Back to Journals » Journal of Inflammation Research » Volume 17
The Role of Different Systemic Inflammatory Indexes Derived from Complete Blood Count in Differentiating Acute from Chronic Calculus Cholecystitis and Predicting Its Severity
Received 13 December 2023
Accepted for publication 19 March 2024
Published 3 April 2024 Volume 2024:17 Pages 2051—2062
DOI https://doi.org/10.2147/JIR.S453146
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Ning Quan
Liling Chen,1 Xinyuan Chen2
1Department of Clinical Laboratory, Wenzhou Seventh People’s Hospital, Wenzhou, Zhejiang Province, People’s Republic of China; 2Department of Clinical Laboratory, Wenzhou Central Hospital, Wenzhou, Zhejiang Province, People’s Republic of China
Correspondence: Xinyuan Chen, Department of Clinical Laboratory, Wenzhou Central Hospital, Bailidonglu Street, Lucheng District, Wenzhou, 325000, People’s Republic of China, Tel +8615858805715, Fax +86057788070190, Email [email protected]
Purpose: This study aimed to evaluate the diagnostic value of the different Complete blood count-derived systemic inflammation indexes, including neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), systemic immune-inflammation index (SII), and neutrophil to lymphocyte × platelet ratio (NLPR) in differential diagnosing the chronic calculus cholecystitis (CCC) and the acute calculus cholecystitis (ACC), as well as determining the severity of ACC.
Patients and Methods: 105 CCC and 88 ACC patients were enrolled. NLR, PLR, SII, and NLPR were evaluated in both cohorts as well as in different severity levels of ACC. The severity of ACC was determined based on the Tokyo Guidelines. Receiver operating characteristic (ROC) curve and Univariate/multivariate regression analyses were conducted.
Results: The levels of NLR, PLR, SII, and NLPR were significantly higher in the ACC group compared to the CCC group. The optimal cutoff values for NLR, PLR, SII, and NLPR were determined to be 3.89, 144.7, 896.8, and 0.031 respectively. NLR> 3.89 demonstrates the highest predictive capability with an AUC of 0.801 and a sensitivity of 72.73%. Multivariate analysis showed that NLR> 3.89 (OR: 4.169, p = 0.004) and NLPR> 0.031 (OR: 4.304, p = 0.005) were dominant in distinguishing ACC from CCC. In ACC patients, the levels of NLR, SII, and NLPR were significantly higher in the Moderate to Severe-degree ACC (MS-ACC) group than in Mild-Degree ACC (M-ACC). NLPR > 0.044 exhibited the highest predictive ability with an AUC of 0.778 and a specificity of 91.67%. Multivariate analysis showed that NLR> 6.399 (OR: 10.308, p = 0.000) was a possible independent prognostic factor for accessing the severity of ACC.
Conclusion: Systemic inflammation indexes can be useful in predicting the risk of ACC and MS-ACC. NLR demonstrates the best distinguishing power and sensitivity for distinguishing ACC from CCC, while NLPR shows the best predictive power and specificity for predicting the severity of ACC.
Keywords: cholecystitis, NLR, PLR, SII, NLPR
Introduction
Cholecystitis is a widespread issue characterized by inflammation of the gallbladder, often prompted by blockage of the cystic duct.1 Calculous cholecystitis (CC) accounts for 95% of cases and can be further classified as chronic calculous cholecystitis (CCC) or acute calculous cholecystitis (ACC) based on the severity of clinical manifestations and the rate of disease progression.2,3
Currently, Cholecystitis cannot be definitively diagnosed through a single examination. Diagnosis relies primarily on a thorough medical history, symptoms, physical examination, and imaging findings.4 The gold standard for differentiating between acute and chronic cholecystitis is the use of pathologic findings from cholecystectomy. During the pre-operative period, imaging of the gallbladder plays a crucial role in distinguishing between the CCC and ACC. While ultrasonography is commonly used, it may not provide conclusive results in some patients.5,6 Computed tomography (CT) has its limitations, including the risk of false-positive and false-negative diagnoses, radiation exposure, and potential nephrotoxic effects from contrast media.7,8 Magnetic resonance imaging (MRI) is accurate in differentiating ACC from CCC due to its superior soft-tissue contrast resolution,5,9 but it can be costly and time-consuming. The use of MRI may be limited to severely ill patients and may not be feasible in settings with limited medical resources.
Research is ongoing on the role of biomarkers in predicting the severity of ACC. Tokyo Guidelines 2018 (TG18) is a widely accepted standard for assessing the severity of ACC using scoring systems.4 However, it involves collecting numerous parameters.
Thus, accurately diagnosing different types of cholecystitis in the pre-operative period often poses challenges for clinicians. Nonetheless, accurate diagnosis is crucial for appropriate treatment and optimal patient outcomes.4,10 For patients exhibiting symptoms of CCC, elective cholecystectomy is recommended. Prompt urgent cholecystectomy is imperative for those with mild ACC while patients with moderate to severe ACC require urgent or early gallbladder drainage in addition to initial medical treatment and organ support.11 Delayed or incorrect diagnosis can lead to complications, including gallbladder perforation, sepsis, and even septic shock. In patients with severe sepsis or shock caused by cholelithiasis, the mortality rate exceeds 60%.12 Therefore, rapid, accurate diagnosis and evaluation are crucial for developing the best treatment plan and providing timely and effective care when cholecystitis occurs.
Previous studies have elucidated that white blood cell (WBC) count and leukocyte subtype cells are valuable indicators for predicting the inflammatory process in acute cholecystitis.13–17 WBC count has been established as the primary biomarker for assessing the severity of cholecystitis.4 Elevated WBC count is often observed due to the robust inflammatory response triggered by gallstone blockage.18 In addition, Platelets also play a role in inflammation and host defense.19 Several inflammatory parameters based on WBC and platelet counts, such as the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), systemic immune-inflammation index (SII), and neutrophil-to-lymphocyte platelet ratio (NLPR), as potential valuable indicators in assessing the inflammatory process. This study aimed to evaluate the diagnostic effectiveness and practical application of these systemic inflammatory indexes in patients with CC. These indices could offer a rapid, accessible, easy-to-calculate, and cost-effective method for differentiating diagnose ACC from CCC as well as determining the severity of ACC, particularly in developing nations where access to advanced imaging and diagnostic tools may be limited.
Materials and Methods
Study Subjects
This prospective, observational, and single-center study was conducted at the hepatobiliary surgery of Wenzhou Central Hospital. The research was carried out from June 2022 to September 2023, involving 250 patients who had undergone cholecystectomy due to ACC or CCC. Histopathological examination was performed on the resected gallbladders. Diagnosis of CCC and ACC before surgery primarily relied on a combination of detailed medical history, comprehensive clinical examination, laboratory tests, and imaging investigations. The final confirmation of the diagnosis of both ACC and CCC was based on the pathological examination of postoperative gallbladder tissue specimens. The ACC patients underwent further classification by the TG18 into three severity grades:4 Moderate ACC is related to any one of the following conditions: (1) elevated WBC count (>18,000/mm3); (2) palpable tender mass in the right upper abdominal quadrant; (3) the duration of complaints > 72 h; (4) marked local inflammation (gangrenous cholecystitis, pericholecystic abscess, hepatic abscess, biliary peritonitis, emphysema cholecystitis). Severe ACC is associated with dysfunction of any one of the following organs/systems: (1) cardiovascular dysfunction: hypotension requiring treatment with dopamine ≥ 5 μg/kg per minute, or any dose of norepinephrine; (2) neurological dysfunction: decreased level of consciousness; (3) respiratory dysfunction: PaO2 /FiO2 ratio < 300; (4) renal dysfunction: oliguria, creatinine > 2.0 mg/dL; (5) hepatic dysfunction: PT international normalized ratio (INR)> 1.5; (6) hematological dysfunction: platelet count < 100,000/mm3. Mild ACC does not meet the criteria for “Moderate” or “Severe” ACC. Patients with Moderate- and severe-degree inflammations were grouped as the high-degree inflammation group and compared with the mild-degree inflammation group. The criteria for exclusion were established as follows: (1) Patients below 18 years of age or above 90 years of age, (2) complicated with gallbladder polyp or gallbladder carcinoma, (3) complicated with intrahepatic or extrahepatic cholelithiasis, (4) complicated with serious medical diseases such as heart, lung, brain or kidney, (5) complicated with other acute or chronic infections, autoimmune, malignant tumors, or inflammatory diseases, (7) non-calculous cholecystitis.
Blood sampling and Biochemical Analysis
Blood specimens were collected under sterile conditions on Day 1 of hospital admission. EDTA-anticoagulated blood sample (2 mL) was used for the determination of routine blood count through the Sysmex XE-2100 Hematology System (East Asia Company, Japan). Blood parameters, such as neutrophil counts, lymphocyte counts, and platelet counts were all recorded. The NLR, PLR, SII, and NLPR were calculated as follows: NLR (neutrophils/lymphocytes ratio), PLR (platelets/lymphocytes ratio), SII ((neutrophils × platelets)/lymphocytes), NLPR (neutrophils/ (lymphocytes × platelets ratio)). Peripheral blood (5 mL) was collected into pre-coagulation tubes and centrifuged for the serum. The serum was then analyzed for various biochemical parameters including ALT (alanine transaminase), AST (aspartate transaminase), GGT (gamma-glutamyl transpeptidase), ALP (alkaline phosphatase), TC (total cholesterol), TG (triglyceride), HDL-C (high-density lipoprotein cholesterol), LDL-C (low-density lipoprotein cholesterol), Apo AI (apolipoprotein AI), Apo B (apolipoprotein B), and Lp (a) (a-lipoprotein), CREA (creatinine) using the Beckman Coulter AU5800 Automatic Biochemical Analyzer (Beckman Coulter Co. Ltd. USA). Sodium citrate-anticoagulation blood sample (5 mL) was used for the INR analysis through the STA-R Evolution® Experts series (STAGO, France). All determinations were performed in the Clinical Science Experiment Center of the Wenzhou Central Hospital. The normal ranges of serum TC, TG, HDL-C, LDL-C, Apo AI, Apo B, and Lp (a) levels in our Clinical Science Experiment Center were 2.44–5.17, 0.40–1.70, 1.16–1.42, 2.07–3.10 mmol/L, 1.00–1.6, 0.60–1.1 g/L and 0–300 mg/L, respectively.
Statistical Analysis
All statistical analyses were performed using SPSS v.27 (SPSS Inc., Chicago, IL, USA). Kolmogorov–Smirnov test was used to determine whether variables were normally distributed. Mean ± standard deviation (SD) was used to present normally distributed variables, and median and interquartile range (IQR) values were used for abnormally distributed variables, while categorical variables were reported as percentages. Comparisons between groups were performed using the Mann–Whitney test and Chi-square test for numerical and categorical variables, respectively. Receiver operating characteristics (ROC) curve analysis was performed to estimate optimal cut-off values, maximizing sensitivity and specificity according to the Youden index. Univariate analysis and multivariate regression analysis for each factor were performed by logistics regression analysis. These parameters were treated as binary variables and were dichotomized based on optimal cut-off values or mean values. Variables with statistical significance (P-value < 0.1) in univariable regression models were included in the multivariable regression model using the “forward LR” method to determine their significance after adjustment for potential confounders. All tests were two-tailed and P-value < 0.05 was considered statistically significant.
Results
General Patient Characteristics
A total of 105 patients with CCC (36 male, 69 female) with a median age of 52 years (range: 18–80) and 88 patients with ACC (51 male, 37 female) with a median age of 56.5 years (range: 23–88) were included in this study based on specific inclusion and exclusion criteria. The laboratory findings indicated that patients with ACC had significantly higher levels of liver function enzymes such as AST, ALP, and GGT compared to CCC patients, with GGT showing the most notable increase. Conversely, ACC patients exhibited decreased concentrations of TC, TG, LDL-C, Apo AI, and Apo B in comparison to CCC patients. Furthermore, ACC patients had higher White blood cell and neutrophil counts but lower relative lymphocyte counts compared to CCC patients. Detailed demographic information and serum parameter distributions of the patients can be found in Table 1.
 |
Table 1 Comparison of Important Laboratory Parameters Between CCC and ACC |
Among the patients with ACC, there were 36 cases of mild-degree inflammation (M-ACC) and 52 cases of moderate- and severe-degree inflammation (MS-ACC). Severe ACC was present in only three patients, with one case involving hepatic dysfunction, another with respiratory complications, and the third demonstrating cardiological dysfunction. The average age of patients with M-ACC was 50.4 years, while for the MS-ACC group, it was 59.5 years. Apo AI levels were notably lower in MS-ACC patients compared to those with M-ACC. Analysis of blood parameters revealed a significant increase in WBC and neutrophil counts in MS-ACC patients compared to M-ACC patients, whereas the lymphocyte count was significantly lower in the MS-ACC group than in the M-ACC group. The additional laboratory findings for M-ACC and MS-ACC patients are shown in Table 2.
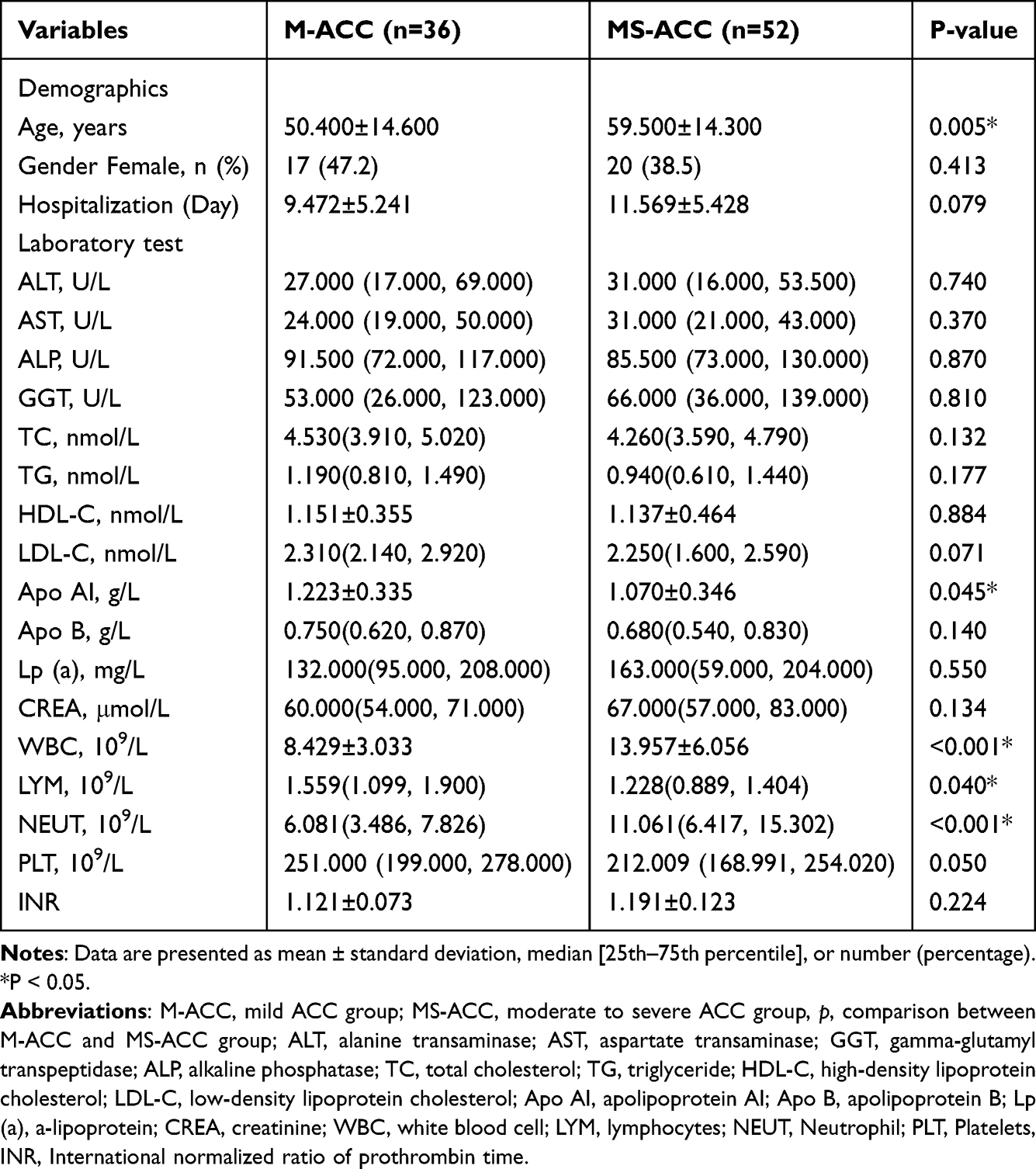 |
Table 2 Demographic Data and Laboratory Results of the ACC Patients Stratified According to the Severity Grade |
The Results of the Assessed Systemic Inflammatory Indexes in Each Group of Patients with CC
The NLR value was markedly higher in ACC patients [6.444 (3.199–11.446)] compared to the CCC group [1.971 (1.519–3.301), P <0.001]. Also, there was a notable rise in the PLR [169.121 (125.75–246.336) and 127.253 (98.612–174.706); respectively, P <0.001], SII [1470.792 (689.186–2758.316)) and 440.228 (315.366–872.194); respectively, P <0.001] and NLPR [0.030 (0.014–0.058) and 0.008 (0.006–0.015); respectively, P < 0.001], in ACC patients compared to the CCC group (Figure 1).
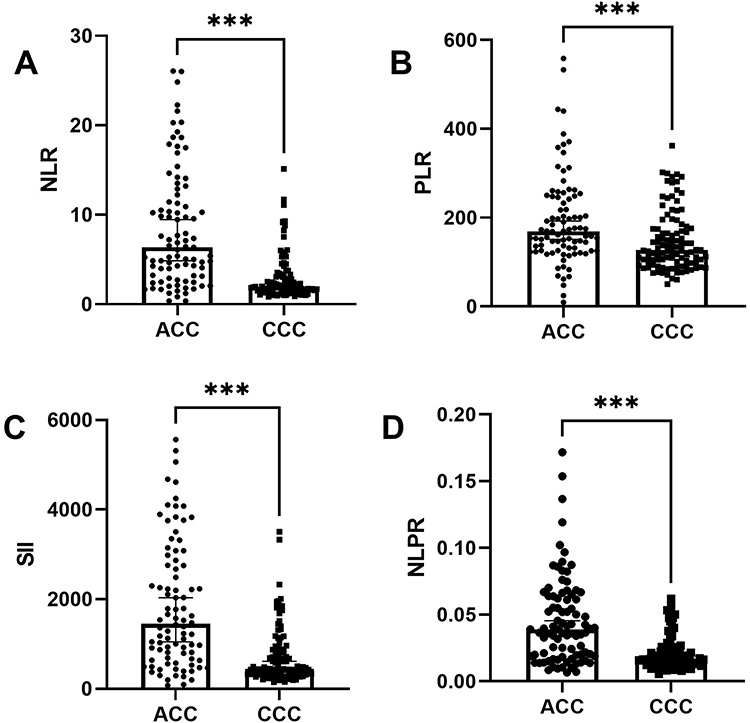 |
Figure 1 Comparison of Systemic Inflammatory Indexes between ACC and CCC patients. (A) neutrophil-to-lymphocyte ratio (NLR). (B) platelet-to-lymphocyte ratio (PLR). (C) systemic immune inflammatory (SII). (D) neutrophil to lymphocyte × platelet ratio (NLPR). ***p < 0.001. Abbreviations: ACC, acute calculous cholecystitis; CCC, chronic calculous cholecystitis. |
Furthermore, in MS-ACC patients, the NLR, SII, and NPLR values were significantly higher compared to M-ACC patients (NLR:9.747 (5.068–14.065) Vs 4.093 (2.020, 5.411); p < 0.001; SII:2218.176 (1176.878–3349.847) vs 932.005 (491.654–1572.093); p < 0.001; NLPR:0.047 (0.026–0.069) VS 0.018 (0.008–0.028); p < 0.001) (Figure 2). However, there was no significant difference between the two groups in the value of PLR.
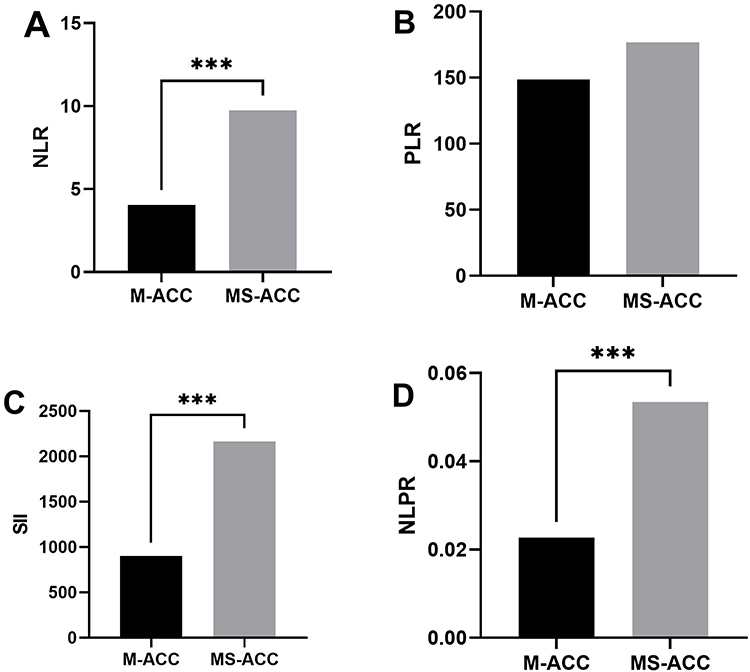 |
Figure 2 Comparison of Systemic Inflammatory Indexes between M-ACC and MS-ACC patients. (A) neutrophil-to-lymphocyte ratio (NLR). (B) platelet-to-lymphocyte ratio (PLR). (C) systemic immune inflammatory (SII). (D) neutrophil to lymphocyte × platelet ratio (NLPR). ***p < 0.001. Abbreviations: M-ACC, mild acute calculous cholecystitis; MS-ACC, moderate to severe acute calculous cholecystitis. |
Comparison for Assessing the Discriminative Ability of Each Inflammation Indexes to Distinguishing AAC from CCC Patients
Receiver operating characteristic (ROC) curve analysis was conducted to assess the discriminative ability of various inflammation indices in differentiating between AAC and CCC patients. The NLR demonstrated a sensitivity of 72.73%, a specificity of 80.95%, and an AUC of 0.801 at a cut-off of 3.89 (P < 0.001). The PLR showed a sensitivity of 68.18%, a specificity of 61.9%, and an AUC of 0.662 at a cut-off of 144.7. Additionally, the SII exhibited a sensitivity of 69.32%, a specificity of 76.19%, and an AUC of 0.777 at a cut-off of 896.8 (P < 0.001), while the NLPR had a sensitivity of 63.64%, a specificity of 86.67%, and an AUC of 0.776 at a cut-off of 0.031 (P < 0.001). Overall, the NLR displayed the highest AUC and sensitivity among the indexes assessed (Table 3).
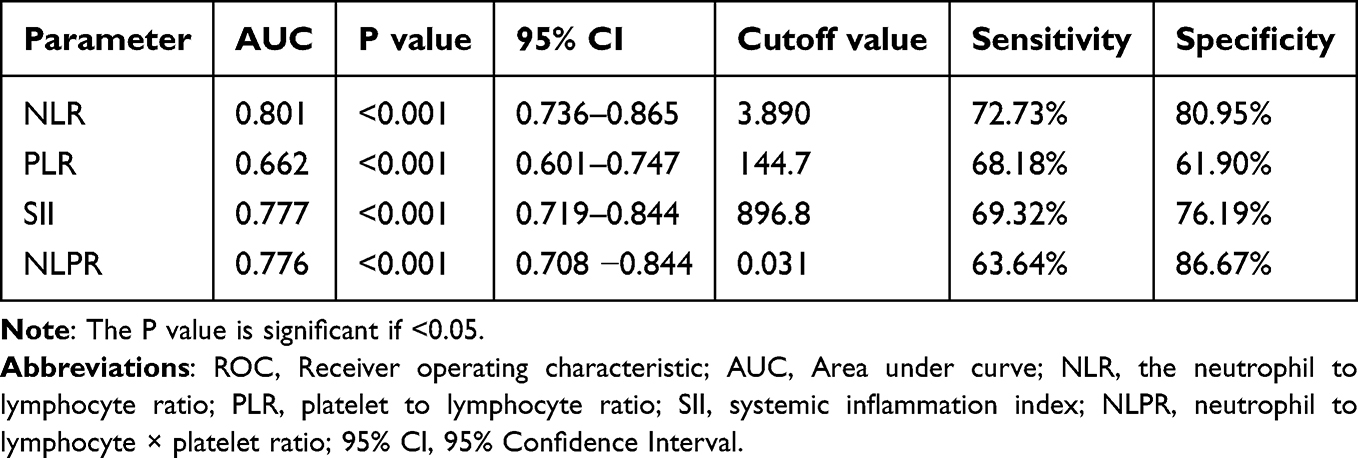 |
Table 3 ROC Curve Analysis for Different Inflammation Indices for Determining the Cut-off Between CCC and AAC Patients |
Comparison for Assessing the Discriminative Ability of Each Inflammation Indexes to Predict the Severity of ACC
In addition, ROC Curve Analysis demonstrated that NLR, SII, and NLPR might be acceptable in the differentiation of M-ACC and MS-ACC patients. The areas under the curve (AUC) for NLR, SII, and NLPR were 0.760, 0.723, and 0.778, respectively. The optimal cut-off values were identified as 6.399, 1261, and 0.044 for NLR, SII, and NLPR. Sensitivities for NLR, SII, and NLPR were found to be 71.15%, 72.22%, and 61.54%, while specificities were 80.56%, 73.08%, and 91.67%. Nonetheless, the diagnostic potential of PLR was not supported by the ROC analysis, as it did not reach a significant level (P = 0.309) (Table 4).
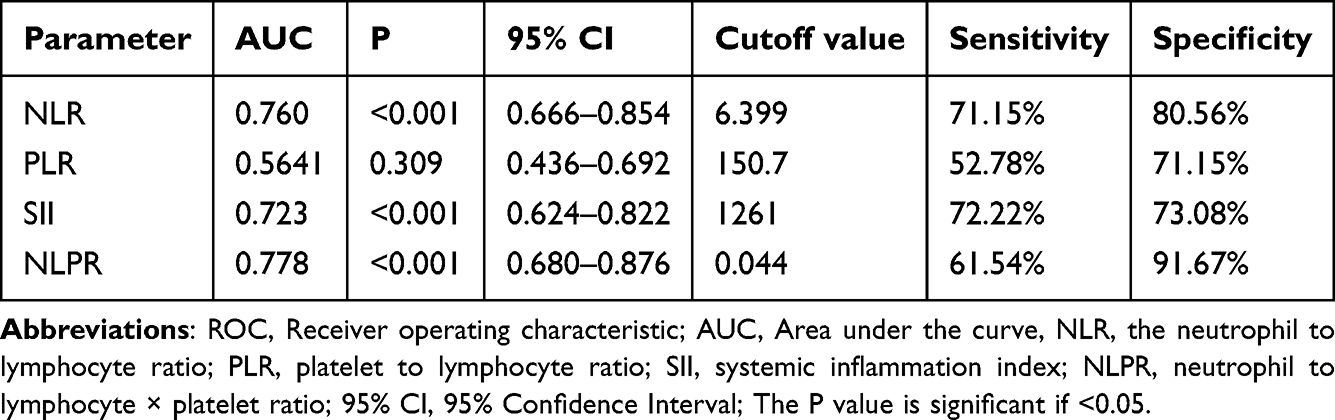 |
Table 4 Comparison of ROC Curve Analysis of Different Inflammation Indices in Predicting the Severity of Cholecystitis |
Univariate and Multivariate Logistic Regression Analysis
Univariate and multivariable binary logistic analyses were conducted to evaluate the clinical significance of Inflammation Indices as biomarkers in distinguishing between ACC and CCC patients. Variables that demonstrated a P-value of <0.1 in the univariate analysis were subsequently included in the multivariable binary logistic analysis, encompassing TC, TG, LDL-C, Apo AI, Apo B, sex, NLR, PLR, SII, and NLPR. Notably, in the mutivariate analysis, several variables were found to be significant in discriminating between ACC and CCC, including Apo AI/ nmol/L (<1.13) (OR: 2.284, P = 0.031), Sex (%) (OR: 2.369, P = 0.025), NLR >3.89 (OR: 4.169, P = 0.004), and NLPR >0.031 (OR: 4.304, P = 0.005) (Table 5).
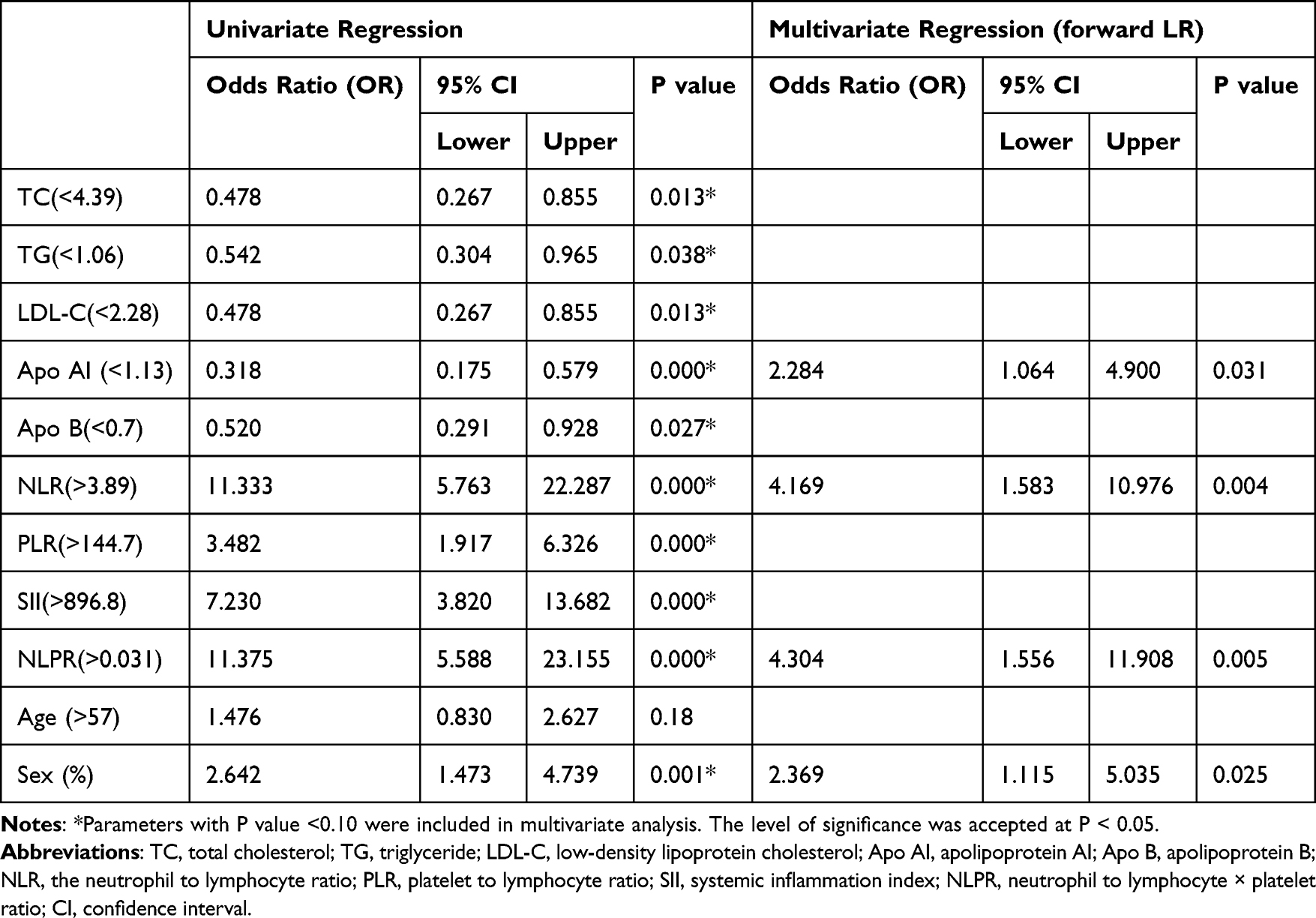 |
Table 5 Univariate and Multivariate Logistic Regression Analysis for the Factors Distinguishing ACC from CCC Patients |
Furthermore, the univariate analysis identified NLR, SII, NLPR, and age as risk factors for MS-ACC. Multiple logistic regression models further confirmed that age and NLR were significant independent predictive factors of severity in ACC patients. It was shown that when the NLR was more than the cutoff value, there was an increased risk of (10.308 times higher) moderate to severe degree inflammation compared to the lower NLR (Table 6).
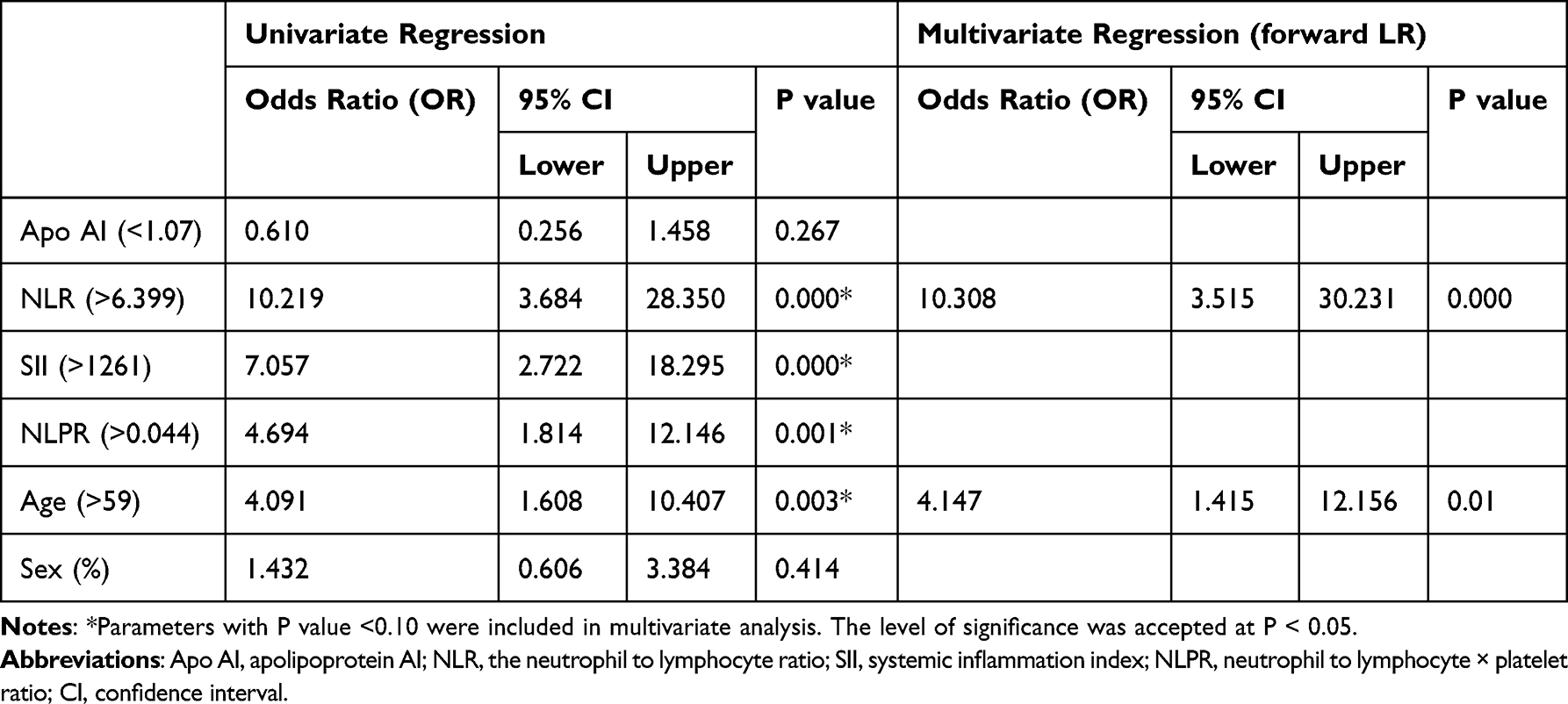 |
Table 6 Univariate and Multivariate Logistic Regression Analysis of Variables Potentially Associated with Severity of Calculous Cholecystitis |
Discussion
In this study, we aimed to assess the diagnostic role of various systemic inflammatory indices derived from Complete Blood Count in acute and chronic cholecystitis, as well as in differentiating between M-ACC and MS-ACC patients. Our research revealed that elevated levels of NLR, PLR, SII, and NLPR were associated with ACC compared to CCC patients. Additionally, among ACC patients, there was a significant increase in NLR, SII, and NLPR in those with MS-ACC compared to M-ACC patients. We indicated that the cut-off values for NLR, PLR, SII, and NLPR in differentiating between ACC and CCC patients were 3.89, 144.7, 896.8, and 0.031 (respectively), while in distinguishing between M-ACC and MS-ACC patients, the cut-off value for NLR, SII, and NLPR was much higher (6.39, 1261 and 0.044, respectively). These findings may contribute to the preoperative identification and prediction of ACC and its severity, thereby potentially assisting in averting complications and fatalities.
Considering the four inflammatory parameters associated with CC, NLR has been extensively studied and is considered a reliable marker for prognosticating diseases involving inflammatory and infective processes.20,21 Previous literature has shown that NLR is significantly higher in acute cholecystitis compared to healthy controls, ranging from 5.29–12.16 compared to 1.73–2.98.14,22–25 However, there have been limited studies focusing on the predictive value of NLR in differentiating acute and chronic cholecystitis. Our study supports previous findings that NLR levels were significantly higher in acute cholecystitis compared to chronic cholecystitis.23 We found that an NLR value above 3.89 was significant in the ACC group compared to the CCC group, and above 6.399 was significant in the MS-ACC patients. The binary logistic regression analysis revealed that an NLR exceeding the cutoff value independently predicts ACC and its severity. The increase in NLR cutoff values corresponds to higher estimates of inflammatory severity, which can be attributed to an imbalance in the inflammatory response with elevated neutrophil levels. This imbalance may result in the exhaustion of the immune system and a decrease in lymphocyte counts, subsequently triggering an aggressive inflammatory reaction through the activation of the innate immune system.26 Consistent with our findings, a study by Sang Kuon Lee et al observed a significant association between NLR and gangrenous cholecystitis (GC), where each standard deviation increase in NLR corresponded to a 48% heightened probability of GC.24 Nevertheless, a recent meta-analysis has suggested that while NLR can predict acute cholecystitis, it may not have the ability to predict disease severity.25 The ability of NLR to accurately differentiate the severity of ACC is a topic of ongoing debate, potentially influenced by variations in severity grade definitions across different studies. Further research is needed to clarify this matter.
PLR, another inflammatory marker based on complete blood count values, has shown potential as a prognostic marker in inflammatory diseases and malignancies. In our research, we observed that a PLR of 144.7 effectively distinguished between ACC and CCC, with a sensitivity of 68.18%, specificity of 61.9%, and ROC AUC of 66.20%. A recently published study has also indicated that a PLR of 148.13 could be considered a valuable inflammatory biomarker for ACC, demonstrating a sensitivity of 77.9%, specificity of 76.2%, and ROC AUC of 74.14%.27 Gökçe F et al highlighted the potential of NLR and PLR in guiding CRP and leukocyte values in acute cholecystitis.23 while Turhan et al’s study identified a PLR value over 146.90 as a predictive marker of complicated cholecystitis.28 Furthermore, another study showcased that a PLR equal to or greater than 154.73 indicates severe cholecystitis.29 However, our investigation did not yield significant evidence for using PLR to assess the severity of ACC. Similarly, in a recent study evaluating PLR, it was found that it can identify gangrenous acute cholecystitis with a cutoff value greater than 175, but PLR was not found to be an independent factor for gangrene.18 PLR holds promise as a prognostic and diagnostic tool in various inflammatory conditions, although further research is needed to fully understand its potential in assessing disease severity.
SII, as determined by peripheral lymphocyte, neutrophil, and platelet counts, has proven to be a valuable indicator for evaluating the immune and inflammatory status of patients. Previous studies have shown its potential for diagnosing and predicting various diseases, such as esophageal and pancreatic cancers.30,31 In the context of cholecystitis, previous studies have revealed that SII levels exhibit a significant elevation in patients with acute cholecystitis compared to healthy individuals.32 Furthermore, SII can serve as a positive predictor for the severity of acute cholecystitis.33 It has also demonstrated associations with short-term outcomes and advanced forms of acute cholecystitis.13,34 Within our study, we observed that the cutoff value of SII for differentiating between ACC and CCC was 896.8, and for predicting MS-ACC it was >1261. These findings indicated the potential clinical utility value of SII in assessing the severity and prognosis of acute cholecystitis.
NLPR, also describing the interaction of acute processes of the immune system and immunobiotics involving neutrophils, lymphocytes, and platelets,35 has not yet been extensively studied in patients with cholecystitis. However, NLPR has been investigated as a routine CBC inflammation index in other diseases, such as COVID-19 and acute kidney injury, showing potential as a risk factor or marker of disease severity.36,37 In our study, we have observed that the NLPR value is the most reliable parameter indicating the severity of ACC, with the highest AUC of 0.778 and specificity of 91.67%. Moreover, based on multivariate analysis, NLPR was also identified as an independent risk factor, its cut-off value for the predictive of ACC was 0.031. Further research is needed to explore the utility of NLPR in cholecystitis and other inflammatory conditions.
Our research encountered several limitations. Initially, the patient pool was confined to a single hospital, which may have restricted the broader applicability of the results. Additionally, the sample size of 193 cases, with just three severe ACC instances, was deemed inadequate. Subsequent studies ought to incorporate larger cohorts to affirm the efficacy of inflammation indexes for severe ACC cases. Lastly, our investigation did not delve into the correlation between Inflammation Indexes and the development of postoperative complications.
Conclusion
Our research shows that indicators such as NLR, PLR, SII, and NPLR have the potential to differentiate between ACC and CCC patients. NLR demonstrates the highest sensitivity and accuracy in this differentiation. Additionally, an increase in NLR, SII, and NPLR, from specific cut-off values, but not PLR, can predict the severity of ACC in patients. Notably, NPLR exhibits the highest specificity among the studied indicators. Importantly, our analysis identified NLR as the only factor independently and precisely associated with the severity of ACC. These findings highlight the potential of CBC as a readily available, and inexpensive test for predicting the severity of cholecystitis early on, thus facilitating more accurate clinical decision-making. This approach may be particularly beneficial for medical professionals in countries with limited resources.
Ethics Approval and Consent to Participate
The study was in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of the Wenzhou Central Hospital (approval number: L2022-02-052). All participants provided written informed consent.
Acknowledgments
No funding was received for this study. The authors thank hepatobiliary surgery of Wenzhou Central Hospital for the valuable support of this work.
Author Contributions
All authors made a significant contribution to the work reported, whether it was in the conception, study design, execution, data acquisition, analysis, and interpretation, or all these areas. All authors took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wadhwa V, Jobanputra Y, Garg SK, et al. Nationwide trends of hospital admissions for acute cholecystitis in the United States. Gastroenterol Rep. 2017;5(1):36–42. doi:10.1093/gastro/gow015
2. Editorial Board of Chinese Journal of Digestion. Chinese consensus on the internal medical treatment of chronic cholecystitis and gallstone (2014, Shanghai). Chin J Gastroenterol. 2015;20:292–296.
3. Branch of Biliary Surgery, Chinese Society of Surgery, Chinese Medical Association. Guidelines for diagnosis and treatment of acute biliary tract infections (2021). Zhonghua Wai Ke Za Zhi. 2021;59(6):422–429. doi:10.3760/cma.j.cn112139-20210421-00180
4. Yokoe M, Hata J, Takada T, et al. Tokyo Guidelines 2018: diagnostic criteria and severity grading of acute cholecystitis (with videos). J Hepato-Biliary-Pancreatic Sci. 2018;25(1):41–54. doi:10.1002/jhbp.515
5. Altun E, Semelka RC, Elias J, et al. Acute cholecystitis: MR findings and differentiation from chronic cholecystitis. Radiology. 2007;244(1):174–183. doi:10.1148/radiol.2441060920
6. Menu Y, Vuillerme MP. Non-traumatic abdominal emergencies: imaging and intervention in acute biliary conditions. Eur Radiol. 2002;12(10):2397–2406. doi:10.1007/s00330-002-1613-x
7. Hwang H, Marsh I, Doyle J. Does ultrasonography accurately diagnose acute cholecystitis? Improving diagnostic accuracy based on a review at a regional hospital. Can J Surg J Canadien de Chirurgie. 2014;57(3):162–168. doi:10.1503/cjs.027312
8. Smith EA, Dillman JR, Elsayes KM, et al. Cross-sectional imaging of acute and chronic gallbladder inflammatory disease. AJR. 2009;192(1):188–196. doi:10.2214/AJR.07.3803
9. Wang A, Shanbhogue AK, Dunst D, et al. Utility of diffusion-weighted MRI for differentiating acute from chronic cholecystitis. J Magnet Reson Imag. 2016;44(1):89–97. doi:10.1002/jmri.25128
10. Yokoe M, Takada T, Hwang TL, et al. Validation of TG13 severity grading in acute cholecystitis: Japan-Taiwan collaborative study for acute cholecystitis. J Hepatobiliary Pancreat Sci. 2017;24(6):338–345. doi:10.1002/jhbp.457
11. Miura F, Strasberg SM, Solomkin JS, et al. TG13 flowchart for the management of acute cholangitis and cholecystitis. J Hepato-Biliary-Pancreatic Sci. 2013;20(1):47–54. doi:10.1007/s00534-012-0563-1
12. Shou-Wu L, Sheng-Shun Y, Chi-Sen C, et al. Impact of the Tokyo guidelines on the management of patients with acute calculous cholecystitis. J Gastroenterol Hepatol. 2010;24(12):1857–1861.
13. Serban D, Stoica PL, Dascalu AM, et al. The Significance of Preoperative Neutrophil-to-Lymphocyte Ratio (NLR), Platelet-to-Lymphocyte Ratio (PLR), and Systemic Inflammatory Index (SII) in predicting severity and adverse outcomes in acute calculous cholecystitis. J Clin Med. 2023;12(21):6946. doi:10.3390/jcm12216946
14. Micić D, Stanković S, Lalić N, et al. Prognostic value of preoperative neutrophil-to-lymphocyte ratio for prediction of severe cholecystitis. J Med Biochem. 2018;37(2):121–127. doi:10.1515/jomb-2017-0063
15. Chen J, Gao Q, Huang X, et al. Prognostic clinical indexes for prediction of acute gangrenous cholecystitis and acute purulent cholecystitis. BMC Gastroenterol. 2022;22(1):491. doi:10.1186/s12876-022-02582-6
16. Sato N, Kinoshita A, Imai N, et al. Inflammation-based prognostic scores predict disease severity in patients with acute cholecystitis. Eur J Gastroenterol Hepatol. 2018;30(4):484–489. doi:10.1097/MEG.0000000000001063
17. Er S, Ozden S, Celik C, et al. Can we predict severity of acute cholecystitis at admission? Pakist J Med Sci. 2018;34(5):1293–1296. doi:10.12669/pjms.345.14502
18. Ares JAD, Garcia RM, Vidagany NE, et al. Can inflammatory biomarkers help in the diagnosis and prognosis of gangrenous acute cholecystitis? A prospective study. Revista Espanola De Enfermad Digest. 2021;113:41–45.
19. Nording HM, Seizer P, Langer HF. Platelets in inflammation and atherogenesis. Front Immunol. 2015;6:98. doi:10.3389/fimmu.2015.00098
20. Buonacera A, Stancanelli B, Colaci M, et al. Neutrophil to lymphocyte ratio: an emerging marker of the relationships between the immune system and diseases. Int J Mol Sci. 2022;23(7):3636. doi:10.3390/ijms23073636
21. Zahorec R. Neutrophil-to-lymphocyte ratio, past, present and future perspectives. Bratisl Lek Listy. 2021;122(7):474–488. doi:10.4149/BLL_2021_078
22. Prakash G, Hasan M. The accuracy of neutrophil-to-lymphocyte ratio and abdominal computed tomography to predict the severity of acute cholecystitis. Cureus. 2022;14(12):e32243. doi:10.7759/cureus.32243
23. Gökçe F, Gökçe A. Is c-reactive protein a superior marker of inflammation over the neutrophil/lymphocyte ratio or platelet/lymphocyte ratio in acute cholecystitis. Dicle Med J. 2019;46(4):839–845. doi:10.5798/dicletip.661406
24. Lee SK, Lee SC, Park JW, et al. The utility of the preoperative neutrophil-to-lymphocyte ratio in predicting severe cholecystitis: a retrospective cohort study. BMC Surg. 2014;14:100. doi:10.1186/1471-2482-14-100
25. Kler A, Taib A, Hajibandeh S, et al. The predictive significance of neutrophil-to-lymphocyte ratio in cholecystitis: a systematic review and meta-analysis. Langenbecks Arch Surg. 2022;407(3):927–935. doi:10.1007/s00423-021-02350-2
26. Peng J, Qi D, Yuan G, et al. Diagnostic value of peripheral hematologic markers for coronavirus disease 2019 (COVID-19): a multicenter, cross-sectional study. J Clin Lab Analysis. 2020;34(10):e23475. doi:10.1002/jcla.23475
27. Bedel C. Can we use neutrophil lymphocyte ratio and platelet lymphocyte ratio as a potential biomarker for acute cholecystitis? Ortadogu Tip Dergisi. 2019;11(4):404–408. doi:10.21601/ortadogutipdergisi.505193
28. Turhan VB, Gök HF, Ünsal A, et al. Pre-operative neutrophil/lymphocyte and platelet/lymphocyte ratios are effective in predicting complicated acute cholecystitis. Ulus Travma Acil Cerrahi Derg. 2022;28(4):471–476. doi:10.14744/tjtes.2021.49956
29. Santharaj DS, K NDP. Neutrophil-Lymphocyte Ratio (NLR), Platelet-Lymphocyte Ratio (PLR) and sonological findings in predicting severe cholecystitis. SAS J Surg. 2022;8(3):107–117. doi:10.36347/sasjs.2022.v08i03.008
30. Zeng X, Ye L, Luo M, et al. Prognostic value of pretreatment systemic immune-inflammation index in Chinese esophageal squamous cell carcinoma patients receiving radical radiotherapy: a meta-analysis. Medicine. 2023;102(25):e34117. doi:10.1097/MD.0000000000034117
31. Murthy P, Zenati MS, Al Abbas AI, et al. Prognostic value of the systemic immune-inflammation index (SII) after neoadjuvant therapy for patients with resected pancreatic cancer. Ann Surg Oncol. 2020;27(3):898–906. doi:10.1245/s10434-019-08094-0
32. Yildiz G, Selvi F, Bedel C, et al. Systemic inflammation response index and systemic immune inflammation index for predicting acute cholecystitis. Indian J Med Specialities. 2023;14(2):88–92. doi:10.4103/injms.injms_5_23
33. Cakcak İE, Kula O. Predictive evaluation of SIRI, SII, PNI, and GPS in cholecystostomy application in patients with acute cholecystitis. Turkish J Trauma Emerg Surg. 2022;28:7.
34. Özdemir S, Altunok İ, Abuzer Ö, et al. The role of the hematological inflammatory index and systemic immuno-inflammation index in acute cholecystitis; 2022.
35. Lu Y, Tang Y, Wang B, et al. Predicting immunoglobulin resistance in Kawasaki disease: an assessment of neutrophil to lymphocyte platelet ratio. Italian J Pediat. 2022;48(1):208. doi:10.1186/s13052-022-01400-9
36. de Hond TAP, Khairoun M, Haitjema S, et al. MO313: haematological ratios as risk factor for acute kidney injury in patients suspected of an infection at the emergency department. Nephrol Dial Transplant. 2022;37. doi:10.1093/ndt/gfac068.023
37. Ghobadi H, Mohammadshahi J, Javaheri N, et al. Role of leukocytes and systemic inflammation indexes (NLR, PLR, MLP, dNLR, NLPR, AISI, SIR-I, and SII) on admission predicts in-hospital mortality in non-elderly and elderly COVID-19 patients. Front Med. 2022;9:916453. doi:10.3389/fmed.2022.916453
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Neutrophil-to-Lymphocyte Ratio and Platelet-to-Lymphocyte Ratio Can Predict the Severity in COVID-19 Patients from Ethiopia: A Retrospective Study
Ayalew G, Mulugeta B, Haimanot Y, Adane T, Bayleyegn B, Abere A
International Journal of General Medicine 2022, 15:7701-7708
Published Date: 7 October 2022
Clinical Significance and Diagnostic Utility of NLR, LMR, PLR and SII in the Course of COVID-19: A Literature Review

Kosidło JW, Wolszczak-Biedrzycka B, Matowicka-Karna J, Dymicka-Piekarska V, Dorf J
Journal of Inflammation Research 2023, 16:539-562
Published Date: 11 February 2023
Inflammatory Markers in Women with Infertility: A Cross-Sectional Study
Duan Y, Zhou Y, Peng Y, Shi X, Peng C
International Journal of General Medicine 2023, 16:1113-1121
Published Date: 27 March 2023
Neutrophil/Lymphocyte Ratio (NLR) and Lymphocyte/Monocyte Ratio (LMR) – Risk of Death Inflammatory Biomarkers in Patients with COVID-19
Dymicka-Piekarska V, Dorf J, Milewska A, Łukaszyk M, Kosidło JW, Kamińska J, Wolszczak-Biedrzycka B, Naumnik W
Journal of Inflammation Research 2023, 16:2209-2222
Published Date: 23 May 2023
Pretreatment Prognostic Nutritional Index Predicts Progression-Free Survival in BCLC Stage C Hepatocellular Carcinoma Treated with Sorafenib

Aydın U, Dikilitaş M, Balıkçı Çiçek İ, Pamuk ÖA, Sadak Öcal Z, Danacı Y, Alizade E
Cancer Management and Research 2026, 18:621105
Published Date: 14 July 2026