")
Back to Journals » Infection and Drug Resistance » Volume 15
A Pilot Study of 0.4% Povidone-Iodine Nasal Spray to Eradicate SARS-CoV-2 in the Nasopharynx
Authors Sirijatuphat R, Leelarasamee A , Puangpet T, Thitithanyanont A
Received 4 October 2022
Accepted for publication 9 December 2022
Published 21 December 2022 Volume 2022:15 Pages 7529—7536
DOI https://doi.org/10.2147/IDR.S391630
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Rujipas Sirijatuphat,1 Amorn Leelarasamee,1,2 Thanapat Puangpet,3 Arunee Thitithanyanont4
1Department of Medicine, Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand; 2Faculty of Medicine, Siam University, Bangkok, Thailand; 3Samut Sakhon Hospital, Samut Sakhon, Thailand; 4Department of Microbiology, Faculty of Science, Mahidol University, Bangkok, Thailand
Correspondence: Amorn Leelarasamee, Department of Medicine, Faculty of Medicine Siriraj Hospital, Mahidol University, 2 Thanon Wang Lang, Siriraj, Bangkoknoi, Bangkok, 10700, Thailand, Tel/Fax +66 2 419 7783, Email [email protected]
Purpose: This study aimed to evaluate the virucidal efficacy of 0.4% povidone-iodine (PVP-I) nasal spray against SARS-CoV-2 in the patients’ nasopharynx at 3 minutes and 4 hours after PVP-I exposure.
Patients and Methods: The study was an open-label, before and after design, single-arm pilot study of adult patients with RT-PCR-confirmed COVID-19 within 24 hours. All patients received three puffs of 0.4% PVP-I nasal spray in each nostril. Nasopharyngeal (NP) swabs were collected before the PVP-I spray (baseline, left NP samples), and at 3 minutes (left and right NP samples) and 4 hours post-PVP-I spray (right NP samples). All swabs were coded to blind assessors and transported to diagnostic laboratory and tested by RT-PCR and cultured to measure the viable SARS-CoV-2 within 24 hours after collection.
Results: Fourteen patients were enrolled but viable SARS-CoV-2 was cultured from 12 patients (85.7%). The median viral titer at baseline was 3.5 log TCID50/mL (IQR 2.8– 4.0 log TCID50/mL). At 3 minutes post-PVP-I spray via the left nostril, viral titers were reduced in 8 patients (66.7%). At 3 minutes post-PVP-I, the median viral titer was 3.4 log TCID50/mL (IQR 1.8– 4.4 log TCID50/mL) (P=0.162). At 4 hours post-PVP-I spray via the right nostril, 6 of 11 patients (54.5%) had either the same or minimal change in viral titers. The median viral titer 3 minutes post-PVP-I spray was 2.7 log TCID50/mL (IQR 2.0– 3.9 log TCID50/mL). Four hours post-PVP-I spray the median titer was 2.8 log TCID50/mL (IQR 2.2– 3.9 log TCID50/mL) (P=0.704). No adverse effects of 0.4% PVP-I nasal spray were detected.
Conclusion: The 0.4% PVP-I nasal spray demonstrated minimal virucidal efficacy at 3 minutes post-exposure. At 4 hours post-exposure, the viral titer was considerably unchanged from baseline in 10 cases. The 0.4% PVP-I nasal spray showed poor virucidal activity and is unlikely to reduce transmission of SARS-CoV-2 in prophylaxis use.
Keywords: povidone iodine, COVID-19, SARS-CoV-2, viral eradication, viral culture, nasopharyngeal swab
Introduction
Coronavirus disease 2019 (COVID-19) is an acute viral respiratory infection caused by the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2) that emerged in December 2019 causing a pandemic that has killed millions.1 The SARS-CoV-2 can persist in the upper respiratory tract of the patients at least seven days and spreads mainly via droplet and airborne transmission.2 Patients are infectious for two to three days before the onset of symptoms and are most contagious one to two days before the patients feel sick.3
Povidone iodine (PVP-I) possesses rapid in-vitro virucidal activity against SARS-CoV-2.4–7 It can reduce SARS-CoV-2 titers by approximately 100-fold within 30 seconds after 0.45–10% PVP-I exposure.5 It is a broad-spectrum antiseptic and used for topical application in skin solutions and throat sprays.8–10 PVP-I has a good safety profile and is available in Thailand. The 0.4% PVP-I nasal spray is prepared and use to spray aerosols into nasal cavities and nasopharynx. The aerosols containing PVP-I will lay down easily on the mucosa in the turbinate and nasopharynx and exert PVP-I virucidal activity onsite. Nasal spray used by ordinary people is easy and more convenient than nasopharynx irrigation which needs to adjust head position and the patients has to hold breathing while performing irrigation to avoid suffocation.
Many researchers and clinicians hypothesized that a nasal spray of PVP-I would decrease viable virus titers in the upper airway. One practice guideline advises the use of 0.4% PVP-I nasal application and 0.5% oropharyngeal application to reduce the risk of COVID-19 transmission.11 However, evidence of in vivo efficacy against SARS-CoV-2 in humans is very limited. Two previous studies reported that 0.5–1% PVP-I has virucidal efficacy against SARS-CoV-2 in the oral cavity of COVID-19 patients,12,13 while other studies have not demonstrated a virucidal effect of 1–2% PVP-I in humans.14–16
Therefore, the aim of this study was to measure the speed of virucidal activity at three minutes and the sustainability of virucidal action at four hours after administration of a 0.4% PVP-I nasal spray in the patients with laboratory-confirmed COVID-19 infection. If the virucidal effect of PVP-I was rapid and at least 10-fold reduction from baseline was demonstrated in the patients’ nasopharynx, it would be beneficial to public and healthcare professionals since PVP-I nasal spray would become a simple and cost-effective measure for preventing cross-contamination and community transmission of SARS-CoV-2.
Materials and Methods
This was an open-label, before and after study design, single-arm pilot study conducted from February 15, 2021, to March 15, 2021, at Siriraj Hospital and Samut Sakhon Hospital in Thailand and the patients were followed up for 24 hours in the hospital. The study protocol was approved by the Siriraj Institutional Review Board, Mahidol University, Thailand (COA. 408/2020), and by the Ethic Committees of Samut Sakhon Hospital (SKH REC 10/2564/V.1). Written informed consent was obtained from all study participants. This study has been registered at Thai Clinical Trials Registry under registration id. TCTR20210125002. The authors confirmed that all ongoing trials for PVP-I were registered before the patient enrollment.
Eligible patients were adults aged 18–60 years with asymptomatic or mild disease due to SARS-CoV-2 with a cycle threshold (Ct) value less than 25 of either the N gene or ORF1ab by reverse transcriptase polymerase chain reaction (RT-PCR) in the 24 hours before study enrollment. Patients with an iodine allergy or thyroid disease, pregnant or lactating women, and patients who had received antiviral agents (ie, remdesivir and favipiravir) were excluded.
The 0.4% PVP-I was made by mixing 10% PVP-I solution with normal saline in 1:30 ratio and used as nasal spray. The following intervention was performed sequentially in all patients; 1) specimen collection by nasopharyngeal (NP) swab via the left nostril (pre-exposure specimen), 2) administration of 0.4% PVP-I nasal spray via the left and right nostrils, 3) wait 3 minutes and collect NP swab specimens through the left and right nostrils, 4) wait 4 hours and collect an NP swab specimen through the right nostril, 5) all participants were hospitalized to observe symptoms and side effects for at least 24 hours after the PVP-I nasal spray. All NP specimens were assigned numbers to blind laboratory technicians and kept in viral transport media (VTM) at 4 °C and sent to the microbiology laboratory for testing by RT-PCR and viral culture within 24 hours.
The rapidity of 0.4% PVP-I antiviral activity was demonstrated by comparing the numbers of viral titer in the left side of nasopharynx (pre-exposure specimen) before and at 3 minutes after PVP-I exposure. The comparison between the average viral titer in the left side of nasopharynx (pre-exposure specimens) and that of the right side of nasopharynx at 3 minutes after PVP-I exposure was performed to provide an additional information of virucidal speed assuming that the viral titers of the left and right sides of nasopharynx were equal before the PVP-I exposure. The sustainability of antiviral activity was evaluated by comparing the viral titers in the right side of nasopharynx at 3-minutes and 4-hours after PVP-I exposure.
RNA was extracted from 200 μL of viral transport media from the NP swab samples using MagDEA® Dx kit (Precision System Science, Chiba, Japan), and SARS-CoV-2 RT-PCR was performed by amplification of SARS-CoV-2 N and ORF1ab fragments using the Detection Kit for 2019 Novel Coronavirus (2019-nCoV) RNA (PCR-Fluorescence Probing) (Da An Gene Co., Ltd. of Sun Yat-sen University, Guangdong, China), with a cycle threshold ≤40 considered positive.17 For the viral culture test, titers were determined as the 50% tissue culture infectious dose (TCID50) of the virus. Vero E6 cells expressing the type II transmembrane serine protease (Vero-TMPRSS2)18 were seeded into 96-well plates and incubated with a serial dilution of the nasopharyngeal specimen. Cytopathic effects were evaluated daily until a 7-day incubation was completed.
Assuming that 70% of the pairs switch from the initial values of viable SARS-CoV-2 counts in cell culture to less than 10 fold after 3 minute of PVP-I nasal exposure and 0% from the initial value to higher viable viral count after 3 minutes of PVP-I nasal exposure, and after applying continuity correction, the pilot study would require a sample size of 10 pairs to achieve a power of 80% and a two-sided significance of 5% for detecting a difference of −0.70 between the discordant proportions.19
Statistical Analysis
Demographic data were described with descriptive statistics. Quantitative data were described with mean ± standard deviation, or median and interquartile range. Qualitative data were described in frequency (percent). The median of Ct value and viral titers were compared at each time point using the Wilcoxon signed-rank test and Mann–Whitney U-test. A p-value of <0.05 was considered statistically significant.
The study complies with the World Medical Association (WMA) Declaration of Helsinki.
Results
Fourteen patients were enrolled, and viable culture was obtained from 12 patients (85.7%) (Figure 1). Six patients were male (50%) with a median age 34.0 years (interquartile range (IQR) 27.5–45.0 years). Nine patients had mild disease and three patients had asymptomatic infection. The median duration from symptom onset to study enrollment was 3.0 days (IQR 1.5–4 days) (Table 1). No adverse events from PVP-I administration were observed during hospitalization.
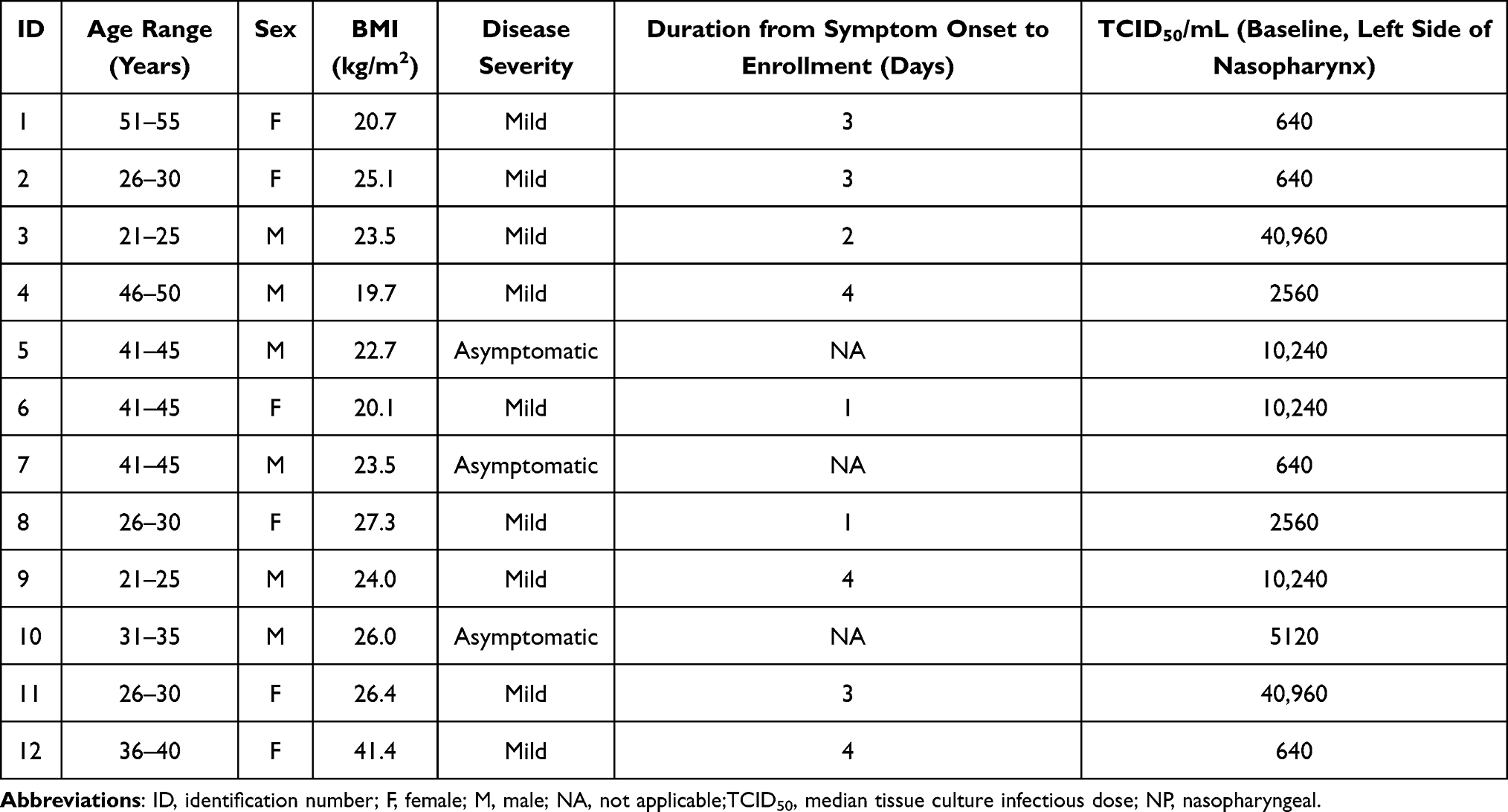 |
Table 1 Demographic Data of 12 Patients with Culturable NP Samples |
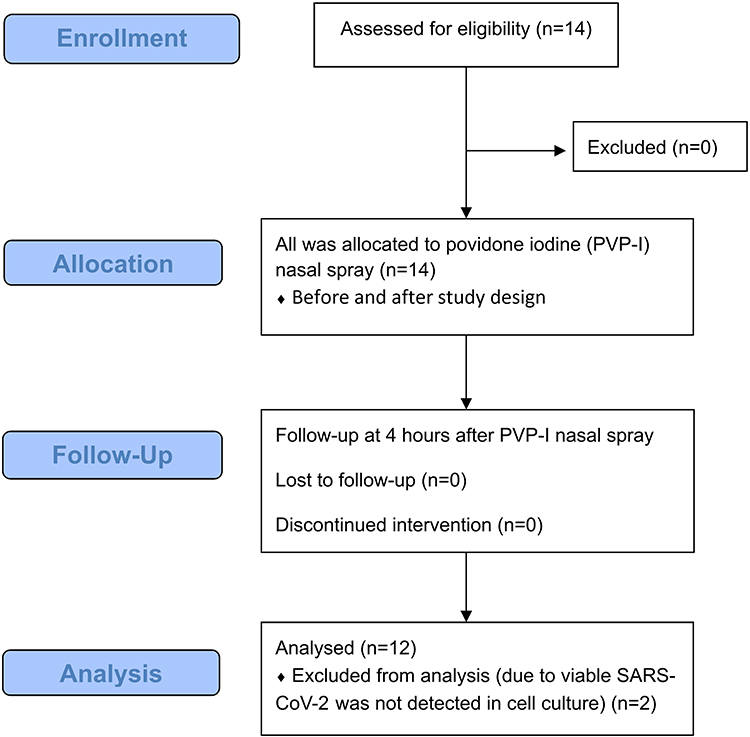 |
Figure 1 CONSORT flow diagram of the pilot study. Note: Adapted from Schulz KF, Altman DG, Moher D, for the CONSORT Group. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. PLoS Med. 2010;7(3): e1000251. Copyright: © 2010 Schulz et al. Creative Commons Attribution License.20 |
At 3 minutes post-PVP-I nasal spray, eight of the 12 patients (66.7%) had a reduction of viral titers. The median viral titer at baseline was 3.5 log TCID50/mL (IQR 2.8–4.0 log TCID50/mL), and the median viral titer at 3 minutes post-PVP-I exposure was 3.4 log TCID50/mL (IQR 1.8–4.4 log TCID50/mL) (P=0.162) (Tables 2 and 3). A median value of 0.1 log reduction of viable viruses (IQR −0.05–0.23 log reduction) and 75.0% virus reduction (IQR −225.0–93.8%) were found. The median baseline Ct value of the N gene was 19.84 (IQR 17.77–21.52), whereas the median Ct value of the N gene at 3 minutes post-PVP-I was 19.49 (IQR 16.95–23.10) (P=0.569). The median baseline Ct value of the ORF1ab gene was 19.84 (IQR 16.82–22.22), and the median Ct value of the ORF1ab gene at 3 minutes post-PVP-I was 19.17 (IQR 15.81–24.87) (P=0.469).
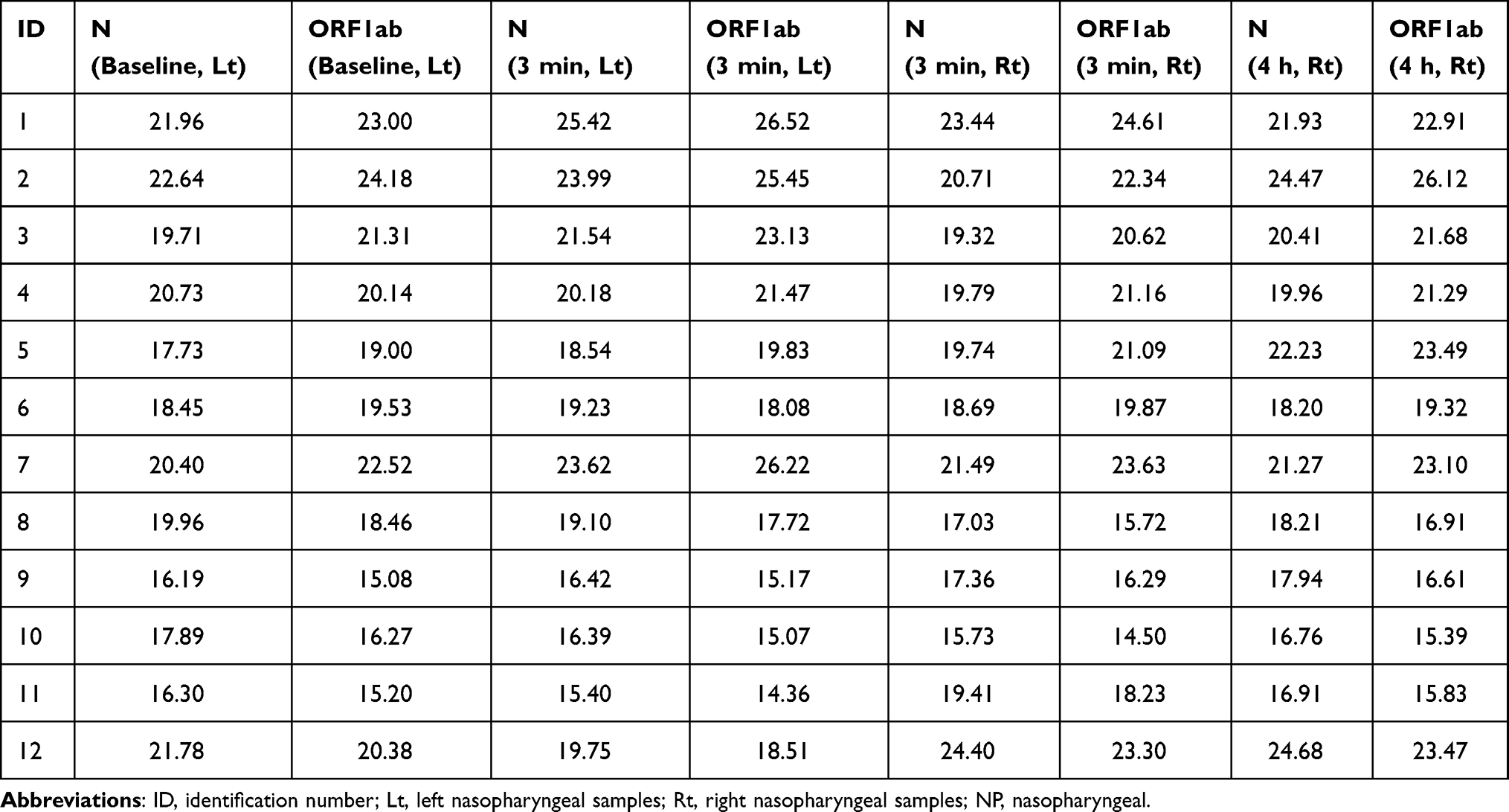 |
Table 2 Cycle Threshold (Ct) Values for Culturable NP Samples |
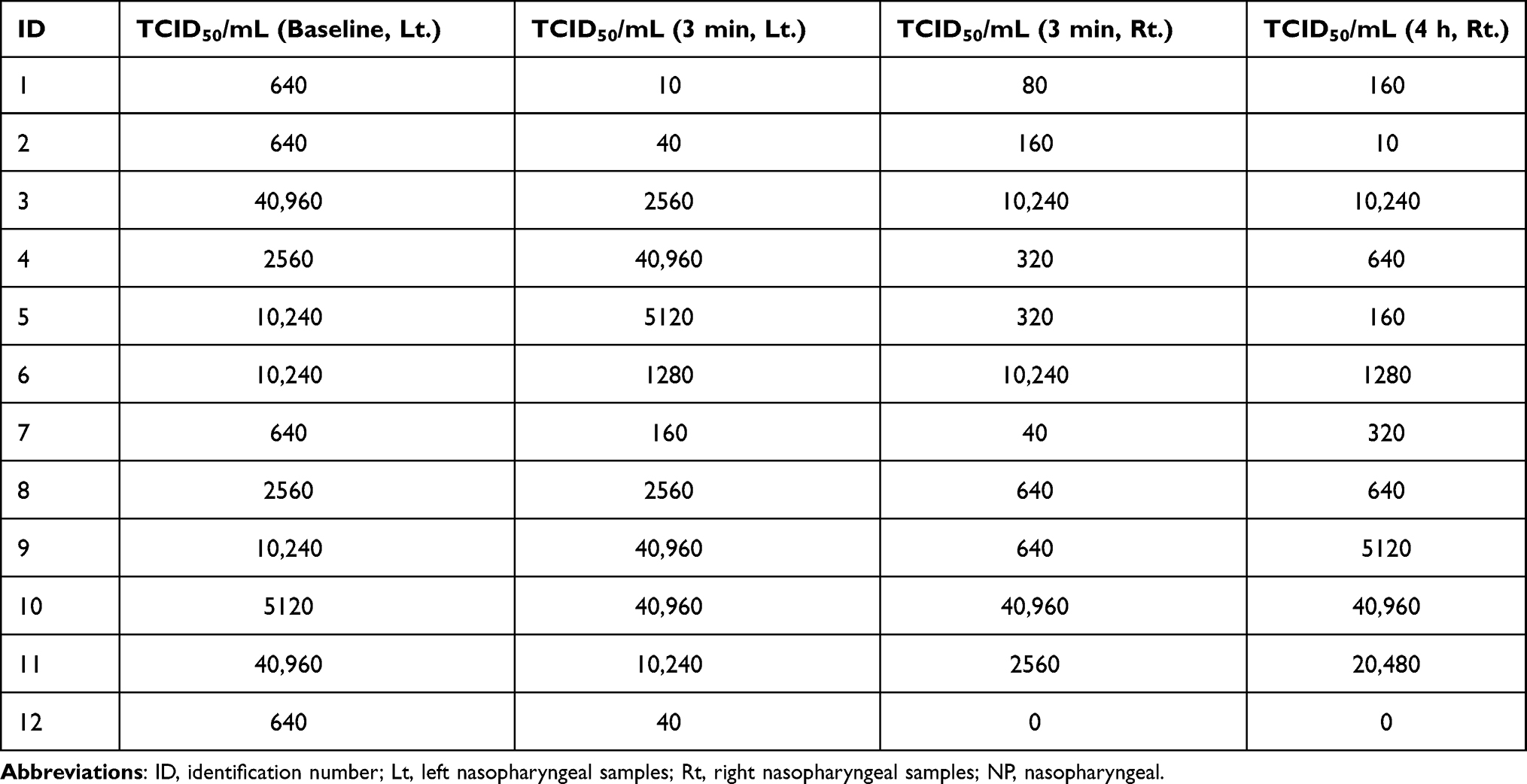 |
Table 3 Viral Titers for Culturable NP Samples |
The median viral titers of the left and right NP specimens at 3 minutes post-PVP-I exposure were 3.4 log TCID50/mL (IQR 1.8–4.4 log TCID50/mL) and 2.7 log TCID50/mL (IQR 2.0–3.9 log TCID50/mL), respectively (P=0.433). The median Ct value of the N gene of the left and right-side NP specimens at 3 minutes post-PVP-I were 19.49 (IQR 16.95–23.10) and 19.58 (IQR 17.69–21.30), respectively (P=0.977). The median Ct value of the ORF1ab gene of the left and right-side NP specimens at 3 minutes post-PVP-I were 19.17 (IQR 15.81–24.87) and 20.86 (IQR 16.78–23.06), respectively (P=0.885).
At 4 hours post-PVP-I nasal spray, six of the 11 patients (54.5%) were observed to have either the same titer or a minimal reduction of viral titers, and five patients had increased titers from the samples collected at 3 minutes post-PVP-I. The median viral titer at 3 minutes post-PVP-I exposure was 2.7 log TCID50/mL (IQR 2.0–3.9 log TCID50/mL), and the median viral titer at 4 hours post-PVP-I exposure was 2.8 log TCID50/mL (IQR 2.2–3.9 log TCID50/mL) (P=0.704). The median Ct value of the N gene at 3 minutes post-PVP-I exposure was 19.58 (IQR 17.69–21.30), and the median Ct value of the N gene at 4 hours post-PVP-I exposure was 20.19 (IQR 18.01–22.16) (P=0.339). The median Ct value of the ORF1ab gene at 3 minutes post-PVP-I exposure was 20.86 (IQR 16.78–23.06), and the median Ct value of the ORF1ab gene at 4 hours post-PVP-I was 21.49 (IQR 16.69–23.38) (P=0.433).
Only one case (no. 12) showed viral titers decreased approximately ten folds. The rest showed only within 1–4 fold reduction which could be due to sampling variation or weak PVP-I anti-viral activity. Five cases even had increased viral titers after PVP-I exposure (Table 4). Overall, the decrease of viral titers is not rapid and not as much as shown by the in vitro test which is about at least 100-fold decrease in 30 seconds contact time after PVP-I exposure.5 At 4 hours after PVP-I exposure, minimal or no change in viral titer was demonstrated. Compare to the baseline value of viral culture obtained from left nasopharynx of each individual, seven specimens showed about tenfold reduction of viral titer, 22 specimens revealed within 4 folds reduction and 7 specimens showed no change or even increase in viral titer. Overall, the PVP-I did not demonstrate the rapid and strong virucidal activity as has been shown by the in vitro test. Raw data of clinical setting and viral culture at baseline; 3 min, Lt.; 3 min, Rt.; and 4 h, Rt. were available in the attached file (391,630-raw-data-from-clinical-trial-pvp-i.xlsx). Individual deidentified participant data on demographic data, clinical symptoms, viral cultures before and after PVP-I exposure or other study documents are available from the publisher or from the first author for one year after publication through the following e-mail address. (e-mail address: [email protected]; [email protected]).
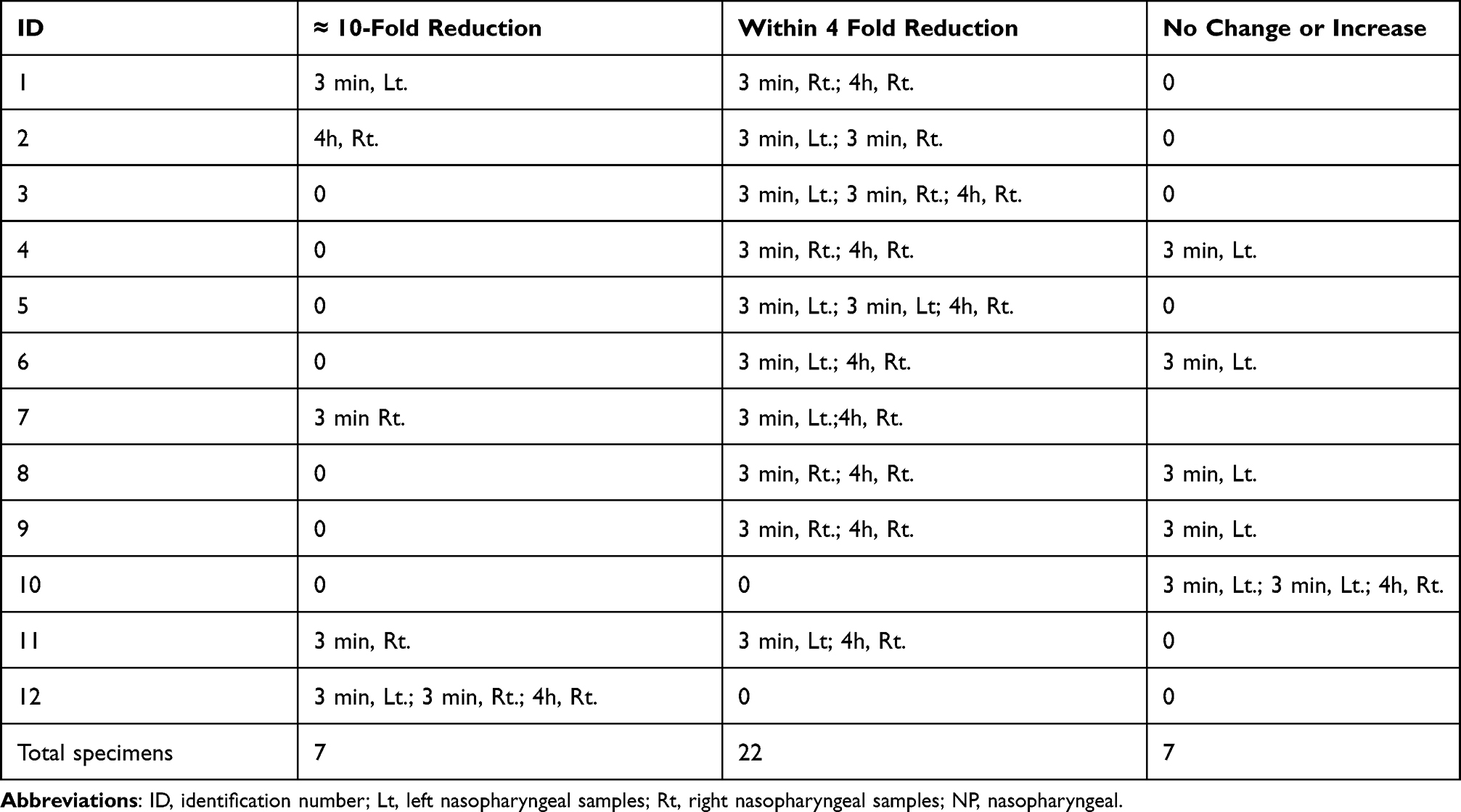 |
Table 4 Change in Viral Titers After 3 Minutes and 4 Hours Exposure to PVP-I as Compared to the Baseline Value from Left NP Specimens |
Discussion
The TCID50/mL of the 12 patients with culturable NP samples varied from 640 to 40,960, which was not related to either disease severity or the onset of clinical symptoms when NP swabs were taken. Because all cases recovered uneventfully, the initial values of TCID50/mL did not predict the treatment outcome. However, the sample size was small and this study was not designed for evaluating the relationship between the initial viral titers and disease severity or clinical outcome.
A median one-fold reduction of SARS-CoV-2 viral titer from nasopharyngeal swabs at 3 minutes post-PVP-I exposure in the left side of nasopharynx was observed. This was in marked contrast to in vitro studies that reported as much as a 100-fold reduction in viral titer.5 At 4 hours post-exposure to 0.4% PVP-I nasal spray, the viral titer in the right side of nasopharynx was unchanged from baseline in 10 cases.
Although the in vitro rapid activity of PVP-I against SARS-CoV-2 has been established in several studies,5–7 evidence of in vivo activity in humans is limited. Two studies have reported that PVP-I administration into the upper aerodigestive tract of COVID-19 patients was associated with lower SARS-CoV-2 viral load and Ct values.12,13 However, other studies have not confirmed their results.14–16 To measure potential reductions in viral shedding, the RT-PCR alone is insufficient and viral culture is needed. Using viral culture, PVP-I administration probably reduced infectious viral titers in the upper respiratory tract of COVID-19 patients in two recent studies.21,22 Friedland et al demonstrated that 0.5% PVP-I nasal spray was associated with a reduction of viral titers in five of the six study participants (83%) five minutes after PVP-I application.21 Seikai et al revealed that gargling with PVP-I was associated with significantly decreased viral titers at 60 minutes after PVP-I exposure.22
This present study demonstrated that PVP-I nasal spray had poor in vivo efficacy in this study. This could be explained by several factors including insufficient concentration, improper formulation and/or amount of PVP-I, inadequate duration of exposure, inappropriate method of administration, and mucociliary clearance of PVP-I from the nasal cavity.21 As aforementioned, 0.45–10% PVP-I exposure showed the good in vitro virucidal activity against SARS-CoV-2,5 however, in previous human studies, the concentrations of PVP-I applications were ranged from 0.5% to 2%12–16 and the studies that used higher concentrations (1% or 2%) of PVP-I did not demonstrate the virucidal efficacy of SARS-CoV-2 in COVID-19 patients. The 0.4% PVP-I that used in this study was based on the recommendations from the clinical practice guidelines,11 and this concentration may not be adequate for SARS-CoV-2 eradication in nasal pathways of humans. Moreover, the PVP-I in this study was applied by nasal spray without clear penetration of the patient’s nasopharynx and the NP swabs were collected for determining the viral titers by culture method, therefore, inadequate PVP-I exposure at the nasopharynx may be occurred.
Our study also revealed that 0.4% PVP-I nasal spray did not change the Ct value of the N and ORF1ab segments and did not interfere with PCR-mediated laboratory diagnosis of COVID-19. Finally, 0.4% PVP-I administered as a nasal spray was safe and well-tolerated.
This present study had some limitations. First, this was a small, single-arm, pre- and post-exposure pilot study, therefore, the study result may differ from larger-scale studies. Second, the study participants were likely infected with the strain B.1.36.16 of SARS-CoV-2 that caused infections in Thailand during the study period.23 Our findings may not be generalizable to other variants of SARS-CoV-2.
However, since the PVP-I has been shown to exhibit broad-spectrum, rapid virucidal activity against various respiratory viruses by the in vitro tests, the finding of our study in patients infected with SARS-CoV-2 should give warning against its use for prophylaxis in ordinary people.
Conclusion
The 0.4% PVP-I nasal spray had minimal virucidal activity in the nasopharynx of infected patients. Hence, it is unlikely that this treatment would reduce airborne or droplet transmission of COVID-19. Other preventive measures such as vaccination, face masking, and personal protective equipment should be emphasized to limit COVID-19 transmission.
Ethical Approval
This study was approved by the Institutional Review Board of the Faculty of Medicine Siriraj Hospital, Mahidol University (COA. 408/2020), and by the ethic committees of Samut Sakhon Hospital (SKH REC 10/2564/V.1).
Acknowledgments
The authors gratefully acknowledge Mrs Sukanya Chanboonchuay for her assistance with project management, Dr Paraya Assanasen (ENT physician) for making the 0.4% PVP-I nasal spray, Miss Suwimon Manopwisedjaroen, M.Sc. and Miss Chanya Srisaowakarn, M.Sc. for microbiological laboratory assistance. The authors also thank the COVID-19 patient care team of Samut Sakhon Hospital (Mr Chaiyot Ra-ngubpai, Miss Punyanee Triamkan, Miss Laksamee Suddee, Miss Kitima Limprasert and Mrs Walaiporn Jaiaree) for providing patient information, specimen collection, and patient observation during hospitalization.
Funding
This work was supported by the Health Systems Research Institute (Thailand), Nonthaburi, Thailand; and, by the Faculty of Medicine Siriraj Hospital, Mahidol University, Bangkok, Thailand. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors declared that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Wang H, Paulson KR, Pease SA; COVID-19 Excess Mortality Collaborators. Estimating excess mortality due to the COVID-19 pandemic: a systematic analysis of COVID-19-related mortality, 2020–21. Lancet. 2022;399(10334):1513–1536. doi:10.1016/S0140-6736(21)02796-3
2. Badu K, Oyebola K, Zahouli JZB, et al. SARS-CoV-2 viral shedding and transmission dynamics: implications of WHO COVID-19 discharge guidelines. Front Med. 2021;8:648660. doi:10.3389/fmed.2021.648660
3. Casey-Bryars M, Griffin J, McAloon C, et al. Presymptomatic transmission of SARS-CoV-2 infection: a secondary analysis using published data. BMJ Open. 2021;11:e041240. doi:10.1136/bmjopen-2020-041240
4. Pelletier JS, Miller D, Liang B, Capriotti JA. In vitro efficacy of a povidone-iodine 0.4% and dexamethasone 0.1% suspension against ocular pathogens. J Cataract Refract Surg. 2011;37:763–766. doi:10.1016/j.jcrs.2010.11.028
5. Anderson DE, Sivalingam V, Kang AEZ, et al. Povidone-iodine demonstrates rapid in vitro virucidal activity against SARS-CoV-2, the virus causing COVID-19 disease. Infect Dis Ther. 2020;9:669–675. doi:10.1007/s40121-020-00316-3
6. Bidra AS, Pelletier JS, Westover JB, Frank S, Brown SM, Tessema B. Rapid in-vitro inactivation of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) using povidone-iodine oral antiseptic rinse. J Prosthodont. 2020;29(6):529–533. doi:10.1111/jopr.13209
7. Shet M, Hong R, Igo D, Cataldo M, Bhaskar S. In vitro evaluation of the virucidal activity of different povidone-iodine formulations against murine and human coronaviruses. Infect Dis Ther. 2021;10:2777–2790. doi:10.1007/s40121-021-00536-1
8. Nagatake T, Ahmed K, Oishi K. Prevention of respiratory infections by povidone-iodine gargle. Dermatology. 2002;204(Suppl 1):32–36. doi:10.1159/000057722
9. Ghaddara HA, Kumar JA, Cadnum JL, Ng-Wong YK, Donskey CJ. Efficacy of a povidone iodine preparation in reducing nasal methicillin-resistant Staphylococcus aureus in colonized patients. Am J Infect Control. 2020;48:456–459. doi:10.1016/j.ajic.2019.09.014
10. Peng HM, Wang LC, Zhai JL, Weng XS, Feng B, Wang W. Effectiveness of preoperative decolonization with nasal povidone iodine in Chinese patients undergoing elective orthopedic surgery: a prospective cross-sectional study. Braz J Med Biol Res. 2017;51:e6736. doi:10.1590/1414-431x20176736
11. Krajewska Wojciechowska J, Krajewski W, Zub K, Zatoński T. Review of practical recommendations for otolaryngologists and head and neck surgeons during the COVID-19 pandemic. Auris Nasus Larynx. 2020;47:544–558. doi:10.1016/j.anl.2020.05.022
12. Seneviratne CJ, Balan P, Ko KKK, et al. Efficacy of commercial mouth-rinses on SARS-CoV-2 viral load in saliva: randomized control trial in Singapore. Infection. 2021;49:305–311. doi:10.1007/s15010-020-01563-9
13. Elzein R, Abdel-Sater F, Fakhreddine S, et al. In vivo evaluation of the virucidal efficacy of Chlorhexidine and Povidone-iodine mouthwashes against salivary SARS-CoV-2. A randomized-controlled clinical trial. J Evid Based Dent Pract. 2021;21:101584. doi:10.1016/j.jebdp.2021.101584
14. Guenezan J, Garcia M, Strasters D, et al. Povidone iodine mouthwash, gargle, and nasal spray to reduce nasopharyngeal viral load in patients with COVID-19: a randomized clinical trial. JAMA Otolaryngol Head Neck Surg. 2021;147:400–401. doi:10.1001/jamaoto.2020.5490
15. Zarabanda D, Vukkadala N, Phillips KM, et al. The effect of povidone-iodine nasal spray on nasopharyngeal SARS-CoV-2 viral load: a randomized control trial. Laryngoscope. 2021;132:2089–2095. doi:10.1002/lary.29935
16. Ferrer MD, Barrueco ÁS, Martinez-Beneyto Y, et al. Clinical evaluation of antiseptic mouth rinses to reduce salivary load of SARS-CoV-2. Sci Rep. 2021;11:24392. doi:10.1038/s41598-021-03461-y
17. Wang H, Tan W, Tan W, Tan W. Summary of the detection kits for SARS-CoV-2 approved by the national medical products administration of China and their application for diagnosis of COVID-19. Virol Sin. 2020;35:699–712. doi:10.1007/s12250-020-00331-1
18. Sasaki M, Uemura K, Sato A, et al. SARS-CoV-2 variants with mutations at the S1/S2 cleavage site are generated in vitro during propagation in TMPRSS2-deficient cells. PLoS Pathog. 2021;17:e1009233. doi:10.1371/journal.ppat.1009233
19. Dhand NK, Khatkar MS. Statulator: an online statistical calculator. sample size calculator for comparing two paired proportions. Available from: http://statulator.com/SampleSize/ss2PP.html.
20. Schulz KF, Altman DG, Moher D, for the CONSORT Group. CONSORT 2010 Statement: Updated Guidelines for Reporting Parallel Group Randomised Trials. PLoS Med. 2010;7(3): e1000251. Copyright: © 2010 Schulz et al. Creative Commons Attribution License.
21. Friedland P, Tucker S, Goodall S, et al. In vivo (human) and in vitro inactivation of SARS-CoV-2 with 0.5% povidone-iodine nasal spray. Aust J Otolaryngol. 2022;5:2. doi:10.21037/ajo-21-40
22. Seikai T, Takada A, Hasebe A, et al. Gargling with povidone iodine has a short-term inhibitory effect on SARS-CoV-2 in patients with COVID-19. J Hosp Infect. 2022;123:179–181. doi:10.1016/j.jhin.2022.01.001
23. Kunno J, Supawattanabodee B, Sumanasrethakul C, Wiriyasivaj B, Kuratong S, Kaewchandee C. Comparison of different waves during the COVID-19 pandemic: retrospective descriptive study in Thailand. Adv Prev Med. 2021;2021:5807056. doi:10.1155/2021/5807056
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.