Back to Journals » International Journal of General Medicine » Volume 17
Anemia in Heart Failure: A Perspective from 20-Year Bibliometric Analysis
Authors Yang Q ![]() , Dong T
, Dong T ![]() , Lyu D, Xue D, Zhuang R, Ma L, Zhang L
, Lyu D, Xue D, Zhuang R, Ma L, Zhang L
Received 28 January 2024
Accepted for publication 27 April 2024
Published 2 May 2024 Volume 2024:17 Pages 1845—1860
DOI https://doi.org/10.2147/IJGM.S456558
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Redoy Ranjan
Qiwen Yang,1,2,* Tairan Dong,1,* Diyang Lyu,2 Donghua Xue,1,2 Rui Zhuang,2 Liyong Ma,2 Lijing Zhang2
1Graduate School, Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 2Department of Cardiology, Dongzhimen Hospital, Beijing University of Chinese Medicine, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Lijing Zhang, Department of Cardiology, Dongzhimen Hospital, Beijing University of Chinese Medicine, Beijing, People’s Republic of China, Email [email protected]
Background & Objective: Anemia in patients with heart failure (HF) is a growing concern. However, there has no bibliometric analysis in this area up to now. The aim of this study is to explore the status and trends in the field of anemia in HF through the bibliometric analysis, and to provide an outlook on future research.
Methods: We retrieved publications from the Web of Science Core Collection database, and the following data analysis and visualization tools were utilized to perform data processing, statistical computing and graphics generation: VOSviewer (v.1.6.18), CiteSpace (v.6.2 R5), Scimago Graphica (v.1.0.36), Biblimatrix and Microsoft Excel.
Results: We identified a total of 3490 publications from 2004 to 2023. The publications in the field of anemia in HF are growing steadily. The United States, the United Kingdom, and Italy were the leading countries in this area. Stefan D Anker, as the most influential author, held the most total citations and publications. Harvard University was the most productive institution in this area. The European Journal of Heart Failure had published the most papers. Through the analysis of co-citations, 14 major clusters based on cluster labels were identified. Keyword analysis showed that mortality, outcome, prevalence, and risk were the most frequent keywords, and the potential research hotspots in the future will be intravenous iron and iron deficiency.
Conclusion: This study provides a comprehensive analysis of countries, authors, institutions, journals, co-cited references, and keywords in the field of anemia in HF through bibliometric analysis and data visualization. The status, hotspots and future trends in this field offer a reference for in-depth research. Further studies are necessary in the future to broaden the spectrum of research in this field, to evaluate comprehensive approaches to treating anemia in patients with HF, and to find rational targets for the management of anemia.
Keywords: anemia, heart failure, hemoglobin, iron deficiency, bibliometrics
Introduction
Heart failure (HF) is a common clinical syndrome that can be caused by a variety of cardiac diseases and often identified by characteristic symptoms such as fatigue and dyspnea caused by structural or functional defects in ventricular filling or ejection of blood.1–4 It is estimated that about 64 million people worldwide suffer from heart failure.5 Due to the fact that most clinical studies include only confirmed cases of HF, the true prevalence is likely to be higher.6 The clinical burden of HF includes impaired quality of life,4,7 high rates of hospitalization,8,9 and poor prognosis.10,11 Considering the current state of HF, its prevention and management has become a formidable task.
Anemia is also a global public health concern12,13 with a significant impact on both morbidity and mortality.4,14,15 It is defined by the World Health Organization (WHO) as a serum hemoglobin level of less than 13 g/dL for adult males and less than 12 g/dL for adult females.16 The WHO criteria are widely used to define anemia in HF patients.4,17,18 It is estimated that the prevalence of anemia is 17% in patients with new-onset HF and ≈30% in stable and ≈50% in hospitalized HF patients.18,19 Unfortunately, this is a more serious problem for developing countries. Compared to in Sweden, HF patients in Tanzania have more frequent anemia (57% vs 9%).20 And in Egypt, the prevalence of anemia in non-hospitalized HF patients is up to 62.9%.21 Reduced hemoglobin concentration leads to impaired oxygen-carrying capacity of the blood, and anemia may lead to exercise intolerance when compensations of the cardiovascular and skeletal muscle systems are exceeded. This generally happens only for severe anemia but may happen for a lesser degree of anemia in patients with HF.22 As a consequence, compared with patients with normal hemoglobin, anemic HF patients have lower peak oxygen consumption (peak VO2)23 and shorter distances during the 6-minute walk test.24 In addition, observational studies and meta-analysis have suggested that anemia is associated with an increased risk of poor prognosis in patients with HF.19,25–27 Therefore, anemia should be considered as an important prognostic-related factor in patients with HF. Optimizing the management of anemia in HF is key to improving the quality of life and reducing the risk of hospitalization and mortality, and research is advancing in this area. A recent high-quality review summarized current treatment for anemia in HF.17 However there is still a lack of studies that illustrate the structure and frontiers of this complex field.
Bibliometrics is a cross-discipline science that combines statistical and mathematical methods and is commonly applied to quantitative analysis of academic publications.28 It is a combination of mathematics, statistics, and bibliography that visually reveals the evolution and frontiers of a particular field. Comprehensive bibliometric studies can advance a field in novel and meaningful ways.29 Bibliometric analysis has been widely performed in studies related to HF,30,31 but little has concerned anemia in HF. Regarding the importance of anemia in HF, this study aims to analyze the global publications in this field from 2004 to 2023 via a bibliometric perspective to gain insights into: (i) the countries, authors, institutions, journals, co-cited references, and keywords; (ii) the current status, hotspots and future trends of research in the field of anemia in HF.
Materials and Methods
Paper Retrieval and Data Extraction
We conducted a systematic literature search and data extraction from Web of Science Core Collection (WoSCC) database for published articles from 2004 to 2023. We used the search strategy TS = (“anemia” OR “anaemia”) AND TS = (“HF” OR “heart failure” OR “cardiac failure” OR “heart decompensation” OR “myocardial failure”) to retrieve articles and reviews related to anemia and HF. All publications were retrieved up to October 6, 2023. Only articles and reviews in English were included, while other forms of publications, such as meeting abstract, editorial material, letter, proceeding paper, early access, book chapters, correction, retracted publications were excluded. Duplicate publications were identified and removed using Citespace (v.6.2 R5). A total of 2938 articles and 552 reviews were obtained (Figure 1).
 |
Figure 1 Flow chart of publications selection. |
Bibliometric Analysis
We analyzed the bibliometric indicators, including the number of publications (NP) and total citations (TC), obtained from the WoSCC database to evaluate the quality of the publications. We employed statistical computing, graphics, and data visualization tools including VOSviewer (v.1.6.18), Citespace (v.6.2 R5), Scimago Graphica (v.1.0.36), Biblimatrix (a package for the R statistical programming language), and Microsoft Excel. CiteSpace was set up with the following parameters: (1) the time slice was set to 1 year; (2) the node type was set to “countries”, “institutions”, “authors”, and “keywords” respectively, to generate the co-occurrence networks; other parameters were set by default. In VOSviewer, we selected the minimum number of documents for the nodes according to the needs of data visualization and other documents were set by default. Most of the visualizations were produced by Citespace and VOSviewer. While Scimago Graphica was used to enhance the visual analysis of countries and publications, and trend topics by year were generated by Biblimatrix. Other variables including average article citations, total link strength, the publication year of start and centrality were analyzed by Citespace and Bibilimatrix, and collated using Microsoft Excel. As defined by Jorge E. Hirsch, the h-index is “the number of papers with citation number ≥ h”, which reflects the impact of a scientist’s cumulative research contributions.32 The h-index was obtained from Scopus (https://www.scopus.com).
Results
Annual Publication Trends
With our search strategy, we identified a total of 3490 publications (including 2938 articles and 552 reviews) from 2004 to 2023, containing 969 journals, 20,124 authors, 13,270 institutions. The annual publication volume is on the rise, reflecting the pace and progress of research in this field, as well as the level of interest it has generated. The cumulative publications can be accurately modeled by a quadratic function (R2=0.9999), indicating a consistent upward trend (Figure 2). We anticipate that this trend will remain stable in the future.
 |
Figure 2 Growth trend of publications from 2004 to 2023. |
Country Analysis
The analysis of publications from different countries provides valuable insights into the importance placed on a research area by a country and the degree of its influence in the area. Table 1 displays the top 10 countries receiving the most total citations (TC), which indicates a country’s influence and publication quality in the field of anemia in HF. The United States obtained the most citations (42,024) and publications (902), followed by the United Kingdom and Italy with 10,089 and 8971 total citations, respectively. Most countries in the table had an average of more than 30 citations per publication, except Japan and Spain, with 15.3 and 27.9 average citations respectively.
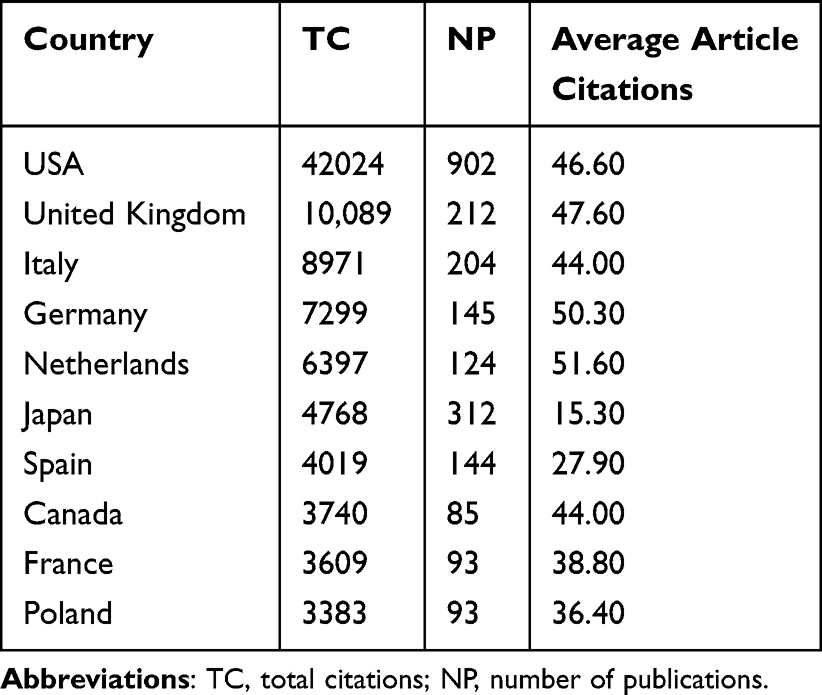 |
Table 1 Top 10 Countries Rated by Total Citations |
We utilized Vosviewer to generate cooperation and clusters between countries/regions of all authors, and Scimago Graphica to create a geographical map (Figure 3A). Among the different cooperative network clusters, inter-country cooperation was general, and the United States displayed a remarkable inter-country cooperation in this area. This finding suggests that countries should further deepen their cooperation to promote the development of the discipline. Figure 3B shows the trend over time in the number of publications from the top 10 countries with the most total citations. The number of publications in the United States has been far ahead from 2004 to 2023 and has maintained the highest growth rate. The publication rates of other countries have either remained stable or have shown a mild upward trend.
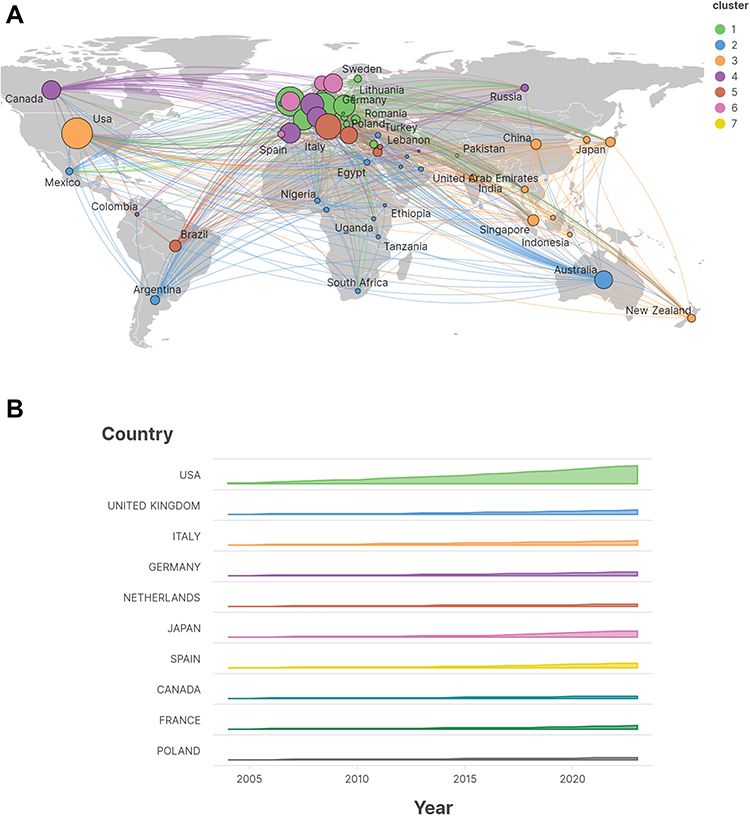 |
Figure 3 Country analysis. (A) The cooperation map of countries/regions. (B) The trend over time in the number of publications from the top 10 countries. |
Author and Institution Analysis
The top 10 authors with the highest number of publications are listed in Table 2. Stefan D Anker from Charité Campus Virchow-Klinikum, Berlin, Germany got the first place with both highest number of total citations (8426) and publications (87) in this area, followed by Piotr Ponikowski and Dirk J van Veldhuisen. Figure 4A presents the author co-occurrence network developed by Citespace. Authors with more citations and publications tend to collaborate more. Figure 4B shows the visualization of the earliest publication time and publication volume of institutions by year generated by Scimago Graphica, and top 10 institutions with the largest number of publications are listed in Table 3. Harvard University was the most productive institution with 138 articles, followed by University of Groningen with 114 articles, University of California System with 109 articles.
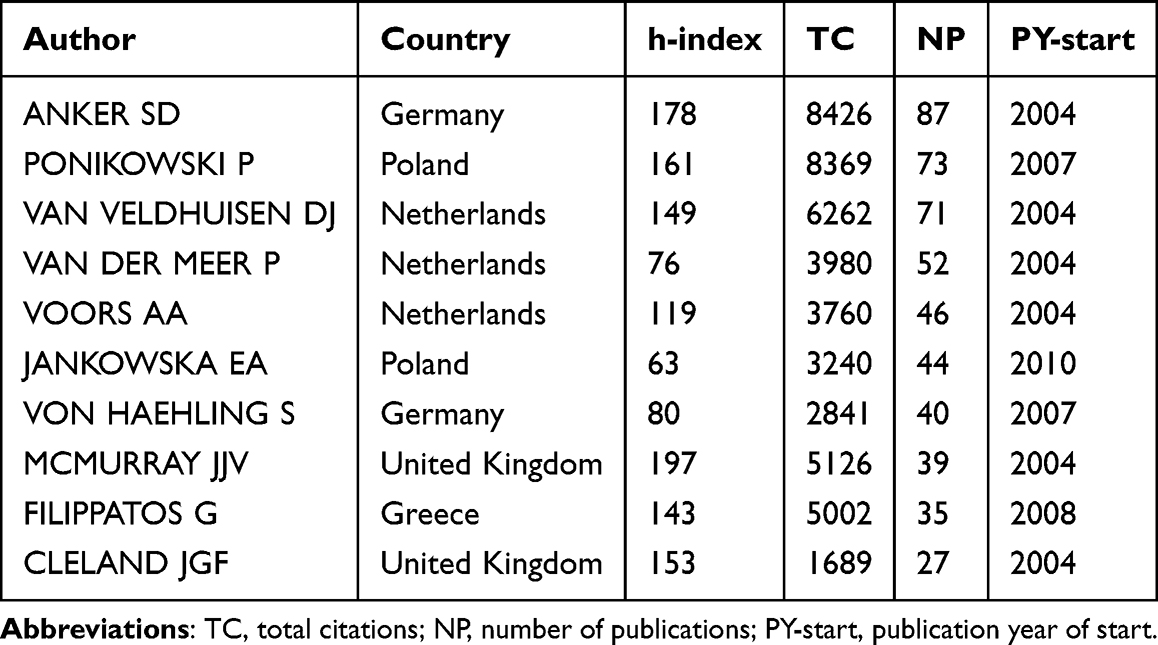 |
Table 2 Top 10 Authors Rated by the Number of Publications |
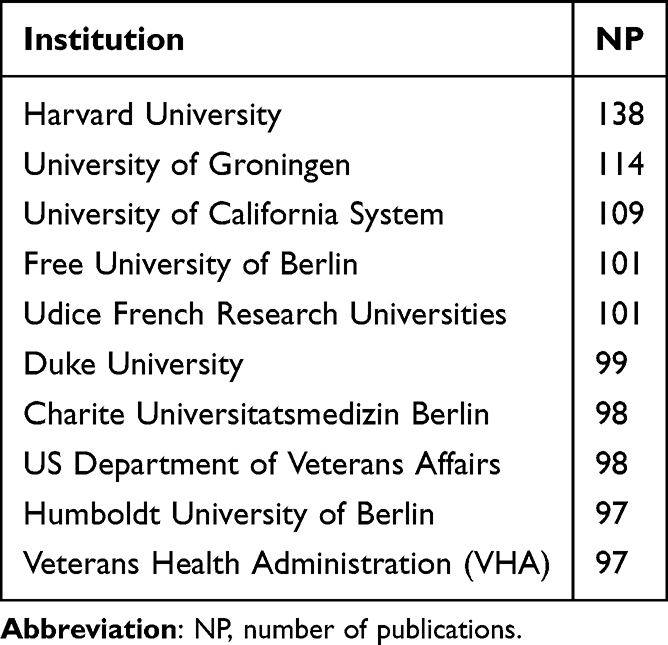 |
Table 3 Top 10 Institutions Rated by Number of Publications |
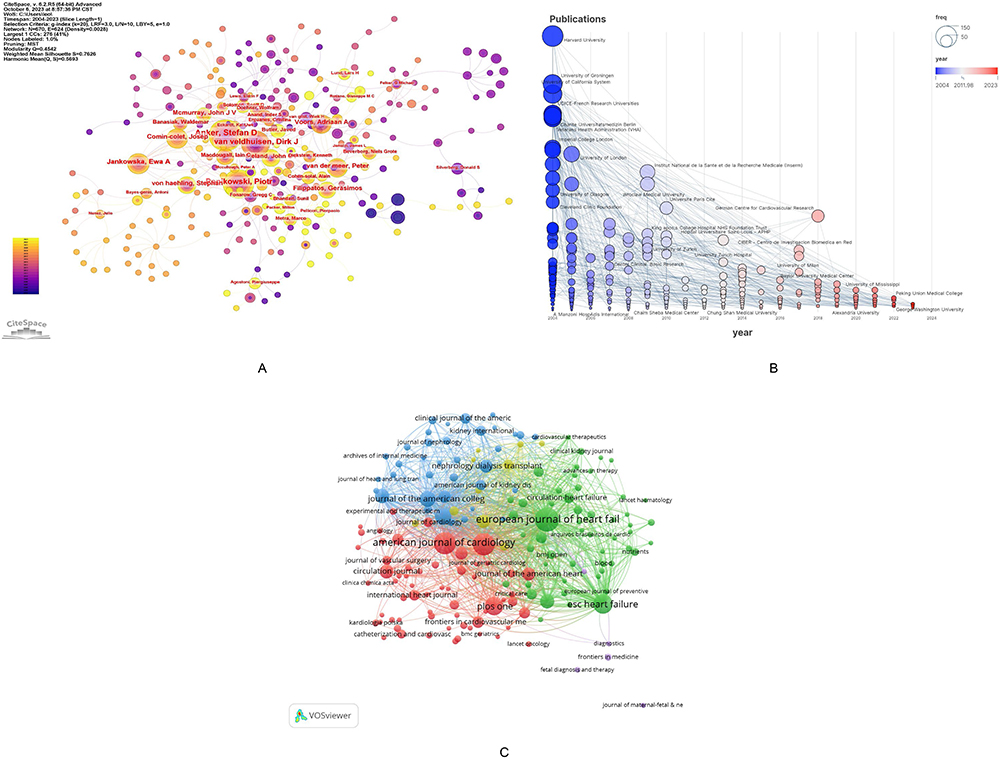 |
Figure 4 Analysis of authors, institutions, and journals. (A) Collaboration network of authors. (B) The earliest publication time and volume of institutions by year. (C) Co-occurrence map of journals. |
Bibliometric Analysis of Journals
The VOSviewer software was used to identify the most prominent and productive journals related to anemia in HF. In total, 3490 publications were found in 969 academic journals, and the top 10 journals with the most publications are listed in Table 4. European Journal of Heart Failure, with the impact factor (IF) of 18.2 according to Clarivate’s Journal Citation Reports, published the most papers with a total of 110. American Journal of Cardiology, with an IF of 2.8 and 94 publications, ranked second. International Journal of Cardiology was found to be the most cited journal. The journal co-occurrence map (Figure 4C) indicates that European Journal of Heart Failure is the largest node.
 |
Table 4 Top 10 Journals Rated by Number of Publications |
Reference Analysis
The reference co-citation analysis is one of the core functions of CiteSpace, which can extract cluster labels based on cited documents.33 The cited documents represent the research frontier and knowledge base.34 Therefore, analyzing typical clusters can help to understand the core information of research in this field, as well as its evolution and development. We set a recommended scale factor of k = 25 to identify homogenized groups of highly cited documents in the field. We also checked and explained the co-citation of references. Cluster analysis can be used to study the structure of knowledge and the boundaries of research interests. By conducting cluster analysis on co-cited documents, we summarized the research areas and identified hotspots, as well as research directions.35 From the 207 clusters extracted from a total of 81,462 references, we identified the 14 largest clusters based on cluster labels extracted from the title of cited publications using the Log-likelihood ratio (LLR) and mutual information (MI) algorithm, including #0 ferric carboxymaltose, #1 iron deficiency, #2 heart disease, #3 heart failure, #4 cardiovascular risk, #5 chronic heart failure, #6 treatment option, #7 sodium-glucose co-transporter, #8 cardiorenal syndrome, #9 red cell distribution width, #10 chronic obstructive pulmonary disease, #11 graft survival, #12 current intravenous iron preparation, #17 hospital-acquired anemia, see Figure 5.
 |
Figure 5 Cluster network of co-cited references and the dependencies between clusters. |
The modularity Q value was 0.7212, and the weighted mean silhouette of each cluster was 0.8948, indicating satisfactory cluster quality. Darker contours represent more recent clusters, such as #1 and #7, while lighter contours represent earlier clusters, such as #4 and #5. Node size in the network is proportional to the betweenness centrality, which measures the probability that a node lies on the shortest path between any two nodes in the network. Nodes with high betweenness centrality may act as mediators between different clusters or within clusters, facilitating the transformation of research topics and paradigms.36,37 Cluster dependencies reflect dependencies between clusters. For example, some clusters could build on several others, and one cluster may provide a knowledge base for several others. As shown in Figure 5, the arrows point to the earlier clusters, which indicates the dependencies between clusters and the evolution of research in the field. Cluster #2 and Cluster #0 are pivotal clusters. Meanwhile, Cluster #17 developed independently. Table 5 lists the top 10 references ranked by centrality. Five out of the top 10 references are in Cluster #0, and three in Cluster #2, indicating these two groups are the most influential clusters.
 |
Table 5 Top 10 References Ranked by Centrality |
Keywords
VOSviewer was utilized for keyword co-occurrence and clustering analysis. A total of 8910 keywords were extracted, of which 24 had more than 200 appearances and 46 had more than 100 appearances. The keyword density plot identified high frequency co-occurring words and revealed research hotspots (Figure 6C). Excluding search terms, the most significant keywords were mortality, outcome, prevalence, and risk. Clustering analysis was used to reveal the knowledge structure of the research area.36 Based on the strength of the links between the top 200 co-occurring keywords, the network was divided into four clusters with clear homogeneity among terms within each cluster (Figure 6A). The size of the nodes indicates the frequency of occurrence. Cluster 1 (red) was the largest and the most important cluster, containing 100 keywords, which is related to mortality, outcome, risk, and disease. Cluster 2 (green) comprised 41 keywords, containing prevalence, intravenous iron, ferric carboxymaltose, and iron deficiency. Cluster 3 (blue) contained 40 keywords, including chronic kidney disease, erythropoietin, risk factors, and congestive heart failure. Cluster 4 (yellow) was the smallest cluster with 16 keywords, including hemoglobin, morbidity, iron deficiency, and renal function.
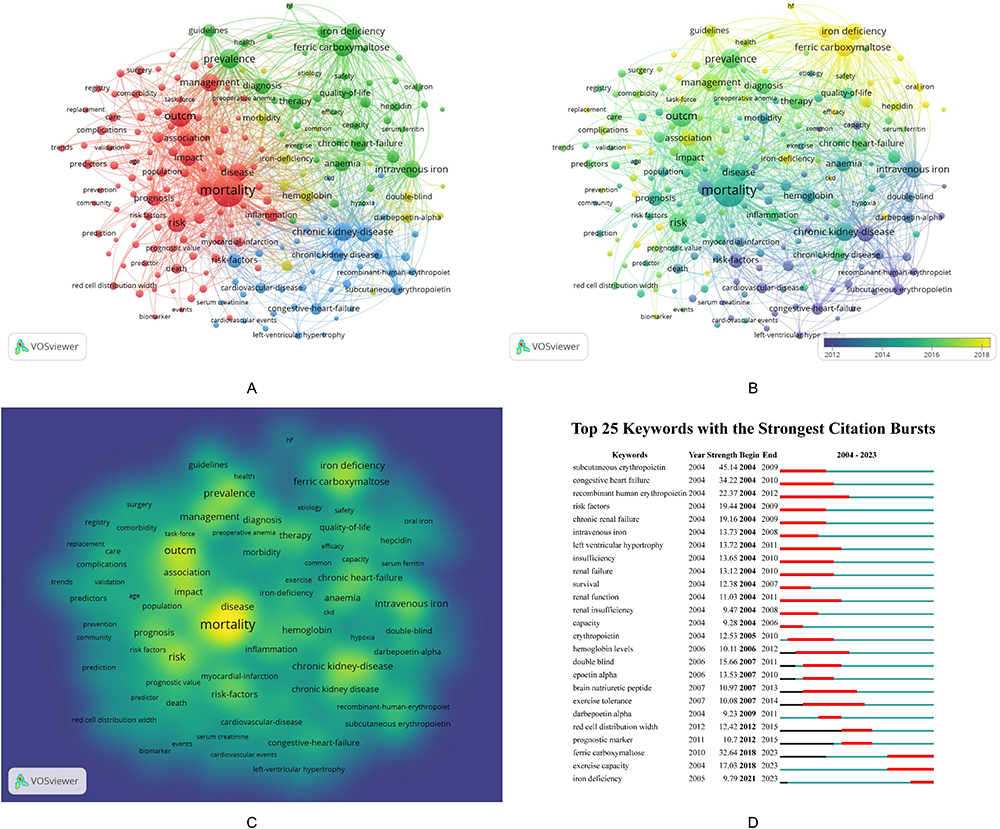 |
Figure 6 Keywords analysis. (A) Keyword co-occurrence network. (B) Keyword co-occurrence network based on publication time. (C) Density map of keywords. (D) Top 25 keywords with the strongest citation bursts. |
The timeline map of high-frequency keywords was generated by CiteSpace to display the evolutionary process in different clusters.38 Keyword bursts were utilized to detect the frequency and magnitude of keyword occurrences, which described the relationship between clusters from a temporal perspective. The keyword timeline map and burst analysis provided a depiction of the temporal characteristics of clustering. The color of each keyword was plotted according to the year it first appeared, and the color of the link indicated the year in which both keywords first appeared simultaneously (Figure 6B). We identified 25 keywords that represented the research field in terms of burst intensity, duration, and timing through CiteSpace for burst analysis of keywords (Figure 6D). Timeline analysis of keywords is shown in Figure 7A. Trend topics were generated by Biblimatrix for hotspots and trend analysis, see Figure 7B.
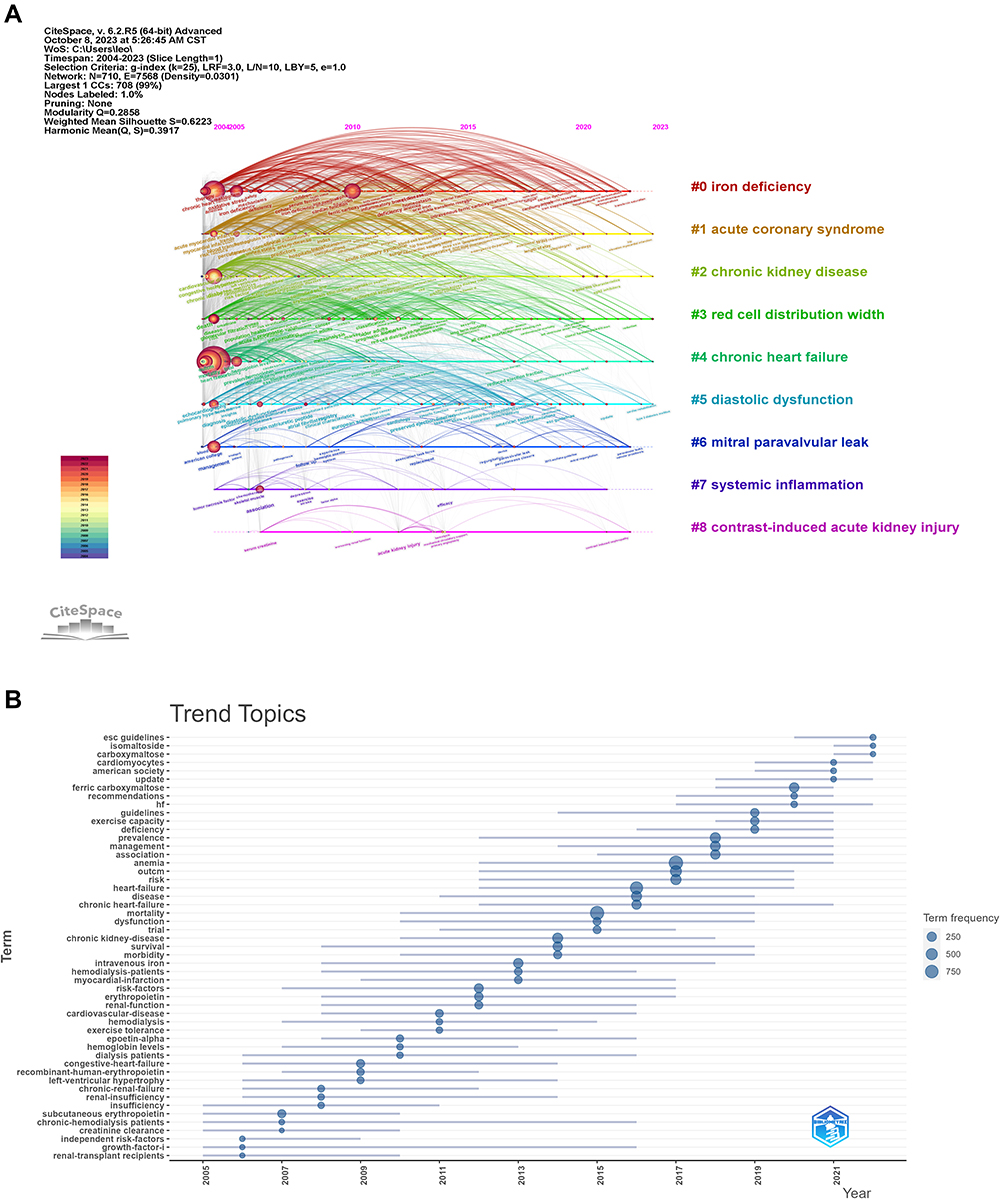 |
Figure 7 Timeline view and trend topics. (A) Timeline view of keywords categorized by cluster. (B) Trend topics in the field of anemia in HF. |
Discussion
Anemia significantly affects the prognosis of HF, and vigorously dealing with anemia improves the quality of life, as well as reduces the risk of hospitalization and death in HF patients.
Citespace and Vosviewer are now widely used to analyze scientific dynamics and hotspots that present the structure, patterns, and distribution of knowledge and summarize the relationships between authors, countries, journals, and institutions through visualized mapping. Our findings suggested that from 2004 to October 6, 2023, a total of 3490 papers and reviews were published. The number of publications within a certain period reflects trends in the impact of the research as well as the level of interest. As the trend in cumulative publications shows, publications related to anemia in HF are increasing, and nearly half of the total number of studies has been published in the last 7 years (2017–2023). This indicates that the field is gradually receiving more attention. One possible reason is that anemia was first recognized as one of the comorbidities associated with morbidity and mortality in the guidelines published in 2005 by the American College of Cardiology (ACC) and the American Heart Association (AHA).39 This may lead researchers to focus on the pathophysiology, pathogenesis, and treatment of anemia in heart failure. From that time on, the data has become increasingly extensive. As clinical evidence grew, in the 2021 Update to the 2017 ACC Expert Consensus Decision Pathway for Optimization of Heart Failure Treatment, one of 10 key points included anemia assessment and treatment throughout the hospitalization period.40 This may further promote investigations into the management of anemia in HF.
The total citations suggest that the United States, the United Kingdom, and Italy dominate the field. These countries (especially the United States) are the main connecting points for inter-country communication that promote international academic research and cooperation. Netherlands has more average article citations than any other country, demonstrating the high quality of its publications. Meanwhile, Japan is the only Asian country in the top 10 of total citations, but its average article citations are significantly lower than other countries, reflecting a need for improvement in the quality of research. China has cooperative relationships mainly with the United States and Asia-Pacific countries and given its high number of publications and low number of citations, it is recommended to deepen China’s cooperation with other countries to enhance international influence and the quality of research. Considering the publication trends, the number of publications in the United States has maintained a significantly higher growth rate than other countries. Combined with its top number of publications and total citations, this indicates that the United States is playing a leading role in the field of anemia in HF.
Interestingly, the top 10 authors are all from Europe, without any from the United States. Stefan D Anker from Germany has received numerous recognitions for his scholarship as the most influential author with the most total citations. His research interests include the pathophysiology and treatment of HF, cardiac device therapy, and cardiovascular biomarkers. The health status and prognosis of HF patients with anemia have been the focus of his research in recent years.41,42 Iron deficiency is a common trigger for the deterioration of anemia in HF patients, which needs to be tackled to reduce hospitalizations and improve quality of life, his team noted.43 In addition to conventional oral and intravenous iron therapy, his team found that in HF patients, empagliflozin rapidly increased hemoglobin and reduced the rate of new-onset anemia, leading to better prognosis.44 Furthermore, the collaboration network reveals that authors with more citations and publications have more tendency to collaborate. Stefan D Anker, Piotr Ponikowski and Dirk J van Veldhuisen are key nodes in the network, which may explain their higher total citations than other authors.
Major research institutions in terms of publications include Harvard University, University of Groningen, and University of California System. Most of these research institutions are universities, located in the United States, Germany, France, and Netherlands, which points to the key position of these regions. The publication time and volume of institutions by year indicated that most of highly productive institutions were also the first to engage in this field. While German Centre for Cardiovascular Research has not been involved in this area of until the last 5 years but has produced a conspicuous volume of publications.
The impact factor of the top 10 journals with the most publications is less impressive, with only 3 journals having an impact factor greater than 5, and all were Q1 journals, including European Journal of Heart Failure, Journal of Cardiac Failure, and Journal of the American College of Cardiology. European Journal of Heart Failure has the greatest number of publications, but surprisingly it is the least cited journal. This may be related to the late publication time of relevant articles. European Journal of Heart Failure and International Journal of Cardiology have the highest total link strength, highlighting their contributions to inter-institutional collaboration in this area. We are looking forward to more innovative and groundbreaking studies emerging in high-quality journals to promote research in this field.
We identified 14 major clusters based on the Log-likelihood ratio (LLR) and mutual information (MI) algorithm. Cluster #2 and Cluster #0 are key nodes in the development of the field of anemia in HF, which play a role as a bridge between earlier and more recent research. Each cluster has a different focus, and we classified these clusters into four categories based on characteristics.
The following clusters are dedicated to the pathophysiology, treatment, and prognosis of HF. Cluster #1 investigated the pathophysiology of iron deficiency in HF, as well as the causes, pathogenesis, and management of iron deficiency and anemia in HF patients.18,45 Cluster #6 explored the non-hematopoietic biological effects of erythropoietin, including anti-apoptotic and pro-angiogenic effects of potential benefits to HF.46–48 Cluster #7 focused on the involvement of Sodium-Glucose Co-Transporter 2 (SGLT2) in HF during energy metabolism regulation, hemodynamics, erythropoiesis, iron bioavailability and inflammatory set points.49 The clinical findings are inspiring, and empagliflozin, by simply inhibiting SGLT2 expressed in renal tubular epithelial cells, not only effectively controls blood glucose levels, but also improves the prognosis of HF.50,51 SGLT2 inhibitor, one of the hotspots in the field of HF, has recently been proven to increase hemoglobin levels,52 which reinforces its position in the treatment of anemia in HF. Cluster #8 was concerned about cardiorenal co-morbidities, in which kidney dysfunction took an important role in the pathogenesis and prognosis of HF.53,54 Cardiorenal syndrome (CRS) reflects the tangled relationship between simultaneous cardiac and renal damage. In CRS, loss of function in one organ contributes to reduced function in the other organ, which is attributed to mechanisms such as activation of neurohormonal networks, oxidative injury, and inflammatory cytokines.55 Comorbid anemia may occur in patients with CRS, and ultimately develop cardiorenal anemia syndrome (CRAS), which represents a vicious cycle where each of the 3 factors activates each other and results in tissue damage.55 A retrospective study from the Middle East suggests that 1 in 3 patients have CRS and 1 in 4 patients have CRAS among HF patients.56 Studies from developed countries such as Italy, Australia and Korea have showed similar prevalence of CRAS.57–59 While Tanzania’s HF patients had a notably higher prevalence of CRAS (44.4%).60 It appears that CRAS may be a more serious problem in developing countries. To date, data on optimal treatment strategies for CRAS are limited,55 and future research needs to pay more attention to multidisciplinary approaches in the management of CRAS.
The following clusters focus on drugs and clinical trials of anemia in HF. Cluster #0 evaluated the benefits and safety of using ferric carboxymaltose to rectify iron deficiency and anemia in patients with HF.61,62 Cluster #3 emphasized the benefits of rectifying iron deficiency in HF patients whether combined with anemia or not.63 Cluster #5 explored the effect of anemia on HF prognosis and the benefits of erythropoietin therapy on exercise capacity and quality of life, but its safety was in doubt.19,64,65 Cluster #12 reviewed the advantages and disadvantages of several common intravenous iron agents. Ferric carboxymaltose, as the third-generation intravenous iron agent, has overcame the limitations of previous intravenous iron agents, providing effective and rapid treatment of iron-deficiency anemia.66
The following clusters discussed the factors affecting the prognosis of HF. Cluster #2 assessed the impact of anemia on the prognosis of HF and suggested that anemia should be considered as a practical prognostic marker.26,67 Cluster #4 centered around anemia, HF, and chronic kidney disease.68,69 It highlighted the fact that these three interacted with each other in a vicious cycle known as cardiorenal anemia syndrome. Cluster #9 focused on red cell distribution width (RDW) and found that RDW levels were independently associated with morbidity, long-term prognosis, and mortality in HF.70–72 RDW is traditionally used for differential diagnosis of anemia, and it is expected to evaluate the prognosis of HF independently or in combination with hemoglobin.73,74
The following clusters were associated with comorbidities of HF. Cluster #10 established a correlation between HF and chronic obstructive pulmonary disease (COPD).75 It is not rare for patients to have these two conditions simultaneously and they can be confused by the common cardinal symptom of breathlessness. Cluster #11 suggested the need to focus on cardiovascular comorbidities in kidney transplant recipients, who are more vulnerable to HF, and graft survival is related to hemoglobin levels.76,77 Cluster #17 concerned about the prevalence, risk factors and clinical outcomes of hospital-acquired anaemia in patients with cardiovascular disease.78 The key to the management of hospital-acquired anemia is to avoid bleeding and blood wastage, eg avoiding unnecessary laboratory tests and the use of smaller blood collection tubes, which gives a clue to the management of anemia in HF.
By analyzing the keywords in the field of anemia in HF, it was found that the most common keywords were mortality, outcome, risk, and disease. Four distinct clusters were formed based on the above high-frequency keywords: “mortality, outcome, risk, and disease”; “prevalence, intravenous iron, ferric carboxymaltose, and iron deficiency”; “chronic kidney disease, erythropoietin, risk factors, and congestive heart failure”; “hemoglobin, morbidity, iron deficiency, and renal function”. These themes have boosted research related to anemia in HF.
Citation burst reveals trends and changes in subject by analyzing keywords with a sudden increase in frequency over a certain period. The red lines in Figure 6D indicate the duration of time the keyword lasted from the year it suddenly appeared. It is evident that ferric carboxymaltose, exercise capacity, and iron deficiency have shown a tendency to become research hotspots in the last 5 years. The proliferation of these keywords anticipates that therapeutic targets for anemia in HF are progressively concentrating on rectifying iron deficiency, with ferric carboxymaltose as the topical drug. While exercise capacity has received equal attention due to its close association with anemia. These are fast-growing hotspots for future research in the field with promising outlook.
By analyzing the timeline view of keywords and trend topics, dynamic tracking of hotspots and trends in different periods can be achieved. Researchers have made many advances in the field of anemia in HF, from the early focus on anemia in cardiorenal comorbidities and subcutaneous erythropoietin for anemia rectification, to the exploration of risk factors, morbidity, and prognosis, as well as in recent years to the concern with third-generation intravenous iron agents, including ferric carboxymaltose and iron isomaltoside.
In summary, it is reasonable to believe that research in this field will continue to focus on intravenous iron and iron deficiency in the foreseeable future. Meanwhile several flaws in the research of this field have been exposed. First, it should be noted that the current research hotspots are relatively homogeneous, and even the guidelines are mainly addressing iron deficiency rather than anemia.79 Certainly iron deficiency is a common cause of anemia. However, there are various factors that contribute to anemia, and in terms of common causes, these include malnutrition (iron, folic acid, and vitamin B12 deficiencies), renal dysfunction, inflammatory diseases, and unexplained anemia.67,80 Therefore, there is an urgent need to expand the spectrum of future research beyond iron deficiency. And fully exploring the mechanisms of anemia in HF may lead to new strategies for the treatment. Second, the optimal therapeutic target for anemia in HF is currently inconclusive. It has been found that in patients with HF, the mortality follows a J-shaped curve with hemoglobin levels, ie mortality increases when the level of hemoglobin is <13-14g/dL or >16-17g/dL.81,82 Moreover, repeated intravenous iron administration over time may lead to iron overload, which may aggravate heart damage.18 Thus, it is necessary to find an appropriate therapeutic target for the treatment of anemia and optimize the prognosis of HF. Third, compared to developed countries, fewer studies in this field have been conducted in developing countries, where anemia in HF is a more serious problem. This suggests that developing countries should pay more attention to this field in further research. Finally, plenty of studies have demonstrated a strong correlation between anemia and poorer outcomes in patients with HF. Due to the many potential confounding factors, however, in patients with HF, it is not completely certain whether anemia is an independent predictor of outcomes or simply a mirror of severity and comorbidities.83 For progress on these issues, future clinical trials are necessary to evaluate comprehensive approaches and therapeutic goals for treating anemia in HF and to further elucidate the role of anemia in HF.
Limitations
There are some hard-to-avoid limitations to our study. First, we did not analyze data from developing countries separately, meanwhile a large amount of data was from Europe and North America, which to some extent limited the reference value of our study for developing countries. For example, the large-scale use of intravenous iron recommended by the guidelines may not be practical in lower- and middle-income countries because of the cost.84 Second, we collected publications only from the WoSCC database and with a cutoff date of October 6, 2023, which may have led to incomplete inclusion and biased analysis of research trends. Third, we only included publications in English, and other languages were excluded. However, considering the small number of publications in other languages that we excluded compared to the publications we included, this has a modest impact on the results.
Conclusion
This is the first bibliometric study in the field of anemia in HF, and we comprehensively analyzed countries, authors, institutions, journals, co-cited references, and keywords from 2004 to 2023. The results illustrated that this field has received extensive attention from researchers over the past two decades. Moreover, the focus of the research varies in each period, suggesting that research in this field is constantly developing. There will be a need for more mechanistic studies and clinical trials to broaden the spectrum of research in the field of anemia in HF, to evaluate comprehensive approaches, and to find appropriate therapeutic targets. While investigating the independent predictive ability of anemia on HF prognosis is also one of the important future works. In brief, anemia is expected to receive increasing attention in HF, and our study can help researchers to quickly understand the knowledge structure, hotspots, and trends in this field.
Funding
This study is supported by National Key Research and Development Program of China (2022YFC3500101).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Paulus WJ, Tschöpe C, Sanderson JE, et al. How to diagnose diastolic heart failure: a consensus statement on the diagnosis of heart failure with normal left ventricular ejection fraction by the heart failure and echocardiography associations of the European society of cardiology. Eur Heart J. 2007;28(20):2539–2550. doi:10.1093/eurheartj/ehm037
2. Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American college of cardiology foundation/American heart association task force on practice guidelines. J Am Coll Cardiol. 2013;62(16):e147–e239. doi:10.1016/j.jacc.2013.05.019
3. Rossignol P, Hernandez AF, Solomon SD, Zannad F. Heart failure drug treatment. Lancet. 2019;393(10175):1034–1044. doi:10.1016/S0140-6736(18)31808-7
4. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the task force for the diagnosis and treatment of acute and chronic heart failure of the European society of cardiology (ESC) with the special contribution of the heart failure association (HFA) of the ESC. Eur Heart J. 2021;42(36):3599–3726. doi:10.1093/eurheartj/ehab368
5. James SL, Abate D, Abate KH, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990-2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2018;392(10159):1789–1858. doi:10.1016/S0140-6736(18)32279-7
6. van Riet EES, Hoes AW, Limburg A, Landman MAJ, van der Hoeven H, Rutten FH. Prevalence of unrecognized heart failure in older persons with shortness of breath on exertion. Eur J Heart Fail. 2014;16(7):772–777. doi:10.1002/ejhf.110
7. Calvert MJ, Freemantle N, Cleland JGF. The impact of chronic heart failure on health-related quality of life data acquired in the baseline phase of the CARE-HF study. Eur J Heart Fail. 2005;7(2):243–251. doi:10.1016/j.ejheart.2005.01.012
8. Ziaeian B, Fonarow GC. Epidemiology and aetiology of heart failure. Nat Rev Cardiol. 2016;13(6):368–378. doi:10.1038/nrcardio.2016.25
9. Lawson CA, Zaccardi F, Squire I, et al. 20-year trends in cause-specific heart failure outcomes by sex, socioeconomic status, and place of diagnosis: a population-based study. Lancet Public Health. 2019;4(8):e406–e420. doi:10.1016/S2468-2667(19)30108-2
10. Janaswamy P, Walters TE, Nazer B, Lee RJ. Current treatment strategies for heart failure: role of device therapy and LV reconstruction. Curr Treat Options Cardiovasc Med. 2016;18(9):57. doi:10.1007/s11936-016-0479-1
11. Tsao CW, Lyass A, Enserro D, et al. Temporal trends in the incidence of and mortality associated with heart failure with preserved and reduced ejection fraction. JACC Heart Fail. 2018;6(8):678–685. doi:10.1016/j.jchf.2018.03.006
12. Le CHH. The prevalence of anemia and moderate-severe anemia in the US population (NHANES 2003-2012). PLoS One. 2016;11(11):e0166635.
13. Stevens GA, Paciorek CJ, Flores-Urrutia MC, et al. National, regional, and global estimates of anaemia by severity in women and children for 2000-19: a pooled analysis of population-representative data. Lancet Glob Health. 2022;10(5):e627–e639. doi:10.1016/S2214-109X(22)00084-5
14. Culleton BF, Manns BJ, Zhang J, Tonelli M, Klarenbach S, Hemmelgarn BR. Impact of anemia on hospitalization and mortality in older adults. Blood. 2006;107(10):3841–3846. doi:10.1182/blood-2005-10-4308
15. Yusufu I, Cliffer IR, Yussuf MH, et al. Factors associated with anemia among school-going adolescents aged 10-17 years in Zanzibar, Tanzania: a cross sectional study. Bmc Public Health. 2023;23(1):1814. doi:10.1186/s12889-023-16611-w
16. McLean E, Cogswell M, Egli I, Wojdyla D, de Benoist B. Worldwide prevalence of anaemia, WHO vitamin and mineral nutrition information system, 1993–2005. Public Health Nutr. 2009;12(4):444–454. doi:10.1017/S1368980008002401
17. Bianchi VE, von Haehling S. The treatment of chronic anemia in heart failure: a global approach. Clin Res Cardiol. 2023. doi:10.1007/s00392-023-02275-4
18. Anand IS, Gupta P. Anemia and iron deficiency in heart failure. Circulation. 2018;138(1):80–98. doi:10.1161/CIRCULATIONAHA.118.030099
19. Ezekowitz JA, McAlister FA, Armstrong PW. Anemia is common in heart failure and is associated with poor outcomes. Circulation. 2003;107(2):223–225. doi:10.1161/01.CIR.0000052622.51963.FC
20. Makubi A, Hage C, Sartipy U, et al. Heart failure in Tanzania and Sweden: comparative characterization and prognosis in the Tanzania Heart Failure (TaHeF) study and the Swedish Heart Failure Registry (SwedeHF). Int J Cardiol. 2016;220:750–758. doi:10.1016/j.ijcard.2016.06.239
21. Hassanein M, Abdelhamid M, Ibrahim B, et al. Clinical characteristics and management of hospitalized and ambulatory patients with heart failure–results from ESC heart failure long-term registry–Egyptian cohort. Esc Heart Fail. 2015;2(3):159–167. doi:10.1002/ehf2.12046
22. Del Buono MG, Arena R, Borlaug BA, et al. Exercise Intolerance in patients with heart failure: JACC state-of-the-art review. J Am Coll Cardiol. 2019;73(17):2209–2225. doi:10.1016/j.jacc.2019.01.072
23. Cattadori G, Agostoni P, Corrà U, et al. Heart failure and anemia: effects on prognostic variables. Eur J Intern Med. 2017;37:56–63. doi:10.1016/j.ejim.2016.09.011
24. von Haehling S, Gremmler U, Krumm M, et al. Prevalence and clinical impact of iron deficiency and anaemia among outpatients with chronic heart failure: the PrEP Registry. Clin Res Cardiol. 2017;106(6):436–443. doi:10.1007/s00392-016-1073-y
25. Goh VJ, Tromp J, Teng TK, et al. Prevalence, clinical correlates, and outcomes of anaemia in multi-ethnic Asian patients with heart failure with reduced ejection fraction. Esc Heart Fail. 2018;5(4):570–578. doi:10.1002/ehf2.12279
26. Groenveld HF, Januzzi JL, Damman K, et al. Anemia and mortality in heart failure patients: a systematic review and meta-analysis. J Am Coll Cardiol. 2008;52(10):818–827. doi:10.1016/j.jacc.2008.04.061
27. Xia H, Shen H, Cha W, Lu Q. The prognostic significance of anemia in patients with heart failure: a meta-analysis of studies from the last decade. Front Cardiovasc Med. 2021;8:632318.
28. Miao Y, Quan W, Dong X, et al. A bibliometric analysis of ferroptosis, necroptosis, pyroptosis, and cuproptosis in cancer from 2012 to 2022. Cell Death Discov. 2023;9(1):129. doi:10.1038/s41420-023-01421-1
29. Donthu N, Kumar S, Mukherjee D, Pandey N, Lim WM. How to conduct a bibliometric analysis: an overview and guidelines. J Bus Res. 2021;133:285–296. doi:10.1016/j.jbusres.2021.04.070
30. Ying H, Zhang X, He T, et al. A bibliometric analysis of research on heart failure comorbid with depression from 2002 to 2021. Heliyon. 2023;9(2). doi:10.1016/j.heliyon.2023.e13054
31. Yang Z, Zhong Z, Zhao C, et al. Global trends and frontiers in research on exercise training for heart failure: a bibliometric analysis from 2002 to 2022. Front Cardiovasc Med. 2023;10. doi:10.3389/fcvm.2023.1181600
32. Hirsch JE. An index to quantify an individual’s scientific research output. Proc Natl Acad Sci. 2005;102(46):16569–16572. doi:10.1073/pnas.0507655102
33. Chen C. CiteSpace II: detecting and visualizing emerging trends and transient patterns in scientific literature. J Am Soc Inf Sci Technol. 2006;57(3):359–377. doi:10.1002/asi.20317
34. Chen C, Ibekwe-SanJuan F, Hou J. The structure and dynamics of cocitation clusters: a multiple-perspective cocitation analysis. J Am Soc Inf Sci Technol. 2010;61(7):1386–1409. doi:10.1002/asi.21309
35. Qin Y, Zhang Q, Liu Y. Analysis of knowledge bases and research focuses of cerebral ischemia-reperfusion from the perspective of mapping knowledge domain. Brain Res Bull. 2020;156:15–24. doi:10.1016/j.brainresbull.2019.12.004
36. Freeman LC. Centrality in social networks conceptual clarification. Soc Networks. 1978;1(3):215–239. doi:10.1016/0378-8733(78)90021-7
37. Brandes U. A faster algorithm for betweenness centrality*. J Math Sociol. 2001;25(2):163–177. doi:10.1080/0022250X.2001.9990249
38. Chen C. Science Mapping: a Systematic Review of the Literature. J Data Info Sci. 2017;2(2):1–40. doi:10.1515/jdis-2017-0006
39. Hunt SA. ACC/AHA 2005 guideline update for the diagnosis and management of chronic heart failure in the adult: a report of the American College of Cardiology/American Heart Association task force on practice guidelines (writing committee to update the 2001 guidelines for the evaluation and management of heart failure). J Am Coll Cardiol. 2005;46(6):e1–e82. doi:10.1016/j.jacc.2005.08.022
40. Maddox TM, Januzzi JL, Allen LA, et al. 2021 Update to the 2017 ACC expert consensus decision pathway for optimization of heart failure treatment: answers to 10 pivotal issues about heart failure with reduced ejection fraction: a report of the American College of Cardiology solution set oversight committee. J Am Coll Cardiol. 2021;77(6):772–810. doi:10.1016/j.jacc.2020.11.022
41. Siddiqi TJ, Anker SD, Filippatos G, et al. Health status across major subgroups of patients with heart failure and preserved ejection fraction. Eur J Heart Fail. 2023;25(9):1623–1631. doi:10.1002/ejhf.2831
42. Chioncel O, Benson L, Crespo-Leiro MG, et al. Comprehensive characterization of non-cardiac comorbidities in acute heart failure: an analysis of ESC-HFA EURObservational research programme heart failure long-term registry. Eur J Prev Cardiol. 2023;30(13):1346–1358. doi:10.1093/eurjpc/zwad151
43. Chopra VK, Anker SD. Anaemia, iron deficiency and heart failure in 2020: facts and numbers. Esc Heart Fail. 2020;7(5):2007–2011. doi:10.1002/ehf2.12797
44. Ferreira JP, Anker SD, Butler J, et al. Impact of anaemia and the effect of empagliflozin in heart failure with reduced ejection fraction: findings from EMPEROR-Reduced. Eur J Heart Fail. 2022;24(4):708–715. doi:10.1002/ejhf.2409
45. Alnuwaysir RIS, Hoes MF, van Veldhuisen DJ, van der Meer P, Grote Beverborg N. Iron deficiency in heart failure: mechanisms and pathophysiology. J Clin Med. 2022;11(1):125.
46. Arcasoy MO. The non-haematopoietic biological effects of erythropoietin. Brit J Haematol. 2008;141(1):14–31. doi:10.1111/j.1365-2141.2008.07014.x
47. van der Meer P, Lipsic E, Henning RH, et al. Erythropoietin induces neovascularization and improves cardiac function in rats with heart failure after myocardial infarction. J Am Coll Cardiol. 2005;46(1):125–133. doi:10.1016/j.jacc.2005.03.044
48. van der Meer P, Voors AA, Lipsic E, van Gilst WH, van Veldhuisen DJ. Erythropoietin in cardiovascular diseases. Eur Heart J. 2004;25(4):285–291. doi:10.1016/j.ehj.2003.11.017
49. Sano M. A role of sodium-glucose co-transporter 2 in cardiorenal anemia iron deficiency syndrome. Int J Mol Sci. 2023;24(6):5983.
50. Anker SD, Butler J, Filippatos G, et al. Empagliflozin in heart failure with a preserved ejection fraction. New Engl J Med. 2021;385(16):1451–1461. doi:10.1056/NEJMoa2107038
51. Packer M, Anker SD, Butler J, et al. Cardiovascular and renal outcomes with empagliflozin in heart failure. New Engl J Med. 2020;383(15):1413–1424. doi:10.1056/NEJMoa2022190
52. Docherty KF, Curtain JP, Anand IS, et al. Effect of dapagliflozin on anaemia in DAPA-HF. Eur J Heart Fail. 2021;23(4):617–628. doi:10.1002/ejhf.2132
53. Metra M, Felker GM, Zacà V, et al. Acute heart failure: multiple clinical profiles and mechanisms require tailored therapy. Int J Cardiol. 2010;144(2):175–179. doi:10.1016/j.ijcard.2010.04.003
54. Hillege HL, Nitsch D, Pfeffer MA, et al. Renal function as a predictor of outcome in a broad spectrum of patients with heart failure. Circulation. 2006;113(5):671–678. doi:10.1161/CIRCULATIONAHA.105.580506
55. McCullough PA. Anemia of cardiorenal syndrome. Kidney Int Suppl. 2021;11(1):35–45. doi:10.1016/j.kisu.2020.12.001
56. Manla Y, Kholoki O, Bader F, et al. The prevalence of cardiorenal anemia syndrome among patients with heart failure and its association with all-cause hospitalizations: a retrospective single-center study from the Middle East. Front Cardiovasc Med. 2023;10.
57. Scrutinio D, Passantino A, Santoro D, Catanzaro R. The cardiorenal anaemia syndrome in systolic heart failure: prevalence, clinical correlates, and long-term survival. Eur J Heart Fail. 2011;13(1):61–67. doi:10.1093/eurjhf/hfq167
58. Lu KJ, Kearney LG, Hare DL, et al. Cardiorenal anemia syndrome as a prognosticator for death in heart failure. Am J Cardiol. 2013;111(8):1187–1191. doi:10.1016/j.amjcard.2012.12.049
59. Kim CJ, Choi I, Park H, et al. Impact of cardiorenal anemia syndrome on short- and long-term clinical outcomes in patients hospitalized with heart failure. Cardiorenal Med. 2016;6(4):269–278. doi:10.1159/000443339
60. Pallangyo P, Fredrick F, Bhalia S, et al. Cardiorenal anemia syndrome and survival among heart failure patients in Tanzania: a prospective cohort study. Bmc Cardiovasc Disor. 2017;17(1):59. doi:10.1186/s12872-017-0497-2
61. Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129–2200. doi:10.1093/eurheartj/ehw128
62. Ponikowski P, van Veldhuisen DJ, Comin-Colet J, et al. Beneficial effects of long-term intravenous iron therapy with ferric carboxymaltose in patients with symptomatic heart failure and iron deficiency†. Eur Heart J. 2015;36(11):657–668. doi:10.1093/eurheartj/ehu385
63. Cappellini MD, Comin-Colet J, de Francisco A, et al. Iron deficiency across chronic inflammatory conditions: international expert opinion on definition, diagnosis, and management. Am J Hematol. 2017;92(10):1068–1078. doi:10.1002/ajh.24820
64. Tang Y, Katz SD. Anemia in chronic heart failure. Circulation. 2006;113(20):2454–2461. doi:10.1161/CIRCULATIONAHA.105.583666
65. Mancini DM, Katz SD, Lang CC, LaManca J, Hudaihed A, Androne A. Effect of erythropoietin on exercise capacity in patients with moderate to severe chronic heart failure. Circulation. 2003;107(2):294–299. doi:10.1161/01.CIR.0000044914.42696.6A
66. Qunibi WY. The efficacy and safety of current intravenous iron preparations for the management of iron-deficiency anaemia: a review. Arzneimittelforschung. 2010;60(06):399–412. doi:10.1055/s-0031-1296304
67. Anand IS. Anemia and chronic heart failure: implications and treatment options. J Am Coll Cardiol. 2008;52(7):501–511. doi:10.1016/j.jacc.2008.04.044
68. Silverberg DS, Wexler D, Iaina A, Steinbruch S, Wollman Y, Schwartz D. Anemia, chronic renal disease and congestive heart failure—the cardio renal anemia syndrome: the need for cooperation between cardiologists and nephrologists. Int Urol Nephrol. 2006;38(2):295–310. doi:10.1007/s11255-006-0064-8
69. Silverberg DS, Wexler D, Blum M, et al. The effect of correction of anaemia in diabetics and non‐diabetics with severe resistant congestive heart failure and chronic renal failure by subcutaneous erythropoietin and intravenous iron. Nephrol Dial Transpl. 2003;18(1):141–146. doi:10.1093/ndt/18.1.141
70. Tonelli M, Sacks F, Arnold M, Moye L, Davis B, Pfeffer M. Relation between red blood cell distribution width and cardiovascular event rate in people with coronary disease. Circulation. 2008;117(2):163–168. doi:10.1161/CIRCULATIONAHA.107.727545
71. Förhécz Z, Gombos T, Borgulya G, Pozsonyi Z, Prohászka Z, Jánoskuti L. Red cell distribution width in heart failure: prediction of clinical events and relationship with markers of ineffective erythropoiesis, inflammation, renal function, and nutritional state. Am Heart J. 2009;158(4):659–666. doi:10.1016/j.ahj.2009.07.024
72. Pascual-Figal DA, Bonaque JC, Redondo B, et al. Red blood cell distribution width predicts long-term outcome regardless of anaemia status in acute heart failure patients. Eur J Heart Fail. 2009;11(9):840–846. doi:10.1093/eurjhf/hfp109
73. Wołowiec A, Rogowicz D, Banach J, et al. Prognostic significance of red cell distribution width and other red cell parameters in patients with chronic heart failure during two years of follow-up. Kardiologia Polska. 2016;74(7):657–664. doi:10.5603/KP.a2016.0004
74. Rahamim E, Zwas DR, Keren A, et al. The ratio of hemoglobin to red cell distribution width: a strong predictor of clinical outcome in patients with heart failure. J Clin Med. 2022;11(3):886.
75. Vestbo J, Hurd SS, Agustí AG, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. Am J Resp Crit Care. 2013;187(4):347–365. doi:10.1164/rccm.201204-0596PP
76. Rigatto C, Parfrey P, Foley R, Negrijn C, Tribula C, Jeffery J. Congestive heart failure in renal transplant recipients: risk factors, outcomes, and relationship with ischemic heart disease. J Am Soc Nephrol. 2002;13(4):1084–1090.
77. Moore J, He X, Cockwell P, Little MA, Johnston A, Borrows R. The impact of hemoglobin levels on patient and graft survival in renal transplant recipients. Transplantation. 2008;86(4):564–570.
78. Salisbury AC, Kosiborod M. Hospital-acquired anemia in patients with cardiovascular disease: incidence, outcomes, and opportunities for prevention. Rcm. 2012;13(4):150–160.
79. McDonagh TA, Metra M, Adamo M, et al. 2023 Focused update of the 2021 ESC guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the task force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2023;44(37):3627–3639. doi:10.1093/eurheartj/ehad195
80. Guralnik JM, Eisenstaedt RS, Ferrucci L, Klein HG, Woodman RC. Prevalence of anemia in persons 65 years and older in the United States: evidence for a high rate of unexplained anemia. Blood. 2004;104(8):2263–2268. doi:10.1182/blood-2004-05-1812
81. Dunlay SM, Weston SA, Redfield MM, Killian JM, Roger VL. Anemia and heart failure: a community study. Am j Med. 2008;121(8):726–732. doi:10.1016/j.amjmed.2008.03.039
82. Go AS, Yang J, Ackerson LM, et al. Hemoglobin level, chronic kidney disease, and the risks of death and hospitalization in adults with chronic heart failure. Circulation. 2006;113(23):2713–2723. doi:10.1161/CIRCULATIONAHA.105.577577
83. Kosiborod M, Curtis JP, Wang Y, et al. Anemia and outcomes in patients with heart failure: a study from the national heart care project. Archives of Internal Medicine. 2005;165(19):2237–2244. doi:10.1001/archinte.165.19.2237
84. Makubi A, Roberts DJ. Investigation and treatment for iron deficiency in heart failure: the unmet need in lower and middle income countries. Brit J Haematol. 2017;177(6):896–904. doi:10.1111/bjh.14650
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Decrease in Hb and Hypoproteinemia: Possible Predictors of Complications in Neonates with Late-Onset Sepsis in a Developing Country
Cai N, Liao W, Chen Z, Tao M, Chen S
International Journal of General Medicine 2022, 15:6583-6589
Published Date: 13 August 2022
The Clinical and Biological Manifestations in Women with Iron Deficiency Without Anemia Compared to Iron Deficiency Anemia in a General Internal Medicine Setting: A Retrospective Cohort Study
Hirosawa T, Hayashi A, Harada Y, Shimizu T
International Journal of General Medicine 2022, 15:6765-6773
Published Date: 23 August 2022
Evaluation of Minimal Optimal Dose of Intravenous Ferric Carboxymaltose for Treatment of Iron Deficiency Anemia and Risk of Transient Hyperferritinemia
Alharbi AA, Alharbi AA, Bashen DS, Owaidah T
Journal of Blood Medicine 2022, 13:681-690
Published Date: 17 November 2022
Dapagliflozin Improves Erythropoiesis and Iron Metabolism in Type 2 Diabetic Patients with Renal Anemia
Osonoi T, Shirabe S, Saito M, Hosoya M, Watahiki N, Douguchi S, Ofuchi K, Katoh M
Diabetes, Metabolic Syndrome and Obesity 2023, 16:1799-1808
Published Date: 20 June 2023
Anemia and Associated Risk Factors in Pediatric Patients
Martinez-Torres V, Torres N, Davis JA, Corrales-Medina FF
Pediatric Health, Medicine and Therapeutics 2023, 14:267-280
Published Date: 4 September 2023