Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Sleep Quality Among People with Type 2 Diabetes Mellitus During COVID-19 Pandemic: Evidence from Qatar’s National Diabetes Center
Authors Abdu Y ![]() , Naja S, Mohamed Ibrahim MI
, Naja S, Mohamed Ibrahim MI ![]() , Abdou M, Ahmed R, Elhag S, Saleh AO, Yassin M
, Abdou M, Ahmed R, Elhag S, Saleh AO, Yassin M ![]() , Bougmiza I
, Bougmiza I
Received 18 May 2023
Accepted for publication 23 August 2023
Published 14 September 2023 Volume 2023:16 Pages 2803—2812
DOI https://doi.org/10.2147/DMSO.S421878
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Konstantinos Tziomalos
Yasamin Abdu,1 Sarah Naja,1 Mohamed Izham Mohamed Ibrahim,2 Mariam Abdou,1 Romaisa Ahmed,3 Salma Elhag,4 Ahmed O Saleh,5 Mohamed Yassin,6 Iheb Bougmiza7,8
1Community Medicine Department, Hamad Medical Corporation, Doha, Qatar; 2College of Pharmacy, QU Health, Qatar University, Doha, Qatar; 3University of Elimam Almahadi, Khartoum, Sudan; 4Wad Medani College of Medical Sciences and Technology, Jazeera, Sudan; 5Department of Internal Medicine, Unity Hospital, Rochester, NY, USA; 6Hematology Department, Hamad Medical Corporation, Doha, Qatar; 7Community Medicine Department, Primary Health Care Corporation, Doha, Qatar; 8Community Medicine Department, College of Medicine, Sousse University, Sousse, Tunisia
Correspondence: Yasamin Abdu, Community Medicine Department, Hamad Medical Corporation, P.O. Box 3050, Doha, Qatar, Tel + 97466900210, Email [email protected]; [email protected]
Purpose: Sleep disturbance is suspected to increase during the COVID-19 pandemic, and people with type 2 DM are known to have a higher risk of sleep disturbance. We aimed to determine the prevalence and determinants of sleep disturbance through Pittsburgh Sleep Quality Index (PSQI) during the COVID-19 pandemic.
Patients and Methods: We randomly selected two hundred eighty-eight people with T2DM from the outpatient clinics of the National Diabetes Centre in Qatar. We used Chi-square, Mann–Whitney, Spearman, and Point Biserial correlation tests to examine the association between sleep quality and the independent variables. Finally, we conducted multiple logistics regression to identify the predictors of poor sleep quality and set the alpha level at 0.05.
Results: In our sample, the mean age (±SD) was 51.4 (± 9.5) years, and 64.3% of the study participants were males. The median (IQR) duration of diabetes was 10 (11) years. Additionally, 6.3% of the participants were on insulin. The median HbA1c was 7.6% (2.4). Three in ten patients reported poor sleep quality (PSQI> 5); (n=103; 35.8%). Poor sleep quality was statistically associated with young age, previous history of sleep disturbance, prior diagnosis of sleep disorders, high depression score, and high perceived stress score. After adjusting for confounders, only high depressive symptoms score and previous history of sleep disorder were significant predictors of poor sleep quality (p < 0.001), with adjusted odd ratios of (aOR = 1.421; 95% CI: 1.242– 1.625) and (aOR = 3.208; 95% CI: 1.574– 6.537), respectively.
Conclusion: The prevalence of poor sleep quality among people with T2DM during the COVID-19 pandemic is high. Physicians must screen for depression, stress, and previous history of sleep disorder to tackle poor sleep among T2DM.
Keywords: poor sleep quality, sleep disturbance, T2DM, COVID-19, depression
Introduction
Part of the crucial human well-being pillars is good sleep hygiene, which includes adequate duration, appropriate timing, good quality, and lack of sleep disturbances.1,2
Sleep disorder prevalence is around 20% in the general population (insomnia 6–15%, restless leg syndrome affects 6%, sleep paralysis affects about 6%, and sleep apnea affects around 2–4%). However, the prevalence of this disorder is nearly double among people with type 2 Diabetes Mellitus (T2DM).3–5 Where cumulative evidence from thirty-six studies revealed that the prevalence of sleep disorders among people with T2DM is 52%, specifically 69% of people with T2DM suffer from unspecified sleep apnea, and 60% have obstructive sleep apnea.6
Glycemic control is multifactorial; it is affected by low self-care activities,7–10 and psychosocial factors such as stress and depression.11,12 In addition, sleep disorders negatively impact the health of people with T2DM, increasing the risk of nocturia, peripheral neuropathy, fluctuations in blood glucose levels during the night, and depression.13 Specifically, inappropriate sleep time interval (less than 6 hours and more than 9 hours), alterations of sleep duration, chronic sleep restriction, excessive sleep; sleep fragmentation; circadian rhythm disorders and disruption (ie, shift work); and obstructive sleep apnea (OSA) influence glycemic control and provoke complications.14–16
Sleep disturbance, sleep fragmentation, and hypoxia increase sympathetic activity decrease insulin sensitivity and thus increase blood glucose levels.17 Moreover, the frequent arousal episodes caused by respiratory disturbance and the consequent sleep loss may enhance the development of metabolic disorders.18
Sleep disturbance is suspected to increase in stressful conditions such as the spread of the lethal viral infection and lockdown policies, including confinement at home, working from home, and distance learning that increases fear and disrupts the sleep-wake cycle, circadian and homeostatic factors.19
Diabetes is one of the critical non-communicable diseases that affect the population in Qatar. The prevalence of Type 2 Diabetes mellitus among aged 18–64 in 2021 was 10.4%.20
Assessment of sleep quality, sleep disorders, and sleep hygiene has a massive importance in people with T2DM. The latest American Diabetes Association 2023 guidelines21 recommended that assessment of sleep pattern and duration should be a part of the comprehensive medical evaluation in people with T2DM based on emerging evidence about the relationship between sleep quality and glycemic control. Before the pandemic, more than 50% of people withT2DM had excess daytime sleepiness and suffered from low sleep quality.
In Qatar, a study conducted in 200922 showed that 60.1%of T2DM patients had excess daytime sleepiness; however, this study did not investigate the effect of sleep quality on disease control. Another recent study23 assessed sleep quality and its impact on glycemic management using data from Qatar Biobank; however, they studied only the sleep duration part and the daytime napping. To our knowledge, there is no study in Qatar conducted among diabetic patients during COVID-19 to assess the burden of poor sleep quality and the associated factors, as well as its potential impact on glycemic control, using a validated tool with high sensitivity and specificity (PSQI). Our study aimed to fill the gap to inform the policy makers about the prevalence and burden of poor sleep quality among diabetic patients during the pandemic, reflecting on the programs and policies needed at the tertiary health-care level.
Materials and Methods
Study Design and Recruitment
We conducted an analytical cross-sectional study. In addition, we surveyed patients attending the National Diabetes Centre in Hamad General Hospital from January 2021 and June 2022. The National Diabetes Centre is the main center for diabetes in Qatar,24 providing tertiary care through a multidisciplinary team staffed by endocrinologists, retinal specialists, podiatrists, nutritionists, education specialists, nurses, pharmacists, and technicians who all deliver diabetes care.
The National Diabetes Centre receives more than 120,000 visits and over 30,000 people with T2DM annually; it provides health care for the entire registered population, nationals, and expatriates. Specifically, people with T2DM who have outside glucose target and those eligible for T2DM complications screening receive care in this center.
We selected participants randomly from the attendance list using an automated random number generator, a simple random technique. Participants were interviewed after securing written consent. The target population included adult patients (18 years and above) diagnosed with T2DM and able to communicate in Arabic or English. We excluded pregnant women and patients with cognitive impairment that interfered with communication. A written informed consent was obtained from all the study participants. Ethical approval was obtained from the Institutional Review Board (IRB) of Hamad Medical Corporation (MRC-01-21-317).
Sample Size Equation
We utilized the prevalence of poor sleep quality among people with type 2 DM in Qatar prior to the pandemic of 60%,22 with a 5% degree of precision and 95% confidence limits. Accordingly, the minimum sample size of 370 was calculated using the following formula:25
Variables and Measurement Tools
Sleep quality is our dependent variable; it is theoretically defined as the person or individual’s self-satisfaction with all aspects of the sleep experience. Four domains contribute to sleep quality: wake after sleep onset, sleep efficiency, latency, and duration.26
We used the English and Arabic versions of the Pittsburgh Sleep Quality Index (PSQI) to assess sleep. It is a nineteen-item self-rated questionnaire to evaluate sleep quality over the previous month across seven component domains: subjective sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbances, use of sleep medication, and daytime dysfunction. Each component scored from zero to three; the higher the score, the more significant the sleep problem.
The PSQI demonstrated great criterion validity for the English and Arabic versions. A score of five and above indicated poor sleep quality with an acceptable sensitivity (89.6%) and specificity (86.5%). Furthermore, good internal consistency alpha=0.77.27–29
Regarding the independent variables, Personal interviews using the structured questionnaire were conducted with people with T2DM to collect information about sociodemographic and health-related characteristics (the independent variables) such as COVID-19 infection and vaccination status, health habits, comorbidities, diabetes complications, latest Hemoglobin A1C (HbA1C) in the previous 3 months, and lipid profile.
Perceived stress is one of the essential dependent variables that can influence sleep, and it is defined as the degree to which patients appraise situations in their lives as stressful. We utilized the English and Arabic versions of the self-administered Perceived Stress Scale (PSS-4) to assess the perceived stress level.30 The scale consisted of four items and showed acceptable internal validity (alpha=0.8). There is no established cutoff point for (PSS-4), but the higher the perceived stress level.
As for depressive symptoms assessment, we utilized the English and Arabic versions of the Patient Health Questionnaire (PHQ-9). It is a self-administered instrument that is shown to be a good screening tool with 88% sensitivity and 88% specificity for major depression when utilizing a cutoff of 10.31 In addition, the Arabic version of PHQ-9 showed acceptable reliability in a neighbouring country Saudi Arabia (alpha=0.857).32
Analysis
We utilized software package SPSS version v29 (Armonk, NY: IBM Corp) for statistical analysis. Quantitative variables were described in the form of mean and standard deviation, while qualitative variables were presented in the form of frequency and percentage. Inferential statistics, ie, Mann–Whitney, Chi-Square, Spearman correlation, and Point Biserial correlation tests, were used to test the association between sleep quality and the independent variables. In addition, multiple logistic regression was carried out to identify the predictors of poor sleep quality among people with T2DM. The a priori alpha level was set at 0.05.
Results
Sample Size Realization
During the data collection period (January 2021 to June 2022), we approached three hundred seventy people with T2DM and two hundred eighty-eight participants completed the study, with a twenty-two percent non-response rate.
Sociodemographic and Health-Related Characteristics of the Sample
The patients’ mean ± (SD) age was 51 ± (9.5) years. More than 50% of the sample were males and employed. The median (IQR) of the perceived stress score and patient health questionnaire nine score among people with T2DM was 8 (3) and 1 (3), respectively. The duration of T2DM ranged between one and forty-five years, with a median (IQR) of 10 (11). Less than 10% were on insulin (n=15; 6.3%), and one-third of the sample (n=65; 28.3%) were on combined insulin therapy and other antihyperglycemic agents. Most of our patients had blood glucose level above the target (HbA1c >7%) with desirable levels of LDL (3.36–4.11 mmol/L), HDL (>1 mmol/L), and total cholesterol (<5 mmol/L) 63%, 85.5%, 72.7%and 78.2%, respectively. Ten percent of the sample was diagnosed with sleep disturbance before COVID-19, as seen in Table 1.
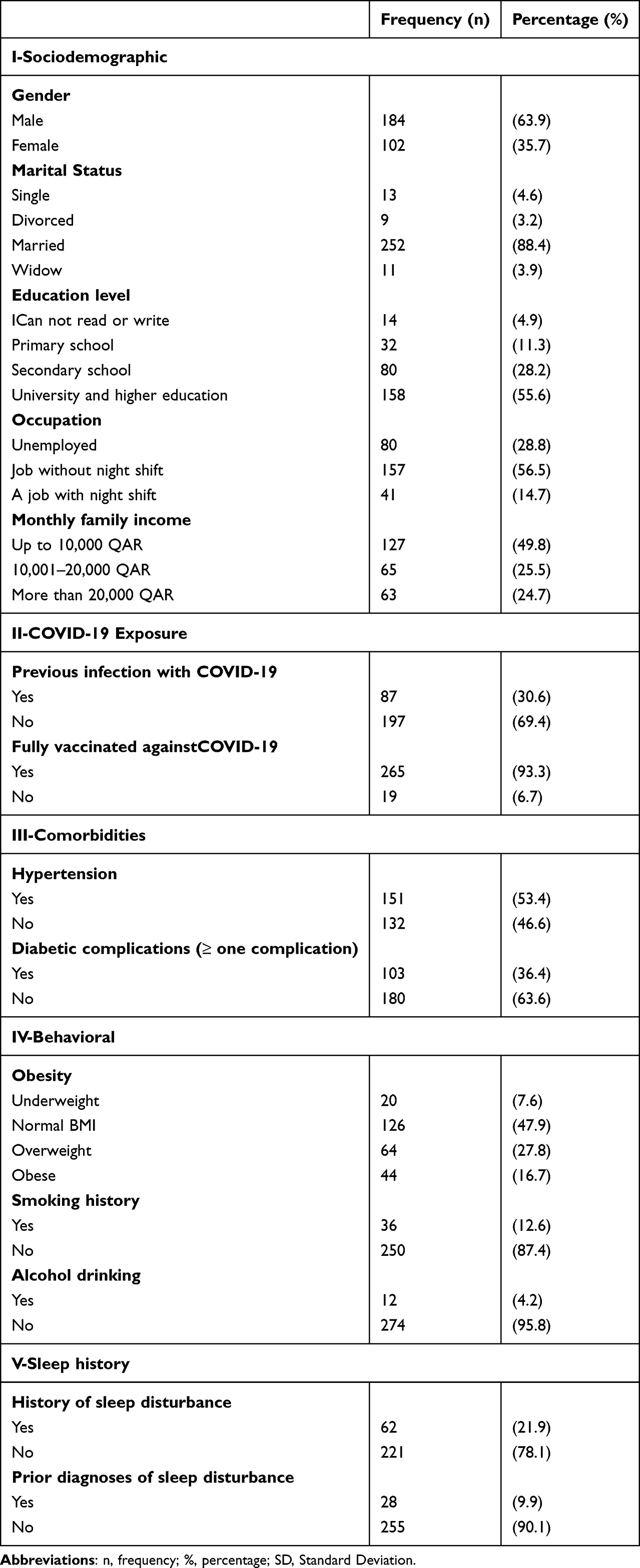 |
Table 1 Sociodemographic and Health-Related Characteristics of Patients with T2DM at the National Diabetes Center (N=288) |
Prevalence of Poor Sleep Quality
Nearly one-third of the sample reported poor sleep quality (n=83; 35.8%), and Table 2 shows the distribution of the different components of the PSQI score. The median (IQR)age of those patients with poor sleep quality was 50 (14) and 53 (13) in patients with good sleep quality.
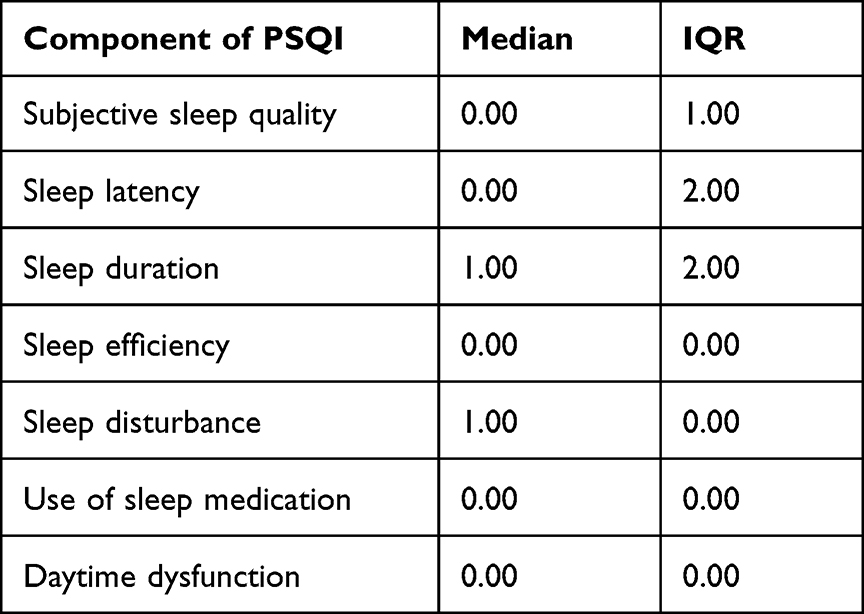 |
Table 2 Component of PSQI Score of Patients with T2DM at the National Diabetes Center |
Determinants of Poor Sleep Quality
Poor sleep quality was significantly associated with the participant’s age, perceived stress, and depression score; moreover, previous history of sleep disturbance and diagnosis were found to be significant determinants. However, no statistical association was found between poor sleep quality and other sociodemographic variables, as seen in Table 3.
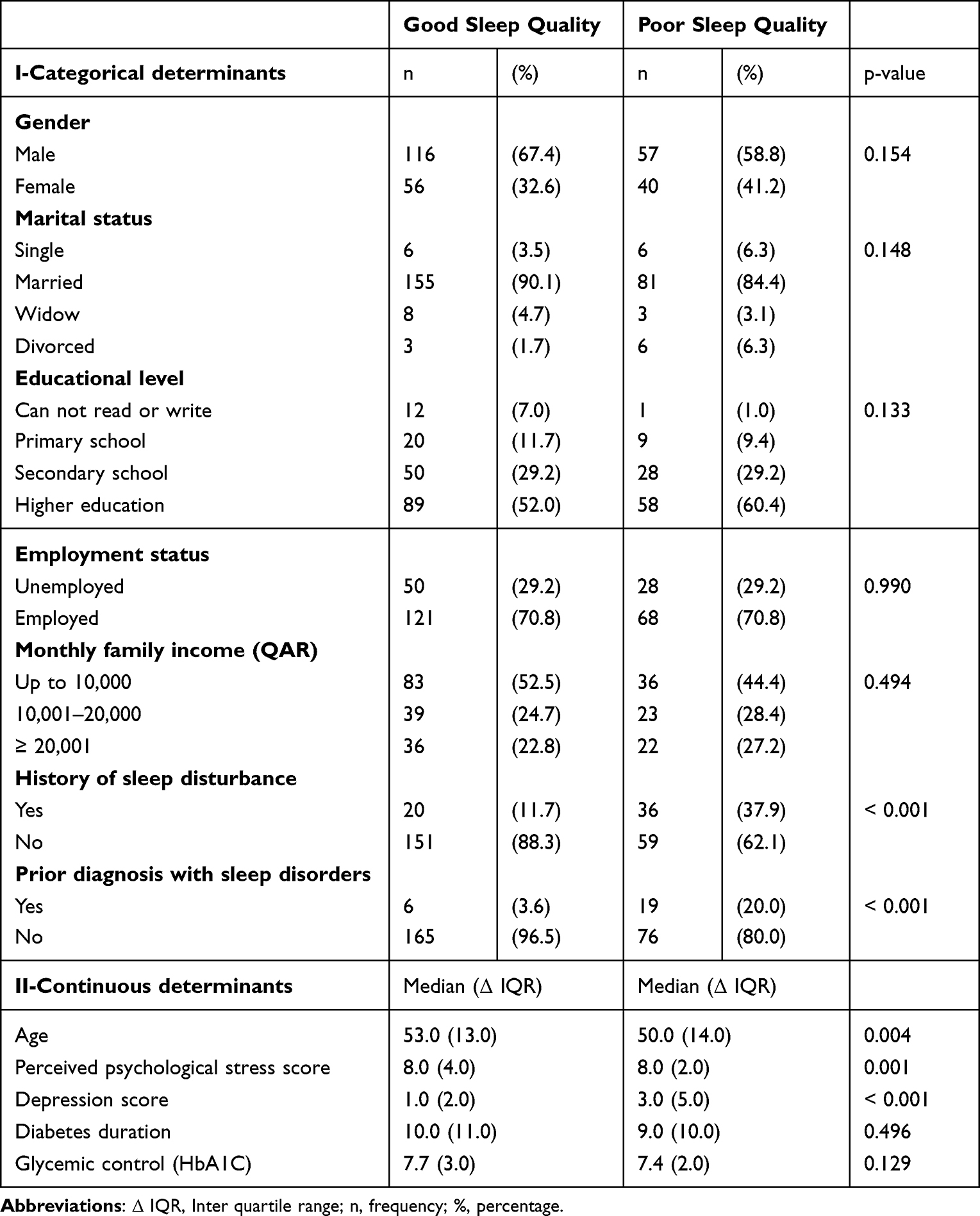 |
Table 3 Determinants of Poor Sleep Quality of Patients with T2DM at the National Diabetes Center (N=288) |
Correlations
Perceived stress and depressive symptoms scores were positively correlated with sleep quality scores, as shown in Table 4.
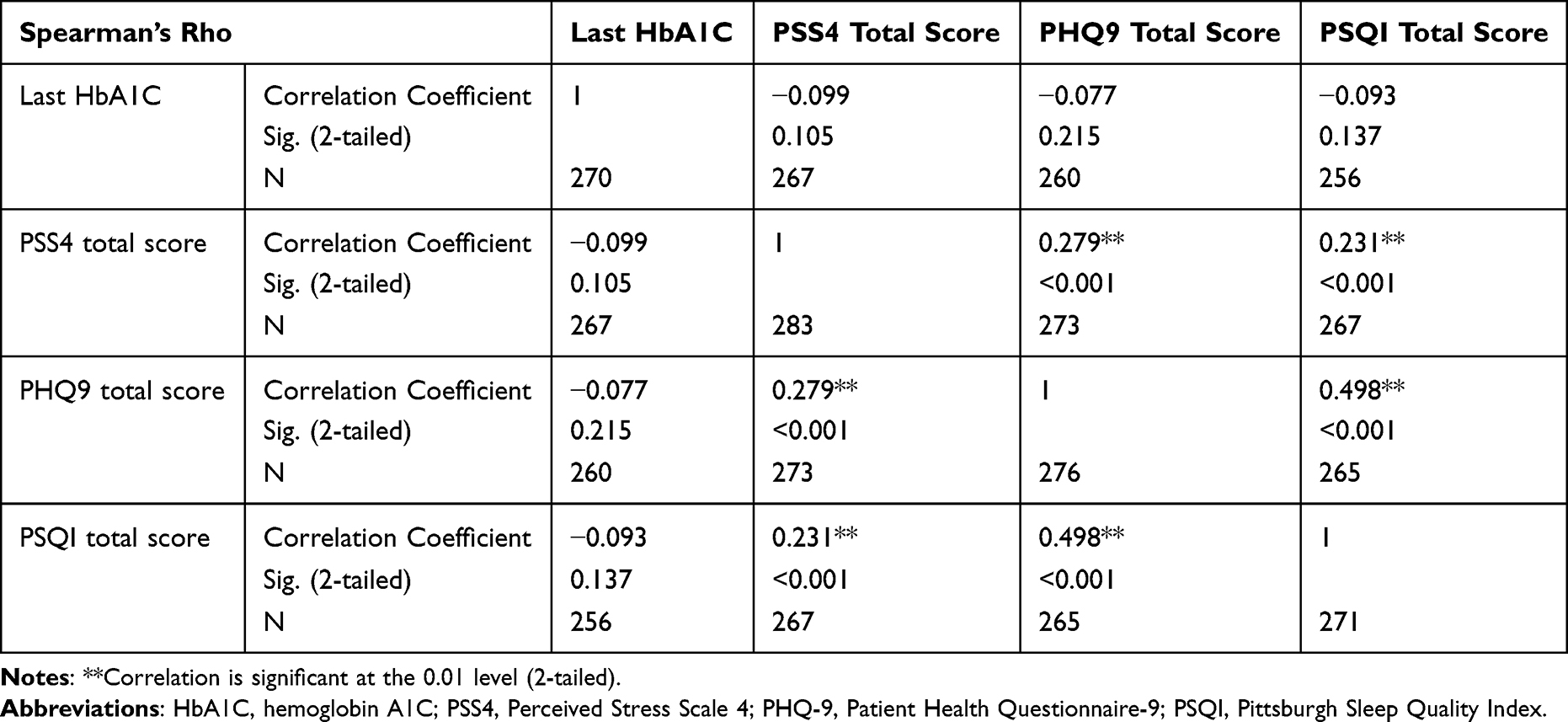 |
Table 4 Correlation Between Sleep Quality Index, HbA1c, Perceived Psychological Stress Score, and Depression Score Among Patients with T2DM at the National Diabetes Center (N=288) |
Predictors
We ran binary logistic regression to determine the significant predictors for poor sleep quality (coded as 1). We included significant variables (ie, age, previous history of sleep disorders, depression score, and perceived psychological stress score) of the preliminary analysis of the model. The regression revealed depression as a significant predictor of poor sleep quality. Patients with higher depression scores were 1.4 times more likely to experience poor sleep quality (Adjusted OR = 1.421; 95% CI: 1.242–1.625) than patients with good sleep quality. Furthermore, patients with an earlier history of sleep disorder were 3.2 times more likely to experience poor sleep quality (Adjusted OR = 3.208; 95% CI: 1.574–6.537) than patients with good sleep quality. Age and higher stress scores failed to predict poor sleep quality (p>0.05), as seen in Table 5.
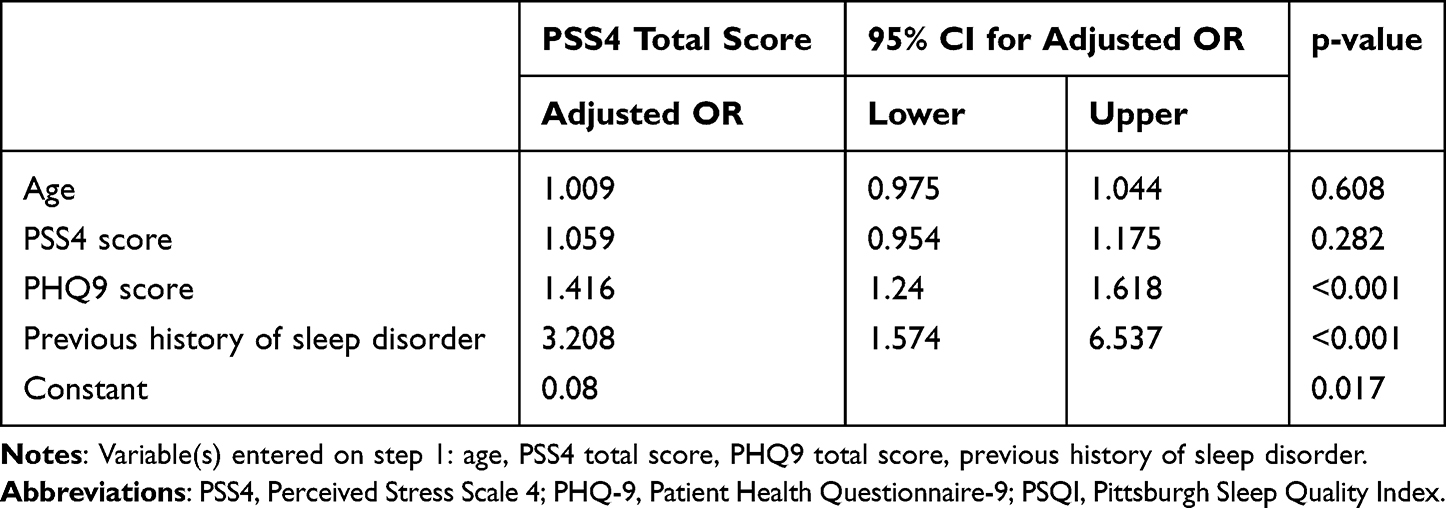 |
Table 5 Predictors of Poor Sleep Quality Among Patients with T2DM at the National Diabetes Center (N=288) |
Discussion
This study investigated the sleep quality among people with T2DM visiting the National Diabetes Center in Qatar during the COVID-19 pandemic. Almost one-third of the participants (35.8%) demonstrated poor sleep quality. In addition, a significant association was found between poor sleep quality and a previous history of sleep disturbance, high perceived stress, and depressive symptoms.
Our study showed that the prevalence of sleep disturbance among people with diabetes during the pandemic is significantly higher than the prevalence reported among the general population during the pandemic in Qatar (5%).33
Few studies investigated sleep quality among people with diabetes during the pandemic. In Southern Brazil, social distancing, home confinement, practicing less physical activity, and irregular sleep times contributed to sleep disorders in three-quarters of a cohort of people with type 2 diabetes.34 Furthermore, half of the participants reported taking morning naps and 30% perceived worse sleep quality through Mini-Sleep Questionnaire (MSQ).34 Despite using different sleep assessment tools, they revealed a similar prevalence to our study. Possible explanations include concerns about the risk of contracting COVID-19 while having diabetes that can play an important role and fluctuating blood sugar levels with frequent hyperglycaemia and hypoglycaemia episodes during the night leading to insomnia and next-day fatigue.34
We found that age is a significant determinant for poor sleep quality, which could be explained by the fact that young adults with diabetes exhibit more stage two sleep and tend to have less deep sleep during the first half of the night.35 However, later this variable failed to predict sleep quality in the logistic model, indicating its confounding effect.
Considering gender, our analysis revealed that gender is not statistically related to poor sleep quality. Similar to another study implemented in southeast India.36
Regarding sleep duration, this clinical variable did not affect sleep quality among people with diabetes. Our finding is similar to a study conducted in the United States.37 However, in Ethiopia, they revealed that diabetes duration could be a significant determinant of poor sleep quality. Specifically, patients over 10 years were three times more likely to have poor sleep than individuals with a shorter duration of diabetes.38
Sleep disorders and depression are closely related. For example, in our study, high depressive symptom scores were associated with poor sleep quality. Moreover, a statistically significant positive correlation was found between them, similar to another survey done in the USA.39 In one study, 41% of patients experienced a sleep disorder before a major depressive disorder;40 also, other studies found that people with depression usually have difficulties falling asleep, frequent sleep fragmentations, and early morning get-up time,38,41 and this might be attributed to the fact that insomnia is one of the typical early symptoms of depression. Moreover, depressed patients usually present with physical symptoms such as fatigue and sleep disturbance.42
A high perceived stress score was significantly associated with poor sleep quality. Fear, anxiety, and stress about a novel disease and what could happen can be and can have a considerable impact on people withT2DM and can disrupt their psychosocial life. Other studies have also documented the association between psychological distress and poor sleep quality among people with T2DM.43–45
In our study, we did not find a statistically significant association between poor sleep quality and the control of HbA1C, in line with other studies.46–48 In contrast, two studies49,50 found a statistically significant association between sleep quality and HbA1C.
To our knowledge, this study is the first to investigate the prevalence of low sleep quality during the pandemic. We selected patients randomly (probability sampling) and from the main diabetes centre in Qatar to ensure the generalization of results. However, our study comes with limitations. First, we did not use diagnostic measures to assess sleep quality (lack of polysomnography and lack of actinography). Second, we utilized a cross-sectional design that compromised the temporality and causality of the association between the variables.
Despite these limitations, our results will significantly impact public health. Using fully adjusted models, we found that high depression scores and a history of sleep disorder were significant predictors of poor sleep quality among people with T2DM; thus, clinicians caring about those patients should screen for and treat depressive symptoms and poor sleep quality. Moreover, a psychologist should be involved in the routine care of those patients, which can help in tackling both depressive symptoms and sleep disturbance, which can improve the overall quality of life of people with T2DM.
Conclusion
Our study showed that poor sleep quality is prevalent among people with type 2 during Covid 19; moreover, high depressive symptoms score and prior history of sleep disorders significantly predict poor sleep quality among those patients. Therefore, clinicians should screen for and treat sleep difficulties and depressive symptoms in people with type 2 diabetes.
Ethical Statement
The study was conducted in full conformance with the principles of the “Declaration of Helsinki” and Good Clinical Practice (GCP). The study was reviewed and approved by the Institutional Review Board (IRB) of the Medical Research Center (MRC) of Hamad Medical Corporation (MRC-01-22-200). The participants provided their written informed consent to participate in this study.
Acknowledgments
We would like to thank the Community Medicine and the Endocrinology departments at Hamad Medical Corporation (HMC) for their support in conducting this research. Moreover, we would like to thank Qatar National Libaray for providing open access funds for this article.
Funding
This study was funded by the Qatar National Library.
Disclosure
The authors declare that the research was conducted without any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Siwasaranond N, Nimitphong H, Manodpitipong A, et al. The relationship between diabetes-related complications and obstructive sleep apnea in type 2 diabetes. J Diabetes Res. 2018;2018:1–9. doi:10.1155/2018/9269170
2. Lee SWH, Ng KY, Chin WK. The impact of sleep amount and sleep quality on glycemic control in type 2 diabetes: a systematic review and meta-analysis. Sleep Med Rev. 2017;31:91–101. doi:10.1016/j.smrv.2016.02.001
3. Ohayon MM. Prevalence and comorbidity of sleep disorders in general population. Rev Prat. 2007;57(14):1521–1528.
4. Gupta R, Grover S, Basu A, et al. Changes in sleep pattern and sleep quality during COVID-19 lockdown. Indian J Psychiatry. 2020;62(4):370–378. doi:10.4103/psychiatry.IndianJPsychiatry_523_20
5. Skomro R, Ludwig S, Salamon E, Kryger M. Sleep complaints and restless legs syndrome in adult type 2 diabetics. Sleep Med. 2001;2(5):417–422. doi:10.1016/S1389-9457(01)00110-1
6. Anothaisintawee T, Reutrakul S, Van Cauter E, Thakkinstian A. Sleep disturbances compared to traditional risk factors for diabetes development: systematic review and meta-analysis. Sleep Med Rev. 2016;30:11–24. doi:10.1016/j.smrv.2015.10.002
7. Spellman CW. Achieving glycemic control: cornerstone in the treatment of patients with multiple metabolic risk factors. J Osteopathic Med. 2009;109(s51):8–13.
8. Albisser AM, Harris RI, Albisser JB, Sperlich M. The impact of initiatives in education, self-management training, and computer-assisted self-care on outcomes in diabetes disease management. Diabetes Technol Ther. 2001;3(4):571–579. doi:10.1089/15209150152811199
9. Aikens JE, Perkins DW, Lipton B, Piette JD. Longitudinal analysis of depressive symptoms and glycemic control in type 2 diabetes. Diabetes Care. 2009;32(7):1177–1181. doi:10.2337/dc09-0071
10. Pibernik-Okanovic M, Begic D, Szabo S, Renar I, Metelko Z. Interaction of depressive symptoms, diabetes-related distress and glycaemic control in type 2 diabetic patients. In: Diabetologia. Springer; 2007.
11. Peyrot M, McMurry JF Jr, Kruger DF. A biopsychosocial model of glycemic control in diabetes: stress, coping and regimen adherence. J Health Soc Behav. 1999;40(2):141–158. doi:10.2307/2676370
12. Piette JD, Richardson C, Valenstein M. Addressing the needs of patients with multiple chronic illnesses: the case of diabetes and depression. American J Managed Care. 2004;10(2; PART 2):152–162.
13. Resnick HE, Redline S, Shahar E, et al. Diabetes and sleep disturbances: findings from the sleep heart health study. Diabetes Care. 2003;26(3):702–709. doi:10.2337/diacare.26.3.702
14. Koren D, O’Sullivan KL, Mokhlesi B. Metabolic and glycemic sequelae of sleep disturbances in children and adults. Curr Diab Rep. 2015;15(1):1–10. doi:10.1007/s11892-014-0562-5
15. Gozashti MH, Eslami N, Radfar MH, Pakmanesh H. Sleep pattern, duration and quality in relation with glycemic control in people with type 2 diabetes mellitus. Iran J Med Sci. 2016;41(6):531. doi:10.2307/2651611
16. Whitaker KM, Lutsey PL, Ogilvie RP, et al. Associations between polysomnography and actigraphy-based sleep indices and glycemic control among those with and without type 2 diabetes: the multi-ethnic study of atherosclerosis. Sleep. 2018;41(11):zsy172. doi:10.1093/sleep/zsy172
17. Stamatakis KA, Punjabi NM. Effects of sleep fragmentation on glucose metabolism in normal subjects. Chest. 2010;137(1):95–101. doi:10.1378/chest.09-0791
18. Punjabi NM, Polotsky VY. Disorders of glucose metabolism in sleep apnea. J Appl Physiol. 2005;99(5):1998–2007. doi:10.1152/japplphysiol.00695.2005
19. Borbély AA. A two process model of sleep regulation. Hum Neurobiol. 1982;1(3):195–204.
20. Al-Thani MH, Al-Mutawa KA, Alyafei SA, et al. Characterizing epidemiology of prediabetes, diabetes, and hypertension in Qataris: a cross-sectional study. PLoS One. 2021;16(10):e0259152. doi:10.1371/journal.pone.0259152
21. ElSayed NA, Aleppo G, Aroda VR, et al. 4. Comprehensive medical evaluation and assessment of comorbidities: standards of Care in Diabetes—2023. Diabetes Care. 2023;46(Supplement_1):s49–s67. 2. doi:10.2337/dc23-S004
22. Bener A, Al-Hamaq AO. Sleep quality and excessive daytime sleepiness in a Arab diabetic popula. Biomed Res. 2010;2(4):333–340.
23. Bawadi H, Al Sada A, Al Mansoori N, et al. Sleeping duration, napping and snoring in association with diabetes control among patients with diabetes in Qatar. Int J Environ Res Public Health. 2021;18(8):4017. doi:10.3390/ijerph18084017
24. National Diabetes Center. National Diabetes Center at Hamad Medical Corporation; 2023. Available from: https://www.hamad.qa/EN/Hospitals-and-services/Hamad-General-Hospital/Hospital-Services/Clinical-Departments/Pages/National-Diabetes-Center.aspx#:~:text=It%20is%20a%20multi%2Ddisciplinary,department%20at%20Hamad%20General%20Hospital.
25. Charan J, Biswas T. How to calculate sample size for different study designs in medical research? Indian J Psychol Med. 2013;35(2):121–126. doi:10.4103/0253-7176.116232
26. Nelson KL, Davis JE, Corbett CF. Sleep quality: an evolutionary concept analysis. In: Nursing Forum. Wiley Online Library; 2022.
27. Buysse DJ, Hall ML, Strollo PJ, et al. Relationships between the Pittsburgh Sleep Quality Index (PSQI), Epworth Sleepiness Scale (ESS), and clinical/polysomnographic measures in a community sample. J Clin Sleep Med. 2008;4(6):563–571. doi:10.5664/jcsm.27351
28. Suleiman KH, Yates BC, Berger AM, Pozehl B, Meza J. Translating the Pittsburgh sleep quality index into Arabic. West J Nurs Res. 2010;32(2):250–268. doi:10.1177/0193945909348230
29. Al Maqbali M, Hughes C, Gracey J, Rankin J, Dunwoody L, Hacker E. Validation of the Pittsburgh Sleep Quality Index (PSQI) with Arabic cancer patients. Sleep Biol Rhythms. 2020;18(3):217–223. doi:10.1007/s41105-020-00258-w
30. Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983;24(4):385–396. doi:10.2307/2136404
31. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
32. AlHadi AN, AlAteeq DA, Al-Sharif E, et al. An Arabic translation, reliability, and validation of patient health questionnaire in a Saudi sample. Ann Gen Psychiatry. 2017;16(1):1–9. doi:10.1186/s12991-017-0155-1
33. Khaled SM, Petcu C, Al-Thani MA, et al. Prevalence and associated factors of DSM-5 insomnia disorder in the general population of Qatar. BMC Psychiatry. 2021;21(1):1–10. doi:10.1186/s12888-020-03035-8
34. Erthal IN, Alessi J, Teixeira JB, et al. Lifestyle pattern changes, eating disorders, and sleep quality in diabetes: how are the effects of 18 months of COVID-19 pandemic being felt? Acta Diabetol. 2022;59(10):1265–1274. doi:10.1007/s00592-022-01927-7
35. Jauch-Chara K, Schmid SM, Hallschmid M, Born J, Schultes B. Altered neuroendocrine sleep architecture in patients with type 1 diabetes. Diabetes Care. 2008;31(6):1183–1188. doi:10.2337/dc07-1986
36. Rajendran A, Parthsarathy S, Tamilselvan B, Seshadri KG, Shuaib M. Prevalence and correlates of disordered sleep in Southeast Asian Indians with type 2 diabetes. Diabetes Metab J. 2012;36(1):70–76. doi:10.4093/dmj.2012.36.1.70
37. Luyster FS, Dunbar-Jacob J. Sleep quality and quality of life in adults with type 2 diabetes. Diabetes Educ. 2011;37(3):347–355. doi:10.1177/0145721711400663
38. Zewdu D, Gedamu H, Beyene Y, Tadesse M, Tamirat M, Muluken S. Sleep quality and associated factors among type 2 Dm patients and non-Dm individuals in Bahir Dar governmental hospitals: comparative cross-sectional study. Sleep Sci & Prac. 2022;6(1):10. doi:10.1186/s41606-022-00079-5
39. Knutson KL, Ryden AM, Mander BA, Van Cauter E. Role of sleep duration and quality in the risk and severity of type 2 diabetes mellitus. Arch Intern Med. 2006;166(16):1768–1774. doi:10.1001/archinte.166.16.1768
40. Manber R, Chambers AS. Insomnia and depression: a multifaceted interplay. Curr Psychiatry Rep. 2009;11(6):437–442. doi:10.1007/s11920-009-0066-1
41. Liao C, Feng Z, Zhou D, et al. Dysfunction of fronto-limbic brain circuitry in depression. Neuroscience. 2012;201:231–238. doi:10.1016/j.neuroscience.2011.10.053
42. Fang H, Tu S, Sheng J, Shao A. Depression in sleep disturbance: a review on a bidirectional relationship, mechanisms and treatment. J Cell Mol Med. 2019;23(4):2324–2332. doi:10.1111/jcmm.14170
43. Liu Y, Croft J, Wheaton AA. Association between perceived insufficient sleep, frequent mental distress, obesity and chronic diseases among US adults, 2009 behavioral risk factor surveillance system. BMC Public Health. 2013;13(1):84. doi:10.1186/1471-2458-13-84
44. Grandner MA, Petrov MER, Rattanaumpawan P, Jackson N, Platt A, Patel NP. Sleep symptoms, race/ethnicity, and socioeconomic position. J Clin Sleep Med. 2013;9(9):897–905. doi:10.5664/jcsm.2990
45. Sariarslan H, Gulhan Y, Unalan D, Basturk M, Delibas S. The relationship of sleep problems to life quality and depression. Neurosci. 2015;20(3):236–242. doi:10.17712/nsj.2015.3.20150157
46. Jin Q-H, Chen -H-H, H-L Y, T-L L. The relationship between sleep quality and glucose level, diabetic complications in elderly type 2 diabetes mellitus. Zhonghua Nei Ke Za Zhi. 2012;51(5):357–361.
47. Lou P, Qin Y, Zhang P, et al. Association of sleep quality and quality of life in type 2 diabetes mellitus: a cross-sectional study in China. Diabetes Res Clin Pract. 2015;107(1):69–76. doi:10.1016/j.diabres.2014.09.060
48. Cho E-H, Lee H, Ryu OH, Choi MG, Kim S-W. Sleep disturbances and glucoregulation in patients with type 2 diabetes. J Korean Med Sci. 2014;29(2):243–247. doi:10.3346/jkms.2014.29.2.243
49. Zhu BQ, Li XM, Wang D, Yu XF. Sleep quality and its impact on glycaemic control in patients with type 2 diabetes mellitus. Int J Nursing Sci. 2014;1(3):260–265. doi:10.1016/j.ijnss.2014.05.020
50. Tsai YW, Kann N-H, Tung TH, et al. Impact of subjective sleep quality on glycemic control in type 2 diabetes mellitus. Fam Pract. 2012;29(1):30–35. doi:10.1093/fampra/cmr041
 © 2023 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.
© 2023 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a
Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the
original author and source are credited.
Recommended articles
Physical Activity, Dietary Habits and Factors Associated with Depression Among Medical Students of Sindh, Pakistan, During the COVID-19 Pandemic
Khidri FF, Riaz H, Bhatti U, Shahani KA, Kamran Ali F, Effendi S, Rani K, Chohan MN
Psychology Research and Behavior Management 2022, 15:1311-1323
Published Date: 25 May 2022
Assessment of Insomnia and Associated Factors Among Patients Who Have Recovered from COVID-19 in Vietnam
Huynh G, Nguyen HV, Vo LY, Le NT, Nguyen HTN
Patient Preference and Adherence 2022, 16:1637-1647
Published Date: 8 July 2022
Factors Affecting the Psychological Well-Being of Health Care Workers During the COVID-19 Crisis
Alharthi MH, Alshomrani AT, Bazaid K, Sonpol HMA, Ibrahim IAE, Alashkar AM
Psychology Research and Behavior Management 2022, 15:1931-1942
Published Date: 28 July 2022
Pre- and Post-Pandemic (COVID-19) Mental Health of International Students: Data from a Longitudinal Study
Jamshaid S, Bahadar N, Jamshed K, Rashid M, Imran Afzal M, Tian L, Umar M, Feng X, Khan I, Zong M
Psychology Research and Behavior Management 2023, 16:431-446
Published Date: 15 February 2023
Dietary Supplement Consumption and Mental Health in Indonesian Adults During Second Wave of COVID-19 Pandemic
Yusof J, d'Arqom A, Andriani AP, Nasution MZ, Fatimah N, Mustika A, Handayani S, Syed Abdul Kadir SZ
Patient Preference and Adherence 2023, 17:1799-1811
Published Date: 24 July 2023