")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 18
Resilience Moderates the Association of Sleep Disturbance and Sleep Reactivity with Depressive Symptoms in Adult Volunteers
Authors Terao I, Masuya J , Morishita C , Higashiyama M, Shimura A , Tamada Y , Inoue T , Fujimura Y
Received 6 February 2022
Accepted for publication 3 June 2022
Published 20 June 2022 Volume 2022:18 Pages 1249—1257
DOI https://doi.org/10.2147/NDT.S361353
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Taro Kishi
Itsuki Terao,1 Jiro Masuya,1 Chihiro Morishita,1 Motoki Higashiyama,1 Akiyoshi Shimura,1 Yu Tamada,1,2 Takeshi Inoue,1 Yota Fujimura1
1Department of Psychiatry, Tokyo Medical University, Tokyo, Japan; 2Department of Psychiatry, Toranomon Hospital Kajigaya, Kawasaki, Kanagawa, Japan
Correspondence: Chihiro Morishita, Department of Psychiatry, Tokyo Medical University, 6-7-1 Nishishinjuku, Shinjuku-ku, Tokyo, 160-0023, Japan, Tel +81 3 3342 6111, Fax +81 3 3340 4499, Email [email protected]
Purpose: Depression poses a substantial burden worldwide. Therefore, elucidating the pathophysiological mechanism of depression is important. Sleep disturbance and sleep reactivity are symptoms of depression and are also known to exacerbate depressive symptoms. On the other hand, it is well known that resilience ameliorates depressive symptoms. To our knowledge, there have been no reports to date regarding the interaction effects among sleep disturbance, sleep reactivity, and resilience on depressive symptoms. We hypothesized that resilience buffers the aggravating effects of sleep disturbance and sleep reactivity on depressive symptoms. To test this hypothesis, we conducted hierarchical multiple regression analyses.
Subjects and Methods: A total of 584 Japanese adult volunteers were recruited between April 2017 and April 2018 by convenience sampling. Their demographic characteristics, sleep disturbance, sleep reactivity, resilience, and depressive symptoms were investigated using self-administered questionnaires. The data were analyzed using hierarchical multiple regression analyses.
Results: Sleep disturbance and sleep reactivity were significantly positively associated with depressive symptoms, whereas resilience was significantly negatively associated with depressive symptoms. Moreover, there was a significant interaction between sleep disturbance or sleep reactivity and resilience on depressive symptoms. Resilience significantly alleviated the aggravating effect of sleep disturbance and sleep reactivity on depressive symptoms.
Conclusion: Our results indicate that people with lower resilience have more severe depressive symptoms that are associated with sleep disturbance and sleep reactivity. Therefore, there is a possibility that the enhancement of resilience will buffer the aggravating effects of sleep disturbance and sleep reactivity on depressive symptoms, and that improving sleep quality might alleviate the negative effect of low resilience on depressive symptoms.
Keywords: depression, resilience, sleep disturbance, sleep reactivity, CD-RISC
Introduction
Depression is a common disease, with a reported lifetime prevalence of 15% to 18%, and is a great burden on economies worldwide.1,2 Multiple factors are assumed to be involved in the etiology of depression, and a large number of studies have investigated the etiology of depression from various points of view. However, the causal factors of depression have not yet been clarified. Several longitudinal studies have suggested that sleep disturbance might be risk factors for depression.3,4 A meta-analysis of 21 longitudinal studies showed that non-depressed people with insomnia have a two-fold higher risk of developing depression compared with people without insomnia.3 These previous studies suggested that sleep disturbance is not fully dependent on depression, but is actually a risk factor for depression, although sleep disturbance is also a symptom of depression and a well-known prodromal symptom.5 Furthermore, there have been some studies on sleep reactivity, which is defined as a tendency to provoke sleep disturbance in response to a variety of stressors or challenges to the sleep system, including environmental factors, such as caffeine intake and a change in bedtime or sleep environment.6–9 It was suggested that sleep reactivity is associated with genetic factors, a family history of insomnia, being female, and environmental stress.7,9,10 Furthermore, some studies indicated that sleep disturbance mediates the effect of sleep reactivity on depressive symptoms, whereas sleep reactivity negatively affects depressive symptoms, independently of sleep disturbance.6,8 Furthermore, an interaction between sleep reactivity and sleep disturbance on depressive symptoms has been reported.8
Most previous studies to date have investigated the risk factors for developing mental illnesses. However, in recent years, resilience (the ability to thrive in the face of adversity) has been gaining attention as a factor that acts against stress, and hence facilitates the recovery from mental illness.11 Recent studies have suggested the possibility that an enhancement of resilience leads to an improvement in depressive symptoms and the prevention of depression.12,13 Other studies have analyzed the association between resilience and sleep disturbance. A prospective study on adolescents reported that daytime dysfunction and sleep disturbance were bidirectionally associated with resilience, and that people with higher resilience had fewer sleep disturbances and shorter sleep latencies.14 In addition, a study of community-dwelling adults suggested that subjective stress is a risk factor for sleep disturbance, and resilience plays a protective role against sleep disturbance.15 Furthermore, this study reported an interactive effect between subjective stress and resilience, and resilience buffered the negative impact of subjective stress on sleep disturbance.15 Another study suggested that sleep disturbance and low resilience are associated with high sleep reactivity related to stress.16 Zhou et al analyzed first-year college students, and found that sleep quality might mediate the association between chronotype and depressive symptoms, and resilience might buffer the exacerbating effects of chronotype and sleep quality on depressive symptoms.17 Considering their findings, sleep and resilience are assumed to interact with each other, and furthermore, this interaction may influence depression.
However, to the best of our knowledge, the interaction between sleep disturbance, sleep reactivity, and resilience on depressive symptoms has not been reported to date. Therefore, we hypothesized that sleep disturbance, sleep reactivity, and resilience interact with each other, and furthermore, that these interactions are associated with depressive symptoms. In this study, we hence aimed to test this hypothesis using hierarchical multiple regression analyses including interaction terms.
Subjects and Methods
Subjects
This study was performed in accordance with the Declaration of Helsinki (amended in Fortaleza in 2013) and was approved by the Institutional Review Board of Tokyo Medical University (study approval number: SH3502). Self-administered paper-based questionnaires were distributed to 1237 nonclinical adult volunteers recruited by convenience sampling through our acquaintances at Tokyo Medical University, between April 2017 and April 2018. All subjects reported that they have no severe suicidal ideations, no organic brain diseases, no severe physical illnesses, and the ability to consent to participating in our study. All subjects were informed that their participation was voluntary, no disadvantage would be caused to people who did not participate, and their anonymity would be guaranteed. Participation was incentivized with gift cards worth 500 Japanese yen. A total of 597 subjects gave informed consent and responded to the questionnaire. After excluding 13 subjects with missing data, the data of a total of 584 subjects were analyzed. The mean age of the subjects was 41.7 ± 12.1 years, and 249 (42.6%) of them were men. Details of the demographic characteristics of the subjects are shown in Table 1.
 |
Table 1 Associations Between PHQ-9 Score and Demographic Characteristics, PSQI-J, FIRST-J, and CD-RISC Scores |
Questionnaires
Patient Health Questionnaire-9 (PHQ-9)
PHQ-9 is a self-administered questionnaire for assessing depressive symptoms.18 The Japanese version of PHQ-9 was developed previously, and its validity and reliability have been confirmed.19 PHQ-9 consists of 9 items (eg, “I am feeling down, depressed, or hopeless.”), and each item is evaluated using a 4-point Likert scale (not at all [0 points], to nearly every day [4 points]), and a higher total score is interpreted as indicating severe depressive symptoms. The Cronbach’s α calculated for PHQ-9 in this study was 0.85. PHQ-9 scores were compared between the depressed outpatients in our previous study20 and the subjects used in this study, using a two-sample t-test, and a significant difference between the 2 groups was confirmed (data not shown).
Connor-Davidson Resilience Scale (CD-RISC)
CD-RISC is a self-administered questionnaire that assesses the resilience of a subject.11 The Japanese version of this scale has been developed, and its validity and reliability have been confirmed.21 CD-RISC consists of 25 items (eg, “I am able to adapt to change.”), and each item is evaluated using a 4-point Likert scale (not true at all [0 points], to true nearly all of the time [4 points]). A higher total score is interpreted as indicating higher resilience. The Cronbach’s α calculated for CD-RISC in this study was 0.95.
Pittsburgh Sleep Quality Index Japanese Version (PSQI-J)
PSQI is a self-administered questionnaire that assesses a subject’s sleep disturbance, and its validity and reliability have been confirmed.22 PSQI consists of 7 subscales (C1: sleep quality; eg, “during the past month, how would you rate your sleep quality overall?”, C2: sleep latency; eg, “during the past month, how long did it usually take you to fall asleep each night?”, C3: sleep duration; eg, “during the past month, how many hours of actual sleep did you get each night?”, C4: habitual sleep efficiency (calculated based on the numbers of hours slept and spent in bed), C5: sleep disturbance; eg, “during the past month, how often have you had trouble sleeping because you wake up in the middle of the night or early morning?”, C6: use of sleeping medication; eg, “during the past month, how often have you taken medicine to help you sleep?”, and C7: daytime dysfunction; eg, “during the past month, how often have you had trouble staying awake while driving, eating meals, or engaging in social activities?”). The range of each subscale score is from 0 to 3, and hence the range of the global score (total score) is from 0 to 21. A higher global score represents poorer subjective sleep quality.22 PSQI was translated into a Japanese version (PSQI-J) and then validated by its back translation.23 PSQI-J was used for the psychometric assessment of subjective sleep quality in groups with and without psychiatric illnesses.24 In the present study, the Cronbach’s α calculated for PSQI-J was 0.64.
Ford Insomnia Response to Stress Test Japanese Version (FIRST-J)
FIRST is a self-administered questionnaire for evaluating sleep vulnerability induced by stress.25 Its Japanese version (FIRST-J) was developed previously, and its validity and reliability have been confirmed.26 FIRST-J consists of 9 questions (eg, “when you experience the following situations, how likely is it for you to have difficulty sleeping?” “before an important meeting the next day”, etc.), and each item is evaluated using a 4-point Likert scale (not likely [1 point], to very likely [4 points]). The total score hence ranges from 9 to 36 points, and a higher total score is associated with higher vulnerability to insomnia. The Cronbach’s α of FIRST-J was 0.90 in this study.
Statistical Analysis
Statistical analyses were conducted using SPSS version 27 (IBM, Armonk, NY, USA), and a p-value of less than 0.05 was judged as statistically significant.
Pearson Correlation Analysis and t-Test
The associations of PHQ-9 scores with the scores of PSQI-J, CD-RISC, FIRST-J, and demographic and clinical characteristics (sex, age, marriage status, year of education, subjective social status score [1: lowest; 10: highest], past history of psychiatric illness, present psychiatric illness, and family history of psychiatric illness) were analyzed using Pearson correlation analysis or the t-test. Furthermore, the association between PHQ-9 total score and each PSQI-J subscale score was analyzed using Pearson correlation analysis.
Hierarchical Multiple Regression Analysis
Before hierarchical multiple regression analysis, to clarify whether PSQI-J scores and FIRST-J scores are independently associated with PHQ-9 scores, multiple regression analysis, in which PSQI-J scores and FIRST-J scores were independent variables, and PHQ-9 scores were a dependent variable, was conducted.
Previously, we reported that affective temperaments, which are personality traits, significantly interact with insomnia on depressive symptoms in Japanese adult community volunteers.27 Considering this interaction on depressive symptoms, in this study, we aimed to assess the effect of the interaction of resilience with sleep disturbance or sleep reactivity on depressive symptoms. In previous studies, the interaction of 2 variables was judged using a moderated regression framework.27,28 The equation for the hypothetical model was as follows:29 dependent factor (PHQ-9 scores) = b0 + b1 (factor 1) + b2 (factor 2) + b3 (factor 1*factor 2), in which b0 is the intercept, b1 is the coefficient associated with the effect of factor 1, b2 is the coefficient associated with the effect of factor 2, and b3 is the coefficient associated with the interaction effect, which is the product of the 2 variables (factor 1 and factor 2). A 3-step hierarchical multiple regression analysis was conducted by the forced entry method, using PHQ-9 scores as a dependent variable, and PSQI-J global scores, CD-RISC scores, interaction term (PSQI-J × CD-RISC), and demographic and clinical characteristics (described below) as independent variables. In step 1, PSQI-J global scores and CD-RISC scores were included as independent variables. In step 2, the interaction term between these 2 variables was added as an independent variable. In step 3, age, sex, marriage status, years of education, subjective social status, past history of psychiatric illness, present psychiatric illness, and family history of psychiatric illness were added as independent variables. Furthermore, sensitivity analysis, considering the possibility that the scores of the item regarding sleep disturbance on the PHQ-9 might be associated with the scores of PSQI-J, which might affect the results, was also performed. In this sensitivity analysis, the scores that were obtained after excluding the score of the item regarding sleep disturbance of the PHQ-9 (ie, the total scores of 8 items of the PHQ-9) were used as a dependent variable. Moreover, hierarchical multiple regression analyses using the PSQI-J subscale scores as independent variables were performed, in the same way as the PSQI-J total scores.
In another set of 3-step hierarchical multiple regression analysis, PHQ-9 scores were included as the dependent variable, and FIRST-J scores, CD-RISC scores, interaction term (FIRST-J × CD-RISC), and demographic and clinical characteristics (described above) were included as independent variables. Analytical procedures were conducted as above.
The adjusted coefficient of determination (R2), which represents the explanatory power of the model formula in each step was calculated, and the statistical significance of the difference of R2 between each step was analyzed. To analyze interaction effects, the scores of PSQI-J, CD-RISC, and FIRST-J were standardized before the analyses.
Results
Demographic and Clinical Characteristics and Scores of PSQI-J (Sleep Disturbance), FIRST-J (Sleep Reactivity), CD-RISC (Resilience), and PHQ-9 (Depressive Symptoms)
The associations of PHQ-9 scores with demographic and clinical characteristics and PSQI-J, FIRST-J, and CD-RISC scores of the subjects are shown in Table 1. As determined by the t-test, being female, unmarried, past history of psychiatric illnesses, and present psychiatric illness were significantly associated with a high score on the PHQ-9. On the other hand, family history of psychiatric illness was not significantly associated with PHQ-9 score. As determined by the Pearson correlation coefficient, subjective social status and CD-RISC score were significantly and negatively correlated with PHQ-9 score, whereas PSQI-J global and FIRST-J scores were significantly and positively correlated with PHQ-9 score. However, age and years of education were not significantly correlated with PHQ-9 score. Furthermore, all subscale scores on the PSQI-J (C1, C2, C3, C4, C5, C6, and C7) were significantly and positively associated with PHQ-9 score (data not shown).
Hierarchical Multiple Regression Analysis
We performed multiple regression analysis before the hierarchical multiple regression analysis to confirm that PSQI-J global and FIRST-J scores were independently associated with PHQ-9 score. The multiple regression analysis, with the dependent variable being PHQ-9 scores, included PSQI-J and FIRST-J scores as independent variables. PSQI-J global and FIRST-J scores were significantly and independently associated with PHQ-9 scores (adjusted R2 = 0.352, F (2545) = 155.957, p < 0.001; PSQI-J global score, standardized partial regression coefficient β = 0.473, p < 0001; FIRST-J score, β = 0.230, p < 0.001). The variance inflation factor was 1.188, and multicollinearity was denied.
The results of hierarchical multiple regression analyses including PSQI-J global scores and FIRST-J scores as independent variables are shown in Tables 2 and 3, respectively. In steps 1, 2, and 3, PSQI-J global and FIRST-J scores were significantly positively associated with PHQ-9 scores, whereas CD-RISC scores were significantly negatively associated with PHQ-9 scores. Additionally, in steps 2 and 3, the interaction terms of CD-RISC with PSQI-J global and FIRST-J scores were significantly negatively associated with PHQ-9 scores. Furthermore, in step 2 of the model including PSQI-J scores as an independent variable, the adjusted R2 was 0.400, which indicated that 40.0% of the variance in PHQ-9 scores was explained by the model (Table 2). Additionally, in step 2 of the model including FIRST-J scores as an independent variable, the adjusted R2 was 0.261, which indicated that 26.1% of the variance in PHQ-9 was explained by the model (Table 3).
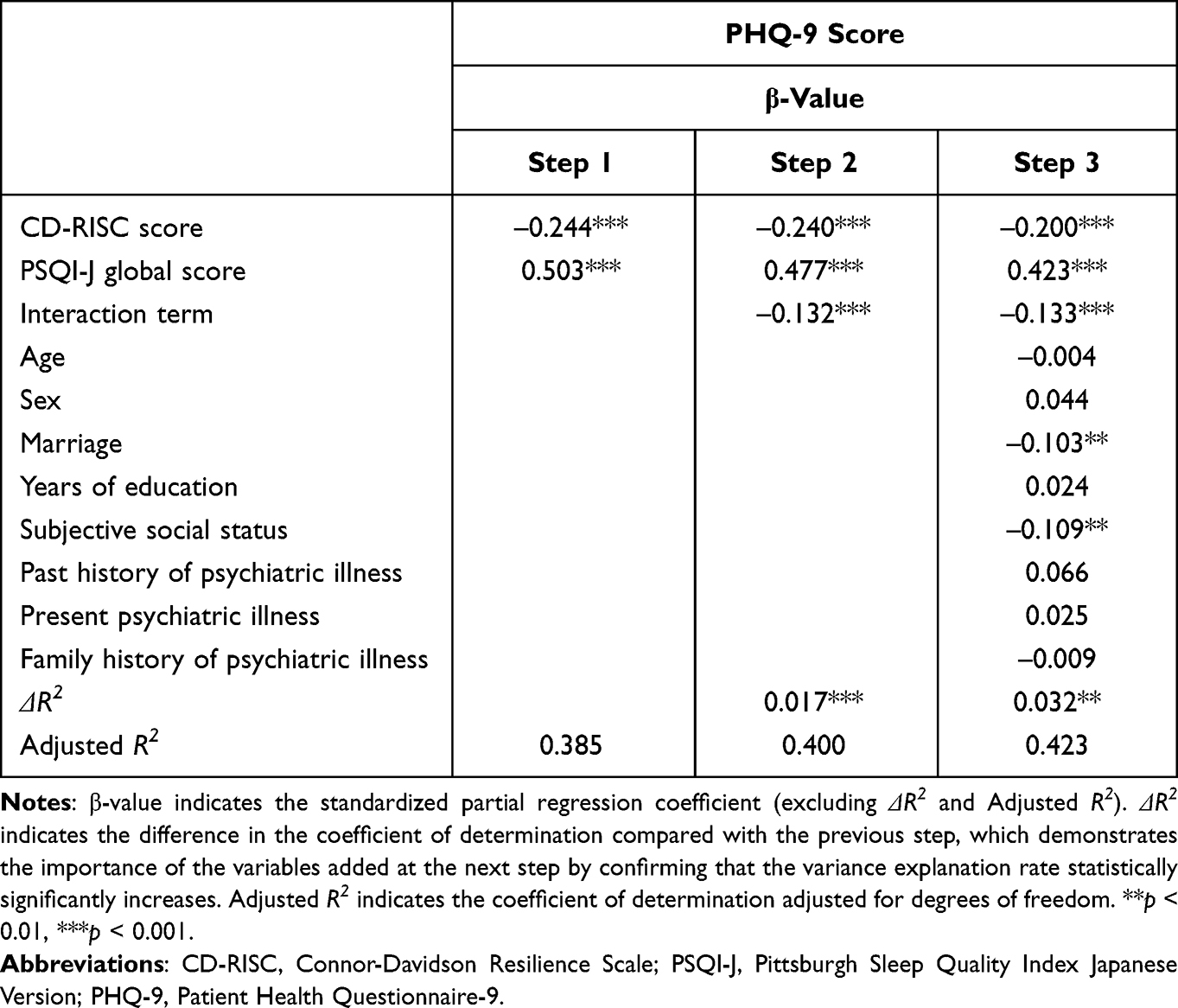 |
Table 2 Analysis of Interactions by Hierarchical Multiple Regression Analysis of PSQI-J, CD-RISC, and PHQ-9 Scores |
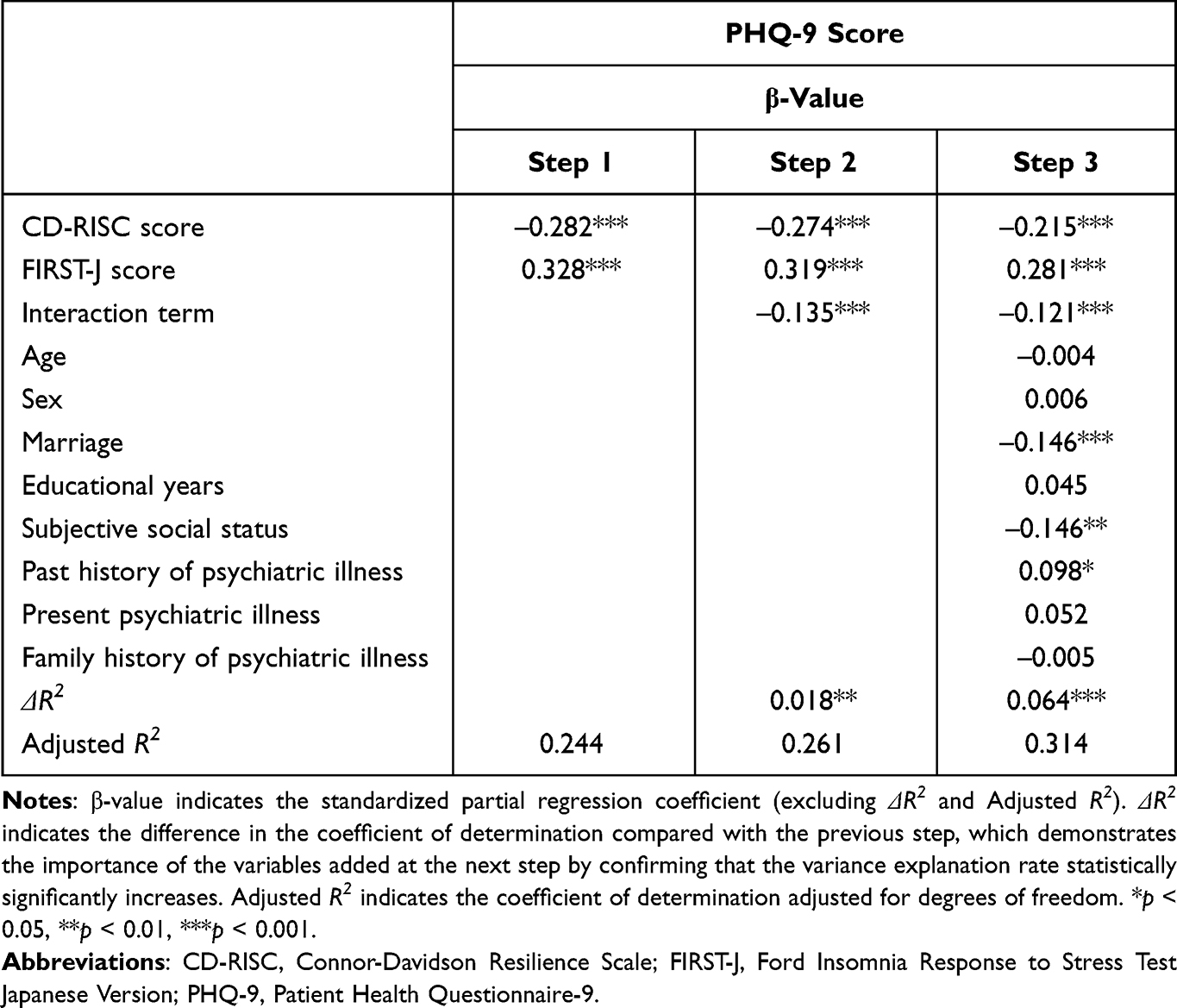 |
Table 3 Analysis of Interactions by Hierarchical Multiple Regression Analysis of FIRST-J, CD-RISC, and PHQ-9 Scores |
In the sensitivity analysis of total scores of 8 items on PHQ-9, which were obtained after excluding the item regarding sleep disturbance, PSQI-J global and FIRST-J scores were significantly positively associated with PHQ-9, whereas CD-RISC scores were significantly negatively associated with PHQ-9 in steps 1, 2, and 3 (data not shown). Additionally, in steps 2 and 3, the interaction terms of CD-RISC scores with PSQI-J global and FIRST-J scores were significantly negatively associated with PHQ-9 scores, respectively (data not shown). The variance inflation factors in these models were calculated, and multicollinearity was denied.
In the hierarchical multiple regression analyses using the subscale scores of PSQI-J as independent variables, the interaction terms between 5 PSQI-J subscores (C1: sleep quality, C2: sleep latency, C5: sleep disturbance, C6: use of sleeping medication, and C7: daytime dysfunction) and CD-RISC scores were significantly negatively associated with PHQ-9 scores, whereas the interaction terms between 2 PSQI-J subscores (C3: sleep duration, and C4: habitual sleep efficiency) and CD-RISC scores were not significantly associated with PHQ-9 scores (data not shown). We confirmed no multicollinearity between the subscale scores of PSQI-J and CD-RISC scores.
Discussion
In this study, we showed that sleep reactivity and sleep disturbance are significantly associated with depressive symptoms, and that these factors explain about one-third of the variance of depressive symptoms in Japanese adult volunteers. Furthermore, resilience was significantly negatively associated with depressive symptoms. Moreover, resilience was found to interact with sleep reactivity and sleep disturbance, and buffer the exacerbating effects of sleep reactivity and sleep disturbance on depressive symptoms. The above results were also found to be significant by sensitivity analyses. To the best of our knowledge, this is the first study to date to report the interaction effects of resilience with sleep reactivity and sleep disturbance on depressive symptoms.
As mentioned in the Introduction section, there have been some studies regarding the association of depressive symptoms with sleep disturbance and sleep reactivity. Some studies reported that sleep reactivity or sleep disturbance is associated with depressive symptoms.4,6,8,30,31 Our present findings are consistent with the results of these previous studies, suggesting that sleep reactivity and sleep disturbance are closely associated with depressive symptoms in Japanese adult volunteers, and that the intervention of improving sleep disturbance and sleep reactivity is important for the prevention and treatment of depression.
Furthermore, previous studies have shown that resilience is useful for the improvement of depressive symptoms, which is consistent with our present findings.12,13 It has also been reported that resilience may be affected by various factors, such as psychosocial and biological factors.11,32 In this study, resilience was significantly associated with sex, marriage status, subjective social status, and past history of psychiatric illness (data not shown). After adjustment for these factors in the hierarchical multiple regression analysis, the association of resilience with depressive symptoms remained significant. In other words, the present analyses confirmed that resilience was associated with depressive symptoms independently of other relevant factors.
In this study, we showed that sleep reactivity and sleep disturbance interact with resilience on depressive symptoms; ie, resilience moderates the effects of sleep reactivity and sleep disturbance on depressive symptoms. These findings suggest that interventions of improving resilience may be useful for improving depressive symptoms in people with sleep reactivity and sleep disturbance. As mentioned in the Introduction section, Zhou et al reported that resilience might moderate the effects of chronotype and sleep quality on depressive symptoms in the first-year college students,17 which supported the moderator effect of resilience in the present study. In the analysis of the interactions between the 7 PSQI-J subscores and resilience scores, resilience buffered the aggravating effects of subjective sleep quality, sleep latency, sleep disturbance, use of sleeping medication, and daytime dysfunction on depressive symptoms. There was, however, no significant interactions of resilience with sleep duration and habitual sleep efficiency, which suggested that the association with resilience is different for each PSQI-J subscale. There have been no reports on the interactions between the subscales of PSQI-J and resilience, but a report showed that daytime dysfunction and sleep disturbance were associated bidirectionally with resilience, which partially supports our present findings.14
The results of the present study provide some clinical implications. It is important to evaluate resilience in subjects with sleep reactivity and sleep disturbance. Our results suggest that people with lower resilience are likely to develop depression associated with sleep reactivity and sleep disturbance. When a patient’s resilience is considered to be low, interventions to enhance his/her resilience are expected to prevent or ameliorate the worsening effect of sleep reactivity and sleep disturbance on depressive symptoms. For example, meta-analyses have shown that cognitive behavioral therapy (cognitive reconstruction, behavioral activation, problem-solving, and social skills training) enhances resilience.13,33 Additionally, some reports suggested that exercise is likely to enhance resilience.34,35 Treatment with antidepressants was suggested to enhance resilience in patients with posttraumatic stress disorder.36 Furthermore, the amelioration of sleep reactivity and sleep disturbance may lead to buffering of the exacerbation of depressive symptoms induced by low resilience.
Limitations
The present study is a cross-sectional study, which cannot conclude the causal associations of sleep disturbance, sleep reactivity, and resilience with depressive symptoms. To confirm these causal associations, a long-term prospective longitudinal study is required. Moreover, the present findings cannot be generalized to patients with depression because the study subjects were non-clinical adult volunteers. Furthermore, sleep disturbance was evaluated subjectively in the present study, and hence further studies are necessary to assess the interaction between resilience and sleep disturbance based on objective data.
Conclusion
Our results suggest that resilience interacts with sleep reactivity and sleep disturbance, and resilience has a moderator effect that buffers the exacerbating effects of sleep reactivity and sleep disturbance on depressive symptoms. Therefore, the enhancement of resilience might lead to the amelioration of depressive symptoms associated with sleep disturbance and sleep reactivity. Our present findings are expected to lead to the future development of treatment strategies for depression focusing on resilience.
Acknowledgments
We thank Dr. Nobutada Takahashi of Fuji Psychosomatic Rehabilitation Institute Hospital, Dr. Hiroshi Matsuda of Kashiwazaki Kosei Hospital, Dr. Yasuhiko Takita (deceased) of Maruyamasou Hospital, and Dr. Yoshihide Takaesu of Izumi Hospital for their collection of subject data. We thank Dr. Helena Popiel of the Department of International Medical Communications, Tokyo Medical University, for editorial review of the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Jiro Masuya has received personal compensation from Otsuka Pharmaceutical, Eli Lilly, Astellas, and Meiji Yasuda Mental Health Foundation, and grants from Pfizer. Akiyoshi Shimura has received personal compensation from Dainippon Sumitomo Pharma, Yoshitomiyakuhin, Meiji Seika Pharma, and Eisai. Takeshi Inoue has received personal compensation from Mochida Pharmaceutical, Takeda Pharmaceutical, Eli Lilly, Janssen Pharmaceutical, MSD, Taisho Toyama Pharmaceutical, Yoshitomiyakuhin, and Daiichi Sankyo; grants from Shionogi, Astellas, Tsumura, and Eisai; and grants and personal compensation from Otsuka Pharmaceutical, Dainippon Sumitomo Pharma, Mitsubishi Tanabe Pharma, Kyowa Pharmaceutical Industry, Pfizer, Novartis Pharma, and Meiji Seika Pharma; and is a member of the advisory boards of Pfizer, Novartis Pharma, and Mitsubishi Tanabe Pharma. Yota Fujimura has received research and grant support from Novartis Pharma, Otsuka Pharmaceutical, Astellas, Dainippon Sumitomo Pharma, and Shionogi. The other authors declare that they have no actual or potential conflicts of interest associated with this study.
References
1. Bromet E, Andrade LH, Hwang I, et al. Cross-national epidemiology of DSM-IV major depressive episode. BMC Med. 2011;9:90. doi:10.1186/1741-7015-9-90
2. Malhi GS, Mann JJ. Depression. Lancet. 2018;392(10161):2299–2312. doi:10.1016/S0140-6736(18)31948-2
3. Baglioni C, Battagliese G, Feige B, et al. Insomnia as a predictor of depression: a meta-analytic evaluation of longitudinal epidemiological studies. J Affect Disord. 2011;135(1–3):10–19. doi:10.1016/j.jad.2011.01.011
4. Kalmbach DA, Arnedt JT, Song PX, Guille C, Sen S. Sleep disturbance and short sleep as risk factors for depression and perceived medical errors in first-year residents. Sleep. 2017;40(3):zsw073. doi:10.1093/sleep/zsw073
5. Perlis ML, Giles DE, Buysse DJ, Tu X, Kupfer DJ. Self-reported sleep disturbance as a prodromal symptom in recurrent depression. J Affect Disord. 1997;42(2–3):209–212. doi:10.1016/S0165-0327(96)01411-5
6. Drake CL, Pillai V, Roth T. Stress and sleep reactivity: a prospective investigation of the stress-diathesis model of insomnia. Sleep. 2014;37(8):1295–1304. doi:10.5665/sleep.3916
7. Fernandez-Mendoza J. Evidence for the etiopathogenesis of insomnia and its psychiatric risk. Sleep. 2014;37(8):1273–1275. doi:10.5665/sleep.3906
8. Nakajima S, Komada Y, Sasai-Sakuma T, et al. Higher sleep reactivity and insomnia mutually aggravate depressive symptoms: a cross-sectional epidemiological study in Japan. Sleep Med. 2017;33:130–133. doi:10.1016/j.sleep.2016.12.023
9. Kalmbach DA, Anderson JR, Drake CL. The impact of stress on sleep: pathogenic sleep reactivity as a vulnerability to insomnia and circadian disorders. J Sleep Res. 2018;27(6):e12710. doi:10.1111/jsr.12710
10. Riemann D, Spiegelhalder K, Feige B, et al. The hyperarousal model of insomnia: a review of the concept and its evidence. Sleep Med Rev. 2010;14(1):19–31. doi:10.1016/j.smrv.2009.04.002
11. Connor KM, Davidson JR. Development of a new resilience scale: the Connor-Davidson Resilience Scale (CD-RISC). Depress Anxiety. 2003;18(2):76–82. doi:10.1002/da.10113
12. Kermott CA, Johnson RE, Sood R, Jenkins SM, Sood A. Is higher resilience predictive of lower stress and better mental health among corporate executives? PLoS One. 2019;14(6):e0218092. doi:10.1371/journal.pone.0218092
13. Ma L, Zhang Y, Huang C, Cui Z. Resilience-oriented cognitive behavioral interventions for depressive symptoms in children and adolescents: a meta-analytic review. J Affect Disord. 2020;270:150–164. doi:10.1016/j.jad.2020.03.051
14. Wang J, Zhang X, Simons SR, Sun J, Shao D, Cao F. Exploring the bi-directional relationship between sleep and resilience in adolescence. Sleep Med. 2020;73:63–69. doi:10.1016/j.sleep.2020.04.018
15. Liu X, Liu C, Tian X, et al. Associations of perceived stress, resilience and social support with sleep disturbance among community-dwelling adults. Stress Health. 2016;32(5):578–586. doi:10.1002/smi.2664
16. Palagini L, Moretto U, Novi M, et al. Lack of resilience is related to stress-related sleep reactivity, hyperarousal, and emotion dysregulation in insomnia disorder. J Clin Sleep Med. 2018;14(5):759–766. doi:10.5664/jcsm.7100
17. Zhou J, Hsiao FC, Shi X, et al. Chronotype and depressive symptoms: a moderated mediation model of sleep quality and resilience in the 1st-year college students. J Clin Psychol. 2021;77(1):340–355. doi:10.1002/jclp.23037
18. Spitzer RL, Kroenke K, Williams JB. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. JAMA. 1999;282(18):1737–1744. doi:10.1001/jama.282.18.1737
19. Muramatsu K, Miyaoka H, Kamijima K, et al. The patient health questionnaire, Japanese version: validity according to the mini-international neuropsychiatric interview-plus. Psychol Rep. 2007;101(3Pt1):952–960. doi:10.2466/pr0.101.3.952-960
20. Toda H, Inoue T, Tsunoda T, et al. Affective temperaments play an important role in the relationship between childhood abuse and depressive symptoms in major depressive disorder. Psychiatry Res. 2016;236:142–147. doi:10.1016/j.psychres.2015.12.016
21. Nakajima S, Kim Y, Konishi T, Ito M, Sirai A. Reliability and validity of Japanese version of the Connor-Davidson resilience scale. The Ministry of Health Labour and Welfare sponsored grant for Research on the actual situation of psychiatric illnesses caused by large-scale disasters and crime damage and the development of intervention methods, FY 2009 report (in Japanese); 2010:93–97.
22. Buysse DJ, Reynolds CF, Monk TH, Berman SR, Kupfer DJ. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
23. Doi Y, Minowa M, Okawa M, Uchiyama M. Development of the Japanese version of the Pittsburgh Sleep Quality Index (in Japanese). Jpn J Psychiatr Treat. 1998;13(6):755–763.
24. Doi Y, Minowa M, Uchiyama M, et al. Psychometric assessment of subjective sleep quality using the Japanese version of the Pittsburgh Sleep Quality Index (PSQI-J) in psychiatric disordered and control subjects. Psychiatry Res. 2000;97(2–3):165–172. doi:10.1016/S0165-1781(00)00232-8
25. Drake C, Richardson G, Roehrs T, Scofield H, Roth T. Vulnerability to stress-related sleep disturbance and hyperarousal. Sleep. 2004;27(2):285–291. doi:10.1093/sleep/27.2.285
26. Nakajima S, Okajima I, Sasai T, et al. Validation of the Japanese version of the Ford Insomnia Response to Stress Test and the association of sleep reactivity with trait anxiety and insomnia. Sleep Med. 2014;15(2):196–202. doi:10.1016/j.sleep.2013.09.022
27. Toyoshima K, Inoue T, Masuya J, Fujimura Y, Higashi S, Kusumi I. Affective temperaments moderate the effect of insomnia on depressive symptoms in adult community volunteers. J Affect Disord. 2021;282:726–731. doi:10.1016/j.jad.2020.12.138
28. Nakai Y, Inoue T, Chen C, et al. The moderator effects of affective temperaments, childhood abuse and adult stressful life events on depressive symptoms in the nonclinical general adult population. J Affect Disord. 2015;187:203–210. doi:10.1016/j.jad.2015.08.011
29. Caspi A, Sugden K, Moffitt TE, et al. Influence of life stress on depression: moderation by a polymorphism in the 5-HTT gene. Science. 2003;301(5631):386–389. doi:10.1126/science.1083968
30. Fang H, Tu S, Sheng J, Shao A. Depression in sleep disturbance: a review on a bidirectional relationship, mechanisms and treatment. J Cell Mol Med. 2019;23(4):2324–2332. doi:10.1111/jcmm.14170
31. Srinivasan V, Pandi-Perumal SR, Trakht I, et al. Pathophysiology of depression: role of sleep and the melatonergic system. Psychiatry Res. 2009;165(3):201–214. doi:10.1016/j.psychres.2007.11.020
32. Fritz J, de Graaff AM, Caisley H, van Harmelen AL, Wilkinson PO. A systematic review of amenable resilience factors that moderate and/or mediate the relationship between childhood adversity and mental health in young people. Front Psychiatry. 2018;9:230. doi:10.3389/fpsyt.2018.00230
33. Liu H, Zhang C, Ji Y, Yang L. Biological and psychological perspectives of resilience: is it possible to improve stress resistance? Front Hum Neurosci. 2018;12:326. doi:10.3389/fnhum.2018.00326
34. Childs E, de Wit H. Regular exercise is associated with emotional resilience to acute stress in healthy adults. Front Physiol. 2014;5:161. doi:10.3389/fphys.2014.00161
35. Holmes PV. Trophic mechanisms for exercise-induced stress resilience: potential role of interactions between BDNF and galanin. Front Psychiatry. 2014;5:90.
36. Davidson JR, Payne VM, Connor KM, et al. Trauma, resilience and saliostasis: effects of treatment in post-traumatic stress disorder. Int Clin Psychopharmacol. 2005;20(1):43–48. doi:10.1097/00004850-200501000-00009
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Narrative Review of Research on Adjustment to Spinal Cord Injury and Mental Health: Gaps, Future Directions, and Practice Recommendations
Sandalic D, Arora M, Pozzato I, Simpson G, Middleton J, Craig A
Psychology Research and Behavior Management 2022, 15:1997-2010
Published Date: 5 August 2022
Psychological Disturbances and Their Association with Sleep Disturbance in Patients Admitted for Arrhythmia Diseases
Hu LX, Tang M, Hua W, Ren XQ, Jia YH, Chu JM, Zhang JT, Liu XN
Neuropsychiatric Disease and Treatment 2022, 18:1739-1750
Published Date: 17 August 2022
Resilience and Depressive Symptoms Mediated Pathways from Social Support to Suicidal Ideation Among Undergraduates During the COVID-19 Campus Lockdown in China
Zhang X, Liu X, Mi Y, Wang W, Xu H
Psychology Research and Behavior Management 2022, 15:2291-2301
Published Date: 23 August 2022
Relationships Among Trajectories of Sleep Disturbance, Depression, and Antiretroviral Therapy in Persons Newly Diagnosed with HIV: A One-and-a-Half-Year Observational Longitudinal Study
Chen CC, Liu HY, Chen YC, Ko NY
Nature and Science of Sleep 2022, 14:2133-2142
Published Date: 2 December 2022
The Mediating Effect of Resilience on the Relationship Between Symptom Burden and Anxiety/Depression Among Chinese Patients with Primary Liver Cancer After Liver Resection
Zhang X, Zhang H, Zhang Z, Fan H, Li S
Patient Preference and Adherence 2023, 17:3033-3043
Published Date: 20 November 2023