Back to Journals » Infection and Drug Resistance » Volume 16
Prognostic Value of C-Reactive Protein in SARS-CoV-2 Infection: A Simplified Biomarker of COVID-19 Severity in Northern Ethiopia
Authors Gebrecherkos T ![]() , Challa F
, Challa F ![]() , Tasew G, Gessesse Z, Kiros Y
, Tasew G, Gessesse Z, Kiros Y ![]() , Gebreegziabxier A, Abdulkader M
, Gebreegziabxier A, Abdulkader M ![]() , Desta AA
, Desta AA ![]() , Atsbaha AH, Tollera G, Abrahim S, Urban BC, Schallig H
, Atsbaha AH, Tollera G, Abrahim S, Urban BC, Schallig H ![]() , Rinke de Wit T, Wolday D
, Rinke de Wit T, Wolday D
Received 25 February 2023
Accepted for publication 5 May 2023
Published 16 May 2023 Volume 2023:16 Pages 3019—3028
DOI https://doi.org/10.2147/IDR.S410053
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Suresh Antony
Teklay Gebrecherkos,1 Feyissa Challa,2 Geremew Tasew,3 Zekarias Gessesse,4 Yazezew Kiros,4 Atsbeha Gebreegziabxier,5 Mahmud Abdulkader,1 Abraham Aregay Desta,6 Ataklti Hailu Atsbaha,7 Getachew Tollera,8 Saro Abrahim,5 Britta C Urban,9 Henk Schallig,10 Tobias Rinke de Wit,11,12 Dawit Wolday1,5
1Department of Medical Microbiology and Immunology, College of Health Sciences (CHS), Mekelle University (MU), Mekelle, Tigray, Ethiopia; 2National Reference Laboratory for Clinical Chemistry, Ethiopian Public Health Institute, Addis Ababa, Ethiopia; 3Department of Bacteriology, Parasitology and Zoonosis, Ethiopian Public Health Institute, Addis Ababa, Ethiopia; 4Department of Internal Medicine, College of Health Sciences, Mekelle University, Mekelle, Tigray, Ethiopia; 5HIV/TB Research Directorate, Ethiopian Public Health Institute, Addis Ababa, Ethiopia; 6Public Health Research and Emergency Management, Tigray Health Research Institute, Mekelle, Tigray, Ethiopia; 7Department of Microbiology, Tigray Health Research Institute, Mekelle, Tigray, Ethiopia; 8Research and Technology Transfer Directorate, Ethiopian Public Health Institute, Addis Ababa, Ethiopia; 9Department of Clinical Sciences, Respiratory Clinical Research Group, Liverpool School of Tropical Medicine, Liverpool, UK; 10Department of Medical Microbiology and Infection Prevention, Experimental Parasitology Unit, Academic Medical Center, University of Amsterdam, Amsterdam, Netherlands; 11Amsterdam Institute of Global Health and Development, Department of Global Health, Amsterdam University Medical Center, Amsterdam, the Netherlands; 12Joep-Lange Institute, Amsterdam, the Netherlands
Correspondence: Teklay Gebrecherkos, Department of Medical Microbiology and Immunology, Mekelle University, P.O. Box 1871, Mekelle, Tigray, Ethiopia, Email [email protected]
Purpose: To evaluate the role of C-reactive protein (CRP) in predicting severe COVID-19 patients.
Methods: A prospective observational cohort study was conducted from July 15 to October 28, 2020, at Kuyha COVID-19 isolation and treatment center hospital, Mekelle City, Northern Ethiopia. A total of 670 blood samples were collected serially. SARS-CoV-2 infection was confirmed by RT-PCR from nasopharyngeal swabs and CRP concentration was determined using Cobas Integra 400 Plus (Roche). Data were analyzed using STATA version 14. P-value < 0.05 was considered statistically significant.
Results: Overall, COVID-19 patients had significantly elevated CRP at baseline when compared to PCR-negative controls [median 11.1 (IQR: 2.0– 127.8) mg/L vs 0.9 (IQR: 0.5– 1.9) mg/L; p=0.0004)]. Those with severe COVID-19 clinical presentation had significantly higher median CRP levels compared to those with non-severe cases [166.1 (IQR: 48.6– 332.5) mg/L vs 2.4 (IQR: 1.2– 7.6) mg/L; p< 0.00001)]. Moreover, COVID-19 patients exhibited higher median CRP levels at baseline [58 (IQR: 2.0– 127.8) mg/L] that decreased significantly to 2.4 (IQR: 1.4– 3.9) mg/L after 40 days after symptom onset (p< 0.0001). Performance of CRP levels determined using ROC analysis distinguished severe from non-severe COVID-19 patients, with an AUC value of 0.83 (95% CI: 0.73– 0.91; p=0.001; 77.4% sensitivity and 89.4% specificity). In multivariable analysis, CRP levels above 30 mg/L were significantly associated with an increased risk of developing severe COVID-19 for those who have higher ages and comorbidities (ARR 3.99, 95% CI: 1.35– 11.82; p=0.013).
Conclusion: CRP was found to be an independent determinant factor for severe COVID-19 patients. Therefore, CRP levels in COVID-19 patients in African settings may provide a simple, prompt, and inexpensive assessment of the severity status at baseline and monitoring of treatment outcomes.
Keywords: CRP, COVID-19, SARS-CoV-2, biomarker
Introduction
Infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), the etiology of the coronavirus disease 2019 (COVID-19), has resulted in an unprecedented global pandemic with a total of over 670 million cases and over 6.8 million deaths globally as of March 30, 2023.1 COVID-19 presents with a multitude of clinical features, spanning from asymptomatic or mild to severe or critical form.2,3 Severe and critical COVID-19 is associated with acute respiratory distress syndrome, requiring hospitalization, supplemental oxygen, and/or mechanical ventilation. Risk factors associated with the severe disease include older age and the presence of comorbidities, such as hypertension, diabetes, chronic obstructive lung diseases, and chronic kidney diseases.4–8
In the Sub-Saharan Africa (SSA) context, similar risk factors have also been reported.9,10 The whole mark characteristics of the severe form of COVID-19 have been linked to the overproduction of several pro-inflammatory cytokines, leading to cytokine storms.11,12 When compared to mild/moderate COVID-19 cases, patients with severe disease have markedly increased levels of pro-inflammatory cytokines, including interleukin (IL)-1, IL-2, IL-6, IL-8, IL-10, IL-12, IL-17, tumor necrosis factor (TNF)-α and interferon (IFN)-γ.4,13–17 In addition to cytokine deregulation, cytokine storm in severe COVID-19 is also associated with coagulopathy.18–20
C-reactive protein (CRP) belongs among the surrogate biomarkers of cytokine storm.21 CRP is an acute phase reactant produced by the liver that serves as an early marker of infection and inflammation and is largely produced in response to IL-6.22 Emerging evidence indicates that IL-6 plays a pivotal role in the pathogenesis of cytokine storm associated with severe COVID-19,23–26 and CRP levels may act as a reliable surrogate for IL-6 bioactivity.21,22 Cumulative reports have demonstrated that levels of CRP increased during severe COVID-19.27–29
Few mild/ moderate COVID‐19 patients develop a severe disease level. Thus, it is crucial to early identify and put into treatment this group of patients to reduce and improve their disease severity. Some studies showed that the degree of severity and mortality of patients with COVID‐19 is due to an altered level of some blood markers; CRP has been found as an important biomarker in determining changes in patients with severe COVID‐19.28,30,31 Moreover, CRP could be used effectively as a routine blood parameter to determine the prognosis and diagnosis of COVID‐19.32,33
Measurement of the various cytokine levels associated with cytokine storms in the setting of SSA, particularly in Ethiopia is not realistic given the challenges faced concerning suboptimal laboratory infrastructure. However, recent improvements in the determination of low concentration by the high-sensitivity CRP (hs-CRP) methods are developed, which are rapid, easy, inexpensive, and readily available in the majority of SSA healthcare facilities.34 Unfortunately, there is no data available on the role of CRP as a determinant prognostic marker for COVID-19 severity status in northern Ethiopia and there is a paucity of data on the kinetics of CRP levels among Ethiopian COVID-19 patients. In this study, therefore, we aimed to assess the prognostic value of CRP levels in the various categories of COVID-19 patients as stratified by severity status.
Methods
Study Design, Period, and Population
This study is part of the ongoing Profile-Cov study, a prospective observational cohort study being undertaken in Ethiopia (Clinicaltrials.gov: NCT04473365). Consecutive patients (n=78) with confirmed real-time polymerase chain reaction (RT-PCR) test results for SARS-CoV-2 and RT-PCR negative controls (n = 50) were enrolled. They were prospectively recruited from Kuyha Hospital COVID-19 Isolation and Treatment Center, College of Health Science, Mekelle University, Northern Ethiopia, between July 15 and October 28, 2020.
Data Collection
Socio-demographic and clinical data were collected using standardized Case Record Forms (CRFs) adapted from the International Severe Acute Respiratory and Emerging Infection Consortium’s (ISARIC) CRFs for emerging severe acute respiratory infections.35 The patient’s clinical status was stratified following WHO criteria as asymptomatic, mild/moderate, severe (with dyspnea, respiratory rate ≥ 30 breaths per minute, O2 saturation ≤ 93%, lung infiltrates ≥ 50% of the lung fields within 24–48 hours), and critical (with respiratory failure, septic shock, and/or multiple organ failure).36 For this study, asymptomatic and mild/moderate cases were considered non-severe cases and both severe and critical patients were considered severe cases. The date of symptom onset was determined for symptomatic cases. For asymptomatic patients, however, we added 6 days (median time between symptom onset and date of PCR testing among symptomatic cases) to post-PCR testing.
Sample Collection Process
For the confirmation of SARS-CoV-2 infection, nasopharyngeal swabs were collected and put in virus transport media and then sent immediately to the Ayder Central Laboratory of the University Hospital for diagnosis. For the analysis of the kinetics of CRP levels, 3–5 mL of whole blood was collected using an EDTA tube, and a total of 620 blood samples were drawn longitudinally from the 78 COVID-19 patients. Whenever possible, samples were drawn every 3 days until day 30 post-admission.
The samples were stored at room temperature for at least 30 min and then centrifuged at 3500 g for 5 min at room temperature. After separation of the plasma, the specimen was promptly separated into 2 aliquots of 3 mL in Nalgene cryovials and stored at –80 ◦C Ayder Central Laboratory of the University hospital. Specimens were immediately transported to EPHI Clinical Chemistry Laboratory for further analysis. In addition to the above, for determining specificity, RT-PCR negative controls (n = 50) were obtained during the COVID-19 pandemic (August and September 2020) from individuals not suspected of SARS-CoV-2 infection.
Laboratory Assays
SARS-CoV-2 infection was confirmed by RT-PCR on samples obtained from nasopharyngeal swabs. The swabs collected were then put onto virus transport media and sent immediately to the central laboratory. RT-PCR for the detection of SARS-CoV-2 infection was based on the LightMix® Modular SARS and Wuhan CoV E-gene kit (TIB Molbiol, Berlin, Germany), as described previously.9 CRP concentration was determined by immune-turbidimetric (reagent CRPHS Ref. 04628918190) assay analyzed using the Cobas Integra 400® Plus (Roche Diagnostics GmbH, Mannheim, Germany) at the EPHI National Reference Laboratory for Clinical Chemistry, as per the manufacturer’s instructions described previously.34
Quality Control
Data quality was maintained using standardized Case Record Forms (CRFs) adapted from the International Severe Acute Respiratory and Emerging Infection Consortium’s (ISARIC) CRFs for emerging severe acute respiratory infections. The reliability of the findings was guaranteed by implementing quality control measures throughout the whole process of laboratory work. Two internal quality control materials at two different levels (PreciControl ClinChem Multi 1 ref. 05947626190, CRP T Control N Ref. 20766321322) were also analyzed during all analytical series. The analytical characteristics of CRP are as follows: the limit of the blank, the limit of detection, and the limit of quantitation were 0.1, 0.2, and 0.3 mg/L, respectively. Over the study period, the assay had a 1.23% coefficient of variation (CV) with a 10.6 mg/L mean (CRP T Control) and a 4.30% CV with a 7.9 mg/L mean for Preci Control Clin Chem Multi 1. The National Reference Laboratory for Clinical Chemistry participated in the external quality assurance program (One World Accuracy), which is accredited by the Ethiopia National Accreditation Office.
Statistical Analysis
Data were entered into electronic medical records and checked for completeness and analyzed using STATA (Statistical package v. 14.0, StataCorp, Texas, USA).
Baseline characteristics for continuous variables were expressed as the median with interquartile range (IQR), and for categorical variables as proportions. Whereas categorical variables were compared using x2 test or Fisher’s exact test, continuous variables were compared by Mann–Whitney U, or Kruskal–Wallis tests, as appropriate. Normality of distribution of variables was ascertained by running Wilk test of normality, before analysis by Mann–Whitney U, or Kruskal–Wallis tests. The area under the receiver operating characteristic (ROC) curve (AUC) was analyzed to assess the diagnostic value of CRP by comparing PCR-confirmed COVID-19 patients with PCR-negative controls as well as to predict COVID-19 severity. The maximum potential effectiveness of CRP as a biomarker was calculated using the Youden index. Poisson regression analysis was used to determine risk factors associated with developing severe COVID-19. p <0.05 were considered statistically significant.
Results
Characteristics of Study Participants
A total of 78 COVID-19 patients who tested positive on RT-PCR for SARS-CoV-2 were included in the study. The majority of study participants (76.3%) were male (Table 1). The median age of the cohort was 34 (IQR: 28–50) years, with 53.0% being in the age range of 24 to 44 years. Whereas 49 (62.8%) patients were asymptomatic or mild/moderate cases (non-severe COVID-19), the remaining 29 (37.2%) patients presented with severe disease. Although there was no difference in gender distribution between non-severe and severe groups, COVID-19 patients presenting with severe clinical status were older [median age 50 years (IQR: 36–66) vs 30 years (IQR: 26–37); p<0.00001]. Patients with severe disease symptoms when compared to non-severe cases were more dyspneic (86.2% vs 10.2%), had more cough (82.8% vs 24.5%), fever (55.2% vs 14.3%), headache (41.4% vs 18.4%), chest pain (24.0% vs 2.0%), sore throat (17.2% vs 2.0%), and myalgia ((17.2% vs 2.0%). Nasal congestion, diarrhea, and loss of smell and/or taste were not frequent in both patient groups. Patients with severe COVID-19 were significantly more likely to be tachypneic when compared to those with non-severe disease [median 29 (IQR: 28–31] vs 20 (IQR: 18–22) breaths/minute; p<0.00001]. Likewise, patients with severe disease were significantly more likely to be tachycardic when compared to those with non-severe cases [median 105 (IQR: 98–112] vs 76 (IQR: 73–83) beats/minute; p<0.00001]. Lymphocyte count was also significantly lower among severe COVID-19 patients compared to those with non-severe clinical manifestations. Comorbidities were significantly higher among severe COVID-19 cases when compared to non-severe (65.5% vs 4.1%; p<0.0001). In addition, COVID-19 patients with severe disease have more NCDs than non-severe cases (55.2% vs 4.1%; p<0.0001). Moreover, all severe cases of COVID-19 patients were admitted to the intensive care unit and received supplemental oxygen therapy, or mechanical ventilation (Table 1).
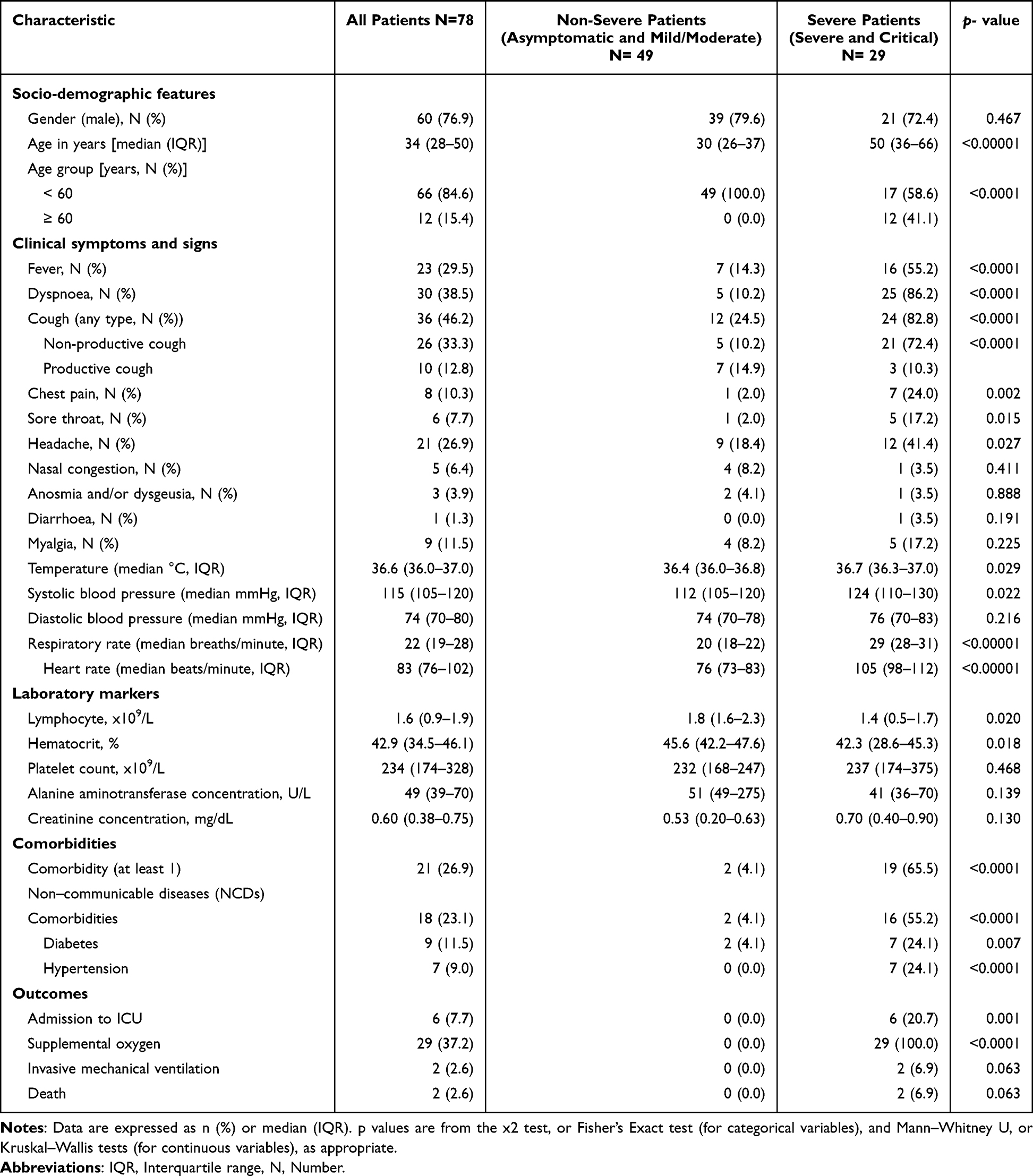 |
Table 1 Baseline Socio-Demographic and Clinical Characteristics of COVID-19 Patients |
Kinetics of CRP Levels Among COVID-19 Patients
As shown in Figure 1A, PCR-confirmed COVID-19 patients had significantly elevated CRP at baseline when compared to PCR-negative controls [median 11.1 (IQR: 2.0–127.8) mg/L vs 0.9 (IQR: 0.5–1.9) mg/L; p=0.0004)]. Moreover, COVID-19 patients with non-severe clinical presentation had higher levels of CRP compared to PCR-negative controls [median 2.4 (IQR: 1.2–7.6) mg/L vs 0.9 (IQR: 0.5–1.9) mg/L; p=0.0007)]. Those with severe COVID-19 clinical presentation had significantly higher median CRP levels compared to those with non-severe cases [166.1 (IQR: 48.6–332.5) mg/L vs 2.4 (IQR: 1.2–7.6) mg/L; p<0.00001)].
 |
Figure 1 CRP levels among PCR-negative controls, PCR-confirmed COVID-19 patients, and COVID-19 patients stratified by severity status (A); kinetics of CRP levels following symptom onset and during hospitalization (B), and stratified by severity status (C). Data are median and 25% to 75% interquartile ranges. Heat-map plot analysis of CRP levels of COVID-19 patients clustered according to severity status (D). |
The Kinetics of CRP levels is shown in Figure 1B–D. Overall, COVID-19 patients exhibited higher median CRP levels at baseline [58 (IQR: 2.0–127.8) mg/L] that decreased significantly to 4.7 (IQR: 1.5–31.5) mg/L after day 7 to 10 after the onset of symptom(s) (p<0.0001), and to 2.4 (IQR: 1.4–3.9) mg/L after 40 days after symptom onset (p<0.0001). Nonetheless, severe cases had significantly elevated median CRP levels at admission [83.1 (IQR: 62.6–258.7) mg/L], maintained at > 30 mg/L up until day 7 post symptom onset, and decreased slowly during hospitalization significantly to a median of 3.0 (IQR: 1.8–9.6) mg/L after 40 days of symptom onset (p<0.0001 for trend) (Figure 1C). Non-severe COVID-19 patients exhibited low-level CRP levels throughout the disease. Notably, persistently elevated levels of CRP were exhibited among those with comorbidities and higher age groups (Figure 1D). In addition, the proportion of COVID-19 patients with elevated CRP levels is higher in severe cases when compared to non-severe patients considering CRP levels at cut-off values of 3.0, 8.0, 30.0, and 50.0 mg/L (Figure 2). In the severe group, over 40% of patients had persistently elevated CRP levels up until day 30 following symptom onset (Figure 2). Six patients with severe COVID-19 admitted to the ICU (of whom two died) exhibited persistently elevated CRP levels throughout the disease (Figure 3).
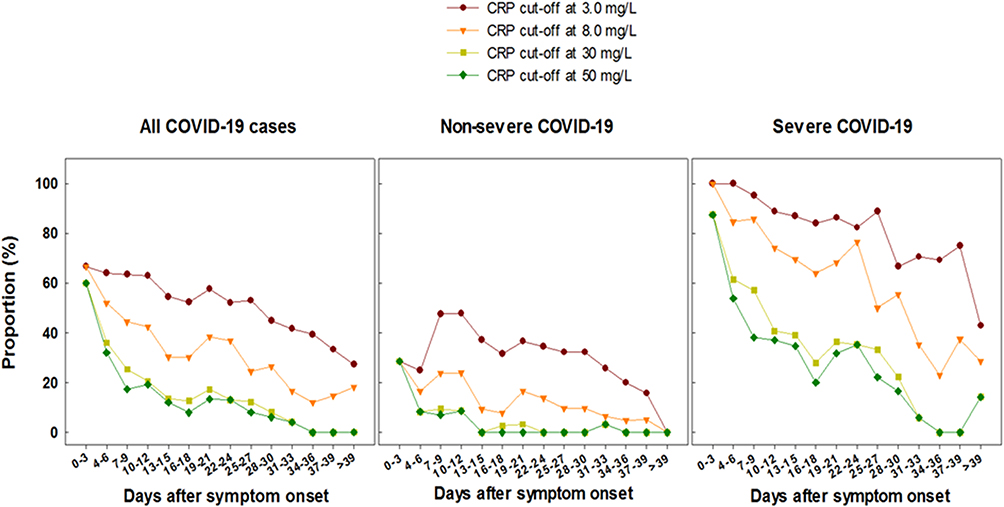 |
Figure 2 Kinetics of CRP levels in all, non-severe and severe COVID-19 patients at different CRP cut-off values. |
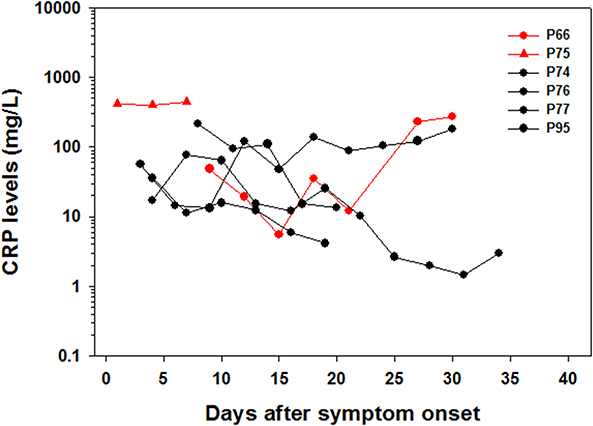 |
Figure 3 Kinetics of CRP levels in six COVID-19 patients admitted to the ICU. The red lines represent two patients who died during follow-up. Black lines denote 4 patients admitted to the ICU, but who survived. |
To assess the diagnostic value of CRP, we initially determined the AUC and compared the CRP levels in PCR-confirmed COVID-19 patients and PCR-negative controls. For this comparison, we considered CRP level >1.0 mg/L as an increased CRP level, based on our previous results obtained by determining CRP level in the general population in Ethiopia. Of note, PCR-negative controls in our study had a median CRP level of 0.9 (IQR: 0.5–1.9) mg/L, which is similar to the median CRP level of 0.8 mg/L obtained from the population-based study in Ethiopia. ROC analysis of CRP levels distinguished PCR-confirmed COVID-19 patients from the ones with PCR-negative non-COVID-19 individuals, with an AUC value of 0.77 (95% CI: 0.68–0.84; p=0.001; 76.7% sensitivity and 76.3% specificity) (Figure 4A). In addition, we further determined the performance of CRP levels in distinguishing severe from non-severe COVID-19. Here, we considered a cut-off of 30 mg/L. Thus, ROC analysis distinguished severe from non-severe COVID-19 patients, with an AUC value of 0.83 (95% CI: 0.73–0.91; p=0.001; 77.4% sensitivity and 84% specificity) (Figure 4B).
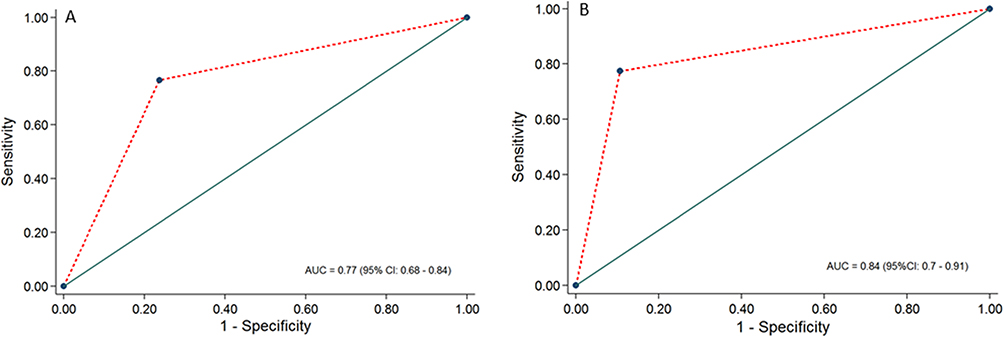 |
Figure 4 AUCs analysis of CRP between PCR-confirmed COVID-19 patients and PCR-negative controls (A), and between severe and non-severe COVID-19 patients (B). |
After adjusting for age and the presence of comorbidities, the multivariate Poisson regression analysis showed that CRP levels ≥ 8 mg/L were significantly associated with an increased risk of developing severe COVID-19 (AOR 3.99 (95% CI: 1.35–11.82), p=0.013 (Table 2).
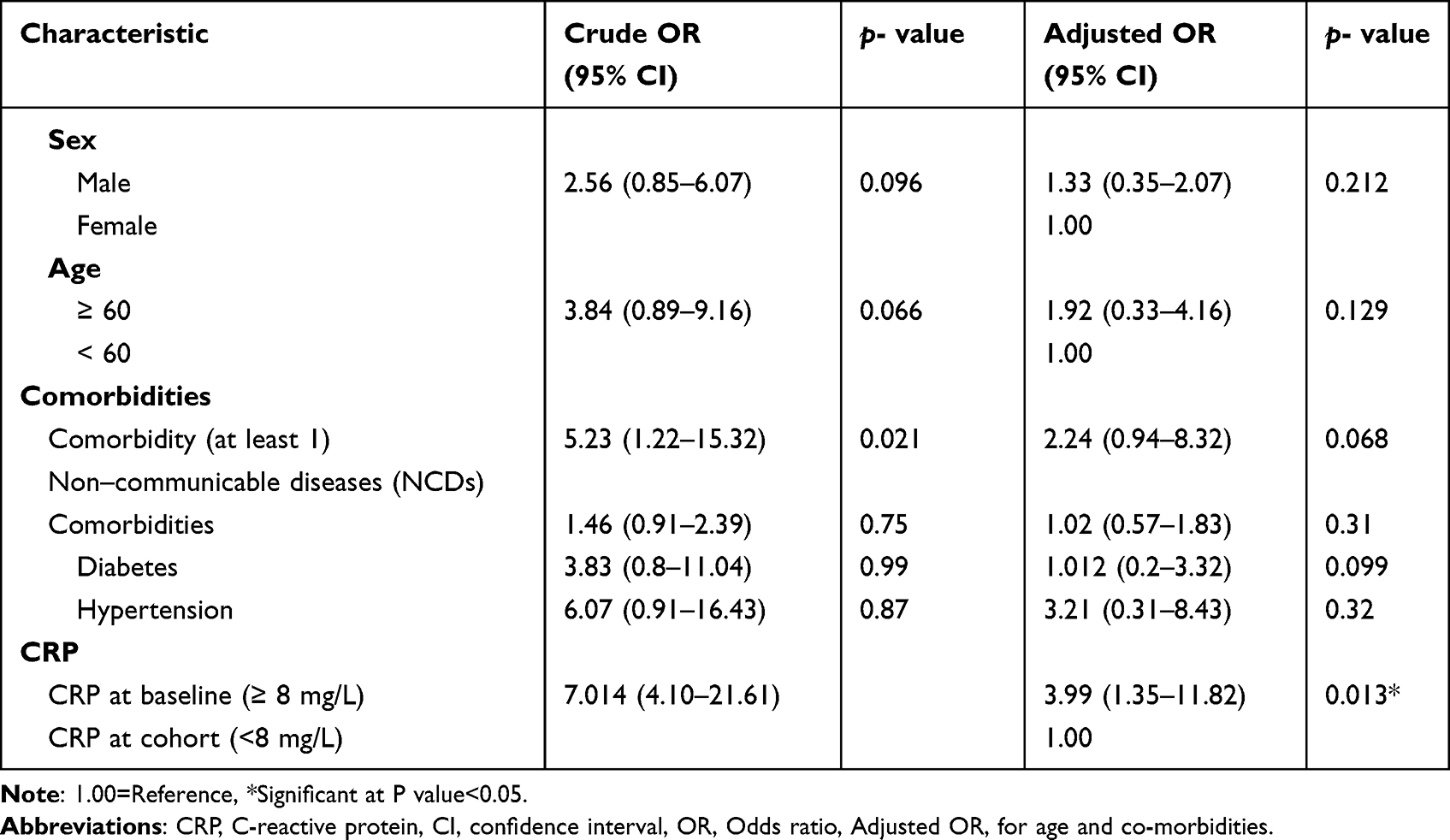 |
Table 2 Factors Associated with the Risk of Developing Severe COVID-19 Disease |
Discussion
Several reports have demonstrated that inflammatory cytokines, such as IL-6 serve as a surrogate risk biomarker for severe COVID-19.13,14,16,18–20 However, determining such biomarkers is not easy in a setting of SSA like Ethiopia. Thus, simple, readily available, and inexpensive biomarkers for assessing the degree of severity of COVID-19 patients in Ethiopia are urgently needed. CRP is such a biomarker that can easily and promptly be determined to assess the severity status of COVID-19 patients for immediate assessment in Ethiopia, including monitoring of any therapeutic intervention.
In this study, we determined CRP levels in SARS-CoV-2 PCR-negative individuals as well as COVID-19 patients from Ethiopia with a different spectrum of clinical severity. Our results extend findings from earlier reports that CRP level in COVID-19 patients is in general elevated when compared to healthy controls,25 as well as it is significantly increased in severe than in non-severe COVID-19 patients.23–29 Among the symptomatic cohort participants, the most common symptoms noted at presentation were dyspneic, had more cough, fever, headache, chest pain, sore throat, and myalgia. This was similar to the findings of studies from Nigeria37 and South Africa.38 We noted that the risk of developing severe COVID-19 in patients with baseline 8 mg/L or above is increased significantly by around 4-fold when compared to those below 8 mg/L. In addition, we observed a significant elevation of CRP in those with comorbidities, particularly those with NCDs were more prevalent than communicable diseases, indicating a more intense induction of hyperinflammation. This is in line with previous studies of Fachri et al,39 and Chen et al,27 who showed CRP were increased in COVID-19 patients co-infected by NCDs.
To the best of our knowledge, this is the first study to analyze the longitudinal profile of CRP among hospitalized COVID-19 patients with different categories of clinical spectrum in the setting of SSA. We demonstrated that the CRP levels are persistently elevated in COVID-19 patients that require ICU admission, including those who died. Our findings are in line with those reported previously from other non-African settings.24–29 Hence, special attention should be taken to identify such cases to provide necessary intervention and to reduce morbidity and mortality.
Analysis of the receiver operating characteristic curve was found to be an independent distinguishing factor for severe COVID-19 patients with a cut-off of 30 mg/L from non-severe cases. This is lower than previous reports by Stringer et al, CRP > 40 mg/L,40 and Sadeghi et al, CRP >64.75 mg/L.41 This indicates that the performance of CRP in predicting severe COVID-19 patients is better than the previous studies with an AUC value of 0.83 (95% CI: 0.73–0.91; p=0.001; 77.4% sensitivity and 89.4% specificity). In addition to assessing CRP level as a risk biomarker for categorizing COVID-19 patient severity, determining longitudinal CRP levels is relevant in assessing response to therapeutic intervention. Indeed, treatment of severe COVID-19 patients with an anti-IL-6 monoclonal antibody, tocilizumab, showed a significant reduction in CRP level, from 75.1 mg/L at baseline to 2.7 mg/L at day 5 post tocilizumab therapy.42
The present study showed the success of CRP in distinguishing PCR-confirmed COVID-19 patients from these PCR-negative non-COVID-19 individuals with an AUC value of 77%, 76.7% sensitivity, and 76.3% specificity. Huyut et al have noted the diagnostic performances of CRP with an AUC value of 73.4% as an effective predictive biomarker of COVID-19 mortality.31 Numerous other studies have shown that CRP and other routine immunological and hematological parameters could be the most effective diagnostic markers of COVID-19 patients.32,43,44
The strength of the study includes a prospective study design with longitudinal follow-up of CRP level allowed us to monitor the severity of COVID-19 during follow-up. Nonetheless, the small sample size and lack of comparative assessment of other biomarkers are considered shortcomings of the study.
Conclusion
We have shown that CRP levels are significantly elevated among COVID-19 patients compared to PCR-negative controls and that CRP levels were significantly elevated in severe than in non-severe COVID-19 patients. CRP was found to be an independent distinguishing factor for severe COVID-19 patients with a cut-off of 30 mg/L from non-severe cases. In addition, persistently elevated CRP levels were associated with the risk of developing severe COVID-19 including the requirement for admission to the ICU and death. Determining CRP levels in COVID-19 patients in the SSA setting may provide a simple, prompt, and inexpensive assessment of the severity status at baseline and monitoring of treatment outcomes.
Data Sharing Statement
The data used to support the findings of this study are included in the article.
Ethics Approval and Consent to Participate
Participants enrolled provided written consent to participate in the Profile-CoV study. The study protocol was reviewed and approved by the Health Research Ethics Review Committee of Mekelle University College of Health Sciences (#ERC 1769/2020) and the Ethiopian Public Health Institute (#EPHI 6.13/814). The study did not use any personal patient information, and all data were kept confidential following the revised Declaration of Helsinki.
Acknowledgments
We would like to express our gratitude to the staff of the Quiha COVID-19 Isolation and Treatment Centre, Mekelle University College of Health Sciences and Clinical Chemistry Department, at Ethiopian Public Health Institute for their commitment to caring for the patients, and combatting COVID-19 in Ethiopia.
Funding
This research was supported by grants from the European and Developing Countries Clinical Trials Partnership (EDCTP), supported by the European Union (RIA-2020EF-2095) and Joep Lange Institute for Global Health and Development, The Netherlands.
Disclosure
The authors have no competing interests to declare
References
1. Lemos S, Solari PN. John Hopkins got incidence rate wrong: a close look at John Hopkins University’s web-based interactive dashboard for real-time tracking of COVID-19. Johns Hopkins Coronavirus Resource Center (jhu.edu); 2023.
2. Guan W, Ni Z, Hu Y, et al. Clinical characteristics of coronavirus disease. N Engl J Med. 2019;2019:1708–1720.
3. de Lemos JA, McGuire DK, Drazner MH. B-type natriuretic peptide in cardiovascular disease. Lancet. 2003;362(9380):316–322. doi:10.1016/S0140-6736(03)13976-1
4. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
5. Richardson S, Hirsch JS, Narasimhan M, et al. Presenting characteristics, comorbidities, and outcomes among 5700 patients hospitalized with COVID-19 in the New York City area. JAMA. 2020;323(20):2052–2059. doi:10.1001/jama.2020.6775
6. Wu Z, McGoogan JM. Characteristics of and important lessons from the coronavirus disease 2019 (COVID-19) outbreak in China: summary of a report of 72 314 cases from the Chinese Center for disease control and prevention. JAMA. 2020;323(13):1239–1242. doi:10.1001/jama.2020.2648
7. Zhou F, Yu T, Du R, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. 2020;395(10229):1054–1062. doi:10.1016/S0140-6736(20)30566-3
8. Yang X, Yu Y, Xu J, et al. Clinical course and outcomes of critically ill patients with SARS-CoV-2 pneumonia in Wuhan, China: a single-centered, retrospective, observational study. Lancet Respir Med. 2020;8(5):475–481. doi:10.1016/S2213-2600(20)30079-5
9. Abraha HE, Gessesse Z, Gebrecherkos T, et al. Clinical features and risk factors associated with morbidity and mortality among patients with COVID-19 in northern Ethiopia. Int J Infect Dis. 2021;105:776–783. doi:10.1016/j.ijid.2021.03.037
10. Nachega JB, Ishoso DK, Otokoye JO, et al. Clinical characteristics and outcomes of patients hospitalized for COVID-19 in Africa: early insights from the Democratic Republic of the Congo. Am J Trop Med Hyg. 2020;103(6):2419. doi:10.4269/ajtmh.20-1240
11. Moore JB, June CH. Cytokine release syndrome in severe COVID-19. Science. 2020;368(6490):473–474. doi:10.1126/science.abb8925
12. Tay M, Poh C, Nia LRX, MacAry PA, Ng LFP. The trinity of 467 COVID-19: immunity, inflammation and intervention. Nat Rev Immunol. 2020;20:363–374. doi:10.1038/s41577-020-0311-8
13. Chen G, Wu D, Guo W, et al. Clinical and immunological features of severe and moderate coronavirus disease 2019. J Clin Investig. 2020;130(5):2620–2629. doi:10.1172/JCI137244
14. Xu Z, Shi L, Wang Y, et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. Lancet Respir Med. 2020;8(4):420–422. doi:10.1016/S2213-2600(20)30076-X
15. Qin C, Zhou L, Hu Z, et al. Dysregulation of immune response in patients with coronavirus 2019 (COVID-19) in Wuhan, China. Clin Infect Dis. 2020;71(15):762–768. doi:10.1093/cid/ciaa248
16. Lucas C, Wong P, Klein J, et al. Longitudinal analyses reveal immunological misfiring in severe COVID-19. Nature. 2020;584(7821):463–469. doi:10.1038/s41586-020-2588-y
17. Mathew D, Giles JR, Baxter AE, et al. Deep immune profiling of COVID-19 patients reveals distinct immunotypes with therapeutic implications. Science. 2020;369(6508):eabc8511. doi:10.1126/science.abc8511
18. D’Alessandro A, Thomas T, Dzieciatkowska M, et al. Serum proteomics in COVID-19 patients: altered coagulation and complement status as a function of IL-6 level. J. Proteome Res. 2020;19(11):4417–4427. doi:10.1021/acs.jproteome.0c00365
19. Jose RJ, Manuel A. COVID-19 cytokine storm: the interplay between inflammation and coagulation. Lancet Respir Med. 2020;8(6):e46–e47. doi:10.1016/S2213-2600(20)30216-2
20. Giamarellos-Bourboulis EJ, Netea MG, Rovina N, et al. Complex immune dysregulation in COVID-19 patients with severe respiratory failure. Cell Host Microbe. 2020;27(6):992–1000. doi:10.1016/j.chom.2020.04.009
21. Lee DW, Gardner R, Porter DL, et al. Current concepts in the diagnosis and management of cytokine release syndrome. Am J Hematol. 2014;124(2):188–195.
22. Pepys MB, Hirschfield GM. C-reactive protein: a critical update. J Clin Investig. 2003;111(12):1805–1812. doi:10.1172/JCI200318921
23. Liu F, Li L, Xu M, et al. Prognostic value of interleukin-6, C-reactive protein, and procalcitonin in patients with COVID-19. J Clin Virol. 2020;127:104370. doi:10.1016/j.jcv.2020.104370
24. Herold T, Jurinovic V, Arnreich C, et al. Elevated levels of IL-6 and CRP predict the need for mechanical ventilation in COVID-19. J Allergy Clin Immunol. 2020;146(1):128–136. doi:10.1016/j.jaci.2020.05.008
25. Han H, Ma Q, Li C, et al. Profiling serum cytokines in COVID-19 patients reveals IL-6 and IL-10 are disease severity predictors. Emerg Microbes Infect. 2020;9(1):1123–1130. doi:10.1080/22221751.2020.1770129
26. Bergantini L, Bargagli E, d’Alessandro M. d’Alessandro M, et al. Prognostic bioindicators in severe COVID-19 patients. Cytokine. 2021;141:155455. doi:10.1016/j.cyto.2021.155455
27. Chen W, Zheng KI, Liu S, Yan Z, Xu C, Plasma QZ. CRP level is positively associated with the severity of COVID-19. Ann Clin Microbiol Antimicrob. 2020;19(1):1–7. doi:10.1186/s12941-020-00362-2
28. Tan C, Huang Y, Shi F, et al. C‐reactive protein correlates with computed tomographic findings and predicts severe COVID‐19 early. J Med Virol. 2020;92(7):856–862. doi:10.1002/jmv.25871
29. Bhargava A, Fukushima EA, Levine M, et al. Predictors for severe COVID-19 infection. Clin Infect Dis. 2020;71(8):1962–1968. doi:10.1093/cid/ciaa674
30. Wang G, Wu C, Zhang Q, et al. C-reactive protein level may predict the risk of COVID-19 aggravation.
31. Huyut MT, Huyut Z, Ilkbahar F, Mertoğlu C. What is the impact and efficacy of routine immunological, biochemical and hematological biomarkers as predictors of COVID-19 mortality? Int Immunopharmacol. 2022;105:108542. doi:10.1016/j.intimp.2022.108542
32. Huyut MT, Ilkbahar F. The effectiveness of blood routine parameters and some biomarkers as a potential diagnostic tool in the diagnosis and prognosis of Covid-19 disease. Int Immunopharmacol. 2021;98:107838. doi:10.1016/j.intimp.2021.107838
33. Mertoglu C, Huyut MT, Arslan Y, Ceylan Y, Coban TA. How do routine laboratory tests change in coronavirus disease 2019? Scand J Clin Lab Invest. 2021;81(1):24–33. doi:10.1080/00365513.2020.1855470
34. Challa F, Gelibo T, Getahun T, et al. Distribution and determinants of serum high-sensitivity C-reactive protein in Ethiopian population. Clin Chim Acta. 2021;517:99–107. doi:10.1016/j.cca.2021.02.013
35. International Severe Acute Respiratory and Emerging Infection Consortium, COVID- 19 CRF ISARIC. Clinical data collection – the COVID-19 Case Report Forms (CRFs); 2020. Available from: https://isarictghnorg/COVID-19-CRF/.
36. Haran G, Cohen R, Bar LK, Barenholz Y. Transmembrane ammonium sulfate gradients in liposomes produce efficient and stable entrapment of amphipathic weak bases. Biochimica et biophysica acta. 1993;1151(2):201–215. doi:10.1016/0005-2736(93)90105-9
37. Abayomi A, Odukoya O, Osibogun A, et al. Presenting symptoms and predictors of poor outcomes among 2184 patients with COVID-19 in Lagos State, Nigeria. Int J Infect Dis. 2021;102:226–232. doi:10.1016/j.ijid.2020.10.024
38. Parker A, Koegelenberg CF, Moolla MS, et al. High HIV prevalence in an early cohort of hospital admissions with COVID-19 in Cape Town, South Africa. SAMJ. 2020;110(9):1. doi:10.7196/SAMJ.2020.v110i10.15067
39. Fachri M, Hatta M, Widowati E, et al. Correlations between comorbidities, chest x-ray findings, and C-Reactive protein level in patients with COVID-19. Ann Med Surg. 2022;77:103553. doi:10.1016/j.amsu.2022.103553
40. Stringer D, Braude P, Myint PK, et al. The role of C-reactive protein as a prognostic marker in COVID-19. Int J Epidemiol. 2021;50(2):420–429. doi:10.1093/ije/dyab012
41. Sadeghi-Haddad-Zavareh M, Bayani M, Shokri M, et al. C-reactive protein as a prognostic indicator in COVID-19 patients. Interdiscip Perspect Infect Dis. 2021;2021:1–5. doi:10.1155/2021/5557582
42. Xu X, Han M, Li T, et al. Effective treatment of severe COVID-19 patients with tocilizumab. Proc Natl Acad Sci. 2020;117(20):10970–10975. doi:10.1073/pnas.2005615117
43. Huyut MT, Velichko A. Diagnosis and Prognosis of COVID-19 disease using routine blood values and LogNNet neural network. Sensors. 2022;22(13):4820. doi:10.3390/s22134820
44. Huyut M. Automatic detection of severely and mildly infected COVID-19 patients with supervised machine learning models. IRBM. 2023;44(1):100725. doi:10.1016/j.irbm.2022.05.006
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
COVID-19 and Saudi Arabia: Awareness, Attitude, and Practice
Fawzy MS, AlSadrah SA
Journal of Multidisciplinary Healthcare 2022, 15:1595-1618
Published Date: 26 July 2022
Comparison of the Diagnostic Performance of a Rapid Antigen Test with Real-Time Polymerase Chain Reaction for Detection of SARS-CoV-2 Among Patients Diagnosed with COVID-19 at Selected Hospitals in Addis Ababa, Ethiopia
Desalegn Z, Sebre S, Yohannes M, Seman A, Shiferaw W, Ademe M, Biazin H, Firdawoke E, Asemamaw Y, Teka B, Teshome S, Amogne W, Addissie A, Gebrehiwot Y, Kantelhardt E, Abebe T
Infection and Drug Resistance 2022, 15:4299-4305
Published Date: 6 August 2022
A Pilot Study of 0.4% Povidone-Iodine Nasal Spray to Eradicate SARS-CoV-2 in the Nasopharynx
Sirijatuphat R, Leelarasamee A, Puangpet T, Thitithanyanont A
Infection and Drug Resistance 2022, 15:7529-7536
Published Date: 21 December 2022
Distinct Features of Vascular Diseases in COVID-19
Ceasovschih A, Sorodoc V, Shor A, Haliga RE, Roth L, Lionte C, Onofrei Aursulesei V, Sirbu O, Culis N, Shapieva A, Tahir Khokhar MA, Statescu C, Sascau RA, Coman AE, Stoica A, Grigorescu ED, Banach M, Thomopoulos C, Sorodoc L
Journal of Inflammation Research 2023, 16:2783-2800
Published Date: 6 July 2023
Re-Emerging COVID-19: Controversy of Its Zoonotic Origin, Risks of Severity of Reinfection and Management
Chala B, Tilaye T, Waktole G
International Journal of General Medicine 2023, 16:4307-4319
Published Date: 20 September 2023