Back to Journals » Journal of Inflammation Research » Volume 15
An Overview of Neurological and Psychiatric Complications During Post-COVID Period: A Narrative Review
Authors Li D, Wang Q ![]() , Jia C, Lv Z, Yang J
, Jia C, Lv Z, Yang J ![]()
Received 20 May 2022
Accepted for publication 19 July 2022
Published 26 July 2022 Volume 2022:15 Pages 4199—4215
DOI https://doi.org/10.2147/JIR.S375494
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ning Quan
Dan Li,1,2 Qiang Wang,3 Chengyou Jia,1 Zhongwei Lv,1 Jianshe Yang1,3
1Shanghai Tenth People’s Hospital, Tongji University School of Medicine, Shanghai, 200072, People’s Republic of China; 2Sun Yat-Sen Memorial Hospital, Sun Yat-Sen University, Guangzhou, 510120, People’s Republic of China; 3Basic Medical School, Gansu Medical College, Pingliang, 744000, People’s Republic of China
Correspondence: Jianshe Yang, Shanghai Tenth People’s Hospital, Tongji University School of Medicine, Shanghai, 200072, People’s Republic of China, Tel/Fax +86-21-66302721, Email [email protected]
Abstract: The coronavirus disease 2019 (COVID-19), induced by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is a multi-organ and multi-system disease with high morbidity and mortality in severe cases due to respiratory failure and severe cardiovascular events. However, the various manifestations of neurological and psychiatric (N/P) systems of COVID-19 should not be neglected. Some clinical studies have reported a high risk of N/P disorders in COVID-19 and post-COVID-19 patients and that their outcomes were positively associated with the disease severity. These clinical manifestations could attribute to direct SARS-CoV-2 invasion into the central nervous system (CNS), which is often complicated by systemic hypoxia, the dysfunctional activity of the renin–angiotensin system and other relevant pathological changes. These changes may remain long term and may even lead to persistent post-COVID consequences on the CNS, such as memory, attention and focus issues, persistent headaches, lingering loss of smell and taste, enduring muscle aches and chronic fatigue. Mild confusion and coma are serious adverse outcomes of neuropathological manifestations in COVID-19 patients, which could be diversiform and vary at different stages of the clinical course. Although lab investigations and neuro-imaging findings may help quantify the disease’s risk, progress and prognosis, large-scale and persistent multicenter clinical cohort studies are needed to evaluate the impact of COVID-19 on the N/P systems. However, we used “Boolean Operators” to search for relevant research articles, reviews and clinical trials from PubMed and the ClinicalTrials dataset for “COVID-19 sequelae of N/P systems during post-COVID periods” with the time frame from December 2019 to April 2022, only found 42 in 254,716 COVID-19-related articles and 2 of 7931 clinical trials involved N/P sequelae during post-COVID periods. Due to the increasing number of infected cases and the incessant mutation characteristics of this virus, diagnostic and therapeutic guidelines for N/P manifestations should be further refined.
Keywords: COVID-19, neurological, post-COVID, psychiatric, SARS-CoV-2, sequelae
Introduction
The coronavirus disease 2019 (COVID-19), induced by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), is a multi-organ and multi-system disease1 and a global pandemic, with more than 500 million confirmed cases and 6 million deaths. COVID-19 has high morbidity because the SARS-CoV-2, especially its latest Omicron variant,2 is highly infectious, can be transmitted via multiple routes and has high mortality in severe cases due to respiratory failure and lethal cardiovascular events.3,4
As the neurological system is susceptible to SARS-CoV-2 infection,5–7 the various manifestations of neurological and psychiatric (N/P) systems during its acute and subsequent phases should not be neglected. Clinical studies reported a high risk of N/P disorders in COVID-19 and post-COVID-19 patients and also found that their outcomes were positively associated with the severity of COVID-19.8–10 These clinical manifestations occur due to the direct invasion of SARS-CoV-2 into the central nervous system (CNS), often complicated by systemic hypoxia, dysfunctional activity of the renin–angiotensin system and other relevant pathological changes. These changes may remain long term and persistently causing post-COVID-19 CNS-related symptoms such as difficulties in memory, attention and focus, persistent headaches, lingering loss of sense of smell and taste, enduring muscle aches and chronic fatigue. Mild confusion and coma are among the most serious adverse outcomes of the neuropathological manifestations in COVID-19 patients.11,12 N/P manifestations in COVID-19 patients are diversiform and vary at different stages of their clinical course. Though lab investigations and neuro-imaging findings are helpful in quantifying the disease progress and patients’ risks and prognosis, large-scale and persistent multicenter clinical cohort studies are needed to evaluate the impact and interaction of COVID-19 on the N/P systems. Due to the increasing population being infected and the continual mutation capabilities of this virus, symptomatic and standard therapy practices for N/P manifestations should be further refined, and decisions of N/P sequelae during post-COVID should be made with caution.
Based on our current understanding of COVID-19 and SARS-CoV-2, we used “Boolean Operators” such as AND, OR and NOT to search relevant research articles, reviews and clinical trials from PubMed and the ClinicalTrials database for “COVID-19 sequelae of N/P systems during post-COVID periods”; the time frame of the data is from December 2019 to April 2022. A total of 254,716 reviews and research articles were obtained from the PubMed database, among which only 918 articles were associated with N/P research, and 42 among them reported on N/P sequelae during the post-COVID-19. In the ClinicalTrials.gov dataset, 7931 clinical trials related to COVID-19 were from major countries worldwide, among which 13 trials were closely associated with N/P research, and only 2 focused on N/P sequelae during post-COVID-19 (Figure 1). We reviewed these studies to provide an overall understanding of post-COVID impacts on the N/P systems and evaluated the management of post-COVID sequelae on the N/P systems, in order to refine the diagnostic and therapeutic guidelines for N/P manifestations.
 |
Figure 1 Flow chart of PubMed and clinical Trials studies. COVID-19: All references or trials related to COVID-19; COVID-19-N/P: All references or trials related to COVID-19 with neurological and psychiatric manifestations; COVID-19-N/P-Sequelae: All references or trials related to COVID-19 with neurological and psychiatric manifestations during the post-COVID period. |
COVID-19 – a Multi-Organ/System Disease
COVID-19 is a complex disease that can affect multiple organs and systems of the body. Traditional treatments such as drugs, mono-antibodies and vaccines have had limited treatment efficacies. Deep learning (DL) methods have shown promising potential in helping to better understand its underlying mechanisms, which has led to drug discoveries and the identification of feasible clinical therapies. For instance, ACE2 can lead the viruses to enter host cells, allowing antiviral components to block their expression and efficiently inhibit the infection, but at the expense of potential impact on the renin–angiotensin system (RAS), which could result in abnormal glomeruli filter rate, blood pressure fluctuation and even cardiac dysfunction. This multi-system problem complicates clinical decision-making for treating COVID-19, and in this regard, DL has been shown to relieve some of the workloads.
Commonly, DL can be performed through generative adversarial networks (GANs), extreme learning machines (ELM), and long-/short-term memory (LSTM). They can offer physicians and researchers a user-friendly platform to integrate a continuum of structured and unstructured data, thereafter accelerating decision-making processes for diagnosing and treating COVID-19.13,14
Immediate and Post-Impact of COVID-19 on Neurological and Psychiatric Systems
Along with high morbidity and mortality due to pulmonary and cardiovascular events, COVID-19 patients often suffer from various neurological and psychiatric lesions during their acute and subsequent phases. It is estimated that among the 300 million confirmed COVID-19 cases worldwide, about 40,000 to 200,000 patients have had N/P symptoms and experienced neurological complications. Existing clinical studies have reported a prevalence of ≥50% N/P symptoms in the acute phase of hospitalized COVID-19 patients, posing concerns about the potential serious N/P adverse outcomes, while interests in the long-term impacts on N/P systems are rare.15 (Figure 1) During the acute COVID-19 period and after recovery, milder neurological manifestations may be common.16 In the first 14–90 days after SARS-CoV-2 infection, patients may present with significant psychiatric symptoms compared to those with several other acute illnesses.17 Ischemic and hemorrhagic strokes are the severe neurological manifestations of COVID-19 patients18 and have a higher risk of cerebrovascular events such as ischemic stroke and intracranial hemorrhage, comparable to the incidence of 10% in patients with encephalopathy. In a COVID-19 case report, it was reported that patients had clinical manifestations of Guillain-Barré syndrome (GBS), though this result is yet to be validated in large-scale epidemiological studies.19 In a previous study, the researchers reported that people with neuromuscular disease (NMD) could potentially be infected with SARS-CoV-2 and develop severe COVID-19 conditions. Moreover, these NMD patients accompanied with COVID-19 are unmanageable due to the absence of effective pharmacological and rehabilitative approaches.20 In addition, the relationship between COVID-19 and several neurological diseases, such as parkinsonism and dementia, is equivocal, and research data on such topics are sparse.17 Based on numerous studies and meta-analyses, it can be inferred that COVID-19 patients often present with mild and moderate N/P manifestations in the acute phase, but severe and disabling neurological disorders are uncommon.21 Further, it may be reasonable to assume that severe neuropsychiatric sequelae such as postencephalitis, Parkinson’s disease (PD) and new-onset dementia do not occur during the early period of COVID-19 unless the delay time is more than one year.
The Incidence of N/P Systems Disorders in COVID-19 Patients
A recent retrospective cohort study based on the electronic health records of COVID-9 patients showed that almost one-third of the 236,379 patients reported neurological or psychiatric symptoms within 6 months of their COVID-19 diagnosis.22 The estimated incidence of N/P disorders in these patients admitted to the intensive care unit (ICU) was 46.42%, compared with 33.62% in the overall group. For individual N/P manifestations in this study, the incidence of intracranial hemorrhage was 0.56%, 2.10% for ischemic stroke, 0.11% for PD, 0.67% for dementia, 17.39% for anxiety disorder, and 1.40% for mental disorder. However, the incidence of ICU admission was 6.62% for ischemic stroke, 2.66% for intracranial hemorrhage, 0.26% for PD, 1.74% for dementia, 19.15% for anxiety disorders and 2.77% for psychotic disorders, with the incidence being higher in patients with severe disease. Thus, the prevalence is influenced by disease severity, ICU admission, and encephalopathy.
Taquet et al22 investigated the incidence of various neurological and psychiatric disorders, including ischemic stroke, intracranial hemorrhage, PD, GBS, muscular nerve connectivity disorders, encephalitis, insomnia, anxiety disorders, and dementia, in COVID-19 patients 6 months after their diagnosis and found a substantial incidence of neurological and psychiatric disorders in those patients even though they did not require hospitalization.
Overall, the severity of the disease has a clear effect on the subsequent neurological diagnosis for patients requiring hospitalization, especially those requiring ICU admission or with encephalopathy have a higher prevalence. There are associations between COVID-19 and neurodegenerative diseases such as PD, which may be a delayed outcome, raising further concerns about post-COVID PD syndrome due to eosinophilic encephalitis. Further, studies supporting a possible association between COVID-19 and dementia have noted that 2.66% of patients >65 years old and 4.72% with encephalopathy were diagnosed with dementia within 6 months of their COVID-19 onset.22
Moreover, encephalopathy is common in critically ill patients with COVID-19. In a cohort study of 2088 COVID-19 patients admitted to the ICU, it was reported that 55% of the cases presented with psychoconfusion.23 Another study involving 509 hospitalized COVID-19 patients showed that 31.8% of the cases had encephalopathy.24 Although data about the incidence and outcomes of COVID-19 accompanied by delirium are variable,25 it is estimated to range from 25% to 33% for hospitalized patients but 65% for those admitted to the ICU.26 After the acute phase of COVID-19, the prevalence of neurological and psychiatric diagnoses was found to be significant during the following 6 months of diagnosis. Indeed, the association between COVID-19, cerebrovascular events and neurodegenerative diagnosis may depend on the severity and subsequent course and prolongation time of COVID-19. A significantly increased risk of psychiatric disorders, such as insomnia, depression, and substance use disorders, exists in COVID-19 survivors, which is more common in a long COVID-19 course. Neurosis and psychosis after the onset of COVID-19 appear to be prevalent and may last for 6 months or more. Common psychiatric disorders (mood and anxiety disorders) are less strongly associated with the incidence of COVID-19 severity compared with neurological disorders.
Manifestations of N/P Systems in COVID-19 Patients
COVID-19 patients have a high-risk tendency for neurological and psychiatric disorders. Various neurological and psychiatric manifestations and adverse outcomes can occur during and after the acute phase, which are related to the severity of the disease. After matching propensity scores for other factors such as age or prior cerebrovascular disease, the associated risk of neurological and psychiatric outcomes was reported to be greater in patients requiring hospitalization and was significantly increased in patients requiring ICU admission or developing encephalopathy.22
Encephalopathy is common in severe and critically ill COVID-19 patients with confusion, disorientation and agitation. It is also a risk factor for various N/P manifestations and adverse outcomes during the disease process. A previous cohort study reported that 55% of COVID-19 patients admitted to the ICU presented with delirium, suggesting a high rate of psychiatric incidence in severe patients.23 Another study of 509 hospitalized COVID-19 patients revealed that elder people (66 versus 55 years) were more prone to develop encephalopathy (31.8%), which was also associated with other potential high-risk factors such as male gender (male > female) and comorbidities such as cancer, cerebrovascular disease, chronic kidney disease, diabetes, heart failure, hypertension, or smoking.19
The etiology of encephalopathy in COVID-19 patients remains unclear but can be considered more prominent in critically ill patients suffering from toxic metabolic encephalopathy, cerebrovascular diseases, non-convulsive seizures or adverse drug effects. Increasing risk factors of insanity in COVID-19 patients admitted to the ICU commonly include mechanical ventilation, use of vasopressors or restraint, continuous opioid injections, and others. Further evaluations, such as neuroimaging for patients with focal or lateral neurological signs, and magnetic resonance imaging (MRI) and electroencephalography (EEG) for patients with central nervous system infection, may be needed to exclude other causes.
COVID-19 patients with encephalopathy have a poor prognosis, longer hospital stays, possible dysfunction at discharge, and higher 30-day mortality rates.24 A certain proportion of critically ill patients may suffer from neurological dysfunctions for a long time even after their acute disease is resolved. However, some severe COVID-19 patients with long-term consciousness disorders may recover later,27 with one-third being subjectively cognitively impaired at discharge, while others might improve substantially in subsequent weeks.16 However, the evaluation standard of neurological recovery has not yet been found and should be urgently addressed.
Pathological Mechanisms, Manifestations of N/P Systems in COVID-19
Pathological Mechanisms of N/P Systems in COVID-19
COVID-19 patients usually present with neurological symptoms and psychiatric disorders, and the etiopathology of neurological involvement in these patients is diverse and multifactorial, as described above. The long-term effects of COVID-19 on the CNS are uncertain, though some studies have suggested that encephalopathy could be associated with poorer functional outcomes in COVID-19 inpatients with lasting effects. One study found neuronal damage associated with swelling and inflammation in the brain tissues of a COVID-19 patient.28 Another report described the case of a patient with demyelination causing irreversible neuronal injury,29 in addition to ischemic stroke, cerebral hemorrhage and memory loss, which could be lifelong in some patients.
Neurological Injury Due to Direct Viral Invasion
Previous studies revealed that SARS-CoV-2 could directly invade neurons.30 Moreover, it was shown that SARS-CoV-2 could infect the neurons of organoids, killing some of the neurons and inhibiting synapses formation.31 One important unanswered question is whether SARS-CoV-2 can directly infect brain neurons. Although SARS-CoV-2 particles have been detected in brain specimens,32 there is no relevance between the severity of neuropathology and viral infection.
Autopsy studies provided evidence showing direct endothelial invasion by SARS-CoV-2, along with endodermatitis and vascular lesions in the lungs, heart, kidneys, liver and small intestine.33 Although this evidence suggests that SARS-CoV-2 could infect the cerebral vessels, there is no confirmed manifestation of cerebral vasculitis induced by SARS-CoV-2.34 A clinical study analyzing the neurological or psychiatric effects of 125 COVID-19 patients found that 62% of them presented with a cerebrovascular injury such as stroke and bleeding, and 31% had mental status alteration such as confusion or prolonged unconsciousness, accompanied by swelling and inflammation of brain tissue.35 Other studies showed that the most common neurological effects were stroke and encephalitis. The latter could deteriorate into severe acute disseminated encephalomyelitis, where the brain and spinal cord were inflamed and demyelinated.36,37
Neurological Injury Due to Immune Dysfunction
Currently, there is no clear evidence that SARS-CoV-2 can invade and infect the brain, similar to other viruses. The clinical manifestation of COVID-19 impacting the CNS is simply speculation based on the dysfunction, instability, and hyperactivity of the immune system. The dysregulated systemic immune response to SARS-CoV-2 infection has been suggested to be associated with damage and dysfunction to other organs.38,39 Antibodies directed against the virus produced by the immune system appear to react with neuronal tissues. Damage to the nervous system or other organs may disappear over time or cause persistent effects in long COVID-19 course.
Dysfunction and sustained activation of inflammation due to a cytokine storm may be an alternative mechanism of nervous system injury in SARS-CoV-2 infection. The C-reactive protein (CRP) and leukocytes are major inflammatory markers, with an abnormal elevation in their levels indicating the presence of or an imminent cytokine storm that could cause vascular leakage, activation of the complement and coagulation cascade, in addition to high levels of D-dimer suggesting potential hypercoagulability and endogenous fibrinolysis effects. Further, an increase in some cytokines such as IL-6, IL-1 and TNF secretion after SARS-CoV-2 infection may activate the hypothalamic–pituitary–adrenal cortex (HPA) axis, the core factor regulating systemic immunity, inducing the blood–brain barrier (BBB) dysfunction and neurovascular inflammation. Moreover, micro-environmental alterations can induce vasodilatation, hypercarbonation, hypoxia and anaerobic metabolism, which can lead to neuronal swelling, cerebral edema and elevated intracranial pressure, eventually manifesting as neurological dysfunctions.40
SARS-CoV-2 may activate HPA by inducing immunosuppression and lymphopenia, leading to norepinephrine and glucocorticoid release. Furthermore, SARS-CoV-2 spike (S) protein with pro-inflammatory response plays a key role in attacking brain endothelial and destroying the BBB function. Patients with severe COVID-19 exhibit systemic inflammatory signs consistent with cytokine storm. These signs usually include persistent fever and elevated inflammatory markers, pro-inflammatory cytokines and peripheral TNF, TNF-alpha and IL-6. The pro-inflammatory state is prone to endotheliatitis and encephalopathy, and is associated with the risk of thrombotic inflammation, stroke, and other thrombotic events.41 Complement activation is a high-risk event for thrombotic microvascular injury in severe COVID-19 patients.42 Cytokine storms may also contribute to brain damage via microglial activation, neurophagtosis and systemic inflammatory responses.43
Further, encephalopathy and other neurological manifestations occur frequently in COVID-19 regardless of respiratory disease severity, indicating a possible immunological etiology. This is supported by evidence from a retrospective analysis involving 509 hospitalized COVID-19 patients who presented with various neurological manifestations, including myalgias, headache, dysgeusia, anosmia, and encephalopathy. It was documented that 42% of the patients had at least one neurological symptom at onset, and 82% experienced at least one at any time during COVID-19. Further analysis showed that encephalopathy correlated independently with adverse functional outcomes and higher mortality.24 A retrospective analysis of 509 hospitalized COVID-19 patients found that some patients showed multiple neurological symptoms, such as myalgia, headache, taste disturbance, anosmia, and encephalopathy. Among them, 42% had at least one neurological symptom at disease onset, and 82% had at least one neurological symptom during COVID-19, suggesting that encephalopathy was independently associated with adverse outcomes and higher mortality. In addition, this also suggests that encephalopathy and other neurological symptoms often occur in COVID-19, regardless of the severity of the respiratory disease, which could be related to the etiology of the immune system disorder.
Neurological Injury Due to Hypoxia and Ischemia
Acute pneumonia is the most severe pathology in COVID-19 patients, which can cause systemic hypoxia, injuring the brain and nerve cells. Further, metabolic disorders, such as hypoxemia, hydroelectrolyte dysregulation, hormone dysfunction, and accumulation of toxic metabolites, appear to play a role in encephalopathy caused by astrocytic and neuronal damage in patients with moderate-to-severe COVID-19. In the CNS, especially in the brain stem, a certain amount of focal and global hypoxic/ischemic changes and size infarcts were observed, as well as microglial activation and neurophagtosis. However, the accumulation of T lymphocytes in perivascular regions or brain parenchyma was minimal, and the detectable viruses are rare in the brain, independent of histopathological lesions. These findings strongly confirmed that hypoxia and ischemia due to systemic inflammation contributed to neurological injury.44 Furthermore, the neuroimaging findings in server COVID-19 patients were consistent with delayed post-hypoxic leukoencephalopathy, similar to manifestations in patients with non-COVID-19 acute respiratory distress syndrome (ARDS).45,46 These findings further confirm that hypoxia and ischemia are important causes of nervous system damage in COVID-19 patients, especially in severe cases.
Neurological Injury Due to RAS Dysfunction
The renin–angiotensin system (RAS) can perform important functions in neuropathogenesis rather than only in urinary and circulatory systems. The binding of the S protein and ACE2 receptors enables and facilitates SARS-CoV-2 entering host cells, further causing endothelitis and dysfunctional endothelium, disabling mitochondrial function and inactivating endothelial nitric oxide synthetase. A potential mechanism may be that this binding in endothelial cells upregulates redox stress, resulting in AMPK deactivation, MDM2 upregulation, ultimately ACE2 destabilization, and worsening RAS dysregulation.47 Since ACE2 is essential for ensuring homeostasis in the cardiovascular and immune systems, dysregulation of RAS could lead to various secondary cardiovascular and cerebrovascular effects.47 The direct consequences of S protein/ACE2 binding and the immunologic injury eventually cause the deregulation of RAAS and the kinin-kinase system (KKS) through ACE2 down-regulation, while this deregulation may deeply impact the cardiovascular and cerebrovascular homeostasis.48 It has been suggested that endothelial dysfunction during COVID-19 may exacerbate various harmful events by stimulating inflammatory and microvascular thrombosis, as well as pulmonary and extrapulmonary immune thrombosis complications in patients with severe COVID-19.49 Due to the N/P manifestations, dysfunctional RAS activity accounts for various aspects of neuropathogenesis.
Zonulin Hypothesis and Routes for Neuro-Injury
Some unique symptoms of COVID-19, such as anosmia and dysgeusia, suggest the neuroaffinity of SARS-CoV-2 and the possibility of invading the CNS via the olfactory nerves. However, it has been demonstrated that direct viral invasion into the CNS is not the primary route of infection, with a positive rate of SARS-CoV-2 in CSF being <3%.50 Further, a clinical autopsy on 67 patients who died of COVID-19 revealed that the consistently detectable virus was rare in the brain and olfactory bulbs.51 In another study, SARS-CoV-2 was significantly rare in the brain tissue compared to other organs, assuming the low expression level of ACE2 receptors in brain tissues.52 Although an increased MRI signal to the olfactory cortex may imply that viral infection has occurred,53 this makes us consider the involvement of microvascular endothelial cells in this process. These controversial views make us guess the possibility of SARS-CoV-2 accessing the CNS through paracellular pathways of the GI tract. This pathway may rely on the elevated intestinal permeability, internalized viruses infecting retrograde neurons, and then through retrograde neuronal route reaching synapses region linked to brain neurons. Gastrointestinal involvement has been demonstrated by a significant association with the presentation of neurological symptoms, suggesting that the presence of GI symptoms may be a risk factor for developing neurological manifestations and complications.
Nowadays, the Zonulin hypothesis has been used to explain how the virus accesses the nervous system in COVID-19, which sounds reasonable. Briefly, Zonulin is a 47 KDa protein capable of binding and activating the TLR4 receptors and promoting pro-inflammatory cytokine overexpression via MyD-88. Zonulin is secreted into the intestinal lumen through the binding of PAR2 to disassemble tight junctions (TJ) of the intestinal epithelial barrier (IEB). The virus can bind to the brain zonulin receptor to induce Zonulin overexpression and elevate the permeability of BBB through TJ looseness to eventually cause neuroinvasion. Indeed, both neurological and gastrointestinal symptoms are common in COVID-19 inpatients, at 54.5% and 53.2%, respectively.54 However, the association between them needs to be evaluated following this hypothesis. Furthermore, the complement system activated by Zonulin proteins and the cytokine storm induced during viral infection have been confirmed to disrupt the BBB.55
SARS-CoV-2 Entry Route Through Blood Circulation
Typically, viruses in the peripheral circulation can enter the cerebral circulation attributing to the low blood flow rate in the microcirculation, which promotes the effective binding of S proteins to ACE2 receptors in the microvascular endothelium; leading to viral proliferation in endothelial cells to further its spread to the brain and brainstem regions through the surrounding microvascular Vershaw-Robin space. Experimental studies where SARS-CoV-2 was shown to directly infect engineered human vascular organoids in vitro partly provide evidence for this mechanism.30,31 Furthermore, virus-like particles actively crossing endothelial cells in the brain capillary endothelium were observed. So, blood circulation may be a highly likely route for SARS-CoV-2 to infect the brain regions. Consistent with the mechanism of increased intestinal permeability caused by Zonulin overexpression, this may provide the entry of SARS-CoV-2 into the blood or lymphatic system, infecting the endothelial cells of blood or lymphatic vessels, followed by the spread of the virus to CNS.
SARS-CoV-2 Entry Through Retrograde Nerve Route
It is postulated that the retrograde spread through the vagus nerve may be another route for SARS-VoV-2 entering into CNS. This neuroinvasion route may involve vagal afferents from the GI tract and gut-brain axis. Enteric glial cells are the antigen-presenting cells of immune cells of gut-associated lymphoid tissue (GALT). Stimulated by viruses, GALT can initiate immune responses and release IL-6 and other inflammatory factors, which may increase endothelial cell permeability and consequently provide the opportunity for SARS-CoV-2 to infect enteric neuroendothelial cells.56 Indeed, partial diarrhea and gastrointestinal dysfunction in COVID-19 patients may be clinical manifestations of the enteric nervous system/neuroglia which attends the pathogenesis of gastrointestinal COVID-19.57
The Paracellular Pathway for Virus Transmission
Disassemble of cellular tight junctions is another route for a virus entering the blood and transmission, where impairments in TJ have been detected, especially in severe COVID-19 cases. Viruses passing through this pathway may disrupt the epithelial or endothelial barrier, including the BBB. The zonulin hypothesis explains the mechanisms of brain inflammation and neuronal damage induced by the spread of SARS-CoV-2 due to increased BBB permeability and subsequently elevated cytokines such as IL-6 and the overexpression of Zonulin. As described in the above part, Zonulin can regulate intestinal paracellular permeability by disrupting cellular tight junctions. They were also found to be overexpressed in parenteral tissues, such as lung and brain tissues of severe COVID-19 patients. Thus, overexpressed Zonulin can reach the brain tissue and enhance BBB permeability, additionally with the BBB disruption attributed to hypoxia and hyperimmune response, and finally facilitating SARS-CoV-2 entry and damage to CNS of severe COVID-19 patients.58
Clinical Characteristics of N/P Systems in COVID-19
SARS-CoV-2 Neurotropism and Neurological Affliction
SARS-CoV-2 exhibits neurotropism, can modulate immune activation and promote hypercoagulation, thereby affecting brain functions.6,59,60 ACE2 expression was not detected in human brain tissue at the early stage61 until later, low levels of ACE2 mRNA were detected in brain tissues using RT-PCR and determined that ACE2 only had abundant immune activation features in brain endothelial and smooth muscle cells. Furthermore, a small quantity of ACE2 expression was found in neurons and glial cells.62 Besides the classic symptoms of respiratory viral disease, some neurological symptoms like headache, nausea, loss of smell, vomiting, myalgia/fatigue, dizziness, confusion, disorientation, disorders of consciousness and ataxia are usually affected in COVID-19 patients. Viral myositis commonly has the symptoms of myalgia and fatigue,63 which have a high prevalence in Italy.64 Typically, COVID-19-related neurological manifestations have been categorized into CNS, peripheral nervous system (PNS) and skeletal muscle injury manifestations. These symptoms occur mainly in severe patients, most of which emerge at early onset.
The prevalence of neurological manifestations may vary by geographical location and patient characteristics, with most researchers reporting it to be at approximately ≥50%. Meanwhile, more neurological complications were found to be closely associated with the severity of COVID-19. In a Wuhan clinical trial, characteristic neurological manifestations induced by SARS-CoV-2 were identified in 36.4% (78 of 214) of hospitalized patients and accounted for 45.5% in severe cases.63 In another study, it was shown that 57.4% of hospitalized COVID-19 patients had neurological manifestations.65 Furthermore, the in-hospital mortality in COVID-19 patients with neurological disorders was reported to be significantly higher than in those without neurological disorders.66 Other variables such as gender, age, comorbid conditions and undefined genetic factors may also contribute to the diversity of neurological manifestations during the disease course.
Anosmia and dysgeusia were reported in over 80% of COVID-19 patients as common early symptoms.67 In a meta-analysis involving over 27,000 patients, the authors reported that 48% of the patients had olfactory dysfunction.68 These symptoms may be the initial presentation of COVID-19, which can occur alone (not accompanied by nasal congestion) or after discharge. It is speculated that the inflammation-induced micro-environmental alteration of sustentacular cells within the nasal epithelium resulted in transient anosmia rather than the virus directly damaging the olfactory neurons.69 Strong evidence came from the MRI finding of oedematous obstruction in the olfactory cleft of nasal cavities among 20 COVID-19 patients with anosmia,70 which showed that olfactory function could be gradually recovered with the resolution of the obstruction. In another study, it was reported that 33% of COVID-19 patients recovered within 8 days after onset,67 and a survey of non-hospitalized patients with olfactory dysfunction reported that 83% of the patients completely recovered within a mean of 37 days.71
Major Clinical Neurological Manifestations
The major neurological manifestations may include the following: 1) Encephalopathy generally presents with disorders, such as confusion, disorientation, ataxia, agitation, lethargy and altered consciousness, due to hypoxia and electrolyte imbalance; 2) Encephalitis and meningitis usually develop symptoms such as fever, altered mental status, seizures and focal brain abnormalities; 3) Acute cerebrovascular disease and cerebral perfusion abnormalities are generally attributed to the hypercoagulability of the blood. For instance, in COVID-19 patients, stroke incidence is relatively low, and an ischemic stroke is more likely to occur than intracranial hemorrhage during a highly systemic prothrombotic state.72 The risk of stroke may vary based on the severity of the COVID-19. It was found that <1% of patients with mild disease may develop stroke, while the possibility could be as high as 6% in ICU patients.63 Further, patchy microthrombus, lacunar infarction and occasional myelitis are also symptoms of neurological injuries in COVID-19 patients.
Post-Infectious Neurological Manifestations
Viral infection-induced dysregulation of the immune system may have delayed effects on both the CNS and PNS, commonly manifested as acute disseminated encephalomyelitis and acute necrotizing hemorrhagic encephalopathy. Although fewer GBS cases have been reported since the COVID-19 pandemic, no causal relationship has been reported between COVID-19 and GBS risk.19,28,73,74
Neuropsychiatric Manifestations in COVID-19
Long-term medical isolation or home isolation and limited social interaction may lead to anger, fear and anxiety and have a serious negative impact on mental health; inducing psychological disorders such as depression, anxiety and loneliness, and causing post-traumatic stress disorder. One study showed that 65%, 69% and 21% of COVID-19 patients under intensive care developed confusion, agitation and altered consciousness, and separately, 33% developed executive disorder syndrome at discharge,16 suggesting that the psychiatric evaluation is required during hospitalization, especially in the long term of follow-up. Acute stress can evoke behavioral changes by activating the immune system, stimulating corticotropin release, regulating impulsivity and releasing pro-inflammatory cytokines such as IL-6 and TNF-α, causing it to protect oneself from harm. Cytokine storms also activate the sympathetic nervous system and synergistically promote the release of pro-inflammatory factors.
Autonomic Nervous System-Related Manifestations
There is evidence showing that SARS-CoV-2 can directly disrupt the CNS in a direct-invasive or immune-mediated manner. Patients with chronic infection often experience orthostatic hypotension, vascular vagal syncope and postural orthostatic tachycardia syndrome. Tachycardia, chest pain and dyspnea can arise from the abnormal release of adrenaline and norepinephrine, resulting in an orthostatic intolerance syndrome. The virus can cause immune-mediated neurologic syndromes, and studies have found that autoantibodies to the muscarinic and α/β adrenaline receptors can cause autonomic dysfunction.75
Pre-Existing Neurological Disease-Related Manifestations
COVID-19 may synergistically promote pre-existing neurodegenerative diseases, such as PD and dementia, with SARS-CoV-2 neurotropism potentially exacerbating the outcomes in this setting. COVID-19 patients with a previous history of neurological impairment such as stroke have a higher risk of ICU admission, thromboembolic events and new cerebrovascular events arising from thrombotic microangiopathy and hypercoagulable blood status, and a higher mortality rate.76 PD patients with SARS-CoV-2 infection may present with increased anxiety and worsening compliance, which may worsen their symptoms and make needing hospitalization.77
COVID-19-Related N/P Systems Complications
Coagulation-Induced Neuropathy and Associated Neurological Manifestations
SARS-CoV-2 infection may lead to prolonged prothrombin duration, platelet abnormalities, elevated D-dimer levels and increased fibrinogen degradation, ultimately causing an abnormal state of intravascular coagulopathy.78 Patients with severe COVID-19 usually present with hypoxia. Activating hypoxia-induced transcriptional regulation may increase blood viscosity and promote thrombosis, which could lead to severe consequences79 and complications, including venous thromboembolism, acute coronary syndrome, myocardial infarction and cerebral infarction.80,81 In this pathological state, systemic inflammation and coagulopathy present with complex and mutually causal relationships. In summary, systemic inflammation can drive tissue factor-mediated thrombin generation and inhibit endogenous fibrinolysis to activate the coagulation cascade, while causing aberrant activation of the coagulation system that may affect inflammatory activities and aggravate inflammation-mediated nerve injury. Therefore, the abnormal activation and release of the coagulation cascade may lead to the massive formation of thrombosis, cause local ischemia and increase the risk of ischemic stroke, especially in elderly COVID-19 patients, and could be more severe after ischemic stroke.82,83 Both ischemic and hemorrhagic strokes are cerebrovascular events highly associated with encephalopathy in COVID-19 patients. There is a 10% incidence of ischemic stroke in COVID-19 patients after SARS-CoV-2 infection.22
Risk Factors and Associated Comorbid Conditions in COVID-19
It is reported that an elevated neutrophil-to-lymphocyte ratio may be regarded as an independent risk factor for mortality in hospitalized COVID-19 patients.84 Some COVID-19 patients with ocular dysfunction may often be accompanied by elevated neutrophil counts,85 which mark the formation of extracellular traps and could be due to acute brain injury-induced microvascular occlusion and cerebral hypoperfusion.86 Several comorbidities, such as obesity, high body mass index, diabetes and hypertension, may potentially enhance infection rates and worsen neurological dysfunctions.87–90 Also, it was found that COVID-19 patients could present with more severe neurological manifestations if they have myasthenia gravis91 or multiple sclerosis (MS).92
N/P System Complications in Different Aged COVID-19 Patients
Many studies have demonstrated that the age is also a risk factor of N/P damages in COVID-19 patients. Children and adolescents were greatly impacted by the abnormal social activities during COVID-19 pandemic, resulting in stress on mental health.93 Most elderly COVID-19 patients exposed to a higher lethal risk than the youngsters, especially those concurrent with a certain degree of chronic inflammation may exacerbate the severity of COVID-19. Meanwhile, elderly people with psychiatric disorders may suffer from persistent inflammatory state, and the concurrent COVID-19 can accentuate psychiatric disorders.94,95
N/P System Manifestations of Long-Term COVID-19
Prevalence of N/P Manifestations in Long COVID
Long COVID sequelae are a series of long-lasting disorders in hospitalized or discharged patients following SARS-CoV-2 infection. These symptoms are diverse and may involve almost all organs and tissues of the body. Davis et al96 reported more than 205 symptoms in a study investigating over 3500 patients, among which fatigue, post-exertional malaise and cognitive dysfunction were the most common ones. Of course, these symptoms are very volatile and will be improved or even cured under clinical intervention. However, some of them may relapse and seriously disturb the patient’s physical and mental health.97 It is certain that COVID-19 is a multi-system disease because its symptoms may involve almost all organs and tissues, mainly manifested as viral invasions of the CNS, hypercoagulability of the blood, and neural effects of an immune response.98
The N/P Affliction and Morbidities in Long-Term COVID-19
There is strong evidence showing N/P morbidity in patients with long-lasting COVID-19 disease. A retrospective cohort study investigated the prevalence of various neurological and psychiatric sequelae in post-COVID-19 patients by analyzing the TriNetX electronic health data.22 They found a collection of manifestations such as stroke, nerve disorders, myoneural junction disease and more, which were associated with the severity of COVID-19 but were not so relevant for the psychiatric disorders in terms of incidence.
COVID-19 patients may suffer from these N/P sequelae for a long period. The important issues of concern to clinicians are the severe and widespread neurological and adverse psychiatric outcomes of COVID-19 at onset.16 The psychiatric manifestations were found to be more common during the 14–90 days after SARS-CoV-2 infection.17 The relationship between COVID-19 and ischemic stroke has been well described, and both of them are strong risk factors for hemorrhagic stroke; however, corresponding data on dementia are limited.18 The same relationship between GBS, encephalitis lethargica, PD and COVID-19 have not been verified by large-scale epidemiological studies.19
The Prolonged N/P Manifestations in Long-Term COVID-19
Patients with severe COVID-19 may have neurological complications, such as confusion, cognitive difficulties and memory loss, but different symptoms persist in the long COVID-19 stages after the disappearance of these acute symptoms. They may suffer from prolonged loss of smell and/or taste. One of the most common long-term effects of viral infection on the N/P system of COVID-19 patients is severe fatigue, experienced as severe tiredness and malaise. A study on 143 discharged COVID-19 patients showed that 53% felt tired, while 43% developed shortness of breath within an average of 2 months after symptom onset.64 A clinical study from China found that 25% of patients developed abnormal lung function 3 months after the onset, and 16% were still feeling tired.99 These symptoms have highly similar clinical features to chronic fatigue syndrome and are also known as myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS). Patients with ME/CFS usually exhibit generalized debilitating symptoms, such as fatigue, sleep deprivation, cognitive difficulties, and so on. In addition, the deregulation of the immune system caused by COVID-19 may also lead to various autoimmune diseases, such as inflammation of the vascular system, GBS and persistent PD-like symptoms (Tables 1 and 2).
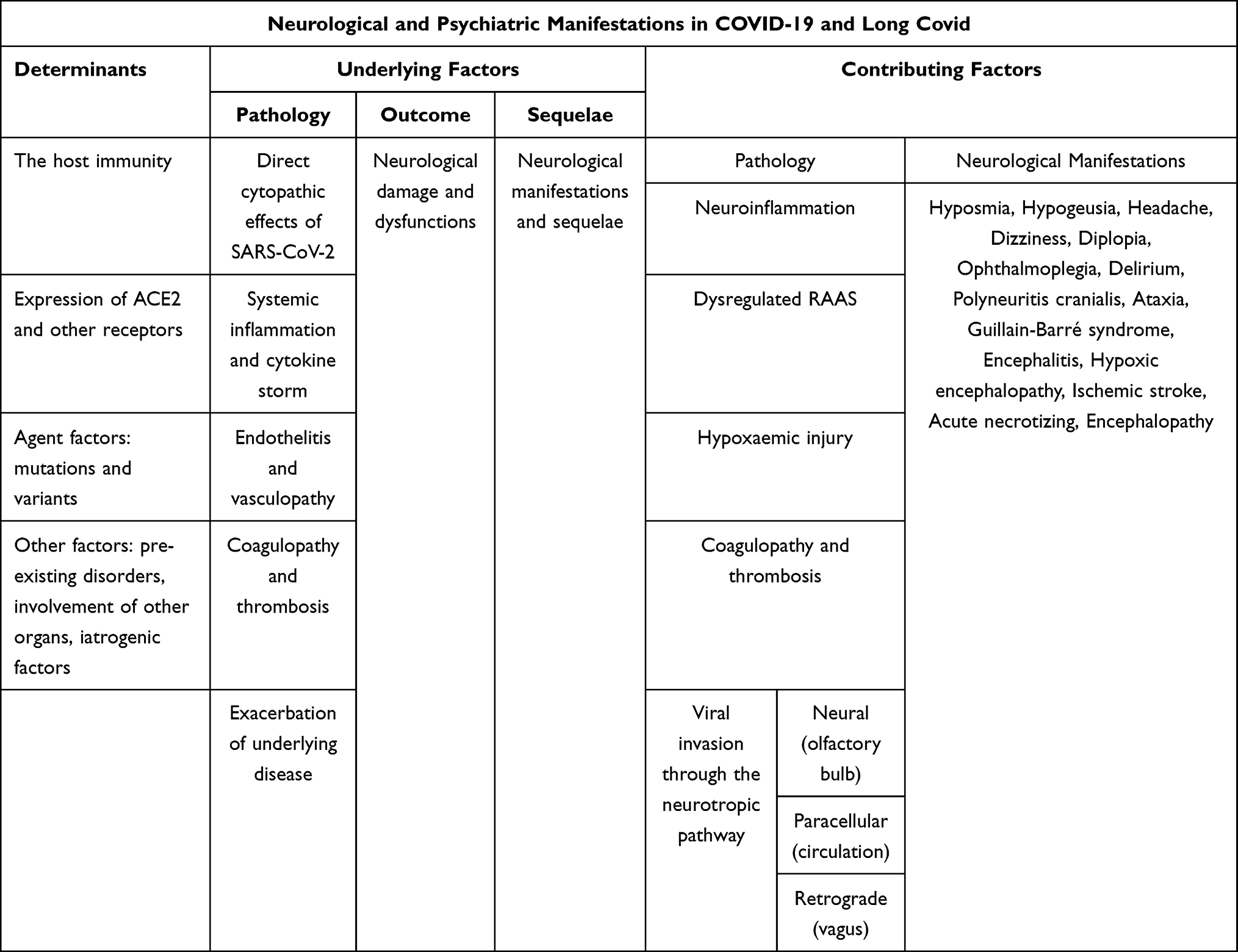 |
Table 1 N/P Complications, Outcomes and Sequelae are Reported as N and P Damage and Dysfunctions |
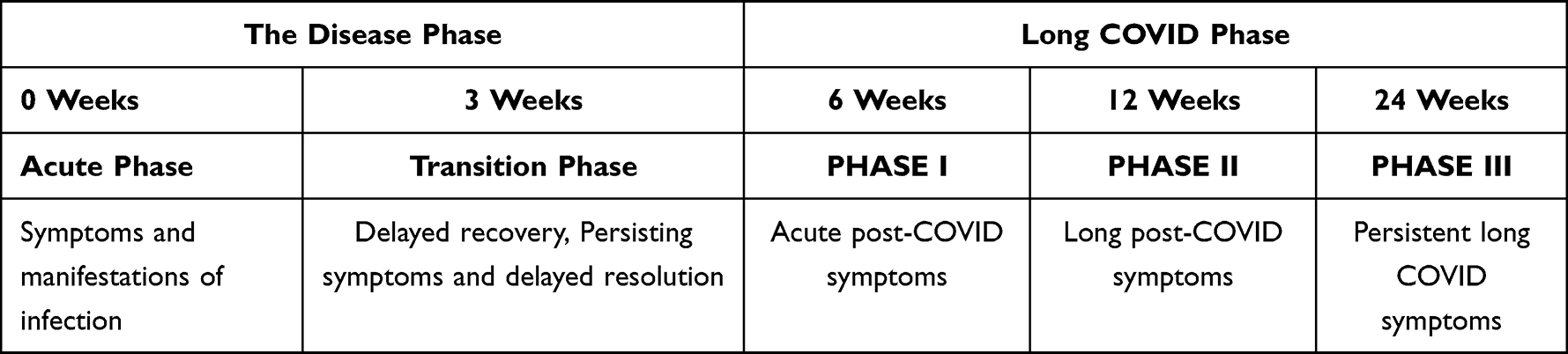 |
Table 2 Timeline for Neurological and Psychiatric Manifestations of COVID-19 |
Managing N/P Manifestations in COVID-19 Patients
Investigations and Imaging for N/P Symptoms
Clinical and laboratory examinations of COVID-19 patients with CNS symptoms usually point to confusion and agitation, with some patients also experiencing lethargy and decreased consciousness.63
Overall, severe COVID-19 patients with CNS symptoms have higher lymphocyte levels, platelet counts, and blood urea nitrogen levels than those without CNS symptoms. No difference was found between mild-to-moderate subgroups. This tendency was also observed in COVID-19 groups with or without muscle symptoms characterized by creatine kinase and lactate dehydrogenase levels.100
Most COVID-19 patients with encephalopathy usually do not have direct evidence from CSF or neuroimaging studies, suggesting the insidious evidence in CSF or the uncertainty of direct viral infection in brain tissues. Some COVID-19 patients’ pathological reports showed no leukocytes in CSF, negative SARS-CoV-2 test by RT-PCR, and nonspecific electroencephalography.25 A study involving 111 ICU patients showed that 57% had electrocardiographic signs of bradycardia, 30% had epileptiform status, and 7% had seizures.101
Neuroimaging Findings in Patients with CNS Symptoms
COVID-19 patients with encephalopathy do not have specific abnormal neuroimaging features. COVID-19-related neuro-pathological patterns on MRI include abnormal medial temporal lobe signals, multifocal white matter lesions visualized by fluid attenuation inversion recovery (FLAIR), and microbleeding in the white matter on diffusion-weighted imaging (DWI). MRI patterns of COVID-19 patients with ischemic stroke commonly show focal or lateralizing signs and leptomeningeal enhancement. After SARS-CoV-2 infection, adult patients with encephalopathy and a few children with concurrent multi-system inflammatory syndrome were found to have cytotoxic lesions in the splenium of the corpus callosum upon MRI examination.102,103
Therapeutic and Rehabilitation Measures
Overall, the N/P symptoms of COVID-19 patients are diverse and vary. They may persist throughout the disease course, even after discharge, and are likely to leave relevant sequelae. However, little is known about rehabilitation strategies regarding the long-term effects of COVID-19 on N/P issues.104 Usually, the symptoms or sequelae of N/P should be treated based on the existing conditions. For instance, the first step in patients with intracranial hemorrhage is to control blood pressure, anticoagulation intervention may be recommended in patients with ischemic stroke, and intravenous immunoglobulin may have some effects in patients with GBS. The German Society of Neurology has developed special nursing guidelines concerning N/P issues and sequelae of COVID-19 patients for hospitalized and post-hospitalized patients.105 The British Association of Neurologists has also proposed guidelines for addressing the risk of concurrent N/P disease in patients with COVID-19. Following these guidelines and a broader consensus, grading the risk of concurrent N/P symptoms in COVID-19 patients and implementing corresponding clinical treatment based on different risk grades have become the temporary standard for managing neurological disorders and their sequelae after a SARS-CoV-2 outbreak. However, the risk–benefit ratio associated with N/P in each COVID-19 patient should be individually assessed and treated to achieve optimal treatment effects.106
The Disease Tolerance Approach
In the current environment of the global COVID-19 pandemic, the primary task is surviving an infection because efforts to eliminate the virus seem currently out of reach.107 Some researchers and clinicians consider SARS-CoV-2 as a completely new virus different from traditional human knowledge, although taxonomically, it belongs to the coronavirus genus. According to traditional prevention and control methods of virus infection, vaccination or drug interventions should have been able to effectively control its transmission. The prevention and control of COVID-19 still require multi-dimensional, systematic and comprehensive measures, such as the government needs to formulate policies to quarantine and maintain social distancing, intensify clinical and scientific research efforts to develop more efficient vaccines and antiviral drugs, explore the detailed underlying mechanisms of their interaction with the virus, and evaluate the positive and side effects comprehensively and objectively.
Antiviral drugs may be effective for mild-to-moderate COVID-19 patients as they have been shown to reduce the length of hospitalization and risk of further spread. For severe patients, antiviral strategies have been less effective as they usually develop ARDS, septic shock and multiple organ failure.
For patients with severe illness, the existing strategy is to maintain physiological functions through supportive measures, such as the use of mechanical ventilators and adequate oxygen uptake. In addition to developing antiviral drugs, medicines that can promote physiological functions should be promoted. These therapies can potentially promote survival rates and reduce the risk of morbidity and mortality through a disease tolerance approach.108
Cell Therapy Strategies and Applications
Initially, it was thought that SARS-CoV-2 could only cause pneumonia, ARDS and respiratory failure. Clinical evidence of its effects on the immune system, gastrointestinal tract, heart, nervous systems and all human tissues and organs were gradually acquired. For COVID-19, whether for its acute symptoms or chronic sequelae, the focus is to specifically address acute injuries, maintain and restore normal physiological functions, and cope with its long-term consequences. Cell therapies can potentially replenish damaged tissues and organs and address disturbed immune system issues.109 In terms of the pathogenesis characteristics of COVID-19, cell therapy should be feasible, but some core factors, such as cell input dose, delivery route, the immunogenicity of heterogeneous cells, autologous cells and others should be strictly considered. Commonly, ACE2 receptors distributed in tissues or organs can promote the cellular tropism of SARS-CoV-2; thus, those with high expression levels of ACE2 may be more prone to SARS-CoV-2 infection. However, not all the tissues or organs with high ACE2 levels do this, indicating that other receptors like TMPRSS2 and NRP1 may be involved in the infectious pathway. The potential cells for COVID-19 therapy may include mesenchymal stem cells (MSCs),110 induced pluripotent stem cells (iPSCs)111 and T cells.112 Oligodendrocyte precursor cells and neural precursor cells may be used to restore and regenerate the depleted myelin sheath layer, indicating that myelin and oligodendrocytes are promising targets to alleviate brain injury.113
Conclusions
COVID-19 presented the comprehensive and complicated impact on neurological and psychiatric systems during acute phase and long COVID. Understanding of long COVID sequelae is still limited. It is extremely urgent to concentrate more research on the acute and long-term consequences of COVID-19, develop safer and more effective treatment modalities. Large-scale and persistent multi-center clinical cohort studies are required to gain a deeper understanding of the sequelae of SARS-CoV-2 infection, especially those of the N/P systems. In terms of the continuously increasing number of infected cases and incessant mutation characteristics of SARS-CoV-2, therapeutic practices for N/P manifestations should be further refined.
Abbreviations
ARDS, acute respiratory distress syndrome; BBB, blood–brain barrier; CNS, central nervous system; COVID-19, coronavirus disease 2019; CRP, C-reactive protein; CSF, cerebrospinal fluid; DL, deep learning; ECG, electroencephalography; ELM, extreme learning machine; FLAIR, fluid-attenuated inversion recovery; GALT, gut-associated lymphoid tissue; GANs, generative adversarial networks; GBS, Guillain-Barré syndrome; GI, gastrointestinal; HPA, hypothalamic-pituitary-adrenocortical; ICU, intensive care unit; IEB, intestinal epithelial barrier; IL-6, interleukin-6; iPSCs, pluripotent stem cells.KKS, Kinin Kallikrein system; LSTM, long/short term memory; ME/CFS, myalgic encephalomyelitis/chronic fatigue syndrome; MRI, magnetic resonance imaging; MS, multiple sclerosis; MSCs, mesenchymal stromal cells; NMD, neuromuscular disease; PD, Parkinson’s disease; RAAS, renin-angiotensin-aldosterone system; RAS, renin–angiotensin system; SARS-CoV-2, severe acute respiratory syndrome coronavirus 2; TJ, tight junctions.
Funding
This work was supported by the National Natural Science Foundation of China (82071964, 72171170), Shanghai Municipal Health Commission (GWV-10.1-XK09), Shanghai Shenkang Center (SHDC2020CR2054B) and Key Research Project of Pingliang Science and Technology (PL-STK-2021A-004).
Disclosure
The authors declared that they had no conflict of interest.
References
1. AbdelMassih AF, Kamel A, Mishriky F, et al. Is it infection or rather vascular inflammation? Game-changer insights and recommendations from patterns of multi-organ involvement and affected subgroups in COVID-19. Cardiovasc Endocrinol Metab. 2020;9(3):110–120. doi:10.1097/XCE.0000000000000211
2. Viana R, Moyo S, Amoako DG, et al. Rapid epidemic expansion of the SARS-CoV-2 Omicron variant in Southern Africa. Nature. 2022;603(7902):679–686. doi:10.1038/s41586-022-04411-y
3. Nyberg T, Ferguson NM, Nash SG, et al. Comparative analysis of the risks of hospitalisation and death associated with SARS-CoV-2 omicron (B.1.1.529) and delta (B.1.617.2) variants in England: a cohort study. Lancet. 2022;399(10332):1303–1312. doi:10.1016/S0140-6736(22)00462-7
4. Krutikov M, Stirrup O, Nacer-Laidi H, et al. Outcomes of SARS-CoV-2 omicron infection in residents of long-term care facilities in England (VIVALDI): a prospective, cohort study. Lancet Healthy Longev. 2022;3(5):e347–e355. doi:10.1016/S2666-7568(22)00093-9
5. Solomon T. Neurological infection with SARS-CoV-2 - the story so far. Nat Rev Neurol. 2021;17(2):65–66. doi:10.1038/s41582-020-00453-w
6. Yachou Y, El Idrissi A, Belapasov V, Ait Benali S. Neuroinvasion, neurotropic, and neuroinflammatory events of SARS-CoV-2: understanding the neurological manifestations in COVID-19 patients. Neurol Sci. 2020;41(10):2657–2669. doi:10.1007/s10072-020-04575-3
7. Harapan BN, Yoo HJ. Neurological symptoms, manifestations, and complications associated with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease 19 (COVID-19). J Neurol. 2021;268(9):3059–3071. doi:10.1007/s00415-021-10406-y
8. Beghi E, Giussani G, Westenberg E, et al. Acute and post-acute neurological manifestations of COVID-19: present findings, critical appraisal, and future directions. J Neurol. 2022;269(5):2265–2274. doi:10.1007/s00415-021-10848-4
9. Hosey MM, Needham DM. Survivorship after COVID-19 ICU stay. Nat Rev Dis Primers. 2020;6(1):60. doi:10.1038/s41572-020-0201-1
10. Stefano GB. Historical insight into infections and disorders associated with neurological and psychiatric sequelae similar to long COVID. Med Sci Monit. 2021;27:e931447. doi:10.12659/MSM.931447
11. Roy D, Ghosh R, Dubey S, Dubey MJ, Benito-León J, Kanti Ray B. Neurological and neuropsychiatric impacts of COVID-19 pandemic. Can J Neurol Sci. 2021;48(1):9–24. doi:10.1017/cjn.2020.173
12. Deng J, Zhou F, Hou W, et al. The prevalence of depression, anxiety, and sleep disturbances in COVID-19 patients: a meta-analysis. Ann N Y Acad Sci. 2021;1486(1):90–111. doi:10.1111/nyas.14506
13. Jamshidi MB, Lalbakhsh A, Talla J, et al. Artificial intelligence and COVID-19: deep learning approaches for diagnosis and treatment. IEEE Access. 2020;8:109581–109595. doi:10.1109/ACCESS.2020.3001973
14. Jamshidi MB, Lalbakhsh A, Talla J, et al. Emerging Technologies During the Era of COVID-19 Pandemic. Studies in Systems, Decision and Control. Springer, Cham; 2021:9–31.
15. Balcom EF, Nath A, Power C. Acute and chronic neurological disorders in COVID-19: potential mechanisms of disease. Brain. 2021;144(12):3576–3588. doi:10.1093/brain/awab302
16. Rogers JP, Chesney E, Oliver D, et al. Psychiatric and neuropsychiatric presentations associated with severe coronavirus infections: a systematic review and meta-analysis with comparison to the COVID-19 pandemic. Lancet Psychiatry. 2020;7(7):611–627. doi:10.1016/S2215-0366(20)30203-0
17. Rogers JP, David AS. A longer look at COVID-19 and neuropsychiatric outcomes. Lancet Psychiatry. 2021;8(5):351–352. doi:10.1016/S2215-0366(21)00120-6
18. Tan YK, Goh C, Leow AST, et al. COVID-19 and ischemic stroke: a systematic review and meta-summary of the literature. J Thromb Thrombolysis. 2020;50:587–595. doi:10.1007/s11239-020-02228-y
19. Keddie S, Pakpoor J, Mousele C, et al. Epidemiological and cohort study finds no association between COVID-19 and Guillain-Barré syndrome. Brain. 2020;144:682–693. doi:10.1093/brain/awaa433
20. Liguori S, Moretti A, Paoletta M, Gimigliano F, Iolascon G. Rehabilitation of neuromuscular diseases during COVID-19: pitfalls and opportunities. Front Neurol. 2021;12:626319. doi:10.3389/fneur.2021.626319
21. Carod-Artal FJ. Post-COVID-19 syndrome: epidemiology, diagnostic criteria and pathogenic mechanisms involved. Rev Neurol. 2021;72(11):384–396. doi:10.33588/rn.7211.2021230
22. Taquet M, Geddes JR, Husain M, Luciano S, Harrison PJ. 6-month neurological and psychiatric outcomes in 236379 survivors of COVID-19: a retrospective cohort study using electronic health records. Lancet Psychiatry. 2021;8(5):416–427. doi:10.1016/S2215-0366(21)00084-5
23. Pun BT, Badenes R, Heras La Calle G, et al; COVID-19 Intensive Care International Study Group. Prevalence and risk factors for delirium in critically ill patients with COVID-19: a multicentre cohort study. Lancet Respir Med. 2021;9(3):239–250. doi:10.1016/S2213-2600(20)30552-X
24. Liotta EM, Batra A, Clark JR, et al. Frequent neurological manifestations and encephalopathy-associated morbidity in COVID-19 patients. Ann Clin Transl Neurol. 2020;7(11):2221–2230. doi:10.1002/acn3.51210
25. Helms J, Kremer S, Merdji H, et al. Neurologic features in severe SARS-CoV-2 infection. N Engl J Med. 2020;382(23):2268–2270. doi:10.1056/NEJMc2008597
26. Garcez FB, Aliberti MJR, Poco PCE, et al. Delirium and adverse outcomes in hospitalized patients with COVID-19. J Am Geriatr Soc. 2020;68(11):2440–2446. doi:10.1111/jgs.16803
27. Abdo WF, Broerse CI, Grady BP, et al. Prolonged unconsciousness following severe COVID-19. Neurology. 2021;96(10):e1437–e1442. doi:10.1212/WNL.0000000000011355
28. Moriguchi T, Harii N, Goto J, et al. A first case of meningitis/encephalitis associated with SARS-Coronavirus-2. Int J Infect Dis. 2020;94:55–58. doi:10.1016/j.ijid.2020.03.062
29. Zanin L, Saraceno G, Panciani PP, et al. SARS-CoV-2 can induce brain and spine demyelinating lesions. Acta Neurochir. 2020;162(7):1491–1494. doi:10.1007/s00701-020-04374-x
30. Song E, Zhang C, Israelow B, et al. Neuroinvasion of SARS-CoV-2 in human and mouse brain. J Exp Med. 2021;218(3):e20202135. doi:10.1084/jem.20202135
31. Mesci P, Macia P, Saleh A, et al. Sofosbuvir protects human brain organoids against SARS-CoV-2. bioRxiv. 2020. doi:10.1101/2020.05.30.125856
32. Matschke J, Lütgehetmann M, Hagel C, et al. Neuropathology of patients with COVID-19 in Germany: a post-mortem case series. Lancet Neurol. 2020;19(11):919–929. doi:10.1016/S1474-4422(20)30308-2
33. Varga Z, Flammer AJ, Steiger P, et al. Endothelial cell infection and endothelitis in COVID-19. Lancet. 2020;395(10234):1417–1418. doi:10.1016/S0140-6736(20)30937-5
34. Thakur KT, Miller EH, Glendinning MD, et al. COVID-19 neuropathology at Columbia University Irving Medical Center/New York Presbyterian Hospital. Brain. 2021;144(9):2696–2708. doi:10.1093/brain/awab148
35. Varatharaj A, Thomas N, Ellul MA, et al. Neurological and neuropsychiatric complications of COVID-19 in 153 patients: a UK-wide surveillance study. Lancet Psychiatry. 2020;7(10):875–882. doi:10.1016/S2215-0366(20)30287-X
36. Paterson RW, Brown RL, Benjamin L, et al. The emerging spectrum of COVID-19 neurology: clinical, radiological and laboratory findings. Brain. 2020;143(10):3104–3120. doi:10.1093/brain/awaa240
37. Ellul MA, Benjamin L, Singh B, et al. Neurological associations of COVID-19. Lancet Neurol. 2020;19(9):767–783. doi:10.1016/S1474-4422(20)30221-0
38. Muccioli L, Pensato U, Cani I, Guarino M, Cortelli P, Bisulli F. COVID-19-associated encephalopathy and cytokine-mediated neuroinflammation. Ann Neurol. 2020;88(4):860–861. doi:10.1002/ana.25855
39. Pilotto A, Padovani A; ENCOVID-BIO Network. Reply to the letter “COVID-19-associated encephalopathy and cytokine-mediated neuroinflammation”. Ann Neurol. 2020;88(4):861–862. doi:10.1002/ana.25856
40. Fotuhi M, Mian A, Meysami S, Raji CA. Neurobiology of COVID-19. J Alzheimers Dis. 2020;76(1):3–19. doi:10.3233/JAD-200581
41. Connors JM, Levy JH. Thromboinflammation and the hypercoagulability of COVID-19. J Thromb Haemost. 2020;18(7):1559–1561. doi:10.1111/jth.14849
42. Magro C, Mulvey JJ, Berlin D, et al. Complement associated microvascular injury and thrombosis in the pathogenesis of severe COVID-19 infection: a report of five cases. Transl Res. 2020;220:1–13. doi:10.1016/j.trsl.2020.04.007
43. Al-Dalahmah O, Thakur KT, Nordvig AS, et al. Neuronophagia and microglial nodules in a SARS-CoV-2 patient with cerebellar hemorrhage. Acta Neuropathol Commun. 2020;8(1):147. doi:10.1186/s40478-020-01024-2
44. Solomon IH, Normandin E, Bhattacharyya S, et al. Neuropathological features of COVID-19. N Engl J Med. 2020;383(10):989–992. doi:10.1056/NEJMc2019373
45. Kandemirli SG, Dogan L, Sarikaya ZT, et al. Brain MRI findings in patients in the intensive care unit with COVID-19 infection. Radiology. 2020;297(1):E232–E235.
46. Radmanesh A, Derman A, Lui YW, et al. COVID-19-associated diffuse leukoencephalopathy and microhemorrhages. Radiology. 2020;297(1):E223–E227. doi:10.1148/radiol.2020202040
47. Lei Y, Zhang J, Schiavon CR, et al. SARS-CoV-2 spike protein impairs endothelial function via downregulation of ACE2. Circ Res. 2021;128(9):1323–1326. doi:10.1161/CIRCRESAHA.121.318902
48. Cooper SL, Boyle E, Jefferson SR, et al. Role of the renin-angiotensin-aldosterone and kinin-kallikrein systems in the cardiovascular complications of COVID-19 and long COVID. Int J Mol Sci. 2021;22(15):8255. doi:10.3390/ijms22158255
49. Bernard I, Limonta D, Mahal LK, Hobman TC. Endothelium infection and dysregulation by SARS-CoV-2: evidence and caveats in COVID-19. Viruses. 2020;13(1):29. doi:10.3390/v13010029
50. Al Saiegh F, Ghosh R, Leibold A, et al. Status of SARS-CoV-2 in cerebrospinal fluid of patients with COVID-19 and stroke. J Neurol Neurosurg Psychiatry. 2020;91(8):846–848. doi:10.1136/jnnp-2020-323522
51. Bryce C, Grimes Z, Pujadas E, et al. Pathophysiology of SARS-CoV-2: targeting of endothelial cells renders a complex disease with thrombotic microangiopathy and aberrant immune response. The Mount Sinai COVID-19 autopsy experience. medRxiv. 2020. doi:10.1101/2020.05.18.20099960
52. Li MY, Li L, Zhang Y, Wang XS. Expression of the SARS-CoV-2 cell receptor gene ACE2 in a wide variety of human tissues. Infect Dis Poverty. 2020;9(1):45. doi:10.1186/s40249-020-00662-x
53. Kandemirli SG, Altundag A, Yildirim D, Tekcan Sanli DE, Saatci O. Olfactory bulb MRI and paranasal sinus CT findings in persistent COVID-19 anosmia. Acad Radiol. 2021;28(1):28–35. doi:10.1016/j.acra.2020.10.006
54. Llorens S, Nava E, Muñoz-López M, Sánchez-Larsen Á, Segura T. neurological Symptoms of COVID-19: the Zonulin Hypothesis. Front Immunol. 2021;12:665300. doi:10.3389/fimmu.2021.665300
55. Santiesteban-Lores LE, Amamura TA, da Silva TF, et al. A double edged-sword - the complement system during SARS-CoV-2 infection. Life Sci. 2021;272:119245.
56. Costela-Ruiz VJ, Illescas-Montes R, Puerta-Puerta JM, Ruiz C, Melguizo-Rodríguez L. SARS-CoV-2 infection: the role of cytokines in COVID-19 disease. Cytokine Growth Factor Rev. 2020;54:62–75. doi:10.1016/j.cytogfr.2020.06.001
57. Villapol S. Gastrointestinal symptoms associated with COVID-19: impact on the gut microbiome. Transl Res. 2020;226:57–69. doi:10.1016/j.trsl.2020.08.004
58. Alquisiras-Burgos I, Peralta-Arrieta I, Alonso-Palomares LA, Zacapala-Gómez AE, Salmerón-Bárcenas EG, Aguilera P. Neurological complications associated with the blood-brain barrier damage induced by the inflammatory response during SARS-CoV-2 infection. Mol Neurobiol. 2020;58:520–535. doi:10.1007/s12035-020-02134-7
59. Wang C, Zhang M, Jr GG, et al. ApoE-isoform-dependent SARS-CoV-2 neurotropism and cellular response. Cell Stem Cell. 2021;28(2):331–342.e5. doi:10.1016/j.stem.2020.12.018
60. Hu J, Jolkkonen J, Zhao C. Neurotropism of SARS-CoV-2 and its neuropathological alterations: similarities with other coronaviruses. Neurosci Biobehav Rev. 2020;119:184–193. doi:10.1016/j.neubiorev.2020.10.012
61. Placantonakis DG, Aguero-Rosenfeld M, Flaifel A, et al. SARS-CoV-2 is not detected in the cerebrospinal fluid of encephalopathic COVID-19 patients. Front Neurol. 2020;11:587384. doi:10.3389/fneur.2020.587384
62. Kumar M, Thakur AK. Neurological manifestations and comorbidity associated with COVID-19: an overview. Neurol Sci. 2020;41(12):3409–3418. doi:10.1007/s10072-020-04823-6
63. Mao L, Jin H, Wang M, et al. Neurological manifestations of hospitalized patients with coronavirus disease 2019 in Wuhan, China. JAMA Neurol. 2020;77(6):683–690. doi:10.1001/jamaneurol.2020.1127
64. Carfì A, Bernabei R, Landi F; Gemelli Against COVID-19 Post-Acute Care Study Group. Persistent symptoms in patients after acute COVID-19. JAMA. 2020;324(6):603–605. doi:10.1001/jama.2020.12603
65. Romero-Sánchez CM, Díaz-Maroto I, Fernández-Díaz E, et al. Neurological manifestations in hospitalized patients with COVID-19: the ALBACOVID registry. Neurology. 2020;95(8):e1060–e1070. doi:10.1212/WNL.0000000000009937
66. Jarrahi A, Ahluwalia M, Khodadadi H, et al. Neurological consequences of COVID-19: what have we learned and where do we go from here? J Neuroinflammation. 2020;17(1):286. doi:10.1186/s12974-020-01957-4
67. Lechien JR, Chiesa-Estomba CM, De Siati DR, et al. Olfactory and gustatory dysfunctions as a clinical presentation of mild-to-moderate forms of the coronavirus disease (COVID-19): a multicenter European study. Eur Arch Otorhinolaryngol. 2020;277(8):2251–2261. doi:10.1007/s00405-020-05965-1
68. Saniasiaya J, Islam MA, Abdullah B. Prevalence of olfactory dysfunction in coronavirus disease 2019 (COVID-19): a meta-analysis of 27492 patients. Laryngoscope. 2021;131(4):865–878. doi:10.1002/lary.29286
69. Bilinska K, Jakubowska P, Von Bartheld CS, Butowt R. Expression of the SARS-CoV-2 entry proteins, ACE2 and TMPRSS2, in cells of the olfactory epithelium: identification of cell types and trends with age. ACS Chem Neurosci. 2020;11(11):1555–1562. doi:10.1021/acschemneuro.0c00210
70. Eliezer M, Hamel AL, Houdart E, et al. Loss of smell in patients with COVID-19: MRI data reveal a transient edema of the olfactory clefts. Neurology. 2020;95(23):e3145–e3152. doi:10.1212/WNL.0000000000010806
71. Paderno A, Mattavelli D, Rampinelli V, et al. Olfactory and gustatory outcomes in COVID-19: a prospective evaluation in non-hospitalized subjects. Otolaryngol Head Neck Surg. 2020;163(6):1144–1149. doi:10.1177/0194599820939538
72. Beyrouti R, Adams ME, Benjamin L, et al. Characteristics of ischaemic stroke associated with COVID-19. J Neurol Neurosurg Psychiatry. 2020;91(8):889–891. doi:10.1136/jnnp-2020-323586
73. Abu-Rumeileh S, Abdelhak A, Foschi M, Tumani H, Otto M. Guillain-Barré syndrome spectrum associated with COVID-19: an up-to-date systematic review of 73 cases. J Neurol. 2021;268(4):1133–1170. doi:10.1007/s00415-020-10124-x
74. Khera D, Didel S, Panda S, Tiwari S, Singh K. Concurrent longitudinally extensive transverse myelitis and Guillain-Barré syndrome in a child secondary to COVID-19 infection: a severe neuroimmunologic complication of COVID-19. Pediatr Infect Dis J. 2021;40(6):e236–e239. doi:10.1097/INF.0000000000003124
75. Guilmot A, Maldonado Slootjes S, Sellimi A, et al. Immune-mediated neurological syndromes in SARS-CoV-2-infected patients. J Neurol. 2020;268(3):751–757. doi:10.1007/s00415-020-10108-x
76. Sluis WM, Linschoten M, Buijs JE, et al. Risk, clinical course, and outcome of ischemic stroke in patients hospitalized with COVID-19: a Multicenter Cohort Study. Stroke. 2021;52(12):3978–3986. doi:10.1161/STROKEAHA.121.034787
77. Suzuki K, Numao A, Komagamine T, et al. Impact of the COVID-19 pandemic on the quality of life of patients with parkinson’s disease and their caregivers: a single-center survey in Tochigi prefecture. J Parkinsons Dis. 2021;11(3):1047–1056. doi:10.3233/JPD-212560
78. Tang N, Bai H, Chen X, Gong J, Li D, Sun Z. Anticoagulant treatment is associated with decreased mortality in severe coronavirus disease 2019 patients with coagulopathy. J Thromb Haemost. 2020;18(5):1094–1099. doi:10.1111/jth.14817
79. Gupta N, Zhao YY, Evans CE. The stimulation of thrombosis by hypoxia. Thromb Res. 2019;181:77–83. doi:10.1016/j.thromres.2019.07.013
80. Lodigiani C, Iapichino G, Carenzo L, et al. Venous and arterial thromboembolic complications in COVID-19 patients admitted to an academic hospital in Milan, Italy. Thromb Res. 2020;191:9–14. doi:10.1016/j.thromres.2020.04.024
81. Helms J, Tacquard C, Severac F, et al. High risk of thrombosis in patients with severe SARS-CoV-2 infection: a multicenter prospective cohort study. Intensive Care Med. 2020;46(6):1089–1098. doi:10.1007/s00134-020-06062-x
82. Siniscalchi A, Could GL. COVID-19 represent a negative prognostic factor in patients with stroke? Infect Control Hosp Epidemiol. 2020;41(9):1115–1116. doi:10.1017/ice.2020.146
83. Siniscalchi A, Gallelli L, Malferrari G, et al. Cerebral stroke injury: the role of cytokines and brain inflammation. J Basic Clin Physiol Pharmacol. 2014;25(2):131–137. doi:10.1515/jbcpp-2013-0121
84. Liu Y, Du X, Chen J, et al. Neutrophil-to-lymphocyte ratio as an independent risk factor for mortality in hospitalized patients with COVID-19. J Infect. 2020;81(1):e6–e12. doi:10.1016/j.jinf.2020.04.002
85. Wu P, Duan F, Luo C, et al. Characteristics of ocular findings of patients with coronavirus disease 2019 (COVID-19) in Hubei Province. China. JAMA Ophthalmol. 2020;138(5):575–578. doi:10.1001/jamaophthalmol.2020.1291
86. Vaibhav K, Braun M, Alverson K, et al. Neutrophil extracellular traps exacerbate neurological deficits after traumatic brain injury. Sci Adv. 2020;6:eaax8847. doi:10.1126/sciadv.aax8847
87. Simonnet A, Chetboun M, Poissy J, et al. High prevalence of obesity in severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) requiring invasive mechanical ventilation. Obesity. 2020;28(7):1195–1199. doi:10.1002/oby.22831
88. Nakeshbandi M, Maini R, Daniel P, et al. The impact of obesity on COVID-19 complications: a retrospective cohort study. Int J Obes. 2020;44(9):1832–1837. doi:10.1038/s41366-020-0648-x
89. Malik VS, Ravindra K, Attri SV, Bhadada SK, Singh M. Higher body mass index is an important risk factor in COVID-19 patients: a systematic review and meta-analysis. Environ Sci Pollut Res Int. 2020;27(33):42115–42123. doi:10.1007/s11356-020-10132-4
90. Apicella M, Campopiano MC, Mantuano M, Mazoni L, Coppelli A, Del Prato S. COVID-19 in people with diabetes: understanding the reasons for worse outcomes. Lancet Diabetes Endocrinol. 2020;8(9):782–792. doi:10.1016/S2213-8587(20)30238-2
91. Delly F, Syed MJ, Lisak RP, Zutshi D. Myasthenic crisis in COVID-19. J Neurol Sci. 2020;414:116888. doi:10.1016/j.jns.2020.116888
92. Barzegar M, Mirmosayyeb O, Nehzat N, et al. COVID-19 infection in a patient with multiple sclerosis treated with fingolimod. Neurol Neuroimmunol Neuroinflamm. 2020;7(4):e753. doi:10.1212/NXI.0000000000000753
93. de Figueiredo CS, Sandre PC, Portugal LCL, et al. COVID-19 pandemic impact on children and adolescents’ mental health: biological, environmental, and social factors. Prog Neuropsychopharmacol Biol Psychiatry. 2022;106:110171. doi:10.1016/j.pnpbp.2020.110171
94. Grolli RE, Mingoti MED, Bertollo AG, et al. Impact of COVID-19 in the mental health in elderly: psychological and biological updates. Mol Neurobiol. 2021;58(5):1905–1916. doi:10.1007/s12035-020-02249-x
95. Aamir A, Awan S, de Filippis R, Diwan MN, Ullah I. Effect of COVID-19 on mental health rehabilitation centers. J Psychosoc Rehabil Ment Health. 2020;21:1–4.
96. Davis HE, Assaf GS, McCorkell L, et al. Characterizing long COVID in an international cohort: 7 months of symptoms and their impact. EClinicalMedicine. 2021;38:101019. doi:10.1016/j.eclinm.2021.101019
97. Ziauddeen N, Gurdasani D, O’Hara ME, et al. Characteristics of Long COVID: findings from a social media survey. medRxiv. 2021. doi:10.1101/2021.03.21.21253968
98. Ayoubkhani D, Khunti K, Nafilyan V, et al. Epidemiology of post-COVID syndrome following hospitalisation with coronavirus: a retrospective cohort study. medRxiv. 2021. doi:10.1101/2021.01.15.21249885
99. Zhao YM, Shang YM, Song WB, et al. Follow-up study of the pulmonary function and related physiological characteristics of COVID-19 survivors three months after recovery. EClinicalMedicine. 2020;25:100463. doi:10.1016/j.eclinm.2020.100463
100. Zhang T, Huang WS, Guan W, et al. Risk factors and predictors associated with the severity of COVID-19 in China: a systematic review, meta-analysis, and meta-regression. J Thorac Dis. 2020;12(12):7429–7441. doi:10.21037/jtd-20-1743
101. Pellinen J, Carroll E, Friedman D, et al. Continuous EEG findings in patients with COVID-19 infection admitted to a New York academic hospital system. Epilepsia. 2020;61(10):2097–2105. doi:10.1111/epi.16667
102. Kremer S, Lersy F, de Sèze J, et al. Brain MRI findings in severe COVID-19: a Retrospective Observational Study. Radiology. 2020;297(2):E242–E251. doi:10.1148/radiol.2020202222
103. Abdel-Mannan O, Eyre M, Löbel U, et al. Neurological and radiographic findings associated with COVID-19 infection in children. JAMA Neurol. 2020;77(11):1440–1445. doi:10.1001/jamaneurol.2020.2687
104. Marshall M. The lasting misery of coronavirus long-haulers. Nature. 2020;585(7825):339–341. doi:10.1038/d41586-020-02598-6
105. Berlit P, Bösel J, Gahn G, Isenmann S, Meuth SG, Nolte CH. “Neurological manifestations of COVID-19”-guideline of the German society of neurology. Neurol Res Pract. 2020;2:51. doi:10.1148/radiol.2020201697
106. Association of British Neurologists Guidance on COVID-19 for people with neurological conditions, their doctors and carers; 2020. Available from: https://cdn.ymaws.com/www.theabn.org/resource/collection/C5F38B64-DC8F-4C67-B6FCF22B2CDB0EE5/ABN_Neurology_COVID-19_Guidance_v6_9.4.20_FP.pdf.
107. Ayres JS. Surviving COVID-19: a disease tolerance perspective. Sci Adv. 2020;6(18):eabc1518. doi:10.1126/sciadv.abc1518
108. McCarville JL, Ayres JS. Disease tolerance: concept and mechanisms. Curr Opin Immunol. 2018;50:88–93. doi:10.1016/j.coi.2017.12.003
109. Zaki MM, Lesha E, Said K, et al. Cell therapy strategies for COVID-19: current approaches and potential applications. Sci Adv. 2021;33:eabg5995. doi:10.1126/sciadv.abg5995
110. Jamshidi E, Babajani A, Soltani P, Niknejad H. Proposed mechanisms of targeting COVID-19 by delivering mesenchymal stem cells and their exosomes to damaged organs. Stem Cell Rev Rep. 2021;17(1):176–192. doi:10.1007/s12015-020-10109-3
111. Spitalieri P, Centofanti F, Murdocca M, et al. Two different therapeutic approaches for SARS-CoV-2 in hiPSCs-derived lung organoids. Cells. 2022;11(7):1235. doi:10.3390/cells11071235
112. Toor SM, Saleh R, Sasidharan Nair V, Taha RZ, Elkord E. T-cell responses and therapies against SARS-CoV-2 infection. Immunology. 2021;162(1):30–43. doi:10.1111/imm.13262
113. Chen D, Huang Y, Shi Z, et al. Demyelinating processes in aging and stroke in the central nervous system and the prospect of treatment strategy. CNS Neurosci Ther. 2020;26(12):1219–1229. doi:10.1111/cns.13497
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
COVID-19 and Saudi Arabia: Awareness, Attitude, and Practice
Fawzy MS, AlSadrah SA
Journal of Multidisciplinary Healthcare 2022, 15:1595-1618
Published Date: 26 July 2022
Comparison of the Diagnostic Performance of a Rapid Antigen Test with Real-Time Polymerase Chain Reaction for Detection of SARS-CoV-2 Among Patients Diagnosed with COVID-19 at Selected Hospitals in Addis Ababa, Ethiopia
Desalegn Z, Sebre S, Yohannes M, Seman A, Shiferaw W, Ademe M, Biazin H, Firdawoke E, Asemamaw Y, Teka B, Teshome S, Amogne W, Addissie A, Gebrehiwot Y, Kantelhardt E, Abebe T
Infection and Drug Resistance 2022, 15:4299-4305
Published Date: 6 August 2022
A Pilot Study of 0.4% Povidone-Iodine Nasal Spray to Eradicate SARS-CoV-2 in the Nasopharynx
Sirijatuphat R, Leelarasamee A, Puangpet T, Thitithanyanont A
Infection and Drug Resistance 2022, 15:7529-7536
Published Date: 21 December 2022
Distinct Features of Vascular Diseases in COVID-19
Ceasovschih A, Sorodoc V, Shor A, Haliga RE, Roth L, Lionte C, Onofrei Aursulesei V, Sirbu O, Culis N, Shapieva A, Tahir Khokhar MA, Statescu C, Sascau RA, Coman AE, Stoica A, Grigorescu ED, Banach M, Thomopoulos C, Sorodoc L
Journal of Inflammation Research 2023, 16:2783-2800
Published Date: 6 July 2023
Re-Emerging COVID-19: Controversy of Its Zoonotic Origin, Risks of Severity of Reinfection and Management
Chala B, Tilaye T, Waktole G
International Journal of General Medicine 2023, 16:4307-4319
Published Date: 20 September 2023