Back to Journals » Infection and Drug Resistance » Volume 16
Plasma 25(OH)D Level is Associated with the Nucleic Acid Negative Conversion Time of COVID-19 Patients: An Exploratory Study
Authors Chen C, Li P ![]() , Chen J, Liu C, Wang X, Cai J, Xiang E, Gu Z, Chen P
, Chen J, Liu C, Wang X, Cai J, Xiang E, Gu Z, Chen P
Received 7 December 2022
Accepted for publication 9 February 2023
Published 15 February 2023 Volume 2023:16 Pages 937—947
DOI https://doi.org/10.2147/IDR.S400561
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Suresh Antony
Changqiang Chen,1,* Pu Li,1,* Jiuming Chen,1,* Chunxiao Liu,2 Xiaodan Wang,3 Jialin Cai,4 Enfei Xiang,4 Zhidong Gu,1,5 Peizhan Chen4
1Department of Laboratory Medicine, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 2Department of Pediatrics, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 3Department of Neurology & Institute of Neurology, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 4Clinical Research Center, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, People’s Republic of China; 5Department of Laboratory Medicine, Ruijin-Hainan Hospital, Shanghai Jiao Tong University School of Medicine (Hainan Boao Research Hospital), Hainan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Peizhan Chen, Clinical Research Center, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, 201821, People’s Republic of China, Tel +86 13918550745, Email [email protected] Zhidong Gu, Department of Laboratory Medicine, Ruijin Hospital, Shanghai Jiao Tong University School of Medicine, Shanghai, 201821, People’s Republic of China, Tel +86 13801653534, Email [email protected]
Purpose: Vitamin D, an essential nutrient and a pleiotropic steroid hormone, has been reported to be associated with the risk and severity in patients infected with Coronavirus Disease-2019 (COVID-19). The role of vitamin D in predicting clinical outcome for COVID-19 patients is unknown. Here, we aimed to determine the prognostic value of plasma 25(OH)D level in COVID-19 patients.
Patients and Methods: A total of 158 patients infected with novel COVID-19 Omicron variants in Shanghai were recruited in this study and were categorized into three groups by the tertile levels of plasma 25(OH)D. Plasma 25(OH)D level was determined along with routine blood tests related to liver and renal functions in newly diagnosed COVID-19 patients at admission. The nucleic acid negative conversion time of throat swab samples was evaluated as the primary clinical outcome. The prognostic value of clinical characteristics and plasma 25(OH)D level was assessed using the Kaplan–Meier plot and Cox proportional hazards regression tests.
Results: Higher level of plasma 25(OH)D level in COVID-19 patients was independently associated with shorter nucleic acid negative conversion time from COVID-19 infection (multivariate adjusted HR: 0.54, 95%CI: 0.35– 0.82, P=0.004, tertile 2 vs 1; multivariate adjusted HR: 0.60, 95%CI: 0.39– 0.90, P=0.014, tertile 3 vs 1).
Conclusion: Plasma 25(OH)D level may serve as an independent prognostic factor in COVID-19 patient. Our findings indicate the protective roles of vitamin D supplementation in the regiment of patients with COVID-19.
Keywords: SARS-CoV-2, COVID-19, plasma 25(OH)D level, nucleic acid negative conversion time
Introduction
COVID-19 (coronavirus disease-2019) is a novel coronavirus infected pneumonia which is caused by the novel coronavirus named SARS-COV-2 (severe acute respiratory syndrome coronavirus-2). Transmitted mainly via respiratory droplets and contact, SARS-COV-2 has caused a global public pandemic with more than 500-million infected cases. COVID-19 is assigned as a category B infectious disease but publicly controlled as category A infectious disease in China since December, 2019 to December, 2022.1 In March 2022, a new surge of coronavirus occurred in Shanghai, China. Reverse transcription-polymerase chain reaction (RT-PCR) analysis suggested that coronavirus strain in this round of epidemic was Omicron variant BA.2.2 The BA.2 strain is least pathogenic but highly transmissible among all existing SARS-CoV-2 strains until March 2022.3 The virus nucleic acid load usually determined by RT-PCR methods is closely associated with the clinical symptoms of COVID-19 patients. Patients with lower viral load showed reduced risk of transmission. The viral load is also an important indicator for disease progression. In clinic, patients with two consecutive negative nucleic acid tests (sampling interval should be at least 24 h apart) for COVID-19 virus RNA in respiratory specimens including sputum or nasopharyngeal swabs are discharged from the hospital.4
Serum or plasma 25(OH)D level has been widely accepted as the indicator of vitamin D nutritional status. Circulating 25(OH)D is the inactive and circulating form of vitamin D.5 It is an essential nutrition and also a precursor of potent steroid hormones that regulate a broad spectrum of physiological processes.6 25(OH)D is well known for its role in the regulation of calcium homeostasis and bone mineralization.5 Vitamin D deficiency is associated with the increased risks of infectious and noncommunicable diseases such as upper respiratory infections.7–9 Recently, a substantial body of evidence showed that vitamin D deficient status was associated with increased COVID-19 infection risk and severity.10–17 However, the majority of the retrospective research determined that the circulating 25(OH)D level from preceding collected blood samples rather than at the time of diagnosis, which may cause a bias. Several randomized controlled trials (RCTs) have investigated the therapeutic effects of vitamin D in COVID-19, but inconsistent results were noticed for the preventive roles of vitamin D on mortality, intensive care requirement and hospital duration stay.18,19 Thus, the roles of vitamin D in clinical outcome for COVID-19 patients are still largely illusive. In the current study, using the newly diagnosed COVID-19 patients, we explored the relationship between plasma 25(OH)D level at the diagnosis and the nucleic acid conversion time of COVID-19 patients, which may provide deeper insights of the antiviral activities of vitamin D.
Materials and Methods
Participants Recruitment
From June 1 to July 5 to in 2022, adult novel coronavirus Omicron variant-infected patients (≥18 years old) admitted to Ruijin Hospital were enrolled in our study. Diagnosis of COVID-19 patients following the Diagnosis and Treatment Protocol for COVID-19 patients (tentative 9th Edition) by the National Health Commission (NHC) of China.4 We excluded patients who met the following criteria: (1) refuse to participate in the study; (2) with nucleic acid test Ct >35 (recognized as nucleic acid negative) after initial hospital admission; (3) with a hospitalization duration time less than 2 days; (4) incomplete laboratory test results; (5) did not provide the sufficient data about the nucleic acid results; (6) had received any antivirial regimens including Paxlovid (Nirmatrelvir/ritonavir) or VV116. This study was approved by the Institutional Review Board of Shanghai Ruijin Hospital (Agreement Number: 2022-119), with informed consent was obtained for individual patients. This study was performed in accordance with the Declaration of Helsinki.
Data Collection
Using the COVID-19 electronic medical record system of Ruijin Hospital, the basic information of patients such as the body mass index (BMI), age, gender, comorbidities as well as the COVID-19 vaccination status were obtained. Nasopharyngeal swab specimens of all patients were collected every other day and were tested by real-time quantitative PCR (RT-qPCR) of the N gene and 0rfla/b gene of Omicron coronavirus species. The results were presented as cycle threshold (Ct) values and patient with a Ct value over 35 in RT-qPCR test of viral RNA were recognized as negative according to the manufactures’ instructions. The interval of the respiratory tract specimen negative conversion time of patients was defined as the time from illness onset to the first time of two consecutive nucleic acid negative test of respiratory tract specimens with an interval of at least 24 h.
Blood Sample Collection and Storage
At the time of admission, a total of 7 mL of the overnight fasting blood samples were collected from novel coronavirus Omicron variant-infected patients before they received further medical treatments. All peripheral blood samples were collected using EDTA vacuum tubes and centrifuged at 3000 rpm for 15 min at room temperature to separate the plasma within two hours to ensure freshness. The serum samples were collected in gel clot activator vacuum tubes in aliquots and were stored at −80°C until use. The collection, procession and preservation of samples followed the corresponding biological safety rules.
Laboratory Analysis
The plasma 25(OH)D levels of COVID-19 patients were measured in batches with a highly sensitive electrochemiluminescence method by Roche Elecsys2010 at Ruijin Hospital (Roche Diagnostics, AZ, USA). Routine analysis of blood was performed on an XN-9000 Automated Hematology System (Sysmex Corporation, Hyogo, Japan) and serum biochemistry tests related to liver and renal function were performed through an automatic biochemical analyzer (model ci16200, Abbott Laboratories, IL, USA) using corresponding reagents according to the manufacturer’s instructions.
Statistical Analysis Methods
Categorical variables were displayed as count number and the proportion of groups. The normal distribution of the continuous blood parameters of the patients was tested using Shapiro–Wilk test, and the non-normal data were categorized into higher or lower groups based on the median values. The chi-squared tests were used to assess the proportion difference between the patient groups stratified by plasma 25(OH)D level. The univariate and multivariate Cox proportional hazard regression models were used to investigate the risk factors associated with the nucleic acid conversion time of COVID-19 infected patients. Variants included in the multivariate Cox proportional hazard regression models were selected using the stepwise backward selection based on the Akaike information criterion (AIC) value. The association between plasma 25(OH)D level and the nucleic acid negative conversion time of COVID-19 infected patients was also determined by Kaplan–Meier method in together with the log rank tests. All analyses were performed with SPSS (v 20.0.0) software and the two-sided P<0.05 was considered statistically significant.
Results
Baseline Characteristics of COVID-19 Patients
Three hundred and fifty-three participants (aged ≥18 years) were recruited in current study. According to the excluding criteria, a total of 158 eligible patients – 90 (56.96%) were male and 68 (43.04%) were female – were recruited and enrolled in current study (Supplementary Figure 1). The age of the subjects was range from 18 to 78 years old with 41.77% ≥60 years old. Sixty-two (39.24%) patients had not received any COVID-19 vaccination, three (1.90%) had received a single dose vaccination while 43 (27.22%) had received two doses and 50 (31.65%) had received three doses. Among the 239 doses of vaccination that patients received, detailed information was available for 186 (77.82%). 55.38% of the vaccines were Sinopharm BIBP (Beijing Institute of Biological Products Co., Ltd), 33.87% were Sinovac (Sinovac Life Sciences Co., Ltd), 5.38% were Sinopharm WIBP (Wuhan Institute of Biological Products Co., Ltd), 2.69% were CanSinoBio (CanSino Biologics Inc) and 2.69% were of Zhifei brand (Anhui Zhifei Longcom Biopharmaceutical) (Supplementary Table 1). For BMI, 39 (24.68%) patients had normal BMI (range: 18.5–23.9 kg/m2), 33 (20.89%) were underweight (BMI <18.5 kg/m2), 20 (12.66%) were categorized as overweight (range: 24–27.9 kg/m2), 49 (31.01%) were categorized as obese (BMI >27.9 kg/m2) and 17 (10.76%) were unknown. The main comorbidities were history of arterial hypertension (24.05%), followed by diabetes mellitus (13.29%) and coronary artery disease (3.80%). There is no significant difference in comorbidities distribution among three group of patients (P=0.28) (Table 1). Patients were treated with clinical routine methods including anti-fever medicine such as Lianhua Qingwen capsule, Ibuprofen and cough syrup etc. The nasopharyngeal swab specimens were used to detect the COVID-19 viral load each other day. The mean nucleic acid negative conversion time was 14.76 days (range: 4–30 days).
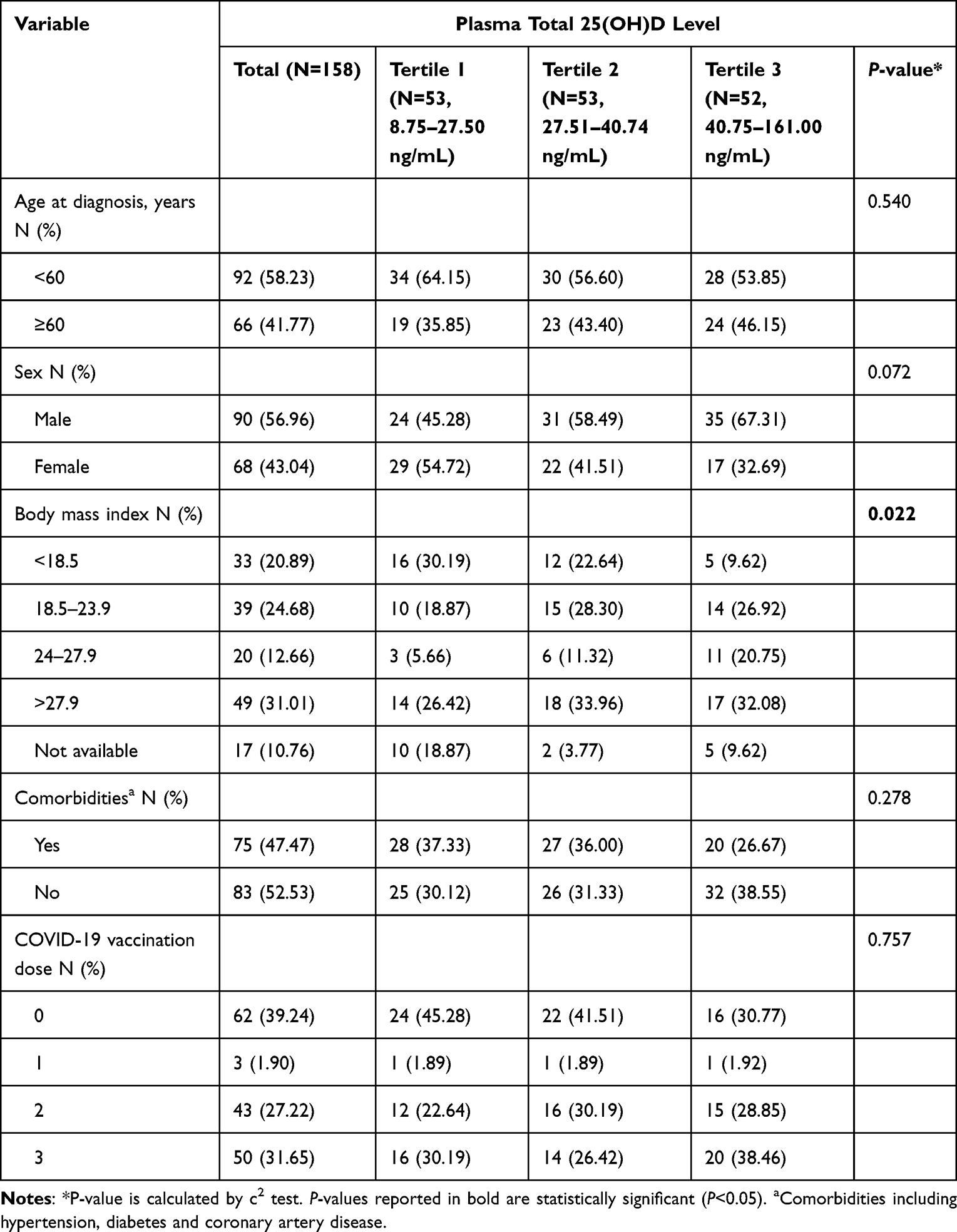 |
Table 1 Associations Between Demographic and Clinical Parameters with Plasma Total 25(OH)D Level in COVID-19 Patients (N=158) |
Associations Between Plasma 25(OH)D Levels and Clinical Characteristics of COVID-19 Patients
Among 158 patients, the mean plasma 25(OH)D level was 36.70±18.14 ng/mL with a median concentration at 32.71 ng/mL. Patients were categorized into three groups by the tertile levels of plasma 25(OH)D (tertile 1, 8.75–27.50 ng/mL; tertile 2, 27.51–40.74 ng/mL; tertile 3, 40.75–161.00 ng/mL). For clinical features, we noticed that patients with higher BMI usually have lower plasma 25(OH)D level (P=0.022; Table 1). No significant association of the plasma 25(OH)D level with the clinical characteristics including age, sex, comorbidities and the vaccination status was noticed (Table 1). In further, we also found no significant correlation between vitamin D and the blood parameters of patients (Figure 1).
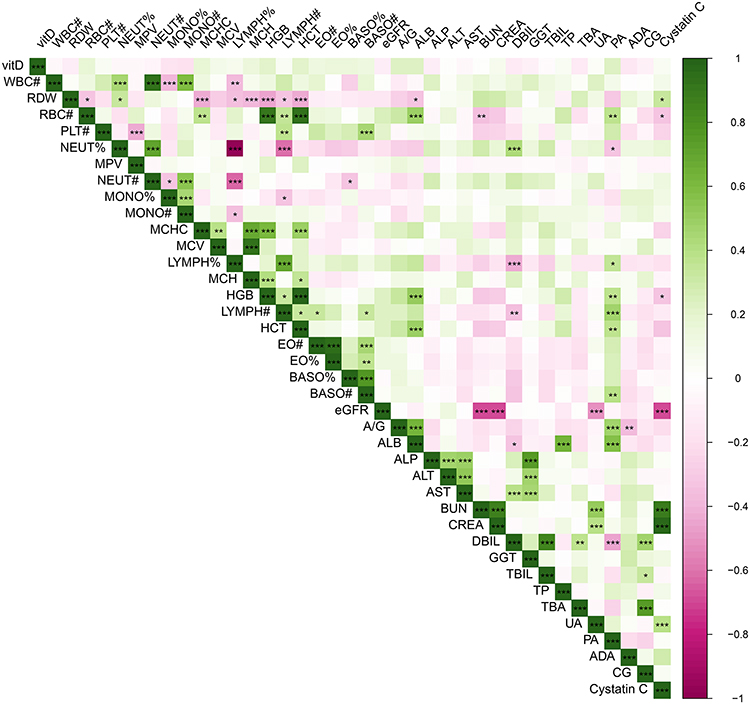 |
Figure 1 Correlations between the plasma 25(OH)D level and blood parameters in COVID-19 patients. ***P<0.001, **P<0.01, *P<0.05. Abbreviations: vitD, plasma 25(OH)D level; WBC#, white blood cell count; RDW, red blood cell distribution width; RBC#, red blood cell count; PLT#, platelet count; NEUT%, neutrophil percentage; MPV, mean platelet volume; NEUT#, neutrophil count; MONO%, monocyte percentage; MONO#, monocyte count; MCHC, mean corpuscular hemoglobin concentration; MCV, mean corpuscular volume; LYMPH%, lymphocyte percentage; MCH, mean corpuscular hemoglobin; HGB, hemoglobin; LYMPH#, lymphocyte count; HCT, hematocrit; EO#, eosinophil count; EO%, eosinophil percentage; BASO%, basophil percentage; BASO#, basophil count; A/G, albumin-globulin ratio; ALB, albumin; ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; UREA, urea; CREA, creatinine; DBIL, direct bilirubin; GGT, γ-glutamyl transpeptidase; TBIL, total bilirubin; TP, total protein; TBA, total biliary acid; UA, uric acid; PA, prealbumin; ADA, adenosine deaminase; eGFR, estimated glomerular filtration rate; CG, cholyglycine. |
Associations Between Plasma 25(OH)D Level and the Nucleic Acid Conversion Time of COVID-19 Patients
The univariate and multivariate Cox regression analyses were performed to identify patients’ characteristics that were significantly associated with the virus nucleic acid negative conversion time. We found that lower albumin (ALB; P<0.001) and elevated red blood cell distribution width (RDW; P=0.018), lymphocyte percentage (LYMPH%; P=0.037), neutrophil count (NEUT#; P<0.001), age more than 60 and underweight or obese (P<0.05) were associated with longer nucleic acid negative conversion time (Table 2, Table 3 and Supplementary Table 2). The Kaplan–Meier plot suggested that COVID-19 patients with a higher plasma 25(OH)D level had a shorter nucleic acid negative conversion time (log rank test, P=0.019; Figure 2A) compared to patients with lower level. Similar results were obtained in the univariate Cox analysis. In the multivariate analysis, we found that the plasma 25(OH)D was independently associated with the nucleic acid negative conversion time of COVID-19 patients (multivariate adjusted HR: 0.54, 95%CI: 0.35–0.82, P=0.004, tertile 2 vs 1; multivariate adjusted HR: 0.60, 95%CI: 0.39–0.90, P=0.014, tertile 3 vs 1; Table 3). Furthermore, the log rank tests were conducted to explore the associations between plasma 25(OH)D level and nucleic acid negative conversion time of COVID-19 patients in stratification groups to exclude potential bias caused by sex and age. Significant association between vitamin D and COVID-19 conversion time was observed both in the male group (P=0.023; Figure 2B) and the female group (P=0.011; Figure 2C), as well as in patients ≤60 years old (P=0.020; Figure 2D). However, no significant association was noticed in patients over 60 years old (Supplementary Figure 2).
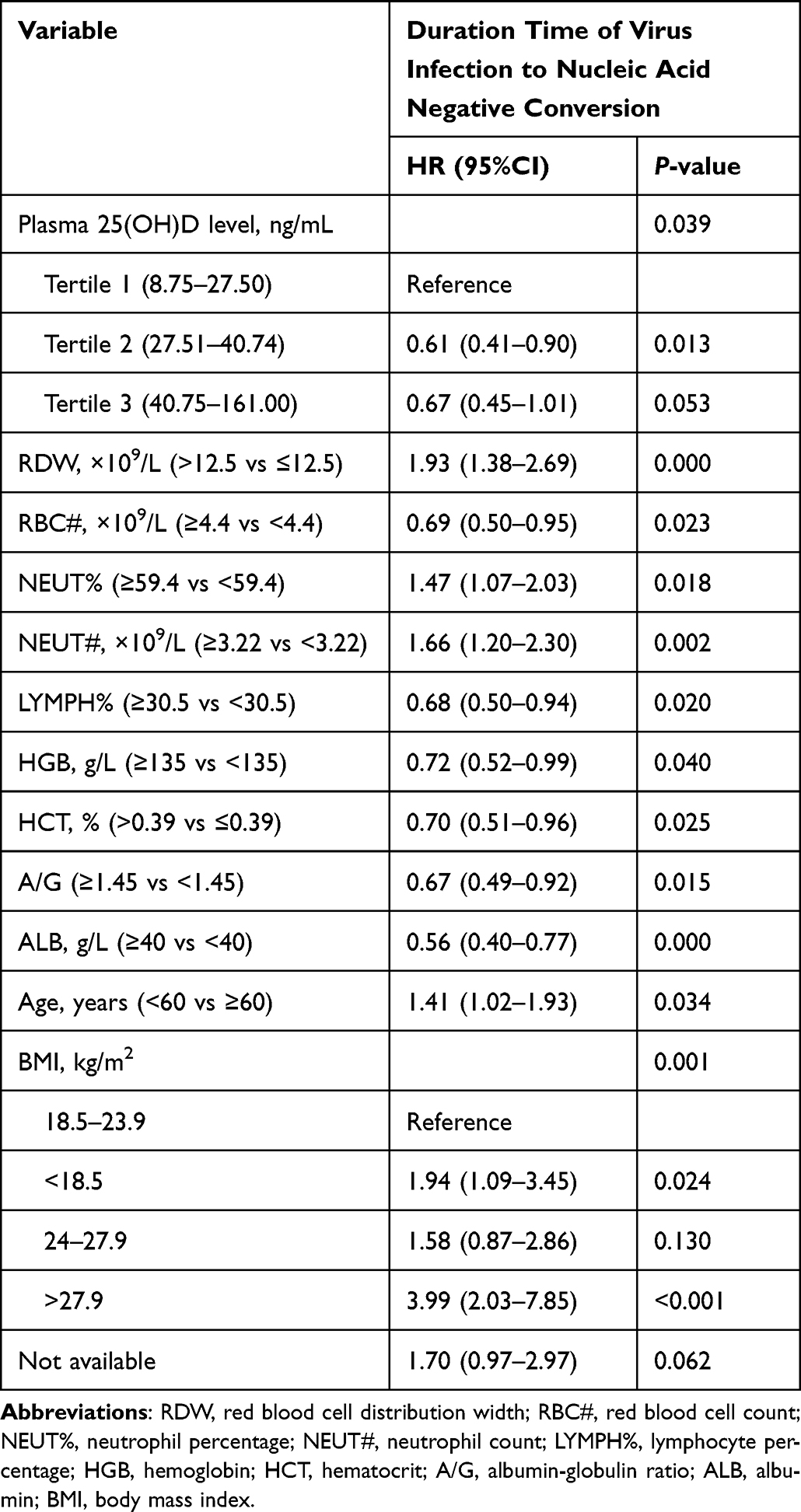 |
Table 2 Parameters That Significantly Associated with Nucleic Acid Negative Conversion Time in COVID-19 Patients Suggested by the Univariate Cox Proportional Hazard Regression Analysis (N=158, P<0.05) |
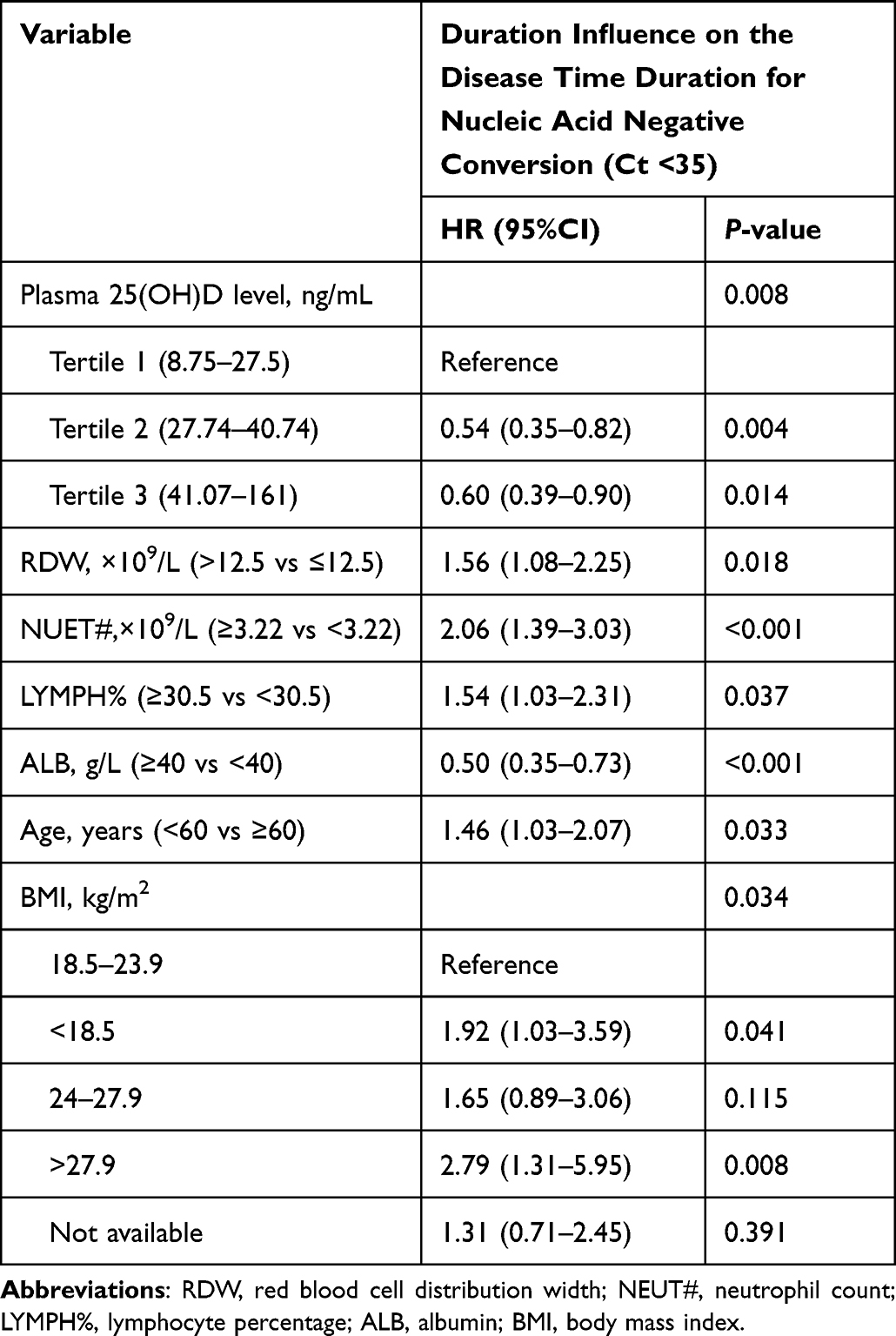 |
Table 3 Multivariate Cox Proportional Hazard Regression Analysis of the Associations Between Total 25(OH)D Level and Nucleic Acid Negative Conversion Time in COVID-19 Patients (N=158) |
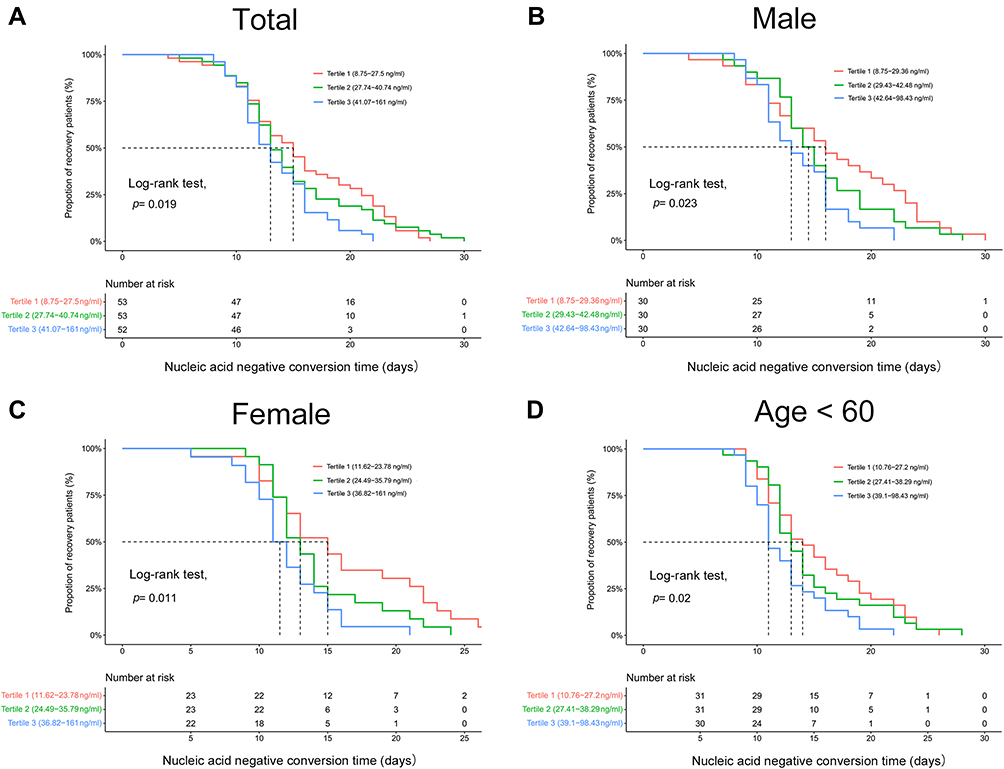 |
Figure 2 Kaplan–Meier plot for duration time from infection to the nucleic acid negative conversion time and the plasma 25(OH)D level in all COVID-19 patients (A), male (B), female group (C) and patients with age ≤60 years old (D). |
Discussion
In the current study, we evaluated the influence of circulating 25(OH)D level and clinical characteristics of COVID-19 infection patients and the time of nucleic acid conversion time in a wave of Omicron infection patients from Shanghai. We found patients with higher plasma 25(OH)D had relatively shorter virus infection duration, suggesting that plasma 25(OH)D level may serve as a predictive factor in COVID-19 patient recovery and vitamin D supplement may be a valuable therapeutic method.
Vitamin D is an essential nutrition and a pleiotropic steroid hormone in human which acts through its transcriptional nuclear receptor VDR (vitamin D receptor). Lung epithelial cells are potential vitamin D targets, with high expressed VDR.20 Previous studies have revealed that vitamin D insufficiency led to higher risk and poorer outcomes in patients with acute respiratory tract infection such as influenza,21,22 and COVID‐19.23–25 Clinical trials suggested that supplementary of vitamin D could significantly decrease the risk of acute respiratory tract infection and the risks of COVID-19 infection.9,26–28 Using animal models of pandemic H1N1 influenza and SARS-CoV-2 infection, Arora et al found that vitamin D deficiency enhanced disease severity,20 and vitamin D sufficiency/supplementation reduced the inflammation level post infection with H1N1 influenza or SARS-CoV-2. Similar results were noticed from previous studies. 25(OH)D played a prophylactic effect on influenza A virus infection by downregulating pro-inflammatory cytokines IL-5 and IFN-γ in mice.29 Furthermore, 1a,25-(OH)2D treatments could reduce the inflammation levels in lipopolysaccharide-induced lung injury model through regulating expression of angiotensin converting enzymes (ACEs, targets of SARS-CoV-2) in rat lung epithelium.30 A recent systematic review and meta-analysis showed that vitamin D supplementation significantly reduced ICU admission rate, the need for mechanical ventilation as well as mortality from COVID-19.31 However, most of the included epidemiological studies in this meta-analysis were non-RCT studies and the sample size of the studies was relatively small (sample size range from 43 to 508).31 Moreover, the vitamin D intervention dose and duration in each individual study is also varied, which may contribute to the heterogeneity between the studies.31 Thus, more well-designed studies with larger sample size are warranted to address whether vitamin D intervention could reduce the infection duration and severity of the COVID-19 virus infected patients in future.
We also noticed several blood traits were associated with infection duration time in COVID-19 patients. Serum albumin, which usually reflect patient nutritional status, is important for maintenance of healthy organs. In this study, decreased albumin levels were associated with longer infection duration time, which is consistent with a previous study that found decreased albumin level delays the clearance of SARS-CoV-2 RNA.32 Meanwhile, a previous retrospective cohort study performed by Huang et al reported that hypoalbuminemia has a negative impact on the immune response and increases short-term mortality in hospitalized patients with acute infectious diseases.33 Red blood cell distribution width (RDW), a parameter reflecting the heterogeneity of red blood cell volume, which indicates the variability of circulating red blood cell size, is a potential clinical indicator to reflect the prognosis of COVID-19 patients.34 Here, we noticed higher RDW was associated with longer infection duration time, which verified the results reported by Foy et al.35 We noticed that higher neutrophil percentage and lymphocyte cell number in COVID-19 patients were associated with longer infection duration time, which is consistent with the previous study reported that higher lymphocyte number is usually correlated with more severe disease status in COVID-19 patients.36 Moreover, Huang et al found that patients with ICU admission had a higher neutrophil count than patients without ICU admission.37 These results suggested that the immune status of COVID-19 patients may influence the infection duration time.
Besides the blood parameters, we also noticed that patients with obesity were associated with prolonged nucleic acid conversion. We noticed that patients with higher BMI usually have lower plasma 25(OH)D level, which is consistent with previous analysis.38 Severe obesity (BMI >35) usually promotes respiratory infections and inflammatory lung diseases, which is an additional risk in the case of COVID-19.39 Clinical epidemiological studies also found that patients with hypovitaminosis D and overweight were more associated with severe disease and worse inflammatory response and respiratory parameters.38 These results indicated that the association between vitamin D and nucleic acid conversion may be influenced by the BMI status. In multivariate Cox regression analysis, we found that lower circulating vitamin D was associated with longer nucleic acid conversion time with the adjustments of BMI, suggesting vitamin D is an independent factor for nucleic acid conversion.
While previous studies mainly focus on the Alpha or Delta strain, our study included patients all infected by the Omicron variant. In addition, the plasma 25(OH)D level of each patient were tested at the admission time to ensure the validity of patients’ vitamin D status. Some limitations should be acknowledged. First, the retrospective data represented a relatively low number of patients from a single hospital center and prospective cohort studies with larger sample size or RCT studies should be conducted to verify our results. Second, the severity status of most COVID-19 patients was only asymptomatic to mild patients. Whether vitamin D level was associated with infection duration time in those patients with higher severity are still unknown. Finally, the biological availability of vitamin D in human body depends on the genetic background and the vitamin D binding protein level.40 Whether the bioavailable 25(OH)D showed stronger association with the infection duration still needs to be addressed. Moreover, the information of vitamin D supplements used or vitamin D fortified food intake levels of the recruited patients are missing. These limitations showed be addressed with more well-designed clinical studies.
Conclusion
This study demonstrated that higher plasma 25(OH)D in COVID-19 patients was associated with shorter infection duration time, suggesting the antiviral activities of vitamin D. Well-designed randomized controlled trials with larger sample size are warranted to address whether vitamin D could be used as therapeutic regimens to improve clinical outcomes of COVID-19 infected patients.
Abbreviations
vitD, plasma 25(OH)D level; WBC#, white blood cell count; RDW, red blood cell distribution width; RBC#, red blood cell count; PLT#, platelet count; NEUT%, neutrophil percentage; MPV, mean platelet volume; NEUT#, neutrophil count; MONO%, monocyte percentage; MONO#, monocyte count; MCHC, mean corpuscular hemoglobin concentration; MCV, mean corpuscular volume; LYMPH%, lymphocyte percentage; MCH, mean corpuscular hemoglobin; HGB, hemoglobin; LYMPH#, lymphocyte count; HCT, hematocrit; EO#, eosinophil count; EO%, eosinophil percentage; BASO%, basophil percentage; BASO#, basophil count; A/G, albumin-globulin ratio; ALB, albumin; ALP, alkaline phosphatase; ALT, alanine aminotransferase; AST, aspartate aminotransferase; UREA, urea; CREA, creatinine; DBIL, direct bilirubin; GGT, γ-glutamyl transpeptidase; TBIL, total bilirubin; TP, total protein; TBA, total biliary acid; UA, uric acid; PA, prealbumin; ADA, adenosine deaminase; eGFR, estimated glomerular filtration rate; CG, cholyglycine.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported, in part, by the National Natural Science Foundation of Shanghai (Grant No. 20ZR1434100), and the Shanghai Shenkang Three-Year Action grant (SHDC2022CRS031).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ye Q, Wang B, Mao J, et al. Epidemiological analysis of COVID-19 and practical experience from China. J Med Virol. 2020;92(7):755–769. doi:10.1002/jmv.25813
2. Zhang X, Zhang W, Chen S. Shanghai’s life-saving efforts against the current omicron wave of the COVID-19 pandemic [published correction appears in Lancet. 2022 May 19;:]. Lancet. 2022;399(10340):2011–2012. doi:10.1016/S0140-6736(22)00838-8
3. Cheung PH, Chan CP, Jin DY. Lessons learned from the fifth wave of COVID-19 in Hong Kong in early 2022. Emerg Microbes Infect. 2022;11(1):1072–1078. doi:10.1080/22221751.2022.2060137
4. Diagnosis and treatment protocol for novel coronavirus pneumonia (Trial Version 9); 2022. Available from: http://www.gov.cn/zhengce/zhengceku/2022-03/15/content_5679257.htm.
5. Luo L, Ye J, Shao C, et al. Vitamin D status presents different relationships with severity in metabolic-associated fatty liver disease patients with or without hepatitis B infection. Nutrients. 2022;14(10):2114. doi:10.3390/nu14102114
6. Jeon SM, Shin EA. Exploring vitamin D metabolism and function in cancer. Exp Mol Med. 2018;50(4):1–14. doi:10.1038/s12276-018-0038-9
7. de La Puente-Yagüe M, Cuadrado-Cenzual MA, Ciudad-Cabañas MJ, Hernández-Cabria M, Collado-Yurrita L. Vitamin D: and its role in breast cancer. Kaohsiung J Med Sci. 2018;34(8):423–427. doi:10.1016/j.kjms.2018.03.004
8. Jagannath VA, Filippini G, Di Pietrantonj C, et al. Vitamin D for the management of multiple sclerosis. Cochrane Database Syst Rev. 2018;9(9):CD008422. doi:10.1002/14651858.CD008422.pub3
9. Martineau AR, Jolliffe DA, Hooper RL, et al. Vitamin D supplementation to prevent acute respiratory tract infections: systematic review and meta-analysis of individual participant data. BMJ. 2017;356:i6583. doi:10.1136/bmj.i6583
10. Kaufman HW, Niles JK, Kroll MH, Bi C, Holick MF. SARS-CoV-2 positivity rates associated with circulating 25-hydroxyvitamin D levels. PLoS One. 2020;15(9):e0239252. doi:10.1371/journal.pone.0239252
11. Merzon E, Tworowski D, Gorohovski A, et al. Low plasma 25(OH) vitamin D level is associated with increased risk of COVID-19 infection: an Israeli population-based study. FEBS J. 2020;287(17):3693–3702. doi:10.1111/febs.15495
12. D’Avolio A, Avataneo V, Manca A, et al. 25-hydroxyvitamin D concentrations are lower in patients with positive PCR for SARS-CoV-2. Nutrients. 2020;12(5):1359. doi:10.3390/nu12051359
13. Im JH, Je YS, Baek J, Chung MH, Kwon HY, Lee JS. Nutritional status of patients with COVID-19. Int J Infect Dis. 2020;100:390–393. doi:10.1016/j.ijid.2020.08.018
14. Abdollahi A, Kamali Sarvestani H, Rafat Z, et al. The association between the level of serum 25(OH) vitamin D, obesity, and underlying diseases with the risk of developing COVID-19 infection: a case-control study of hospitalized patients in Tehran, Iran. J Med Virol. 2021;93(4):2359–2364. doi:10.1002/jmv.26726
15. Liu N, Sun J, Wang X, Zhang T, Zhao M, Li H. Low vitamin D status is associated with coronavirus disease 2019 outcomes: a systematic review and meta-analysis. Int J Infect Dis. 2021;104:58–64. doi:10.1016/j.ijid.2020.12.077
16. De Smet D, De Smet K, Herroelen P, Gryspeerdt S, Martens GA. Serum 25(OH)D level on hospital admission associated with COVID-19 stage and mortality. Am J Clin Pathol. 2021;155(3):381–388. doi:10.1093/ajcp/aqaa252
17. Baktash V, Hosack T, Patel N, et al. Vitamin D status and outcomes for hospitalised older patients with COVID-19. Postgrad Med J. 2021;97(1149):442–447. doi:10.1136/postgradmedj-2020-138712
18. Entrenas Castillo M, Entrenas Costa LM, Vaquero Barrios JM, et al. Effect of calcifediol treatment and best available therapy versus best available therapy on intensive care unit admission and mortality among patients hospitalized for COVID-19: a pilot randomized clinical study. J Steroid Biochem Mol Biol. 2020;203:105751. doi:10.1016/j.jsbmb.2020.105751
19. Murai IH, Fernandes AL, Sales LP, et al. Effect of a single high dose of vitamin D3 on hospital length of stay in patients with moderate to severe COVID-19: a randomized clinical trial. JAMA. 2021;325(11):1053–1060. doi:10.1001/jama.2020.26848
20. Arora J, Patel DR, Nicol MJ, et al. Vitamin D and the ability to produce 1,25(OH)2D are critical for protection from viral infection of the lungs. Nutrients. 2022;14(15):3061. doi:10.3390/nu14153061
21. Jolliffe DA, Griffiths CJ, Martineau AR. Vitamin D in the prevention of acute respiratory infection: systematic review of clinical studies. J Steroid Biochem Mol Biol. 2013;136:321–329. doi:10.1016/j.jsbmb.2012.11.017
22. Zhu Z, Zhu X, Gu L, Zhan Y, Chen L, Li X. Association between vitamin D and influenza: meta-analysis and systematic review of randomized controlled trials. Front Nutr. 2022;8:799709. doi:10.3389/fnut.2021.799709
23. Lau FH, Majumder R, Torabi R, et al. Vitamin D insufficiency is prevalent in severe COVID-19. medRxiv. 2020. doi:10.1101/2020.04.24.20075838
24. Daneshkhah A, Agrawal V, Eshein A, Subramanian H, Roy HK, Backman V. Evidence for possible association of vitamin D status with cytokine storm and unregulated inflammation in COVID-19 patients. Aging Clin Exp Res. 2020;32(10):2141–2158. doi:10.1007/s40520-020-01677-y
25. Rhodes J, Dunstan F, Laird E, Subramanian S, Kenny RA. COVID-19 mortality increases with northerly latitude after adjustment for age suggesting a link with ultraviolet and vitamin D. BMJ Nutr Prev Health. 2020;3(1):118–120. doi:10.1136/bmjnph-2020-000110
26. Charan J, Goyal JP, Saxena D, Yadav P. Vitamin D for prevention of respiratory tract infections: a systematic review and meta-analysis. J Pharmacol Pharmacother. 2012;3(4):300–303. doi:10.4103/0976-500X.103685
27. Bergman P, Lindh AU, Björkhem-Bergman L, Lindh JD. Vitamin D and respiratory tract infections: a systematic review and meta-analysis of randomized controlled trials. PLoS One. 2013;8(6):e65835. doi:10.1371/journal.pone.0065835
28. Ma H, Zhou T, Heianza Y, Qi L. Habitual use of vitamin D supplements and risk of coronavirus disease 2019 (COVID-19) infection: a prospective study in UK Biobank. Am J Clin Nutr. 2021;113(5):1275–1281. doi:10.1093/ajcn/nqaa381
29. Hayashi H, Okamatsu M, Ogasawara H, et al. Oral supplementation of the vitamin D metabolite 25(OH)D3 against influenza virus infection in mice. Nutrients. 2020;12(7):2000. doi:10.3390/nu12072000
30. Xu J, Yang J, Chen J, Luo Q, Zhang Q, Zhang H. Vitamin D alleviates lipopolysaccharide‑induced acute lung injury via regulation of the renin‑angiotensin system. Mol Med Rep. 2017;16(5):7432–7438. doi:10.3892/mmr.2017.7546
31. Tentolouris N, Samakidou G, Eleftheriadou I, Tentolouris A, Jude EB. The effect of vitamin D supplementation on mortality and intensive care unit admission of COVID-19 patients. A systematic review, meta-analysis and meta-regression. Diabetes Metab Res Rev. 2022;38(4):e3517. doi:10.1002/dmrr.3517
32. Fu Y, Han P, Zhu R, et al. Risk factors for viral RNA shedding in COVID-19 patients. Eur Respir J. 2020;56(1):2001190. doi:10.1183/13993003.01190-2020
33. Huang W, Sun Y, Xing Y, Wang C. Functional impairment and serum albumin predict in-hospital mortality in nonagenarians with acute infection: a retrospective cohort study. BMC Geriatr. 2019;19(1):269. doi:10.1186/s12877-019-1301-1
34. Henry BM, Benoit JL, Benoit S, et al. Red Blood Cell Distribution Width (RDW) predicts COVID-19 severity: a prospective, observational study from the Cincinnati SARS-CoV-2 emergency department cohort. Diagnostics. 2020;10(9):618. doi:10.3390/diagnostics10090618
35. Foy BH, Carlson JCT, Reinertsen E, et al. Association of red blood cell distribution width with mortality risk in hospitalized adults with SARS-CoV-2 infection. JAMA Netw Open. 2020;3(9):e2022058. doi:10.1001/jamanetworkopen.2020.22058
36. Wang C, Deng R, Gou L, et al. Preliminary study to identify severe from moderate cases of COVID-19 using combined hematology parameters. Ann Transl Med. 2020;8(9):593. doi:10.21037/atm-20-3391
37. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China [published correction appears in Lancet. 2020 Jan 30;:]. Lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
38. Di Filippo L, Allora A, Doga M, et al. Vitamin D levels are associated with blood glucose and BMI in COVID-19 patients, predicting disease severity. J Clin Endocrinol Metab. 2022;107(1):e348–e360. doi:10.1210/clinem/dgab599
39. Biesalski HK. Obesity, vitamin D deficiency and old age a serious combination with respect to coronavirus disease-2019 severity and outcome. Curr Opin Clin Nutr Metab Care. 2021;24(1):18–24. doi:10.1097/MCO.0000000000000700
40. Li C, Chen P, Duan X, et al. Bioavailable 25(OH)D but not total 25(OH)D is an independent determinant for bone mineral density in Chinese postmenopausal women. EBioMedicine. 2017;15:184–192. doi:10.1016/j.ebiom.2016.11.029
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
COVID-19 and Saudi Arabia: Awareness, Attitude, and Practice
Fawzy MS, AlSadrah SA
Journal of Multidisciplinary Healthcare 2022, 15:1595-1618
Published Date: 26 July 2022
Comparison of the Diagnostic Performance of a Rapid Antigen Test with Real-Time Polymerase Chain Reaction for Detection of SARS-CoV-2 Among Patients Diagnosed with COVID-19 at Selected Hospitals in Addis Ababa, Ethiopia
Desalegn Z, Sebre S, Yohannes M, Seman A, Shiferaw W, Ademe M, Biazin H, Firdawoke E, Asemamaw Y, Teka B, Teshome S, Amogne W, Addissie A, Gebrehiwot Y, Kantelhardt E, Abebe T
Infection and Drug Resistance 2022, 15:4299-4305
Published Date: 6 August 2022
A Pilot Study of 0.4% Povidone-Iodine Nasal Spray to Eradicate SARS-CoV-2 in the Nasopharynx
Sirijatuphat R, Leelarasamee A, Puangpet T, Thitithanyanont A
Infection and Drug Resistance 2022, 15:7529-7536
Published Date: 21 December 2022
Distinct Features of Vascular Diseases in COVID-19
Ceasovschih A, Sorodoc V, Shor A, Haliga RE, Roth L, Lionte C, Onofrei Aursulesei V, Sirbu O, Culis N, Shapieva A, Tahir Khokhar MA, Statescu C, Sascau RA, Coman AE, Stoica A, Grigorescu ED, Banach M, Thomopoulos C, Sorodoc L
Journal of Inflammation Research 2023, 16:2783-2800
Published Date: 6 July 2023
Re-Emerging COVID-19: Controversy of Its Zoonotic Origin, Risks of Severity of Reinfection and Management
Chala B, Tilaye T, Waktole G
International Journal of General Medicine 2023, 16:4307-4319
Published Date: 20 September 2023