")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Efficacy and Safety of Empagliflozin in Patients with Type 2 Diabetes Mellitus Fasting During Ramadan: A Real-World Study from Bangladesh
Authors Pathan MF , Akter N , Selim S, Saifuddin M, Qureshi NK , Kamrul-Hasan ABM , Hannan MA, Ahmed MAU, Mustari M , Chakraborty AK
Received 4 August 2022
Accepted for publication 15 November 2022
Published 22 December 2022 Volume 2022:15 Pages 4011—4021
DOI https://doi.org/10.2147/DMSO.S380544
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Juei-Tang Cheng
MD Faruque Pathan,1 Nazma Akter,2 Shahjada Selim,3 M Saifuddin,4 Nazmul Kabir Qureshi,5 ABM Kamrul-Hasan,6 Mohammad Abdul Hannan,7 Md Ashraf Uddin Ahmed,1 Marufa Mustari,3 Ashish Kumar Chakraborty1
1BIRDEM General Hospital, Dhaka, Bangladesh; 2MARKS Medical College & Hospital, Dhaka, Bangladesh; 3Bangabandhu Sheikh Mujib Medical University, Dhaka, Bangladesh; 4Dhaka Medical College, Dhaka, Bangladesh; 5National Healthcare Network, Dhaka, Bangladesh; 6Mymensingh Medical College & Hospital, Mymensingh, Bangladesh; 7North East Medical College & Hospital, Sylhet, Bangladesh
Correspondence: MD Faruque Pathan, BIRDEM General Hospital, 122 Kazi Nazrul Islam Avenue, Dhaka, 1000, Bangladesh, Tel +8801713032888, Email [email protected]
Aim: In Bangladesh, there is a large population of Muslims with type 2 diabetes mellitus (T2DM) who fast during Ramadan. Changes in the pattern of meal and fluid intake during this long-fasting hours may increase the risk of hypoglycaemia, hyperglycaemia, and dehydration. Our key point of focus was to evaluate the efficacy and safety of Empagliflozin, a sodium-glucose co transporter 2 inhibitor (SGLT2i), in patients with T2DM while fasting during Ramadan.
Methods: This was a 24-weeks, multi-centre, open-label, two-arm parallel-group study. In this prospective type of observational study, we enrolled patients taking Empagliflozin and Metformin with or without a DPP-4 inhibitor in one group (n = 274) and a parallel group (n = 219) who were treated with Metformin with or without a DPP-4 inhibitor. The primary endpoint of this study was HbA1c reduction, weight loss and the number of reported or symptomatic hypoglycemic events. In secondary endpoints, we evaluated the changes from baseline in blood pressure, estimated glomerular filtration rate (eGFR), serum creatinine, and serum electrolyte, the proportion of volume depletion (≥ 1 event) and incidence of other adverse events (AEs) of interest potentially related to SGLT2 inhibitor.
Results: During Ramadan, HbA1c reduction was significant in Empagliflozin arm (− 0.49% vs − 0.12%); [p < 0.001]. From before to the end of the study, significant weight reduction was seen in the Empagliflozin arm (− 1.4 kg vs − 0.09 kg); [p < 0.001]. We observed no significant increase in the incidence of hypoglycemia (0.7% vs 0.4%, p = 0.267) and volume depletion (2.6% vs 1.8%; p = 0.55) in both arm. All these milder forms events did not require any hospital admission. There was no report of serious adverse events or any discontinuation, or reduction of prescribed doses of empagliflozin during Ramadan.
Conclusion: Empagliflozin is efficacious and safe for treating adults with T2DM during Ramadan.
Keywords: empagliflozin, Ramadan, efficacy, safety, T2DM, SGLT2i, SGLT2 inhibitors
Introduction
There are about 116 million Muslims with diabetes worldwide.1–5 Most Muslims fast during the holy month of Ramadan despite high risk and are exempted from fasting, according to Quran and Fiqh.6–8 During this fasting period, Muslims abstain from food and drink, including oral medications, from dawn to dusk. The population-based Epidemiology of Diabetes and Ramadan (EPIDIAR) and CREED studies showed that patients with type 2 diabetes mellitus (T2DM) who fasted during the month of Ramadan were at 7.5 times higher risk of developing hypoglycemia and 5 times higher risk of hyperglycemia.6,7 Since 2005, the American Diabetes Association (ADA) and other international bodies have recommended risk stratification during Ramadan, and focus education programs at least 3 months before Ramadan. A physician must respect the patient’s desire to fast despite falling into the high-risk or very high-risk groups and counsel to reduce the risks. In addition to changes in meal time and, patterns, and physical activities, most subjects with diabetes need to continue antidiabetic medications with modifications to avoid hypoglycemia.9–12 The risk varies according to the oral antidiabetic agent.6,7 Many clinical trials have assessed the safety of various pharmacological diabetes treatments during Ramadan. Certain anti-diabetic agents like sulphonylurea (SU) that promote insulin secretion may cause hypoglycemia with potentially serious or life-threatening consequences.13 The UK VECTOR study revealed that 41.7% of patients receiving sulphonylurea developed hypoglycemia.14 Rare hypoglycemia events were reported in patients receiving sitagliptin and vildagliptin compared with various SU in combination therapy with metformin.15–17 Short-acting insulin secretagogues, such as repaglinide and nateglinide, are effective with a low risk of hypoglycemia during fasting, particularly given their short duration of action.18 Thiazolidinediones (TZDs), such as pioglitazone, have long been regarded as a safe agent during Ramadan because of their low risk of hypoglycemia; however, long-term treatment has been associated with fluid retention, peripheral edema, and weight gain.19 Hypoglycemia occurs more commonly with insulin therapy and often has life-threatening consequences.20 Oral antidiabetic agents with insulin-independent mechanisms may be ideal for patients who intend to fast during Ramadan or at other times throughout the year to avoid weight gain and hypoglycemia.21
Sodium-glucose cotransporter 2 (SGLT2) is the major transport protein in renal proximal convoluted tubules to regulate glucose reabsorption and SGLT2 inhibitor decreases renal glucose reabsorption, thereby increasing urinary glucose excretion and reduce hyperglycemia.22 Empagliflozin (Jardiance) is part of this oral hypoglycemic agents (SGLT2 inhibitors), which also include canagliflozin (Invokana) and dapagliflozin (Farxiga).23–25 Empagliflozin has been approved for type 2 diabetes as either mono therapy or as an add-on therapy.26 This drug is reported to reduce glycated hemoglobin levels in patients with type 2 diabetes without undue concerns regarding the development of hypoglycemia in treated patients, including those with stage 2 or 3a chronic kidney disease.21
Empagliflozin has exhibited a competent efficacy and safety profile in a wide range of patients with T2DM. Empagliflozin is highly selective for the SGLT2 over SGLT1 receptors, potentially minimizing off-target effects. While the insulin-independent mechanism of SGLT2 inhibitors leads to a low inherent risk of hypoglycemia, the mild osmotic diuresis may be associated with an increased risk of volume–depletion events, including dehydration.21,26 Two studies using the same population of patients also showed a decrease of selected inflammatory mediators in subjects treated with SGLT-2i compared to those treated with sulphonylureas and reaching the glycemic equipoise.27
The published EMPA-REG and CANVAS trials have reported additional benefits of SGLT2 inhibitors on cardiovascular and renal outcomes among patients with T2DM and increased cardiovascular risk.24,25 Physicians across the globe now are considering this agent as an essential component in treatment algorithms, considering the potential benefit beyond glycemic control.8,9
Rationale
The efficacy and safety of canagliflozin and dapagliflozin during Ramadan fasting in patients with T2DM have been studied previously.28,29 But data on empagliflozin in this regard are still not available. Most of the population in Bangladesh are Muslim, who religiously fast during Ramadan.30 There is an unmet need to evaluate the efficacy and safety of empagliflozin during Ramadan fasting.
This study aimed to evaluate the efficacy and safety of Empagliflozin in patients with T2DM during Ramadan fasting. The primary objective was to assess the efficacy and safety of Empagliflozin in terms of HbA1c (%), weight loss (kg) and hypoglycemia (number of events) when used to treat patients observing Ramadan fasting. Secondary objectives were to assess volume–depletion events (symptomatic or confirmed event of dehydration or hypovolemia), to evaluate changes in blood pressure (mm Hg), eGFR (mL/min) and to observe adverse events potentially related to SGLT2i (eg, urinary tract infection, or genital mycotic infections).
Methods
The study was performed in compliance with the principles of the Declaration of Helsinki, the International Conference of Harmonization Guideline for Good Clinical Practice, and applicable regulatory requirements. All participants provided written informed consent. The study received ethical permission from the Diabetic Association of Bangladesh (reference number BADAS-ERC/EC/20/00301).
Study Design
This was a real-world, multi-centre, open-label, two-arm parallel-group study. It was conducted during Ramadan of 2021 at the Diabetes out-patient department of respective authors and contributors. In this prospective observational study, we enrolled patients in two groups according to treated with Empagliflozin or not and followed-up for 24-weeks.
Eligibility Criteria
Inclusion Criteria
Adults who had a confirmed diagnosis of T2DM for at least 12 months before enrolment, aged >18 years, who intended to fast during the month of Ramadan without any contraindication to fast; and having inadequately controlled glycemic status (HbA1c%: >7.0% to ≤10%), eGFR >45 mL/min/1.73m2 and had been treated with Empagliflozin on a background therapy of Metformin with or without DPP-4 inhibitor for the last 3 months before enrolment or those who had been treated with Metformin with or without DPP-4 inhibitor for the last 3 months approximately before enrolment were included into this study.
Potentially interested adults were screened 12 weeks before enrolling in the pre-Ramadan period (4 weeks before the onset of Ramadan). During enrollment, patients were entered into one of two parallel treatment cohort groups (>200 patients in each group) based on their ongoing T2DM therapy as follows [Figure 1].
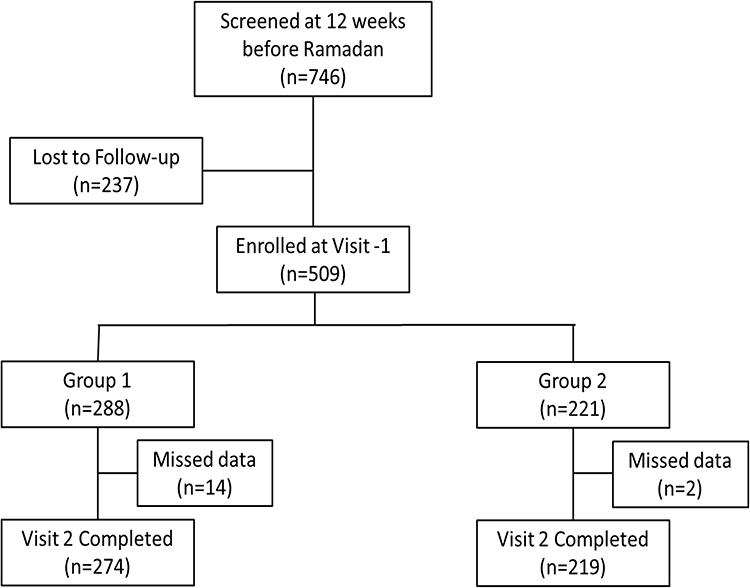 |
Figure 1 Patient disposition. |
Group 1(Empagliflozin Group): Patients treated with Empagliflozin (10 mg or 25 mg/day) and Metformin (>1000 mg/day) with or without a DPP-4 inhibitor (sitagliptin 100mg or vildagliptin 100 mg or linagliptin 5mg/day).
Group 2(Non-Empagliflozin Group): Patients treated with Metformin (>1000 mg/day) with or without a DPP-4 inhibitor (sitagliptin 100 mg or vildagliptin 100 mg or linagliptin 5mg/day).
Exclusion Criteria
Patients with T1DM, pregnant or breastfeeding mothers, patients who were treated with insulin, sulphonylurea or any other antidiabetic therapy other than Empagliflozin, Metformin and DPP4i, with a history of severe hypoglycemic events or having a history of severe volume depletion events within the 6 months before enrolment, with history of diabetic ketoacidosis, having an estimated glomerular filtration rate (eGFR) <45 mL/min/1.73m2 or alanine transaminase levels >2.5 times the upper normal limit, having a history of recurrent urinary tract infections, malignancy, cardiovascular events within the last 90 days before enrolment, or having any contraindication for Ramadan fasting were excluded from the study.
Patients were enrolled with clinical and biochemical test records at the first visit during Pre-Ramadan (4 weeks before Ramadan month). Patients were counseled on a meal plan, physical activities, home blood glucose monitoring, when to break the fast, and drug modification during fasting. Every patient was guided adequately to maintain a log book for 30 days to record blood glucose profile, hypoglycemia events (either symptomatic or recorded, or need any assistance) and other adverse effects like genitourinary infection, hypotension, or dizziness (either symptomatic or reported). The second visit was scheduled during post-Ramadan (up to 4 weeks after the end of the Ramadan month) with clinical and advised biochemical tests.
Initially, 746 patients were screened; later, 509 patients were enrolled (visit 1). Data were recorded in a pre-formed standard printed data collection form after explaining the study purpose and procedure and taking informed consent of study participants. All co-researchers were trained properly, and the data collection procedure was briefed before the commencement of this study in multiple small group discussions. After data editing and cleaning, a total of 493 patients who completed the first and second visits (274 in group 1:Empagliflozin Group and 219 in group 2:Non-Empagliflozin Group) were included in the final statistical analysis. Due to the COVID outbreak, some changes were made in the study protocol [mentioned in “Study Amendment, Section 12”], which states that due to the COVID-19 outbreak, many enrolled patients could not visit their investigators for post-Ramadan follow-up. Therefore, the follow-up data were collected digitally by phone or WhatsApp.
Operational Definition and Study Tools
During Pre-Ramadan and Post-Ramadan periods in both groups-
Participants were examined regarding
Height: Standing height was measured in centimetres (cm) using a stadiometer and height rod. Height was documented to the nearest 1 mm. The lower reading was recorded when the reading fell between two values.
Weight: Weight was measured in kilograms from a standard measuring device after placing it on a hard flat surface, and zero balance was checked before measurement. Weight was measured at the nearest 0.5 kg.
BMI: The BMI of participants was calculated by dividing weight by kg with the square of height in meters using the formula kg/m2. BMI: As defined for the Asia-Pacific population by the Western Pacific Regional Office of the WHO, BMI was classified as follows: BMI <18.50 kg/m2: underweight; BMI 18.50–22.99 kg/m2: Normal; BMI 23.0–27.49 kg/m2: Overweight, and BMI 27.5.0 kg/m2: Obesity.31
Systolic Blood Pressure (SBP) and Diastolic blood pressure (DBP): Two readings of systolic blood pressure and diastolic blood pressure were taken, using a standard zero mercury sphygmomanometer after at least 10–15 min of rest. After that, the average of the two readings was obtained.32
The following events were noted
Hypoglycemia: It has been defined as a plasma glucose value ‚<70 mg/dL (<3.9 mmol/L), and severe hypoglycemia is defined as an event of hypoglycemia characterized by altered mental and/or physical status requiring assistance for recovery.33,34 Hypoglycaemia episodes include symptomatic episodes (ie, symptoms of dizziness, visual blurring, palpitations, nausea, sweating, confusion, tremor, or intense hunger with or without biochemical confirmation); biochemically confirmed episodes (ie, self-monitored blood glucose measurement of <3.9 mmol/L with or without symptoms); and severe episodes (ie, episodes for which the patient required assistance from another person or that resulted in seizure or loss of consciousness).29
Volume depletion: Volume depletion is characterized by a reduction in extracellular fluid volume that occurs when salt and fluid losses exceed intake on a sustained basis,34 symptoms of hypotension, orthostatic hypotension, postural dizziness, dehydration, syncope, or presyncope.29
UTI: A urinary tract infection (UTI) is an infection in any part of the urinary system (kidneys, ureters, bladder and urethra). Most infections usually involve the lower urinary tract.35
Other adverse events: An unexpected medical problem was recorded during treatment with a drug or other therapy. Adverse events may be mild, moderate, or severe and may be caused by something other than the drug or therapy.36
Laboratory Investigations
Following Laboratory Investigations Were Done
A blood sample of 10 mL was collected through venipuncture from each participant after fasting for 10 h into vacutainer tubes containing EDTA. The samples were kept at room temperature and transported within 2 h to a certified laboratory. Glycosylated haemoglobin (HbA1c) was analyzed using a high-performance liquid chromatography method. Other biochemical values such as sodium, potassium, creatinine, electrolytes, and eGFR were also measured. Serum creatinine levels were measured with the calorimetric Jaffe method.32,37 Estimated GFR was calculated using the MDRD equation and the CKD-EPI formula.
Endpoints
The Primary endpoints of This Study were
1. Reduction of HbA1c
2. Weight loss and
3. Hypoglycemia.
The Secondary Endpoints of This Study were
Changes from baseline in blood pressure (SBP, DBP), eGFR, serum creatinine, serum electrolyte, the proportion of patients with volume depletion (≥1 event) and incidence of other AEs of interest potentially related to SGLT2 inhibition (including urinary tract infections, genital mycotic infection, and osmotic diuresis–related AEs).
Statistical Analysis
Data were analyzed with SPSS Inc, Chicago, Illinois, USA software version 25. The means and standard deviations were used to describe continuous data. For categorical data, frequencies and percentages were estimated. Categorical variables were compared with each other using the chi-square test. Among the basic characteristics of the studied participants, the continuous variables were compared with each other using the ANOVA test. For parametric parameters paired t-test was used to analyze the changes in clinical and biochemical parameters before and after Ramadan. Statistical significance was set at P < 0.05. The model had a change in parameters as the dependent variable, treatment as a fixed effect and parameters as a covariate.
Results
Among 509 participants; 493 (96.85%) participants completed the study. 274 patients from Empagliflozin Group and 219 patients from Non-Empagliflozin Group were found to have completed two visits with all data (Figure 1).
Demographics
The mean age of the study participants was 49.0±11.8 (SD) and 49.7±10.5 (SD) years in Group 1 and 2, respectively. Among the studied population, sex ratio was 0.95 and 0.76 in Empagliflozin and non-Empagliflozin Group, respectively. Demographic and baseline characteristics in between this group are mentioned in Table 1.
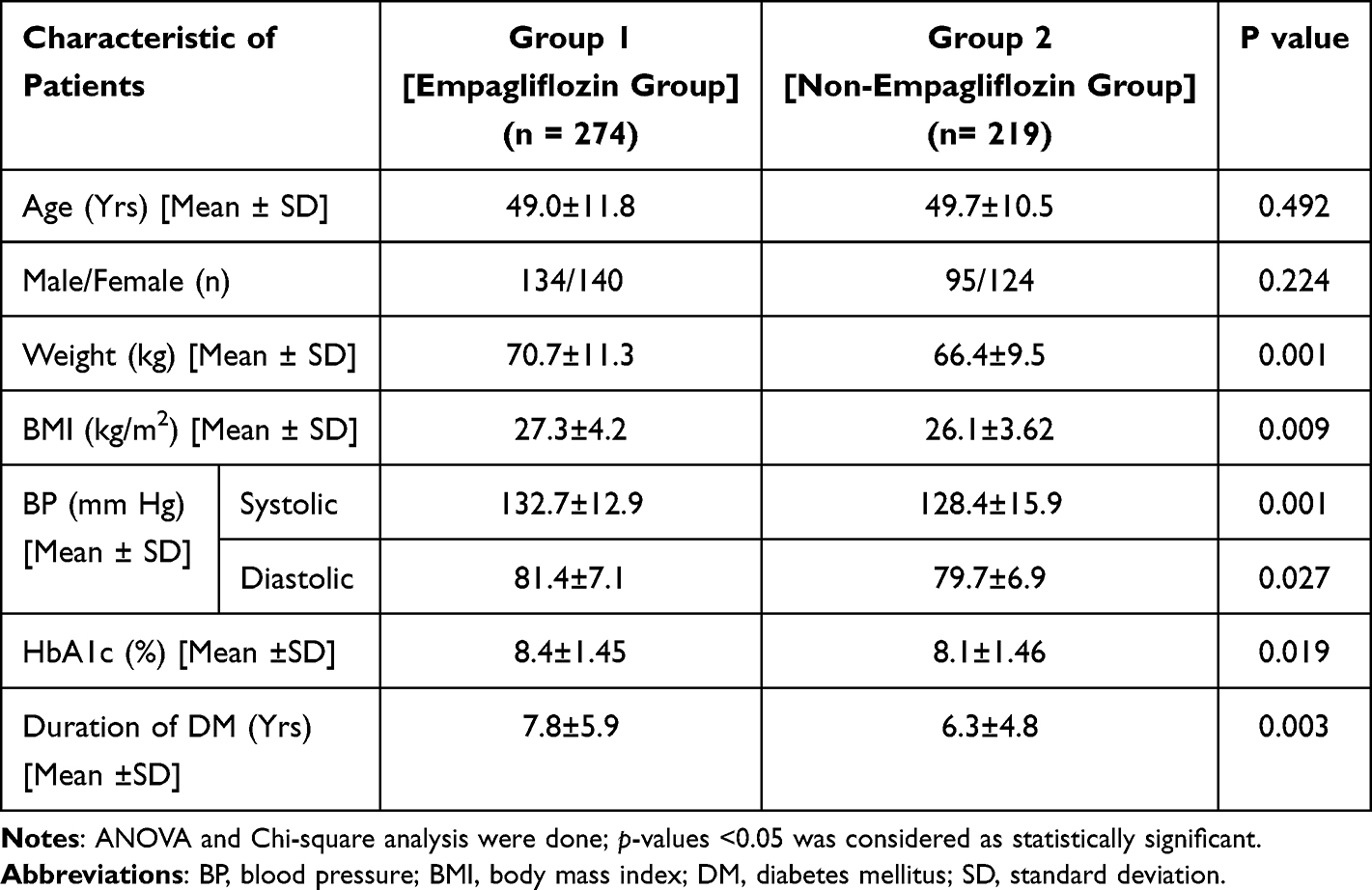 |
Table 1 Demographic and Baseline Characteristics |
Usage Pattern
274 (55.57%) participants received Empagliflozin and Metformin with or without DPP4i, whereas 219 (44.42%) participants received Metformin and DPP4i.
Efficacy Evaluation
- Efficacy Endpoints:
- Effect of HbA1c: The mean change in HbA1c (%) from before to the end of the study was 0.49% and 0.1% in Empagliflozin Group and non-Empagliflozin Group, respectively; (p < 0.001). The difference in HbA1c (%) between both groups was 0.3%. (95% CI −0.56 to −0.28) [Table 2].
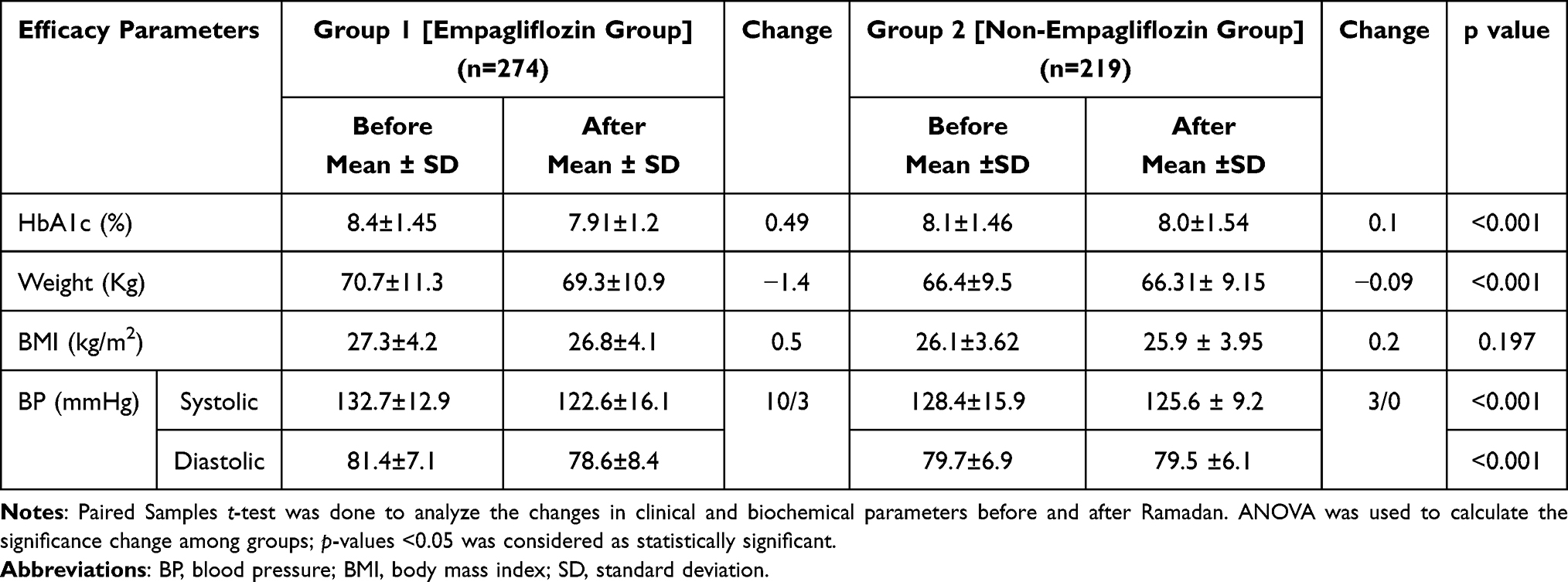 |
Table 2 Mean Change in Efficacy Parameters in Studied Population |
In Empagliflozin Group, 25.91% of subjects could achieve good glycemic control (HbA1c <7%), whereas before Ramadan, that was 10.58%; (p < 0.05 value); [Table 3].
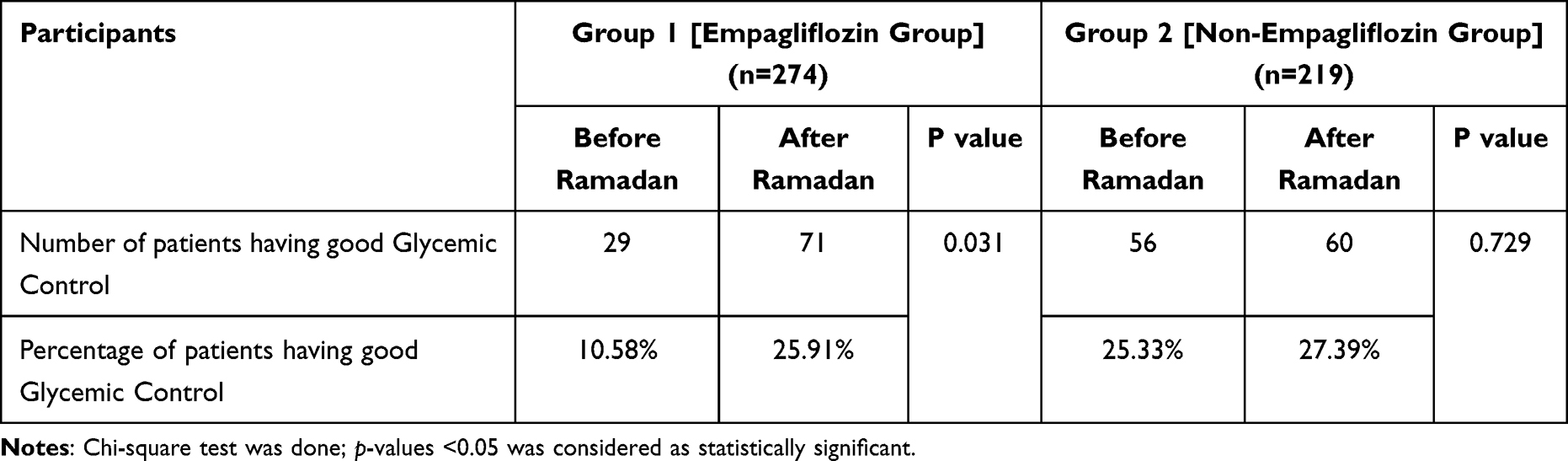 |
Table 3 Participants Having Good Glycemic Control (HbA1c <7%) |
No subjects in either treatment arm reported any serious adverse events during the study, and no meaningful differences were observed between the treatment arm [Table 4].
- Effect on hypoglycaemia: Two patients (0.7%) in Empagliflozin Group and one (0.4%) in non-Empagliflozin Group reported confirmed hypoglycemia during Ramadan. However, this difference was not statistically significant; (p = 0.26).
- Urinary Tract infection: Six subjects (2.1%) reported UTI in Empagliflozin Group, and four (1.8%) reported the same in non-Empagliflozin Group; (p = 0.81).
- Volume depletion: Symptomatic volume depletion was reported in seven (2.6%) subjects in Empagliflozin Group and four (1.8%) in non-Empagliflozin Group; (p = 0.55). Three reported a reduction in blood pressure; others reported symptoms like vertigo, increased thirst, nausea, and headache.
- Effect on Blood Pressure: Blood pressure was also seen to be significantly reduced by 10/3 mm Hg in Empagliflozin Group than non-Empagliflozin Group (p < 0.001); [Table 2].
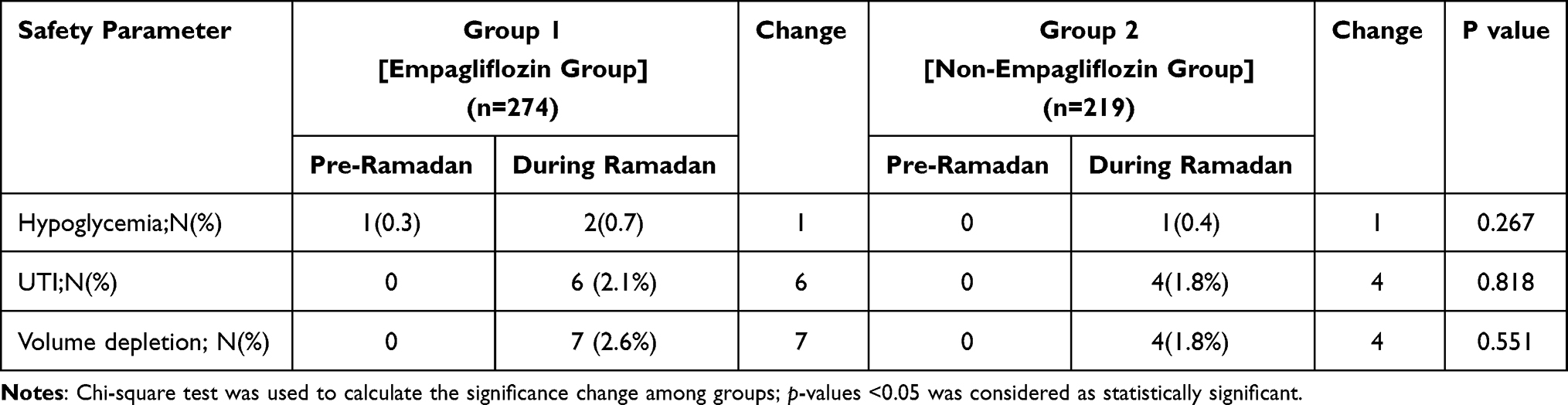 |
Table 4 Changes in Safety Parameters in Studied Population |
Laboratory Parameters
No deterioration of renal function was found during fasting in both groups. Both the treatment groups showed no significant changes in biochemical parameters like Na, K, Cl, HCO3, eGFR or creatinine levels [Table 5].
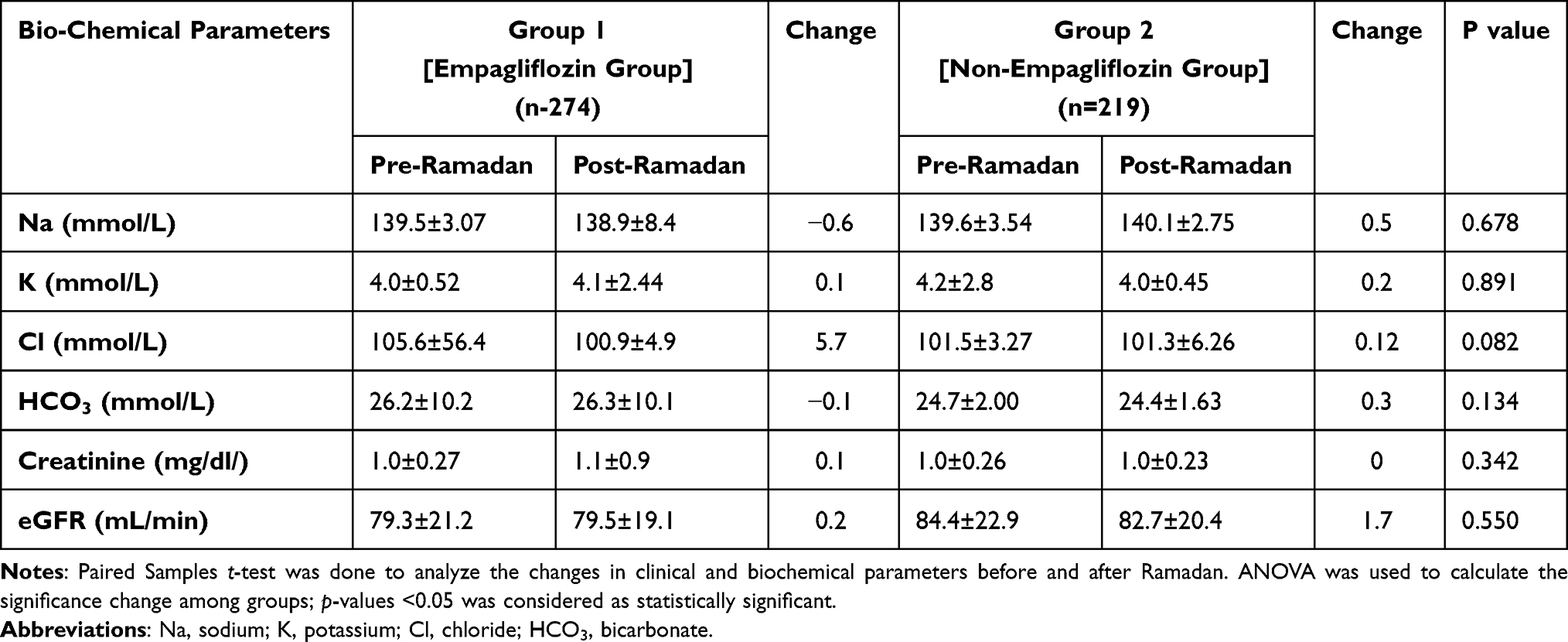 |
Table 5 Changes in Laboratory Parameters |
Compliance and Adherence
All the subjects continued the drug regime as prescribed. Some of the confirmed hypoglycemic events were due to missed Suhoor meal, and other was due to acute enteritis. Hypoglycemic events and volume depletion symptoms were mild and did not require any hospital admission. Patients with confirmed hypoglycemia (two patients in Empagliflozin Group and one in non-Empagliflozin Group) and volume depletion symptoms, ie, hypotension, dizziness (two patients in the Empagliflozin group and four in the non-Empagliflozin group) broke the fast on a single occasion; (p = 0.52). There were no reports of discontinuation, dose change, or reduction of prescribed doses of antidiabetic drugs during Ramadan. All these patients continued their fast following counselling for a proper meal plan and sufficient water intake during the non-fasting hours. The other subjects completed the Ramadan fast.
Discussion
During Ramadan fasting, patients with diabetes and high or very high-risk status are well known to have the risk of hypoglycemia, particularly during the day, unnoticed hyperglycemia, especially at night, dehydration and diabetic ketoacidosis. It is therefore important to choose an evidence-based recommended antidiabetic agent, which usually does not cause hypoglycemia, thus compelling the patient to break the fasting. In this context, SGLT2 inhibitors have demonstrated effective glycemic control, weight reduction, and cardiac and renal benefits without the risk of hypoglycemia.28,29 SGLT2i are well tolerated and safe in the elderly and appear as an effective therapeutic option, though some caution is also suggested, especially in more fragile subjects.38 In our study, empagliflozin treated patient had a mean age of 49.0±11.8 years with a sex ratio of 0.95 and mean duration of diabetes of 7.8±5.9 years.
In our study, Empagliflozin during Ramadan fasting was associated with a significant reduction in HbA1c from baseline to the end of the study (Empagliflozin Group vs non-Empagliflozin Group: 0.49% vs 0.1%; p < 0.001). A greater number of patients achieved HbA1c <7%, from 10.58% at baseline to 25.91% in Empagliflozin Group), whereas there was no significant change in Group 2 (25.33% to 27.39%). A similar statistically significant reduction of HbA1c was also found in the CRATOS comparing the canagliflozin and SU group (0.4% vs 0.2%).29 However, Wan et al did not notice any difference in HbA1c reduction.28 Bashier et al reported a significant reduction in HbA1c from baseline in the SGLT2-I plus insulin and SGLT2-I plus oral antidiabetic drugs (8.2–1.5% vs 7.4–1.4%, respectively, p < 0.001).39 Abdelgadir et al also showed a significant improvement in HbA1c from 7.95 ± 1.1% to 7.6 ± 1.1%, p = 0.028) in SGLT2 inhibitor group without improvement non-SGLTi group (7.7 ±1.0% to 7.6 ± 1.0%, p = 0.56).39
In our study, weight reduction from baseline was numerically higher in Empagliflozin Group (70.7± 11.3kg vs 69.3 ± 10.9kg, a difference of 1.4%) compared to non-Empagliflozin Group (66.4±9.5kg vs 66.31 ±9.15 kg, difference 0.09%). Body weight reduction was also observed in the CRATOS study.29 Basheir et al also reported a mean reduction in weight (83.9 ±17 kg vs83.8 ±10.6 kg.34 On the other hand, Abdulgadir et al did not find weight reduction in their study.40
We found a non-significant reduction in BMI from baseline in Empagliflozin Group, whereas no change was found in non-Empagliflozin Group (27.3 ± 4.2 to 26.8 ± 4.13; vs 26.1 ± 3.62 to 25.9 ± 3.95). But, Wan et al and Shao et al did find any reduction in BMI in their study.28,41
We also observed a reduction in both systolic and diastolic blood pressure in the Empagliflozin group (132.7/81.4 and 122.6/78.6 mm Hg before and after Ramadan); (p < 0.001) and in the non-Empagliflozin group (128.4/79.7 and 125.6/79.5 mm Hg before and after Ramadan); (p < 0.001) which is also consistent with CRATOS study.29 No reduction in blood pressure was documented in some other studies.40,41
In our study, only two patients in the Empagliflozin group (Group 1) and one in the non-Empagliflozin group (Group 2) reported hypoglycemia during the fasting period. They broke the fast on that single occasion. In two patients, the hypoglycemic events were mild and were confirmed by SMBG <3.9 mmol/L, and another reported non-confirmed symptoms of hypoglycemia. But none of them required any hospital admission. A similar lower incidence of hypoglycemia was reported (6 vs 45 episodes in the canagliflozin group vs SU group, respectively) in CRATOS study.29 Flash glucose monitoring by Abdelgadir et al revealed a few events of less severe hypoglycemia in the afternoon in the SGLT2 inhibitor group.40 Bashier et al also showed that confirmed and severe hypoglycemia was higher in the SGLT2 inhibitor plus insulin group than in the SGLT2 inhibitor plus oral antidiabetic drug.39
Eleven patients reported having volume depletion (a symptom of postural giddiness). Of them, seven (2.6%) were in the Empagliflozin group and four (1.8%) in the non-Empagliflozin group. Three reported a reduction in blood pressure; others showed symptoms like vertigo, increased thirst, nausea, and headache. Volume depletion symptoms were mild, and among them, only six people broke fast (two patients in the Empagliflozin group and four in the non-Empagliflozin group) on a single occasion. In the study by Basheir et al, 9.3% of patients also reported volume depletion.39 A higher incidence of volume depletion was observed (8.6% vs 3.0%) by Shao et al.41 Of the total events of volume depletion reported by Hassanein et al, 86.3% (44/51) were in the canagliflozin group and 76% (10/13) in the SU group based on symptoms of dehydration.29 In the Shao et al study, 8.6% complained of postural giddiness.41
We observed six (2.1%) cases of genitourinary infection in the Empagliflozin group and four (1.8%) cases reported UTI in the non-Empagliflozin group. Practicing personal hygiene using the wet method might have caused a lower incidence of UTIs in our study. Only one case of UTI was reported in the CRATOS study.29
No significant change or deterioration of renal function (eGFR and serum creatinine) was found in our study in both groups during the fasting period. A similar finding was also observed in CRATOS as well by Abdelgadir et al29,40 Shao et al also did not find a significant change in eGFR in their participants during the fasting period.41
Limitations
There is a large number of patients who use insulin and secretagogues along with SGLT2 inhibitors during fasting Ramadan. So a further study is warranted on subjects receiving insulin and secretagogues. Though current guidelines recommend for three blood pressure measurements. But in our study, blood pressure has been measured twice rather thrice according to older guideline. Due to the Covid-19 pandemic situation, follow-up was done over the telephone, which could alter the reporting.
Conclusion
Our prospective study findings suggest that the use of Empagliflozin for the treatment of adults with T2DM is efficacious and safe during Ramadan with no significant increase in hypoglycemia and hypovolemia compared with non-Empagliflozin group. Moreover, continuing Empagliflozin can reduce HbA1c and weight and maintain blood pressure during Ramadan fasting.
Contributing Investigators
Dr. Mohaiminul Abedin, Dr. Md. Jahangir Alam, Dr. Mohammad Motiur Rahman, Dr. Md. Shakhawat Hussain, Dr. Dulal Chandra Ray, Dr. Saila Mazed, Dr. Minakshi Gupta, Dr. Mana Banik, Dr. Rozina Begum Chaya, Dr. Fariba Rashid, Dr. Pronab Choudhury, Dr. Biswajit Ray Chowdhury, Dr. Shahanaz Begum, Dr. Abdullah Al Mamun, Dr. Lalit Mohan Nath, Dr. S. M. Hasan Murad, Dr. Uttam Kumar Dey.
Acknowledgments
All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work, and have given final approval for the version to be published. The authors thank Dr Punit Srivastava of Mediception Science Pvt. Ltd (www.mediception.com) for providing medical writing support during the preparation of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation. All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. International Diabetes Federation. IDF Diabetes Atlas. Brussels, Belgium: International Diabetes Federation; 2021.
2. Lipka M, Hackett C. Why Muslims are the World Growing Religious Group. Pew Research Center; 2017.
3. Center Pew Research. The future of world religions: population growth projections; 2010–2060. Available from: http://www//Pewqforum.org/2017.
4. International Diabetes Federation. Diabetes and Ramadan: practical guidelines. International Diabetes Federation (IDF), in collaboration with the Diabetes and Ramadan (DAR) International Alliance; 2016. Available from: http://www.idf.org/sites/default/files/IDF-DAR-Practical-Guidelines-Final-Low.pdf.
5. Hassan A, Meo SA. Diabetes during Ramadan: underestimated, under-investigated, needs more attention. Eur Rev Med Pharmacol Sci. 2014;18(22):3528–3533.
6. Salti I, Bénard E, Detournay B, et al. A population-based study of diabetes and its characteristics during the fasting month of Ramadan in 13 countries: results of the Epidemiology of Diabetes and Ramadan 1422/2001 (EPIDIAR) study. Diabetes Care. 2004;27:2306–2311. doi:10.2337/diacare.27.10.2306
7. Babineaux SM, Toaima D, Boye KS, et al. Multi-countries retrospective observational study of management and outcomes of patients with type 2 diabetes during Ramadan in 2010 (CREED). Diab Med. 2015;32(6):819–828. doi:10.1111/dme.12685
8. Beshyah SA. Fasting during month of Ramadan for people with Diabetes: medicine and Fiqh united at last. IJMBS. 2009;1:58–60.
9. Al-Arouj M, Bouguerra R, Buse J, et al. Recommendations for management of diabetes during Ramadan. Diabetes Care. 2005;9:2301–2311.
10. Al-Arouj M, Assaad-Khalil S, Buse J, et al. Recommendations for management of diabetes during Ramadan: update 2010. Diabetes Care. 2010;33(8):1895–1902. doi:10.2337/dc10-0896
11. International Diabetes Federation and DAR international Alliance. Diabetes and Ramadan: practical guidelines 2021. Brussels, Belgium: IDF; 2021. Available from: www.daralliance.org.
12. Ahmedani MY, Zainudin SB, Alozairi ZE. Pre-Ramadan Assessment and Education. Diabetes and Ramadan Practical Guidelines 2021. International Diabetes Federation and DAR International Alliance; 2021:122–130.
13. Aravind S, Tayeb KA, Ismail SB, et al. Hypoglycemia in sulphonylurea-treated subjects with type 2 diabetes undergoing Ramadan fasting: a five country observational study. Curr Med Res Opin. 2011;27(6):1237–1242. doi:10.1185/03007995.2011.578245
14. Hassanein M, Hanif W, Malik W, et al. Comparison of the dipeptidyl peptidase-4 inhibitor vildagliptin and the sulphonylurea gliclazide in combination with Metformin, in Muslim patients with type 2 diabetes mellitus fasting during Ramadan: results of the VECTOR study. Curr Med Res Opin. 2011;27:1367–1374. doi:10.1185/03007995.2011.579951
15. Al Safri S, Basiounny A, Echtay A, et al. The incidence of hypoglycemia in Muslim patients with type 2 diabetes treated with sitagliptin or a sulphonylurea during Ramadan: a randomized trial. Int J Clin Pract. 2011;65(11):1132–1140. doi:10.1111/j.1742-1241.2011.02797.x
16. Al Arouj M, Hassoun AAK, Medlej R, et al. The effect of vildagliptin relative to sulphonylurea in Muslim patients with type 2 diabetes fasting during Ramadan: the Virtue study. Int J Clin Pract. 2013;67(10):957–963.
17. Hassanein M, Abdallah K, Schweizer A. A double-blind, randomized trial including frequent physician-patient contacts and Ramadan focused advice, assessing vildagliptin and gliclazide in patients with type 2 diabetes fasting during Ramadan: the STEADFAST study. Vasc Health Risk Manag. 2014;10:319–325. doi:10.2147/VHRM.S64038
18. Mafauzy M. Repaglinide versus glibenclamide treatment of Type 2 diabetes during Ramadan fasting. Diabetes Res Clin Pract. 2002;58:45–53. doi:10.1016/S0168-8227(02)00104-3
19. Jain R, Osei K, Kupfer S, Perez AT, Zhang J. Long-term safety of pioglitazone versus glyburide in patients with recently diagnosed type 2 diabetes mellitus. Pharmacotherapy. 2006;26:1388–1395. doi:10.1592/phco.26.10.1388
20. Hajjaji IM, Eshwihdi N, Barrowman N. Comparison of analog insulin mix 50:50 with human insulin mix 30:70 in persons with type 2 diabetes during Ramadan. Inter J Clin Pract. 2019;73(6):e13348. doi:10.1111/ijcp.13348
21. Häring HU, Merker L, Seewaldt-Becker E, et al. Empagliflozin as add-on to metformin plus sulfonylurea in patients with type 2 diabetes: a 24-week, randomized, double-blind, placebo-controlled trial. Diabetes Care. 2013;36:3396–3404. doi:10.2337/dc12-2673
22. Gallo LA, Wright EM, Vallon V. Probing SGLT2 as a therapeutic target for diabetes: basic physiology and consequences. Diab Vasc Dis Res. 2015;12:78–89. doi:10.1177/1479164114561992
23. McGill JB. The SGLT2 inhibitor empagliflozin for the treatment of type 2 diabetes mellitus: a bench to bedside review. Diabetes Ther. 2014;5:43–63. doi:10.1007/s13300-014-0063-1
24. Zinman B, Wanner C, Lachin JM, et al.; Investigators of EMPAREG outcome. Empagliflozin, cardiovascular outcomes, and mortality in type 2 diabetes. N Engl J Med. 2015;373(22):2117–2128. doi:10.1056/NEJMoa1504720
25. Neal B, Perkovic V, Mahaffey KW, et al. Canagliflozin and cardiovascular and renal events in type 2 diabetes PubMed PMID: 28605608. N Engl J Med. 2017;377(7):644–657. doi:10.1056/NEJMoa1611925
26. Boehringer Ingelheim Pharmaceuticals. Jardiance (empagliflozin) tablets; prescribing information. Available from: http://bidocs.boehringer-ingelheim.com/BIWebAccess/ViewServlet.ser?docBase=renetnt&folderPath=/Prescribing+Information/PIs/Jardiance/jardiance.pdf.
27. Garvey WT, Van Gaal L, Leiter LA, et al. Effects of canagliflozin versus glimepiride on adipokines and inflammatory biomarkers in type2 diabetes. Metabolism. 2018;85:32–37. doi:10.1016/j.metabol.2018.02.002
28. Wan SW, Kori N, Rajoo S, et al. Switching from sulphonylurea to a sodium-glucose cotransporter 2 inhibitor in the fasting month of Ramadan is associated with a reduction in hypoglycemia. Diab Obs Metab. 2016;18(6):628–632.
29. Hassanein M, Echtay A, Hassoun A, et al. Tolerability of canagliflozin in patients with type2 diabetes mellitus fasting during Ramadan: results of the Canagliflozin in Ramadan Tolerance Observational Study(CRATOS). Inter J Clin Pract. 2017;71(10):e12991. doi:10.1111/ijcp.12991
30. Amin F, Afsana F, Nazneen NE, et al. Lifestyle practice and awareness during Ramadan fasting in Bangladesh diabetic population. BIRDEM Med J. 2016;6:26–31. doi:10.3329/birdem.v6i1.28407
31. World Health Organization, Western Pacific Region. International Association for the Study of Obesity (IASO) and the International Obesity Task Force (IOTF). The Asia-Pacific Perspective: Redefining Obesity and Its Treatment. Crows Nest, NSW, Australia: Health Communications Australia; 2000.
32. Liz S. New AHA recommendations for blood pressure measurement: American Heart Association Practice guidelines. Am Fam Physician. 2005;72(7):1391–1398.
33. Seaquist ER, Anderson J, Childs B, et al. Hypoglycemia and diabetes: a report of a workgroup of the American Diabetes Association and the Endocrine Society. Diabetes Care. 2013;36:1384–1395. doi:10.2337/dc12-2480
34. Mange K, Matsuura D, Cizman B, et al. Language guiding therapy: the case of dehydration versus volume depletion. Ann Intern Med. 1997;127(9):848–853. doi:10.7326/0003-4819-127-9-199711010-00020
35. Mayo Foundation for Medical Education and Research Urinary tract infection (UTI) Mayo Clinic; September, 2022 Available from: https://www.mayoclinic.org/diseases-conditions/urinary-tractinfection/symptomscauses/syc-20353447.
36. National Cancer Institute NCI Dictionary of Cancer terms Available from: https://www.cancer.gov/publications/dictionaries/cancer-terms/def/adverse-event.
37. Dogan I, Eser B, Kayadibi H. The effect of Ramadan fasting on renal functions in patients with chronic kidney disease. Turk J Biochem. 2019;44(2):189–196. doi:10.1515/tjb-2018-0373
38. Lunati ME, Cimino V, Gandolfi A, et al. SGLT2-inhibitors are effective and safe in the elderly: the SOLD study. Pharmacol Res. 2022;183:106396. doi:10.1016/j.phrs.2022.106396
39. Bashier A, Khalifa AA, Abdelgadir EI, et al. Safety of sodium- glucose co transporter 2 inhibitors (SGLT2-I) during the month of Ramadan in Muslim patients with type 2 diabetes. Oman Med J. 2018;33(2):104–110. doi:10.5001/omj.2018.21
40. Abdelgadir E, Rashid F, Basheir A, et al. Use of flash glucose monitoring system in assessing safety of the SGLT2 inhibitors during Ramadan fasting in high risk insulin treated patients with type 2 diabetes. Diab Metab Syndr. 2019;13:2927–2932. doi:10.1016/j.dsx.2019.07.055
41. Shao Y, Lim GJ, Chua CL, et al. The effect of Ramadan fasting and continuing sodium -glucose co-transporters-2 (SGLT2) inhibitor use on ketonemia, blood pressure and renal function in Muslim patients with type 2 diabetes. Diab Res Clin Pract. 2018;142:85–91. doi:10.1016/j.diabres.2018.05.022
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.