Back to Journals » Infection and Drug Resistance » Volume 16
Is Neutrophil Lymphocyte Ratio, Platelet Lymphocyte Ratio or Red Blood Cell Distribution Width Associated with Risk of Mortality in Patients with Necrotizing Fasciitis
Authors Wu H, Li C, Liu S, Yao S, Song Z, Ren D, Wang P
Received 18 March 2023
Accepted for publication 7 June 2023
Published 16 June 2023 Volume 2023:16 Pages 3861—3870
DOI https://doi.org/10.2147/IDR.S413126
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Haotian Wu,1,* Chunxia Li,2,* Song Liu,1 Shuangquan Yao,1 Zhaohui Song,1 Dong Ren,1 Pengcheng Wang1
1Department of Orthopaedic Surgery, The 3rd Hospital of Hebei Medical University, Shijiazhuang, Hebei, 050051, People’s Republic of China; 2Department of Imaging Medicine, General Hospital of Inner Mongolia Autonomous Region, Hohhot, Inner Mongolia, 010017, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Haotian Wu, Department of Orthopaedic Surgery, The 3rd Hospital, Hebei Medical University, No. 139 Ziqiang Road, Shijiazhuang, 050051, People’s Republic of China, Tel +86-311-88603682, Fax +86-311-87023626, Email [email protected]
Purpose: Neutrophil lymphocyte ratio (NLR), platelet lymphocyte ratio (PLR), and red blood cell distribution width (RDW) are novel biomarkers to indicate the inflammatory/immune response, and demonstrated to be effective in diagnosis, severity evaluation, and prognosis in a variety of chronic or acute conditions. This study aims to examine whether NLR, PLR and EDW are independently associated with mortality in necrotizing fasciitis (NF).
Methods: This study retrospectively enrolled patients diagnosed with NF and based on vitality status during hospitalization or within 30 days after discharge, survival and non-survival groups were defined. For distinctly comparing NLR, PLR, RDW and others, we enrolled the matched healthy controls of the same age and sex as the survivors of NF in a 1:1 ratio, which constituted the healthy control group. Comparisons were made between three groups. Variables tested with a P value < 0.10 were further entered into the multivariate logistic regression model to identify their independent association with mortality.
Results: A total of 281 subjects were included, including 127 healthy controls, 127 survivors, and 27 nonsurvivors with NF, respectively, indicating a mortality rate of 17.5%. ROC analysis showed that the optimal cutoff value for NLR, PLR and RDW was 11.1, 196.0 and 15.5%, respectively, and was tested as significant only for the first two (P < 0.001, = 0.004). Multivariate logistic analysis showed that NLR ≥ 11.1 (OR, 2.51) and PLR ≥ 196.0 (OR, 2.09) were independently associated with an increased risk of mortality in NF patients, together with age ((OR, 1.28, for each 10-year increment), comorbid diabetes mellitus (OR, 2.69) and liver disease (OR, 1.86), and elevated creatinine level (OR, 1.21 for each 10 umol/L elevation).
Conclusion: Elevated NLR and PLR are significant and independent predictors of mortality and can be considered for use when evaluating patients at risk of mortality.
Keywords: necrotizing fasciitis, prognosis, NLR, PLR, RDW
Introduction
Necrotizing fasciitis (NF) is a rare and potentially fatal acute bacterial infection characterized by extensive necrosis of the skin, subcutaneous tissue, and superficial fascia, and rapid progression. International epidemiological studies suggested that its annual incidence ranges from 0.72 to 9.2 per 100,000 person-years.1–3 Despite improvements in medical and surgical care, mortality of NF patients is still high, from 9.3% to 76%.4,5 Early diagnosis, rapid resuscitation, and aggressive surgical intervention are well established as the regimen of choice; however, how to identify high-risk patients in the early course of NF remains the biggest challenge due to a paucity of specific clinical findings.
During recent years, there has been an increasing interest in exploring new and effective biomarkers or derived ones that can be used to aid in diagnosis or improve the index of suspicion. The neutrophil-to-lymphocyte ratio (NLR) and platelet-to-lymphocyte ratio (PLR) reflect inflammation and stress to chronic or acute events,6 which, in theory, can be used to evaluate the severity of NF and/or predict prognosis. In previous studies, NLR and PLR have been shown to be effective in multiple settings, such as cancer,7–9 chronic/acute inflammatory conditions,10–12 rheumatic diseases,13 thromboembolic diseases14,15 and even trauma.16,17 However, their role in prognosis in the setting of NF has been rarely studied.18 Theoretically, NLR and PLR may provide clinical implications in the prognosis of NF (eg, mortality); in Ravindhran et al’s study they demonstrated preoperative elevated NLR rather than PLR were independently associated with “poor outcomes” in NF patients.18 Red blood cell distribution width (RDW) is a quantitative indicator that measures the heterogeneity or variability in the size of red blood cells and is often included in a complete blood count (CBC). RDW has proved to be a useful tool for assessing a variety of health conditions, including chronic heart failure, severe sepsis, and infections caused by Gram-negative bacteria,19–21 but its prognostic role in NF is rarely investigated22 or questioned.23,24
The purpose of the present study is to investigate the association between NLR, PLR and RDW with mortality in patients with NF at a single university-affiliated tertiary referral institution over a period of 7 years.
Methods
We performed this retrospective analysis of data on patients diagnosed with NF who were admitted to the Third Hospital of Hebei Medical University through the emergency department or the traumatic emergency center from January 1, 2015, to December 31, 2021. Our institution is a university affiliated hospital and a general tertiary referral hospital, in the city of Shijiazhuang, the provincial capital of Hebei province, has a capacity of 1200 beds in the general ward.
Electronic research was carried out to identify adult hospitalized patients (18 years or older) who had a discharge diagnosis of NF, underwent surgical interventions (debridement, amputation, or others), and had complete data on variables of interest and outcome data during hospitalization or within 30 days after discharge. The diagnosis of NF was based primarily on the operative findings that included the presence of grayish necrotic fascia, the lack of resistance of normally adherent muscular fascia to blunt dissection, and the presence of foul-smelling “dishwater” fluid; microbiological or histopathological results can only be available in a proportion of patients, therefore, not as necessary for the diagnosis of NF.
Patients were excluded if they were under 18 years, had missing data of interest, or outcome data.
Based on vitality status, patients were classified into the “survival” group and “non-survival” group. To facilitate a more intuitive comparison, an equal number of healthy individuals who were matched for age and sex in a 1:1 ratio with the survival group were randomly selected from the health management center registry of our institution during the same study period.
Measurements of Inflammatory Indexes
Upon admission, all subjects received 2 mL of venous blood after an 8-hour fast, using potassium-ethylenediaminetetraacetic acid tubes (dipotassium EDTA tube). Within an hour of venipuncture, the Sysmex-XE 2000i automated blood cell analyzer (Sysmex, Kobe, Japan) was used to measure the count of white blood cells (WBC), neutrophils, lymphocytes, eosinophils, red blood cells (RBC, x 1012/L), hemoglobin (g/L), hematocrit (percentage), red cell distribution width (RDW) (percentage) and platelet count (x 1012/L). NLR was calculated by dividing the absolute neutrophil count (x 109/L) by the lymphocyte count (x 109/L), while PLR was calculated by dividing the absolute neutrophil count (x 109/L) by the lymphocyte count (x 109/L).
Covariates
Due to the fact that multiple conditions could affect the variation of these biomarkers, we included several covariates for adjustment, including age, gender, body mass index (BMI – computed by dividing body weight in kilograms by the square of height in meters), smoking habits, alcohol consumption, time from presentation to the first operation and the presence of comorbidities (such as hypertension, diabetes, heart disease, liver disease, cerebrovascular disease, and renal disease). Data on diagnosis of comorbidities were extracted from the hospitalization medical record, which were generally documented by the treating surgeon based on the patients’ self-reports. Liver disease was defined as liver cirrhosis due to any cause, chronic viral hepatitis alcoholic or non-alcoholic fatty liver disease. Renal disease was defined as pre-existing chronic kidney disease or end-stage renal disease requiring dialysis.
This study was approved by the ethics committee of The Third Hospital of Hebei Medical University (No H2017-011-1), which waived the requirement of informed consent due to deidentified data used. This study was conducted in accordance with the Declaration of Helsinki (Version, 2008) and was reported in accordance with the Strengthening the Reporting of Surgical Cohort Studies (STROCSS) criteria.25
Statistical Analysis
First, we used the Kolmogorov–Smirnov test to evaluate the distribution of continuous variables data (expressed as mean (standard deviation [SD]), and depending on the normal or skewed distribution status, they were statistically analyzed by analysis of variance (ANOVA) or Kruskal–Wallis test for comparison between three groups. For variables with significant P < 0.05, post hoc test, Bonferroni corrected Mann–Whitney U-test was applied for pairwise comparisons.
NLR, PLR, and RDW were univariably evaluated as both continuous and dichotomous variables, with the latter based on the optimal cutoff value for each, as determined by the receiver operating curve at the maximal Youden index (ie, sensitivity+specificity-1).
To determine the independent association of these variables with mortality, any variables tested with P <0.10, along with other covariates, were entered into the multivariate logistic regression model, using the stepwise backward elimination method to identify significant factors. We used the Hosmer–Lemeshow (H-L) test to examine the goodness-of-fit of the multivariable model, with P >0.05 considered acceptable, and the adjusted Nagelkerke R square value to quantify the result, with higher indicating a better fit. All analyses considered two-tailed P values less than 0.05 as statistically significant.
All analyses were performed using SPSS 26.0 software (SPSS Inc., New York, USA).
Results
We finally enrolled 281 subjects, including 185 males and 96 females, and the average age was 60.6±6.2 years, and their demographic data, comorbidities and laboratory results are summarized in Table 1. Most (78.6%, 121/154) cases were diagnosed in our institution at initial onset and the remainder (21.4%, 33/154) were referred from other hospitals. The infection most often affected the lower limbs (n = 102, 66.2%), followed by the trunk (n = 37, 24.0%), and the upper extremities (n = 15, 9.8%). All patients underwent surgical debridements (average, 2.5±1.6) and 47.4% (73/154) underwent the first operation within 24 hours, and 11 (7.1%) patients underwent major limb amputation. There were 127, 127, and 27 in the healthy control group, the survivor, and the non-survival group, respectively, representing a mortality rate of 17.5%. Sixteen (10.4%) patients died during hospitalization, and eleven (7.1%) died within 30 days after discharge.
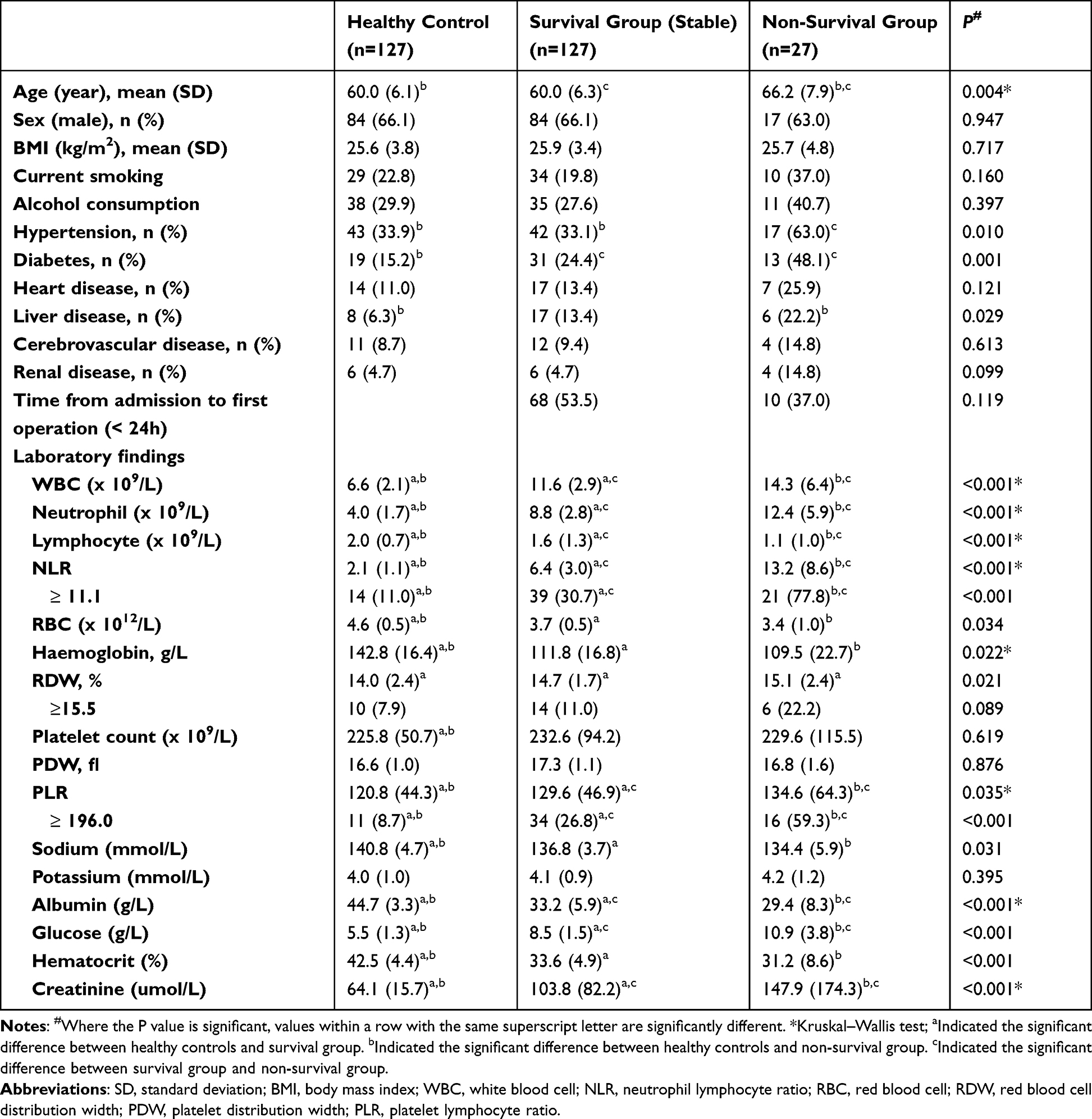 |
Table 1 Comparisons Between 3 Groups in Terms of Clinical Characteristics and Laboratory Results |
All NF patient underwent bacterial culture, with a positivity for culture of 80.5% (124/154); among 124 culture positive patients, there were 73 patients with monomicrobial infection, with Methicillin-susceptible Staphylococcus aureus in 13 (17.8%), Vibrio species in 12 (16.4%), Methicillin-resistant Staphylococcus aureus in 10 (13.7%), Streptococcus species in 10 (13.7%), Aeromonas species in 9 (12.3%), Klebsiella pneumoniae in 7 (9.6%), Pseudomonas aeruginosa in 4 (5.5%), Escherichia coli in 2 (2.7%), and others (6, 8.2%); and the and 51 with polymicrobial infection, with involving Enterococcus faecalis (27.4%, 14/51), Escherichia coli (23.5%, 12/51), Methicillin-resistant Staphylococcus aureus (23.5%, 12/51) and Streptococcus species (21.6%, 11/51) accounting for the most. Bacterial culture findings were available for 19 of 27 dead patients, with 13 dying in polymicrobial infection and 6 in monomicrobial infection, significantly differing from survival group (P = 0.017).
NLR, PLR, and RDW in healthy controls was 2.1 ± 1.1, 120.8 ± 44.3, and 14.0 ± 2.5%, respectively; all of which were lower than in NF patients, regardless of survival or non-survival. ROC analysis showed that the optimal cut-off value for NLR, PLR, and RDW was 11.1, 196.0 and 15.5%, respectively; but the first two were tested as significant, with AUC of 0.790 (P < 0.001) and 0.679 (P = 0.004), respectively. The details are presented in Table 2 and depicted in Figure 1.
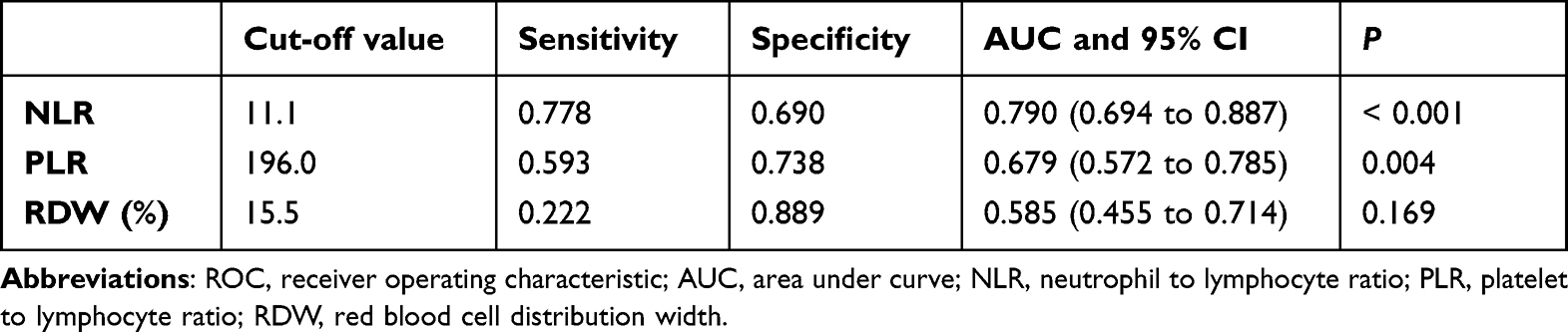 |
Table 2 The Analysis of the ROC Curve for the Three Variables of Interest |
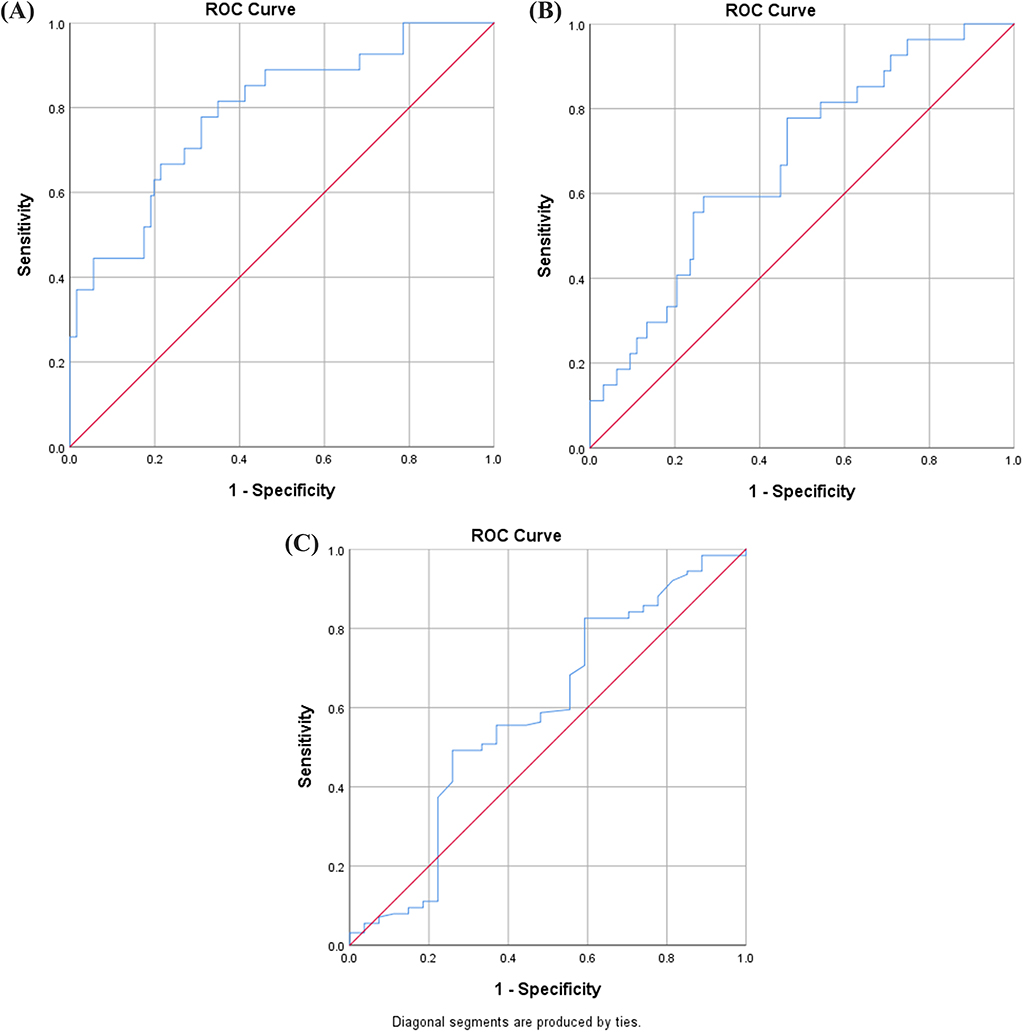 |
Figure 1 The ROC curve for the NLR (A), PLR (B) and RDW (C), with the respective AUC of 0.790 (95% CI, 0.694 to 0.887), 0.679 (95% CI, 0.572 to 0.785) and 0.585 (95% CI, 0.455 to 0.714). |
Significant differences were found between healthy controls, patients in the survival and non-survival group, in terms of age (P = 0.004), prevalence of hypertension, diabetes mellitus and liver disease, WBC count, neutrophil, lymphocyte and RBC, concentration of serum hemoglobin, sodium, albumin, glucose and creatinine, NLR and PLR in both continuous and categorical variables, RDW in continuous but not categorical variable and hematocrit. Pairwise comparisons showed that patients in the non-survival group significantly differed from the survival group in terms of age, prevalence of hypertension and diabetes mellitus, count of WBC, neutrophil and lymphocyte, NLR and PLR in both continuous and categorical variables, albumin, glucose and creatinine, which were subsequently entered into the logistic regression model (Table 1).
Multivariate logistic analysis showed that age (OR, 1.28, for each 10 years increase), comorbid diabetes mellitus (OR, 2.69) and liver disease (OR, 1.86), NLR ≥ 11.1 (OR, 2.51), PLR ≥ 196.0 (OR, 2.09) and elevated creatinine level (OR, 1.21 for each 10 umol/L elevation) were independently associated with the increased risk of mortality in NF patients (Table 3). The H-L test showed an acceptable result (P=0.514) and the adjusted Nagelkerke R2 value was 0.383.
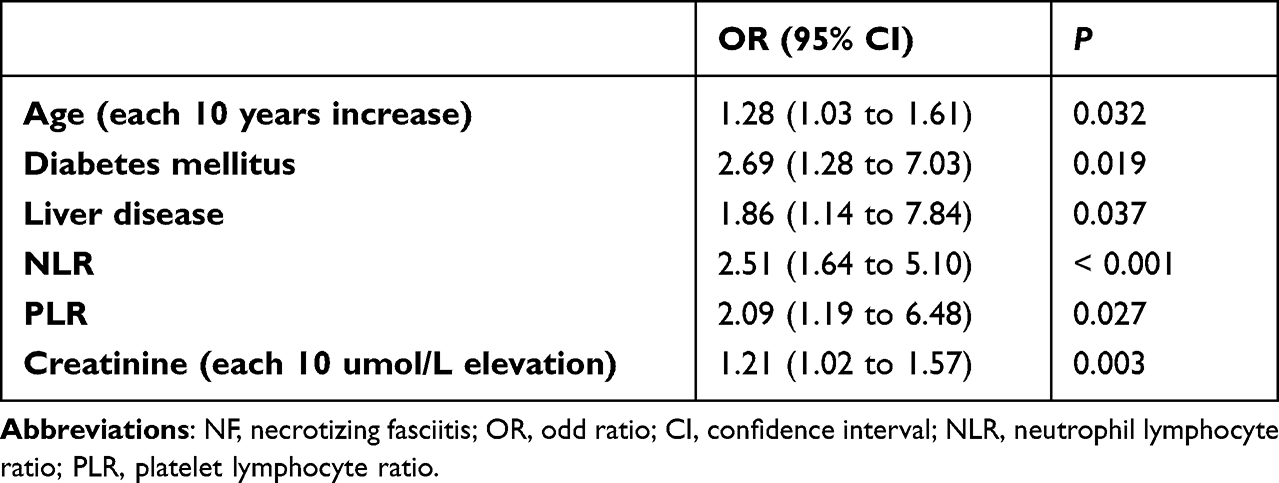 |
Table 3 Risk Factors for Mortality in Patients with NF by Logistic Regression Analysis |
Figure 2 depicts a typical case of NF in a 70-year man who had a ten-year diabetes history and an obvious inducement (injury).
 |
Figure 2 A 70-year-old male with a diabetes history for 10 years, had his right ankle sprained 2 weeks ago, no fracture, with local plaster immobilization. Ten days afterwards, he had redness, pain and swelling at the affected site, with no specific treatment. One day ago, spontaneous ulceration and pus flow presented (A) and he presented at emergence department of our institution, mentally languid, with a fever. Emergent surgery was performed for fasciotomy and removal of the necrotic tissues (B and C), and culture of wound specimens confirmed β-hemolytic Streptococcus. Systemic toxic symptoms disappeared several days after, and the patient wound bed became better ((D and E), day 20; F, day 30). |
Discussion
In this study, we focused on examining the relationship between NLR, PLR, and RDW and mortality in patients with NF. Our findings demonstrated that the mortality rate during hospitalization and within 30 days after discharge was 17.5%, and elevated NLR (≥11.1) and PLR (≥196.0), but not RDW, were independently associated with an increased risk of mortality, after adjustment for multiple confounders and covariables.
NLR/PLR in relation to adverse outcomes (morbidity and mortality) has been studied repeatedly in a variety of settings, including cancer, chronic/acute medical conditions or trauma.7,10,11,16,17 However, specifying at NF, there were only two studies evaluating the utility of NLR/PLR: Ravindhran et al18 suggested that a preoperative NLR of >7.5, but not PLR, significantly increased the risk of morbidity/mortality, and Johnson et al26 found a moderate correlation of NLR with in-hospital mortality, which could be further improved by evaluating the ratio of NLR to platelet count. Our findings showed that both NLR and PLR were independently associated with mortality in patients with NF, confirming this relationship. The mechanism underlying the association of elevated NLR/PLR with mortality not entirely clear, but was largely attributable to severe underlying inflammatory process caused by triggered release of arachidonic acid metabolites and platelet-activating factors, which resulted in neutrophilia and thrombocytosis, and cortisol-induced relative lymphopenia.18,27 Due to that they are simple to calculate, readily available, and not involving additional costs, they can be considered aiding in diagnosis of NF; but it should be noted that, due to the nonspecific nature, they should be used in combination with diverse findings from physical examination, laboratory results, imaging, and the isolated bacterial species.
Our finding that elevated RDW was not independently associated with an increased risk of mortality contradicted the previous study.22 In that study of 98 patients with NF, the authors observed an OR of 9.14 for the risk of mortality in patients with admission RDW >14.5% (normal upper limit for their hospital), and overall, 31.6% (31/98) of patients had an elevated RDW. In contrast, we used the ROC curve to determine that the optimal cut-off value of RW is 15.5%, and the unadjusted OR was 2.0, but not significant in the multivariate model. According to their applied cut-off value, 83.8% of patients would be deemed to have elevated RDW, much higher than theirs (31.6%). We were unaware of what exactly should explain this large discrepancy, but largely it was largely related to the age (substantially older than ours), comorbidity (cancer, chronic anemia) and severity of NF (tissue hypoxia, decompensation). The role of RDW in predicting mortality in NF patients was not inclusive and questioned by some researchers,23,24,28 and therefore future studies should continue to address this topic.
LRINEC is a classic index derived from six laboratory biomarkers: WBC, hemoglobin, creatinine, glucose, serum sodium, and CRP, with a total score of 0 to 13, to distinguish necrotizing fasciitis from other similar infections (eg, cellulitis or abscess); a score ≥6 has a 92% positive predictive value and 96% negative predictive value.29 However, its role in assessing prognosis has not been proven and even considered unreliable.30,31 In this study, we included 5 of the 6 components of LRINEC, except CRP, because CRP was performed only in patients who were highly suspected of having an infection at the time of presentation. Four of the five biomarkers were tested as significant in the univariate analysis, but only serum creatinine remained significant in the multivariate model (risk of mortality increased by 21% for every 10 umol/L increase). This finding is consistent with previous reports.32,33 Therefore, serum creatinine should be closely monitored upon a high suspicion of NF, and debridement procedure should be initiated as soon as possible only if an increasing trend of creatinine was observed.
Time to the first surgical intervention is the most important modifiable factor in the prognosis of NF patients; however, the literature showed the inconsistent findings. For example, Holena et al34 and Wong et al’s35 study suggested the time to operative debridement as an independent factor of mortality, but other studies, including our study, did not.36–39 We speculated that the limited sample size would be primarily responsible for the non-significance, possibly conferring the type II statistical error. For example, in Hadeed et al’s36 study of 87 patients, a remarkable clinical difference of mortality rate, 7.5% in the early (<6 hours from presentation) and 17.5% in the late (≥6 h) intervention group (6 h), but not reaching statistical significance. The trend was the same as ours where 37% of nonsurvivors and 63% of survivors underwent surgery within 24 hours from presentation, a substantial clinical difference, rather than a statistical difference (P = 0.119). Another reason might be related to the definition of time to surgery, mainly from presentation, and it would have been better to collect data from the onset of clinical symptoms better than from presentation. Due to the setting of a tertiary referral hospital, a certain proportion of patients were referred from primary or secondary hospitals, and thus the time lapsed during transfer between hospitals might also be a concern.
The utilization of NLR/PLR as a risk stratification tool has the potential to identify patients presenting with NF who are at an increased risk of mortality at the time of presentation. When patients with NF initially visit primary care settings, their physical symptoms or signs may be nonspecific, leading to a misdiagnosis of a less severe condition such as cellulitis. However, by assessing the NLR/PLR, together with other typical risk factors, primary care physicians can promptly identify the higher-risk population and refer them to tertiary care hospitals, thus allowing the surgical team to be more proactive in management of higher-risk patients. This also allows to anticipate the potential death and provide appropriate counseling to both the patient and their family members.
Some limitations of this study must be noted. First, data were retrospectively collected, and especially comorbidities were self-reported by patients, which could have affected the accuracy of the data and reliability of the findings. This study that examines the role of objectively measured parameters or those derived from them could partially compensate for this bias. Second, this study was conducted in a university-affiliated tertiary referral hospital, therefore, it is likely that patients with a poorer systemic status or NF of greater severity would be referred. More experienced providers, access to better equipment, and interdisciplinary cooperation allow the provision of better patient care, but it is less possible for secondary or primary institutions. Third, the relatively smaller number of samples is also a limitation, and it is likely that this study was underpowered, because only 154 patients were enrolled. This could have led to the type II error, missing a significant association when one is present. The fourth limitation may be the unmeasured, unconsidered or unknown variables that might have affected the outcome measure (mortality), the exposure variable (NLR/PLR), or their association in NF, therefore the residual confounding remains. Future studies with prospective design, multi-center, inclusion of more confounders for adjustment, and large-sample cohort studies are warranted to confirm the finding.
In conclusion, we identified NLR and PLR, not RDW, as independent predictors of mortality in patients with NF, together with others. These results would be helpful in predicting early mortality and patients involving them should be stratified into different risk groups and, accordingly, be administered with tailored medical or surgical interventions to improve the outcome. Additional research with a larger sample size and a prospective design across various institutions is necessary to confirm these findings. Future research could focus on exploring the mechanism underlying the elevated NLR/PLR with increased mortality risk, the dynamic changes relative to the surgery and thus identifying the appropriate surgical intervention timing, to improve the prognosis.
Data Sharing Statement
The data and materials used or analyzed during the study are available from the corresponding author on reasonable request, and contacted by mail if necessary.
Ethical Approval
The study protocol was approved by our institutional ethics committee.
Consent to Participate
All patients enrolled in the study signed informed consent forms.
Consent to Publish
All authors stated that they consented to publish this paper.
Acknowledgment
We thank professor X.Z. of Department of Statistics and Epidemiology of Hebei Medical University for her kind help.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by S&T Program of Hebei project plan (NO.18277777D).
Disclosure
All authors declare no conflicts of interest in this work.
References
1. Mulla ZD, Gibbs SG, Aronoff DM. Correlates of length of stay, cost of care, and mortality among patients hospitalized for necrotizing fasciitis. Epidemiol Infect. 2007;135(5):868–876. doi:10.1017/S0950268806007448
2. Das DK, Baker MG, Venugopal K. Increasing incidence of necrotizing fasciitis in New Zealand: a nationwide study over the period 1990 to 2006. J Infect. 2011;63(6):429–433. doi:10.1016/j.jinf.2011.07.019
3. Das DK, Baker MG, Venugopal K. Risk factors, microbiological findings and outcomes of necrotizing fasciitis in New Zealand: a retrospective chart review. BMC Infect Dis. 2012;12:348. doi:10.1186/1471-2334-12-348
4. Liu TJ, Tai H-C, Chien K-L, et al. Predisposing factors of necrotizing fasciitis with comparison to cellulitis in Taiwan: a nationwide population-based case-control study. J Formos Med Assoc. 2020;119(1 Pt 1):18–25. doi:10.1016/j.jfma.2019.01.014
5. Fontes RA, Ogilvie CM, Miclau T. Necrotizing soft-tissue infections. J Am Acad Orthop Surg. 2000;8(3):151–158. doi:10.5435/00124635-200005000-00002
6. Zahorec R. Ratio of neutrophil to lymphocyte counts-rapid and simple parameter of systemic inflammation and stress in critically ill. Bratisl Lek Listy. 2001;102(1):5–14.
7. Cheng H, Bhushan S, Li N, et al. Preoperative neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio are correlated with tumor-node-metastasis stages in patients with non-small cell lung cancer. J Cancer Res Ther. 2022;18(6):1666–1673. doi:10.4103/jcrt.jcrt_473_21
8. Gawiński C, Michalski W, Mróz A, et al. Correlation between Lymphocyte-to-Monocyte Ratio (LMR), Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR) and Tumor-Infiltrating Lymphocytes (TILs) in left-sided colorectal cancer patients. Biology. 2022;11(3). doi:10.3390/biology11030385
9. Schobert IT, Savic LJ, Chapiro J, et al. Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios as predictors of tumor response in hepatocellular carcinoma after DEB-TACE. Eur Radiol. 2020;30(10):5663–5673. doi:10.1007/s00330-020-06931-5
10. Noor A, Akhtar F, Tashfeen S, et al. Neutrophil-to-lymphocyte ratio, derived neutrophil-to-lymphocyte ratio, platelet-to-lymphocyte ratio and lymphocyte-to-monocyte ratio as risk factors in critically ill COVID-19 patients, a single centered study. J Ayub Med Coll Abbottabad. 2020;32(4):S595–s601.
11. Qin B, Ma N, Tang Q, et al. Neutrophil to lymphocyte ratio (NLR) and platelet to lymphocyte ratio (PLR) were useful markers in assessment of inflammatory response and disease activity in SLE patients. Mod Rheumatol. 2016;26(3):372–376. doi:10.3109/14397595.2015.1091136
12. Karataş M, Gündüzöz M, Öziş TN, et al. Neutrophil to lymphocyte ratio and platelet to lymphocyte ratio as haematological indices of inflammatory response in ceramic workers’ silicosis. Clin Respir J. 2019;13(3):159–165. doi:10.1111/crj.12997
13. Gasparyan AY, Ayvazyan L, Mukanova U, et al. The platelet-to-lymphocyte ratio as an inflammatory marker in rheumatic diseases. Ann Lab Med. 2019;39(4):345–357. doi:10.3343/alm.2019.39.4.345
14. Kurtipek E, Büyükterzi Z, Büyükterzi M, et al. Endothelial dysfunction in patients with pulmonary thromboembolism: neutrophil to lymphocyte ratio and platelet to lymphocyte ratio. Clin Respir J. 2017;11(1):78–82. doi:10.1111/crj.12308
15. Karahan SZ, Gazioglu S, Dilaver I, et al. The role of thrombo-inflammatory biomarkers in the prognosis of cerebral venous sinus thrombosis. Curr Neurovasc Res. 2021;18(2):237–243. doi:10.2174/1567202618666210607151518
16. Niu S, Pei Y, Hu X, et al. Relationship between the neutrophil-to-lymphocyte ratio or platelet-to-lymphocyte ratio and deep venous thrombosis (DVT) following femoral neck fractures in the elderly. Front Surg. 2022;9:1001432. doi:10.3389/fsurg.2022.1001432
17. Alexandru L, Haragus H, Deleanu B, et al. Haematology panel biomarkers for humeral, femoral, and tibial diaphyseal fractures. Int Orthop. 2019;43(7):1567–1572. doi:10.1007/s00264-019-04305-1
18. Ravindhran B, Rajan S, Kerketta D, et al. Neutrophil to lymphocyte ratio (NLR) and platelet to lymphocyte ratio (PLR) versus laboratory risk indicator for necrotizing fasciitis (LRINEC) as predictors of outcome in Necrotising fasciitis. Indian J Surg. 2020;82:325–330. doi:10.1007/s12262-019-01929-w
19. Felker GM, Allen LA, Pocock SJ, et al. Red cell distribution width as a novel prognostic marker in heart failure: data from the CHARM Program and the Duke Databank. J Am Coll Cardiol. 2007;50(1):40–47. doi:10.1016/j.jacc.2007.02.067
20. Allen LA, Felker GM, Mehra MR, et al. Validation and potential mechanisms of red cell distribution width as a prognostic marker in heart failure. J Card Fail. 2010;16(3):230–238. doi:10.1016/j.cardfail.2009.11.003
21. Ku NS, Kim H-W, Oh HJ, et al. Red blood cell distribution width is an independent predictor of mortality in patients with gram-negative bacteremia. Shock. 2012;38(2):123–127. doi:10.1097/SHK.0b013e31825e2a85
22. Weng CL, Wang C-H, Chen I-C, et al. Red cell distribution width is an independent predictor of mortality in necrotizing fasciitis. Am J Emerg Med. 2014;32(10):1259–1262. doi:10.1016/j.ajem.2014.08.001
23. Shih HM. Is red blood cell distribution width enough to predict prognosis of necrotizing fasciitis: author’s reply. Am J Emerg Med. 2015;33(3):468. doi:10.1016/j.ajem.2014.12.004
24. Shih HM. Can red cell distribution width predict mortality rate in patients with necrotizing fasciitis? The author’s reply. Am J Emerg Med. 2014;32(12):1538. doi:10.1016/j.ajem.2014.10.001
25. Bashaireh K, Aljararhih O, Alawneh K. Impact of body mass index on hemoglobin level and blood transfusion in total knee arthroplasty: a retrospective case control study. Ann Med Surg. 2020;55:180–184. doi:10.1016/j.amsu.2020.05.028
26. Johnson SR, Benvenuti T, Nian H, et al. Measures of admission immunocoagulopathy as an indicator for in-hospital mortality in patients with necrotizing fasciitis: a retrospective study. JB JS Open Access. 2023;8(1):154.
27. Tamhane UU, Aneja S, Montgomery D, et al. Association between admission neutrophil to lymphocyte ratio and outcomes in patients with acute coronary syndrome. Am J Cardiol. 2008;102(6):653–657. doi:10.1016/j.amjcard.2008.05.006
28. Sertoglu E, Uyanik M, Kayadibi H. Is red blood cell distribution width enough to predict prognosis of necrotizing fasciitis? Am J Emerg Med. 2015;33(2):301–302. doi:10.1016/j.ajem.2014.11.021
29. Wong CH, Khin L-W, Heng K-S, et al. The LRINEC (Laboratory Risk Indicator for Necrotizing Fasciitis) score: a tool for distinguishing necrotizing fasciitis from other soft tissue infections. Crit Care Med. 2004;32(7):1535–1541. doi:10.1097/01.CCM.0000129486.35458.7D
30. Crowe CS, Yu JL, Yesantharao P, et al. Predictors of mortality and amputation in patients with necrotizing soft tissue infections of the upper extremity. J Hand Surg Am. 2022;47(7):629–638. doi:10.1016/j.jhsa.2022.02.017
31. Collins CM, McCarty A, Jalilvand A, et al. Outcomes of patients with necrotizing soft tissue infections: a propensity-matched analysis using the national inpatient sample. Surg Infect (Larchmt). 2022;23(3):304–312. doi:10.1089/sur.2021.317
32. Horn DL, Shen J, Roberts E, et al. Predictors of mortality, limb loss, and discharge disposition at admission among patients with necrotizing skin and soft tissue infections. J Trauma Acute Care Surg. 2020;89(1):186–191. doi:10.1097/TA.0000000000002636
33. Huang KF, Hung M-H, Lin Y-S, et al. Independent predictors of mortality for necrotizing fasciitis: a retrospective analysis in a single institution. J Trauma. 2011;71(2):467–73; discussion 473. doi:10.1097/TA.0b013e318220d7fa
34. Holena DN, Mills AM, Carr BG, et al. Transfer status: a risk factor for mortality in patients with necrotizing fasciitis. Surgery. 2011;150(3):363–370. doi:10.1016/j.surg.2011.06.005
35. Wong CH, Chang H-C, Pasupathy S, et al. Necrotizing fasciitis: clinical presentation, microbiology, and determinants of mortality. J Bone Joint Surg Am. 2003;85(8):1454–1460. doi:10.2106/00004623-200308000-00005
36. Hadeed GJ, Smith J, O’Keeffe T, et al. Early surgical intervention and its impact on patients presenting with necrotizing soft tissue infections: a single academic center experience. J Emerg Trauma Shock. 2016;9(1):22–27. doi:10.4103/0974-2700.173868
37. Keung EZ, Liu X, Nuzhad A, et al. Immunocompromised status in patients with necrotizing soft-tissue infection. JAMA Surg. 2013;148(5):419–426. doi:10.1001/jamasurg.2013.173
38. Anaya DA, Bulger EM, Kwon YS, et al. Predicting death in necrotizing soft tissue infections: a clinical score. Surg Infect (Larchmt). 2009;10(6):517–522. doi:10.1089/sur.2008.112
39. Cheng NC, Tai H-C, Chang S-C, et al. Necrotizing fasciitis in patients with diabetes mellitus: clinical characteristics and risk factors for mortality. BMC Infect Dis. 2015;15:417. doi:10.1186/s12879-015-1144-0
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio Can Predict the Severity in COVID-19 Patients from Ethiopia: A Retrospective Study
Ayalew G, Mulugeta B, Haimanot Y, Adane T, Bayleyegn B, Abere A
International Journal of General Medicine 2022, 15:7701-7708
Published Date: 7 October 2022
Clinical Significance and Diagnostic Utility of NLR, LMR, PLR and SII in the Course of COVID-19: A Literature Review

Kosidło JW, Wolszczak-Biedrzycka B, Matowicka-Karna J, Dymicka-Piekarska V, Dorf J
Journal of Inflammation Research 2023, 16:539-562
Published Date: 11 February 2023
Inflammatory Markers in Women with Infertility: A Cross-Sectional Study
Duan Y, Zhou Y, Peng Y, Shi X, Peng C
International Journal of General Medicine 2023, 16:1113-1121
Published Date: 27 March 2023
Neutrophil/Lymphocyte Ratio (NLR) and Lymphocyte/Monocyte Ratio (LMR) – Risk of Death Inflammatory Biomarkers in Patients with COVID-19
Dymicka-Piekarska V, Dorf J, Milewska A, Łukaszyk M, Kosidło JW, Kamińska J, Wolszczak-Biedrzycka B, Naumnik W
Journal of Inflammation Research 2023, 16:2209-2222
Published Date: 23 May 2023
Pretreatment Prognostic Nutritional Index Predicts Progression-Free Survival in BCLC Stage C Hepatocellular Carcinoma Treated with Sorafenib

Aydın U, Dikilitaş M, Balıkçı Çiçek İ, Pamuk ÖA, Sadak Öcal Z, Danacı Y, Alizade E
Cancer Management and Research 2026, 18:621105
Published Date: 14 July 2026