez-Rivera T, Khamashta M, et al. 10 Years of belimumab experience: what have we learnt? Lupus. 2021;30:1705–1721. doi:10.1177/09612033211028653
57. Furie R, Stohl W, Ginzler EM, et al. Biologic activity and safety of belimumab, a neutralizing anti-B-lymphocyte stimulator (BLyS) monoclonal antibody: a Phase I trial in patients with systemic lupus erythematosus. Arthritis Res Ther. 2008;10:R109. doi:10.1186/ar2506
58. Maslen T, Bruce IN, D’Cruz D, et al. Efficacy of belimumab in two serologically distinct high disease activity subgroups of patients with systemic lupus erythematosus: post-hoc analysis of data from the phase III programme. Lupus Sci Med. 2021;8:2. doi:10.1136/lupus-2020-000459
59. Dashiell-Aje E, Harding G, Pascoe K, DeVries J, Berry P, Ramachandran S. Patient evaluation of satisfaction and outcomes with an autoinjector for self-administration of subcutaneous belimumab in patients with systemic lupus erythematosus. Patient. 2018;11:119–129. doi:10.1007/s40271-017-0276-2
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Post-Acute SARS-CoV-2 Symptoms are Fewer, Less Intense Over Time in People Treated with Mono-Clonal Antibodies for Acute Infection
Price JK, Gerber LH, Stepanova M, de Avila L, Weinstein AA, Pham H, Nader F, Afendy M, Terra K, Austin P, Keo W, Racila A, Estep JM, Gerber S, Verma M, Golabi P, Lam BP, Younossi Z
International Journal of General Medicine 2023, 16:1479-1490
Published Date: 24 April 2023
Co-Infection Talaromyces marneffei and Pneumocystis jirovecii in a Patient with Systemic Lupus Erythematosus
Chen R, Li X, Zheng D, Cao C, Su J
Infection and Drug Resistance 2023, 16:4913-4918
Published Date: 27 July 2023
Experiences of Heart Failure and the Treatment Journey: A Mixed-Methods Study Among Patients with Heart Failure in Sweden

Liljeroos M, Agvall B, Eek D, Fu M
Patient Preference and Adherence 2023, 17:1935-1947
Published Date: 9 August 2023
Potential Mechanism of Fatigue Induction and Its Management by JAK Inhibitors in Inflammatory Rheumatic Diseases
Felis-Giemza A, Massalska M, Roszkowski L, Romanowska-Próchnicka K, Ciechomska M
Journal of Inflammation Research 2023, 16:3949-3965
Published Date: 8 September 2023