")
Back to Journals » Drug Design, Development and Therapy » Volume 17
Clinical Evaluation of Risankizumab in the Treatment of Adults with Moderately to Severely Active Crohn’s Disease: Patient Selection and Reported Outcomes
Received 29 November 2022
Accepted for publication 17 January 2023
Published 31 January 2023 Volume 2023:17 Pages 273—282
DOI https://doi.org/10.2147/DDDT.S379446
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Sara Horst,1 Raymond K Cross2
1Vanderbilt University Medical Center, Nashville, TN, USA; 2University of Maryland School of Medicine, Baltimore, MD, USA
Correspondence: Sara Horst, Vanderbilt University Medical Center, Inflammatory Bowel Disease Clinic, 719 Thompson Lane, Suite, 20500, Nashville, TN, 37204, USA, Tel +1 615-343-4758, Email [email protected]
Abstract: This article will review risankizumab, a monoclonal antibody targeting interleukin 23 (IL-23) for the treatment of moderate-to-severe Crohn’s disease. The article will detail the mechanism of action and dosing strategies. Efficacy in induction and maintenances will be reviewed from available clinical trials as well as an evaluation of safety of the medication for use in Crohn’s disease and other immune mediated diseases. Finally, a discussion of when to use this medication for treatment in Crohn’s disease as well as how to monitor patients after medication initiation will be discussed.
Keywords: Crohn’s disease, risankizumab, biological therapy, interleukin-23 subunit p19, remission induction
Introduction
Although there are increasing biologic therapy options for therapy for patients with moderate-to-severe Crohn’s disease, many patients even in phased clinical trials fail to meet clinical remission. There is also a significant loss of response to biologic therapy; therefore, increasing options for management of refractory disease are needed. Risankizumab has recently been approved for the treatment of moderate-to-severe Crohn’s disease. Risankizumab is a humanized IgG1 monoclonal antibody targeting the p19 subunit on the cytokine interleukin 23 (IL-23). IL-23 is in the IL-12 family of cytokines, which consists of four cytokines IL-12, IL-23, IL-27, and IL-35.1 These cytokines are thought to be integral in differentiating T-helper (Th)-1 and −17 responses.2 IL-12 consisting of protein subunits p35 and p40, was discovered first, arising from efforts to identify cytokines derived from specific natural killer (NK) cells and eventually was found to drive Th1 responses. It was found that neutralization or disruption of the IL-12p40 subunit protected against experimentally induced autoimmune disease.3 However, disruption of the subunit p35 did not seem to offer the same benefit of immune protection. As research continued, another subunit p19 was found to be bonded with subunit p40, resulting in a novel interleukin discovery, IL-23.4,5 IL-23 is involved in signaling and function of Th-17 pathways. This activation triggers Janus kinase and signal transducer and activator of transcription (STAT) pathways. Also other pathways involving innate immunity are disrupted, promoting gut inflammation6 (Figure 1). The interplay of the IL-12 cytokine family remains complex. However, research increasingly shows that this IL-23 pathway is a major contributor to significant pathologic intestinal inflammation in inflammatory bowel disease. For example, translational research shows high IL-23 serum levels in patients with UC which correlate with disease severity. Higher expression of IL 23 p19 mRNA has been shown in patients with Crohn’s disease compared to healthy volunteers.7 In some patients with IBD, genetic studies have found a single nucleotide polymorphism in the IL-23 receptors. This could suggest a link to disease susceptibility as well.8,9
 |
Figure 1 Mechanism of action of risankizumab (used with permission from AbbVie, Inc.). |
Dosing
Risankizumab is approved for treatment of moderately to severely active Crohn’s disease in adults.10 Patients receive three intravenous induction doses of 600 mg over at least one hour at weeks 0, 4, and 8. They then start 180 mg/1.2 mL or 360 mg/2.4 mL injections at week 12 and continue every 8 weeks with an on-body injector device. The patients store the medication in a refrigerated area (between 36 degrees F to 46 degrees F). When they are ready to use, the patient will take the medication out of the refrigerated area and allow to warm to room temperature (at least 45 to 90 minutes). Patients load a prefilled cartridge into the on-body injector. They will then use adhesive to attach the on-body injector to their body at their upper front thigh or abdomen (at least 2 inches from their navel) after cleaning the area with an alcohol swab. The on-body injector will flash an indicator light when ready and the patient pushes a gray start button deploying a small 29-gauge needle. The medication runs in over a period of approximately 5 minutes10 (Figure 2).
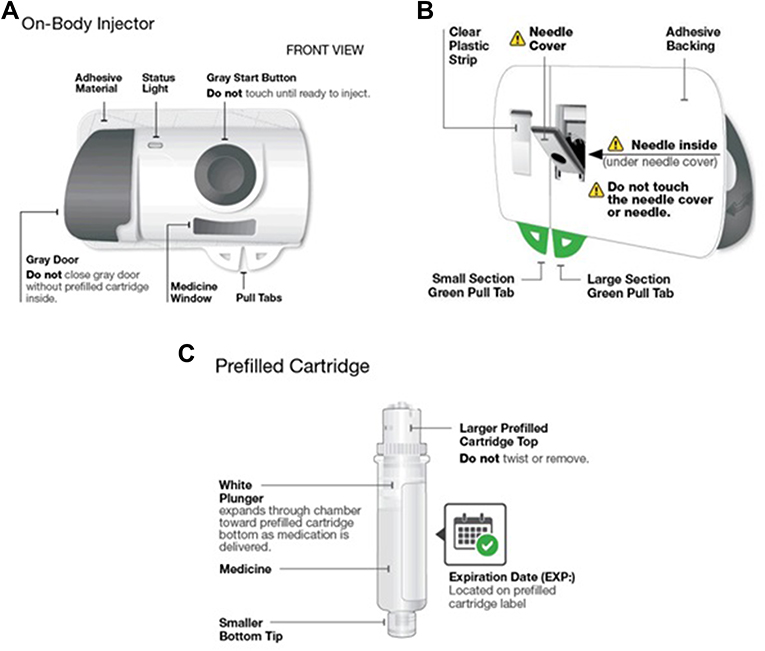 |
Figure 2 (A–C) Risankizumab on-body injector (used with permission from AbbVie, Inc.) (A). On-body injector front view (B). On-body injector back view (C). Prefilled cartridge. |
Efficacy in Induction
The phased placebo-controlled clinical trials for risankizumab are the first completed trials to incorporate dual primary endpoints. These included clinical remission (Crohn’s disease activity index [CDAI] <150 in the US and patient outcomes of stool frequency and abdominal pain scores in Europe) and endoscopic response (Simple Endoscopic Score for Crohn’s disease [SES-CD] with 50% decrease from baseline or at least a two-point reduction if isolated ileal disease SES-CD baseline equaled four). This is important as objective endpoints for inflammatory burden such as endoscopic improvement are being increasingly promoted in disease management.11 Other significant secondary endpoints included clinical response at week 4 and week 12 (CDAI score reduction by ≥ 100 points or significant decrease from baseline of stool frequency and abdominal pain scores). CDAI clinical remission as well as stool frequency and abdominal pain score remission was also evaluated at week 4. Endoscopic remission at week 12 (defined by an SES-CD ≤4 and at least a 2-point reduction from baseline and no subscore >1) was evaluated. Other endoscopic endpoints included ulcer-free endoscopy at week 12, and a composite endpoint of clinical remission and endoscopic response at week 12. Laboratory parameters were evaluated including high sensitivity C-reactive protein (hs-CRP) and fecal calprotectin. A prior phase 2a study showed that evaluating IL-22 may be important, as those with a decrease in IL-22 had greater clinical remission and response rates.12 Therefore, IL-22 was evaluated at several time points in the clinical trials.
Two induction trials looked at different infusion induction strategies for risankizumab (600 mg vs 1200 mg vs placebo). The intention to treat population included patients who received at least one dose of study drug in the 12-week induction period. In the intention to treat populations, ADVANCE included 850 patients who were a mix of bio naïve patients (42%) and those who had experienced biologic failure (58%). MOTIVATE included 569 patients, all of whom had failed biologic therapy and 53% with more than one biologic failure including 19% who had failed the anti-IL-12/23 therapy ustekinumab. No significant differential improvement occurred with the 1200 mg induction dose compared to the 600 mg dose. In ADVANCE and MOTIVATE, all co-primary endpoints were met, with 45% and 42% of patients achieving clinical remission at week 12 with the approved 600 mg dosing strategy compared to 25.2% and 19.8% of patients on placebo (p < 0.0001). Also, 40% vs 12% in ADVANCE and 29% vs 11% in MOTIVATE had endoscopic response at week 12 (p < 0.0001) (Table 1). The overall immunogenicity was low (<2%).13 Most secondary endpoints were met, including clinical remission and response rates at week 4 as well as endoscopic response and composite clinical/endoscopic endpoints at week 12. Importantly, significant reductions in hs-CRP and fecal calprotectin were seen at most time points in both induction studies. IL-22 decreased significantly at week 12 in patients who received risankizumab but was not predictive of clinical remission or endoscopic response or remission.13
 |
Table 1 Risankizumab Clinical Trial Results for Co-Primary Endpoints of Clinical Remission and Endoscopic Response in Induction (ADVANCE and MOTIVATE) and Maintenance (FORTIFY) |
In ADVANCE, patients who were bio-naïve were more likely to have improved clinical outcomes compared to patients who had previous bio-failure. CDAI remission rates and stool frequency/abdominal pain score remission rates were 49% and 48% in bio-naïve compared to 43% and 41% in bio-failure patients for those patients who received the 600 mg induction dosing. Endoscopic remission rates were 50% in the bio-naïve and 33% in the bio-failure patients at week 12. In subgroup analysis, clinical response rates were similar in both populations.13
Efficacy in Maintenance
Patients with clinical response at week 12 entered the placebo-controlled maintenance trial FORTIFY, which included 462 patients, 73% with biologic failure. Clinical response was defined as clinically significant decrease in mean stool frequency or abdominal pain scores, and both not worse than baseline. Patients were randomized to 180 mg subcutaneous risankizumab every 8 weeks, 360 mg subcutaneous risankizumab every 8 weeks, or withdrawal from risankizumab to receive placebo every 8 weeks. Patients who did not respond could receive open-label rescue dosing of 1200 mg IV risankizumab followed by 360 mg every 8 weeks starting at week 16. Patients were followed for 52 weeks, and co-primary endpoints were the same as the induction trial and included clinical remission and endoscopic response. Secondary endpoints were multiplicity controlled and were similar to induction trials but at a 52-week endpoint. Additional secondary endpoints included durability of clinical remission and steroid-free clinical remission at week 52.
Most patients completed the maintenance study (92% 180 mg group, 88% of the 360 mg group, and 88% of the placebo group). Disease variables were similar across the groups. For patients treated with 180 mg maintenance every 8 weeks, the coprimary endpoints were achieved for both clinical remission (adjusted treatment difference of 15% [95% CI 5–25]) and endoscopic response (adjusted treatment difference of 26% [95% CI 17–35]) at 52 weeks. For patients treated with 360 mg risankizumab maintenance every 8 weeks, the coprimary endpoints were achieved for both clinical remission (adjusted treatment difference of 15% [95% CI 5–25]) and endoscopic response (adjusted treatment difference of 28% [95% CI 19–37]) at 52 weeks14 (Table 1). In evaluation of the secondary endpoints, higher rates of efficacy were found in endpoints of endoscopic remission, ulcer-free endoscopy, composite endpoint of clinical remission and endoscopic response, and deep remission (ie, a composite of clinical remission and endoscopic remission) in the risankizumab treated group compared to placebo withdrawal group. Greater treatment effect was seen in the 360 mg group compared to the 180 mg group. The treatment effect was highest in those patients who were bio naïve. Overall immunogenicity remained low (2% in the Risankizumab treated group).14 A subset analysis of risankizumab rescue therapy in the FORTIFY trials was completed. Starting at week 16, a subset of patients who had inadequate response, defined as average daily stool frequency ≥ 3.3 and/or average daily abdominal pain score ≥ 1.5 as well as high sensitivity CRP ≥ 5 mg/L and/or fecal calprotectin ≥ 250 ug/g; or SES-CD endoscopic score ≥ 6 (≥ 4 for isolated ileal disease) were eligible for open-label rescue therapy (1 IV 1200 mg dose, followed by 360 mg subcutaneously every 8 weeks). Up to two rescue doses ≥ 16 weeks apart were allowed. Efficacy was assessed at week 52 using intent-to-treat population analysis. A greater proportion of the withdrawal (placebo SQ) arm (40.2%, 66/164) were given the rescue therapy compared to the 180 mg SQ (24.2%, 38/157) or 360 SQ (21.3%, 30/141) arms. Median time to rescue therapy in the groups was similar (178, 180, 154 days). Twenty to thirty six percent of patients who received rescue therapy achieved clinical remission (per CDAI or SF/APS) and/or endoscopic response, and this was not significantly different between the 3 groups. This dosing strategy is not currently approved for treatment with risankizumab, but the authors suggest that there may be benefit for this strategy in patients with interruption of treatment or inadequate response. Further data is needed.15
An interesting aspect of this data is looking at the patients who had IV risankizumab induction then were randomized to the withdrawal (subcutaneous placebo) arm. At week 52, 40% of patients in this withdrawal group were in clinical remission. This indicates that some patients could have longer lasting immune effect in altering p19 pathways beyond the medication half-life. However, endoscopic response was not maintained in those who were in the withdrawal arm. Also, all groups had a similar decrease in CRP, fecal calprotectin, and IL-22 at entrance into the maintenance study (week 0) with the IV induction, but these parameters started to increase again by week 52 for the withdrawal arm but not the maintenance risankizumab arm. Based on this data, it is important to continue maintenance dosing. Use of both 180 mg and 360 mg in maintenance had similar rates of primary endpoints of clinical remission and endoscopic response with no significant differences in adverse events. In secondary endpoint evaluation, there were higher numerical rates (approximately 10%) of endoscopic remission for patients receiving 360 mg maintenance dosing. Further data to understand maintenance dosing stratification is needed.
Safety
Risankizumab was evaluated in the phased clinical trials, and safety was assessed in all patients who had received at least one dose of the medication. Risankizumab had similar rates of overall adverse events to placebo. There were overall low rates of severe and serious adverse events and adverse events of special interest.13,14 Serious and opportunistic infections were low in all arms in the induction and maintenance trials. Major cardiovascular events were low. Malignancies, including or excluding non-melanoma skin cancers, were low. In the induction trials, low rates of infusion-related reactions were reported and only one serious hypersensitivity reaction was reported. Serious hypersensitivity reactions were not reported in the maintenance trials. Key safety endpoints are highlighted in Table 2. Overall rates of hepatic events were low overall. However, one patient who was in the 600 mg risankizumab induction arm had a serious hypersensitivity reaction (rash) with elevated liver enzymes reported 80 days after first dose of drug, requiring hospitalization and steroids.13 Therefore, lab requirements prior to initiation of risankizumab include evaluation of exposure to tuberculosis as well as liver enzymes and bilirubin. It is recommended to repeat liver tests in induction (up to 12 weeks). It may be practical to repeat liver tests at the third induction infusion (week 8) or when the patient comes for follow-up prior to the week 12 subcutaneous dose. As with all other biologics, ensuring patients are up to date on health maintenance including vaccines (including influenza, pneumococcal, COVID, shingles if appropriate) is important.16 Vaccine initiation should not preclude medication initiation.
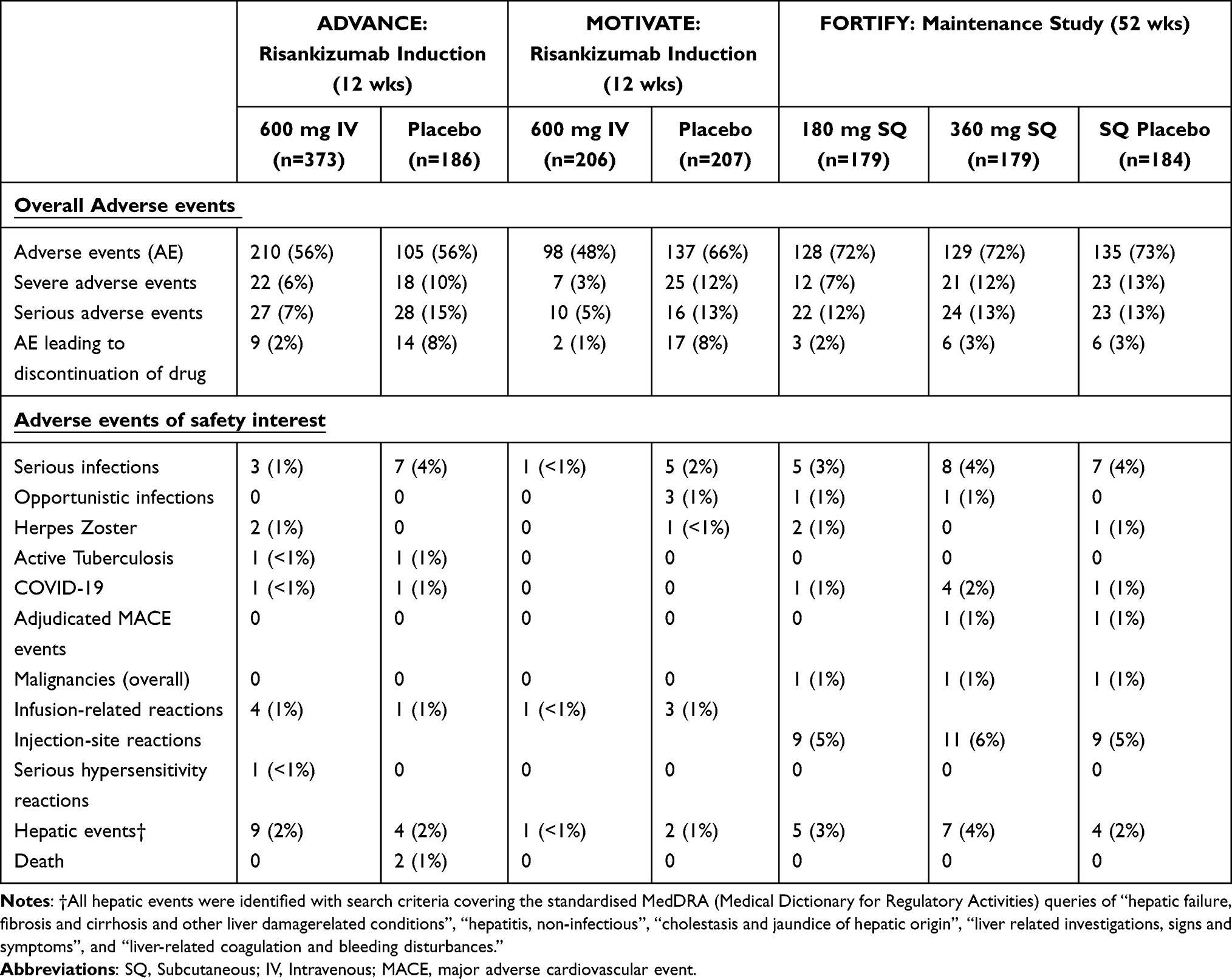 |
Table 2 Adverse Events for Patients on FDA Approved Dosing for Risankizumab Compared to Placebo in Phased 3 Trials for Risankizumab |
Safety data for risankizumab has been evaluated in multiple large trials for patients with psoriasis. It is important to note that there are different dosing strategies for psoriasis patients. In multiple Phase III clinical trials including trials with active comparator arms for patients with psoriasis, risankizumab has overall showed low rates of serious adverse events and a favorable safety profile.17–20 Long-term safety was evaluated in an open-label phase III study following multiple phase II/III studies over 172 weeks and found rates of AE leading to medication discontinuation and AE of safety interest were low.21 Long-term safety was also evaluated combining data from five Phase II and III clinical trials. This included 3072 patients with psoriasis treated with risankizumab (exposure: 7927 patient years, PY). Rates of serious adverse events were low at 7.8 per 100 PY, serious infections were low at 1.2 per 100 PY, nonmelanoma skin cancers (NMSC) were low at 0.7 per 100 PY, and malignant tumors excluding NMSC were low at 0.5 per 100 PY.22
When to Use
The increasing number of medications available for the treatment of moderate-to-severe Crohn’s disease can make decision-making more complicated for gastroenterologists. For instance, will there be differential benefit of an anti-p19 antibody such as risankizumab that only inhibits IL-23 over the anti-p40 antibody ustekinumab that inhibits both IL-12 and IL-23? As discussed above, IL-12 was initially discovered and blockade of this cytokine via binding the p40 subunit was thought to control inflammation. However, over time, the p40 subunit was also found on a new cytokine, IL-23, which is now considered the primary driver of inflammation in IBD. In another immune mediated disorder plaque psoriasis, inhibition of IL-23 had differential benefit over anti-IL-12/23 mechanisms. A head-to-head phased II randomized trial showed risankizumab had significantly higher rates of patients achieving 90% reduction in the Psoriasis Area and Severity index (PASI) compared to ustekinumab (77% vs 40%, p < 0.001).23 This was confirmed in two randomized, controlled Phase 3 clinical trials (UltIMMa-1 and UltIMMa-2). These showed risankizumab (75.3% [229/304] and 74.8% [220/294]) had significantly higher rates of patients achieving 90% reduction in PASI compared to ustekinumab (42.0% [42/100] and 47.5% [47/99]) at week 16.24 However, treatment of immune mediated disease may have different results depending on the disease state even within the same mechanism of action. It is unknown if this difference in efficacy will be also be seen in Crohn’s disease. Small data in post-hoc analysis of clinical trial data showed patients who had failed ustekinumab and treated with risankizumab had numerically higher clinical remission rates compared to placebo (ADVANCE n=16/43, 37.2% vs placebo n=3/19, 15.8% and MOTIVATE n=13/36, 36.1% vs placebo 4/40, 10%) in induction. Higher rates of endoscopic response were also seen in induction (ADVANCE 22.3% vs placebo 5.0% and MOTIVATE 22.3% vs placebo 5.4%). However, the numbers of patients in these groups were small. In the FORTIFY maintenance trial, small numbers of patients who had failed ustekinumab and treated with risankizumab had higher numerical rates of clinical remission (risankizumab 360 mg n=9/17, 51.2% vs risankizumab 180 mg n=6/18, 33.3% vs withdrawal/placebo n=3/15, 20%), highest in the higher 360 mg every 8 weeks dosing strategy. Endoscopic response was higher in the risankizumab treated groups as well (risankizumab 360 mg 29.4% vs risankizumab 180 mg 33.3% vs withdrawal/placebo 20.0%).25 Ongoing larger studies evaluating anti-IL-12/23 comparator groups in anti-IL-23 development programs or head-to-head trials will give more data in the future.26
It is also important to understand where to position risankizumab compared to anti-TNF therapies. A recent network meta-analysis in Crohn’s disease treatment suggests that anti-TNF pathways still may be first line for induction and maintenance of clinical remission in patients with Crohn’s disease compared to other biologics in patients who are bio-naïve.27 However, studies such as network meta-analyses emphasize induction therapy and may compare patient populations and/or outcome measures that are different between studies. One example is that older studies of anti-TNF therapy did not require endoscopy to document active inflammation to enter the clinical trial, increasing the chances that participants with symptoms from other causes were included in the clinical trial (ie, irritable bowel syndrome overlap). Other factors are important when considering therapy as well include Crohn’s disease location, the presence of stricturing and/or fistulizing disease complications, presence or history of perianal disease, presence of extraintestinal manifestations, prior treatment history, and comorbid conditions. These factors influence prescribing and may affect the patient's disease experience and treatment response. In patients with Crohn’s disease and severe fistulizing disease or perianal disease, post-operative resections, or severe extra intestinal manifestations, anti-TNF therapy still has the most robust data for disease control and remission.28–30 When considering anti-TNF therapy, there are several caveats to consider. Immunogenicity can occur with use of anti-TNF therapy a.31 When using an anti-TNF, often patients need to be on concomitant immunomodulator therapy. This can mitigate immunogenicity risk and improve clinical outcomes but is associated with more complex monitoring and a higher rate of serious infection and malignancy (lymphoma and non-melanoma skin cancer).32,33 According to a recent meta-analysis, anti-TNF therapy with or without concurrent immune suppressant may have slightly higher risk of serious infection than the anti-IL-12/23 therapy ustekinumab in Crohn’s disease. Risankizumab was not included in the meta-analysis.34 Ustekinumab has been shown to have a very low risk of serious infection in analyses of long-term extension of pivotal clinical trials.35 It also has been shown to have numerically lower risk of serious infection compared to anti-TNF in registry data for patients with psoriasis, although dosing for psoriasis is lower.36 Low serious infection rates were also shown with risankizumab in the phased clinical trial with data noted above.
So, while anti-TNF may have best efficacy in some meta-analyses, there continues to be the important issue of personalizing medication for patients. Let us consider patients with Crohn’s disease who are biologic naive. The treatment decisions need to include efficacy, safety, durability, speed of onset of action, and drug delivery. Risankizumab has good efficacy in patients who are bio-naïve based on the phased clinical trial data. In ADVANCE, 46% (66/140) of bio-naïve patients on 600 mg risankizumab had CDAI clinical remission at week 12 and 50% (71/141) had endoscopic response at week 12. This was persistent in FORTIFY for those on risankizumab 360 mg, with 64% (25/39) maintaining CDAI clinical remission and 53% (21/39) with endoscopic response at week 52. In evaluating a medication in the same class, anti-IL-12/23 ustekinumab has strong head-to-head clinical trial data showing no difference in efficacy or safety compared to adalimumab for use in patients with inflammatory Crohn’s disease with newer onset disease and no prior biologic use.37 Therefore, it may be very reasonable to consider medications that alter the IL-23 pathway for patients who are biologic naïve given advantages of low immunogenicity, monotherapy use, and excellent safety profiles.
Risankizumab may have a strong position in use for patients with moderate-to-severe Crohn’s disease who have failed anti-TNF.27 There have often been lower response rates for patients who are biologic experienced in most prior phased clinical trials for biologic medications. Risankizumab may have particular benefit in this population given the strong induction data including endoscopic response even in biologic experienced patients. The maintenance trial showed only slightly lower response in long-term clinical remission and endoscopic response between those who did or did not have prior biologic failure.
Currently, there are limited data regarding use of risankizumab in pregnancy. In the development program, toxicity studies on pregnant cynomolgus monkeys at high doses (5 or 50 mg/kg doses weekly) showed increased fetal/infant loss at the 50 mg/kg dose. This is 10 times exposure dose (area under the curve) in induction regimens and 39 times exposure dose for 360 mg maintenance doses for humans. No risankizumab-related side effects on functional or immunological development were observed in infant monkeys from birth to 6 months of age. It is important to note that transport of endogenous IgG antibodies across the placenta occurs and peaks in the third trimester of pregnancy. Because of this, consideration of live vaccine administration to infants exposed to biologics needs to be considered. Most expert consensus currently suggests avoidance of live vaccines in the first 6 months after delivery for babies exposed to biologic medications in utero.38 Increasing data show safety of the continuation of biologics including anti-TNF agents, with significant population-based data as well as prospective studies demonstrating safety throughout pregnancy for pregnant women and their children after birth.38–41 There is limited data about safety of vedolizumab and ustekinumab during pregnancy, but case report data thus far show no increased risk of maternal or fetal complications.38,42
How to Monitor
It is important to understand how we can best monitor for disease activity improvement and appropriate medication continuation. These endpoints are important as we not only want our patients to feel better but increasingly recognize that understanding therapeutic targets will be important as this can modulate long-term disease outcomes such as disability from disease, risk of surgery, and long-term clinical remission. Increasingly, there are initiatives to help clinicians understand how to follow treatment success, including the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) from the Initiative of International Organization for the Study of IBD (IOIBD).11 As we continue to learn about disease management, it is important to consider immediate, intermediate, and long-term treatment targets. In these recommendations, clinical response is an immediate treatment target. Clinical remission is an intermediate treatment target. When considering biomarkers, normalization of CRP and fecal calprotectin may be intermediate treatment targets. In terms of long-term targets, endoscopic healing is the goal of treatment, but in Crohn’s disease, still may be difficult to achieve for many patients.
The results of the phase 3 clinical trials of risankizumab for Crohn’s disease demonstrated improvement in these parameters during induction and maintenance despite inclusion of patients with more refractory disease, with almost ¾ of the patient population having failed biologic medication. Although a significant proportion of patients experienced endoscopic response with risankizumab, only a small proportion of patients achieved endoscopic remission or ulcer-free endoscopy. Therefore, in terms of monitoring patients, a reasonable approach is to get baseline disease evaluation with CRP, fecal calprotectin, and/or endoscopic evaluation with follow-up in 8–12 weeks to assess symptomatic and laboratory response to treatment if abnormal at baseline. Endoscopic evaluation approximately 6 months after treatment initiation is indicated to assess for endoscopic response. At this point in time, there is little to no data to guide optimizing risankizumab beyond labeled doses to improve clinical outcomes.
Summary
Risankizumab is an exciting new treatment option for patients with moderate-to-severe Crohn’s disease. It has strong efficacy and safety data with low immunogenicity. This makes it a good option for patients with Crohn’s disease who are bio-naïve and bioexposed. In fact, risankizumab may be the preferred treatment for patients with Crohn’s disease exposed to prior biologic therapy. Further data is needed for patient populations with severe stricturing and/or fistulizing disease or perianal disease or concurrent extra-intestinal manifestations, where anti-TNF medications have strong data for efficacy. Also, use of risankizumab in the post-operative setting to prevent recurrent disease needs to be further evaluated. An example of an ideal patient for risankizumab may be a patient with inflammatory ileal and/or colonic Crohn’s disease who had primary or secondary non-response to an anti-TNF agent (with adequate drug levels of anti-TNF documented). As always, real-world data is needed to confirm efficacy and safety in patients that would not have been eligible for the pivotal clinical trials and to determine how best to optimize therapy in those with incomplete response or loss of response to treatment.
Disclosure
SH has been a consultant for and reports personal fees from AbbVie, Janssen, Takeda, BMS. RKC has been a consultant for and reports grants or personal fees from AbbVie, BMS, Fresenius Kabi, Fzata, Magellan Health, Janssen, Pfizer, Samsung Bioepis, and Sebela. RKC is on the Data Safety Monitoring Board for Adiso. The authors report no other conflicts of interest in this work.
References
1. Khader SA, Thirunavukkarasu S. The Tale of IL-12 and IL-23: a paradigm shift. J Immunol. 2019;202(3):629–630. doi:10.4049/jimmunol.1801603
2. Ma C, Panaccione R, Khanna R, Feagan BG, Jairath V. IL12/23 or selective IL23 inhibition for the management of moderate-to-severe Crohn’s disease? Best Pract Res Clin Gastroenterol. 2019;38–39:101604. doi:10.1016/j.bpg.2019.02.006
3. Moschen AR, Tilg H, Raine T. IL-12, IL-23 and IL-17 in IBD: immunobiology and therapeutic targeting. Nat Rev Gastroenterol Hepatol. 2019;16(3):185–196. doi:10.1038/s41575-018-0084-8
4. Cua DJ, Sherlock J, Chen Y, et al. Interleukin-23 rather than interleukin-12 is the critical cytokine for autoimmune inflammation of the brain. Nature. 2003;421(6924):744–748. doi:10.1038/nature01355
5. Yen D, Cheung J, Scheerens H, et al. IL-23 is essential for T cell-mediated colitis and promotes inflammation via IL-17 and IL-6. J Clin Invest. 2006;116(5):1310–1316. doi:10.1172/JCI21404
6. Grossberg LB, Papamichael K, Cheifetz AS. Review article: emerging drug therapies in inflammatory bowel disease. Aliment Pharmacol Ther. 2022;55(7):789–804. doi:10.1111/apt.16785
7. Jefremow A, Neurath MF. All are equal, some are more equal: targeting IL 12 and 23 in IBD - A clinical perspective. Immunotargets Ther. 2020;9:289–297. doi:10.2147/ITT.S282466
8. Duerr RH, Taylor KD, Brant SR, et al. A genome-wide association study identifies IL23R as an inflammatory bowel disease gene. Science. 2006;314(5804):1461–1463. doi:10.1126/science.1135245
9. Liu M, Zhu W, Wang J, et al. Interleukin-23 receptor genetic polymorphisms and ulcerative colitis susceptibility: a meta-analysis. Clin Res Hepatol Gastroenterol. 2015;39(4):516–525. doi:10.1016/j.clinre.2014.10.009
10. Risankizumab Prescribing Information. Available from: https://www.rxabbvie.com/pdf/skyrizi_pi.pdf.
11. Turner D, Ricciuto A, Lewis A, et al. STRIDE-II: an update on the selecting therapeutic targets in inflammatory bowel disease (STRIDE) initiative of the international organization for the study of IBD (IOIBD): determining therapeutic goals for treat-to-target strategies in IBD. Gastroenterology. 2021;160(5):1570–1583. doi:10.1053/j.gastro.2020.12.031
12. Sands BE, Chen J, Feagan BG, et al. Efficacy and safety of MEDI2070, an antibody against interleukin 23, in patients with moderate to severe Crohn’s disease: a phase 2a study. Gastroenterology. 2017;153(1):77–86e6. doi:10.1053/j.gastro.2017.03.049
13. D’Haens G, Panaccione R, Baert F, et al. Risankizumab as induction therapy for Crohn’s disease: results from the phase 3 ADVANCE and MOTIVATE induction trials. Lancet. 2022;399(10340):2015–2030. doi:10.1016/S0140-6736(22)00467-6
14. Ferrante M, Panaccione R, Baert F, et al. Risankizumab as maintenance therapy for moderately to severely active Crohn’s disease: results from the multicentre, randomised, double-blind, placebo-controlled, withdrawal phase 3 FORTIFY maintenance trial. Lancet. 2022;399(10340):2031–2046. doi:10.1016/S0140-6736(22)00466-4
15. Baert F, Atreya R, Kakuta Y, et al. DOP85 Efficacy of risankizumab rescue therapy in patients with moderately to severely active Crohn’s Disease and inadequate response to risankizumab maintenance therapy. J Crohns Colitis. 2022;16(Supplement_1):i128. doi:10.1093/ecco-jcc/jjab232.124
16. Kucharzik T, Ellul P, Greuter T, et al. ECCO guidelines on the prevention, diagnosis, and management of infections in inflammatory bowel disease. J Crohns Colitis. 2021;15(6):879–913. doi:10.1093/ecco-jcc/jjab052
17. Blauvelt A, Leonardi CL, Gooderham M, et al. Efficacy and safety of continuous risankizumab therapy vs treatment withdrawal in patients with moderate to severe plaque psoriasis: a phase 3 randomized clinical trial. JAMA Dermatol. 2020;156(6):649–658. doi:10.1001/jamadermatol.2020.0723
18. Warren RB, Blauvelt A, Poulin Y, et al. Efficacy and safety of risankizumab vs. secukinumab in patients with moderate-to-severe plaque psoriasis (IMMerge): results from a Phase III, randomized, open-label, efficacy-assessor-blinded clinical trial. Br J Dermatol. 2021;184(1):50–59. doi:10.1111/bjd.19341
19. Gordon KB, Strober B, Lebwohl M, et al. Efficacy and safety of risankizumab in moderate-to-severe plaque psoriasis (UltIMMa-1 and UltIMMa-2): results from two double-blind, randomised, placebo-controlled and ustekinumab-controlled phase 3 trials. Lancet. 2018;392(10148):650–661. doi:10.1016/S0140-6736(18)31713-6
20. Reich K, Gooderham M, Thaci D, et al. Risankizumab compared with Adalimumab in patients with moderate-to-severe plaque psoriasis (IMMvent): a randomised, double-blind, active-comparator-controlled phase 3 trial. Lancet. 2019;394(10198):576–586. doi:10.1016/S0140-6736(19)30952-3
21. Papp KA, Lebwohl MG, Puig L, et al. Long-term efficacy and safety of risankizumab for the treatment of moderate-to-severe plaque psoriasis: interim analysis of the LIMMitless open-label extension trial beyond 3 years of follow-up. Br J Dermatol. 2021;185(6):1135–1145. doi:10.1111/bjd.20595
22. Gordon KB, Lebwohl M, Papp KA, et al. Long-term safety of risankizumab from 17 clinical trials in patients with moderate-to-severe plaque psoriasis. Br J Dermatol. 2022;186(3):466–475. doi:10.1111/bjd.20818
23. Papp KA, Blauvelt A, Bukhalo M, et al. Risankizumab versus ustekinumab for moderate-to-severe plaque psoriasis. N Engl J Med. 2017;376(16):1551–1560. doi:10.1056/NEJMoa1607017
24. Strober B, Menter A, Leonardi C, et al. Efficacy of risankizumab in patients with moderate-to-severe plaque psoriasis by baseline demographics, disease characteristics and prior biologic therapy: an integrated analysis of the phase III UltIMMa-1 and UltIMMa-2 studies. J Eur Acad Dermatol Venereol. 2020;34(12):2830–2838. doi:10.1111/jdv.16521
25. Ferrante M, Peyrin-Biroulet L, Dignass A, et al. Clinical and Endoscopic Improvements with risankizumab induction and maintenance dosing versus placebo are observed irrespective of number of prior failed biologics. United Eur Gastroenterol J. 2022;10(S8):9–184. doi:10.1002/ueg2.12293
26. ClinicalTrials.gov. Clinical Trial information; 2022. Available from: https://clinicaltrialsgov/ct2/show/NCT04524611.
27. Singh S, Murad MH, Fumery M, et al. Comparative efficacy and safety of biologic therapies for moderate-to-severe Crohn’s disease: a systematic review and network meta-analysis. Lancet Gastroenterol Hepatol. 2021;6(12):1002–1014. doi:10.1016/S2468-1253(21)00312-5
28. Sands BE, Anderson FH, Bernstein CN, et al. Infliximab maintenance therapy for fistulizing Crohn’s disease. N Engl J Med. 2004;350(9):876–885. doi:10.1056/NEJMoa030815
29. Colombel JF, Schwartz DA, Sandborn WJ, et al. Adalimumab for the treatment of fistulas in patients with Crohn’s disease. Gut. 2009;58(7):940–948. doi:10.1136/gut.2008.159251
30. Regueiro M, Kip KE, Baidoo L, Swoger JM, Schraut W. Postoperative therapy with infliximab prevents long-term Crohn’s disease recurrence. Clin Gastroenterol Hepatol. 2014;12(9):1494–502 e1. doi:10.1016/j.cgh.2013.12.035
31. Battat R, Lukin D, Scherl EJ, et al. Immunogenicity of tumor necrosis factor antagonists and effect of dose escalation on anti-drug antibodies and serum drug concentrations in inflammatory bowel disease. Inflamm Bowel Dis. 2021;27(9):1443–1451. doi:10.1093/ibd/izaa313
32. Kennedy NA, Heap GA, Green HD, et al. Predictors of anti-TNF treatment failure in anti-TNF-naive patients with active luminal Crohn’s disease: a prospective, multicentre, cohort study. Lancet Gastroenterol Hepatol. 2019;4(5):341–353. doi:10.1016/S2468-1253(19)30012-3
33. Colombel JF, Sandborn WJ, Reinisch W, et al. Infliximab, azathioprine, or combination therapy for Crohn’s disease. N Engl J Med. 2010;362(15):1383–1395. doi:10.1056/NEJMoa0904492
34. Solitano V, Facciorusso A, Jess T, et al. Comparative risk of serious infections with biologic agents and oral small molecules in inflammatory bowel diseases: a systematic review and meta-analysis. Clin Gastroenterol Hepatol. 2022. doi:10.1016/j.cgh.2022.07.032
35. Sandborn WJ, Rebuck R, Wang Y, et al. Five-year efficacy and safety of ustekinumab treatment in crohn’s disease: the IM-UNITI trial. Clin Gastroenterol Hepatol. 2022;20(3):578–590 e4. doi:10.1016/j.cgh.2021.02.025
36. Papp K, Gottlieb AB, Naldi L, et al. Safety surveillance for ustekinumab and other psoriasis treatments from the psoriasis longitudinal assessment and registry (PSOLAR). J Drugs Dermatol. 2015;14(7):706–714.
37. Sands BE, Irving PM, Hoops T, et al. Ustekinumab versus Adalimumab for induction and maintenance therapy in biologic-naive patients with moderately to severely active Crohn’s disease: a multicentre, randomised, double-blind, parallel-group, phase 3b trial. Lancet. 2022;399(10342):2200–2211. doi:10.1016/S0140-6736(22)00688-2
38. Lamb CA, Kennedy NA, Raine T, et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut. 2019;68(Suppl 3):s1–s106. doi:10.1136/gutjnl-2019-318484
39. Mahadevan U, Long MD, Kane SV, et al. Pregnancy and neonatal outcomes after fetal exposure to biologics and thiopurines among women with inflammatory bowel disease. Gastroenterology. 2021;160(4):1131–1139. doi:10.1053/j.gastro.2020.11.038
40. Broms G, Granath F, Ekbom A, et al. Low risk of birth defects for infants whose mothers are treated with anti-tumor necrosis factor agents during pregnancy. Clin Gastroenterol Hepatol. 2016;14(2):234–41e1–5. doi:10.1016/j.cgh.2015.08.039
41. Luu M, Benzenine E, Doret M, et al. Continuous anti-tnfalpha use throughout pregnancy: possible complications for the mother but not for the fetus. A retrospective cohort on the French national health insurance database (EVASION). Am J Gastroenterol. 2018;113(11):1669–1677. doi:10.1038/s41395-018-0176-7
42. Moens A, van der Woude CJ, Julsgaard M, et al. Pregnancy outcomes in inflammatory bowel disease patients treated with vedolizumab, anti-TNF or conventional therapy: results of the European CONCEIVE study. Aliment Pharmacol Ther. 2020;51(1):129–138. doi:10.1111/apt.15539
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.