Back to Journals » Cancer Management and Research » Volume 18

Pretreatment Prognostic Nutritional Index Predicts Progression-Free Survival in BCLC Stage C Hepatocellular Carcinoma Treated with Sorafenib
Authors Aydın U ![]() , Dikilitaş M, Balıkçı Çiçek İ
, Dikilitaş M, Balıkçı Çiçek İ ![]() , Pamuk ÖA, Sadak Öcal Z, Danacı Y, Alizade E
, Pamuk ÖA, Sadak Öcal Z, Danacı Y, Alizade E
Received 4 May 2026
Accepted for publication 3 July 2026
Published 14 July 2026 Volume 2026:18 621105
DOI https://doi.org/10.2147/CMAR.S621105
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Lei Zhu
Video abstract of “Survival in Hepatocellular Carcinoma Treated With Sorafenib” [621105].
Views: 5
Umut Aydın,1 Mustafa Dikilitaş,1 İpek Balıkçı Çiçek,2 Ömer Arif Pamuk,3 Zehra Sadak Öcal,4 Yurdagül Danacı,1 Elanaz Alizade5
1Department of Medical Oncology, Faculty of Medicine, İnönü University, Malatya, Turkey; 2Department of Biostatistics and Medical Informatics, Faculty of Medicine, İnönü University, Malatya, Turkey; 3Department of Medical Oncology, Faculty of Medicine, Fırat University, Elazığ, Turkey; 4Department of Medical Oncology, Bingöl State Hospital, Bingöl, Turkey; 5Department of Internal Medicine, Faculty of Medicine, Eskişehir Osmangazi University, Eskişehir, Turkey
Correspondence: Umut Aydın, Department of Medical Oncology, Faculty of Medicine, Inonu University, Malatya, Turkey, Email [email protected]; [email protected]
Background: Systemic inflammation and nutritional status are key determinants of tumor progression in advanced hepatocellular carcinoma (HCC). This study aimed to evaluate the prognostic significance of inflammation and nutrition based indices in patients with BCLC stage C HCC treated with sorafenib.
Methods: This retrospective cohort study included 109 patients with Barcelona Clinic Liver Cancer (BCLC) stage C HCC who received sorafenib as first line systemic therapy. A complete-case approach was used for multivariate Cox regression analysis. Progression-free survival (PFS) was defined according to RECIST version 1.1. Kaplan–Meier survival analysis and Cox proportional hazards regression models were used to assess prognostic factors.
Results: In Kaplan–Meier and univariate Cox analyses, several inflammation- and nutrition-based indices, including NLR, PLR, SII, mGPS, PI, and ALBI grade, were significantly associated with PFS. Although the total cohort included 109 patients, the final multivariate Cox regression model for PNI included 78 complete-case patients. In this model, low prognostic nutritional index (PNI) (HR: 2.36, 95% CI: 1.14– 4.87, p=0.020) and prior local ablative treatment (HR: 0.45, 95% CI: 0.24– 0.83, p=0.011) remained independently associated with PFS.
Conclusion: Pretreatment low PNI was independently associated with shorter progression-free survival in patients with BCLC stage C HCC treated with sorafenib. Other inflammation and nutrition-based indices were associated with PFS in univariate analyses but did not retain independent prognostic significance after adjustment. PNI may serve as a simple prognostic marker for risk stratification in real-world settings, although external validation is required.
Keywords: Hepatocellular carcinoma, BCLC stage C, prognosis, progression-free survival, PNI, NLR, PLR, SII, ALBI, mGPS, PI, sorafenib
Introduction
Hepatocellular carcinoma (HCC) is the most common primary malignancy of the liver and represents a major cause of cancer-related mortality worldwide.1 A substantial proportion of patients are diagnosed at an advanced stage, at which curative treatment options such as surgical resection, liver transplantation, or local ablative therapies are no longer feasible. Consequently, systemic therapy constitutes the mainstay of treatment for patients with advanced disease.2,3
Chronic inflammation and impaired nutritional status are fundamental components of hepatocarcinogenesis and tumor progression. Persistent liver inflammation, most commonly related to viral hepatitis, alcohol-associated liver disease, or metabolic dysfunction-associated steatotic liver disease, promotes genomic instability, immune dysregulation, and a pro-tumorigenic microenvironment.4–6
In recent years, several inflammation- and nutrition-based indices derived from routine laboratory parameters have been developed to quantify systemic inflammatory response and host nutritional status. Among these, the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), systemic immune-inflammation index (SII), albumin–bilirubin (ALBI) grade, modified Glasgow Prognostic Score (mGPS), prognostic nutritional index (PNI), and prognostic index (PI) have been widely investigated as potential prognostic markers in patients with HCC. Previous studies have demonstrated associations between these indices and clinical outcomes across different disease stages and treatment settings; however, their relative and independent prognostic value in advanced-stage HCC remains incompletely defined.7,8
Although immunotherapy-based combinations and lenvatinib are currently recommended as preferred first-line systemic therapies for advanced HCC, access to these agents may be limited in real-world clinical practice due to reimbursement policies, regional availability, or patient-related factors. In such settings, sorafenib continues to represent a clinically relevant treatment option, particularly in resource-constrained environments.9,10
PFS was selected as the primary outcome because it directly reflects disease control during sorafenib treatment and is less affected than overall survival by subsequent therapies, heterogeneous post-progression management, and non-cancer-related mortality in a retrospective real-world cohort. Therefore, the aim of the present study was to evaluate the prognostic significance of inflammation and nutrition-based indices in patients with Barcelona Clinic Liver Cancer (BCLC) stage C hepatocellular carcinoma treated with sorafenib, with a specific focus on progression-free survival (PFS).
Materials and Methods
Study Population
This retrospective cohort study included 109 patients diagnosed with hepatocellular carcinoma (HCC) at İnönü University Turgut Özal Medical Center between January 2014 and December 2024. Only patients with Barcelona Clinic Liver Cancer (BCLC) stage C disease and Child–Pugh class A liver function were included. BCLC stage C was defined according to established BCLC criteria, including macrovascular invasion and/or extrahepatic spread in patients who were candidates for systemic therapy.
HCC diagnosis was established based on histopathological findings or characteristic radiological imaging features in accordance with established clinical guidelines. All patients received sorafenib as first-line systemic therapy due to limited access to immunotherapy-based regimens and lenvatinib at the time of treatment initiation. Sorafenib was administered orally at a standard dose of 400 mg twice daily. Dose reductions, treatment interruptions, and supportive management were performed at the discretion of the treating physician according to toxicity, patient tolerance, and routine clinical practice.
Data Collection
Demographic, clinical, and laboratory data were retrospectively collected from electronic medical records. Variables included age, sex, HCC etiology, maximum tumor diameter, presence of vascular invasion, cirrhosis status, and history of prior local ablative treatment.
Inflammation- and nutrition-based indices, including neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), systemic immune-inflammation index (SII), albumin–bilirubin (ALBI) grade, modified Glasgow Prognostic Score (mGPS), prognostic index (PI), and prognostic nutritional index (PNI), were calculated using baseline laboratory values obtained prior to initiation of sorafenib therapy. Definitions and calculation methods of inflammation- and nutrition-based prognostic indices are summarized in Table 1.
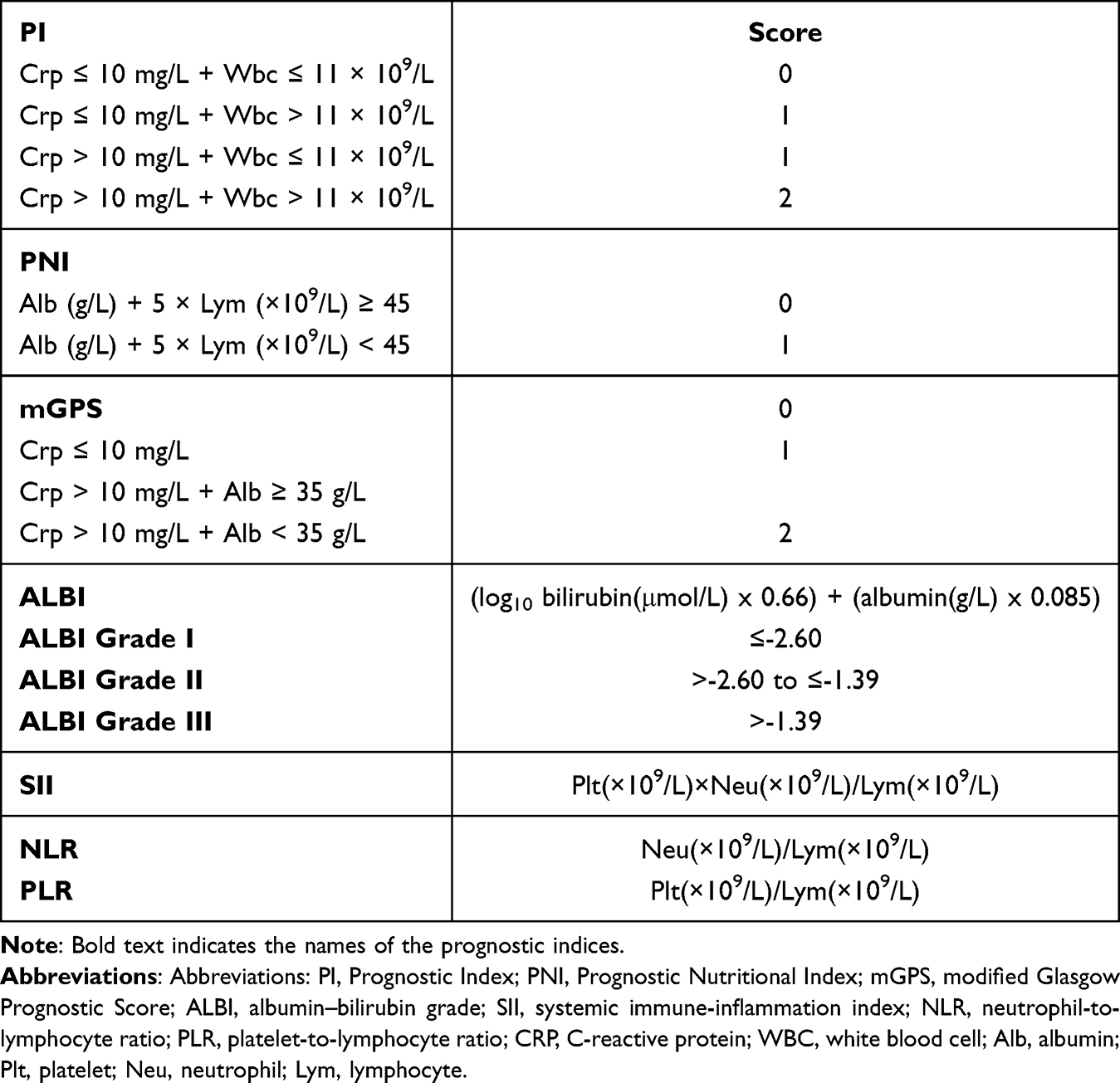 |
Table 1 Inflammation-Based Prognostic Scores |
Outcome Definition
Progression-free survival (PFS) was defined as the time from initiation of sorafenib treatment to radiologically confirmed disease progression or death from any cause. Tumor response and disease progression were evaluated according to Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1 by experienced radiologists blinded to clinical data.
Statistical Analysis
Categorical variables were summarized as frequencies and percentages, while continuous variables were expressed as mean ± standard deviation or median (minimum–maximum), depending on distribution. The normality of continuous variables was assessed using the Shapiro–Wilk test.
Kaplan–Meier survival analysis with Log rank testing was used to compare progression-free survival across predefined groups. Univariate Cox proportional hazards regression analyses were performed to assess the association between individual variables and PFS. Because multiple inflammation- and nutrition-based indices were evaluated, the univariate analyses were considered exploratory.
Multivariate Cox proportional hazards regression models were constructed to identify independent prognostic factors. Each inflammation- or nutrition-based index was evaluated in a separate multivariate Cox regression model adjusted for clinically relevant covariates, including age, maximum tumor diameter (≥5 cm), presence of vascular invasion, cirrhosis status, and history of local ablative treatment. A complete-case approach was used for multivariate Cox regression analysis; therefore, only patients with complete data for all covariates included in each model were analyzed.
The number of events and the events per variable (EPV) were calculated to assess the adequacy of the multivariate Cox regression models. Hazard ratios (HRs) and 95% confidence intervals (CIs) were calculated. A two-sided p-value <0.05 was considered statistically significant. All statistical analyses were performed using IBM SPSS Statistics version 26.0 (IBM Corp., Armonk, NY, USA).
Results
Baseline demographic and clinical characteristics of the study population are presented in Table 2. All patients had Barcelona Clinic Liver Cancer (BCLC) stage C disease and received sorafenib as first-line systemic therapy.
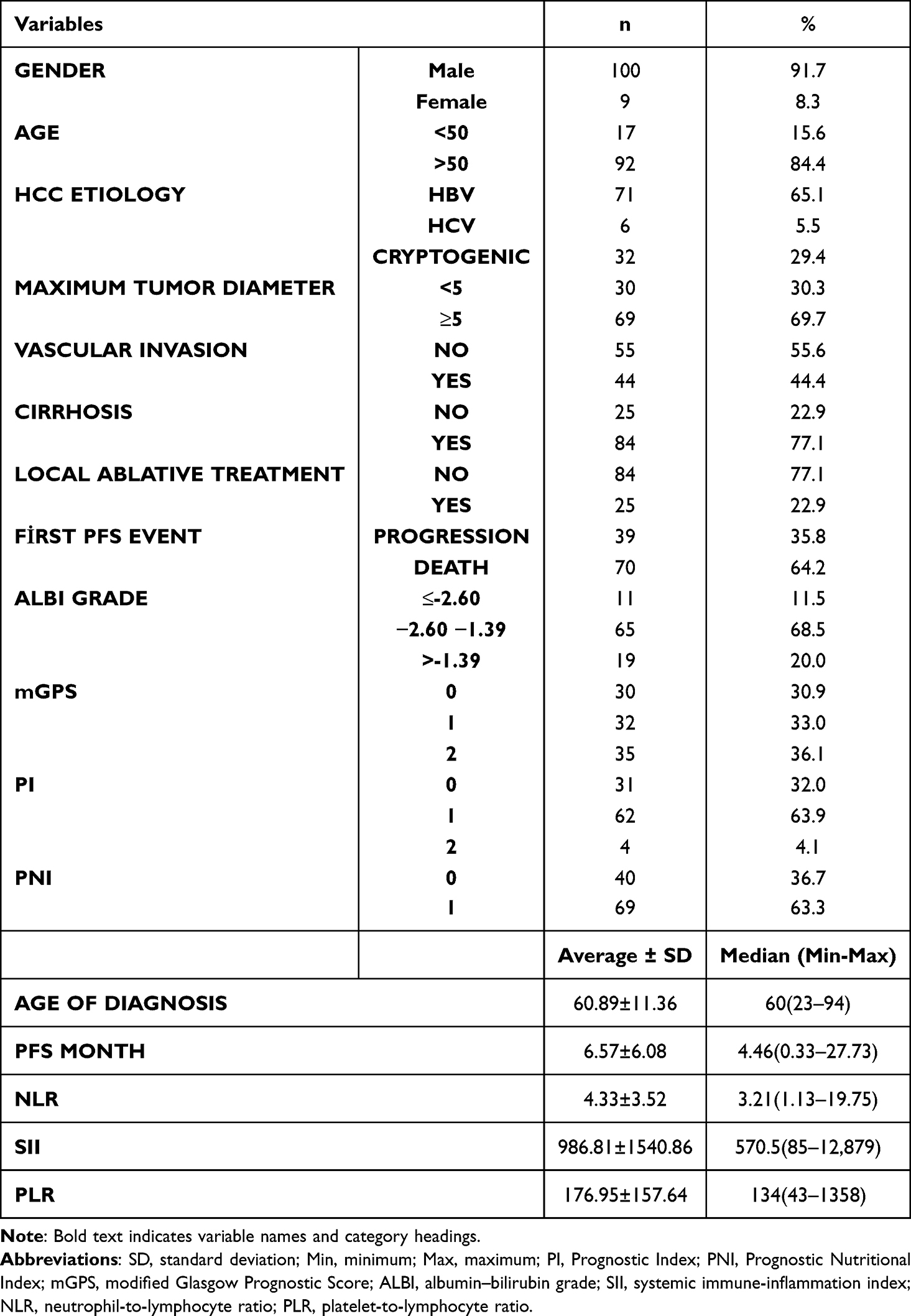 |
Table 2 Baseline Demographic, Clinical, and Laboratory Characteristics of Patients with Hepatocellular Carcinoma |
Missing data were observed for maximum tumor diameter and vascular invasion in 10 patients, ALBI grade in 14 patients, mGPS and PI in 12 patients, and PLR/SII in 1 patient. Therefore, multivariate Cox regression analyses were performed using a complete-case approach. Although the total cohort included 109 patients, the final multivariate Cox regression model for PNI included 78 patients with complete data for all covariates and 78 PFS events. The PNI model included six variables, resulting in an events-per-variable value of 13.
Kaplan–Meier survival analyses demonstrated significant differences in PFS according to several inflammation- and nutrition-based indices. Several inflammation- and nutrition-based indices, including NLR, PLR, SII, mGPS, PI, PNI, and ALBI grade, were significantly associated with PFS in Kaplan–Meier and/or univariate Cox analyses. Kaplan–Meier curves for mGPS, PI, PNI, and ALBI grade are shown in Figures 1–4. In addition, the presence of cirrhosis and the absence of prior local ablative treatment were associated with inferior PFS in Kaplan–Meier analyses (Table 3).
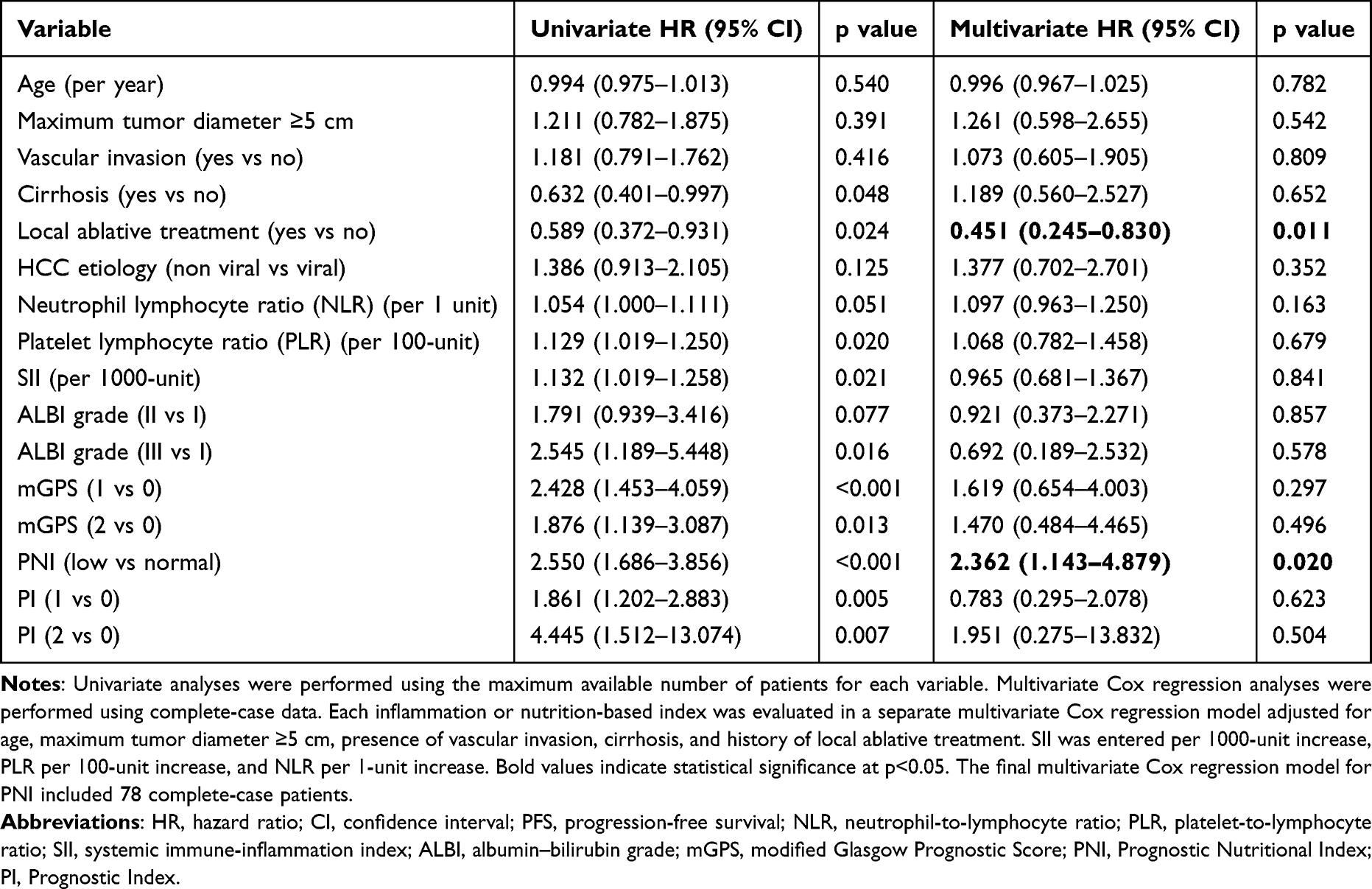 |
Table 3 Univariate and Multivariate Cox Regression Analyses for Progression-Free Survival |
 |
Figure 1 Kaplan–Meier curves for progression-free survival (PFS) stratified by the Modified Glasgow Prognostic Score (mGPS). Patients with an mGPS of 0 demonstrated longer PFS compared with those with mGPS scores of 1 and 2. Detailed survival data are provided in Table 3. |
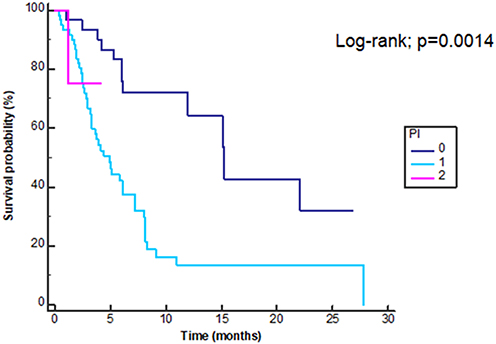 |
Figure 2 Kaplan–Meier curves for progression-free survival (PFS) stratified by the prognostic index (PI). Patients with a PI of zero demonstrated significantly longer PFS compared with those in the PI one and two groups. Detailed survival data are provided in Table 3. |
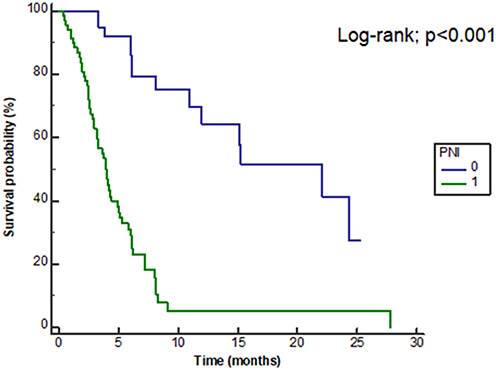 |
Figure 3 Kaplan–Meier curves for progression-free survival (PFS) stratified by the prognostic nutritional index (PNI). Patients with a PNI of 0 demonstrated significantly longer PFS compared with those with a PNI of 1. Detailed survival data are provided in Table 3. |
 |
Figure 4 Kaplan–Meier curves for progression free survival (PFS) according to albumin bilirubin (ALBI) grade. Worsening ALBI grade was associated with shorter progression-free survival. Detailed survival data are provided in Table 3. |
Univariate Cox proportional hazards regression analyses yielded results consistent with the Kaplan–Meier findings. Higher levels of inflammation-based indices and poorer nutritional status were associated with an increased risk of disease progression. Cirrhosis and history of local ablative treatment also demonstrated statistically significant associations with PFS in univariate Cox models (Table 3).
Multivariate Cox proportional hazards regression analyses were performed to identify independent prognostic factors for PFS (Table 3). After adjustment for clinically relevant tumor-related factors and liver function parameters, low PNI and history of local ablative treatment remained independently associated with PFS. The associations observed for other inflammation- and nutrition-based indices were attenuated and did not retain statistical significance after multivariable adjustment.
Discussion
In this retrospective cohort study, we evaluated the prognostic significance of inflammation- and nutrition-based indices in patients with BCLC stage C hepatocellular carcinoma treated with sorafenib. By using a hierarchical analytical approach, associations observed in Kaplan Meier and univariate Cox analyses were further examined in multivariate Cox regression models to determine independent prognostic factors for PFS.
Several inflammation and nutrition based indices, including NLR, PLR, SII, mGPS, PI, and ALBI grade, were significantly associated with PFS in univariate analyses. These findings are consistent with previous reports demonstrating the prognostic relevance of systemic inflammation and nutritional status across different stages and treatment settings in hepatocellular carcinoma. However, after adjustment for clinically relevant tumor related and liver function variables, the prognostic impact of most inflammation based indices was attenuated, suggesting overlapping biological information captured by these composite markers.11–15
Notably, low PNI remained independently associated with shorter PFS in multivariate analysis. PNI is a composite index reflecting both nutritional and immunological status and may capture host-related factors that are not fully represented by conventional tumor burden or liver function parameters. Advanced hepatocellular carcinoma is frequently accompanied by cancer-related cachexia, sarcopenia, and chronic cytokine-mediated catabolism. Elevated levels of proinflammatory cytokines such as interleukin-6 and tumor necrosis factor-α reduce albumin synthesis and lymphocyte counts, thereby compromising both nutritional status and antitumor immune responses. Impaired nutritional and immune status may reduce tolerance to systemic therapy and accelerate disease progression. Collectively, these findings suggest that PNI functions as a composite biomarker of biological resilience and support its role as a clinically meaningful prognostic marker in patients with advanced hepatocellular carcinoma.16–25
In addition, a history of local ablative treatment remained independently associated with improved PFS after multivariable adjustment. Prior locoregional therapy may identify a subgroup of patients with lower effective tumor burden or more favorable tumor biology, even within an advanced stage population. Furthermore, locoregional tumor control may contribute to delayed disease progression when combined with systemic therapy. These findings align with previous studies suggesting a benefit of multimodal treatment strategies in selected patients with advanced hepatocellular carcinoma.26,27
HCC develops in a chronically inflamed hepatic environment characterized by persistent cytokine activation, angiogenesis, immune dysregulation, and progressive parenchymal damage. In our cohort, viral hepatitis represented the predominant etiology, consistent with global epidemiologic data. Chronic inflammation contributes to tumor progression through genomic instability, immune escape, and enhanced metastatic potential.28–30
The presence of cirrhosis was associated with inferior PFS in univariate analyses but did not retain independent significance in multivariate models. This finding likely reflects the close interaction between cirrhosis and other liver function related variables included in the multivariate analysis, rather than a lack of clinical relevance of cirrhosis itself.31,32
Although immunotherapy based combinations and lenvatinib are currently recommended as preferred first line systemic therapies for advanced HCC, access to these agents may be limited in real world clinical practice due to reimbursement policies, regional availability, or patient-related factors. In such settings, sorafenib remains a relevant treatment option, and evaluating prognostic markers in patients treated with sorafenib continues to have clinical importance.33,34
Several limitations of this study should be acknowledged. First, the retrospective and single-center design may limit the generalizability of the findings and may introduce selection bias. Second, the relatively small sample size and missing data for some variables necessitated the use of a complete-case approach in multivariate analyses, which may have reduced statistical power and introduced potential bias if the missing data were not completely random. Third, multiple inflammation- and nutrition-based indices were evaluated, and the univariate analyses should therefore be interpreted as exploratory. Although each index was assessed in a separate multivariate model adjusted for clinically relevant covariates, the possibility of type I error due to multiple testing cannot be fully excluded.
Fourth, prior local ablative treatment was independently associated with improved PFS; however, this finding should be interpreted with caution. Patients who had previously received local ablative treatment may represent a subgroup with a more favorable tumor biology, lower initial tumor burden, or earlier disease detection before progression to BCLC stage C. Therefore, potential lead-time bias and selection bias related to prior local therapy cannot be excluded. Finally, this study did not include an external validation cohort. Independent validation in larger, multicenter cohorts is required before PNI can be incorporated into routine clinical decision-making as a prognostic marker in patients with advanced HCC treated with sorafenib.
Conclusion
In patients with BCLC stage C hepatocellular carcinoma treated with sorafenib, pretreatment low PNI was independently associated with shorter progression-free survival after adjustment for clinically relevant covariates. Other inflammation and nutrition-based indices were associated with PFS in univariate analyses but did not retain independent prognostic significance after multivariable adjustment. These findings suggest that PNI may serve as a simple and readily available prognostic marker for risk stratification in real-world clinical practice. However, external validation in larger, multicenter cohorts is required before routine clinical implementation.
Use of Artificial Intelligence Tools
The authors used artificial intelligence based language editing tools solely to improve the clarity and readability of the manuscript. No AI tools were used for data analysis, data interpretation, or generation of scientific conclusions. All authors take full responsibility for the accuracy and integrity of the content.
Abbreviations
HCC, Hepatocellular Carcinoma; HBV, Hepatitis B; HCV, Hepatitis C; BCLC, Barcelona Clinic Liver Cancer; VEGFR, Vascular Endothelial Growth Factor Receptor; PDGFR, Platelet Derived Growth Factor Receptor; PI, Prognostic Index; PNI, Prognostic Nutritional Index; mGPS, Modified Glasgow Prognostic Score; ALBI, Albumin Bilirubin Index; NLR, Neutrophil Lymphocyte Ratıo; PLR, Platelet Lymphocyte Ratıo; HR, Hazard ratio; ICI, Immune Checkpoint İnhibitor; GITRL, Glucocorticoid induced TNF related ligand; NK, Natural Killer; Alb, Albumin; IL, Interleukin; TNF, Tumor Necrosis Factor; CRP, C-Reactive Protein; OS, Overall Survival; WBC, White blood cells; NSCLC, Non-small cell lung cancer.
Data Sharing Statement
The data associated with present study are available from the corresponding author upon reasonable request.
Ethics Approval
This retrospective study was performed in accordance with the principles of the Declaration of Helsinki. The study protocol was approved by the İnönü University Clinical Research Ethics Committee (Approval No: 2025/7300; Date: 25 March 2025). All patient data were anonymized before analysis, and confidentiality was strictly maintained throughout the study in accordance with institutional regulations.
Consent to Participate
Due to the retrospective design of the study, the requirement for informed consent was waived by the İnönü University Clinical Research Ethics Committee.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Disclosure
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–10. doi:10.3322/caac.21660
2. Siegel RL, Giaquinto AN, Jemal A. Cancer statistics, 2024 [published correction appears in CA Cancer J Clin. 2024 Mar-Apr;74(2):203. doi: 10.3322/caac.21830]. CA Cancer J Clin. 2024;74(1):12–49. doi:10.3322/caac.21820
3. McGlynn KA, Petrick JL, El-Serag HB. Epidemiology of hepatocellular carcinoma. Hepatology. 2021;73(Suppl 1):4–13. doi:10.1002/hep.31288
4. Massarweh NN, El-Serag HB. Epidemiology of hepatocellular carcinoma and intrahepatic cholangiocarcinoma. Cancer Control. 2017;24(3):1073274817729245. doi:10.1177/1073274817729245
5. Yu LX, Ling Y, Wang HY. Role of nonresolving inflammation in hepatocellular carcinoma development and progression. NPJ Precis Oncol. 2018;2(1):6. doi:10.1038/s41698-018-0048-z
6. Bedikian AY, Chen TT, Malahy MA, Patt YZ, Bodey GP. Prognostic factors influencing survival of patients with advanced colorectal cancer: hepatic-artery infusion versus systemic intravenous chemotherapy for liver metastases. J Clin Oncol. 1984;2(3):174–180. doi:10.1200/JCO.1984.2.3.174
7. Pinato DJ, North BV, Sharma R. A novel, externally validated inflammation-based prognostic algorithm in hepatocellular carcinoma: the prognostic nutritional index (PNI). Br J Cancer. 2012;106(8):1439–1445. PMID: 22433965; PMCID: PMC3326674. doi:10.1038/bjc.2012.92
8. Yamamura K, Sugimoto H, Kanda M, et al. Comparison of inflammation-based prognostic scores as predictors of tumor recurrence in patients with hepatocellular carcinoma after curative resection. J Hepatobiliary Pancreat Sci. 2014;21(9):682–688. PMID: 24823966. doi:10.1002/jhbp.114
9. Reig M, Forner A, Rimola J, et al. BCLC strategy for prognosis prediction and treatment recommendation: the 2022 update. J Hepatol. 2022;76(3):681–693. doi:10.1016/j.jhep.2021.11.018
10. Wilhelm SM, Carter C, Tang L, et al. BAY 43-9006 exhibits broad spectrum oral antitumor activity and targets the RAF/MEK/ERK pathway and receptor tyrosine kinases involved in tumor progression and angiogenesis. Cancer Res. 2004;64(19):7099–7109. doi:10.1158/0008-5472.CAN-04-1443
11. Kotsifa E, Machairas N, Angelis A, Nikiteas NI, Dimitroulis D, Sotiropoulos GC. Decoding the prognostic significance and therapeutic implications of inflammation-based scores in hepatocellular carcinoma: a comprehensive review. Cancers. 2024;16(14):2549. doi:10.3390/cancers16142549
12. Johnson PJ, Berhane S, Kagebayashi C, et al. Assessment of liver function in patients with hepatocellular carcinoma: a new evidence-based approach-the ALBI grade. J Clin Oncol. 2015;33(6):550–558. doi:10.1200/JCO.2014.57.9151
13. Liu W, Zhang K, Chen S, Wang X, Yu W. The pretreatment neutrophil-to-lymphocyte ratio as a near-term prognostic indicator in patients with locally advanced hepatocellular carcinoma treated with hepatic arterial infusion chemotherapy: a propensity score matching cohort study. Br J Hosp Med. 2024;85(11):1–16. doi:10.12968/hmed.2024.0393
14. Sun S, Li W, Guo X, Chen J. Prognostic value of the neutrophil-to-lymphocyte ratio and prognostic nutritional index in unresectable hepatocellular carcinoma patients treated with tyrosine kinase inhibitors and immune checkpoint inhibitors. Hum Vaccin Immunother. 2024;20(1):2394268. doi:10.1080/21645515.2024.2394268
15. Lu Y, Lu Y. Clinical predictive factors of the efficacy of immune checkpoint inhibitors and kinase inhibitors in advanced hepatocellular cancer. Clin Transl Oncol. 2025;27:1142–54.doi:10.1007/s12094-024-03644-9
16. Placke T, Salih HR, Kopp HG. GITR ligand provided by thrombopoietic cells inhibits NK cell antitumor activity. J Immunol. 2012;189(1):154–160. doi:10.4049/jimmunol.1103194
17. Hu B, Yang XR, Xu Y, et al. Systemic immune-inflammation index predicts prognosis of patients after curative resection for hepatocellular carcinoma. Clin Cancer Res. 2014;20(23):6212–6222. doi:10.1158/1078-0432.CCR-14-0442
18. Tisdale MJ. Molecular pathways leading to cancer cachexia. Physiology. 2005;20:340–348. doi:10.1152/physiol.00019.2005
19. Daniele A, Divella R, Abbate I, et al. Assessment of nutritional and inflammatory status to determine the prevalence of malnutrition in patients undergoing surgery for colorectal carcinoma. Anticancer Res. 2017;37(3):1281–1287. doi:10.21873/anticanres.11445
20. McMillan DC. Systemic inflammation, nutritional status and survival in patients with cancer. Curr Opin Clin Nutr Metab Care. 2009;12(3):223–226. doi:10.1097/MCO.0b013e32832a7902
21. Tan CS, Read JA, Phan VH, Beale PJ, Peat JK, Clarke SJ. The relationship between nutritional status, inflammatory markers and survival in patients with advanced cancer: a prospective cohort study. Support Care Cancer. 2015;23(2):385–391. doi:10.1007/s00520-014-2385-y
22. Luo B, Zhang Y, Zhu X, et al. Prognostic impact of the high-sensitivity modified glasgow prognostic score on patients undergoing radical surgery for hepatocellular carcinoma: authorship. Langenbecks Arch Surg. 2024;409(1):223. doi:10.1007/s00423-024-03423-8
23. Tsukagoshi M, Araki K, Igarashi T, et al. Lower geriatric nutritional risk index and prognostic nutritional index predict postoperative prognosis in patients with hepatocellular carcinoma. Nutrients. 2024;16(7):940. doi:10.3390/nu16070940
24. Ho CT, Chia-Hui Tan E, Lee PC, et al. Prognostic nutritional index as a prognostic factor for very early-stage hepatocellular carcinoma. Clin Transl Gastroenterol. 2024;15(4):e00678. doi:10.14309/ctg.0000000000000678
25. Grivennikov SI, Karin M. Inflammatory cytokines in cancer: tumour necrosis factor and interleukin 6 take the stage. Ann Rheum Dis. 2011;70(Suppl 1):i104–8. PMID: 21339211. doi:10.1136/ard.2010.140145
26. Patel KR, Menon H, Patel RR, Huang EP, Verma V, Escorcia FE. Locoregional therapies for hepatocellular carcinoma: a systematic review and meta-analysis. JAMA Network Open. 2024;7(11):e2447995. doi:10.1001/jamanetworkopen.2024.47995
27. Ogasawara S, Chiba T, Ooka Y, et al. Efficacy of sorafenib in intermediate-stage hepatocellular carcinoma patients refractory to transarterial chemoembolization. Oncology. 2014;87(6):330–341. PMID: 25227534. doi:10.1159/000365993
28. Ringelhan M, Pfister D, O’Connor T, Pikarsky E, Heikenwalder M. The immunology of hepatocellular carcinoma. Nat Immunol. 2018;19(3):222–232. PMID: 29379119. doi:10.1038/s41590-018-0044-z
29. Llovet JM, Kelley RK, Villanueva A, et al. Hepatocellular carcinoma. Nat Rev Dis Primers. 2021;7(1):6. Erratum in: Nat Rev Dis Primers. 2024 Feb 12;10(1):10. doi: 10.1038/s41572-024-00500-6. PMID: 33479224. doi:10.1038/s41572-020-00240-3
30. Naugler WE, Sakurai T, Kim S, et al. Gender disparity in liver cancer due to sex differences in MyD88-dependent IL-6 production. Science. 2007;317(5834):121–124. Erratum in: Science. 2009 Dec 4;326(5958):1346. PMID: 17615358. doi:10.1126/science.1140485
31. Tandon P, Garcia-Tsao G. Prognostic indicators in hepatocellular carcinoma: a systematic review of 72 studies. Liver Int. 2009;29(4):502–510. PMID: 19141028; PMCID: PMC2711257. doi:10.1111/j.1478-3231.2008.01957.x
32. Ganne-Carrié N, Nahon P, Chaffaut C, et al; CIRRAL group; ANRS CO12 CirVir group. Impact of cirrhosis aetiology on incidence and prognosis of hepatocellular carcinoma diagnosed during surveillance. JHEP Rep. 2021;3(3):100285. PMID: 34522876; PMCID: PMC8424277. doi:10.1016/j.jhepr.2021.100285
33. Kudo M. Selection of systemic treatment regimen for unresectable hepatocellular carcinoma: does etiology matter. Liver Cancer. 2022;11(4):283–289. PMID: 35978599; PMCID: PMC9294945. doi:10.1159/000525467
34. Wang S, Wang Y, Yu J, Wu H, Zhou Y. Lenvatinib as first-line treatment for unresectable hepatocellular carcinoma: a systematic review and meta-analysis. Cancers. 2022;14(22):5525. PMID: 36428618; PMCID: PMC9688932. doi:10.3390/cancers14225525
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Clinical Significance and Diagnostic Utility of NLR, LMR, PLR and SII in the Course of COVID-19: A Literature Review

Kosidło JW, Wolszczak-Biedrzycka B, Matowicka-Karna J, Dymicka-Piekarska V, Dorf J
Journal of Inflammation Research 2023, 16:539-562
Published Date: 11 February 2023
Inflammatory Markers in Women with Infertility: A Cross-Sectional Study
Duan Y, Zhou Y, Peng Y, Shi X, Peng C
International Journal of General Medicine 2023, 16:1113-1121
Published Date: 27 March 2023
Is Neutrophil Lymphocyte Ratio, Platelet Lymphocyte Ratio or Red Blood Cell Distribution Width Associated with Risk of Mortality in Patients with Necrotizing Fasciitis
Wu H, Li C, Liu S, Yao S, Song Z, Ren D, Wang P
Infection and Drug Resistance 2023, 16:3861-3870
Published Date: 16 June 2023
The Role of Different Systemic Inflammatory Indexes Derived from Complete Blood Count in Differentiating Acute from Chronic Calculus Cholecystitis and Predicting Its Severity
Chen L, Chen X
Journal of Inflammation Research 2024, 17:2051-2062
Published Date: 3 April 2024
The Association of Systemic Immune Inflammation Index (SII) and Platelet-to-Lymphocyte Ratio (PLR) on Coagulopathy and Prognosis in Patients with Traumatic Brain Injury
Chen J, Fu J, Liu J, Lu Y, Han D, Zeng J, Zou Z, Li Q, Zhang K, Wei X, Li L, Gu Z
Journal of Inflammation Research 2025, 18:5637-5653
Published Date: 25 April 2025