Back to Journals » Infection and Drug Resistance » Volume 15
Comparison of the Diagnostic Performance of a Rapid Antigen Test with Real-Time Polymerase Chain Reaction for Detection of SARS-CoV-2 Among Patients Diagnosed with COVID-19 at Selected Hospitals in Addis Ababa, Ethiopia
Authors Desalegn Z, Sebre S ![]() , Yohannes M
, Yohannes M ![]() , Seman A
, Seman A ![]() , Shiferaw W, Ademe M
, Shiferaw W, Ademe M ![]() , Biazin H
, Biazin H ![]() , Firdawoke E, Asemamaw Y
, Firdawoke E, Asemamaw Y ![]() , Teka B
, Teka B ![]() , Teshome S
, Teshome S ![]() , Amogne W
, Amogne W ![]() , Addissie A, Gebrehiwot Y, Kantelhardt E
, Addissie A, Gebrehiwot Y, Kantelhardt E ![]() , Abebe T
, Abebe T ![]()
Received 15 January 2022
Accepted for publication 2 July 2022
Published 6 August 2022 Volume 2022:15 Pages 4299—4305
DOI https://doi.org/10.2147/IDR.S353844
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Zelalem Desalegn,1,* Shemse Sebre,1,* Meron Yohannes,2 Aminu Seman,1 Welelta Shiferaw,3 Muluneh Ademe,1 Habtamu Biazin,1 Ededia Firdawoke,1 Yehenew Asemamaw,1 Brhanu Teka,1 Seifegebriel Teshome,1 Wondwossen Amogne,4 Adamu Addissie,5,6 Yirgu Gebrehiwot,7 Eva Kantelhardt,6 Tamrat Abebe1
1Department of Microbiology, Immunology and Parasitology, School of Medicine, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 2Department of Medical Laboratory Sciences, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 3Department of Psychiatry, School of Medicine, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 4Department of Internal Medicine, College of Health Sciences, School of Medicine, Addis Ababa University, Addis Ababa, Ethiopia; 5School of Public Health, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 6Institute of Medical Epidemiology, Biostatistics and Informatics, Martin-Luther-University, Halle, Germany; 7Department of Obstetrics and Gynecology, College of Health Sciences, School of Medicine, Addis Ababa University, Addis Ababa, Ethiopia
*These authors contributed equally to this work
Correspondence: Zelalem Desalegn, Department of Microbiology, Immunology and Parasitology, College of Health Sciences, Addis Ababa University, P.O. Box: 9086, Addis Ababa, Ethiopia, Email [email protected]; [email protected]
Background: When faced with a public health problem such as the COVID-19 pandemic, devising a test with an accurate and rapid diagnostic capacity is critical to contain the disease. We compared the diagnostic performance of a rapid antigen test in comparison with a reference method, namely a real-time polymerase chain reaction (RT-PCR) assay.
Methods: We enrolled patients with confirmed COVID-19 from two selected hospital in Addis Ababa, Ethiopia, between January and November 2021. We assessed the performance of the Standard Q COVID-19 Ag Kit (SD Biosensor, Republic of Korea) in 200 nasopharyngeal and nasal swab samples.
Results: Out of the 200 samples utilized for the diagnostic performance evaluation, equal proportion of the samples were confirmed positive and negative for SARS-CoV-2 based on RT-PCR. Of the 100 confirmed positive cases, 95 showed positive results with the rapid antigen test, yielding a sensitivity of 95% (95% confidence interval [CI] 88.7– 98.4%). Of the 100 confirmed negative cases, there were three false-positive results, yielding a specificity of 97% (95% CI 91.5– 99.4%). The sensitivity of the rapid antigen test was higher for samples with an RT-PCR cycle threshold (Ct) value ≤ 25 compared with samples with a higher Ct value.
Conclusion: The finding demonstrated that the detection capacity of the Standard Q COVID-19 Ag Test meets the requirements set by the Ministry of Health Ethiopia. The high sensitivity and specificity of the test device indicate the possibility of using it for diagnostic and clinical purposes in resource-constrained settings such as Ethiopia.
Keywords: SARS-CoV-2, COVID-19, antigen test
Introduction
The world has been struggling with COVID-19 since it was declared a pandemic by the World Health Organization (WHO) in March 2020.1,2 With such a public health challenge, alternative diagnostic options are critical to monitor active cases, coupled with contact tracing modalities. With this effort, it should be possible to reduce the transmission of the virus (SARS-CoV-2).3,4 So far, there have been extensive efforts to develop various diagnostic tests.1 Although there are many possible options, viral RNA–based tools including real-time polymerase chain reaction (RT-PCR) are considered to be the reference method for COVID-19 diagnosis.2,4
There are some limitations to RT-PCR including cost, a relatively long turnaround time and the required equipment for testing.3,5,6 Consequently, there is a demand for alternative testing methods to halt transmission of the virus quite rapidly, which would provide relief for the health system and patients.5 Accumulated evidence has shown that rapid antigen tests, a type of rapid diagnostic test based on lateral immunochromatography, could be used for point-of-care detection of SARS-CoV-2 antigens.3 Considering the limitations of RT-PCR, a number of companies have developed point-of-care rapid antigen tests.5,7,8 Indeed, a number of helpful rapid antigen tests are currently available for clinical practice.2,3 Among these, the Standard Q COVID-19 Ag Test (SD Biosensor, Inc., Suwon, Korea) applies the principle of a lateral flow assay in a cassette-based format with a visual read-out.9 A previous study indicated that the test had higher sensitivity and specificity compared with other rapid antigen tests.10 Nevertheless, it is critical to evaluate this rapid antigen test for screening of SARS-CoV-2-infected individuals before employing it in a resource-limited context, such as Ethiopia.8
To our knowledge, there has been no research focussing on the evaluation of antigen test performance in the Ethiopian setting. In the present study, we evaluated the performance of the Standard Q COVID-19 Ag Test for the detection of SARS-CoV-2 compared with RT-PCR in patients confirmed SARS-CoV-2 positive and negative at selected hospitals in Addis Ababa, Ethiopia.
Materials and Methods
Study Design, Setting and Participants
We employed a cross-sectional study design to evaluate the diagnostic performance of the Standard Q Antigen Test. We included SARS-CoV-2-confirmed patients from Tikur Anbessa Specialized Hospital and Eka Kotebe General Hospital from January to November 2021. We selected these hospitals based on the availability of COVID-19 diagnostic facilities. Following the emergence of the COVID-19 pandemic, Eka Kotebe, located in Addis Ababa, Ethiopia’s capital, was designated as the first COVID-19 treatment centre in Ethiopia. The hospital was a pioneer in the management of COVID-19 cases could admit 600 cases. During the early phase of the COVID-19 pandemic, the institution had served as the only centre for isolation, care and support of all Ethiopian and non-Ethiopian citizens in the country.11 To evaluate the analytical sensitivity of the intended test, we included confirmed SARS-CoV-2-positive adult patients who were willing to participate in the study and provided their consent to participate. We excluded critically ill patients from the study.
Recruitment of Cases
Nasopharyngeal and nasal samples were collected from patients who were seeking other health services but were required to be screened for SARS-CoV-2 as per the hospital protocol/guideline. SARS-CoV-2 RT-PCR-based analysis was carried out; we used samples with a negative test result by the PCR as the negative controls. As mentioned above, the confirmed SARS-CoV-2 cases were drawn from Tikur Anbessa Specialized Hospital and Eka Kotebe General Hospital. For comparison, we tested samples from the same patients with the Standard Q COVID-19 Ag Test.
Sample Collection, Handling and Transportation
The 200 samples comprised 100 RT-PCR-confirmed SARS-CoV-2-positive cases and 100 RT-PCR-confirmed SARS-CoV-2-negative samples. We collected demographic characteristics of the participants from electronic software. Trained medical laboratory medical technologists collected and handled the samples. They collected two nasopharyngeal samples and one nasal sample from each patient. They placed the first portion of the standard flocked swab into viral transport media (VTM) and transferred it to the Department of Microbiology, Immunology and Parasitology Molecular Biology Laboratory, where technicians performed molecular analysis to detect SARS-CoV-2 as per the established protocol.1,10 They utilised the remaining nasopharyngeal and nasal samples for the Standard Q COVID-19 Ag Test. The details are presented in the following subsections.
Laboratory Tests
The Standard Q COVID-19 Ag Test is a rapid chromatographic immunoassay targeting SARS-CoV-2 nucleocapsid (N) antigen from respiratory specimens.6,9 The test device has a window with two pre-coated lines, namely the control (C) and test (T) bands. The C band is coated with mouse monoclonal anti-chicken IgGγ antibody; the T band is coated with mouse monoclonal anti-SARS-CoV-2 N antigen conjugated with colour particles. The antigen–antibody colour particle complex travels through capillary action and binds to the mouse monoclonal anti-SARS-CoV-2 N antigen at the T band. The intensity of the coloured T band varies depending on the concentration of the N antigen in the sample.9
Briefly, each nasopharyngeal and nasal swab specimen was added to the extraction buffer provided in the kit. The filter nozzle cap was pressed tightly onto the extraction tube. Three drops of the extracted sample were applied to the test device, and the test result was read after 15–30 min. For a positive result, colour appears at both the C and T bands within 30 min.8,9
RNA Extraction SARS-CoV-2 RT-PCR
RNA was extracted using the DAAN kit following the manufacturer’s instructions using samples suspended in 2 mL of VTM. The extracted RNA was stored at −80°C until further application. RT-PCR Kit (BGI) was used for qualitative detection of SARS-CoV-2 nucleic acid. The Master Mix preparation and result interpretation followed the manufacturer’s instructions.12 Samples with a Ct value <37 for the target gene were considered positive for SARS-CoV-2.
Quality Assurance
To ensure the quality of the generated data and the analysis, internal quality assurance systems were in place for all laboratory procedures and there were external quality assurance mechanisms. The methods used had been validated prior to the study and if an amendment and/or modification had to be made, it was documented in the log books and reported to all members of the research group. Standard operating procedures were developed and strictly followed. The quality of the reagents and kits was checked regularly. All laboratory personnel received training for each procedure. Professional medical laboratory technologists collected all samples with the utmost care and attention. The research team and those who are actively participating in COVID-19 testing at the Department of Microbiology, Immunology and Parasitology COVID-19 testing centre performed all the tests and analysis. The research team, with the aid of a designated project manager, monitored every step of the data collection and laboratory analysis.
Data Analysis and Interpretation
We used SPSS Statistics Version 25 (IBM Corp., Armonk, NY, USA) for analysis. We calculated the sensitivity, specificity, positive predictive value and negative predictive value and their 95% confidential intervals (CIs) by using an online statistical tool.13 In an effort to use as much of the heterogeneous data as possible, we relaxed the ranges of cycle threshold (Ct) values by 3 points, namely <25, 25.1–30 and 30.1–36.
Ethical Considerations
We obtained ethical approval from the Department of Microbiology, Immunology and Parasitology Research Ethics Review Committee (protocol no. 022/21) and the College of Health Sciences Institutional Review Board (protocol no. 03-008) of Addis Ababa University. We secured permission to conduct the study from each hospital’s clinical director. We obtained written informed consent from the study participants prior to their recruitment to the study. For study participants under the age of 18, their parents or guardians provided written informed consent. The data collectors informed each study participant that the study was voluntary and that the participants could withdraw at any time without losing any health-related services. We ensured that they followed the guidelines of the Declaration of Helsinki.
Results
Characteristics of the Study Population
We evaluated 200 RT-PCR-confirmed samples from the two hospitals, including 100 SARS-CoV-2-positive and 100 SARS-CoV-2-negative samples. The mean age of the study participant was 46 years (standard deviation [SD] 16.3 years). Around 56% were male, and the rest were female. More than 50% of them presented with one or more symptoms, whereas the others had been tested as part of the routine screening when seeking other health services. More than two-third of the cases were tested <7 days after disease onset. The detailed characteristics of the study participants are presented in Supplementary Table 1.
Overall Diagnostic Performance
Of the 100 RT-PCR-confirmed SARS-CoV-2-positive samples, 95 showed a positive Standard Q COVID-19 Ag Test result. As shown in Table 1, when comparing the antigen test with the reference method (RT-PCR), the sensitivity was 95% (95% CI 88.7–98.4%), the specificity was 97% (95% CI 91.5–99.4%), the positive predictive value was 97% (95% CI 91.21–98.98%) and the negative predictive value was 95% (95% CI 89.19–97.85%).
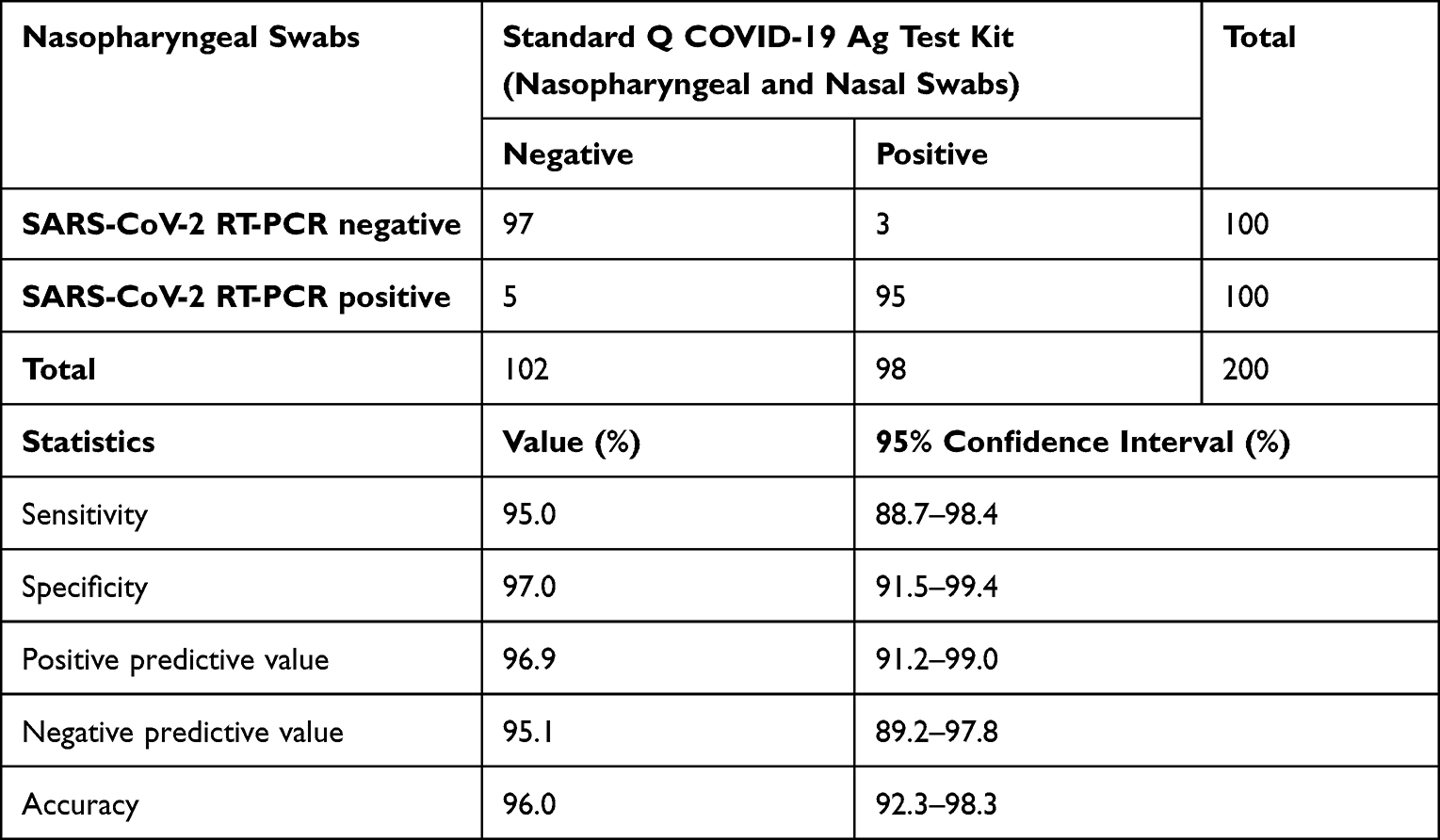 |
Table 1 Comparison of the Diagnostic Performance of the Standard Q COVID-19 Ag Test Kit and Real-Time Polymerase Chain Reaction (RT-PCR) at Selected Hospitals in Addis Ababa, Ethiopia, in 2021 |
Sensitivity of the Standard Q COVID-19 Ag Test with Respect to Ct Value and Symptom Onset
We also evaluated SARS-CoV-2 positivity in relation to Ct values (Table 2). Antigen positivity was higher with a lower Ct value. Indeed, antigen positivity was highest for samples with a Ct value < 25 and decreased dramatically when the Ct value was >30. Hence, there were considerable differences in sensitivity based on Ct values, with the highest sensitivity noted for Ct values <25.
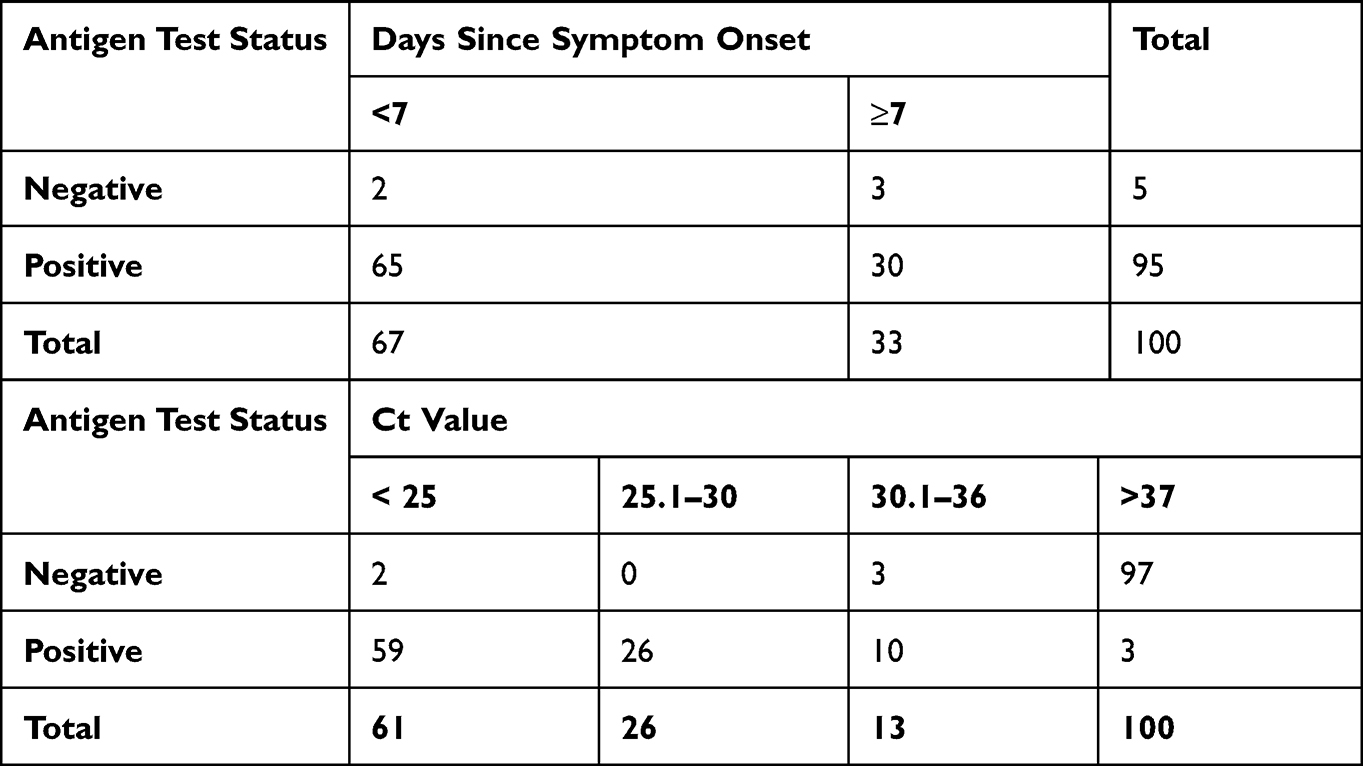 |
Table 2 Diagnostic Performance of the Standard Q COVID-19 Ag Test Kit Based on Symptom Onset and Cycle Threshold (Ct) Values at Selected Hospitals in Addis Ababa, Ethiopia, in 2021 |
We also evaluated SARS-CoV-2 positivity based on the time since symptom onset (Table 2). PCR positivity was higher (97%) among cases with <7 days since disease onset than cases with ≥7 days since symptom onset (91%). Hence, sensitivity was strongly associated with viral load.
Discussion
In the present study, we compared the diagnostic performance of the Standard Q COVID-19 Ag Test with RT-PCR using samples derived from two hospitals in Addis Ababa, Ethiopia. Accumulated evidence has demonstrated that rapid diagnostic tests are essential in providing data in a real-life high incidence test setting.2 Since the burden of COVID-19 is escalating in Ethiopia, there is an acute demand for utilising a rapid, cost-effective, reproducible and technically convenient diagnostic test to control the pandemic. Validation is critical to identify the best-performing technique.
The overall sensitivity and sensitivity of the rapid antigen test in this study met the WHO criteria of a mandatory cut-off of >80% for sensitivity and >97% for specificity for rapid antigen test kits.7 Research conducted in Africa and other locations has produced similar sensitivity and specificity to our study.2,3 Unlike molecular analysis, which demands trained personnel and expensive equipment, antigen-based laboratory methods have played a central role in the prevention and control of the COVID-19 pandemic because they are user-friendly, cost-effective and provide rapid test results. Consequently, it is possible to quickly identify individuals, while they are potential reservoir for further transmission and thus help to interrupt the spread of the virus.2 Differently from our study, there have been reports of low sensitivity (28.6%) but comparable specificity (98.2%).1 On the other hand, studies in other countries have shown comparable sensitivity and specificity as follows: 91.2% and 98.4% respectively, in Germany; 89% and 99.7% respectively, in Switzerland;2 and 98.3% and 98.7%, respectively, in Thailand.8
The majority of the study participants were symptomatic, and SARS-CoV-2 positivity was higher among these patients. The Ct values ranged from 25 to 40. Sensitivity and specificity were correlated with PCR Ct threshold: for both tests, positivity correlated with lower Ct values. Test positivity dropped rapidly from 27.4% to 10.5% when the Ct value increased from 30.1 to 36.0. This finding is in agreement with previous studies carried out in other countries.2,3,14
It has been shown that the viral load is related to symptom onset, with a high viral load noted during the symptomatic phase. Moreover, rapid diagnostic tests show the highest sensitivity in identifying infection among patients who are potentially contagious and would contribute to spread the virus.2,3,15 Such findings are also supported by another study conducted in New Delhi.16 Taken together, rapid diagnostic tests are not reliable in cases with a low viral load, including asymptomatic patients.2 Thus, as it has been suggested by the Standard Q COVID-19 Ag Test Kit protocol, rapid antigen test kits can be used as a potential diagnostic method particularly among symptomatic patients with disease onset <6 days to identify individuals with a high viral load. This information could allow overcoming transmission of the disease.9
Conclusion
We found that using nasopharyngeal and nasal swabs, the Standard Q COVID-19 Ag Test showed good concordance with the reference method (RT-PCR) using samples from patients in Addis Ababa, Ethiopia. We observed notable differences in sensitivity and specificity depending on the Ct value. Moreover, a higher percentage of symptomatic patients was positive for SARS CoV-2 using the antigen test and RT-PCR. Our findings alongside previously conducted research indicate that rapid antigen tests are a promising tool for SARS-CoV-2 detection and infection control, particularly in resource-limited setting such as Ethiopia.
Acknowledgments
It is our pleasure to extend our acknowledgement to all laboratory personnel and staff of Tikur Anbessa Specialized Hospital and Eka Kotebe General Hospital. We are also very grateful to the study participants for being willing to participate in this study. Our heartfelt thanks go to SD Biosensor® (Republic of Korea) for donating the Standard Q COVID-19 Ag Test Kits and for funding to accomplish the intended validation work. We also appreciate Martin Luther University for their additional financial support to realise this project.
Funding
This study was partially financed by Addis Ababa University, SD Biosensor® (Republic of Korea) and Martin Luther University (Halle, Germany).
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Caruana G, Lebrun -L-L, Aebischer O, et al. The dark side of SARS-CoV-2 rapid antigen testing: screening asymptomatic patients. New Microbes New Infec. 2021;42:100899. doi:10.1016/j.nmni.2021.100899
2. Berger A, Nsoga MTN, Perez-Rodriguez FJ, et al. Diagnostic accuracy of two commercial SARS-CoV-2 Antigen-detecting rapid tests at the point of care in community-based testing centers. PLoS One. 2021;16(3):e0248921. doi:10.1371/journal.pone.0248921
3. Bruzzone B, De Pace V, Caligiuri P, et al. Comparative diagnostic performance of rapid antigen detection tests for COVID-19 in a hospital setting. Int J Infect Dis. 2021;107:215–218. doi:10.1016/j.ijid.2021.04.072
4. Caruana G, Croxatto A, Coste AT, et al. Diagnostic strategies for SARS-CoV-2 infection and interpretation of microbiological results. Clin Microbiol Infect. 2020;26(9):1178–1182. doi:10.1016/j.cmi.2020.06.019
5. Schwob JM, Miauton A, Petrovic D, et al. Antigen rapid tests, nasopharyngeal PCR and saliva PCR to detect SARS-CoV-2: a prospective comparative clinical trial. medRxiv. 2020. doi:10.1101/2020.11.23.20237057
6. Oh S-M, Jeong H, Chang E, et al. Clinical application of the standard Q COVID-19 Ag Test for the detection of SARS-CoV-2 infection. J Korean Med Sci. 2021;36(14):e101. doi:10.3346/jkms.2021.36.e101
7. World Health Organization. Antigen-Detection in the Diagnosis of SARS-Cov-2 Infection. Geneva: World Health Organization; 2021.
8. Chaimayo C, Kaewnaphan B, Tanlieng N, et al. Rapid SARS-CoV-2 antigen detection assay in comparison with real-time RT-PCR assay for laboratory diagnosis of COVID-19 in Thailand. Virol J. 2020;17(1):177. doi:10.1186/s12985-020-01452-5
9. Biosensor S. SD Biosensor COVID-19 Ag STANDARD TM Q COVID-19 Ag test. Package leaflet; 2020. Available from: http://sdbiosensor.com/xe/product/7672.
10. Igloi Z, Velzing J, van Beek J, et al. Clinical evaluation of Roche SD biosensor rapid antigen test for SARS-CoV-2 in municipal health service testing site, the Netherlands. Emerg Infect Dis J. 2021;27(5):1323. doi:10.3201/eid2705.204688
11. Abrahim SA, Tessema M, Defar A, et al. Time to recovery and its predictors among adults hospitalized with COVID-19: a prospective cohort study in Ethiopia. PLoS One. 2020;15(12):e0244269. doi:10.1371/journal.pone.0244269
12. Garg A, Ghoshal U, Patel SS, et al. Evaluation of seven commercial RT-PCR kits for COVID-19 testing in pooled clinical specimens. J Med Virol. 2021;93(4):2281–2286. doi:10.1002/jmv.26691
13. MedCalc. Diagnostic test evaluation calculator; 2020. Available from: https://www.medcalc.org/calc/diagnostic_test.php.
14. Corman VM, Haage VC, Bleicker T, et al. Comparison of seven commercial SARS-CoV-2 rapid point-of-care antigen tests: a single-centre laboratory evaluation study. Lancet Microbe. 2021;2(7):e311–e319. doi:10.1016/S2666-5247(21)00056-2
15. Zou L, Ruan F, Huang M, et al. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N Engl J Med. 2020;382(12):1177–1179. doi:10.1056/NEJMc2001737
16. Gupta N, Agrawal S, Ish P, et al. Clinical and epidemiologic profile of the initial COVID-19 patients at a tertiary care centre in India. Monaldi Arch Chest Dis. 2020;90(1):193–196.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
COVID-19 and Saudi Arabia: Awareness, Attitude, and Practice
Fawzy MS, AlSadrah SA
Journal of Multidisciplinary Healthcare 2022, 15:1595-1618
Published Date: 26 July 2022
An Overview of Neurological and Psychiatric Complications During Post-COVID Period: A Narrative Review
Li D, Wang Q, Jia C, Lv Z, Yang J
Journal of Inflammation Research 2022, 15:4199-4215
Published Date: 26 July 2022
A Pilot Study of 0.4% Povidone-Iodine Nasal Spray to Eradicate SARS-CoV-2 in the Nasopharynx
Sirijatuphat R, Leelarasamee A, Puangpet T, Thitithanyanont A
Infection and Drug Resistance 2022, 15:7529-7536
Published Date: 21 December 2022
Distinct Features of Vascular Diseases in COVID-19
Ceasovschih A, Sorodoc V, Shor A, Haliga RE, Roth L, Lionte C, Onofrei Aursulesei V, Sirbu O, Culis N, Shapieva A, Tahir Khokhar MA, Statescu C, Sascau RA, Coman AE, Stoica A, Grigorescu ED, Banach M, Thomopoulos C, Sorodoc L
Journal of Inflammation Research 2023, 16:2783-2800
Published Date: 6 July 2023
Re-Emerging COVID-19: Controversy of Its Zoonotic Origin, Risks of Severity of Reinfection and Management
Chala B, Tilaye T, Waktole G
International Journal of General Medicine 2023, 16:4307-4319
Published Date: 20 September 2023