")
Back to Journals » International Journal of General Medicine » Volume 15
Low Prevalence of Mild Alpha-1-Antitrypsin Deficiency in Hospitalized COVID-19-Patients
Authors Nygren D , Mölstad U, Thulesius H , Hillman M, Broman LM , Tanash H, Landin-Olsson M, Rasmussen M, Thunander M
Received 20 April 2022
Accepted for publication 31 May 2022
Published 28 June 2022 Volume 2022:15 Pages 5843—5848
DOI https://doi.org/10.2147/IJGM.S370434
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
David Nygren,1 Ulrica Mölstad,2 Hans Thulesius,2– 4 Magnus Hillman,5,6 Lars Mikael Broman,7,8 Hanan Tanash,9,10 Mona Landin-Olsson,5,6 Magnus Rasmussen,1 Maria Thunander2,6,11
1Division of Infection Medicine, Department of Clinical Sciences, Lund University, Lund, Sweden; 2Department of Research and Development, Health Care Region Kronoberg, Växjö, Sweden; 3Department of Medicine and Optometry, Linnaeus University, Växjö, Sweden; 4Department of Clinical Sciences, Family Medicine, Lund University, Malmö, Sweden; 5Diabetes Research Laboratory, Biomedical Center, Lund University, Lund, Sweden; 6Department of Clinical Sciences, Endocrinology and Diabetes, Lund University, Lund, Sweden; 7ECMO Centre Karolinska, Pediatric Perioperative Medicine and Intensive Care, Karolinska University Hospital, Stockholm, Sweden; 8Department of Physiology and Pharmacology, Karolinska Institutet, Stockholm, Sweden; 9Department of Clinical Sciences, Respiratory Medicine, Lund University, Malmö, Sweden; 10Department of Respiratory Medicine, Skåne University Hospital, Malmö, Sweden; 11Department of Internal Medicine, Endocrinology, Växjö Central Hospital, Växjö, Sweden
Correspondence: David Nygren, Division of Infection Medicine, Department of Clinical Sciences, Lund University, Lund, Sweden, Tel +4646171192, Fax +4646176002, Email [email protected]
Introduction: Alpha-1-antitrypsin (AAT) has been shown to inhibit SARS-CoV-2 cell entry and suggested as a therapeutic agent for COVID-19. Furthermore, epidemiological association of high prevalence of Alpha-1-antitrypsin deficiency (AATD) and regional severity of COVID-19-impact has been hypothesized. In our study setting, the estimated prevalence rates of mild (PI*MZ, PI*SS or PI*MS) and moderate-to-severe AATD (PI*ZZ or PI*SZ) are high, 9% and 0.2%, respectively. Our primary aim was to examine the prevalence rate of AATD among hospitalized COVID-19-patients.
Methods: In this prospective observational study, enrollment occurred from December 2020 to January 2021 in two COVID-19-units at Skåne University Hospital, Lund, Sweden. Case definition was a patient hospitalized due to COVID-19. Patients were screened for AATD with PI-typing and if results were inconclusive, PCR for the S- and Z-genes were performed. Patients were categorized as severe or moderate COVID-19 and 30-day-mortality data were collected. The primary outcome was prevalence rate of AATD. The secondary outcome investigated association between presence of mild AATD and severe COVID-19.
Results: We enrolled 61 patients with COVID-19. Two patients out of 61 (3%) had mild AATD (PI*MZ) and none had moderate-to-severe AATD. 30/61 (49%) had severe COVID-19. Both patients with mild AATD developed severe COVID-19. Yet, presence of AATD was not significantly associated with severe COVID-19 (p=0.24).
Conclusion: Mild AATD (PI*MS or PI*MZ) was rare in a small cohort of hospitalized patients with COVID-19 in a study setting with a high background prevalence of AATD.
Keywords: alpha-1-antitrypsin, alpha-1-antitrypsin deficiency, COVID-19, SARS-CoV-2, PI-typing, SERPINA1
Introduction
Alpha-1-antitrypsin (AAT) is the most abundant protease inhibitor in plasma and is encoded by the SERPINA1 gene.1 It is involved in inflammatory modulation, including decreasing neutrophil elastase activity.2,3 Patients with severe Alpha-1-antitrypsin deficiency (AATD) are at considerable risk of pulmonary emphysema due to lack of suppression of neutrophil elastase activity. Moderate-to-severe AATD (PI*SZ, PI*ZZ) has been suggested to increase the risk of severe Coronavirus disease 2019 (COVID-19).4 Moreover, mild AATD in the form of heterozygous carriage of PI*MZ has been shown to be associated with lung injury, yet with a low absolute risk.3 Interestingly, the cell-bound protease TMPRSS2 facilitates SARS-CoV-2 cell entry following viral binding to the ACE-2 cell membrane receptor.5 This protease has been shown to be inhibited by AAT, which could possibly inhibit SARS-CoV-2 cell entry and thereby suppress viral replication.6 Therefore, purified AAT-protein from plasma is being studied as a potential therapeutic for COVID-19, given either nebulized as an inhalation or through intravenous infusion.6–8 In addition, a recent review further highlighted theoretical pathogenic pathways in patients with AATD that could impact COVID-19-severity, including decreased inhibition of neutrophil extracellular traps, decreased inhibitory effect on thrombin and potentially an increase in thrombus formation.9
Early during the COVID-19-pandemic an association between areas of high prevalence of AATD and severe impact of COVID-19 was hypothesized.1,10–12 High SARS-CoV-2-positivity rates have also been reported in a cohort of Portuguese patients with moderate-to-severe AATD.4 Based on the evidence of the potential role of AAT in SARS-CoV-2 cell entry and replication as well as previously suggested associations between regional AATD prevalence and severity of the COVID-19-pandemic10,11 a prospective observational study of AATD in hospitalized COVID-19-patients was designed. The study was performed in an area with a high estimated prevalence of mild (PI*MZ, PI*SS, or PI*MS) (9%) and moderate-to-severe AATD (PI*SZ, PI*ZZ) (0.2%).13,14
The primary aim of this study was to evaluate the prevalence rate of mild AATD in patients hospitalized with COVID-19. The secondary aim was to investigate the association between presence of mild AATD and severe COVID-19.
Materials and Methods
Study Design and Setting
In this prospective, observational study of hospitalized COVID-19-patients, participants were enrolled at two designated COVID-19 non-intensive care units at the Skåne University Hospital, Lund, Sweden. Inclusion occurred from December 7, 2020 to January 20, 2021 at the peak of the second wave in this region with society transmission levels averaging 640 cases of SARS-CoV-2/100 000 population and week during the enrollment period.15
Participants
The eligibility criterion was SARS-CoV-2-positivity by PCR in patients aged ≥18 years hospitalized due to COVID-19. Enrollment occurred at any stage of disease and hospitalization. Patients unable to give informed consent (eg, due to decreased cognitive capacity) were excluded. A retrospective review of medical records was performed after 3 months. The study was performed according to the Declaration of Helsinki and its amendments. All patients gave written informed consent. The study was approved by the National Ethical Review Board in Sweden, number 2020–02995.
Outcomes, Groups and Definitions
The primary outcome was prevalence rate of AATD among patients hospitalized with COVID-19. AATD was defined as the presence of PI*MS, PI*SS or PI*MZ (mild AATD) or PI*SZ or PI*ZZ (moderate-to-severe AATD). As our secondary outcome, AATD was compared in hospitalized patients with severe and moderate COVID-19. Patients were defined as severe COVID-19 if they had been treated with high-flow nasal cannula (HFNC)-oxygenation, non-invasive ventilation therapy, ventilator therapy, were admitted to the intensive care unit at any stage of disease or had died within 30 days of admission. All other hospitalized patients in the study were considered moderate COVID-19. In all patients, serum, EDTA-whole blood and EDTA-plasma samples were collected and stored at −80°C pending analysis. Serum was used for PI-typing. PI-typing was performed using isoelectric focusing electrophoresis (NPU10618). If the Laboratory of Clinical Chemistry could not reliably rule out abnormal PI-typing results and gave inconclusive results, a targeted PCR for PI*S and PI*Z in EDTA-whole blood was performed. The analysis was performed using an allelic discrimination assay on the 7900HT real time PCR instrument with TaqMan®-probes. For PI*S the TaqMan® SNP Genotyping Assay 40x (Glu288Val/E288V/rs17580, assay ID:594695_20) was used and for PI*Z the TaqMan® SNP Genotyping Assay 40x (Glu366Lys/E366K/rs28929474, assay ID:34508510_10) was used. These pre-designed assays included primers and fluorescently labeled (FAM and VIC) MGB™ probes for detection of both the wild-type and variant alleles. Serum-AAT-levels were analyzed using a nephelometric assay on BNII (NPU19692). Normal reference ranges using this method were 0.86–1.75 g/L for men and 0.94–1.94 g/L for women. Finally, C-reactive protein (CRP) was analyzed on plasma samples using a particle enhanced turbidimetric assay performed on Cobas (NPU19748). All laboratory analyses were performed at the Laboratory of Clinical Chemistry, Skåne University Hospital, Malmö, Sweden.
On inclusion, age, gender, nation of birth, comorbidities according to the Charlson Comorbidity Index,16 smoking status and duration of symptoms were noted. A retrospective review after 3 months of follow-up was performed through analysis of electronic medical records where data regarding clinical course and mortality was collected.
Statistical Analysis
Continuous variables were described with median and interquartile range (IQR). For serum-AAT-levels, range of all values were also provided. Binary variables were described as counts and percentages. The prevalence rate of AATD among hospitalized COVID-19-patients were calculated. The potential association of the presence of mild AATD in patients with severe COVID-19 was compared using Fischer’s exact test. The study size was determined by the number of hospitalized patients during the enrollment period in the units were enrollment occurred. Statistical significance was defined as p<0.05. Statistical analyses were performed using STATA (StataCorp. 2013. Stata Statistical Software: Release 13. College Station, Texas; StataCorp LP).
Results
Participants and Baseline Characteristics
In total, 62 patients were considered eligible for the study, of whom 61 were enrolled. One patient was unable to give informed consent and was thus excluded. Among enrolled patients, no data was missing. Among enrolled patients, 23/61 (38%) were female, the median age was 66 years (IQR 57–77), 41/61 (67%) were born in Sweden, 57/61 (93%) born in Europe and 4/61 (7%) born outside of Europe (Table 1).
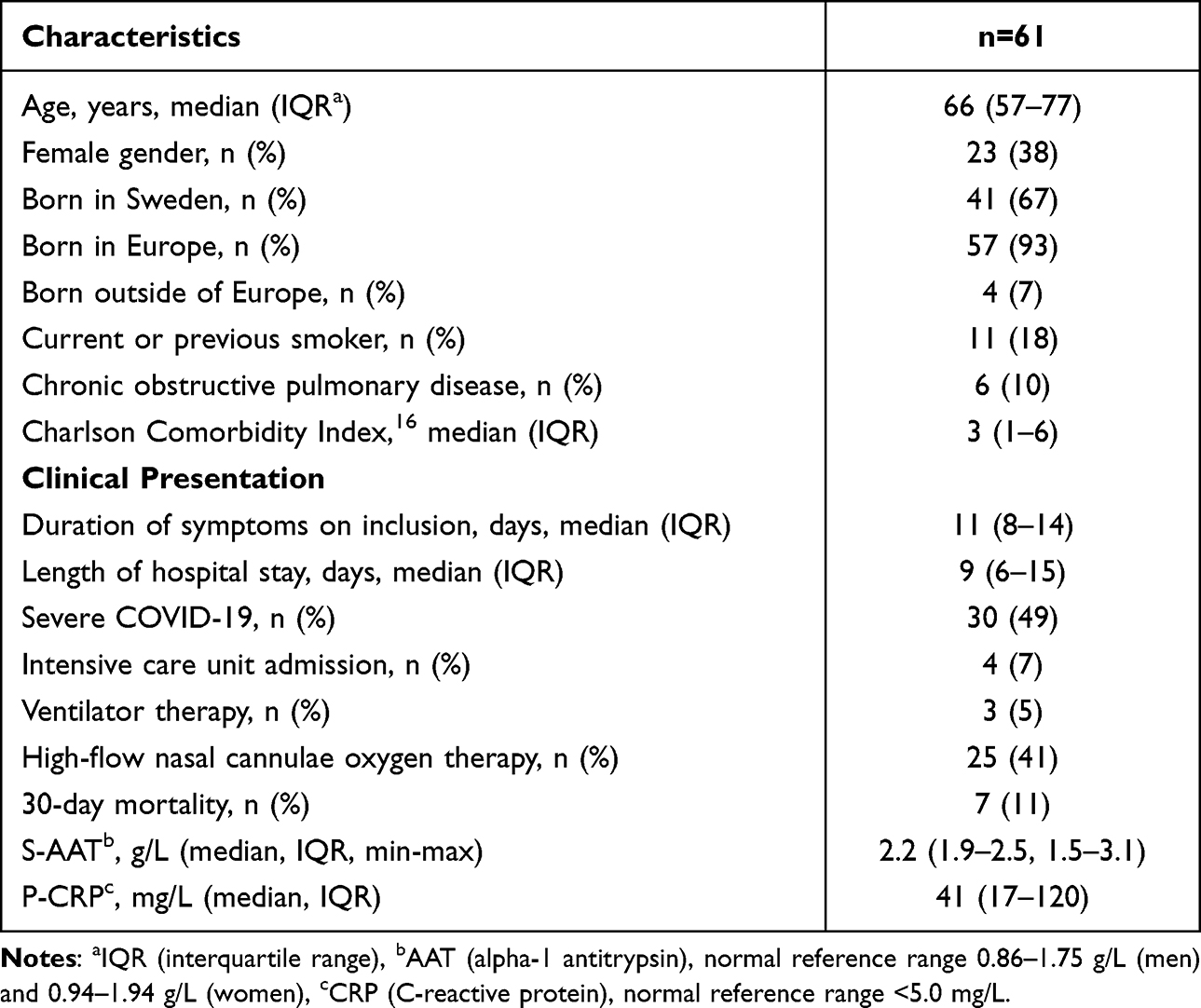 |
Table 1 Characteristics, Clinical and Laboratory Presentation in Patients (n=61) Hospitalized with COVID-19 |
Data for all participants was also presented separately by gender and by severity of COVID-19 in Supplementary Tables 1.1 and 1.2.
Study Outcomes
Of the investigated 61 patients hospitalized for COVID-19, 2 patients (3%) had mild AATD, of which both had heterozygous carriage of the PI*Z allele. In 53/61 samples PI-typing gave conclusive results. Both patients with PI*MZ were identified using this method. No other investigated PI-gene mutations (MS, SZ, SS, ZZ) were identified. In the eight patients with inconclusive PI-typing-results, targeted PCR for the S- and Z-genes were performed with negative results. In all patients, the median S-AAT-level was 2.1 g/L, with a range of 1.5–3.1 g/L. All values were normal or above the normal reference range.
In total, 30/61 (49%) patients had severe COVID-19. Intensive care admission occurred in 4/61 (7%) patients and 25/61 (41%) patients received HFNC oxygen treatment. Thirty-day mortality was seen in 7/61 (11%) patients. One patient was considered as severe COVID-19 despite no preceding HFNC oxygen treatment or intensive care unit-admission due to mortality within 30 days of admission. Both patients with PI*MZ developed severe COVID-19. Yet, no association between presence of mild AATD and severity of COVID-19 was found (p=0.24).
The two patients with heterozygous carriage of PI*Z were both 77 years old and female. One had a history of smoking and a diagnosis of chronic obstructive pulmonary disease with a Charlson Comorbidity Index of 7. She died unexpectedly during the first week of COVID-19, ie during the viral phase, and was not considered in need of treatment with HFNC or intensive care unit admission due to a clinically perceived stable condition. The second patient had a Charlson Comorbidity Index of 4 and required ventilator therapy in the intensive care unit but survived to discharge. Both these patients had elevated S-AAT-levels on inclusion (2.43 and 2.51 g/L).
Discussion
This prospective study of AATD in hospitalized COVID-19-patients in Sweden found a prevalence of mild AATD that was lower than the previously reported background population prevalence.13 While both patients identified with mild AATD did develop severe COVID-19, presence of mild AATD was not significantly associated with development of severe COVID-19. While the conclusions are limited by the small study cohort, our findings do not support mild AATD (PI*MS, PI*SS or PI*MZ) as a strong risk factor for infection or hospitalization with COVID-19. Yet, no conclusions regarding the previously suggested association of moderate-to-severe AATD with severity of COVID-194 can be drawn from this study.
This was the first clinical study to investigate AATD in a cohort of hospitalized COVID-19-patients and was based upon previous findings that AAT inhibits SARS-CoV-2 cell entry and could suppress viral replication6 as well as the previously presented hypothesis of an association between high prevalence of AATD and severe impact of the COVID-19 pandemic.10,11
Strengths of the study include that the study was performed in an area with a high prevalence of AATD,13 enrollment occurred during a period of high societal transmission of SARS-CoV-2 in Sweden and involved a broad spectrum of hospitalized patients. The regional prevalence of AATD in our study setting is well known in part due to the Swedish Neonatal AAT screening that was performed in 1972–1974.17 This cohort is still followed and among those with moderate-to-severe AATD, there is a slight overrepresentation of males (58%)18 which is similar to our study population, reducing potential selection bias due to gender differences. The study size and single-center design are limitations, and due to the rarity of moderate-to-severe AATD, this study can draw no conclusions on the potential association between moderate-to-severe AATD and COVID-19.4 Further limitations to our study include that no patients with COVID-19 were enrolled in the intensive care unit. Enrolled patients treated for COVID-19 in the intensive care unit were either enrolled prior to care at or after discharge from the intensive care unit. No patients who were admitted directly to the intensive care unit and subsequently did not survive were thus enrolled. This introduces a measure of survivorship bias as does the fact that severe AATD is associated with shortened life expectancy.19 However, this study was not powered to draw conclusions on patients with severe AATD, why this type of selection bias was considered negligible. Finally, while S-AAT-levels are raised by inflammation,20 PI-typing was performed in all patients regardless of S-AAT-level and performed according to clinical routine by the Laboratory of Clinical Chemistry. While the interpretation of PI-typing can be complex, and potentially further exacerbated since most patients in our study had acute and ongoing inflammation at the time of recruitment, we performed targeted PCR for the S- and Z-genes when PI-typing did not present fully conclusive results to avoid misclassification.
Interestingly, while mild AATD (PI*MS, PI*SS or PI*MZ) is common (9%)13 in the study region, it was rarely seen in our cohort (3%) and the presence of mild AATD was not significantly associated with development of severe COVID-19. The study site, Skåne University Hospital, Lund, has a catchment population of approximately 370,000 inhabitants. Thus, 33,300/370,000 (9%) inhabitants were estimated to have mild AATD in the study area13 while 2/61 (3%), had mild AATD in our study (x2, p=0.14). While our study constitutes a small cohort of hospitalized COVID-19-patients, our findings are in line with recently published data from the United Kingdom (UK) Biobank, which showed 12,723 (3.0%) positive COVID-19 tests in 426,994 participants that were non-carriers of PI-gene mutations and 1670 (2.8%) positive COVID-19 tests in 60,509 participants that were carriers of any PI-gene mutation (MZ, MS, SZ, SS, ZZ).21
Simultaneously, in patients with positive COVID-19-tests, “Death by COVID-19” was seen in 353 (0.083%) non-carriers and in 53 (0.088%) PI-gene mutation carriers (x2, p=0.69) in the UK Biobank study.21 In addition, on the contrary to previous reports of a suggested association of moderate and severe AATD with severity of COVID-19,4 the UK biobank study did neither identify moderate-to-severe AATD as a risk factor for SARS-CoV-2-positivity or “Death by COVID-19” when compared to non-carriers. However, since there were so few patients with moderate-to-severe AATD, data were not considered robust enough for meaningful conclusions.21 Finally, in our study, both patients with PI*MZ developed severe COVID-19 of whom one died. Yet, both patients had several other known risk factors for severe COVID-19 why this finding necessitates cautious interpretation.
In conclusion, we describe a low prevalence of mild AATD (PI*MS, PI*SS or PI*MZ) in a small cohort of hospitalized patients with COVID-19 in an area with a high background prevalence of COVID-19. No conclusions can be drawn from this study regarding patients with moderate-to-severe AATD (PI*SZ, PI*ZZ) and adequate quantification of this risk would require large registry-based studies. Nevertheless, we encourage further clinical studies on the importance of AAT in the pathogenesis and prognosis of COVID-19 and a potential therapeutic role.
Abbreviations
AAT, alpha-1-antitrypsin; AATD, alpha-1-antitrypsin deficiency; COVID-19, coronavirus disease 2019; CRP, C-reactive protein; HFNC, high-flow nasal cannula; SARS-CoV-2, severe acute respiratory syndrome-coronavirus 2; UK, United Kingdom.
Acknowledgments
The authors are grateful to Mohibullah Hotak, Dr Ning Xu, Dr Magnus Förnvik Jonsson and Dr Camilla Valtonen-André at the Laboratory of Clinical Chemistry at Skåne University Hospital for their assistance.
Funding
The authors of the study report funding from the Swedish Heart Lung Foundation, the Swedish Physicians’ Research Society and Swedish Government Funds for Clinical Research (ALF).
Disclosure
Dr David Nygren reports financial support from The Swedish Government Funds for Clinical Research (ALF), during the conduct of the study. Dr Lars Mikael Broman is part of the Medical Advisory Board for Eurosets Srl., Medolla, Italy and Xenios AG., Heilbronn, Germany, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Yang C, Chapman KR, Wong A, et al. α1-antitrypsin deficiency and the risk of COVID-19: an urgent call to action. Lancet Respir Med. 2021;9(4):337–339. doi:10.1016/S2213-2600(21)00018-7
2. Oguntuyo KY, Stevens CS, Siddiquey MN, et al. In plain sight: the role of alpha-1-antitrypsin in COVID-19 pathogenesis and therapeutics. bioRxiv. 2020. doi:10.1101/2020.08.14.248880
3. Strnad P, Mcelvaney NG, Lomas DA. Alpha1-antitrypsin deficiency. N Engl J Med. 2020;382(15):1443–1455. doi:10.1056/NEJMra1910234
4. Faria N, Inês Costa M, Gomes J, et al. Alpha-1 antitrypsin deficiency severity and the risk of COVID-19: a Portuguese cohort. Respir Med. 2021;181:106387. doi:10.1016/j.rmed.2021.106387
5. Hoffmann M, Kleine-Weber H, Schroeder S, et al. SARS-CoV-2 cell entry depends on ACE2 and TMPRSS2 and is blocked by a clinically proven protease inhibitor. Cell. 2020;181(2):271–280.e278. doi:10.1016/j.cell.2020.02.052
6. Wettstein L, Weil T, Conzelmann C, et al. Alpha-1 antitrypsin inhibits TMPRSS2 protease activity and SARS-CoV-2 infection. Nat Commun. 2021;12(1). doi:10.1038/s41467-021-21972-0
7. Yang C, Keshavjee S, Liu M. Alpha-1 antitrypsin for COVID-19 treatment: dual role in antiviral infection and anti-inflammation. Front Pharmacol. 2020;11. doi:10.3389/fphar.2020.615398
8. Bai X, Hippensteel J, Leavitt A, et al. Hypothesis: alpha-1-antitrypsin is a promising treatment option for COVID-19. Med Hypotheses. 2021;146:110394. doi:10.1016/j.mehy.2020.110394
9. Vianello A, Guarnieri G, Braccioni F, et al. Correlation between α1-antitrypsin deficiency and SARS-CoV-2 infection: epidemiological data and pathogenetic hypotheses. J Clin Med. 2021;10(19):4493. doi:10.3390/jcm10194493
10. Shapira G, Shomron N, Gurwitz D. Ethnic differences in alpha‐1 antitrypsin deficiency allele frequencies may partially explain national differences in COVID‐19 fatality rates. FASEB J. 2020;34(11):14160–14165. doi:10.1096/fj.202002097
11. Vianello A, Braccioni F. Geographical overlap between alpha-1 antitrypsin deficiency and COVID-19 infection in Italy: casual or causal? Archivos de Bronconeumología. 2020;56(9):609–610. doi:10.1016/j.arbres.2020.05.015
12. Ferrarotti I, Ottaviani S, Balderacchi AM, et al. COVID-19 infection in severe Alpha 1-antitrypsin deficiency: looking for a rationale. Respir Med. 2021;183:106440. doi:10.1016/j.rmed.2021.106440
13. Blanco I. Estimated numbers and prevalence of PI*S and PI*Z alleles of Alpha-1-antitrypsin deficiency in European countries. Eur Respir J. 2006;27(1):77–84. doi:10.1183/09031936.06.00062305
14. Hjalmarsson K. Distribution of alpha-1-antitrypsin phenotypes in Sweden. Hum Hered. 1988;38(1):27–30. doi:10.1159/000153750
15. The Public Health Agency of Sweden. Confirmed cases of COVID-19. 2021. Available from: https://www.folkhalsomyndigheten.se/smittskydd-beredskap/utbrott/aktuella-utbrott/covid-19/statistik-och-analyser/bekraftade-fall-i-sverige/.
16. Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. doi:10.1016/0021-9681(87)90171-8
17. Sveger T. Liver disease in alpha1-antitrypsin deficiency detected by screening of 200,000 infants. N Engl J Med. 1976;294(24):1316–1321. doi:10.1056/NEJM197606102942404
18. Mostafavi B, Piitulainen E, Tanash HA. Survival in the Swedish cohort with alpha-1-antitrypsin deficiency, up to the age of 43–45 years. Int J Chron Obstruct Pulmon Dis. 2019;14:525–530. doi:10.2147/COPD.S183205
19. Tanash HA, Ekström M, Rönmark E, et al. Survival in individuals with severe alpha 1-antitrypsin deficiency (PiZZ) in comparison to a general population with known smoking habits. Eur Respir J. 2017;50(3):1700198. doi:10.1183/13993003.00198-2017
20. Sanders CL, Ponte A, Kueppers F. The effects of inflammation on alpha 1 antitrypsin levels in a national screening cohort. J Chronic Obstruct Pulmon Dis. 2018;15(1):10–16. doi:10.1080/15412555.2017.1401600
21. Schneider CV, Strnad P. SARS-CoV-2 infection in alpha1-antitrypsin deficiency. Respir Med. 2021;184:106466. doi:10.1016/j.rmed.2021.106466
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
COVID-19 and Saudi Arabia: Awareness, Attitude, and Practice
Fawzy MS, AlSadrah SA
Journal of Multidisciplinary Healthcare 2022, 15:1595-1618
Published Date: 26 July 2022
An Overview of Neurological and Psychiatric Complications During Post-COVID Period: A Narrative Review
Li D, Wang Q, Jia C, Lv Z, Yang J
Journal of Inflammation Research 2022, 15:4199-4215
Published Date: 26 July 2022
Comparison of the Diagnostic Performance of a Rapid Antigen Test with Real-Time Polymerase Chain Reaction for Detection of SARS-CoV-2 Among Patients Diagnosed with COVID-19 at Selected Hospitals in Addis Ababa, Ethiopia
Desalegn Z, Sebre S, Yohannes M, Seman A, Shiferaw W, Ademe M, Biazin H, Firdawoke E, Asemamaw Y, Teka B, Teshome S, Amogne W, Addissie A, Gebrehiwot Y, Kantelhardt E, Abebe T
Infection and Drug Resistance 2022, 15:4299-4305
Published Date: 6 August 2022
A Pilot Study of 0.4% Povidone-Iodine Nasal Spray to Eradicate SARS-CoV-2 in the Nasopharynx
Sirijatuphat R, Leelarasamee A, Puangpet T, Thitithanyanont A
Infection and Drug Resistance 2022, 15:7529-7536
Published Date: 21 December 2022
Distinct Features of Vascular Diseases in COVID-19
Ceasovschih A, Sorodoc V, Shor A, Haliga RE, Roth L, Lionte C, Onofrei Aursulesei V, Sirbu O, Culis N, Shapieva A, Tahir Khokhar MA, Statescu C, Sascau RA, Coman AE, Stoica A, Grigorescu ED, Banach M, Thomopoulos C, Sorodoc L
Journal of Inflammation Research 2023, 16:2783-2800
Published Date: 6 July 2023