Back to Journals » Infection and Drug Resistance » Volume 19
Real-World Experience with High- versus Low-Dose Polymyxin B for Pulmonary Infections: A Retrospective Cohort Study
Authors Li L, Che H, Guo X, Yang Y, Yi Q, Yang R
Received 17 March 2026
Accepted for publication 15 June 2026
Published 22 June 2026 Volume 2026:19 609874
DOI https://doi.org/10.2147/IDR.S609874
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Oliver Planz
Lin Li,1,2 Hongyu Che,3 Xing Guo,4 Yilei Yang,1 Qiaoyan Yi,1 Rui Yang1
1Department of Clinical Pharmacy, The First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital, Shandong Engineering and Technology Research Center for Pediatric Drug Development, Shandong Medicine and Health Key Laboratory of Clinical Pharmacy, Shandong, Jinan, People’s Republic of China; 2Department of Pharmacy, the People’s Hospital of Binzhou City, Shandong, Binzhou, People’s Republic of China; 3Department of Pharmacy, Shandong Health Zibo Hospital, Shandong, Zibo, People’s Republic of China; 4Department of Pharmacy, the People’s Hospital of Rizhao city, Shandong, Rizhao, People’s Republic of China
Correspondence: Rui Yang, Department of Clinical Pharmacy, The First Affiliated Hospital of Shandong First Medical University & Shandong Provincial Qianfoshan Hospital, Shandong Engineering and Technology Research Center for Pediatric Drug Development, Shandong Medicine and Health Key Laboratory of Clinical Pharmacy, No. 16766, Jingshi Road, Jinan, Shandong, 250014, People’s Republic of China, Email [email protected]
Background: Polymyxin B(PMB) is crucial for treating carbapenem-resistant Gram-negative pulmonary infections. Despite existing guidelines, real-world dosing varies widely. The clinical and economic outcomes associated with higher versus lower dose regimens in routine practice require further elucidation.
Methods: This single-center retrospective cohort study included 235 adult patients with pulmonary infections who received intravenous PMB between January 2020 and December 2024. Based on real-world dosing practices, participants were categorized into high-dose and low-dose groups for comparative analysis of clinical efficacy, safety, and direct medical costs.
Results: A statistically significant difference in 28-day and 42-day all-cause mortality was observed between the two groups, although no significant differences were detected in clinical response rates or hospital length of stay. Safety assessments showed no statistically significant differences in hepatotoxicity, nephrotoxicity, or hematologic toxicity between groups; however, most non-significant adverse events occurred more frequently in the high-dose group. Direct medical costs analysis showed that the low-dose regimen significantly reduced drug costs, although total hospitalization costs did not differ significantly between the two groups.
Conclusion: For pulmonary infections, low-dose PMB (< 1.5 mg/kg/day) combined with extended therapy was associated with lower mortality, better safety, and similar clinical response vs. high dose. Drug costs were lower, suggesting real-world cost savings. These findings support PMB dose optimization, but prospective validation is needed.
Keywords: PMB, pulmonary infections, dosages, efficacy, safety
Introduction
As a major form of hospital-acquired infections, pulmonary infections have attracted global attention due to their high incidence and associated mortality.1 Faced with the limited efficacy of carbapenem antibiotics caused by the spread of drug-resistant bacteria,2 polymyxin-class drugs, with their unique amphipathic molecular structure, can effectively penetrate the outer membrane lipid bilayer of Gram-negative bacteria. Given their efficacy against nearly all carbapenem-resistant organisms (CRO), they have now become one of the important treatment options for infections caused by multidrug-resistant bacteria.3,4 To mitigate the risk of treatment failure and resistance emergence, PMB is seldom administered as monotherapy but is typically combined with other agents based on local antimicrobial susceptibility patterns and guidelines.5
Compared with colistin (polymyxin E), PMB demonstrates more linear pharmacokinetics, less renal tubular accumulation, and a more predictable safety profile, making it a preferred agent for critically ill patients with severe infections.6 However, there is still considerable controversy over the optimal dosing regimen of PMB in clinical treatment.7 The daily dosage recorded in the current drug instructions varies regionally. The Chinese generic drug (YaLe®) uses a fixed daily dose (50–100 million IU/day), while the original U.S. drug recommends a weight-adjusted dose (15,000–25,000 IU/kg/day).8 More notably, there is a conflict between the evidence from evidence-based medicine and the drug’s label recommendations: the 2016 U.S. adult hospital-acquired/ ventilator-associated pneumonia clinical practice guidelines suggest a daily dose of 2.5–3 mg/kg (administered in divided doses) for patients with normal renal function (1 mg = 10,000 IU), while the 2019 international consensus recommends a loading dose (2.0–2.5 mg/kg) combined with a maintenance dose (1.25–1.5 mg/kg, q12h).9
Although some retrospective studies suggest an association between higher doses and clinical outcomes such as in-hospital mortality,10 the majority of available research is based on Western populations. Considering the potential ethnic differences in body weight, renal function, drug metabolism and clinical practice, the conclusions drawn from these studies may not be directly applicable to Chinese patients. Therefore, real-world evidence comparing the effectiveness, safety, and economic impact of different dosing strategies in this specific population is needed. Leveraging real-world clinical data, this retrospective cohort study aims to compare clinical outcomes, safety profiles, and direct medical costs between patients receiving high-dose (HD) versus low-dose (LD) PMB regimens for pulmonary infections. The findings are intended to inform clinical practice and provide a basis for further prospective research.
Materials and Methods
Study Design and Patient
This was a retrospective observational study aimed at reflecting the real-world clinical use of PMB. It was conducted as a single-center cohort study that enrolled adult patients with pulmonary infections who received intravenous PMB at the First Affiliated Hospital of Shandong First Medical University (Qianfoshan Hospital, Shandong Province) from January 2020 to December 2024.
All patients received PMB produced by Shanghai No.1 Biochemical & Pharmaceutical Co., Ltd. (Approval Number H31020844, specification: 500,000 units/bottle). The dosage conversion was performed according to the drug label (1 mg = 10,000 IU).
The dosing threshold for group stratification was set at 1.5 mg/kg/day. The selection of this value was based on the Chinese drug label (YaLe®), the US package insert, and the 2019 international consensus guideline: it represents both the upper limit of the recommended maintenance dose in the international consensus and a reasonable cutoff between the maximum approved dose in China and the minimum recommended dose in the United States. Therefore, the HD group was defined as patients receiving PMB at a dose of ≥1.5 mg/kg/d, while the LD group received <1.5 mg/kg/d.
Inclusion criteria were as follows:
- Hospitalized with a diagnosis of pulmonary infection.
- Received intravenous PMB for at least 3 consecutive days.
- Aged 18 years or older.
Exclusion criteria were as follows:
- Missing key clinical data (eg., baseline liver and kidney function, body weight).
- Pregnancy or lactation.
- Hospitalization duration exceeding 75 days.
Data Extraction
All data were obtained from the hospital’s medical big data cloud platform for single diseases. This platform integrates data from multiple systems, including the Hospital Information System (HIS), Electronic Medical Record (EMR), Laboratory Information System (LIS), Picture Archiving and Communication Systems (PACS), and Nursing Information System (NIS). Data were independently extracted and cross-validated by two investigators. Data extraction was performed in strict accordance with the predefined study protocol, and missing data and outliers were managed using a uniform standardized procedure. This study was approved by the hospital’s ethics committee, and the requirement for informed consent was waived.
Outcomes
The primary outcome of this analysis was the clinical efficacy rate, defined as the improvement or normalization of clinical symptoms and signs, along with microbiological clearance and the normalization of relevant biochemical laboratory parameters after PMB treatment. Secondary outcome measures included 28-day all-cause mortality, 42-day all-cause mortality, length of hospitalization, and adverse events. The definitions are as follows:
- All-cause mortality: Death during hospitalization or abandonment of treatment due to disease deterioration or other reasons within 28 or 42 days of PMB use.
- Adverse events: Assessed according to the Common Terminology Criteria for Adverse Events (CTCAE) 5.0 standard.11
- Nephrotoxicity: Total incidence of nephrotoxicity, acute kidney injury, increased serum creatinine, and increased blood urea nitrogen.
- Hepatotoxicity: Total incidence of hepatotoxicity, increased alanine aminotransferase (ALT), increased aspartate aminotransferase (AST), elevated total bilirubin (TBIL), and increased γ-glutamyl transferase (GGT).
- Hematotoxicity: Total incidence of hematotoxicity, decreased hemoglobin (HGB), and reduced platelet count (PLT).
This study is conducted from the perspective of the medical insurance payer, aiming to provide directly applicable incremental cost-effectiveness evidence for insurance policy decision-making. The analysis considered only direct medical costs, including total hospitalization expenses (covering diagnosis, treatment, examinations, nursing, and bedding fees) and medication cost of PMB.
Statistical Analysis
Statistical analysis was performed using the hospital’s health medical big data single-disease cloud platform system (based on R language). Categorical data are expressed as n (%), and inter-group comparisons were made using the χ2-test. Normally distributed continuous data are presented as mean ± standard deviation, and group comparisons were made using the independent samples t-test. Non-normally distributed continuous data are expressed as median (interquartile range, IQR), and group comparisons were made using the Wilcoxon rank-sum test. Univariate and multivariate logistic regression analyses were employed to identify factors associated with treatment failure and nephrotoxicity. These models calculated the odds ratio (OR) and 95% confidence interval (CI). A two-sided P value of < 0.05 was considered statistically significant.
Results
Patient Characteristics
This study included 235 patients with pulmonary infections (HD, n=106; LD, n=129) after excluding 350 of 585 initially screened patients due to age ≤18 years, treatment duration < 3 days, or missing key data (Figure 1). Baseline characteristics differed significantly between groups, including male and concomitant chronic kidney disease (P < 0.05).
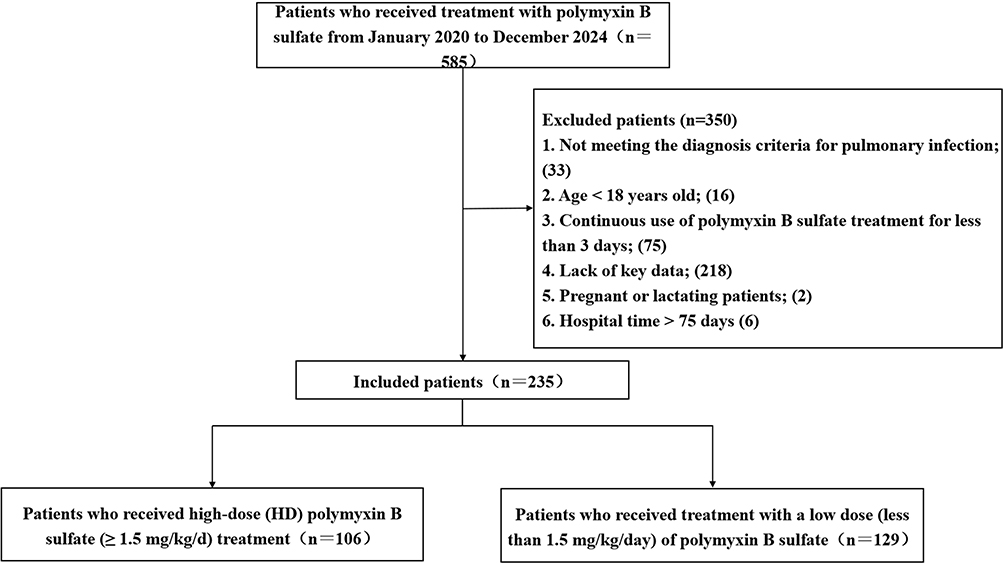 |
Figure 1 Schematic diagram of the patient screening process. |
These discrepancies were addressed in the outcome analysis using univariate and multivariate logistic regression. After adjustment, baseline characteristics were well-balanced (Table 1).
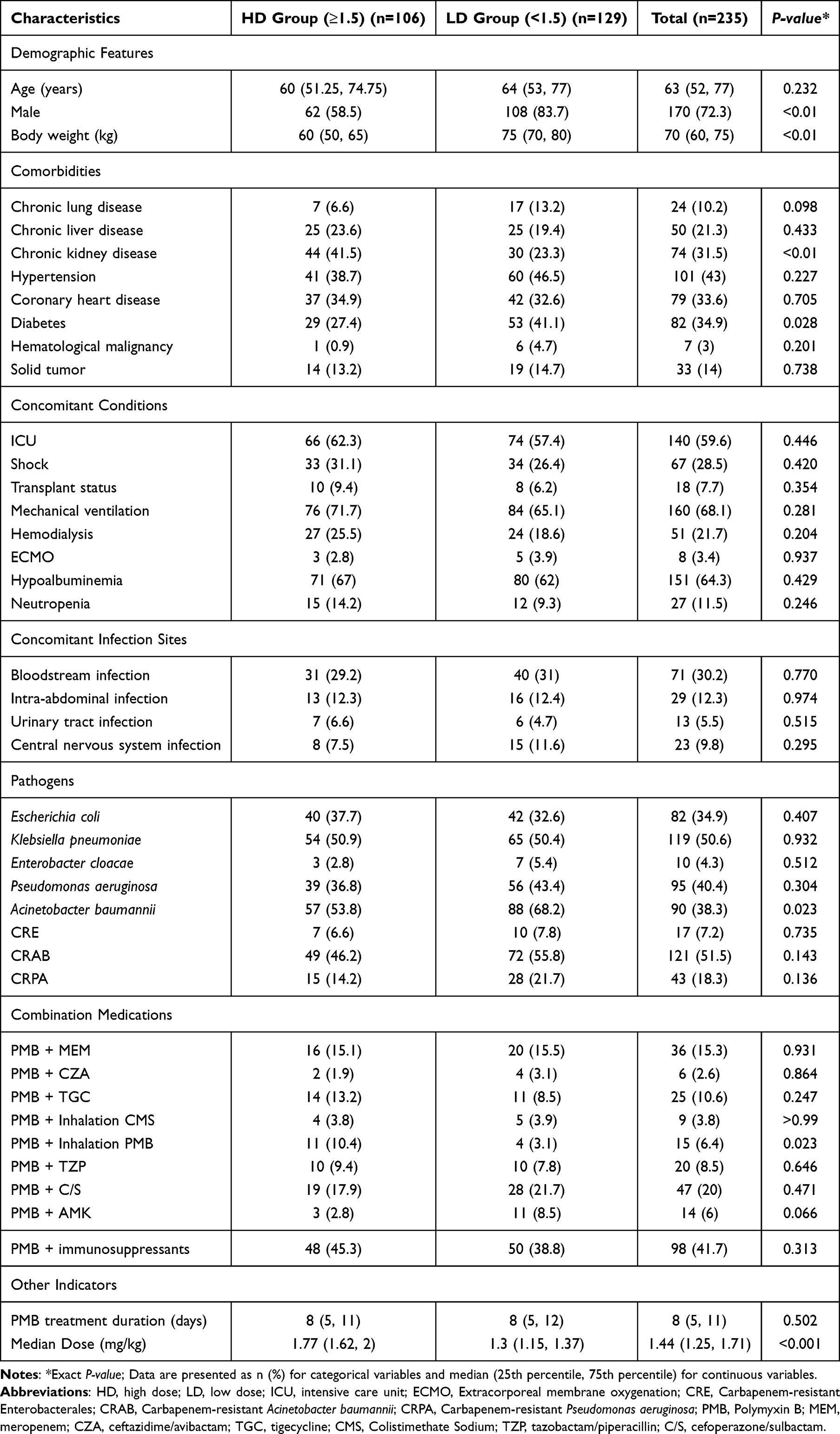 |
Table 1 Patient Characteristics |
Efficacy
After adjusting for baseline confounding factors using multivariate logistic regression (Table 2), statistically significant differences in all-cause mortality were observed between the two groups at 28 days (OR = 2.38, 95% CI: 1.16–4.98, P = 0.019) and 42 days (OR = 2.08, 95% CI: 1.02–4.29, P = 0.045). The Kaplan-Meier survival curves (Figure 2) and Log rank test corroborated the significant difference in survival between the two groups (P = 0.024). In contrast, no statistically significant differences were observed between the two groups in clinical efficacy rate (P = 0.132) or median length of hospital stay (P = 0.205).
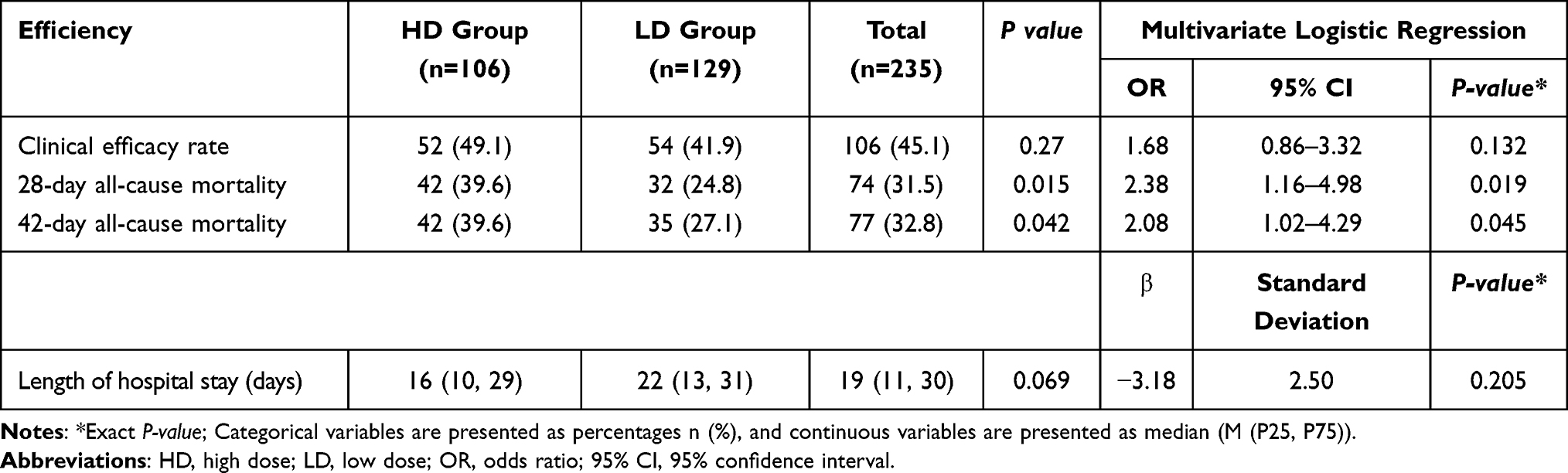 |
Table 2 Comparison of Efficiency and Multivariate Logistic Regression Adjustment |
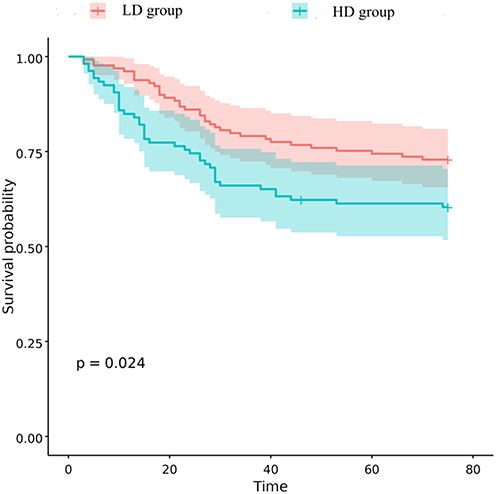 |
Figure 2 42-day survival analysis: Kaplan-Meier survival curve from 42 days after intravenous injection of PMB. |
Both univariate and multivariate logistic regression analyses identified several factors significantly associated with 28-day all-cause mortality (Table 3), including: hemodialysis (P = 0.002), hypoalbuminemia (P =0.001), PMB dosage of ≥1.5 mg/kg/day (P = 0.026), central nervous system infection (P < 0.001). Conversely, a longer duration of PMB therapy correlated inversely with mortality (OR = 0.88, 95% CI: 0.81–0.95, P = 0.001). Subgroup analysis showed there were 161 patients in the survivors group, with a PMB treatment duration of 9 (6, 12) days; and 74 patients in the non-survivors group, with a treatment duration of 6 (4, 9) days. The P-value for the between-group difference by the two-sample Wilcoxon test was < 0.001, indicating a statistically significant difference. Therefore, the treatment duration of PMB was significantly longer in surviving patients than in those who deceased.
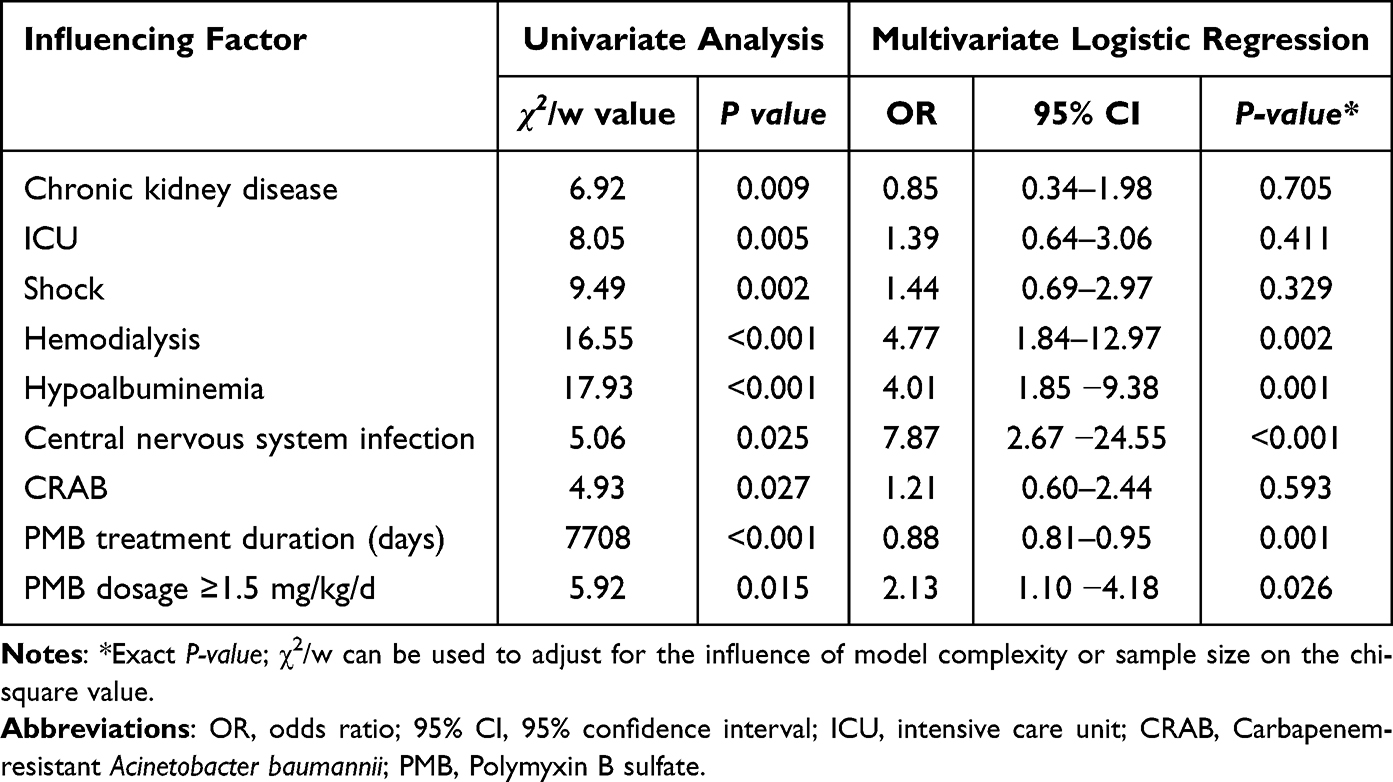 |
Table 3 Univariate and Multivariate Logistic Regression Analysis of Factors Affecting 28-Day All-Cause Mortality |
Safety
After adjusting for confounding factors, no significant differences were observed in the incidence of nephrotoxicity, hepatotoxicity, hematotoxicity, or individual adverse events (including decreased hemoglobin) between the two groups (Table 4). Multivariate analysis revealed that hemodialysis (OR = 3.91, 95% CI: 1.60–9.95, P = 0.003) and hypoalbuminemia (OR = 2.57, 95% CI: 1.19–5.96, P = 0.021) were independently associated with the development of nephrotoxicity (Table 5). In conclusion, while the incidence of adverse events, including nephrotoxicity, was comparable between the LD and HD regimens after adjusting for confounders, multivariate analysis identified hemodialysis and hypoalbuminemia as significant independent risk factors for nephrotoxicity. This underscores that the risk of renal injury is driven more by patient-specific factors than by the dosage regimen itself. Therefore, the comparable safety profile of the LD regimen reinforces its advantages, supporting it as a viable and preferable treatment option given its superior efficacy.
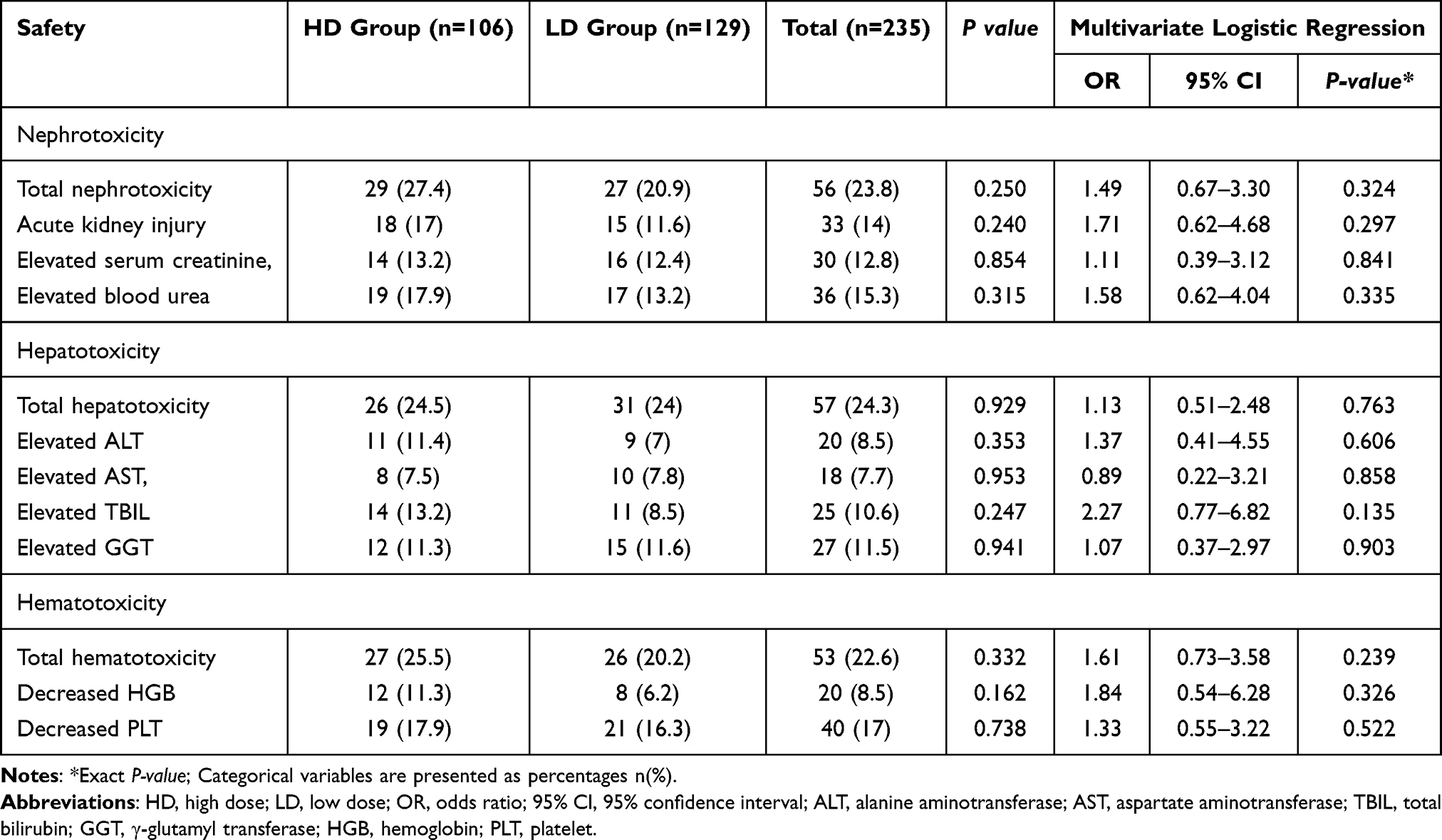 |
Table 4 Comparison of Safety and Adjustment via Multivariate Logistic Regression |
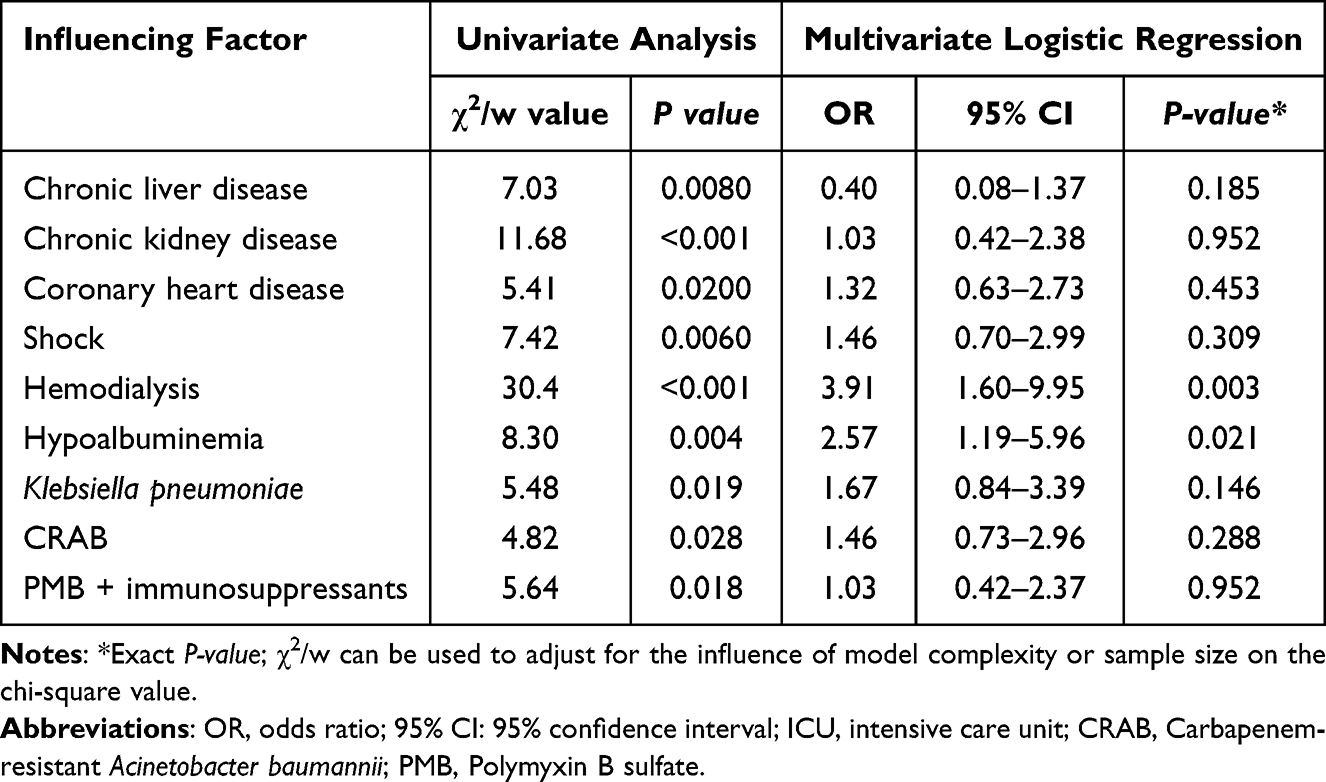 |
Table 5 Univariate and Multivariate Logistic Regression Analyses of Factors Influencing Nephrotoxicity |
Economic Evaluation
Given comparable efficacy between the two groups, cost-minimization analysis (CMA) was performed after adjusting for baseline confounding factors using multivariate logistic regression to evaluate their economic outcomes. Using the HD group as the reference, after adjusting for baseline confounding factors, multivariate regression of economic outcomes (Table 6) showed that the LD regimen significantly reduced PMB drug costs (β = −13,377.02, standard deviation = 4,419.84, P = 0.003). However, there was no statistically significant difference in total hospitalization costs between the HD group and the LD group (β = 11,168.20, standard deviation = 30,590.13, P = 0.715). Overall, the LD regimen significantly reduced drug costs, although total hospitalization costs did not differ significantly between the two groups. Several subgroup analyses were conducted; however, these were hypothesis-generating and should be interpreted with caution.
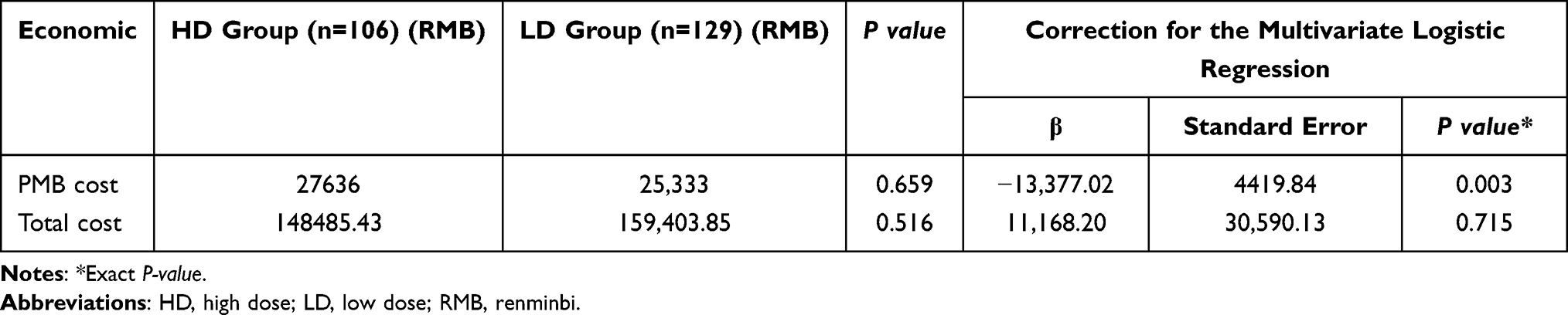 |
Table 6 Comparison of Economics and Adjustment via Multivariate Logistic Regression |
Discussion
Recently, the detection rates of Acinetobacter baumannii, Pseudomonas aeruginosa, and carbapenem-resistant Enterobacterales have been steadily increasing.12 Global surveillance data highlight a growing resistance to carbapenem antibiotics, severely limiting treatment options for treating severe pulmonary infections.13 In response, polymyxins, with their unique amphipathic molecular structure that enables effective penetration of the outer membrane of Gram-negative bacteria, have become one of the key drugs for salvage therapy in multi-drug resistant (MDR) infections.14 However, there remains considerable debate about the optimal administration strategy for PMB in clinical settings.9,15 This study, using real-world data, systematically compares the differences in efficacy, safety, and cost between HD (≥1.5 mg/kg/d) and LD (<1.5 mg/kg/d) regimens in adult patients with pulmonary infections. Given that most existing dosage comparison data are derived from foreign populations, and considering the potential ethnic differences in pharmacokinetics, genetic factors, and susceptibility to nephrotoxicity between Chinese and foreign populations, the goal of this study is to provide reliable evidence-based guidance and decision-making support to guide optimized dosing in domestic clinical practice.
In terms of efficacy, the HD regimen did not significantly improve the clinical response rate (P = 0.132). This finding is consistent with the dose-exploration study conducted by Zhang et al (n = 92).16 In their subgroup analysis of bacterial clearance rate, the advantage of the HD group (2 million IU/d) was no longer significant after multivariate adjustment. Similarly, a prospective study also found that the bacterial clearance rate in the HD group (150 mg/d) showed no significant advantage (35.2% vs 33.3%, P = 0.74).17 However, a study by Xia et al18 on the daily dosage of PMB found that the response rate and bacterial clearance rate in the 2 mg/kg/d and 2.5 mg/kg/d groups were significantly higher than those in the 1.5 mg/kg/d group (P < 0.05). In addition, our study found a significant difference in all-cause mortality between the HD and LD groups at both 28 and 42 days (P < 0.05). In contrast, the study by Liu et al observed no statistically significant difference in either 14-day mortality (23.7% vs. 27.8%, P = 0.42) or 28-day mortality (30.9% vs. 37.7%, P = 0.21) between the HD group and the LD group (100 mg/d). These findings suggest that outcome discrepancies across studies may be influenced by other confounding factors. It is worth noting that the significantly higher all-cause mortality in the HD group, despite no difference in clinical response rate compared with the LD group, is a counterintuitive result that requires in-depth analysis. Several speculative hypotheses may explain this phenomenon: (1) Patients in the HD group may have more severe underlying diseases (eg., advanced organ dysfunction, comorbidities such as diabetes or cardiovascular disease) that were not fully captured in this study. These unmeasured clinical characteristics could lead to a higher baseline mortality risk, and the HD PMB regimen may not offset this inherent risk, resulting in the observed higher mortality rate. (2) Higher doses of PMB within the study range may induce subclinical neurotoxicity (eg., peripheral neuropathy, cognitive disturbances) or electrolyte disturbances (eg., hypokalemia, hypomagnesemia), which are not fully reflected in the safety indicators monitored in this study. For critically ill patients with fragile physiological status, these subtle adverse effects may further aggravate their condition and increase mortality risk. (3) Patients in the HD group may have been prescribed more concurrent medications (eg., other nephrotoxic antibiotics, vasopressors), and the interaction between PMB and these drugs may have exacerbated organ damage (especially renal function impairment), thereby increasing mortality. In addition, the higher drug load of the HD regimen may impose excessive metabolic burden on the kidneys and other vital organs, which is not conducive to the recovery of critically ill patients.
Multivariate analysis identified concurrent CNS infection (OR = 7.87), hemodialysis, and hypoalbuminemia as key risk factors for 28-day all-cause mortality, while longer PMB treatment was associated with survival. Central nervous system infection was the strongest predictor, potentially due to inflammatory disruption of the blood-brain barrier, leading to cerebral edema and neurological damage.19 In hemodialysis patients, catheter-related infections significantly raised mortality—CVC use had higher infection (14.3% vs. 2.2%) and mortality rates (25% vs. 12.7%) than AVF.20 Similarly, studies have also found the treatment duration of PMB was significantly longer in surviving patients than in those who deceased.21,22 Although prolonged PMB therapy correlates with better outcomes, DRG payment systems and insurance constraints necessitate agile clinical assessment and timely sequential therapy. A patient-tailored approach integrating pharmacological and clinical factors is crucial for optimizing outcomes.
Regarding safety, no statistically significant differences were observed in the incidence of nephrotoxicity, hepatotoxicity, or hematological toxicity between the HD and LD regimens of PMB (P > 0.05). This suggests that a moderate increase in PMB dosage within the observed range does not significantly elevate the overall risk of adverse events. However, the incidence of nephrotoxicity, hepatotoxicity, and hematotoxicity (excluding elevated AST and GGT) was numerically higher in the HD group, with a notably higher incidence of decreased hemoglobin (11.3% vs. 6.2%). In terms of nephrotoxicity, the incidence of acute kidney injury (AKI) was 17.0% in the HD group and 11.6% in the LD group, with no significant difference (P = 0.24). Both univariate and multivariate logistic regression analyses indicated that a daily dosage ≥1.5 mg/kg did not increase the risk of nephrotoxicity. However, hemodialysis (OR = 3.91, 95% CI: 1.6–9.95, P = 0.03) and hypoalbuminemia (OR = 2.57, 95% CI: 1.19–5.95, P = 0.021) were independently associated with an increased risk of nephrotoxicity. Notably, a meta-analysis by Zhao et al23 (using a 2 mg/kg/day cutoff) and a Brazilian study by Elias et al10 (using a ≥ 200 mg daily dosage) both suggested that higher doses are linked to a greater risk of nephrotoxicity. Combining existing evidence, the risk of PMB-related nephrotoxicity appears to remain relatively stable within the dosage range of ≤ 1.5–2 mg/kg/day (approximately < 200 mg/day), but increases significantly beyond this threshold. The lack of a significant dose-nephrotoxicity relationship in this study may be attributed to the limited recommended dosage range for domestic generic products (500,000–1,000,000 IU/day), insufficient samples with dosages > 200 mg/day, and relatively short treatment durations (median 8 days). This highlights the need for larger sample sizes and longer follow-up periods to further investigate this relationship. For patients undergoing hemodialysis, changes in antibiotic clearance lead to fluctuations in drug concentrations, potentially exposing the kidneys to inappropriate drug levels.24 A review suggests that renal replacement therapy, including hemodialysis, significantly alters drug exposure, affecting both PK and PD.25 Additionally, hypoalbuminemia may indirectly increase the risk of nephrotoxicity by altering the interaction of PMB with proteins or receptors in certain clearance pathways, thereby increasing the drug’s volume of distribution and clearance rate.26,27
From an economic perspective, the LD group was associated with significantly lower medication costs (β = −13,377.02, P = 0.03) compared to the HD group. This is likely due to the pharmacokinetic characteristics of PMB, which has a long half-life of 11.9 hours.7 This suggests that the drug tends to accumulate in the body, making higher doses more likely to require frequent adjustments to maintain effective and safe concentrations, thereby increasing medication usage and cost. Regarding total hospitalization costs, no statistically significant difference was found between the two groups (β = 11,168.20, P = 0.715). It is plausible that although the HD group incurred higher medication costs, this could have been offset by other factors such as shorter hospital stays resulting from faster infection control in critically ill patients. However, it is important to note that in patients with renal insufficiency or those undergoing continuous renal replacement therapy, the clearance of PMB is increased (sieving coefficient: 0.32–0.59).18,28 In such cases, the need for dosage adjustments might increase, potentially adding to the overall cost.
This study observed a noteworthy phenomenon: among adult patients with pulmonary infections treated with polymyxin B, the HD group (≥ 1.5 mg/kg/d) showed higher mortality. This finding is based on the specific 1.5 mg/kg/d threshold; applying a higher threshold (eg., ≥ 2.0 mg/kg/d) might yield different efficacy and safety profiles, warranting further investigation. For this paradoxical dose-mortality association, we propose two non-mutually exclusive explanations. First, unmeasured confounding—particularly confounding by indication due to disease severity—is likely the primary cause. Critically ill patients with more organ dysfunction tend to receive higher doses. Although multivariate adjustment was performed, the lack of standardized severity scores (eg., APACHE II, SOFA) precludes full correction, making the observed lower mortality in the LD group more reflective of this bias than a causal benefit. Second, dose-related toxicity may contribute: higher doses increase risks of neurotoxicity and electrolyte disturbances, and drug interactions with other nephrotoxic agents could worsen outcomes.
This study has several inherent limitations that must be fully considered when interpreting the results. First, its retrospective observational design limits the strength of causal inference, and residual confounding or confounding by indication cannot be fully excluded. Second, therapeutic drug monitoring (TDM) data were unavailable, while PMB exhibits significant pharmacokinetic variability, and international consensus recommends TDM to optimize therapy. Third, this study reflects real-world practice in China at the time, where no loading dose was administered, which differs from international consensus recommendations based on foreign products. Fourth, although outcome assessment followed predefined criteria and was performed by researchers blinded to group allocation, the lack of a prospective blinded adjudication process remains a methodological limitation.
Conclusion
Based on real-world data, this study found that in adult pulmonary infection patients, the HD PMB regimen (≥1.5 mg/kg/d) showed no superiority over the LD regimen (<1.5 mg/kg/d) in efficacy, safety, or cost-effectiveness, suggesting LD as a viable alternative. However, these findings warrant caution: as a retrospective hypothesis-generating study, the observed dose-mortality association is likely confounded by disease severity, not causal. Limitations include single-center design, small sample, and lack of comparison with novel agents. Future validation via large-scale multicenter prospective trials or advanced observational methods (eg., propensity score weighting, target trial emulation) is needed to confirm these results and assess generalizability.
Ethics Approval
This study was approved by the ethics committee of First Affiliated Hospital of Shandong First Medical University (Shandong Qianfoshan Hospital, no. YXLLKY-2022-026). Because this study is a retrospective study and does not increase the risk to subjects, we hereby apply for exemption from informed consent.
Acknowledgments
The authors thank First Affiliated Hospital of Shandong First Medical University for providing permission to conduct the study.
Funding
This work was supported by the Pharmaceutical Society of Shandong, Jinan (no. Kjyw2024-2).
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The funding from the Pharmaceutical Society of Shandong (Kjyw2024-2) played no role in the study design, data analysis, manuscript drafting, or publication decision-making, and did not affect the objectivity of the research results.
References
1. Candel FJ, Salavert M, Estella A, et al. Ten issues to update in nosocomial or hospital-acquired pneumonia: an expert review. J Clin Med. 2023;12(20):6526. doi:10.3390/jcm12206526
2. Li Q, Zhou XS, Yang R, et al. Carbapenem-resistant gram-negative bacteria (CR-GNB) in ICUs: resistance genes, therapeutics, and prevention - a comprehensive review. Front Public Health. 2024;12:1376513. doi:10.3389/fpubh.2024.1376513
3. Infectious Diseases Society of China, Chinese Thoracic Society, Chinese Society of Critical Care Medicine. Multi-disciplinary expert consensus on the optimal clinical use of the polymyxins in China. Chin J Tuberc Respir Dis. 2021;44(04):292–12. doi:10.3760/cma.j.cn112147-20201109-01091
4. Tamma PD, Heil EL, Justo JA, et al. Infectious diseases society of America 2024 guidance on the treatment of antimicrobial-resistant gram-negative infections. Clin Infect Dis. 2024:ciae403. doi:10.1093/cid/ciae403
5. Nang SC, Azad MAK, Velkov T, et al. Rescuing the last-line polymyxins: achievements and challenges. Pharmacol Rev. 2021;73(2):679–728. doi:10.1124/pharmrev.120.000020
6. Gan Y, Yu M, Liu F, et al. Determination of polymyxin B concentration in plasma and its application in critically ill patients. China Pharm. 2023;34(06):704–709. doi:10.6039/j.issn.1001-0408.2023.06.12
7. Sandri AM, Landersdorfer CB, Jacob J, et al. Population pharmacokinetics of intravenous polymyxin B in critically ill patients: implications for selection of dosage regimens. Clin Infect Dis. 2013;57(4):524–531. doi:10.1093/cid/cit334
8. Erb CT, Patel B, Orr JE, et al. Management of adults with hospital-acquired and ventilator-associated pneumonia. Ann Am Thorac Soc. 2016;13(12):2258–2260. doi:10.1513/AnnalsATS.201608-641CME
9. Tsuji BT, Pogue JM, Zavascki AP, et al. International consensus guidelines for the optimal use of the polymyxins. Pharmacotherapy. 2019;39(1):10–39. doi:10.1002/phar.2209
10. Elias LS, Konzen D, Krebs JM, et al. The impact of polymyxin B dosage on in-hospital mortality of patients treated with this antibiotic. J Antimicrob Chemoth. 2010;65(10):2231–2237. doi:10.1093/jac/dkq285
11. Institute NC. Common Terminology Criteria for Adverse Events (CTCAE), version 5. 0. 2023.
12. Somda NS, Nyarkoh R, Kotey FCN, et al. A systematic review and meta-analysis of carbapenem-resistant Enterobacteriaceae in West Africa. BMC Med Genomics. 2024;17(1):267. doi:10.1186/s12920-024-02043-x
13. Yahav D, Farbman L, Leibovici L, Paul M. Colistin: new lessons on an old antibiotic. Clin Microbiol Infect. 2012;18(1):18–29. doi:10.1111/j.1469-0691.2011.03734.x
14. Poirel L, Jayol A, Nordmann P. Polymyxins: antibacterial activity, susceptibility testing, and resistance mechanisms encoded by plasmids or chromosomes. Clin Microbiol Rev. 2017;30(2):557–596. doi:10.1128/cmr.00064-16
15. Nie R, Li D, Wang P, Yan G, Leng B. Polymyxin B in patients with renal impairment: is it necessary to adjust dose? Front Pharmacol. 2022;13:955633. doi:10.3389/fphar.2022.955633
16. Zhang X, Qi S, Duan X, et al. Clinical outcomes and safety of polymyxin B in the treatment of carbapenem-resistant Gram-negative bacterial infections: a real-world multicenter study. J Transl Med. 2021;19(1):431. doi:10.1186/s12967-021-03111-x
17. Liu S, Wu Y, Qi S, et al. Polymyxin B therapy based on therapeutic drug monitoring in carbapenem-resistant organisms sepsis: the PMB-CROS randomized clinical trial. Crit Care. 2023;27(1):232. doi:10.1186/s13054-023-04522-6
18. Xia GL, Jiang RL. Efficacy and safety of polymyxin B in carbapenem-resistant gram-negative organisms infections. BMC Infect Dis. 2021;21(1):1034. doi:10.1186/s12879-021-06719-y
19. Salimi H, Klein RS. Disruption of the blood-brain barrier during neuroinflammatory and neuroinfectious diseases. Neuroimmune Dis. 2019;195–234.
20. Krzanowski M, Janda K, Chowaniec E, Sułowicz W. Hemodialysis vascular access infection and mortality in maintenance hemodialysis patients. Przeglad lekarski. 2011;68(12):1157–1161.
21. Lu Q, H LG, Qu Q, et al. Clinical efficacy of polymyxin B in patients infected with carbapenem-resistant organisms. Infect Drug Resist. 2021;14:1979–1988. doi:10.2147/IDR.S312708
22. Li M, Peng L, Lan G, Yu J, Li Z, Yuan H. Analysis and evaluation of the application of polymyxin B in inpatients based on clinical guidelines and consensuses. China Pharm. 2023;34(06):730–734. doi:10.6039/j.issn.1001-0408.2023.06.17
23. Zhao YC, Wang CY, Liu JY, et al. Factors affecting the effectiveness and safety of polymyxin B in the treatment of gram-negative bacterial infections: a meta-analysis of 96 articles. Int J Antimicrob Agents. 2024;64(3):107262. doi:10.1016/j.ijantimicag.2024.107262
24. Roberts DM, Sevastos J, Carland JE, Stocker SL, Lea-Henry TN. Clinical pharmacokinetics in kidney disease application to rational design of dosing regimens. Clin J Am Soc Nephro. 2018;13(8):1254–1263. doi:10.2215/Cjn.05150418
25. Matusik E, Boidin C, Friggeri A, et al. Therapeutic drug monitoring of antibiotic drugs in patients receiving continuous renal replacement therapy or intermittent hemodialysis: a critical review. Ther Drug Monit. 2022;44(1):86–102. doi:10.1097/FTD.0000000000000941
26. Fang YW, Huang CH, Jang TN, et al. Pharmacokinetic study of polymyxin B in healthy subjects and subjects with renal insufficiency. Clin Transl Sci. 2024;17(12):e70110. doi:10.1111/cts.70110
27. Moghnieh R, Husni R, Helou M, et al. The prevalence and risk factors of acute kidney injury during colistin therapy: a retrospective cohort study from lebanon. Antibiotics. 2023;12(7):1183. doi:10.3390/antibiotics12071183
28. Mariano F, Leporati M, Carignano P, Stella M, Vincenti M, Biancone L. Efficient removal of colistin A and B in critically ill patients undergoing CVVHDF and sorbent technologies. J Nephrology. 2015;28(5):623–631. doi:10.1007/s40620-014-0143-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Efficacy and Safety of Anlotinib in Extensive-Stage Small Cell Lung Cancer: A Multicenter Real-World Study
Zheng HR, Jiang AM, Gao H, Liu N, Zheng XQ, Fu X, Zhang R, Ruan ZP, Tian T, Liang X, Yao Y
Cancer Management and Research 2022, 14:2273-2287
Published Date: 2 August 2022
Relative Safety and Efficacy of Two Doses of Tandospirone Citrate for Generalized Anxiety Disorder: A Multicenter Randomized Controlled Trial
Li Q, Zhang H, Lin G, Shi S, Zhang Y, Ji J, Yang L, Yao J, Wu W
Neuropsychiatric Disease and Treatment 2022, 18:1653-1664
Published Date: 8 August 2022
Biosimilars: Science, Implications, and Potential Outlooks in the Middle East and Africa
Batran RA, Elmoshneb M, Hussein AS, Hussien OM, Adel F, Elgarhy R, Morsi MI
Biologics: Targets and Therapy 2022, 16:161-171
Published Date: 6 October 2022
Efficacy and Safety of Empagliflozin in Patients with Type 2 Diabetes Mellitus Fasting During Ramadan: A Real-World Study from Bangladesh
Pathan MF, Akter N, Selim S, Saifuddin M, Qureshi NK, Kamrul-Hasan ABM, Hannan MA, Ahmed MAU, Mustari M, Chakraborty AK
Diabetes, Metabolic Syndrome and Obesity 2022, 15:4011-4021
Published Date: 22 December 2022
Clinical Evaluation of Risankizumab in the Treatment of Adults with Moderately to Severely Active Crohn’s Disease: Patient Selection and Reported Outcomes
Horst S, Cross RK
Drug Design, Development and Therapy 2023, 17:273-282
Published Date: 31 January 2023