Back to Journals » Patient Related Outcome Measures » Volume 16
Perspectives on Intravenous Iron Therapy Logistics and Adherence: Results from a Patient Survey
Authors Lee EJ, Louden L, Applequist J, Wilson BJ, Strauss J ![]()
Received 20 May 2025
Accepted for publication 16 September 2025
Published 25 November 2025 Volume 2025:16 Pages 163—179
DOI https://doi.org/10.2147/PROM.S532952
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Mithi Ahmed-Richards
Eun-Ju Lee,1 Les Louden,2 Janelle Applequist,3 Barbara J Wilson,4 Joshua Strauss5
1Hematology/Oncology Department, Columbia University Medical Center, New York, NY, USA; 2St. Joseph’s Hospital Department of Pharmacy, BayCare Health System, Tampa, FL, USA; 3Zimmerman School of Advertising and Mass Communications, University of South Florida, Tampa, FL, USA; 4Clinical Nurse Specialist (Self-Employed), Charlevoix, MI, USA; 5Atlantic Medical Group Hematology and Oncology, Springfield, NJ, USA
Correspondence: Joshua Strauss, Atlantic Medical Group Hematology and Oncology, Springfield, NJ, USA, Tel +1 973 379 2111, Email [email protected]
Purpose: Iron deficiency anemia (IDA) affects approximately 5 million people in the United States (US), significantly impacting quality of life (QoL) and overall health. Iron stores can be replenished through oral iron or, if ineffective/poorly tolerated, through intravenous iron (IVI) therapy. Despite IVI effectiveness, patients do delay/miss infusion appointments, leading to incomplete treatment response. Here we evaluated multiple-dose IVI therapy logistics and adherence from the patient perspective.
Patients and Methods: US adult patients (≥ 18 years) with confirmed IDA who were currently prescribed an IVI treatment course were asked to respond to a 46-question online survey in early 2023. Questions covered patient demographics, appointment logistics, IVI infusion experience, impact of infusion on daily activities, reason(s) for missing any doses, and considerations for improving adherence.
Results: A total of 323 patients completed the survey, 193 of whom were prescribed ≥ 2 IVI infusions per month. Of these patients, 71/193 (36.8%) reported missing at least one dose, despite its effectiveness at improving symptoms. Most patients (122/193 [64.3%]) agreed that multiple-dose IVI therapy adversely impacted their QoL by reducing their productivity (63.4%) and attendance at important events (64.8%), with 80.3% reporting having to schedule their life around therapy. A third of patients (73/193 [38.1%]) were unsatisfied with their infusion frequency, with most (163/193 [84.5%]) agreeing that fewer IVI infusions would improve adherence, and most also (174/193 [90.1%]) preferring a single-dose option if available.
Conclusion: Time spent arranging and receiving multiple IVI infusions per month can interfere with patients’ daily activities, leaving them dissatisfied with their IVI treatment experience. In this study, single-dose IVI infusions were a preferred option for patients with IDA, which may improve adherence to the complete course of treatment and offer improved QoL. Therefore, patient preference, convenience, and satisfaction should be considered and discussed when determining the type of IVI treatment.
Plain Language Summary: Iron deficiency anemia (IDA) is a prevalent health condition where the body does not have enough iron to, among other things, make enough red blood cells, which are needed for carrying oxygen around the body. One way to treat IDA is by delivering iron directly into the bloodstream, which is known as an intravenous iron (IVI) infusion. However, there are insurance plans that require patients to try multi-dose IVI treatments before covering treatments that can be given as a single dose. Some patients with IDA delay or miss their IVI appointments, the latter of which can impact treatment efficacy. To better understand why some patients delay or miss their IVI appointments, a survey asked patients with IDA about their IVI infusion experiences. A total of 323 patients completed the survey, with 193 receiving at least two IVI infusions per month. Most patients agreed that having several monthly IVI infusions per treatment course negatively affected their daily lives by reducing their productivity and causing them to miss important events. A majority also agreed they had to plan their lives around treatment. Among the 71 patients who missed appointments, most agreed that fewer monthly infusions would make it easier to complete the full treatment course and nearly all would prefer a single dose option if available. These results suggest multiple IVI infusions can negatively affect patients’ lives and their commitment to treatment. Therefore, it is important to consider patient convenience and insurance coverage when planning IVI treatment, as single IVI infusions may be more appealing for patients. Patients’ views on this issue are relevant, as their willingness to commit to best treatment practices is key to successful care.
Keywords: anemia, intravenous iron, hemoglobin, iron, iron deficiency anemia, patient adherence
Introduction
Iron deficiency affects approximately 10 million people in the United States (US), including 5 million individuals who have iron deficiency anemia (IDA), and the prevalence of individuals receiving treatment for IDA continues to rise.1,2 IDA occurs when iron intake fails to sufficiently restore physiological or pathological iron loses, leading to the depletion of iron stores (iron deficiency).3 This reduction in iron levels impairs hemoglobin synthesis, resulting in IDA.3 The underlying causes of IDA can be due to reduced iron absorption, (eg, either by dietary intake or reduced gastrointestinal absorption), increased demand for iron (eg, during pregnancy or child development), or chronic blood loss.3 The symptoms associated with IDA largely depend on the magnitude of anemia.4
Although patients can be asymptomatic with mild IDA, most experience symptoms such as lightheadedness, fatigue, cold intolerance, palpitations, restless leg syndrome, and dyspnea, all of which negatively impact quality of life (QoL) for individuals left untreated.5,6 IDA causality should be clarified ahead of treatment and in most cases, oral iron therapy is usually the first-line treatment. However, oral iron can cause gastrointestinal side effects and may be slow to correct the anemia or fully replenish iron stores for specific underlying causes.4 As a result of this, for many individuals, oral iron is ineffective or not tolerated,7,8 In such cases, patients may benefit from intravenous iron (IVI) infusions, which is generally well tolerated and associated with very low rates of infusion-related reactions.9 On average, the iron deficit in patients with IDA is approximately 1000 mg, emphasizing the need for iron repletion to restore normal physiological function.10
A variety of IVI products are available, but course of action often depends on insurance coverage, formulary availability, and physician preference.11 Based on guidelines, real-world evidence, and clinical trials, typical iron replacement treatment courses involve doses of 1000 mg or higher, tailored to the patient’s weight, hemoglobin level, and severity of iron deficiency.10,12–15 IVI products can be grouped into older- and newer-generation products,16 with older-generation products (iron sucrose, sodium ferric gluconate, iron dextran) being Food and Drug Administration (FDA)-approved for administration as multiple infusions of lower doses (<500 mg) in a treatment course. If infused off-label as a single infusion, iron dextran may need several hours to administer (eg, 1–6 hours [one infusion plus an initial test dose]).13,16–19 In contrast, newer-generation products are FDA-approved for administration over 15–20 minutes and require fewer doses to complete a treatment course, such as ferric derisomaltose (one infusion), ferric carboxymaltose (two infusions recommended), and ferumoxytol (two infusions).12,16,19–21 Infusion frequency and duration depend on factors such as blood loss and malabsorption.22
Although IVI effectively replenishes iron stores and improves QoL,23 nonadherence (characterized by delayed appointments or missed doses)24 remains a significant barrier, potentially leading to incomplete treatment response. Despite the potential for newer-generation IVI preparations to reduce the treatment burden and lower healthcare costs, nonadherence to IVI still occurs and is often underestimated.16 As a result, there remains a significant gap in understanding the specific impact of IVI logistics on patients’ daily lives and treatment outcomes, thereby limiting the development of holistic patient-centered solutions.
The average selling price (ASP) of IVI products ranges from ~$165 to $1790,25 and can vary over time. Out-of-pocket costs for patients can vary considerably, and depend on factors such as insurance coverage, copay assistance programs offered by manufacturers, and payor policies. Payor policies frequently require step therapy, or failure on older-generation products before newer-generation options are approved.16 These restrictive policies are primarily focused on drug product cost (eg, ASP), and do not usually factor in patient-reported outcomes, such as drug adherence and impact on activities of daily living (ADL).
Presented here are the results of a survey conducted to evaluate IVI therapy logistics from the patient perspective and to identify any potential barriers to adherence that can be associated with multiple-dose IVI therapy. The primary focus is on patients with IDA who were prescribed multiple IVI infusions per month as part of a treatment course and those who reported missing at least one IVI infusion.
Patients and Methods
A patient-based survey was conducted by The Harris Poll (Chicago, IL, US) between February 15 and March 16, 2023. The purpose of this observational survey was to explore patient experiences with IVI therapy and adherence among individuals with IDA. The study was conducted across the US, with respondents recruited from 41 states. Eligible participants were US adults ≥18 years of age with a confirmed IDA diagnosis, who had recently received or were currently receiving IVI treatment. The survey was deployed online to a panel of patients with IDA through two medical vendors used by The Harris Poll. The Harris Poll is a well-known market research and consulting firm that tracks public opinion, behaviors, and the motivations of US adults and adheres to the American Association for Public Opinion Research’s Code of Professional Ethics and Practices. The initial panels used by the firm gathered information regarding demographics and medical diagnosis to enable identification of certain patient populations for targeted surveys. Patients were then recruited through physicians, in-person sign-ups at disease awareness events, and referrals.
Patients with IDA were invited to take part in the survey via email, and if they chose to participate, underwent opt-in and screening processes to ensure that they were also currently being prescribed IVI. Informed consent was obtained and upon completion of the survey, patients earned points that could be applied towards rewards/incentives to the value of $80. The 46-question survey (see Supplementary File 1) included questions on patient demographics, appointment logistics, IVI infusion experiences, the impact of IVI therapy on QoL, reason(s) for missing any doses, and considerations for improving adherence. The survey was anonymized, non-interventional, and not intended to provide clinical data to support treatment decisions. Furthermore, it was not conducted as a clinical trial for any endpoints. Therefore, separate institutional review board (IRB) approval was not required.
To assess the IVI treatment duration, for simplicity, patients were asked how many infusions per month they received as part of their IVI treatment course, rather than the total duration of their IVI treatment. This translated to infusions being recorded as infusions per treatment course within a month. Patients were not asked about the brand or formulation of IVI that they were treated with. For this analysis, categorical variables were presented as frequencies, and sample data were grouped by the number of infusions per month. Raw data was not weighted and, therefore, results are only representative of the individuals who completed the survey. Descriptive statistics, including mean (± standard deviation [SD]), median (range), and proportion of patients were calculated using Microsoft Excel. Percentages were based on the number of completed responses, with missing data excluded to ensure accuracy and reliability of the reported results.
It should be noted that Akpan et al conducted a detailed analysis of these survey data on a cohort of patients with IDA due to heavy menstrual bleeding and included a subpopulation of patients who were receiving ≥2 IVI infusions per month, those who reported a missed dose, and patients who reported hypophosphatemia as an adverse event.26 This current analysis focuses on surveyed patients with IDA due to any underlying cause, reporting the logistical challenges faced by those who receive ≥2 IVI infusions per month and those who missed a dose, as well as their satisfaction and preferences regarding IVI treatment. Adverse event data was not collected.
Results
All Patients with IDA
In total, 323 patients across 41 US states completed the survey, with varied social demographics in areas of gender, age, marital status, familial status, education, income and employment (Table 1). Patients were either from a suburban environment (46.7%), urban or city area (35.3%) or a small town or rural area (18.0%). The most common reasons for being prescribed IVI treatment were heavy menstrual bleeding (39.0%), inflammatory bowel disease (16.7%), non-steroidal anti-inflammatory drug use (14.6%), and endometriosis (10.2%; Table 2). Over a third of patients (37.5%) also reported receiving oral iron in addition to IVI; however, the length of time patients received oral iron in relation to their diagnosis was not asked in the survey. The median number of IVI infusions received was seven (Table 2).
 |
Table 1 Demographics of All 323 Patients with IDA Who Completed the Survey |
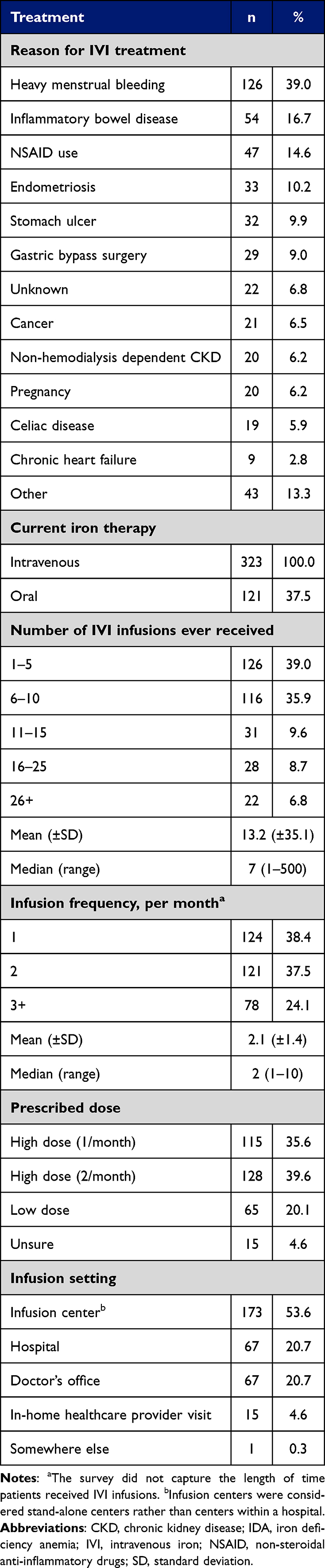 |
Table 2 IVI Treatment Details for All 323 Patients with IDA |
Patients Who Were Prescribed ≥2 IVI Infusions per Month and Missed at Least One IVI Infusion
One hundred and ninety-three (59.8%) patients were prescribed ≥2 IVI infusions per month (a mean of 2.7 [±1.2]) as part of their treatment course. The most common symptoms these patients reported prior to IVI treatment were fatigue (82.4%), weakness (65.8%), dizziness (60.1%), cold hands and feet (58.5%), and headache (56.5%), with improvements in most following IVI treatment (Figure 1A). These patients also experienced improvements in all ADLs after IVI treatment, with more than 50% of patients reporting improvements in “doing things around the house” and “caring for myself” (Figure 1B).
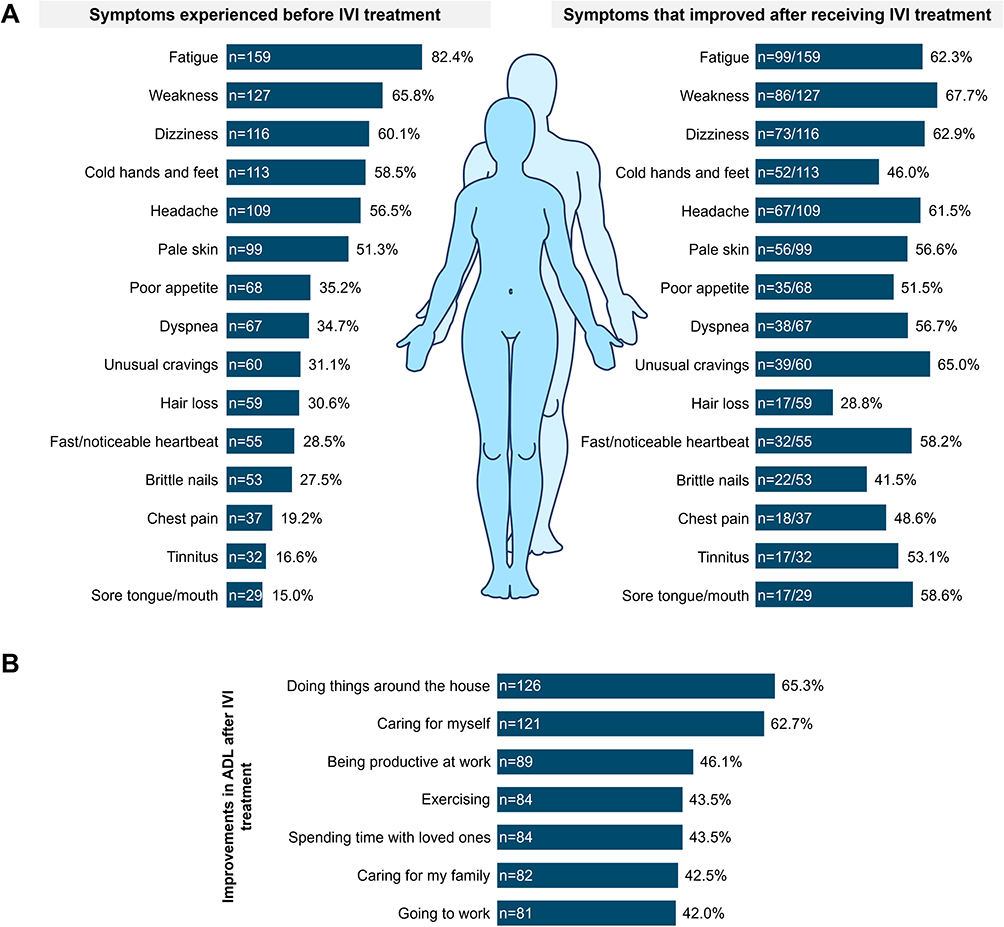 |
Figure 1 Symptoms and impact on ADL reported by all 193 patients prescribed ≥2 IVI infusions per month. (A) Symptoms experienced before IVI treatment and symptoms that improved after receiving IVI treatment. (B) ADL that were reported to be improved since receiving IVI treatment. Abbreviations: ADL, activities of daily living; IVI, intravenous iron. |
Of the 193 patients who were prescribed ≥2 IVI infusions per month as part of their treatment course, 71 (36.8%) reported missing at least one infusion (44 [62.0%] only once; 27 [38.0%] more than once). The demographics of patients who missed an infusion versus those who did not were generally similar; however, those who missed an infusion were more frequently younger White females with children, who were less educated, had a lower income, and were from an urban or city area (Table 3). The 71 patients who reported missing an infusion received a median total of nine infusions (a mean of 2.6 [±1.3] infusions ever).
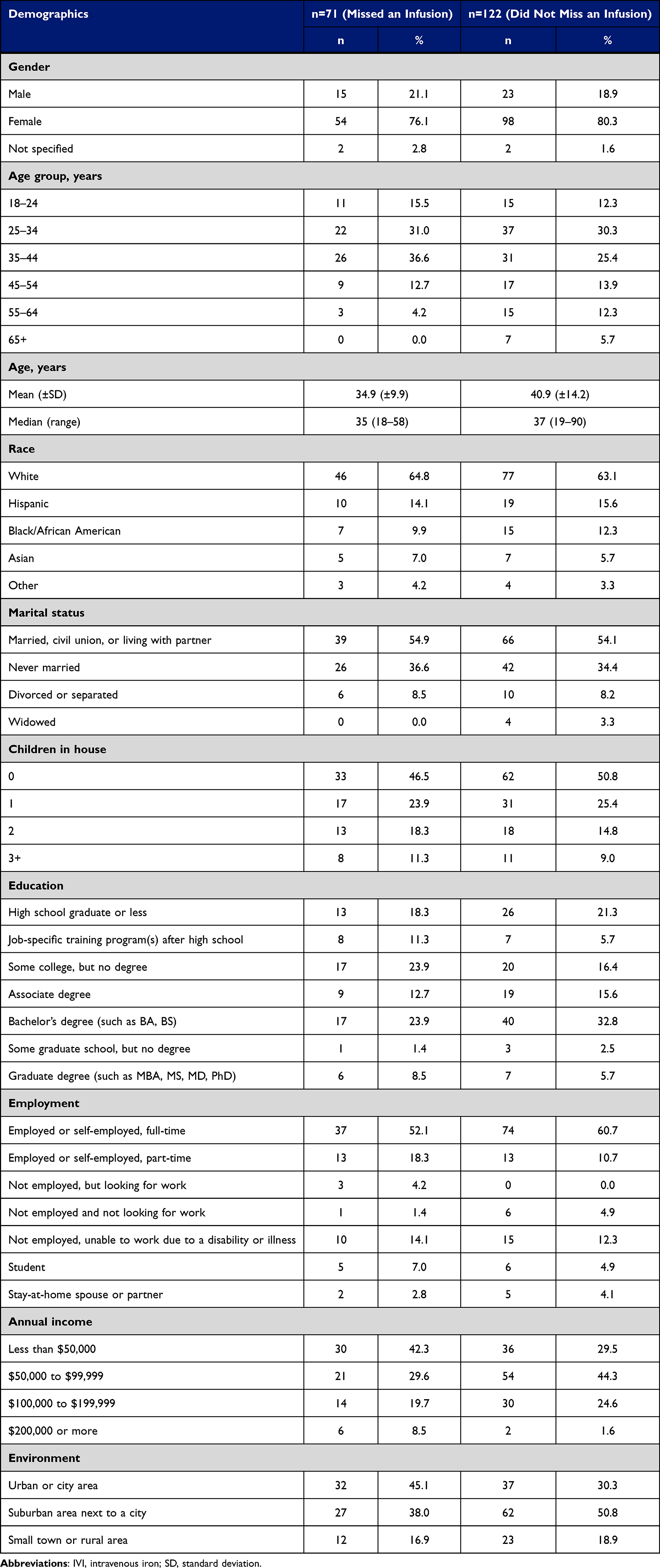 |
Table 3 Demographics of the Patients Who Were Receiving ≥2 IVI Infusions per Month |
Additionally, for the 71 patients who reported missing an infusion, the monthly mean (±SD [median]) reported time spent on appointment logistics included 45.8 (±81.3 [20.0]) minutes scheduling infusions, 75.7 (±74.1 [45.0]) minutes traveling to appointments, 51.0 (±57.9 [30.0]) minutes waiting for the infusion after arriving at the appointment, and 88.7 (±67.1 [75.0]) minutes receiving their infusions. The most common reasons for missing infusion appointments were due to an unforeseen conflict (45.1%), being unable to fit the appointment into their schedule (29.6%), and transportation difficulties (26.8%; Figure 2).
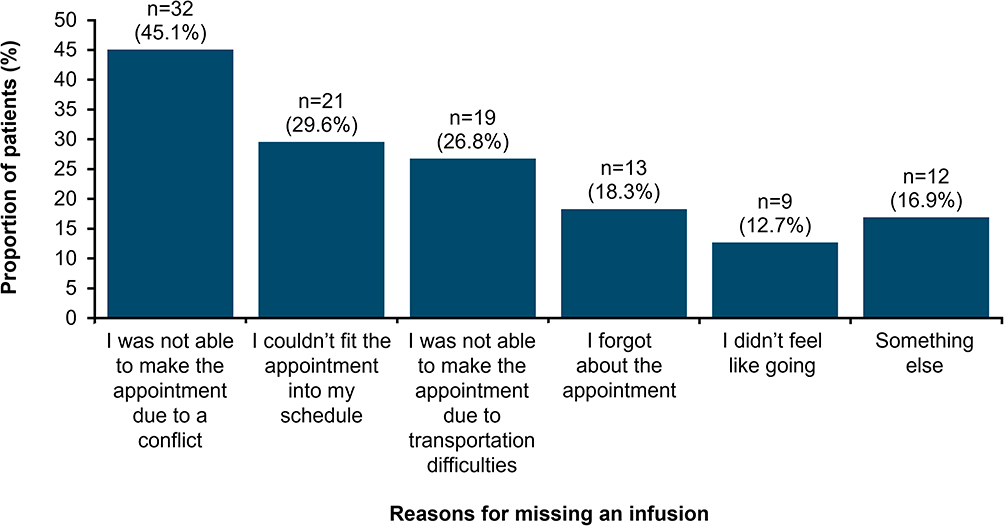 |
Figure 2 Reported reasons for missing an IVI infusion. Abbreviation: IVI, intravenous iron. |
Patient Satisfaction
Over a third of the 71 patients who missed an infusion as part of their IVI treatment course reported being dissatisfied with the frequency of their IVI infusions (38.1%) compared with less than a third of the 122 patients who had never missed an infusion (28.7%; Figure 3A). In comparison, just 15.7% of the 115 patients who were receiving 1 infusion per month were dissatisfied with the frequency of their infusions (data not shown; 15 patients were unsure of their infusion frequency). Patients who reported missing an infusion compared with those who never missed an infusion were more likely to feel that they had to schedule their life around current IVI infusions (80.2% vs 58.2%), that getting IVI infusions made them miss important events (64.8% vs 36.1%), and that IVI infusions got in the way of being productive (63.4% vs 46.7%) (Figure 3B). Most patients receiving ≥2 IVI infusions per month also agreed that they wanted the most convenient IDA treatment (94.3% and 96.7%; Figure 3B).
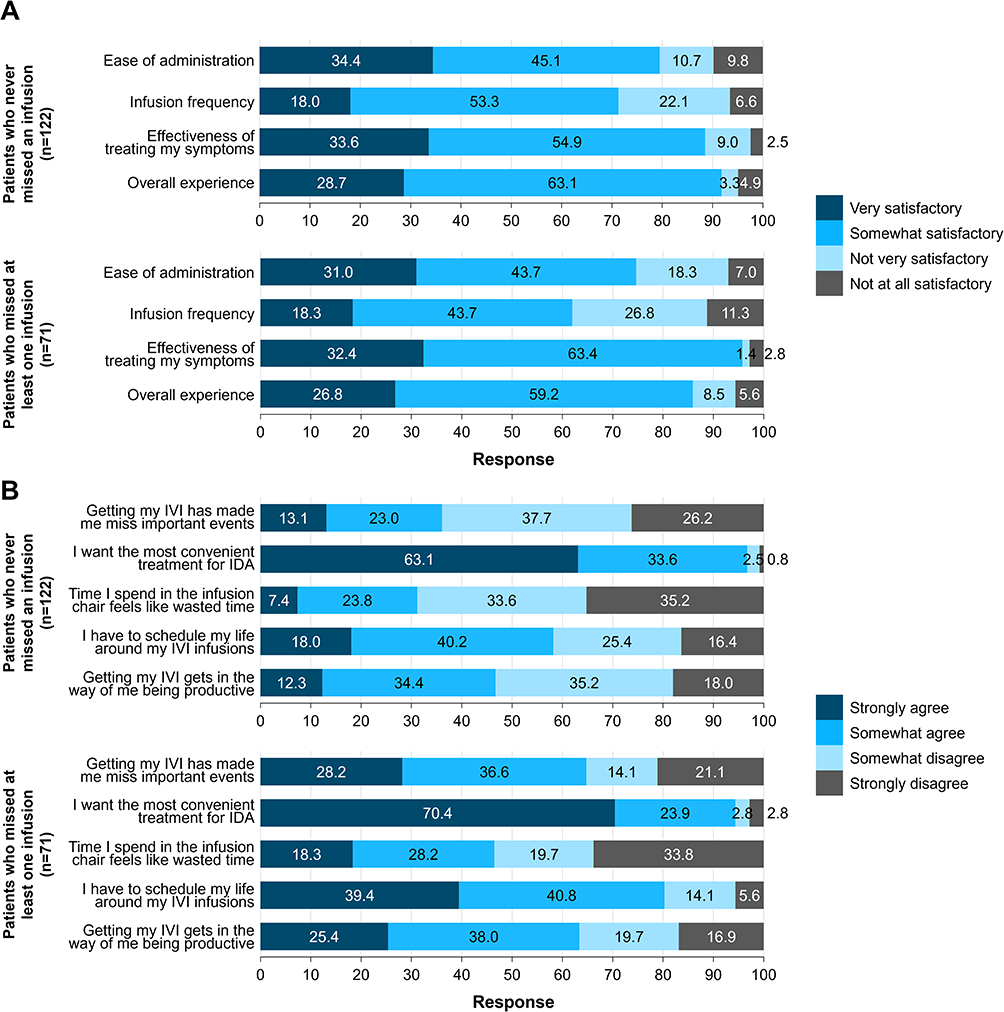 |
Figure 3 Response rates regarding IVI treatment and QoL aspects from patients who were prescribed ≥2 IVI infusions per month. (A) Response rates regarding IVI therapy experiences. (B) Aspects regarding QoL. Data reported from patients who were receiving ≥2 IVI infusions per month, grouped by whether they have ever missed an IVI infusion. Abbreviations: IDA, iron deficiency anemia; IVI, intravenous iron; QoL, quality of life. |
When considering optimal IVI treatment among those who had missed an infusion, the most common considerations for improving the IVI treatment experience were “fewer appointments” (60.6%), “fewer infusions/needle sticks” (56.3%), and “less time spent traveling to appointments” (43.7%; Figure 4A). Most patients who had missed an infusion also agreed that fewer trips to receive their IVI therapy would be better (78.8%) and that they would attend more, if not all, of their IVI therapy appointments if they were less frequent (84.5%; Figure 4B). Most of these patients (90.1%) also agreed that they would be interested in receiving single-dose IVI therapy options if available (Figure 4B).
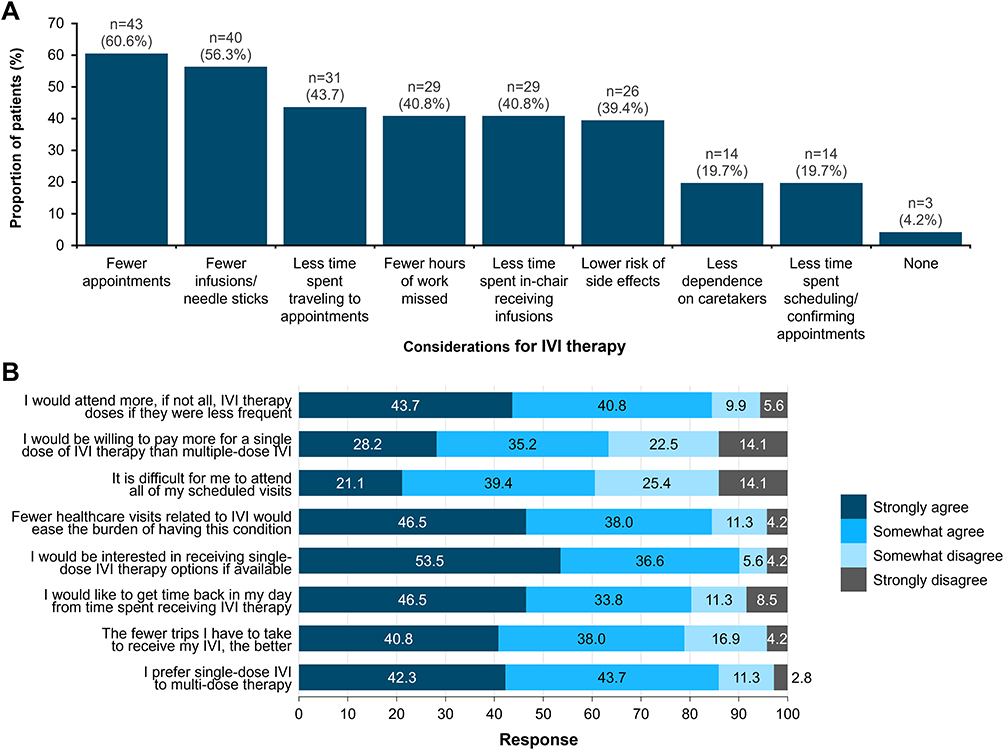 |
Figure 4 Considerations regarding optimal IVI therapy. (A) Considerations regarding optional IVI therapy. (B) Agreement levels regarding optimal IVI therapy. Data reported from the 71 patients who reported missing a dose of their IVI therapy. Abbreviation: IVI, intravenous iron. |
Discussion
For patients with IDA, IVI therapy has been shown to be well tolerated and effective in increasing hemoglobin levels, reducing fatigue, and increasing energy and vitality.27 In this study, fatigue, weakness, and dizziness, which were reported as the most common symptoms before IVI therapy, improved in over 60% of patients receiving multiple-dose IVI. However, some symptoms persisted and only 28.6% of ADLs improved in more than half of patients. These outcomes may reflect missed infusions, the short duration of this survey timeframe, or even the point in the treatment course in which the survey was completed; patients may not have been on IVI therapy long enough for full therapeutic benefits to be realized.
Results of this survey showed significant challenges with adherence to IVI therapy for IDA, despite its therapeutic benefits. Patients who reported nonadherence were predominantly females who were employed and had children, experienced fatigue, and had underlying causes of IDA that often required more than one course of IVI treatment. Although it remains unclear which specific patient characteristics increase the likelihood of missing an infusion, treatment logistics could play a role. Those who missed an infusion reported spending approximately four hours per infusion on IVI appointment logistics, including scheduling, traveling, waiting, and IVI administration. These burdens negatively affected their QoL, including productivity and missing important events. Consequently, the 71 patients who missed an infusion expressed a preference for single-dose IVI therapy, and most were interested in switching to a single-dose IVI therapy option if available. Patients who missed a dose of their IVI therapy agreed that fewer infusions, fewer trips to receive their IVI therapy, and a single-dose option could improve adherence. Notably, approximately two-thirds of patients who missed an IVI infusion stated that they would be willing to pay more for single-dose IVI.
These results align with those from a retrospective study of US administrative claims data of nearly 25,000 patients, where 32.5% of patients were discordant (nonadherent) to IVI treatment that required two or more infusions.16 Together, these data demonstrate a significant compliance issue for formulations that do not offer iron correction in one visit — even for patients in urban areas, where there are typically fewer healthcare barriers than in suburban areas.28 The association between patient experience (including preference and satisfaction) and adherence has been extensively studied,29–31 highlighting the significance of this quality-of-care metric for healthcare organizations, and the potential to impact reimbursement for certain population coverage (eg, Medicare). The current study provides insights into the importance of aligning therapy with patient preferences, as 94% of patients reported that they wanted the most convenient treatment option for IDA.
Other than logistical barriers, some patients may also have a negative perception of the infusion itself.32 This could be a contributing factor behind why patients within the current study reported a strong preference for “fewer infusions/needle sticks” and “single-dose IVI therapy options if available”. The latter also suggests that some patients do not have a choice in their IVI therapy and may be unaware of single-dose IVI therapy; the IVI product prescribed often depends on insurance coverage (which may require step therapy — failure of older-generation IVI before covering newer-generation products), formulary availability, and physician preference.11,33
The preference for single-dose IVI reported here was not only driven by the logistical challenges of multiple appointments, but also by a desire to enhance overall satisfaction. Many patients reported that frequent infusions disrupted their lives and negatively impacted their QoL, which in turn contributed to their nonadherence. Common negative beliefs about multiple-dose IVI therapy included the feeling of having to schedule life around infusions, missing important events, and interference with productivity, concerns that may be evident given that most of these patients were employed. With much time spent on IVI appointment logistics (a component of some hospital satisfaction scores),30 more than one-third of patients prescribed multiple-dose IVI were not satisfied with their infusion frequency. These findings highlight a crucial link between patient satisfaction, therapy choice, and treatment adherence.
The convenience of safely receiving a full iron treatment course as a single-dose IVI infusion may ease the burden of appointment logistics for many patients, as the efficacy and safety of single-dose IVI infusions have been proven to be comparable to multiple-dose treatment courses.34 Single-dose IVI infusions also allow hemoglobin and ferritin levels to increase faster compared to multiple lower doses.34,35 Therefore, to improve patient adherence, patient convenience should be another clear factor to consider in addition to formulary, insurance coverage, and healthcare provider preference. However, though there are IVI products that are both FDA-approved and used off-label for single-dose infusion, it is important to recognize that IVI products have distinct properties and varying safety profiles, and the number of infusions and/or duration required to deliver the desired dose requirements may affect compliance.35 Adverse events such as hypersensitivity reactions, hypophosphatemia, osteomalacia/fractures, and even cardiovascular risks must be considered when selecting the product and dosing strategy, as these can further impact the patient experience.16,36
The cost of IVI therapy was not specifically covered in this patient survey, but cost has been previously reported.11 While the cost can vary substantially depending on the formulation used and the number of infusions required, IVI is indeed a higher cost option than oral iron treatment.11 However, a more significant cost to the healthcare system is that of untreated IDA.11 Single-dose IVI options, as well as being preferred by patients, may help reduce overall healthcare expenditures by improving adherence, minimizing missed appointments, and potentially reduce the need for repeat treatment courses or additional interventions.
While some aspects of the results, such as patient preference for fewer infusions, may seem apparent from the patient perspective, this study is the first to quantify the logistical burden of multiple-dose IVI therapy from the patient perspective in those with IDA using real-world survey data. The extent to which patients reported having to schedule their lives around treatment, missing important events, and experiencing reduced productivity was notably high and provides new insight into the lived experience of IVI therapy. The strong preference for single-dose IVI options, even among patients who had not missed doses, highlights a broader unmet need. However, payor policies often prioritize cost over convenience, overlooking how the number of IVI infusions per treatment course and the duration of infusion can negatively influence treatment adherence and affect the patients’ ability to perform daily activities. Some state-level insurance laws do offer exceptions to step-based therapy based on criteria such as treatment adherence or a decline in the ability to perform daily activities, but most do not.37 While drug cost is an important factor of insurance coverage and payor policies, it is essential to consider other holistic, patient-centered factors, including what is best for the patient, to improve access to care.
This study reinforces the importance of considering patient preference, satisfaction, and convenience when selecting IVI therapy for patients with IDA. Addressing logistical challenges with single-dose IVI options has the potential to improve adherence, reduce treatment burden, and ultimately, enhance patient outcomes. Aligning therapy with patient needs helps mitigate barriers that currently hinder effective management of IDA.
Limitations
This observational study is limited by a small sample size and self-report bias; however, anonymizing survey responses likely mitigated this limitation by encouraging patients to provide honest feedback. Additionally, although 323 patients completed the survey, as the survey was conducted by a third-party polling organization, data on the number of patients approached versus those who declined to participate were not collected or made available, so the response rate could not be determined. Most questions in the survey had fixed answer choices, meaning there was limited ability to explore answers further and so the results depended on whether patients fully interpreted the questions correctly. The survey also did not capture information regarding specific iron formulations or the reason for why patients received a specific formulation. Furthermore, the survey was limited to patients who were currently receiving or who had recently received IVI therapy, so the results may not represent the perspective of all patients who have completed a full course of treatment. Adverse events of IVI were also not captured by the survey; however, hypophosphatemia has been reported in a separate analysis on a subset of patients who were receiving IVI due to heavy menstrual bleeding.26 Symptom improvement results should be interpreted with caution as it can take weeks for iron parameters and symptoms to improve, and it is unclear when patients were surveyed in relation to their IVI infusions. Patients should be made aware of this delay in treatment response and report any later complications following IVI treatment. Together, the results of this survey suggest that further research should be conducted with a larger sample size and other indications for IVI treatment to fully understand how to improve adherence.
Conclusion
This study highlights that over one-third of patients with IDA prescribed multiple-dose IVI therapy reported nonadherence, with the most common reasons being due to unforeseen appointment conflicts, scheduling difficulties, and transportation challenges. Nonadherence was particularly prevalent among patients who reported greater life demands, specifically, younger females with children and employment responsibilities, as these demographics were more common among those who missed at least one IVI infusion. Patients who missed doses reported a preference for fewer infusions and single-dose IVI therapy options when available. QoL impacts included reduced productivity, missing important events, and feeling the needed to schedule life around treatment. Fully understanding the reasons why patients with IDA do not adhere to treatment is essential to ensure patients complete their course of IVI therapy. Patient preference, satisfaction, and convenience all play important roles in adherence to IVI therapy and should be considered for payor and insurance policies, and for clinicians when choosing the treatment for patients. Offering rapid iron replacement using single-dose IVI not only aligns with patient preferences but may potentially improve adherence, reduce the burden of treatment, and ultimately enhance patient outcomes. These findings reinforce the importance of a patient-centered approach in the selection of IVI therapy.
Abbreviations
ADL, activities of daily living; ASP, average selling price; FDA, Food and Drug Administration; IDA, iron deficiency anemia; IRB, institutional review board; IVI, intravenous iron; QoL, quality of life; SD, standard deviation; US, United States.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are not publicly available as on-going sub-analyses are not yet complete and/or published.
A separate analysis of data from the survey used in this publication has also been published by Akpan IJ, Narang M, Zampaglione E, et al. Womens Health (Lond). 2025;21:17455057251321221, which focuses on the cohort of patients with IDA due to heavy menstrual bleeding. This publication also included a subpopulation of patients with IDA due to heavy menstrual bleeding who were receiving ≥2 IVI infusions per month, those who reported a missed dose, and those who reported hypophosphatemia as an adverse event.
Ethics Approval and Informed Consent
Ethical approval was not required since the study was non-interventional, not intended to provide clinical data to support treatment decisions, and was not conducted as a clinical trial for any endpoints. The survey was conducted by The Harris Poll, a well-established and highly regarded organization that adheres to the American Association for Public Opinion Research’s Code of Professional Ethics and Practices. As the online survey posed no risk of harm to respondents, was anonymized, and non-interventional, a separate IRB review was not deemed necessary, consistent with other Harris Poll surveys published in the scientific peer-reviewed literature. The study complies with the Declaration of Helsinki and all patients provided informed consent before completing the survey in this study.
Acknowledgments
We would like to thank The Harris Poll for conducting this survey and Ben McDermott of the Bioscript Group (Macclesfield, UK), who provided medical writing assistance in accordance with Good Publication Practice, which was funded by Pharmacosmos Therapeutics Inc.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was sponsored by PharmacosmosTherapeutics Inc.
Disclosure
E-JL, reports medical consultancy fees from Sanofi. LL and JA report funding from Pharmacosmos Therapeutics Inc., for separate research studies; JA has in place an approved plan with the University of South Florida for managing any potential conflicts of interest arising from this involvement. BJW declares non-financial support from Pharmacosmos, during the conduct of the study. JS reports speaker fees and honoraria from PharmacosmosTherapeutics Inc., Incyte Corporation, Exelixis Inc., Servier Pharmaceuticals, Amgen Inc., and BeiGene Inc. The authors report no other conflicts of interest in this work.
References
1. Miller JL. Iron deficiency anemia: a common and curable disease. Cold Spring Harb Perspect Med. 2013;3(7):a011866. doi:10.1101/cshperspect.a011866
2. Sun H, Weaver CM. Decreased iron intake parallels rising iron deficiency anemia and related mortality rates in the US population. J Nutr. 2021;151(7):1947–1955. doi:10.1093/jn/nxab064
3. Moss AS, Pakbaz Z. Iron deficiency - more than just anemia: a literature review. J Community Hosp Intern Med Perspect. 2025;15(3):38–45. doi:10.55729/2000-9666.1481
4. Auerbach M, DeLoughery TG, Tirnauer JS. Iron deficiency in adults: a review. JAMA. 2025;333(20):1813–1823. doi:10.1001/jama.2025.0452
5. Patil AV, Malagi U. Iron deficiency anaemia: an overview. Pharma Innovation. 2019;8(9):523–527.
6. Wouters HJCM, van der Klauw MM, de Witte T, et al. Association of anemia with health-related quality of life and survival: a large population-based cohort study. Haematologica. 2019;104(3):468–476. doi:10.3324/haematol.2018.195552
7. Blumenstein I, Shanbhag S, Langguth P, et al. Newer formulations of intravenous iron: a review of their chemistry and key safety aspects – hypersensitivity, hypophosphatemia, and cardiovascular safety. Expert Opin Drug Saf. 2021;20(7):757–769. doi:10.1080/14740338.2021.1912010
8. DeLoughery Thomas G. Safety of oral and intravenous iron. Acta Haematol. 2019;142(1):8–12. doi:10.1159/000496966
9. Arastu AH, Elstrott BK, Martens KL, et al. Analysis of adverse events and intravenous iron infusion formulations in adults with and without prior infusion reactions. JAMA Network Open. 2022;5(3):e224488. doi:10.1001/jamanetworkopen.2022.4488
10. LaVallee C, Bansal I, Kamdar S, et al. Relationship between initial parenteral iron therapy dosing and treatment effectiveness: a real-world retrospective analysis. J Blood Med. 2022;13:133–142. doi:10.2147/JBM.S349070
11. Kumar A, Sharma E, Marley A, et al. Iron deficiency anaemia: pathophysiology, assessment, practical management. BMJ Open Gastroenterol. 2022;9(1):e000759. doi:10.1136/bmjgast-2021-000759
12. Monoferric® (ferric derisomaltose). Prescribing information. Pharmacosmos UK Ltd; 2023. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/208171s000lbl.pdf.
13. Ferrlecit® (sodium ferric gluconate). Prescribing information. Sonafi-Aventis U.S. LLC; 2022. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2022/020955s020lbl.pdf.
14. Upadhyay A, Polson M. Intravenous iron treatment considerations in patients with non-dialysis dependent chronic kidney disease.
15. Kidney Disease: Improving Global Outcomes (KDIGO) Anemia Work Group. KDIGO clinical practice guideline for anemia in chronic kidney disease. Kidney Inter. 2012;2:279–335.
16. Polson MK, Bahrain H, Ogden JF, et al. Financial burden associated with discordance to intravenous iron therapies in US patients with iron deficiency anemia. J Manag Care Spec Pharm. 2023;29(7):818–824. doi:10.18553/jmcp.2023.22407
17. Venofer® (iron sucrose). Prescribing information. American Regent, Inc; 2017. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2017/021135s032lbl.pdf.
18. CosmoFer® (iron dextran). Prescribing information. Pharmacosmos UK Ltd; 2023. Available from: https://www.medicines.org.uk/emc/product/48/smpc.
19. Auerbach M, Macdougall I. The available intravenous iron formulations: history, efficacy, and toxicology. Hemodial Int. 2017;21(S1):S83–S92. doi:10.1111/hdi.12560
20. Injectafer® (ferric carboxymaltose). Prescribing information. American Regent, Inc; 2021. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2021/203565s014lbl.pdf.
21. Feraheme® (ferumoxytol). Prescribing information. AMAG Pharmaceuticals, Inc; 2015. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2015/022180s011s013lbl.pdf.
22. Van Doren L, Steinheiser M, Boykin K, et al. Expert consensus guidelines: intravenous iron uses, formulations, administration, and management of reactions. Am J Hematol. 2024;99(7):1338–1348. doi:10.1002/ajh.27220
23. Strauss WE, Auerbach M. Health-related quality of life in patients with iron deficiency anemia: impact of treatment with intravenous iron. Patient Relat Outcome Meas. 2018;9:285–298. doi:10.2147/PROM.S169653
24. Marbouh D, Khaleel I, Al Shanqiti K, et al. Evaluating the impact of patient no-shows on service quality. Risk Manag Healthc Policy. 2020;13:509–517. doi:10.2147/RMHP.S232114
25. Medi-Span Price Rx: online drug pricing tool. Wolters Kluwer. Available from: https://www.wolterskluwer.com/en/solutions/medi-span/price-rx.
26. Akpan IJ, Narang M, Zampaglione E, et al. Iron deficiency anemia in patients with heavy menstrual bleeding: the patients’ perspective from diagnosis to treatment. Womens Health. 2025;21:17455057251321221.
27. Vadhan-Raj S, Strauss W, Ford D, et al. Efficacy and safety of IV ferumoxytol for adults with iron deficiency anemia previously unresponsive to or unable to tolerate oral iron. Am J Hematol. 2014;89(1):7–12. doi:10.1002/ajh.23582
28. Brems C, Johnson ME, Warner TD, et al. Barriers to healthcare as reported by rural and urban interprofessional providers. J Interprof Care. 2006;20(2):105–118. doi:10.1080/13561820600622208
29. NEJM Catalyst. Patient satisfaction surveys. Catalyst Carryover. 2018;4(1). doi:10.1056/CAT.18.0288
30. Anhang Price R, Elliott MN, Zaslavsky AM, et al. Examining the role of patient experience surveys in measuring health care quality. Med Care Res Rev. 2014;71(5):522–554. doi:10.1177/1077558714541480
31. Berkowitz B. The patient experience and patient satisfaction: measurement of a complex dynamic. Online J Issues Nurs. 2016;21(1):1. doi:10.3912/OJIN.Vol21No01Man01
32. Alsbrooks K, Hoerauf K. Prevalence, causes, impacts, and management of needle phobia: an international survey of a general adult population. PLoS One. 2022;17(11):e0276814. doi:10.1371/journal.pone.0276814
33. Rund D. Intravenous iron: do we adequately understand the short- and long-term risks in clinical practice? Br J Haematol. 2021;193(3):466–480. doi:10.1111/bjh.17202
34. Auerbach M, Henry D, Derman RJ, et al. A prospective, multi-center, randomized comparison of iron isomaltoside 1000 versus iron sucrose in patients with iron deficiency anemia; the FERWON-IDA trial. Am J Hematol. 2019;94(9):1007–1014. doi:10.1002/ajh.25564
35. Gozzard D. When is high-dose intravenous iron repletion needed? Assessing new treatment options. Drug Des Devel Ther. 2011;5:51–60. doi:10.2147/DDDT.S15817
36. Schaefer B, Tobiasch M, Wagner S, et al. Hypophosphatemia after intravenous iron therapy: comprehensive review of clinical findings and recommendations for management. Bone. 2022;154:116202. doi:10.1016/j.bone.2021.116202
37. Aimed Alliance State Report. Step Therapy, Oversight, and Artificial Intelligence. 2025. Available from: https://aimedalliance.org/wp-content/uploads/2025/06/AA-2025StateReport_June_2025.pdf.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Decrease in Hb and Hypoproteinemia: Possible Predictors of Complications in Neonates with Late-Onset Sepsis in a Developing Country
Cai N, Liao W, Chen Z, Tao M, Chen S
International Journal of General Medicine 2022, 15:6583-6589
Published Date: 13 August 2022
Dapagliflozin Improves Erythropoiesis and Iron Metabolism in Type 2 Diabetic Patients with Renal Anemia
Osonoi T, Shirabe S, Saito M, Hosoya M, Watahiki N, Douguchi S, Ofuchi K, Katoh M
Diabetes, Metabolic Syndrome and Obesity 2023, 16:1799-1808
Published Date: 20 June 2023
Patient-Reported Outcomes After Ferric Carboxymaltose Treatment for Iron Deficiency Anemia: A Prospective Observational Study
Kwong WJ, Numan S, Hunter TD, Alves D, Patel A, Shanbhag S
International Journal of General Medicine 2023, 16:3291-3300
Published Date: 2 August 2023
Anemia in Heart Failure: A Perspective from 20-Year Bibliometric Analysis
Yang Q, Dong T, Lyu D, Xue D, Zhuang R, Ma L, Zhang L
International Journal of General Medicine 2024, 17:1845-1860
Published Date: 2 May 2024
Inflammatory Monocyte Subsets Correlation with Iron Levels in Low Vitamin D Pediatric Transfusion-Dependent Thalassemia
Ghozali M, Matahari M, Cahyadi AI, Agustini SD, Ghrahani R, Reniarti L, Setiabudiawan B, Panigoro R
Journal of Inflammation Research 2025, 18:421-429
Published Date: 8 January 2025