Back to Journals » International Journal of General Medicine » Volume 16
Ophthalmic Manifestations Among Patients Surviving COVID-19
Authors Loduca Lima V, Soares LCM, Pereira LA, Nascimento PA, Cirillo LRN, Sakuma HT, da Veiga GL ![]() , Abucham-Neto JZ, Fonseca FLA
, Abucham-Neto JZ, Fonseca FLA
Received 7 December 2022
Accepted for publication 20 March 2023
Published 9 May 2023 Volume 2023:16 Pages 1747—1755
DOI https://doi.org/10.2147/IJGM.S399806
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Vagner Loduca Lima,1 Larissa Caroline Mansano Soares,1 Leonardo Amarante Pereira,1 Priscila Alves Nascimento,1 Luciano Rabello Netto Cirillo,1 Hebert Toshiaki Sakuma,1 Glaucia Luciano da Veiga,1,2 Julio Zaki Abucham-Neto,1 Fernando Luiz Affonso Fonseca1– 3
1Departamento de Oftalmologia, Faculdade de Medicina do ABC, Santo André, Brazil; 2Laboratório de Análises Clínicas, Faculdade de Medicina do ABC, Santo André, Brasil; 3Departamento de Ciências Farmacêuticas da Universidade Federal de São Paulo/UNIFESP, Diadema, Brasil
Correspondence: Glaucia Luciano da Veiga, Departamento de Oftalmologia, Faculdade de Medicina ABC, 2000 Lauro Gomes Avenue, Santo André, SP, 09069-870, Brazil, Tel +55 11 4993-5488, Email [email protected]
Background and Aim: To identify ocular findings related to SARS-CoV-2 infection in patients after the resolution of COVID-19 using complete ocular examinations and optical coherence tomography (OCT).
Methods: In this cross-sectional study, conducted from May 30 to October 30, 2020, patients who recovered from various stages COVID-19 underwent eye examination and multimodal retinal imaging (Retinographies and Spectral-OCT).
Results: We included 50 patients, 29 (58%) males, median age of 46.5 [standard deviation 15.8]. Of these, 42% (21) had mild, 18% (9) had severe and 40% (20) had critical disease. The median time interquartile range (IQR) between symptom onset and ocular examination was 55 days [IQR 39– 71]. Seven patients (14%) reported ophthalmic symptoms, transitory low visual acuity (6%) and retroocular pain (8%). On OCT, one patient without comorbidities had sectoral retinal pallor suggestive of acute retinal ischaemia and oedema of the retina’s inner layers and atrophy. All findings progressively and spontaneously improved months after resolution of COVID-19.
Conclusion: Patients with COVID-19 present findings compatible with the general population depending on age and comorbidities; nevertheless, acute retinal findings associated with the disease may be present, such as caused either by the direct effects of retinal SARS-CoV-2 infection, by indirect effects of the cytokine storm or by the pro-thrombotic state associated with COVID-19. Therefore, retinal involvement in patients with COVID-19 remains subject to considerable discussion and study.
Keywords: COVID-19, retina, ophthalmology, Sars-Cov-2, eye manifestations
Introduction
The year 2020 and 2021 was marked by the coronavirus disease 2019 (COVID-19) pandemic, with over 185 million confirmed cases and more than 4.0 million deaths reported to the World Health Organization by July 2021.1 The disease is caused by the severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), first identified in January 2020 as a new human-infecting coronavirus from an outbreak of unexplained pneumonia cases in Wuhan, Hubei Province, China, in late December 2019.1,2 COVID-19 patients usually present with fever and respiratory tract symptoms. However, COVID-19 can affect other organ systems, including cardiovascular, neurological, gustatory, gastrointestinal, hepatic, renal, olfactory, haematological, cutaneous, and ocular systems.1–3,4,5
The ocular manifestations of SARS-CoV-2 infection are not entirely understood; most studies reported ocular surface disorders.5–7 However, there has been a growing interest in possible retinal findings in patients with COVID-19, according to the hypothesis generated by Marinho et al.8 The direct activity/immunogenicity of SARS-CoV-2 or the pro-thrombotic status reported in critically COVID-19 patients is thought to mediate these patients’ retinal damage.9 Several lines of evidence suggest that a subgroup of patients with severe COVID-19 might suffer from cytokine storm syndrome. Coagulation disorders are common in patients with SARS-CoV-2 infection, especially in those with severe disease.10 The retina’s arteries and veins represent a window on the vascular system as they are exposed to the same pathological processes and show changes in many systemic diseases.11 To date, cotton wool spots and retinal haemorrhages have been reported in dilated eye examination of patients with COVID-19.8,9,12 An autopsy study identified viral RNA of SARS-CoV-2 in retinas of deceased COVID-19 patients,13 and there was a correlation identified between retinal veins diameter and disease severity.14 Nevertheless, the relationship between SARS-CoV-2 infection and retinal disease remains a matter of debate.15
To help resolve this question, we performed comprehensive ophthalmologic evaluations, including multimodal retinal imaging in patients who had recovered from all severities of COVID-19 to identify ocular findings that may be related to SARS-CoV-2 infection.
Materials and Methods
Design
A single-centre cross-sectional study was carried out from May 30, 2020, to October 30, 2020, at the Ophthalmology Outpatient Clinic of the Centro Universitário FMABC, Santo André, São Paulo Metropolitan Area, Brazil. The study was approved by the Institutional Research Ethics Committee of the Centro Universitário FMABC under protocol 4.067.204. It was carried out following the relevant guidelines and regulations and ethical principles of the Declaration of Helsinki. Written informed consent was obtained from all patients, consistent with Brazilian’s National Research Ethics Committee resolution for research conducted during the COVID-19 pandemic.
Participants
We included patients with a confirmed diagnosis of COVID-19 by RT-PCR test. These patients were under Delta or Gamma infection in Brazil.16,17 According to the Brazilian Epidemiological Monitoring Guidelines for the Public Health Emergency of COVID-19 published by the Brazilian Ministry of Health on April 3, 2020,16, they were out of the isolation period. Patients were recruited for this study from two sources: those hospitalised in the local referral centre for the treatment of COVID-19 patients after hospital discharge (Mário Covas State Hospital, Santo André, São Paulo Metropolitan Area, Brazil) and health-care workers from the Centro Universitário (FMABC, Santo André, São Paulo Metropolitan Area, Brazil). Patients were classified into mild, severe or critical disease categories according to the World Health Organization’s (WHO) guideline agreement for clinical management of COVID-19, published May 27, 2020.1 Exclusion criteria: use of any eye drop other than artificial tears, eye surgery in the last year, and terminal cancer.
Patients underwent an ophthalmological evaluation only once, except for patients with findings likely related to the COVID-19 condition, who were followed until resolution. All participants received the Free and Informed Consent Form (ICF) which was duly signed. The present study was conducted in accordance with the relevant guidelines and regulations/ethical principles of the Declaration of Helsinki.
Confirmation of COVID-19 Diagnosis
All patients who participated in the study had COVID-19 infection confirmed by molecular testing (RT-PCR) as it is the most sensitive and accurate test available.
Clinical Data
An ophthalmologist on the research team interviewed patients to assess any new ocular symptoms during or after the appearance of systemic COVID-19 symptoms. The clinician also recorded comorbidities, date of symptoms onset, the disease’s clinical course, admission to the intensive care unit (ICU), and the necessity for invasive mechanical ventilation. Patients who needed hospitalization also had medical charts reviewed for collection of any missing information.
Eye Examination and Multimodal Retinal Imaging
Patients underwent comprehensive ophthalmological evaluations performed by an ophthalmologist on the research team, including the following: determination of the best-corrected distance visual acuity using Early Treatment Diabetic Retinopathy Study (ETDRS) visual charts; measurement of intraocular pressure with Goldman’s applanation tonometer; biomicroscopy of the anterior segment; biomicroscopy of the posterior segment using a hand-held 78-dioptre condensing lens; and dilated eye examination using a binocular indirect ophthalmoscope, and a hand-held condensing 20-dioptre lens after 30 min of instillation of tropicamide (1%).
Multimodal retinal imaging included retinographies using the CX-1 Hybrid Digital Mydriatic/Non-Mydriatic Retinal Camera (Canon Medical Systems USA, Tustin, CA, USA) and Heidelberg Spectralis (Heidelberg Engineering, Germany) spectral-domain optic coherence tomography (SD-OCT) using macular fast and seven lines techniques. Macular-centred retinographies of both eyes were performed as well as peripheric photos if any retinal finding was present. Each photo included a colour image and a monochromatic red-free image. Two retinal specialists then analysed Retinographies and SD-OCT images, and the results were described by each specialist individually. Divergent opinions were reconciled by consensus. Any patient who had ophthalmologic findings possibly related to COVID-19 was followed up until the findings resolved.
Statistical Analysis
Before the statistical analysis of the data, a Shapiro–Wilk test was performed, and the p-value was >0.05. In this case, we can consider the values as normal or that the sample follows a normal distribution. The data were expressed as medians and interquartile range (IQR) for continuous variables. Categorical variables were expressed as proportions with 95% confidence intervals computed using the Wilson–Brown hybrid method. These analyses were performed using GraphPad Prism® (GraphPad®, version 8.0, San Diego, CA, USA).
Results
There were 50 subjects (29 males and 21 females) with a median age of 46.5 years [standard deviation 15.8 years]. Of these, 42% (21) of the patients had mild disease, 18% (9) had severe disease, and 40% (20) had critical disease. Eleven (22%) required invasive mechanical ventilation. Fifteen (30%) had a previous diagnosis of hypertension, and 12 (24%) had diabetes mellitus (Table 1).
 |
Table 1 Clinical Characteristics of Post-COVID-19 Patients |
The median time (IQR) between symptom onset and eye examination was 55 days [IQR 39–71]. Seven patients (14%) reported ophthalmic symptoms, three (6%) with transitory low visual acuity and four (8%) retroocular pain during the disease.
At OCT, the most common finding was signs of age-related macular degeneration (Table 2). Three patients had possible retinal changes related to COVID-19, all of whom are described below. A female patient in her 60s with no systemic problems post-COVID-19 presented with sectoral retinal pallor suggestive of acute retinal ischaemia and intracellular oedema of the inner layers, evolving into focal atrophy of the retina during OCT 30 days after onset of symptoms. She was admitted to the infirmary. She did not use vasoactive drugs and had no thrombotic events during hospitalization. At the 70-day follow-up, the retinal pallor area at fundoscopy had disappeared entirely, and the OCT revealed thinning of the inner layers of the retina in the previous pallor area, indicating local atrophy secondary to ischaemia (Figure 1).
 |
Table 2 Ocular Findings on Eye Examination of Patients Post-COVID-19 |
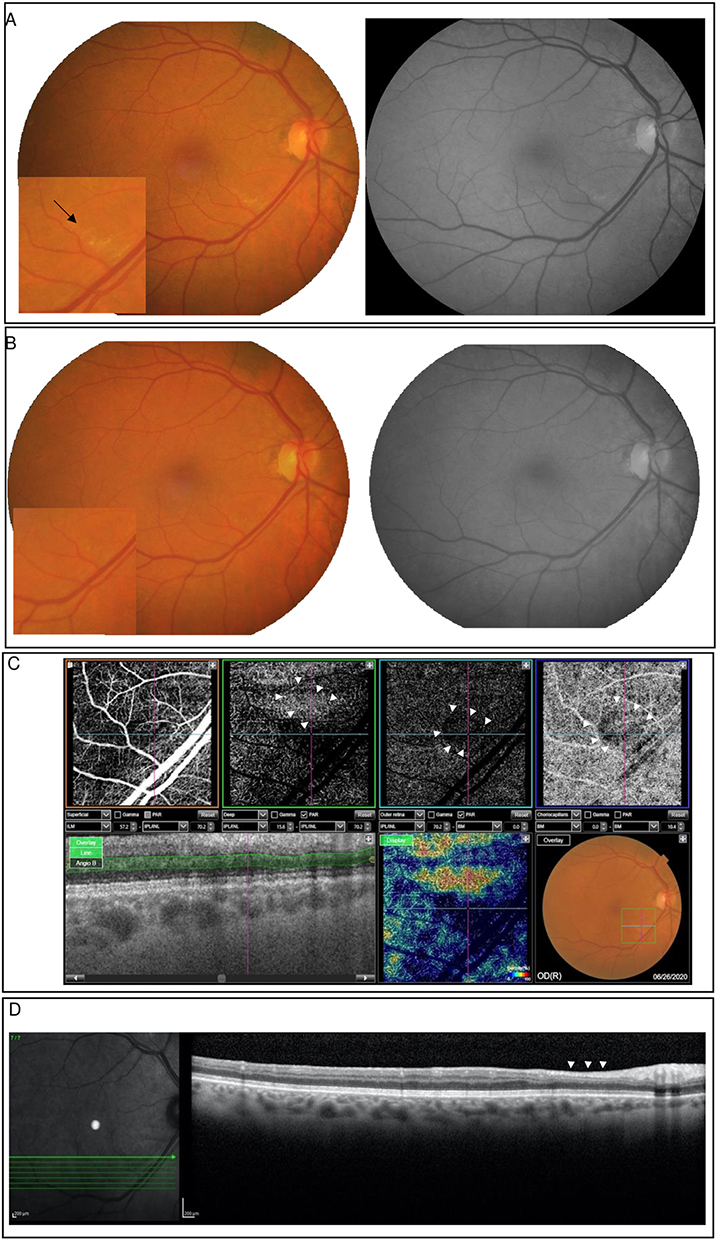 |
Figure 1 Main retinal findings and OCT follow-up patient 1 (A–C). (A) Colour fundus photography and red-free 30-days after symptoms imaging of the right eye of a female patient in her 60s revealing well-delimited sectorial pallor at the lower temporal arcade (black arrow). Vasoactive pharmacological support was not necessary during hospitalisation. (B) Colour fundus photography and red-free 70-days with disappearance of the lesion. (C) OCT-A 30-day follow-up shows a triangular area of low blood flow (white arrowhead), corresponding to the region of retinal pallor. (D) OCT B-scan in the 70-day follow-up of the retinal pallor. Note the local retinal thinning, with loss of differentiation of the inner layers of the retina (white arrowhead). |
A man, age range 40s, hypertension and diabetes mellitus presented with intraretinal cysts in the outer nuclear layer (N = 1; 2%; 95% CI 0.1–10.5) 41 days after onset of symptoms. He was admitted to the ICU and was mechanically ventilated, without vasoactive drugs, but with full-dose anticoagulation. He had uncontrolled blood glucose on admission, requiring an insulin pump. Simple mean of measurements of daily capillary blood sugar during hospitalization was 233 mg/dL. At the 68-day follow-up, the retinal findings had resolved entirely without intervention. He reported good glycaemic control after discharge (Figure 2).
 |
Figure 2 Main retinal findings and OCT follow-up patient 2 (A–C). (A) Colour fundus photography and red-free imaging of the left eye of a male patient revealing a peripapillary and macular flame-shaped haemorrhage (black arrow). Vasoactive pharmacological support was not necessary during hospitalisation. (B) Intraretinal cysts in the outer nuclear layer with 41-day after symptoms. (C) OCT 68-days after symptoms without intraretinal cysts. |
Finally, a male in his 30s, without comorbidities, presented flame-shaped haemorrhages (N = 1; 2%; 95% CI 0.1–10.5) 75 days after the onset of symptoms. He had a mild condition, without hospitalisation. The patient denied using any medication for continuous use. Follow-up was not possible because the patient did not attend subsequent consultations (Figure 3).
 |
Figure 3 Main retinal findings patient 3 (A) Colour fundus photography and red-free imaging of the left eye of a male patient, without comorbidities and revealing a flame-shaped haemorrhage (black arrow). He had a mild condition, without hospitalisation. |
Discussion
This study aimed to provide information on the relationship between SARS-CoV-2 infection and possible retinal changes. The primary objective was to identify ophthalmic findings using complete ocular examination and optical coherence tomography with a cross-sectional sample at various stages of the COVID-19. In our study, 14% of the patients had ophthalmic symptoms during or after the disease, the most frequent being transient low visual acuity (6%) and retroocular pain (8%). The primary findings were cataracts on biomicroscopy, intraocular pressure within the population pattern, hypertensive retinopathy in the retinal scan, and findings compatible with age-related macular degeneration on OCT. These findings are consistent with ophthalmological changes found in the general population.11 Because our sample included patients with advanced age and comorbidities, including systemic arterial hypertension and diabetes mellitus, the most frequent findings were expected.
Nevertheless, there were three findings possibly related to COVID-19. One adult man with no significant past medical history presented with flame-shaped haemorrhages; a woman in her 60s with no significant past medical history or complications during hospitalisation presented with retinal pallor area at fundoscopy that completely disappeared. The OCT revealed thinning of the retina’s inner layers in the previous area of pallor, indicating local atrophy secondary to ischaemia.
Our findings are consistent with those of two recent studies. Marinho et al reported similar changes in four patients who presented with subtle cotton wool spots and microhaemorrhages along the retinal arcade 11–33 days after onset of COVID-19 symptoms.8 Landecho et al evaluated 27 asymptomatic patients, and cotton wool exudates (CWS) were evident in six (22%), suggesting that the occurrence of CWS is an ocular manifestation of COVID-19; fundoscopic examination might help to identify subjects with endothelial disease that are prone to acute vascular events.18
We believe that the primary forms of vascular damage in patients with COVID-19 may be related to the direct action of the virus and its high levels of immunogenicity, leading to endothelial inflammation (similar to vasculitis) or the pro-thrombotic state.18,19 The first hypothesis is because asymptomatic ocular microangiopathic syndrome is highly prevalent in other vascular systemic diseases (ie, diabetes and hypertension) and after viral infections, including the human immunodeficiency virus (HIV) disease.18,20 SARS-CoV-2, a beta-coronavirus, uses the angiotensin-converting enzyme-related carboxypeptidase (ACE2) receptor to gain entry into cells.21 Expression of the ACE2 receptor is also found in many extrapulmonary tissues, including endothelium and retina.6,21 The ACE2 receptor is involved in the pathogenesis of systemic vascular diseases that produce ocular manifestations such as diabetic and hypertensive retinopathy.14,15,18 Therefore, the development of retinal ischaemia may be related to the downregulation of ACE2 in COVID-19.21 The second hypothesis is based on the fact that the state of hypercoagulability is already well established in COVID-19; the retina, as one of the most metabolically active tissues in the human body with a characteristic terminal circulation, is particularly susceptible to ischaemic events.12,22
Finally, a man in his 40s presented macular oedema after glycaemic decompensation during hospitalisation in the ICU for COVID-19. The ocular symptoms spontaneously resolved after discharge and stabilization of his diabetes. Inflammation plays an essential role in DR pathogenesis, characterised by involvement of endothelial cell adhesion molecules, chemokines, and proinflammatory cytokines.22 Raony et al argued that the transmembrane glycoprotein CD147 (also known as basigin) may play a role in retinal changes in diabetic patients with COVID-19.22 This glycoprotein has been reported as a new invasive pathway for SARS-CoV-2 and is expressed at moderate-to-high levels in all types of human retinal cells. Also, there is evidence that CD147 mediates the breakdown of neurovascular barriers induced by pro-inflammatory cytokines in vitro. Therefore, we believe that COVID-19 can aggravate or precipitate retinal lesions in people with diabetes, either by the indirect effects of the cytokine storm associated with COVID-19 or by the direct effects of retinal SARS-CoV-2 infection.22–25
Our cross-sectional study’s strengths were that we performed complete ophthalmological evaluations, including the posterior segment, with a large sample of patients at various stages of the disease and in patients who had different comorbidities. This study had a significant limitation in that there were prolonged intervals between the disease and the exam, allowing for the loss of transient changes. However, new methodological approaches will be necessary to endorse the hypotheses of this study. Furthermore, we acknowledge limitations in this study such as sample size and varying levels of infection. We believe that another possibility that will enrich the findings is to re-evaluate the study participants after 1 year of recovery from infection to reinforce the results.
In conclusion, patients with COVID-19 present findings consistent with those of the general population according to age and comorbidities; nevertheless, based on previous evidence regarding Covid-19 transmission, it is possible that the observed relationship between acute retinal findings and SARS-CoV-2 infection is mediated by cytokine storm, or the pro-thrombotic state associated with COVID-19. However, larger and more comprehensive studies should be conducted to confirm this hypothesis.
Data Sharing Statement
The data will be available under request to corresponding author ([email protected]).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
All authors declare no conflict of interest.
References
1. World Health Organization. WHO Coronavirus Disease (COVID-19) dashboard; 2021. Available from: https://covid19.who.int/.
2. Huang C, Wang Y, Li X, et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. 2020;395(10223):497–506. doi:10.1016/S0140-6736(20)30183-5
3. Lu R, Zhao X, Li J, et al. Genomic characterisation and epidemiology of 2019 novel coronavirus: implications for virus origins and receptor binding. Lancet. 2020;395(10224):565–574. doi:10.1016/S0140-6736(20)30251-8
4. Guan WJ, Ni ZY, Hu Y, et al. Clinical characteristics of coronavirus disease 2019 in China. N Engl J Med. 2020;382:1708–1720. doi:10.1056/NEJMoa2002032
5. Romero-Castro RM, Ruiz-Cruz M, Alvarado-de la Barrera C, et al. Posterior Segment Ocular Findings In Critically Ill Patients with COVID-19. Retina. 2022;42(4):628–633. doi: 10.1097/IAE.0000000000003457
6. Lai CC, Ko WC, Lee PI, Jean SS, Hsueh PR. Extra-respiratory manifestations of COVID-19. Int J Antimicrob Agents. 2020;56(2):106024. doi:10.1016/j.ijantimicag.2020.106024
7. Wu P, Duan F, Luo C, et al. Characteristics of ocular findings of patients with Coronavirus Disease 2019 (COVID-19) in Hubei Province, China. JAMA Ophthalmol. 2020;138(5):575–578. doi:10.1001/jamaophthalmol.2020.1291
8. Marinho PM, Marcos AAA, Romano AC, Nascimento H, Belfort R
9. Xia J, Tong J, Liu M, Shen Y, Guo D. Evaluation of coronavirus in tears and conjunctival secretions of patients with SARS-CoV-2 infection. J Med Virol. 2020;92(6):589–594. doi:10.1002/jmv.25725
10. Mehta P, McAuley DF, Brown M, et al. COVID-19: consider cytokine storm syndromes and immunosuppression. Lancet. 2020;395(10229):1022–1034. doi:10.1016/S0140-6736(20)30628-0
11. Wong TY, Klein R, Sharrett AR, et al. The prevalence and risk factors of retinal microvascular abnormalities in older persons: the cardiovascular health study. Ophthalmology. 2003;110(4):658–666. doi:10.1016/S0161-6420(02)01931-0
12. Pereira LA, Soares LCM, Nascimento PA, et al. Retinal findings in hospitalised patients with severe COVID-19. Br J Ophthalmol. 2020;106:102–105. doi:10.1136/bjophthalmol-2020-317576
13. Casagrande M, Fitzek A, Püschel K, et al. Detection of SARS-CoV-2 in human retinal biopsies of deceased COVID-19 patients. Ocul Immunol Inflamm. 2020;28(5):721–725. doi:10.1080/09273948.2020.1770301
14. Invernizzi A, Torre A, Parrulli S, et al. Retinal findings in patients with COVID-19: results from the SERPICO-19 study. EClinicalMedicine. 2020;27:100550. doi:10.1016/j.eclinm.2020.100550
15. Pirraglia MP, Ceccarelli G, Cerini A, et al. Retinal involvement and ocular findings in COVID-19 pneumonia patients. Sci Rep. 2020;10(1):1–7. doi:10.1038/s41598-020-74446-6
16. Ministério da Saúde. [Brazilian Ministry of Health]. Emergência de Saúde Pública de Importância Nacional pela Doença pelo Coronavírus 2019: vigilância Integrada de Síndromes Respiratórias Agudas Doença pelo Coronavírus 2019, Influenza e outros vírus respiratórios. [Public Health Emergency of National Concern for Coronavirus Disease 2019: Integrated Surveillance of Acute Respiratory Syndromes Coronavirus Disease 2019, Influenza and other respiratory viruses]; 2020. Available from: https://portalarquivos.saude.gov.br/images/pdf/2020/April/07/GuiaDeVigiEpidemC19-v2.pdf.
17. Sgorlon G, Queiroz JADS, Roca TP, et al. Clinical and epidemiological aspects of delta and gamma SARS-CoV-2 variant of concern from the western Brazilian Amazon. Mem Inst Oswaldo Cruz. 2022;117:e220155. doi:10.1590/0074-02760220155
18. Landecho MF, Yuste JR, Gándara E, et al. COVID‐19 retinal microangiopathy as an in vivo biomarker of systemic vascular disease? J Intern Med. 2020;289(1):116–120. doi:10.1111/joim.13156
19. Varga Z, Flammer AJ, Steiger P, et al. Endothelial cell infection and endotheliitis in COVID-19. Lancet. 2020;395(10234):1417–1418. doi:10.1016/S0140-6736(20)30937-5
20. Jaworski C. Morphology of the HIV versus the diabetic cottonwool spot. Optom Vis Sci. 2000;77(11):600–604. doi:10.1097/00006324-200011000-00010
21. Zhang H, Penninger JM, Li Y, Zhong N, Slutsky AS. Angiotensin-converting enzyme 2 (ACE2) as a SARS-CoV-2 receptor: molecular mechanisms and potential therapeutic target. Intensive Care Med. 2020;46(4):586–590. doi:10.1007/s00134-020-05985-9
22. Raony Í, Figueiredo CS. Retinal outcomes of COVID-19: possible role of CD147 and cytokine storm in infected patients with diabetes mellitus. Diabetes Res Clin Pract. 2020;165:108280. doi:10.1016/j.diabres.2020.108280
23. Guzzi PH, Mercatelli D, Ceraolo C and Giorgi FM. Master Regulator Analysis of the SARS-CoV-2/Human Interactome. J Clin Med. 2020;9(4):982. doi:10.3390/jcm9040982
24. Kochi AN, Tagliari AP, Battista Forleo G, Fassini GM, Tondo C Cardiac and arrhythmic complications in patients with COVID-19. J Cardiovasc Electrophysiol. 2020;31(5):1003–1008. doi:10.1111/jce.14479
25. Iba T, Levy JH, Levi M, Connors JM, Thachil J Coagulopathy of Coronavirus Disease 2019. Crit Care Med. 2020;48(9):1358–1364. doi:10.1097/CCM.0000000000004458
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
COVID-19 and Saudi Arabia: Awareness, Attitude, and Practice
Fawzy MS, AlSadrah SA
Journal of Multidisciplinary Healthcare 2022, 15:1595-1618
Published Date: 26 July 2022
A Pilot Study of 0.4% Povidone-Iodine Nasal Spray to Eradicate SARS-CoV-2 in the Nasopharynx
Sirijatuphat R, Leelarasamee A, Puangpet T, Thitithanyanont A
Infection and Drug Resistance 2022, 15:7529-7536
Published Date: 21 December 2022
Transient Increase in Patient Numbers with “Acute Macular Neuroretinopathy” Post SARS-CoV-2 Infection—Case Series During the First Surge of Infection in December 2022
Xu B, Zhang J, Zhang Y, Cheng Y, Huang Q
Journal of Inflammation Research 2023, 16:2763-2771
Published Date: 3 July 2023
Distinct Features of Vascular Diseases in COVID-19
Ceasovschih A, Sorodoc V, Shor A, Haliga RE, Roth L, Lionte C, Onofrei Aursulesei V, Sirbu O, Culis N, Shapieva A, Tahir Khokhar MA, Statescu C, Sascau RA, Coman AE, Stoica A, Grigorescu ED, Banach M, Thomopoulos C, Sorodoc L
Journal of Inflammation Research 2023, 16:2783-2800
Published Date: 6 July 2023
Early-Phase Perceptions of COVID-19’s Impact on Ophthalmology Practice Patterns: A Survey from the Pan-American Association of Ophthalmology
Bonilla-Escobar FJ, Sánchez-Cano D, Lasave AF, Soria J, Franco-Cárdenas V, Reviglio VE, Dantas PE, Palacio Pastrana C, Corbera JC, Chan RY, Diaz AL, Garcia Hernandez M, Maia M, Carpentier C, Wu L, Sanchez M, Murillo Sasamoto M, Murillo Azcárraga G, Roca JA, Serrano MA, Alezzandrini AA, Sanchez Montoya JG, Gabela G, Garcia-Aguirre G, Arevalo JF
Clinical Ophthalmology 2023, 17:3249-3259
Published Date: 31 October 2023