Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Mediating Effect of Depression on Relationship Between Sleep Disturbance and Locomotive Syndrome in Geriatric Cancer Patients
Authors Chen Y, Wang HN, Chen Y, Liang XF, Xu HW, Wu RR, Dong LH, Su H, Yang YL
Received 9 January 2026
Accepted for publication 15 April 2026
Published 28 April 2026 Volume 2026:19 594920
DOI https://doi.org/10.2147/JMDH.S594920
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Linda Yoder
Yao Chen,1,* Hu-Nan Wang,2,3,* Ying Chen,1 Xue-Fen Liang,4 Hai-Wa Xu,4 Rui-Rong Wu,1 Li-Hua Dong,4 Hui Su,1 Yu-Ling Yang1
1Department of Oncology, Affiliated Hospital of Jiangnan University, Wuxi, Jiangsu Province, 214122, People’s Republic of China; 2Laboratory of Oncology Precision Diagnosis and Treatment, Wuxi Medical College of Jiangnan University, Wuxi, 214122, Jiangsu Province, People’s Republic of China; 3Department of Cancer Diagnosis and Treatment Center, Affiliated Hospital of Jiangnan University, Wuxi, Jiangsu Province, 214122, People’s Republic of China; 4Department of Oncology, Donghai County People’s Hospital, Lianyungang, Jiangsu Province, 222300, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yu-Ling Yang, Department of Oncology, Affiliated Hospital of Jiangnan University, 1000 Hefeng Road, Wuxi, 214122, Jiangsu Province, People’s Republic of China, Tel +86-139-1249-7649, Email [email protected] Hui Su, Department of Oncology, Affiliated Hospital of Jiangnan University, 1000 Hefeng Road, Wuxi, Jiangsu Province, 214122, People’s Republic of China, Tel +86-137-7145-1810, Email [email protected]
Objective: To investigate the mediating role of depression between sleep disturbance and locomotive syndrome (LS) in geriatric cancer patients, and to provide a basis for interventions targeting motor function impairment in this population.
Methods: A convenience sample of 600 geriatric cancer patients was recruited in this cross-sectional study. General information questionnaires, the Pittsburgh Sleep Quality Index (PSQI), the Patient Health Questionnaire Depression Scale (PHQ-9), and the Geriatric Locomotive Function Scale (GLFS-25) were administered to measure depression, sleep disturbance, and LS. Multivariate logistic regression was used to evaluate the impact of sleep disturbance on LS. Bootstrap sampling was performed to analyze the mediating effect of depression scores this relationship.
Results: Valid questionnaires were obtained from 584 geriatric cancer patients. Sleep disturbances affected 216 patients (37.0%), including 66 (11.3%) with moderate-to-severe disturbances, while 259 (44.3%) had LS. After controlling for confounding factors, multivariate logistic regression showed that geriatric cancer patients with mild and moderate-to-severe sleep disturbances had 1.42-fold (95% CI: 1.23~1.67, P=0.001) and 1.81-fold (95% CI: 1.31~2.45, P< 0.001) higher risks of LS, respectively. Mediator analysis revealed that depression partially mediated the relationship between sleep disturbances and LS, with an effect size of 0.043 (95% CI: 0.032~0.055, P< 0.001), accounting for 21.15% of the total effect.
Conclusion: Depression, sleep disturbance, and LS are closely related. Sleep disturbance was directly and indirectly associated with LS through depression. Healthcare providers should pay attention to sleep disturbances and depression in geriatric cancer patients. For patients whose sleep quality cannot be effectively improved, alleviating depressive symptoms may help reduce the incidence of LS.
Keywords: sleep disturbance, depression, locomotive syndrome, mediating effect, geriatric cancer patients
Background
Organ aging progresses with advancing age, and aging itself is one of the most significant causes of tumor development. The incidence and mortality rates of tumors increase with age.1 A study by the U.S. National Institutes of Health identified aging as the primary risk factor for tumor development.2 In 2022, China recorded 4.8247 million new cancer cases, with a standardized incidence rate of 201.61 per 100,000 people. The country reported 2.5742 million cancer deaths, with a standardized mortality rate of 96.47 per 100,000 people, both ranking highest globally.3 The data indicate that tumor incidence rises markedly from the 35–39 age group, peaking in the 80–84 age group.3 Mortality rates significantly increase from the 40~44 age group and peak in those aged 85 and older.3 By 2035, approximately 60% of newly diagnosed cancer patients worldwide will be aged 65 or older. As the aging population expands, cancer incidence and mortality rates continue to rise. Malignant tumors have thus become a serious public health issue threatening the lives and health of China’s elderly population.1,4
The Japanese Orthopaedic Association introduced locomotive syndrome (LS).5 Its essence is not defined by traditional pathology but by epidemiology. Its purpose is to raise awareness of musculoskeletal health, enabling timely prevention and treatment of musculoskeletal disorders. This aims to reduce the incidence of mobility-related disabilities among the elderly, thus alleviating the caregiving burden on families and society.6 One of the primary causes of lower back pain includes systemic skeletal disorders affecting bones, joints, and muscles, such as osteoporosis, degenerative arthritis, and degenerative lumbar disorders.7 LS disrupts inflammatory pathways and impairs the central nervous system, leading to neuroendocrine dysfunction and oxidative stress damage. Consequently, patients experience prolonged hospital stays and increased mortality rates.8
With advancing age, elderly individuals experience declines in physiological functions, including changes in sleep duration, circadian rhythms, and sleep efficiency. These alterations manifest as prolonged sleep latency, reduced deep sleep duration, fragmented sleep patterns, and early sleep onset with early awakening.9 Sleep disturbances can disrupt restorative processes, preventing adequate blood circulation to bodily systems. This leads to diminished immune function and metabolic capabilities.10 Older cancer patients may experience reduced sleep quality due to various treatments, pain, and multiple medications. This condition may lead to complications such as cognitive impairment, pain sensitization, arrhythmia, blood pressure fluctuations, and even unexpected death.11
Recently, research has increasingly explored the potential correlation between sleep disturbances and movement disorders in the elderly. Multiple studies demonstrate that poor sleep may be associated with symptoms of movement disorders in geriatric cancer patients. These symptoms include decreased muscle strength and balance, reduced mobility, increased risk of falls, and cognitive decline. Such findings suggest a potential underlying connection between sleep disturbances and movement disorders.12,13 According to authoritative statistics from the WHO, approximately 280 million people (3.8%) worldwide suffer from depression, with the elderly population aged 60 and above accounting for 5.7%.14 Depression increases sympathetic nervous system activity, potentially impairing cerebral vasoconstriction and vasodilation responses, the autoregulation of cerebral blood flow, and the establishment of collateral circulation. This disruption may impede brain functional reorganization, potentially limiting motor function recovery.15 Recent evidence highlights the substantial burden of sleep disturbance and depression in older cancer patients. A systematic review and meta-analysis involving 16,223 cancer patients reported a pooled prevalence of poor sleep quality of 57.4% (95% CI: 53.3%~61.6%), significantly higher than that observed in the general elderly population.16 Another large-scale meta-analysis including 135,015 cancer survivors from over 30 countries revealed a depression prevalence of 23.7% (95% CI: 20.1%~27.4%) and a sleep disorder prevalence of 34.1% (95% CI: 27.9%~40.6%).17 These findings underscore that sleep disturbance and depression are not merely age-related conditions but are significantly amplified by cancer and its treatments, rendering geriatric cancer patients a particularly vulnerable population requiring targeted investigation.
Despite growing evidence linking sleep disturbance to motor dysfunction in the general elderly population, and depression to physical function decline, no studies to date have specifically examined whether depression mediates the relationship between sleep disturbance and locomotive syndrome in geriatric cancer patients.12 Given the high prevalence of both sleep disturbance and depression in this population, and their documented impact on functional outcomes, understanding this mediating mechanism is critical for developing targeted interventions. Geriatric cancer patients represent a distinct subgroup within the elderly population, characterized by the compounded effects of aging, malignancy, and cancer-related treatments.3 Cancer therapies such as chemotherapy and radiation can exacerbate sleep disturbances through direct physiological effects and symptom burden, while the psychological impact of a cancer diagnosis may heighten vulnerability to depression.11 These unique factors may render geriatric cancer patients particularly susceptible to the detrimental effects of sleep disturbance on motor function, potentially through depressive pathways. Therefore, findings from studies on general elderly populations may not be directly generalizable to this clinical population, underscoring the need for population-specific investigation.
Research indicates that poor sleep quality and depression constitute risk factors for LS. Sleep quality also correlates positively with depression. Therefore, depression may serve as a mediating variable between sleep and movement disorders.7,18,19 A mediation framework is conceptually appropriate for this study because we hypothesize that sleep disturbance may associated with LS through two distinct pathways. First, sleep disturbance may directly impair motor function through physiological mechanisms such as circadian rhythm disruption, hormonal imbalances, and impaired tissue repair. Second, sleep disturbance may indirectly affect motor function by exacerbating depressive symptoms, which in turn reduce physical activity engagement, promote social withdrawal, and contribute to muscle deconditioning and functional decline. Testing this mediating pathway can elucidate the mechanisms linking sleep disturbance to motor dysfunction and identify potential intervention targets. This study focuses on geriatric cancer patients and employs structural equation modeling (SEM) to clarify the mediating effect of depression between sleep disturbances and LS. These findings provide clinical evidence for improving patients’ sleep and depressive states, potentially reducing the incidence of LS.
Objects and Methods
This study was a single-center, cross-sectional survey. Participants voluntarily enrolled and provided written informed consent. The study was approved by the Ethics Committee of the Affiliated Hospital of Jiangnan University (No. LS2023101) and registered in the Chinese Clinical Trial Registry (No. ChiCTR2400079958) on January 17, 2024. The study adhered to the principles of the Declaration of Helsinki.
Objects
A convenience sampling method was used to recruit 600 geriatric cancer patients who visited the Cancer Center of Jiangnan University Affiliated Hospital between June 2024 and March 2025.
Inclusion Criteria
(1) Age ≥60 years; (2) Diagnosed with malignant tumors according to the 8th edition of the International Tumor TNM Staging System, without bone metastases; (3) Receiving anticancer chemotherapy or other treatments rather than palliative care; (4) Barthel Index ≥60; (5) No history of motor function disorders caused by primary orthopedic conditions; (6) Voluntarily provided informed consent.
Exclusion Criteria
(1) Any contraindication to exercise; (2) Severe physical or mental illness, such as clinically diagnosed major depressive disorder (diagnosed by a psychiatrist, rather than depressive symptoms measured by scales); (3) Cognitive impairment.
Research Instruments
General Information Questionnaire
A self-developed questionnaire collected data on age, gender, living arrangements, exercise habits, primary tumor type, and comorbidities. Exercise habits were defined as engaging in moderate-to-vigorous physical activity at least three times per week for 30 minutes or more per session. Hypertension, diabetes, coronary heart disease, and cerebrovascular disease were self-reported and confirmed by secondary-level or higher medical institutions.
LS
The Geriatric Locomotive Function Scale (GLFS-25), developed by Seichi in Japan, was used to assess locomotive dysfunction syndrome.20 The GLFS-25 comprises 25 items across four domains: physical pain, activities of daily living (ADL), social activities, and mental state. Each item uses a 5-point Likert scale (0–4 points; total score 0–100 points). The scale shows a Cronbach’s α coefficient of 0.93, indicating high reliability and validity. A score ≥16 indicates the presence of LS in the participant.21,22
Depression
The Patient Health Questionnaire-9 (PHQ-9) was used to assess depressive symptoms. Developed by Kroenke et al in 2001, it evaluates symptoms over the past two weeks, with a Cronbach’s α of 0.879.23 The PHQ-9 contains nine items rated on a 4-point Likert scale from 0 (“not at all”) to 3 (“almost every day”), with a total score ranging from 0 to 27. Higher scores indicate more severe depression. Scores of 0–4 represent no depression, 5–9 mild depression, 10–14 moderate depression, 15–19 moderate-to-severe depression, and 20–27 severe depression.21
Sleep Disturbance
The Pittsburgh Sleep Quality Index (PSQI) was used to assess sleep quality. Developed by Buysse et al at the University of Pittsburgh in 1989, the PSQI evaluates sleep quality over the preceding month, with a Cronbach’s α coefficient of 0.830.24 The scale includes 19 self-report items and 5 rater-report items, though only the first 18 self-report items were used in this study. It assesses seven dimensions: subjective sleep quality, sleep onset latency, sleep duration, sleep efficiency, sleep disturbances, hypnotic medication use, and daytime dysfunction. Each item uses a 4-point Likert scale, with total scores ranging from 0 to 21; higher scores indicate poorer sleep quality. A PSQI score ≥6 indicates sleep disturbance. Scores of 0–5 represent normal sleep, 6–10 poor sleep quality, 11–15 very poor sleep quality, and 16–21 extremely poor sleep quality.25 In this study, poor sleep quality was defined as mild sleep disturbance, and very poor or extremely poor sleep quality as moderate-to-severe sleep disturbance.
Sample Size
The primary scales used (GLFS-25, PHQ-9, and PSQI) comprised 52 variables. The sample size was calculated as 10 times the number of variables, with a 10% attrition rate included. At least 578 participants were required. A total of 600 questionnaires were distributed, with 584 valid responses collected, yielding a valid response rate of 97.3%.
Statistical Methods
Data were entered into EpiData 3.0. Descriptive analysis, χ2 tests, and multivariate logistic regression analyses were performed using SPSS 26.0. The mediating effect of depression on the relationship between sleep disturbances and LS was analyzed using the Bootstrap method. For clinical interpretability, LS was treated as a binary outcome (GLFS-25 score≥16) in the multivariate logistic regression analysis to estimate the risk of LS associated with sleep disturbance and depression. For the mediation analysis, the continuous scores of GLFS-25, PHQ-9, and PSQI were standardized to preserve information richness and enhance statistical power, consistent with the assumptions of the mediation modeling framework. Both analytic approaches serve complementary purposes: logistic regression provides clinically actionable risk estimates, while mediation analysis elucidates the mechanistic pathway. The significance level was set at 0.05 for two-tailed tests. The study workflow is presented in Figure 1.
 |
Figure 1 The Study Workflow. |
Results
General Information
The mean age of the 584 geriatric cancer patients was 68.23 ± 4.78 years. The mean scores for LS, depression, and sleep disturbance were 14.92 ± 7.87, 6.48 ± 3.23, and 7.63 ± 3.72, respectively. The primary tumor types in this population are shown in Figure 2. Among these geriatric cancer patients, 259 (44.3%) had LS. Detailed information is presented in Table 1.
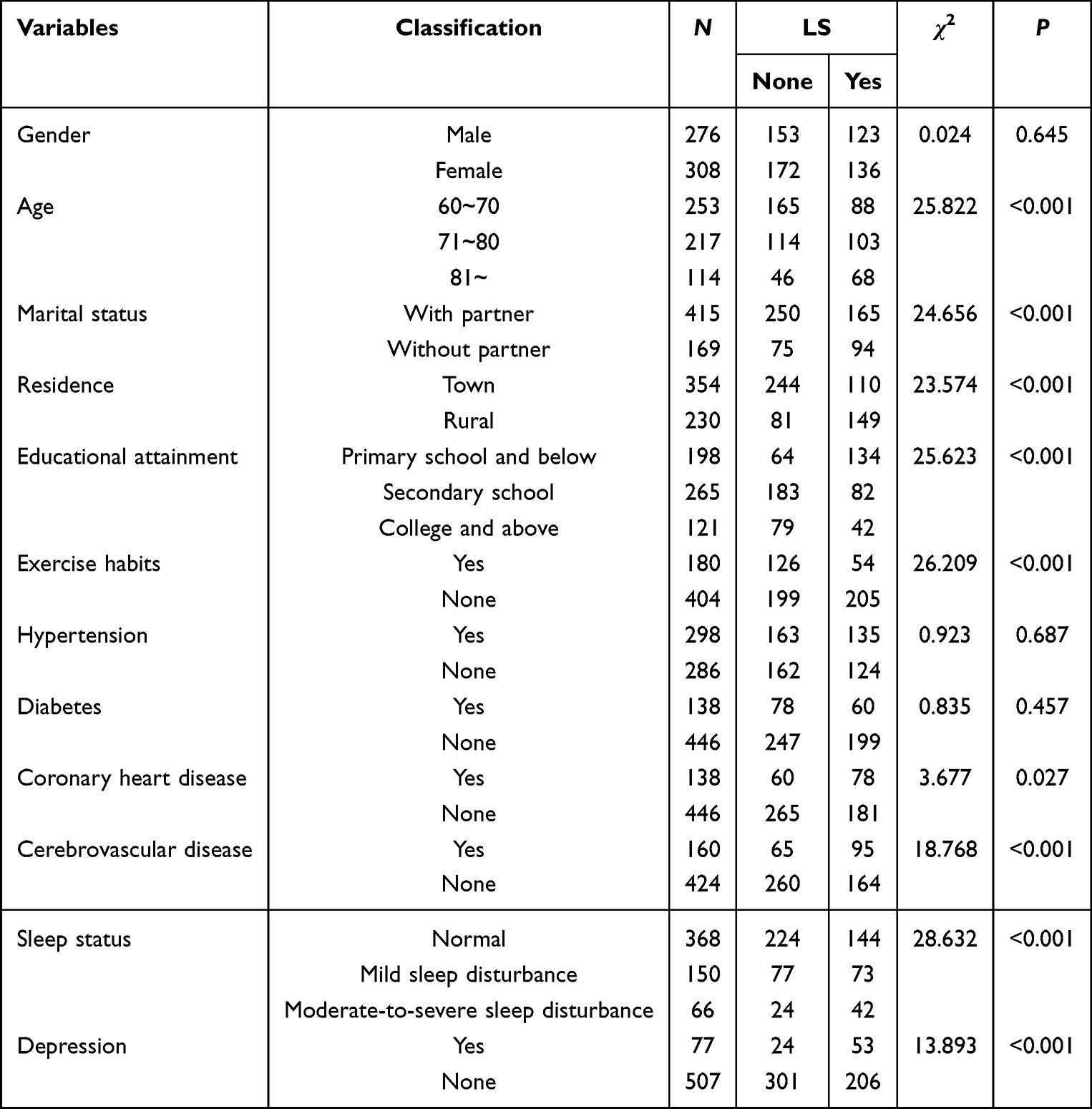 |
Table 1 Comparison of LS Incidence Among Geriatric Cancer Patients with Different Characteristics |
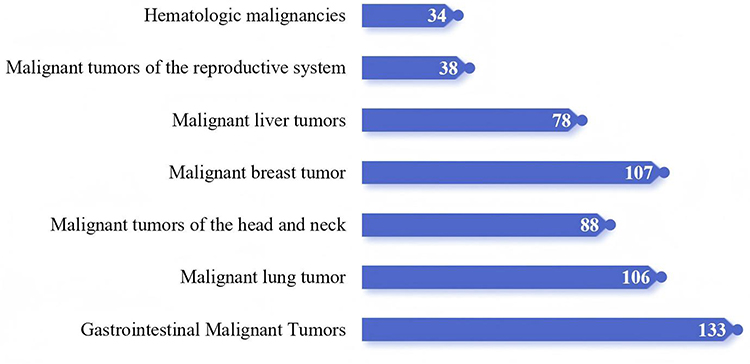 |
Figure 2 The Primary Tumor Types of 584 Geriatric Cancer Patients. |
Impact of Sleep Disturbances and Depression on LS in Geriatric Cancer Patients
Variables with P < 0.05 in Table 1 were set as covariates and controlled in the regression model. Multivariate logistic regression analysis indicated that patients with mild sleep disturbances and moderate-to-severe sleep disturbances had 1.42-fold (95% CI: 1.23–1.67, P = 0.001) and 1.81-fold higher risks (95% CI: 1.31–2.45, P < 0.001) of developing LS, respectively. Patients with depression had a 2.34-fold higher risk of developing LS compared to those without depression (95% CI: 1.85–3.12, P < 0.001), as shown in Table 2.
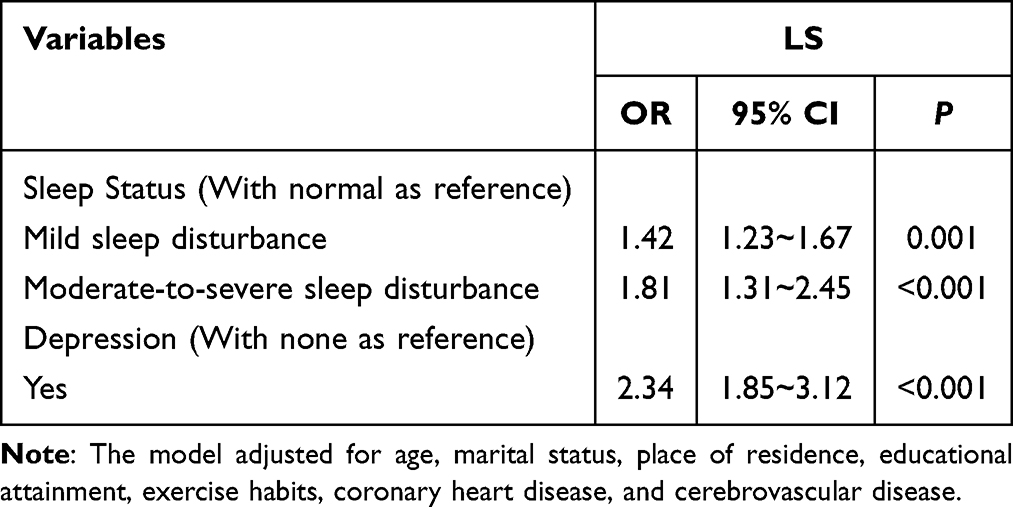 |
Table 2 Multivariate Logistic Regression Analysis of Sleep Disturbances and Depression with LS |
Mediating Effect of Depression Between Sleep Disturbances and LS in Geriatric Cancer Patients
Results in Table 2 indicate that, after adjusting for relevant variables, sleep disturbances and depression remained significantly associated with LS. LS was assessed using the GLFS-25, sleep disturbance with the PSQI, and depression with the PHQ-9. Spearman correlation analysis of GLFS-25, PSQI, and PHQ-9 scores revealed significant correlations among sleep disturbances, depression, and LS (P < 0.001). Correlation results are shown in Table 3.
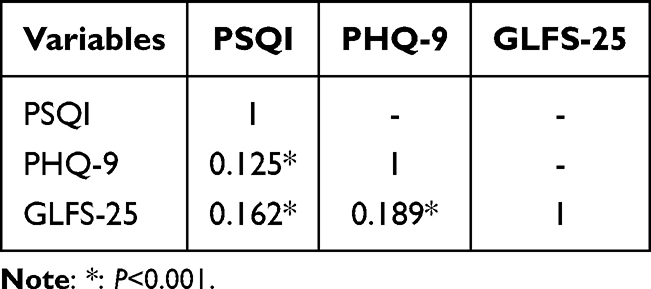 |
Table 3 Correlation Analysis for Sleep Disturbances, Depression, and LS (r, n=584) |
After standardizing the self-reported PSQI, PHQ-9, and GLFS-25 scores, these were treated as the independent variable (X), mediating variable (M), and dependent variable (Y), respectively. The Bootstrap method was employed to examine the mediating effect: Model 1: Regression analysis of the independent variable (X) on the dependent variable (Y); Model 2: Regression analysis of the independent variable (X) on the mediating variable (M); Model 3: Hierarchical regression analysis of the independent variable (X) and mediating variable (M) on the dependent variable (Y) (first-level X, second-level M). Results indicated that the effect of sleep disturbances on depression was 0.132 (95% CI: 0.113–0.164, P < 0.001). The total effect of sleep disturbances on LS was 0.171 (95% CI: 0.143–0.193, P < 0.001), with a direct effect of 0.138 (95% CI: 0.118–0.162, P < 0.001) and an indirect effect of 0.043 (95% CI: 0.032–0.055, P < 0.001). The mediation rate of depression was 21.15% (0.043/0.171 × 100%; Figure 3).
 |
Figure 3 Mediating Effect of Depression on the Relationship between Sleep Disturbances and LS. |
Discussion
Sleep disturbances and motor dysfunction commonly result from neurodegenerative processes in the aging brain.26 This study found significant positive correlations among sleep disturbances, depression, and LS. The findings indicate that sleep disturbances and depression are risk factors for LS. Compared to individuals without sleep disturbances, those with mild and moderate-to-severe sleep disturbances had a 42% and 81% increased risk of LS, respectively. Compared to individuals without depression, those with depression had a 134% increased risk of LS (OR = 2.34). Poor sleep quality may be associated with disruptions in circadian rhythms, hormonal imbalances, impaired immune function, muscle and protein breakdown, and diminished motor function.27,28 Depression may be associated with reduced activity levels, decreased social engagement, impaired mobility, and diminished social interactions. Depressive symptoms often involve negative emotions, which may cause reduced appetite, weight loss, malnutrition, lower physical activity levels, and increased risk of falls, all contributing to impaired physical function.29,30 For geriatric cancer patients, improving sleep and addressing depression can potentially enhance their quality of life.
In epidemiological research, pathways linking exposure (sleep disturbances) to outcomes (LS) need clarification to determine the overall impact. This impact includes direct effects of exposure and indirect effects mediated by an intermediate variable (depression). Together, these effects constitute the total impact of exposure on outcomes. Correlation analysis in this study revealed significant associations among depression, sleep disturbances, and LS. With depression as the mediating variable and after controlling for covariates, depression partially mediated the relationship between sleep disturbances and LS, accounting for 21.15% of the total effect. This suggests that sleep disturbances not only directly increase LS incidence but also indirectly predict LS through depression, consistent with other studies. Good sleep quality is essential for maintaining physical health and enhancing quality of life. Poor sleep quality may be associated with weakened immune function, depressive moods, reduced appetite, weight loss, diminished physical activity, impaired motor function, and ultimately frailty.29
Due to physiological changes, multiple comorbidities, and associated complications, most geriatric cancer patients experience a decline in sleep quality.31 Although few studies have explored the mediating role of depression between sleep disturbances and long-term symptoms, Alison’s research suggested that regular mental health screening may benefit patients’ overall physical well-being.32 Improving sleep disturbances thus not only directly affects LS but also indirectly improves it by alleviating depression. As sleep quality significantly influences locomotor function, enhancing sleep quality in geriatric cancer patients may serve as an important component of preventive and interventional strategies for locomotor dysfunction disorders. For patients whose sleep quality does not improve, multifaceted education, brief cognitive behavioral therapy, and peer-participatory care may relieve depressive symptoms. Understanding how poor sleep quality impacts long-term sequelae (LS) may help reduce LS incidence and improve long-term rehabilitation outcomes.33
The findings of this study provide important directions for future research. First, multicenter prospective cohort studies are needed to validate the stability of depression’s mediating role between sleep disturbance and locomotive syndrome and to explore the causal temporal relationships among these variables. Second, interventional studies could be designed based on our findings, such as comparing the effects of sleep improvement alone, depression relief alone, and combined interventions on preventing or delaying motor function decline in geriatric cancer patients. Furthermore, future studies could incorporate objective measures (eg., activity monitoring devices, inflammatory markers) to further elucidate the biological mechanisms linking sleep, mood, and motor function.
Limitations
This study has several limitations. First, data of this study were collected through a single-center, cross-sectional survey. Future research should validate these findings using larger, multicenter samples. Second, patients undergoing active antitumor therapy at our institution generally had relatively good health and self-care abilities. Therefore, patients who were severely ill or unable to care for themselves were not included. It should be emphasized that, due to the cross-sectional design of this study, although significant associations and a mediating pathway among sleep disturbance, depression, and locomotive syndrome were identified, causal relationships cannot be inferred. Sleep disturbance and depression may mutually influence each other and jointly affect motor function; conversely, declines in motor function may exacerbate sleep disturbance and depressive symptoms. Future studies employing longitudinal designs are warranted to further validate the temporal relationships and causal directions among these variables. Future studies should include larger sample sizes with diverse levels of ADL and employ cohort designs to clarify causal relationships among depression, sleep disturbances, and LS in geriatric cancer patients.
Conclusion
In this cross-sectional study, depression, sleep disturbance, and locomotive syndrome were found to be closely associated among geriatric cancer patients. Sleep disturbance was directly and indirectly associated with LS through depression. These findings underscore the importance of integrated screening for both sleep disturbance and depressive symptoms in geriatric cancer patients, as addressing these interconnected factors may more effectively prevent or delay the onset of locomotive syndrome. For patients whose sleep quality cannot be readily improved, targeted interventions to alleviate depressive symptoms—such as brief cognitive behavioral therapy or peer-support programs—may offer an alternative pathway to reduce the risk of motor function decline. Healthcare providers should therefore pay close attention to both sleep disturbances and depression in this population. Future research should employ longitudinal designs to confirm causal relationships and evaluate the effectiveness of integrated intervention strategies.
Data Sharing Statement
Informed consent was obtained from all participants, which permitted the use of their deidentified data for this study and for associated data sharing purposes. Although the data will not be made publicly or unconditionally available, reasonable requests may be directed to the corresponding author Yu-Ling Yang and Hui Su to discuss the possibility of data access, subject to compliance with relevant ethical and institutional policies. This arrangement will remain in place indefinitely following publication.
Ethics Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Ethics Committee of the Affiliated Hospital of Jiangnan University (No. LS2023101) and completed the Chinese Clinical Trial Registration (No. ChiCTR2400079958). The date of first registration is 17/01/2024.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patients to publish this paper.
Acknowledgments
Yao Chen and Hu-Nan Wang are co-first authors for this study. We appreciate all participants for their time and effort.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research project was funded by the Jiangsu Provincial Traditional Chinese Medicine Science and Technology Development Plan Project (No.MS2024063), Research Project on Hospital Management Innovation in Jiangsu Province (No.JSYGY-3-2024-601), the Regional Medical Center Development Program under the partnership between Jiangnan University Affiliated Hospital and Donghai County People’s Hospital (No.DHBFH202501, No.DHBFH202503 and No.DHBFM202504) and the Scientific and Technological Achievements Promotion Project of Wuxi Municipal Health Commission Project Program (No.T202336). The funders had no role in considering the study design or in the collection, analysis, interpretation of data, writing of the report, or decision to submit the article for publication. The sponsors had no role in the design, execution, interpretation, or writing of the study. We also appreciate all participants for their time and effort.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Cree IA, Ruiz BII, Zavadil J, et al. The international collaboration for cancer classification and research. Int J Cancer. 2021;148(3):
2. Fusco D, Ferrini A, Pasqualetti G, et al. Comprehensive geriatric assessment in older adults with cancer: recommendations by the Italian society of geriatrics and gerontology (SIGG). Eur J Clin Invest. 2021;51(1):e13347. doi:10.1111/eci.13347
3. Han B, Zheng R, Zeng H, et al. Cancer incidence and mortality in China, 2022. J Natl Cancer Cent. 2024;4(1):
4. Jeon M, Jang H, Lim A, Kim S. Frailty and its associated factors among older adults with cancer undergoing chemotherapy as outpatients: a cross~sectional study. Eur J Oncol Nurs. 2022;60:102192. doi:10.1016/j.ejon.2022.102192
5. Nakamura K. Locomotive syndrome: disability-free life expectancy and locomotive organ health in a “super~aged” society. J Orthop Sci. 2009;14(1):
6. Ono R, Murata S, Uchida K, Endo T, Otani K. Reciprocal relationship between locomotive syndrome and social frailty in older adults. Geriatr Gerontol Int. 2021;21(11):
7. Iwamoto Y, Imura T, Hirata K, et al. The risk factors for development or progression of locomotive syndrome: a systematic review. Nagoya J Med Sci. 2025;87(1):
8. Ohba T, Oba H, Koyama K, et al. Locomotive syndrome: prevalence, surgical outcomes, and physical performance of patients treated to correct adult spinal deformity. J Orthop Sci. 2021;26(4):
9. Yaremchuk K. Sleep disturbances in the elderly. Clin Geriatr Med. 2018;34(2):
10. Çavuşoğlu Ç, Deniz O, Doğrul RT, et al. Frailty is associated with poor sleep quality in the oldest old. Turk J Med Sci. 2021;51(2):
11. Lane H, Saunders R, Crookes K, et al. Prevalence of frailty and pain in hospitalised cancer patients: implications for older adult care. Intern Med J. 2024;54(4):
12. Ribeiro BC, AdACE S, LBRd S, JBdA M, Carneiro SR, Neves LMT. Risk stratification for frailty, impairment and assessment of sleep disturbances in community~dwelling older adults. Exp Gerontol. 2024;187:112370. doi:10.1016/j.exger.2024.112370
13. Aditi SSK, Jaiswal AK, Verma M, Verma M. Is there a ubiquitous association between sleep disturbance and frailty? findings from LASI (2017~18). BMC Geriatr. 2023;23(1):429. doi:10.1186/s12877-023-04148-x
14. Global health data exchange(GHDx)[EB/OL].[2023~04~03]. Available from: https://vizhub.healthdata.org/gbd~results/.
15. Zhang J, Du L, Li J, et al. Association between circadian variation of heart rate and mortality among critically ill patients: a retrospective cohort study. BMC Anesthesiol. 2022;22(1):45. doi:10.1186/s12871-022-01586-9
16. Chen MY, Zheng WL, Liu YF, et al. Global prevalence of poor sleep quality in cancer patients: a systematic review and meta-analysis. Gen Hosp Psychiatry. 2024;87:1–10. doi:10.1016/j.genhosppsych.2023.12.004
17. Ge MW, Wang HF, Zhang XQ, et al. Global prevalence of mental health problems among cancer survivors: a meta-analysis from 31 countries. Psychooncology. 2025;34(1):e70058. doi:10.1002/pon.70077
18. Kato M, Ozaki E, Matsui D, et al. Locomotive syndrome and depressive symptoms: a cross~sectional study in middle~aged women. Mod Rheumatol. 2024;34(4):
19. Kato M, Ozaki E, Omichi C, et al. Association between poor sleep quality and locomotive syndrome in middle~aged and older women: a community~based, cross~sectional study. Mod Rheumatol. 2024;34(2):
20. Seichi A, Hoshino Y, Doi T, Akai M, Tobimatsu Y, Iwaya T. Development of a screening tool for risk of locomotive syndrome in the elderly: the 25~question geriatric locomotive function scale. J Orthop Sci. 2012;17(2):
21. Akaras E, Başar S, Koç K, Kasali K. Translation, cultural adaptation, and Turkish validation of the tool 25-question geriatric locomotive function scale. BMC Geriatr. 2025;25(1):961. doi:10.1186/s12877-025-06725-8
22. Yang Y~L, Wang H~H, Su H, et al. Reliability and validity tests of the Chinese version of the geriatric locomotive function scale (GLFS~25) in tumor survivors. Heliyon. 2024;10(9):e29604. doi:10.1016/j.heliyon.2024.e29604
23. Kroenke K, Spitzer RL, Williams JB. The PHQ~9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):
24. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):
25. Chen HC, Hsu NW, Pan PJ, Kuo PH, Chien MY, Chou P. The development of a rapid classification scale for sleep quality in community~dwelling older adults ~ the Yilan study, Taiwan. Nat Sci Sleep. 2021;13:
26. Zhang L, Ukawa S, Zhao W, et al. Daily sleep duration and the risk of incident disability among younger elderly Japanese adults in the new integrated suburban seniority investigation project: a prospective study using competing event analysis. Geriatr Gerontol Int. 2019;19(9):
27. Zou D, Wennman H, Ekblom Ö, et al. Insomnia and cardiorespiratory fitness in a middle~aged population: the SCAPIS pilot study. Sleep Breath. 2019;23(1):
28. Zhang X, Meng X, Chen Y, Leng SX, Zhang H. The biology of aging and cancer: frailty, inflammation, and immunity. Cancer J. 2017;23(4):
29. Zhang S, Stubbs B, Das Munshi J. Complex mental health needs in older people living with frailty. Br J Hosp Med. 2020;81(12):
30. Yarnall AJ, Sayer AA, Clegg A, Rockwood K, Parker S, Hindle JV. New horizons in multimorbidity in older adults. Age Ageing. 2017;46(6):
31. Zhou Z, Yang Y, Sun J, et al. Heterogeneity of pain~fatigue~sleep disturbance symptom clusters in lung cancer patients after chemotherapy: a latent profile analysis. Support Care Cancer. 2024;32(12):821. doi:10.1007/s00520-024-09032-x
32. Zucca A, Sanson~Fisher R, Waller A, Carey M, Boyes AW, Proietto A. Does screening for physical and psychosocial symptoms vary between medical oncology treatment centres? Psychooncology. 2016;25(5):
33. Zyzniewska Banaszak E, Kucharska Mazur J, Mazur A. Physiotherapy and physical activity as factors improving the psychological state of patients with cancer. Front Psychiatry. 2021;12:772694. doi:10.3389/fpsyt.2021.772694
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Resilience Moderates the Association of Sleep Disturbance and Sleep Reactivity with Depressive Symptoms in Adult Volunteers
Terao I, Masuya J, Morishita C, Higashiyama M, Shimura A, Tamada Y, Inoue T, Fujimura Y
Neuropsychiatric Disease and Treatment 2022, 18:1249-1257
Published Date: 20 June 2022
Psychological Disturbances and Their Association with Sleep Disturbance in Patients Admitted for Arrhythmia Diseases
Hu LX, Tang M, Hua W, Ren XQ, Jia YH, Chu JM, Zhang JT, Liu XN
Neuropsychiatric Disease and Treatment 2022, 18:1739-1750
Published Date: 17 August 2022
Therapy for Psychiatric Comorbidities in Patients with Episodic Cluster Headache: A Prospective Multicenter Study
Liu Q, Zhang Y, Hu C, Yuan D, Wang K, Fan W, Pan F, Li Q, Wang Y, Tan G
Journal of Pain Research 2022, 15:3245-3254
Published Date: 18 October 2022
Relationships Among Trajectories of Sleep Disturbance, Depression, and Antiretroviral Therapy in Persons Newly Diagnosed with HIV: A One-and-a-Half-Year Observational Longitudinal Study
Chen CC, Liu HY, Chen YC, Ko NY
Nature and Science of Sleep 2022, 14:2133-2142
Published Date: 2 December 2022
Sleep Quality Among People with Type 2 Diabetes Mellitus During COVID-19 Pandemic: Evidence from Qatar’s National Diabetes Center
Abdu Y, Naja S, Mohamed Ibrahim MI, Abdou M, Ahmed R, Elhag S, Saleh AO, Yassin M, Bougmiza I
Diabetes, Metabolic Syndrome and Obesity 2023, 16:2803-2812
Published Date: 14 September 2023