Back to Journals » Clinical Ophthalmology » Volume 17
Early-Phase Perceptions of COVID-19’s Impact on Ophthalmology Practice Patterns: A Survey from the Pan-American Association of Ophthalmology
Authors Bonilla-Escobar FJ, Sánchez-Cano D ![]() , Lasave AF
, Lasave AF ![]() , Soria J
, Soria J ![]() , Franco-Cárdenas V, Reviglio VE, Dantas PE, Palacio Pastrana C
, Franco-Cárdenas V, Reviglio VE, Dantas PE, Palacio Pastrana C ![]() , Corbera JC, Chan RY, Diaz AL, Garcia Hernandez M, Maia M
, Corbera JC, Chan RY, Diaz AL, Garcia Hernandez M, Maia M ![]() , Carpentier C, Wu L, Sanchez M
, Carpentier C, Wu L, Sanchez M ![]() , Murillo Sasamoto M, Murillo Azcárraga G, Roca JA, Serrano MA, Alezzandrini AA, Sanchez Montoya JG, Gabela G
, Murillo Sasamoto M, Murillo Azcárraga G, Roca JA, Serrano MA, Alezzandrini AA, Sanchez Montoya JG, Gabela G ![]() , Garcia-Aguirre G
, Garcia-Aguirre G ![]() , Arevalo JF
, Arevalo JF ![]()
Received 10 August 2023
Accepted for publication 24 October 2023
Published 31 October 2023 Volume 2023:17 Pages 3249—3259
DOI https://doi.org/10.2147/OPTH.S434776
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Francisco Javier Bonilla-Escobar,1– 3,* Daniel Sánchez-Cano,1,* Andres F Lasave,4 Jaime Soria,5 Valentina Franco-Cárdenas,6 Victor E Reviglio,7 Paulo EC Dantas,8 Claudia Palacio Pastrana,9 Juan Carlos Corbera,10 Rita Yee Chan,11 Alberto Luis Diaz,12 Milton Garcia Hernandez,13 Mauricio Maia,14 Cristian Carpentier,15 Lihteh Wu,16 Martin Sanchez,17 Marcelo Murillo Sasamoto,18 Gonzalo Murillo Azcárraga,18 Jose A Roca,19 Martin A Serrano,20 Arturo A Alezzandrini,21 Juan Gonzalo Sanchez Montoya,22 Gregorio Gabela,23 Gerardo Garcia-Aguirre,24 J Fernando Arevalo25,*
1Fundación Somos Ciencia al Servicio de la Comunidad, Fundación SCISCO/Science to Serve the Community Foundation, SCISCO Foundation, Cali, Colombia; 2Ophthalmology Department, Institute for Clinical Research Education, School of Medicine, University of Pittsburgh, Pittsburgh, PA, USA; 3Vision y Salud Ocular, VISOC, Ophthalmology Department, Universidad del Valle, Cali, Colombia; 4The Retina and Vitreous Department, Private Eyes Clinic, Mar del Plata, Argentina; 5Ophthalmology Department, Clínica Real Visión, Uniofken, CIVE y Funcrisa, Guayaquil, Ecuador; 6Ophthalmology Department, Sanatorio Oftalmológico Mérida, Mexico City, Mexico; 7Ophthalmology Department, Instituto de la Visión Cerro, Sanatorio Allende Cerro & Universidad Católica de Córdoba, Health Science Faculty, Cordoba, Argentina; 8Ophthalmology Department, Sorocaba Eye Bank Hospital, Sorocaba, Brazil; 9Department of Microsurgery of the Anterior Segment, Fundación Hospital Nuestra Señora de la Luz IAP, Mexico City, Mexico; 10Ophthalmology Department, Oftalmica Clinica de la Vision, Lima, Peru; 11Ophthalmology Department, Clinica Nacional de Oftalmologia, Panama City, Panama; 12Ophthalmology Department, Complejo Medico FOSCAL Internacional, Floridablanca, Santander, Colombia; 13Ophthalmology Department, Private Practice, El Salvador, El Salvador; 14Ophthalmology Department, Federal University of Sao Paulo, Sao Paulo, Brazil; 15Ophthalmology Department, Fundación Oftalmológica Los Andes, Santiago, Chile; 16Retina Department, Asociados de Macula Vitreo y Retina de Costa Rica, San Jose, Costa Rica; 17Ophthalmology Department, Hospital de Minas, Montevideo, Uruguay; 18Ophthalmology Department, Instituto Privado de Oftalmología, La Paz, Bolivia; 19Ophthalmology Department, Universidad Peruana Cayetano Heredia, Lima, Peru; 20Retina Department, Centro Médico Docente La Trinidad, Caracas, Venezuela; 21Ophthalmology Department, OFTALMOS, Universidad de Buenos Aires, Facultad de Medicina, Buenos Aires, Argentina; 22Ophthalmology Department, Instituto Nacional de Investigacion en Oftalmologia –INIO and Clinica Oftalmologica de Antioquia, Medellin, Colombia; 23Ophthalmology Department, Hospital Metropolitano, Quito, Ecuador; 24Retina Department, School of Medicine, Tecnológico de Monterrey Asociación Para Evitar la Ceguera en México, Mexico City, Mexico; 25Ophthalmology Department, Johns Hopkins University, Wilmer Eye Institute, Baltimore, MD, USA
*These authors contributed equally to this work
Correspondence: J Fernando Arevalo, Wilmer Eye Institute, Johns Hopkins University School of Medicine, 600 N. Wolfe Street, Maumenee 713, Baltimore, MD, 21287, USA, Email [email protected]
Purpose: The COVID-19 pandemic affected medical practice worldwide due to interventions to prevent spreading. Its effect on ophthalmology practices in Latin America has not yet been explored. We aimed to assess the perceptions about the pandemic from countries’ ophthalmological national and subspecialty retina societies affiliated to the Pan-American Association of Ophthalmology (PAAO).
Patients and Methods: A survey-based study of leaders of national ophthalmological and retinal societies was conducted. The survey was sent by email to 30 societies, from which 20 responded (12 countries, 66.6% response rate). It included closed- and open-ended questions about (1) operational capacity and precautions, (2) telemedicine and virtual care, (3) procedures, and (4) post-pandemic considerations.
Results: There was a marked decline in ophthalmology patient visits (80– 95%) and elective surgeries (90%) during 2020 compared to before the pandemic. Precautions like temperature checks, mask usage, and social distancing were widely implemented while personal protective equipment (PPE) availability varied. Telemedicine use was limited due to lack of experience with it. Reopening plans focused on maintaining precautions and gradually resuming activities. Economic and security concerns were raised, and adherence to guidelines was emphasized. Respondents acknowledged the need to adapt to a “new normal”. Long duration drugs, fewer imaging studies, and shorter wait times were preferred; however, availability of long duration drugs was limited.
Conclusion: The pandemic impacted ophthalmology in Latin America, with reduced patient visits, procedures, and surgeries. Delayed treatment and complications were likely the result of the pandemic.
Keywords: COVID-19, pandemics, international agencies, ophthalmology, retina, medical societies
Introduction
In 2020, the global landscape was reshaped by the outbreak of the coronavirus disease (COVID-19) caused by the SARS-CoV-2 virus.1 During the early stages, this unprecedented pandemic impact on healthcare was multifaceted. First, the virus itself posed a significant threat due to its high contagion and airborne transmission.1 Secondly, national health authorities implemented several interventions including lockdowns and social distancing, among others.2 During the lockdowns, there was a noticeable decline in medical consultations, hospitalizations due to other than COVID-19 medical conditions, and surgical procedures.3 This shift in focus towards managing the new disease and containing its spread inadvertently resulted in neglect and delays in treatment of other medical conditions.4
The COVID-19 early situation in Latin America was marked by intense uncertainty. There was a widespread lack of clarity regarding the pandemic course and the way of handling it was often chaotic.5 Mandatory lockdown measures were implemented across most countries, but each nation implemented them at its own pace and with its own approach.6
The field of ophthalmology was particularly affected by the pandemic both in the operating room and the clinic. Since many ophthalmic surgeries are elective, in settings where resources were scarce or restricted, they were delayed relative to more urgent cases.7 Additionally, ophthalmic assessments require proximity between the ophthalmologist and the patient, thereby increasing the risk of contagion.8,9 These factors contributed to a disruption in ophthalmology practices during the pandemic especially in Latin-America.9
Investigating the clinical patterns and consequences in early stages of this disruption becomes crucial to address the impact on patient outcomes and establish strategies for optimizing ophthalmic care during similar situations in the future. In this study, we used a survey to examine the perceptions of ophthalmologists in their clinical practices amidst the COVID-19 pandemic in countries represented by the presidents of national ophthalmological and retina subspecialty societies affiliated to the Pan-American Association of Ophthalmology (PAAO); a non-profit organization with a mission to prevent blindness through lifelong education and cultural exchange among ophthalmologists in the Western Hemisphere, encompassing over 35 countries.10
Materials and Methods
Setting and Design
This was a survey-based study based on information about the perceptions of the COVID-19 pandemic from the point of view of Latin-American representatives of national ophthalmologic and national retinal societies members of the PAAO. Surveys were collected between May 6 and May 26, 2020.
Participants
The survey participants consisted of the presidents of national ophthalmological and retina societies representing Latin American countries. We invited via email, 19 national societies of ophthalmology and 11 national retina societies. Out of 30 invited societies, 20 responded (66.6% response rate). The invitation clearly communicated to the participants that by opting to engage in the survey, they were providing their informed consent for the utilization of their data for research purposes. This consent was established based on implied consent.
Survey
The survey (Supplementary file 1) was designed based on a literature review of studies describing the perception of ophthalmologists during the pandemic.8,9,11–13 The questions included in the survey were divided into 4 groups for analysis: 1) Operational Capacity and Precautions: This group of questions focuses on the operational capacity of hospitals and clinics during the pandemic. It explores the intensive care unit (ICU) capacity and management, availability and utilization of personal protective equipment (PPE), and in-hospital measurements to prevent the spread of the virus; 2) Telemedicine and Virtual Care: This group of questions examines the adoption of telemedicine and virtual aids in ophthalmology practices during the pandemic. This group of questions highlights the role of technology in providing virtual care and support to patients; 3) Procedures: This group focuses on the impact of the pandemic in prescriptions, general and minor procedures, and in surgeries; and 4) Post-Pandemic Considerations: This group of questions addresses the plans for returning to normal activities, the post-pandemic considerations in ophthalmology practices, and differences in strategies from public or private institutions.
Of the total 38 questions, 24 were close-ended (yes/no, or frequencies), and 14 were open-ended. The answers were collected by email and the data was tabulated using Microsoft Excel.
Analysis
Data was firstly analyzed based on each country’s national representative society responses, and secondly on the responses of retinal societies representatives.
Close-ended questions were analyzed using Stata 18 (StataCorp, TX). Quantitative variables were analyzed using central tendency and dispersion measures while categorical variables were described using frequencies and percentages. A qualitative analysis was carried out through a categorization of open-ended questions. A content analysis using Atlas.ti® was carried out, identifying the points of convergence in the discourse of the respondents.
Participation in the study was voluntary and the study was deemed exempt from IRB approval.
Results
We collected 20 surveys including nine (45%) national ophthalmological societies and eleven (55%) retina societies. We had participation from 12 countries, including Argentina, Bolivia, Brazil, Chile, Colombia, Costa Rica, Ecuador, Mexico, Panamá, Perú, Uruguay, and Venezuela (Figure 1). A summary of the responses can be found in Table 1.
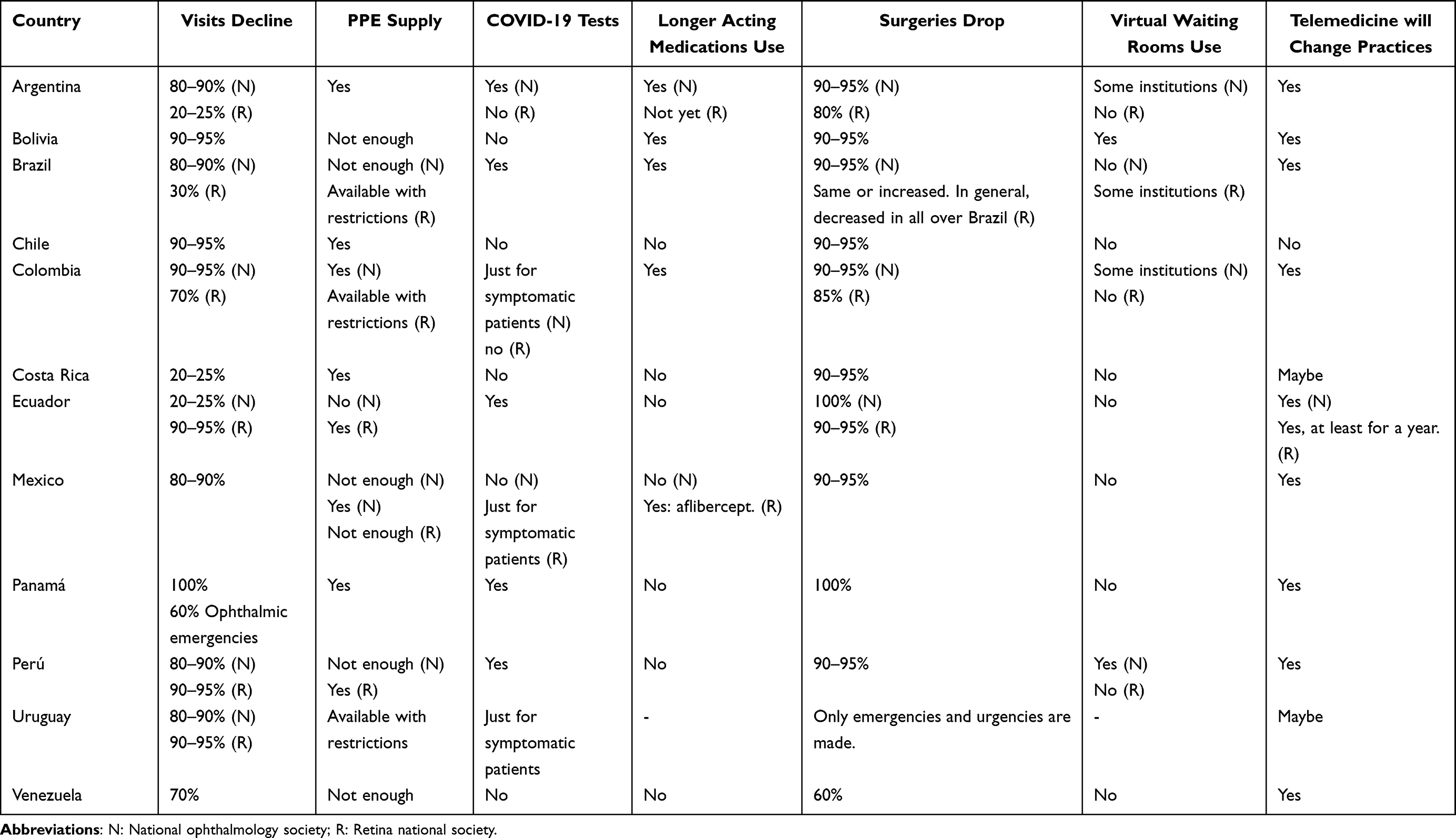 |
Table 1 Country-Specific Responses: Key Findings |
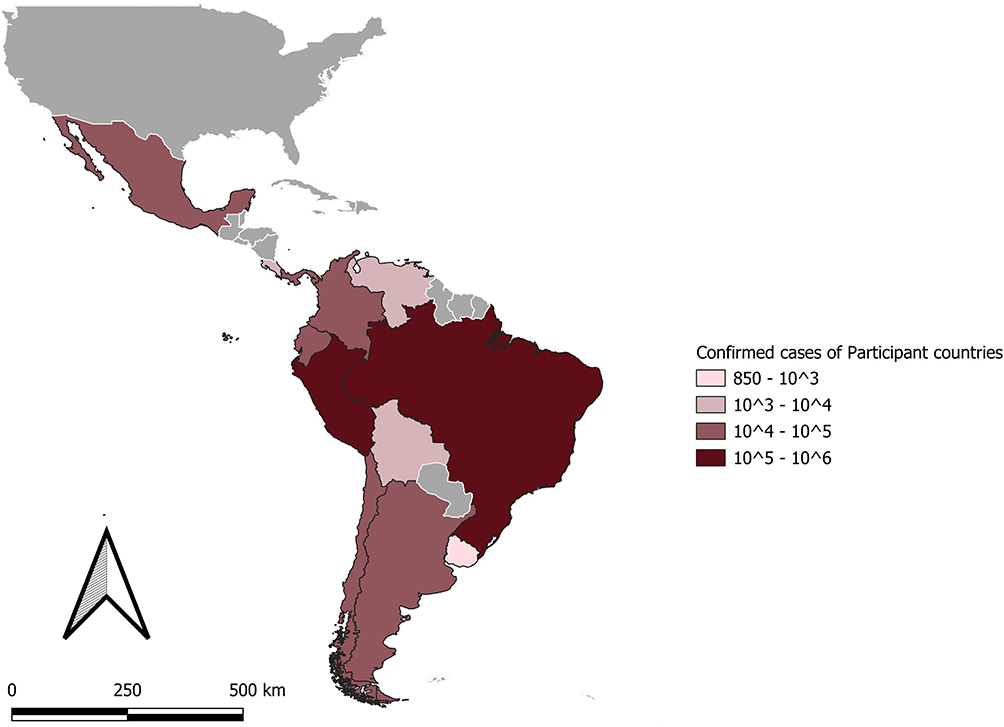 |
Figure 1 Confirmed Covid Cases Geographic Distribution of Responding National Ophthalmological and Retina Societies.2020, America. Notes: Data source: COVID survey May 2020. Pan American Health Organization. Confirmed Case Number PAHO COVID-19 Situation Report, n.10 (1 June 2020consulted from https://iris.paho.org/handle/10665.2/52438). Cartography source: “America”. Downloaded from https://www.efrainmaps.es/descargas-gratuitas/am%C3%A9rica/. Carlos Efraín Porto Tapiquén. Orogénesis Soluciones Geográficas. Porlamar, Venezuela 2015. Based on shapes from Environmental Systems Research Institute (ESRI). Free Distribution. |
Operational Capacity and Precautions
The average ICU capacity reported by the respondents was 3571.25 (±5783.54) beds. They indicated that the occupancy rate ranged from 50% to 80%. About 16.7% of the countries had no lockdown, while 83.3% had varying degrees.
Decrease in visits went down in 80–90% for 41.7% of countries, and up to 95% for 25% of participating countries. For surgeries, 66.7% of participating countries noted a 90–95% reduction, limiting surgeries exclusively to emergency and urgent cases.
PPE availability varied across the surveyed countries: descriptions included “available with restrictions”, “not enough”, “not available at all”, and “available” with 8.3%, 41.7%, 8.3%, and 41.7%, respectively. Staff received PPE in all countries, while N95 masks were provided to ophthalmologists in 9 out of 12 countries (75% of respondents). In one country, N95 masks were limited to aerosol-generating procedures (AGPs), and in another, they were reserved for suspected cases.
Facemask mandates were implemented in 91.67% of countries, with varying degrees in 8.3% of countries. Except for Costa Rica, masking requirements were enforced in almost all participating countries. All countries implemented social distancing measures.
A combination of temperature checks, social distancing, PPE usage, and enhanced cleaning protocols were implemented according to 33.3% of countries. Additionally, 16.7% reported implementing telephone triage, and 16.7% exclusively treated emergencies and post-operative cases.
All participants recognized the need to reduce visits time to minimize the risk of contagion. Some implemented 20–30-minute intervals between patients and aimed to limit visits time to under 2 hours (including testing and imaging). In 83.3% of countries, only essential testing was conducted, while 8.3% performed all necessary tests based on patient symptoms.
COVID-19 testing before consultations was carried out in 41.7% of countries, while an additional 16.7% focused on testing symptomatic patients only. The remaining 41.7% did not perform testing. In terms of surgeries, 75% of preoperative cases involved testing, while in 8.3% of cases, testing was performed only when COVID-19 was suspected.
In Ecuador, OR recovery units were converted into ICUs in some public hospitals, while the remaining 91.7% did not experience this change. In Panama, surgical staff was reassigned to provide support in the ICU.
Telemedicine and Virtual Care
In terms of overall telemedicine usage, 83.3% of the countries reported utilizing it to some extent as the technology and instruments were not in place to provide standard care. Virtual waiting rooms were available in certain institutions in Peru, while virtual scribes were utilized in Mexico, Peru, Brazil, and Bolivia (33.4%).
Regarding the administration of longer-acting medications, 58.3% of the countries do not have access to such medications, and 33.3% confirmed their usage (see Table 1).
Procedures
Regarding surgeries, 66.7% reported a decrease in surgical volume up to 90–95% compared to pre-pandemic numbers, 25% a decrease of 60–85%, and 8.3% stated that surgeries stopped completely. Emergency and urgent surgeries did not stop.
In 33.3% of the surveyed countries, general anesthesia was administered, while 16.7% reserved it for patients who could not be treated otherwise. Among respondents, 41.7% emphasized the use of PPE in the OR. N95 masks were available for OR cases in 66.7% of the countries but 16.6% used them only for confirmed cases. Additionally, 25% avoided general anesthesia, in one country ophthalmologists wore face masks for surgery in some institutions (8.3%), in another country air conditioning in the OR was variable (8.3%), and in one country access to the OR was limited (8.3%).
Regarding surgeries, almost half of the participants (47%) stated that surgeons in their countries did not operate on urgent cases that required more than 1 or 2 days of hospitalization and instead defer them to a later date. There were no delays in surgeries in 41.7% of the countries, while 25% indicated that they experienced delays which was observed more often in public hospitals than in private practices.
In private practices, urgent surgical cases are not considerably delayed, as patients know they are not attending an overcrowded clinic (Respondent #16)
Out of those surveyed, 47% acknowledged delays in patient care, with 27% specifically mentioning delays in retinal detachment cases. Most ophthalmological clinics remained closed during the pandemic, leading patients to seek care in emergency rooms. As a result, non-priority cases experienced further delays. It was mentioned that transportation restrictions also affected patient care.
In 33.3% of the countries, there was a 50 to 80% decrease in emergent/urgent cases, which was more common in private practices. There were also reports of occasional shortages in the OR availability (26%). It was found that as the number of emergencies decreased, more attention was paid to those patients that showed up:
The emergent/urgent cases have been receiving adequate attention as the general number of surgeries has drastically decreased… (Respondent #8)
Minor procedures were conducted only by 16.7% of respondents. Minimal imaging was performed in 41.7% of participating countries, with 25% stating they only did it if necessary or in emergency cases. Most of the sites (91.7%) tend to do short visits to limit time with patients and reducing exposure.
Post-Pandemic Considerations
Reopening plans varied among participants. The number of patient visits were reduced, leading to extended working hours and clinic hours on Saturdays. Doctors would have assigned days for patient care, accommodating a limited number of patients per day.
Participants discussed uncertain timing for returning to normal activities, considering government guidelines and fluctuating measures. They anticipated a phased reintroduction of appointments, prioritizing deferred cases.
The need for extended precautionary measures and a potential longer quarantine period was recognized. There was a significant decline in clinical ophthalmology activities, and a cautious approach was anticipated during reopening. Collaboration with national ophthalmological societies and adherence to government guidelines were emphasized. The “new normal” required adaptations such as telemedicine, reduced waiting room occupancy, and enhanced hygiene standards.
More than two thirds (68%) of countries support a gradual and regulated reopening plan based on government decisions. They proposed limited capacity to ensure relevant care. However, 21% still prioritize telemedicine due to variable biosafety measures and economic challenges.
(reopening) … depends on the Ministry of Health guidelines … So far the country is doing well and some of the measures are starting to be more flexible so maybe by June 2020 we may consider normal activities (Respondent #11)
Almost half of respondents (47%) believed that normalization of retina and ophthalmology practices should consider the availability of a COVID-19 treatment or vaccine. Additionally, 21% anticipate a prolonged timeline to return to usual practices due to persistent fear of contagion. They also highlight the limitations of telemedicine in certain cases:
For the next year, when COVID-19 has passed I expect that our retina clinics return to normal, I hope that my waiting room will be crowed as ever, and that no PPE should be used… Telemedicine in retinal practice is very complicate and you don´t get as much information as you need, so after the pandemic, it won´t be used as much… (Respondent #18)
Concerns about the economy and security were expressed, anticipating reduced spending and heightened fears among the population. Responses demonstrated a cautious and adaptive approach, prioritizing patient safety and adjusting clinical practice.
More than half of the participating countries (58.3%) expressed that “things would never be the same”, while 16.7% believed it would take at least a year to return to normal. When it came to waiting rooms, 58.3% of the participants mentioned that they would be less crowded, with 16.7% expecting this change to last for at least a year, 16.7% disagreed with the notion of less crowded waiting rooms, and 8.3% expressed uncertainty.
Telemedicine gradual implementation and the development of new strategies to improve the efficiency of care was the way to begin for 75% of surveyed participants. They believe this should be practiced until a vaccine is available. However, 8.3% disagree with this perspective.
New approaches such as telemedicine, virtual tools, virtual scribes, and home-based testing will redefine practices in ophthalmology according to 75% of respondents. They expect a reduction in in-person consultations, cost savings, improved follow-up, and increased efficiency. Conversely, 16.7% find this possibility plausible and 8.3% disagree.
Finally, 84% of those surveyed expressed that governmental hospitals have a latent disadvantage since they have scarce resources, lack of equipment, and are limited by governmental decisions. Additionally, they have a larger population and do not have enough personnel to cope.
Private practices has usually more access to PPE and others measures (Respondent #12)
Effects of the Pandemic in Retina Practices
According to the responses from Sub-specialty Retina Societies, it is noteworthy to mention:
- Operational Capacity and Precautions: COVID-19 testing pre-consultation and pre-surgical was not mandatory in most cases. Only in Chile, Peru, Ecuador they were performing COVID-19 testing, while in Mexico and Uruguay only in suspected cases.
- Surgical Procedures and Minor Interventions: All experienced a decline in patient visits, ranging from 20% to 95% decrease. Additionally, there was a significant drop in surgeries, with 90–95% of cases being affected. It was reported that surgical procedures were limited to emergencies only. When asked if they experienced delay in retina surgeries, only 15% of respondents, in Bolivia, Peru and Venezuela, said they had.
When it comes to minor procedures 10% of the practices, in Mexico and Peru, mentioned that they continued to perform them. As for minimal imaging, 80% of the practices reported that they were still performing it, Brazil and Argentina stated they were only performing Optic Coherence Tomography (OCT) while 10% (specifically in Venezuela and Ecuador) indicated that they were not performing any procedures nor imaging.
Intervals between appointments were extended with the use of telemedicine in 70% of retina societies’ responses. In Ecuador, respondents stated that they maintained the same intervals between injections but utilized telemedicine one week before the next appointment to ensure that an OCT was not required.
Willingness to use long-acting medications was observed in 40% of the cases, but most of the remaining respondents stated that they were not available.
- Telemedicine and Virtual Care: Although 80% of respondents (except for Chile and Argentina) stated the use of telemedicine in their practices, it was via telephone consultation mostly, since most of practices did not implement virtual waiting rooms, nor virtual scribes, while only 20% (Brazil and Bolivia) stated they had.
Discussion
COVID-19 was declared a pandemic on March 11th, 2020. In Latin America, Brazil reported its first case on February 25th, 2020, soon followed by confirmations in other nations.6 As of May 29th, 2020, the World Health Organization (WHO) documented an excess of 900,000 cases throughout Latin America and the Caribbean. Beyond these direct epidemiological consequences, it is imperative to recognize the pandemic’s substantial strain on national healthcare systems, particularly in low- and middle-income countries.5
Ophthalmology and retina practices observed a significant decline in patient visits and procedures.14,15 In one side, eye care is considered elective, non-vital or non-urgent.16 On the other side, proximity to patients during examinations and exposure to reusable equipment increased the risk of contagion.14 In this article, we have gathered the insights and practice patterns shared by the presidents of national ophthalmological and retina societies affiliated to the PAAO during the initial stages of the pandemic (May 6-May 26, 2020), shedding light on the experiences and perspectives of the situation in the region.
The Operational Capacity and Precautions
The duration and severity of lockdowns in the Americas varied, with most countries implementing them around mid-March. However, each country had its own approach, leading to a diverse range of measures and restrictions.17 Reasons for the variety of regulations included the severity of the outbreak, healthcare infrastructure, government regulations, and public compliance in each country.17
Social distancing and lockdowns further added to the challenges faced by ophthalmology practices, leading to a considerable decline in patient visits. Operations had to be adapted shifting the allocation of resources and focusing primarily on attending emergencies or urgent cases.18 Highlighting the need for flexibility and adaptability in managing ophthalmic practices during such uncertain and rapidly evolving situations.
Additional precautions, aligned with the WHO recommendations to protect both patients and healthcare professionals, were also used (ie, temperature checks, N95 masks, etc.).19 Other measures such as minimizing patient contact time, increasing intervals between patients, and limiting the overall time per visit, aimed to reduce unnecessary exposure to the virus and reduce transmission.20
Testing for COVID-19 prior to visits and procedures varied across countries. Testing was not uniformly implemented, creating a potential risk as asymptomatic patients could visit the clinic and transmit the virus.21 This risk was particularly concerning in ophthalmology due to the use of reusable equipment.14
Participants raised concerns about continuity of care as patients were not visiting eye clinics. It has been demonstrated that the pandemic increased the burden of eye diseases and complications in different countries.22–25 While the prioritization of urgent cases was necessary, efforts should be made to prevent the backlog of patients and provide timely care in a future pandemic.
Telemedicine and Virtual Care
The survey revealed a widespread acceptance and eagerness to adopt virtual tools and telemedicine as a mean of enhancing patient care. The use of telemedicine has demonstrated its cost-effectiveness and reproducibility not only in ophthalmology but also in other medical specialties.26 This acceptance of virtual care methods reflects a recognition of their potential to optimize healthcare delivery and improve access to medical services, particularly in times of crisis or when physical visits are limited.26 Despite the acceptance rate, the predominant type of telemedicine reported was limited to telephone calls for consultations or pre-consultations. On the other side, virtual care tools such as virtual consultations, point-of-care cameras for imaging, virtual waiting rooms, virtual scribes, assisted calls, among others were underutilized. By adopting a broader range of telemedicine tools, these practices could have overcome barriers posed by physical distancing and limited in-person visits.27 There was a missed opportunity to fully leverage the available telemedicine tools in ophthalmology practices in Latin America during the state of emergency. Further efforts should be made to scale-up teleophthalmology interventions in the region.
Procedures
The survey revealed a decline in the number of surgeries and minor procedures. This decrease can be attributed to the focus on emergent/urgent cases.4 Ophthalmology is a specialty that often performs various procedures during consultations,28 and the decrease in procedures had a direct impact on patient numbers. Fewer patients were seeking ophthalmic care for non-urgent conditions and due to fear of contagion.29 This decline in surgeries and minor procedures did not only affected the financial aspects of these practices but also had an impact on patient access to necessary treatments and interventions.30 Patients with existing eye pathologies who were unable to receive timely attention or vision-saving interventions (ie, intravitreal injections, laser photocoagulation) faced the risk of their conditions worsening or developing complications and blindness.31
The availability of longer-acting medications for intraocular use has been limited in the region. Access to new medications pose a significant challenge in Latin America, where affordability and availability may be limited. While new medications and treatment options may be accessible in high-income countries, the disparity in healthcare systems and resources can hinder their widespread use in the region.32
Post-Pandemic Consideration
Each ophthalmological society responded to the guidelines set by their respective countries’ governments as they navigated the transition to the “new normal”.33 The use of PPE, social distancing, and use of facemasks remained mandatory, although there were variations in its distribution and availability across practices.34
Many practices expressed the belief that the future would not be the same as before, acknowledging the ongoing restrictions and the potential for subsequent waves of contagion.35 Continued vigilance and strict adherence to safety measures were essential to protect the people.
Telemedicine use during the pandemic was perceived as a useful tool. However, it was underutilized for several reasons including the lack of infrastructure and experience with its methods. The use of this strategy helps not only in a situation of crisis, but it can also aid patients in remote regions.26 Further strategies and implementation studies are required to scale up telemedicine interventions.
Respondents pointed out that public hospitals often face significant challenges due to limited resources, inadequate equipment, and budgetary constraints. In contrast, private practices tend to have more autonomy and access to resources. These disparities pose a considerable concern, not only during the pandemic but also in future similar situations. Public hospitals in Latin America, which primarily cater to a larger and disadvantaged population, need adequate support and investment to ensure that they can effectively respond to healthcare crises.36 Efforts should be made to bridge the gap between public hospitals and private practices,37 and to create a more equitable and resilient healthcare system.38
Limitations
The survey may not have captured the full spectrum of nuances and variations within ophthalmology and retina practices in the region. As there where no response from 10 societies, nevertheless these countries had similar characteristics to the ones responded. Answers might have been subject to bias; however, respondents were country’s representatives, and they were invited to describe the national situation within their organizations. Invitations to participate were sent to all the PAAO member societies; nevertheless, not all answered the call for participation. However, we had a wide variety of participating countries from the region, with participation from countries from south, central and north America and from low- to high-income countries. The survey design and the responses received might have contributed to a more generalized view of the practices, thus minimizing potential differences that could exist.
Some responses were limited when the participants were asked to elaborate on their answers. To gain a more comprehensive understanding, further research and surveys with more detailed and specific questions would be beneficial. Furthermore, conducting a phased survey encompassing the entire pandemic timeline could facilitate a comparative analysis of perceptions, contrasting those from the early, mid, and post vaccination. It is also important to consider that variations in practices may exist regionally or institutionally, and a broader sample size or targeted surveys could provide a more accurate representation.
Conclusion
The early stages of the COVID-19 pandemic had a significant impact on ophthalmology practices in Latin America, according to the presidents of ophthalmology and retinal societies of the PAAO. These practices experienced a decline in patient visits, procedures, and surgeries, as governmental authorities classified ophthalmic services as non-essential. Telemedicine, although underutilized, was recognized as a valuable tool for patient care and has the potential for future development in the region. Differences among countries in terms of resource availability, policies, and guidelines created disparities in eye care, emphasizing the need for efforts to bridge these gaps.
Disclosure
Dr Gerardo Garcia-Aguirre reports grants/personal fees and/or non-financial support from Alcon, AbbVie/Allergan, Bayer, Heidelberg Engineering, Nidek, Novartis, Roche Genentech, and Zeiss, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Dhama K, Khan S, Tiwari R, et al. Coronavirus Disease 2019-COVID-19. Clin Microbiol Rev. 2020;33(4). doi:10.1128/CMR.00028-20
2. Jones NR, Qureshi ZU, Temple RJ, Larwood JPJ, Greenhalgh T, Bourouiba L. Two metres or one: what is the evidence for physical distancing in covid-19? BMJ. 2020;370:m3223. doi:10.1136/bmj.m3223
3. Pujolar G, Oliver-Anglès A, Vargas I, Vázquez ML. Changes in Access to Health Services during the COVID-19 Pandemic: a Scoping Review. Int J Environ Res Public Health. 2022;19(3):1749. doi:10.3390/ijerph19031749
4. Agarwal R, Sharma N, Patil A, Thakur H, Saxena R, Kumar A. Impact of COVID-19 pandemic, national lockdown, and unlocking on an apex tertiary care ophthalmic institute. Indian J Ophthalmol. 2020;68(11):2391–2395. doi:10.4103/ijo.IJO_2366_20
5. Bautista-Molano W, Ferreyra Garrot L, Toro C. Exploring the Impact of COVID-19 in Latin America. J Clin Rheumatol. 2020;26(6):218–219. doi:10.1097/RHU.0000000000001523
6. Rodriguez-Morales AJ, Gallego V, Escalera-Antezana JP, et al. COVID-19 in Latin America: the implications of the first confirmed case in Brazil. Travel Med Infect Dis. 2020;35:101613. doi:10.1016/j.tmaid.2020.101613
7. Felfeli T, Ximenes R, Naimark DMJ, et al. The ophthalmic surgical backlog associated with the COVID-19 pandemic: a population-based and microsimulation modelling study. CMAJ Open. 2021;9(4):E1063–e72. doi:10.9778/cmajo.20210145
8. Sahay P, Sharma N, Sinha R, Sachdeva MS. Ophthalmology practice during COVID-19 pandemic: a survey of Indian ophthalmologists. Indian J Ophthalmol. 2021;69(12):3638–3642. doi:10.4103/ijo.IJO_1589_21
9. Kaushik J, Riyaz E, Chaitanya YVK, et al. An insight into the altered ophthalmic dynamics during the COVID-19 pandemic. Indian J Ophthalmol. 2022;70(10):3643–3648. doi:10.4103/ijo.IJO_254_22
10. Bateman JB. The Pan American Association of Ophthalmology. Arch Ophthalmol. 2004;122(10):1534. doi:10.1001/archopht.122.10.1534
11. Bromeo AJ, Grulla-Quilendrino P, Lerit SJ, et al. Changes in Retina Practice Patterns During the COVID-19 Pandemic in the Philippines. Clin Ophthalmol. 2021;15:3493–3504. doi:10.2147/OPTH.S326594
12. Kortuem FC, Ziemssen F, Kortuem KU, Kortuem C. The Role and Views of Ophthalmologists During the COVID-19 Pandemic. Clin Ophthalmol. 2021;15:3947–3956. doi:10.2147/OPTH.S327745
13. Shoji M, Venincasa M, Sridhar J. The Impact of the COVID-19 Pandemic on Ophthalmology Resident Perceptions of Clinical Experience, Surgical Training, and Personal Life. J Academic Ophthalmol. 2021;13:e288–e97. doi:10.1055/s-0041-1740314
14. Romano MR, Montericcio A, Montalbano C, et al. Facing COVID-19 in Ophthalmology Department. Curr Eye Res. 2020;45(6):653–658. doi:10.1080/02713683.2020.1752737
15. Syed AAO, Jahan S, Aldahlawi AA, Alghazzawi EA. Preventive Practices of Ophthalmologists During COVID-19 Pandemic. Clin Ophthalmol. 2021;15:1267–1275. doi:10.2147/OPTH.S295730
16. Savastano A, Ripa M, Savastano MC, Kilian R, Marchini G, Rizzo S. Impact of the COVID-19 pandemic on ophthalmologic outpatient care: experience from an Italian Tertiary Medical Center. Ann Med. 2021;53(1):1349–1357. doi:10.1080/07853890.2021.1964036
17. Schwalb A, Armyra E, Méndez-Aranda M, Ugarte-Gil C. COVID-19 in Latin America and the Caribbean: two years of the pandemic. J Intern Med. 2022;292(3):409–427. doi:10.1111/joim.13499
18. Hu V, Wolvaardt E. Ophthalmology during COVID-19: who to see and when. Community Eye Health. 2020;33(109):20–23.
19. Chiu NC, Chi H, Tai YL, et al. Impact of Wearing Masks, Hand Hygiene, and Social Distancing on Influenza, Enterovirus, and All-Cause Pneumonia During the Coronavirus Pandemic: retrospective National Epidemiological Surveillance Study. J Med Internet Res. 2020;22(8):e21257. doi:10.2196/21257
20. Brodin AC, Tamhankar MA, Whitehead G, MacKay D, Kim BJ, O’Brien JM. Approach of an Academic Ophthalmology Department to Recovery During the Coronavirus Pandemic. Clin Ophthalmol. 2022;16:695–704. doi:10.2147/OPTH.S342300
21. Tan J, Liu S, Zhuang L, et al. Transmission and clinical characteristics of asymptomatic patients with SARS-CoV-2 infection. Future Virol. 2020;15(6):373–380. doi:10.2217/fvl-2020-0087
22. Jayallan B, Ngah NF, Hussain NI, et al. Impact of Postponement of Appointments on Vision and Psychological Well-Being Among Outpatients Attending Ophthalmology Clinics: a Malaysian Perspective. Cureus. 2023;15(5):e38423. doi:10.7759/cureus.38423
23. Zhao X, Meng L, Luo M, et al. The influence of delayed treatment due to COVID-19 on patients with neovascular age-related macular degeneration and polypoidal choroidal vasculopathy. Ther Adv Chronic Dis. 2021;12:20406223211026389. doi:10.1177/20406223211026389
24. Stone LG, Grinton ME, Talks JS. Delayed follow-up of medical retina patients due to COVID-19: impact on disease activity and visual acuity. Graefes Arch Clin Exp Ophthalmol. 2021;259(7):1773–1780. doi:10.1007/s00417-021-05174-4
25. Massamba N, Dirani A, Knoeri J, Pasquier B, Ingram A, Soubrane G. Evaluating the impact of summer vacation on the visual acuity of AMD patients treated with ranibizumab. Eye. 2015;29(11):1453–1457. doi:10.1038/eye.2015.128
26. Dolar-Szczasny J, Barańska A, Rejdak R. Evaluating the Efficacy of Teleophthalmology in Delivering Ophthalmic Care to Underserved Populations: a Literature Review. J Clin Med. 2023;12(9):3161. doi:10.3390/jcm12093161
27. Sharma M, Jain N, Ranganathan S, et al. Tele-ophthalmology: need of the hour. Indian J Ophthalmol. 2020;68(7):1328–1338. doi:10.4103/ijo.IJO_1784_20
28. Grewal DS, Gabr H. Inpatient Ophthalmology Consultations. Med Clin North Am. 2021;105(3):563–576. doi:10.1016/j.mcna.2021.02.006
29. Escribano Villafruela J, de Urquía Cobo A, Martín Luengo F, Antón Modrego V, Chamorro González-Cuevas M. Changing trends in ophthalmological emergencies during the COVID-19 pandemic. PLoS One. 2022;17(5):e0268975. doi:10.1371/journal.pone.0268975
30. Gurnani B, Kaur K. Economical and financial constraints for ophthalmologists during COVID-19 pandemic. Indian J Ophthalmol. 2022;70(1):328. doi:10.4103/ijo.IJO_2173_21
31. Alshammari F, Shaikh S, Hussain A, Alafnan A, Almuzaini I, Alshammari B. Public Awareness of Common Eye Diseases and the Role of Pharmacists in Raising This Awareness in Saudi Arabia: a Cross-Sectional Study. Healthcare. 2021;9(6):56.
32. Homedes N, Ugalde A. Availability and affordability of new medicines in Latin American countries where pivotal clinical trials were conducted. Bull World Health Organ. 2015;93(10):674–683. doi:10.2471/BLT.14.151290
33. Habersaat KB, Betsch C, Danchin M, et al. Ten considerations for effectively managing the COVID-19 transition. Nature Human Behaviour. 2020;4(7):677–687. doi:10.1038/s41562-020-0906-x
34. Soleman SR, Lyu Z, Okada T, et al. Efficacy of personal protective equipment to prevent environmental infection of COVID-19 among healthcare workers: a systematic review. Environ Health Prev Med. 2023;28:1. doi:10.1265/ehpm.22-00131
35. De La-Cruz Hernández SI, Barrera-Badillo G. The Delta variant triggers the third wave of COVID-19 in Mexico. Disaster Med Public Health Prep. 2022;1–5.
36. Litewka SG, Heitman E. Latin American healthcare systems in times of pandemic. Dev World Bioeth. 2020;20(2):69–73. doi:10.1111/dewb.12262
37. Filip R, Gheorghita Puscaselu R, Anchidin-Norocel L, Dimian M, Savage WK. Global Challenges to Public Health Care Systems during the COVID-19 Pandemic: a Review of Pandemic Measures and Problems. J Pers Med. 2022;12(8):1295. doi:10.3390/jpm12081295
38. OECD, Bank TW. Health at a Glance: Latin America and the Caribbean 2023; 2023.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
“We are Tired but Do Not Give Up” the Dilemma and Challenges of Primary Nurses Facing the Omicron Variant: Qualitative Research
Aditya RS, Yusuf A, Alrazeeni DM, Almutairi RL, Solikhah FK, Rahmatika QT, Kotijah S
Journal of Multidisciplinary Healthcare 2023, 16:797-809
Published Date: 27 March 2023
Ophthalmic Manifestations Among Patients Surviving COVID-19
Loduca Lima V, Soares LCM, Pereira LA, Nascimento PA, Cirillo LRN, Sakuma HT, da Veiga GL, Abucham-Neto JZ, Fonseca FLA
International Journal of General Medicine 2023, 16:1747-1755
Published Date: 9 May 2023
COVID-19’s Effects on Macroeconomic Indicators in Ethiopia: Systematic Review of Articles
Denano T
ClinicoEconomics and Outcomes Research 2023, 15:573-578
Published Date: 20 July 2023
The Link Between Gastrointestinal Microbiome and Ocular Disorders
Alfuzaie R
Clinical Ophthalmology 2023, 17:2133-2140
Published Date: 25 July 2023
The Pandemics of Mass Destruction: A Comparative Analysis of HIV/AIDS and Coronavirus (COVID-19)
Kajiita RM, Kang'ethe SM
Journal of Multidisciplinary Healthcare 2024, 17:889-899
Published Date: 1 March 2024