")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Dapagliflozin Improves Erythropoiesis and Iron Metabolism in Type 2 Diabetic Patients with Renal Anemia
Authors Osonoi T, Shirabe S, Saito M, Hosoya M, Watahiki N, Douguchi S, Ofuchi K, Katoh M
Received 20 March 2023
Accepted for publication 8 June 2023
Published 20 June 2023 Volume 2023:16 Pages 1799—1808
DOI https://doi.org/10.2147/DMSO.S411504
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Gian Paolo Fadini
Takeshi Osonoi, Shinichiro Shirabe, Miyoko Saito, Mitsuru Hosoya, Norie Watahiki, Satako Douguchi, Kensuke Ofuchi, Makoto Katoh
Naka Kinen Clinic, Naka-shi, Ibaraki, Japan
Correspondence: Makoto Katoh, Naka Kinen Clinic, 745-5 Nakadai, Naka-shi, Ibaraki, 311-0113, Japan, Tel +81 29 353 2800, Fax +81 29 295 5400, Email [email protected]
Purpose: In this study, we examined the effects of dapagliflozin on changes in hematopoiesis, iron metabolism, and body composition indices in elderly type 2 diabetic patients with renal impairment and investigated the potential of dapagliflozin to treat renal anemia.
Patients and Methods: The participants were elderly type 2 diabetics with renal impairment, and the indices of diabetes management, hematopoiesis, iron metabolism, and body composition were compared before and after dapagliflozin treatment.
Results: Fourteen subjects were given dapagliflozin 5 mg once daily for 12 weeks, three of whom had eligibility criteria deviations, such as serum ferritin < 50 ng/mL. For this purpose, 14 subjects were analyzed as full analysis set (FAS) and 11 as per-protocol set (PPS). FAS analysis revealed that dapagliflozin had no effect on hemoglobin A1c after 12 weeks but significantly decreased body mass index, significantly increased hemoglobin, hematocrit, and red blood cell count, significantly decreased log ferritin level only of iron metabolism index, and no important change in body water content. PPS analysis, on the other hand, revealed that dapagliflozin 12-week treatment showed a significant decrease in log hepcidin, serum iron, and transferrin saturation.
Conclusion: These findings suggest that a 12-week course of dapagliflozin causes an increase in hemoglobin levels due to its hematopoietic effects in elderly type 2 diabetics with renal impairment, but that these effects may be independent of body water loss and iron metabolism improvement.
Keywords: dapagliflozin, anemia, hemoglobin, iron metabolism, body composition
Introduction
Due to age-related decline in renal function, the proportion of chronic kidney disease (CKD) patients is increasing among the elderly.1 Anemia is an independent risk factor for the development and progression of both cardiovascular disease (CVD) and CKD in elderly patients with CKD and/or heart failure (HF).2 The triad of HF, CKD, and anemia is known as cardiorenal anemia syndrome, in which heart disease, kidney disease, and anemia interact in a vicious circle.3 The management of anemia in CKD consists of iron therapy and synthetic derivatives of recombinant erythropoietin.4 However, treating anemia with darbepoetin alfa increased hemoglobin levels but did not reduce the risk of CV outcomes in patients with HF.5
Sodium–glucose cotransporter 2 (SGLT2) inhibitors are known to have hemoglobin-increasing effects in patients with type 2 diabetes mellitus.6–9 Their effects are inconsistent with their HbA1c-lowering effect.6 In large clinical trials, SGLT2 inhibitors have proven cardiorenal protection in patients with diabetic nephropathy, CKD, and HF.7–10 In their post-hoc analyses, SGLT2 inhibitors were reported to increase the rate of anemia correction and reduce the risk of developing new anemia.11–13 These findings suggest that the hemoglobin-increasing effect of SGLT2 inhibitors may also be useful for anemia treatment. However, it is unknown whether SGLT2 inhibitors improve anemia in real-life clinical practice in type 2 diabetics with renal impairment. In addition, the mechanisms by which SGLT2 inhibitors increase hemoglobin levels are not fully established. There is growing evidence that SGLT2 inhibitors may stimulate erythropoiesis by temporarily increasing erythropoietin and enhancing iron metabolism by suppressing hepcidin, whereas initially it was assumed that it merely reflected hemoconcentration brought on by diuresis.14–16
Therefore, the present study aimed to investigate the effect of dapagliflozin 5 mg once daily for 12 weeks on changes in hematopoietic indices (red blood cell count, hemoglobin, hematocrit, reticulocyte count, erythropoietin), iron metabolism indices (serum ferritin, serum iron, transferrin saturation [TSAT], hepcidin), and body composition (body water content) in elderly type 2 diabetics with renal impairment.
Materials and Methods
Study Design
This open-label, single-arm, single-center, prospective observational study was conducted at Naka Kinen Clinic (Ibaraki, Japan). Before the study, the Naka Kinen Clinic Clinical Research Ethics Review Committee reviewed and approved the study protocol on both a scientific and ethical level. The registration number for this study in the University Hospital Medical Information Network is UMIN000043519. All participants provided written informed consent before participation. This study was conducted in accordance with ethical principles based on the Declaration of Helsinki and in compliance with ethical guidelines for human subjects’ medical research.
Study Subjects
Participants in the study who met the following criteria had insufficient glycemic control with diet and exercise and/or treatment with hypoglycemic drugs other than SGLT2 inhibitors: (1) age of 60 years or older; (2) had a baseline hemoglobin A1c (HbA1c) between 6.5% and 10%; (3) had estimated glomerular filtration rate (eGFR) between 30 and 60 mL/min/1.73 m2; (4) renal anemia defined as having CKD and hemoglobin < 12.0 g/dL without iron deficiency defined as serum ferritin levels > 50 ng/mL;15,17 (5) had not changed the dosage of their diabetes medication, erythropoiesis-stimulating agent (ESA), or iron from at least 8 weeks before the day of consent. Patients who met at least one of the following criteria were excluded from the study: (1) had type 1 diabetes mellitus; (2) suffered from severe ketosis, diabetic coma or pre-coma, severe infection, perioperative complication, or severe trauma; (3) had a severe renal dysfunction (eGFR < 30 mL/min/1.73 m²); (4) had a history of any of the following diseases within the last 12 weeks before the day of consent: acute coronary syndrome, cerebrovascular disease, myocarditis, constrictive pericarditis, or severe valvular disease are all examples of such conditions; (5) had a cardiac function classification of IV according to the New York Heart Association (NYHA); (6) had a body mass index (BMI) <18.5 kg/m2; (7) were pregnant, lactating, or may be pregnant; or (8) diagnosed with cancer or suspected of having cancer; (9) were judged by the investigator to be inappropriate for this study.
Outcome Measures
The primary efficacy endpoints of this study were changes in hematopoietic indices (red blood cell count, hemoglobin, hematocrit, reticulocyte count, erythropoietin), and iron metabolism indices (serum ferritin, serum iron, TSAT, and hepcidin) from baseline to week 12. The secondary endpoints were changes in body composition measured by bioimpedance spectroscopy from baseline to week 12 in body fat mass, visceral fat mass, subcutaneous fat mass, lean body mass, muscle mass, body water content, intracellular water content, extracellular water content, protein mass, and mineral mass (X-SCAN PLUS, Owa Medical Co., Fukuoka, Japan). The routine clinical biochemistry tests and vital signs, and safety were measured at baseline and weeks 4, 8, and 12. TSAT was computed using the following formula: TSAT (%) equals serum iron/total iron binding capacity multiplied by 100. The urinary albumin-to-creatinine ratio (UACR) in spot urine samples was calculated from urinary albumin and creatinine levels, and the eGFR was calculated using age, body weight, gender, and serum creatinine. Hepcidin was measured at serum hepcidin-25 (the bioactive form) level by a liquid chromatography-tandem–mass spectrometry (LC-MS/MS) method (LSI Medience Co., Tokyo, Japan).18
Statistical Analysis
Two analysis groups were set for the efficacy of this study: full analysis set (FAS) and per-protocol set (PPS), with FAS being the primary analysis. The FAS population consisted of all eligible patients who received the study drug and had hemoglobin readings at baseline and at least one time point during the observation period. The PPS was the population from the FAS that did not deviate from the study protocol.
Data in all tables and figures are presented as the mean ± standard deviation (SD). Because hepcidin and ferritin data were not normally distributed; they were logarithmically transformed (log). A paired t-test was used to compare the mean value at baseline and after 12 weeks of treatment. A two-sided P value < 0.05 was considered statistically significant. Pearson’s correlation coefficient tests were used to determine the relationship between numerical variables. Statistical analyses were performed using Prism ver. 8.4.3 software (GraphPad Software, Inc., San Diego, USA).
Results
Patients Disposition and Baseline Characteristics
This study was conducted from March 4, 2021, to March 31, 2022. A total of 14 subjects were treated with dapagliflozin 5 mg once daily for 12 weeks (FAS). The PPS included 11 subjects, and three were excluded due to deviations in inclusion criteria, such as serum ferritin levels < 50 ng/mL. The baseline characteristics of the participants under FAS analysis were summarized in Table 1. There were 6 men (42.9%) and 8 women (57.1%), with a mean age of 74.9 years, BMI of 23.4 kg/m2, HbA1c of 7.3%, hemoglobin of 11.6 g/dL, eGFR of 40.6 mL/min/1.73 m2, UACR of 334.5 mg/gCr, systolic blood pressure of 137.2 mmHg, and total cholesterol of 176.6 mg/dL. At the outset, the most commonly prescribed antidiabetic drug was α-glucosidase inhibitor (9 subjects), followed by metformin (7), insulin (7), dipeptidyl peptidase-4 inhibitor (6), glucagon-like peptide-1 agonist (6), and glinide (2). Oral iron was prescribed in 2 subjects, and no ESA was prescribed. Of the 13 hypertensive subjects, 11 were treated with an angiotensin II receptor blocker. Of the 11 dyslipidemia patients, 5 were treated with a statin.
 |
Table 1 Baseline Characteristics of All Treated Patients |
Changes in Hemoglobin Level at Each Time Point and the Other Hematopoiesis Indices Levels
The changes in hemoglobin level from baseline to weeks 4, 8, and 12 are shown in Figure 1. FAS and PPS baseline hemoglobin levels were 11.6 ± 0.6 and 11.6 ± 0.7, respectively. In both FAS and PPS, 4 weeks of dapagliflozin treatment had no significant effect on mean hemoglobin levels compared with baseline. Mean hemoglobin levels in FAS increased significantly at weeks 8 and 12, and in PPS at week 12. At week 12, all subjects had increased hemoglobin levels over baseline. The increase in hemoglobin levels following dapagliflozin administration did not differ between FAS and PPS.
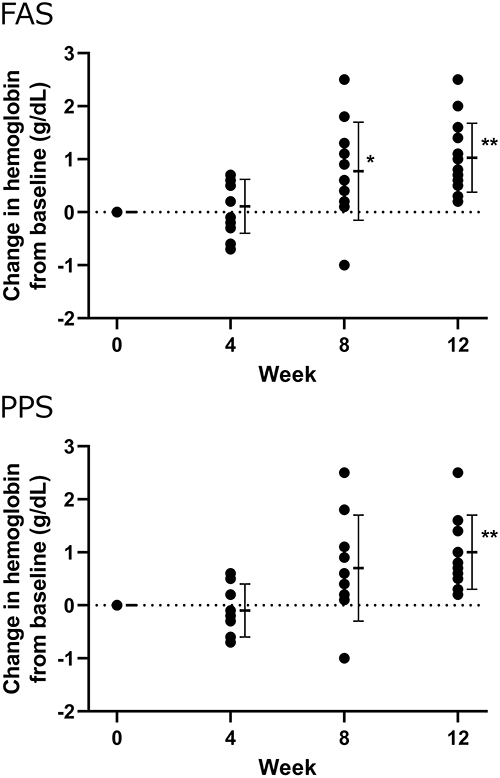 |
Figure 1 The changes in hemoglobin levels from baseline at 4, 8, and 12 weeks after the start of dapagliflozin treatment in the full analysis set (FAS) (upper panel) and per-protocol set (PPS) (lower panel). *P < 0.05, **P < 0.01 vs 0 weeks by paired t-test. |
The changes in hematocrit, red blood cell count, reticulocyte count, and serum erythropoietin level from baseline to week 12 are shown in Figure 2. Hematocrit and red blood cell count increased significantly in both FAS and PPS 12 weeks after the start of dapagliflozin treatment; however, reticulocyte count and serum erythropoietin levels did not change in either group.
 |
Figure 2 The changes in hematocrit, red blood cell count, reticulocyte count, and serum erythropoietin level between baseline and 12 weeks after the start of dapagliflozin treatment in the full analysis set (FAS) (upper panel) and per-protocol set (PPS) (lower panel). **P < 0.01 vs 0 weeks by paired t-test. |
Changes in Iron Metabolism Indices Levels
The changes in log hepcidin, log ferritin, TSAT, and serum iron level from baseline to week 12 are shown in Figure 3. In FAS, log ferritin decreased significantly 12 weeks after the start of dapagliflozin treatment; however, the other iron metabolism indices did not change. In PPS, log hepcidin, log ferritin, TSAT, and serum iron level showed a significant reduction after treatment with dapagliflozin.
 |
Figure 3 The changes in log hepcidin, log ferritin, TSAT, and serum iron level between baseline and 12 weeks after the start of dapagliflozin treatment in the full analysis set (FAS) (upper panel) and per-protocol set (PPS) (lower panel). *P < 0.05, **P < 0.01 vs 0 weeks by paired t-test. TSAT, transferrin saturation. |
Correlation analysis was used to investigate the relationship between the change in log hepcidin and the change in log ferritin, iron, TSAT, or hemoglobin at week 12. There was a significant correlation between each parameter value of log hepcidin change and log ferritin change (correlation coefficient r = 0.78, P < 0.01), iron (r = 0.53, P < 0.05), TSAT (r = 0.64, P < 0.05), but not hemoglobin change (r = 0.08) (Figure 4).
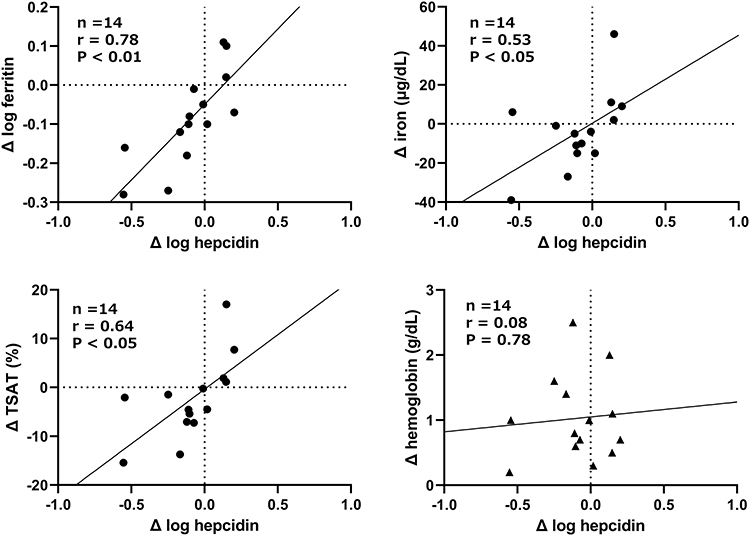 |
Figure 4 Relationship between the change in log hepcidin and the change in log ferritin, iron, transferrin saturation (TSAT), or hemoglobin at week 12. r, correlation coefficient. |
Changes in Body Composition Indices Levels
Body weight decreased significantly from baseline after 12 weeks of dapagliflozin treatment in both FAS and PPS (Table 2). In FAS, a significant decrease in mineral mass was also observed, but its rate was low. Body fat mass, lean body mass, body water content, intracellular water, and extracellular water levels in FAS and PPS did not change significantly from baseline after 12 weeks of dapagliflozin treatment (Table 2). There was no significant relationship between the change in hemoglobin and the change in mineral mass (r = −0.03) or body water content (r = 0.23) (Figure 5).
 |
Table 2 Changes in Body Composition Indices Levels |
 |
Figure 5 Relationship between the change in hemoglobin and the change in body water content and mineral mass at week 12. r, correlation coefficient. |
Changes in HbA1c, BMI, and eGFR Levels
HbA1c levels were not importantly decreased after 12 weeks of dapagliflozin treatment compared to baseline in both FAS and PPS (Figure 6). BMI and eGFR levels decreased significantly from baseline after 12 weeks of dapagliflozin treatment in both FAS and PPS (Figure 6).
 |
Figure 6 In the full analysis set (FAS) (upper panel) and per-protocol set (PPS), the changes in HbA1c, BMI, and eGFR levels between baseline and 12 weeks after the start of dapagliflozin treatment are shown (lower panel). **P < 0.01 vs 0 weeks by paired t-test. Abbreviations: HbA1c, hemoglobin A1c; BMI, body mass index; eGFR, estimated glomerular filtration rate. |
Discussion
Even the low dose of dapagliflozin (5 mg) used in this study was found to increase red blood cell count, hemoglobin, and hematocrit levels in elderly type 2 diabetics with renal impairment. Furthermore, increased hemoglobin levels occurred without diuretic volume depletion or improvement in iron metabolism. These findings suggest that dapagliflozin has an erythropoietic effect and can help improve anemia in people with CKD.
The FAS included three subjects in this study with serum ferritin levels < 20 ng/mL (two of whom received oral iron), while the PPS excluded them from the analysis. The PPS, but not the FAS, showed that the treatment of dapagliflozin was associated with improved iron metabolism in type 2 diabetics with renal anemia. After 12 weeks of dapagliflozin treatment, type 2 diabetics with normal serum ferritin and hemoglobin levels showed an increase in hemoglobin and a decrease in hepcidin.16 Based on these findings, SGLT2 inhibitors may improve iron metabolism differently in patients with and without iron deficiency. However, in a subanalysis of the DAPA-HF trial (Dapagliflozin and Prevention of Adverse-Outcomes in Heart Failure), dapagliflozin was associated with increased hemoglobin and decreased hepcidin compared with placebo, regardless of the presence of iron deficiency.19 More research is needed to determine the effects of SGLT2 inhibitors on iron metabolism in patients with low serum ferritin levels (50 ng/mL or less).
Hepcidin is known to be a key regulator of iron metabolism.20 Dapagliflozin decreased log hepcidin in this study, and there was a significant correlation between the change in log hepcidin and the change in log ferritin, iron, and TSAT. However, after 12 weeks of dapagliflozin treatment, changes in log hepcidin did not correlate with changes in hemoglobin. The reasons for this observation are unknown; however, it has been proposed that there is a mechanism by which an increase in hemoglobin with SGLT2 inhibitors is not associated with an improvement in iron metabolism.
Several previous clinical trials6–9 have shown that using SGLT2 inhibitors increases hemoglobin levels over time regardless of renal impairment. This was thought simply to reflect volume contraction due to diuresis.14 Recently, it was reported that treatment with dapagliflozin has resulted in clinically meaningful increase in hemoglobin due to a diuretic effect (early phase; within 4 weeks) and increased erythropoiesis (late phase; beyond 4 weeks).21 In this study, after 12 weeks of dapagliflozin treatment, there was no change in body water content and no correlation between the change in hemoglobin and change in body water content. In addition, dapagliflozin induces a long-term and dose-dependent elevation in hematocrit that is preserved in patients receiving concomitant insulin treatment, including chronic insulin therapy.22 Insulin is known to have a sustained antinatriuretic effect with concomitant increase in extracellular fluid volume.23,24 Thus, the increase in hemoglobin caused by dapagliflozin cannot be explained by diuretic volume contraction.
The increase in hemoglobin caused by SGLT2 inhibitors is suggested to be due to hematopoiesis; however, the details of the mechanism could not be elucidated. After 4 weeks of treatment, SGLT2 inhibitors temporarily increased serum erythropoietin levels.14,15,25 In contrast, no increase in serum erythropoietin levels was observed after 12 weeks of dapagliflozin treatment in this study. Thus, the increase in erythropoietin levels caused by SGLT2 inhibitors does not explain the persistent increase in hematocrit. It has been reported that the hypoxia–inducible factor prolyl hydroxylase inhibitor roxadustat increases erythropoietin levels within the physiological range, with a peak at 4 hours after administration and returns to baseline levels within 24–48 hours.26 Therefore, to confirm the effect of SGLT2 inhibitors on erythropoietin, it is necessary to consider diurnal variation.
To prevent the progression of anemia in patients with CKD, renal function must be maintained or improved. Treatment with SGLT2 inhibitors induces an initial decline in GFR. This decline is reaching a nadir within 1–2 weeks and slowly returns toward pretreatment values over the next 3–9 months.27 Dapagliflozin 5 mg for 12 weeks significantly reduced eGFR in elderly type 2 diabetics with renal impairment in this study. In addition, dapagliflozin did not decrease the HbA1c level. Because a decrease in GFR decreases the amount of glucose delivered into the proximal tubules, the HbA1c-lowering efficacy of SGLT2 inhibitors decreases roughly in line with a decrease in GFR.6 As a result, the improvement of erythropoiesis by dapagliflozin was independent of its effects on GFR or HbA1c levels.
The small sample size, short duration, and lack of a comparator group limit the study’s ability to draw definitive conclusions. However, several studies have already reported on the erythropoiesis-stimulating effects of SGLT2 inhibitors.14–16 Furthermore, the consistency of dapagliflozin’s effect on hematocrit, hemoglobin, and red blood cell count, as well as the extensive replication of similar findings with other SGLT2 inhibitors in multiple populations, lends robustness to our findings.
Conclusion
In conclusion, even the low dose of dapagliflozin (5 mg) used in the present study improved erythropoiesis, including an increase in red blood cell count, hemoglobin, and hematocrit levels. Furthermore, in patients with high baseline ferritin levels (>50 ng/mL), the use of dapagliflozin was observed to have hematopoietic effects, including improved iron metabolism. These patients are presumed to have renal anemia due to CKD, not iron deficiency anemia. However, serum hepcidin and body water content were not associated with an increase in hemoglobin, implying that dapagliflozin use is associated with an increase in hemoglobin levels regardless of iron status or volume contraction. According to these findings, dapagliflozin improves erythropoiesis and iron metabolism in elderly type 2 diabetics with renal anemia.
Data Sharing Statement
M. Katoh, the corresponding author, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgment
We would like to thank Katsuhiro Kawauchi and Akiko Haginoya for their technical assistance and all the physicians and staff members of the Naka Kinen Clinic.
Author Contributions
T. Osonoi and M. Katoh are involved in the planning of the study. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by a grant for a pathophysiological research conference in chronic kidney disease, in Japan [grant number JKFB20-9].
Disclosure
T. Osonoi received research funding from Novo Nordisk Pharma Ltd., Takeda Pharmaceutical Co., Ltd., Ono Pharmaceutical Co., Ltd., Otsuka Pharmaceutical Co., Ltd., Eli Lilly Japan K.K., Bayer Yakuhin, Ltd., Kowa Pharmaceutical Co., Ltd., Fuji Yakuhin Co., Ltd., Mochida Pharmaceutical Co. Ltd., Sumitomo Pharma Co. Ltd., and Gilead Sciences, and honoraria for lectures from Novo Nordisk Pharma Co., Ltd., and Sumitomo Pharma Co. Ltd. The other authors have no conflicts of interest to declare for this work.
References
1. Coresh J, Astor BC, Greene T, et al. Prevalence of chronic kidney disease and decreased kidney function in the adult US population. Third national health and nutrition examination survey. Am J Kidney Dis. 2003;41:1–12. doi:10.1053/ajkd.2003.50007
2. Fishbane S, Spinowitz B. Update on anemia in ESRD and earlier stages of CKD: core curriculum 2018. Am J Kidney Dis. 2018;71:423–435. doi:10.1053/j.ajkd.2017.09.026
3. Silverberg DS, Wexler D, Blum M, et al. The cardio renal anemia syndrome: correcting anemia in patients with resistant congestive heart failure can improve both cardiac and renal function and reduce hospitalizations. Clin Nephrol. 2003;60(1):S93–102.
4. Mehdi U, Toto RD. Anemia, diabetes, and chronic kidney disease. Diabetes Care. 2009;32:1320–1326. doi:10.2337/dc08-0779
5. Swedberg K, Young JB, Anand IS, et al. Treatment of anemia with darbepoetin alfa in systolic heart failure. N Engl J Med. 2013;368:1210–1219. doi:10.1056/NEJMoa1214865
6. Wanner C, Lachin JM, Inzucchi SE, et al. EMPA-REG OUTCOME Investigators. Empagliflozin and clinical outcomes in patients with type 2 diabetes mellitus, established cardiovascular disease, and chronic kidney disease. Circulation. 2018;137:119–129. doi:10.1161/CIRCULATIONAHA.117.028268
7. Perkovic V, Jardine MJ, Neal B, et al. CREDENCE Trial Investigators. Canagliflozin and renal outcomes in type 2 diabetes and nephropathy. N Engl J Med. 2019;380:2295–2306. doi:10.1056/NEJMoa1811744
8. McMurray JJV, Solomon SD, Inzucchi SE, et al. DAPA-HF trial committees and investigators. Dapagliflozin in patients with heart failure and reduced ejection fraction. N Engl J Med. 2019;381:1995–2008. doi:10.1056/NEJMoa1911303
9. Packer M, Anker SD, Butler J, et al. EMPEROR-reduced trial investigators. Cardiovascular and renal outcomes with empagliflozin in heart failure. N Engl J Med. 2020;383:1413–1424. doi:10.1056/NEJMoa2022190
10. Heerspink HJL, Stefánsson BV, Correa-Rotter R, et al. DAPA-CKD trial committees and investigators. Dapagliflozin in patients with chronic kidney disease. N Engl J Med. 2020;383:1436–1446. doi:10.1056/NEJMoa2024816
11. Oshima M, Neuen BL, Jardine MJ, et al. Effects of canagliflozin on anaemia in patients with type 2 diabetes and chronic kidney disease: a post-hoc analysis from the CREDENCE trial. Lancet Diabetes Endocrinol. 2020;8:903–914. doi:10.1016/S2213-8587(20)30300-4
12. Docherty KF, Curtain JP, Anand IS, et al. DAPA-HF investigators and committees. Effect of dapagliflozin on anaemia in DAPA-HF. Eur J Heart Fail. 2021;23:617–628. doi:10.1002/ejhf.2132
13. Ferreira JP, Anker SD, Butler J, et al. Impact of anaemia and the effect of empagliflozin in heart failure with reduced ejection fraction: findings from EMPEROR-Reduced. Eur J Heart Fail. 2022;24:708–715. doi:10.1002/ejhf.2409
14. Lambers Heerspink HJ, de Zeeuw D, Wie L, et al. Dapagliflozin a glucose-regulating drug with diuretic properties in subjects with type 2 diabetes. Diabetes Obes Metab. 2013;15:853–862. doi:10.1111/dom.12127
15. Maruyama T, Takashima H, Oguma H, et al. Canagliflozin improves erythropoiesis in diabetes patients with Anemia of chronic kidney disease. Diabetes Technol Ther. 2019;21:713–720. doi:10.1089/dia.2019.0212
16. Ghanim H, Abuaysheh S, Hejna J, et al. Dapagliflozin suppresses hepcidin and increases erythropoiesis. J Clin Endocrinol Metab. 2020;105(4):
17. KDOQI; National Kidney Foundation. KDOQI clinical practice guidelines and clinical practice recommendations for anemia in chronic kidney disease. Am J Kidney Dis. 2006;47(5 Suppl 3):S11–145. doi:10.1053/j.ajkd.2006.03.010
18. Kaneko Y, Miyajima H, Piperno A, et al. Measurement of serum hepcidin-25 levels as a potential test for diagnosing hemochromatosis and related disorders. J Gastroenterol. 2010;45:1163–1171. doi:10.1007/s00535-010-0259-8
19. Docherty KF, Welsh P, Verma S, et al. Iron deficiency in heart failure and effect of dapagliflozin: findings from DAPA-HF. Circulation. 2022;146:980–994. doi:10.1161/CIRCULATIONAHA.122.060511
20. Pagani A, Nai A, Silvestri L, Camaschella C. Hepcidin and Anemia: a tight relationship. Front Physiol. 2019;10:1294. doi:10.3389/fphys.2019.01294
21. Stefánsson BV, Heerspink HJL, Wheeler DC, et al. Correction of anemia by dapagliflozin in patients with type 2 diabetes. J Diabetes Complications. 2020;34(12):107729. doi:10.1016/j.jdiacomp.2020.107729
22. Aberle J, Menzen M, Schmid SM, et al. Dapagliflozin effects on haematocrit, red blood cell count and reticulocytes in insulin-treated patients with type 2 diabetes. Sci Rep. 2020;10(1):22396. doi:10.1038/s41598-020-78734-z
23. Brands MW. Role of insulin-mediated antinatriuresis in sodium homeostasis and hypertension. Hypertension. 2018;72:1255–1262. doi:10.1161/HYPERTENSIONAHA.118.11728
24. DeFronzo RA. The effect of insulin on renal sodium metabolism. A review with clinical implications. Diabetologia. 1981;21:165–171. doi:10.1007/BF00252649
25. Ferrannini E, Baldi S, Frascerra S, et al. Renal handling of ketones in response to sodium-glucose cotransporter 2 inhibition in patients with type 2 diabetes. Diabetes Care. 2017;40:771–776. doi:10.2337/dc16-2724
26. Besarab A, Provenzano R, Hertel J, et al. Randomized placebo-controlled dose-ranging and pharmacodynamics study of roxadustat (FG-4592) to treat anemia in nondialysis-dependent chronic kidney disease (NDD-CKD) patients. Nephrol Dial Transplant. 2015;30:1665–1673. doi:10.1093/ndt/gfv302
27. Bailey CJ, Day C, Bellary S. Renal protection with SGLT2 inhibitors: effects in acute and chronic kidney disease. Curr Diab Rep. 2022;22:39–52. doi:10.1007/s11892-021-01442-z
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.