Back to Journals » ImmunoTargets and Therapy » Volume 14
Increased Co-Expression of PD-L1 and CTLA-4 Predicts Poor Overall Survival in Patients with Acute Myeloid Leukemia Following Allogeneic Hematopoietic Stem Cell Transplantation
Authors Chen C ![]() , Qiu K, Chen J, Wang S, Zhang Y, Wang C, Li Y
, Qiu K, Chen J, Wang S, Zhang Y, Wang C, Li Y ![]()
Received 13 October 2024
Accepted for publication 14 January 2025
Published 20 January 2025 Volume 2025:14 Pages 25—33
DOI https://doi.org/10.2147/ITT.S500723
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jadwiga Jablonska
Cunte Chen,1,2,* Kangjie Qiu,2,* Jie Chen,3,* Shunqing Wang,1 Yuping Zhang,1 Caixia Wang,1 Yangqiu Li2
1Department of Hematology, Guangzhou First People’s Hospital, Institute of Blood Transfusion and Hematology, Guangzhou Medical University, Guangzhou, 510180, People’s Republic of China; 2Institute of Hematology, School of Medicine, Key Laboratory for Regenerative Medicine of Ministry of Education, Jinan University, Guangzhou, People’s Republic of China; 3Department of Hematology, First Affiliated Hospital, Jinan University, Guangzhou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yangqiu Li, Institute of Hematology, School of Medicine, Key Laboratory for Regenerative Medicine of Ministry of Education, Jinan University, Guangzhou, 510632, People’s Republic of China, Email [email protected] Caixia Wang, Department of Hematology, Guangzhou First People’s Hospital, Institute of Blood Transfusion and Hematology, Guangzhou Medical University, Guangzhou, 510180, People’s Republic of China, Email [email protected]
Purpose: Our previous study has demonstrated that high expression of immune checkpoints (ICs) was significantly associated with adverse clinical outcomes in patients with acute myeloid leukemia (AML). This study aims to investigate the significance of the alteration of IC co-expression for evaluating the prognosis of AML patients following allogeneic hematopoietic stem cell transplantation (allo-HSCT).
Patients and Methods: Quantitative real-time PCR (qRT-PCR) data of bone marrow (BM) samples from 62 de novo AML patients, including 37 patients who received allo-HSCT and 25 patients who received chemotherapy only, were used for prognostic analysis.
Results: High expression of PD-1, PD-L1, PD-L2, CTLA-4, and LAG-3 was associated with poor overall survival (OS) in AML patients receiving allo-HSCT, while the expression levels of PD-1, PD-L2, CTLA-4, and LAG-3, other than PD-L1, were not significantly correlated with OS in AML patients receiving chemotherapy. Importantly, PD-L1/CTLA-4 was the best combination model for predicting poor OS in AML patients following allo-HSCT, especially combined with minimal residual disease (MRD).
Conclusion: High expression of ICs in BM of AML patients following allo-HSCT was related to poor outcomes, and increasing co-expression of PD-L1 and CTLA-4 might be one of the best immune biomarkers to predict outcomes in patients with AML.
Keywords: acute myeloid leukemia, allo-HSCT, immune checkpoint, biomarker, prognosis
Introduction
Allogeneic hematopoietic stem cell transplantation (allo-HSCT) is the most effective consolidation therapy for patients with intermediate and high-risk acute myeloid leukemia (AML).1 Although allo-HSCT significantly improves the long-term survival of AML patients, the strong heterogeneity of AML leads to recurrence in approximately 40% of patients and is the main cause of mortality after allo-HSCT.2,3 The main reason is not only related to the clinical and genomic diversity of AML but also closely related to the patients’ T cell dysfunction which is induced by AML immune suppression microenvironment.4,5
T cell dysfunction is mainly manifested by T cell senescence and exhaustion, the latter is thought to be induced by high expression of immune checkpoints (ICs), such as programmed cell death 1 (PD-1), cytotoxic T-lymphocyte associated protein 4 (CTLA-4), T-cell immunoglobulin and mucin-domain containing-3 (TIM-3), and lymphocyte activation gene-3 (LAG-3) etc.6–10 High expression of PD-1 in T cells and PD-L1 in AML cells has been observed, contributing to the inability of the immune system to effectively eliminate leukemic cells, which allows AML cells to persist and potentially relapse post-transplantation.11 Recently, several studies have investigated the safety and efficacy of IC inhibitors (ICIs) in relapsed AML patients after allo-HSCT.12,13 However, the overall response rate (complete remission and partial remission) was 25%, and another 25% of the patients achieved stable disease.11 Therefore, it is necessary to explore the important role of combining two ICIs under allo-HSCT, as well as the prognostic value of the co-expression pattern of the two ICs in AML. Our previous findings demonstrated that high expression of ICs predicts poor overall survival (OS) in AML patients.4,14,15 However, the prognostic significance of the co-expression patterns of ICs in AML patients following allo-HSCT is still unclear. In this study, the prognostic value of ICs in de novo AML patients following allo-HSCT from our clinical center was investigated.
Materials and Methods
AML Patients
During the period ranging from January 1, 2013, to December 31, 2018, a total of 62 BM samples were obtained from patients newly diagnosed with AML at our clinical center, including 37 patients who received allo-HSCT and 25 patients who received chemotherapy only, and the clinical characteristics were listed in Table S1. The median follow-up time for the 62 surviving patients was 45.6 months (range: 22.7–80.5 months). Positive minimal residual disease (MRD) was defined as ≥0.1% following the European Leukemia Net (ELN) recommendations.16,17 In addition, BM samples from 12 healthy individuals were used as controls.
Extraction of RNA and Quantitative Real-Time PCR (qRT-PCR)
Total RNA was extracted based on the manufacturer’s protocol for the TRIzol reagent (Invitrogen). RNA was reverse transcribed into cDNA using a reverse transcription kit (Promega, USA). The expression levels of PD-1, PD 1 ligand 1 (PD-L1), PD 1 ligand 2 (PD-L2), CTLA-4, and LAG-3 were quantified with a qRT-PCR kit (TIANGEN, China), and 18S rRNA was used as an internal control using the Real-Time System (Bio-Rad, USA).4 The list of primers for qRT-PCR is shown in Table S2. The expression levels of PD-1, PD-L1, PD-L2, CTLA-4, and LAG-3 are presented as 2−ΔΔCT values.
Statistical Analysis
All statistics were performed on SPSS (version 22.0, IBM, Armonk, NY, USA) and R (version 4.3.2, https://www.r-project.org/), as appropriate. Differences between the two or multiple groups of categorical variables were determined by chi-square or Fisher tests, as appropriate. Differences in Kaplan–Meier curves were analyzed using the Log rank test.18–20 The nomogram model was constructed using the R packages “foreign” and “rms”.21 The area under curve (AUC) in the receiver operating characteristic (ROC) curve was determined by the R package “pROC”. The best model was obtained by the package “glmulti”.22 The “survRM2” package was used to confirm the restricted mean survival time (RMST). The optimal cut-points of quantitative variables were determined by X-tile software (version 3.6.1, Yale University, New Haven, CT, USA). A two-tailed P value <0.05 was considered statistically significant.
Results
Higher Expression of ICs Was Associated with Poor OS in AML Patients Receiving allo-HSCT
Based on our previous findings that higher expression of PD-1, PD-L1, PD-L2, CTLA-4, and LAG-3 predicted poor OS in AML patients;4 thus, these five ICs were used for prognostic analysis in AML patients treated with allo-HSCT (Figure 1). Interestingly, a clear trend suggesting that high expression of PD-1 was associated with poor OS in AML patients, although there is no significant difference at that point [hazard ratio (HR) = 2.70, 95% confidence interval (CI): 0.83–8.80, P = 0.086; Figure 2A]. Moreover, the high expression of PD-L1 was associated with poor OS in AML patients (HR = 5.91, 95% CI: 1.90–18.33, P < 0.001), as well as PD-L2 (HR = 5.34, 95% CI: 1.18–24.22, P = 0.015) (Figure 2B and C). Additionally, the high expression of CTLA-4 and LAG-3 significantly predicts poor OS in AML patients (CTLA-4: HR = 6.72, 95% CI: 1.84–24.57, P < 0.001; LAG-3: HR = 6.56, 95% CI: 1.79–24.00, P < 0.001) (Figure 2D and E). However, the expression levels of PD-1, PD-L2, CTLA-4, and LAG-3, other than PD-L1, were not significantly correlated with OS in AML patients who underwent chemotherapy (P > 0.05, Figure S1A–E).
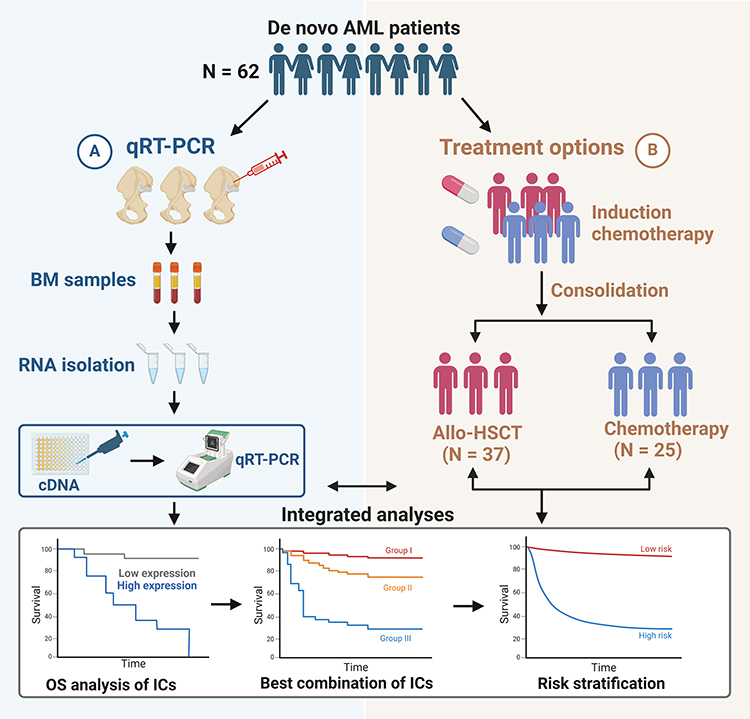 |
Figure 1 Study schematics. A total of 62 bone marrow (BM) samples from de novo AML patients were first collected for quantitative real-time PCR (qRT-PCR) detection of immune checkpoints (IC) mRNA expression levels, of which 37 patients received allogeneic hematopoietic stem cell transplantation (allo-HSCT) and 25 patients received chemotherapy. Then, overall survival (OS) analysis of ICs and identifies the optimal combination to predict the prognosis of AML patients and construct new risk stratification. |
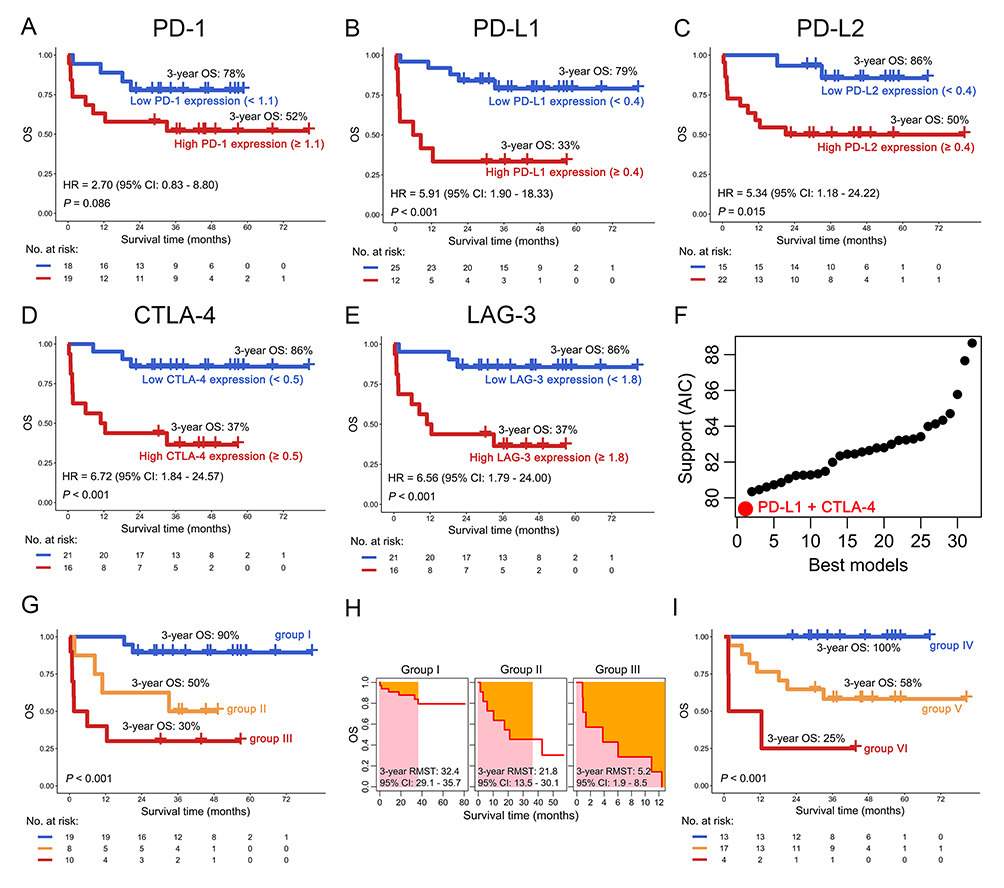 |
Figure 2 Overall survival (OS) analysis of immune checkpoints (ICs) in AML patients receiving allo-HSCT. (A–E) OS differences between AML patients with high and low expression of PD-1 (A), PD-L1 (B), PD-L2 (C), CTLA-4 (D), and LAG-3 (E). (F) Akaike information criterion (AIC) support profile from the best to the worst models of IC combinations. The red dots represent the best IC combination. (G and H) The differences of OS and 3-year restricted mean survival time (RMST) in groups I, II, and III based on the expression of PD-L1 and CTLA-4. Group I: PD-L1low and CTLA-4low; group II: PD-L1high/CTLA-4low and PD-L1low/CTLA-4high; group III: PD-L1high and CTLA-4high. (I) The differences of OS in groups IV, V, and VI based on the status of minimal residual disease (MRD) and expression of PD-L1/CTLA-4. Group IV: PD-L1low, CTLA-4low and negative MRD; group V: PD-L1high or CTLA-4high or positive MRD; group VI: PD-L1high, CTLA-4high and positive MRD. |
PD-L1/CTLA-4 Was the Best Combination Model for Predicting Poor OS in AML Patients Following allo-HSCT
Our previous publications indicated that increased co-expression of ICs was better than a single one in predicting adverse clinical outcomes for patients with hematological malignancies.4,23 In this study, we analyzed co-expression patterns of ICs and also found that PD-L1/CTLA-4 was the best combination model for predicting poor OS in AML patients following allo-HSCT (Figure 2F). AML with PD-L1highCTLA-4high (group I) has worse OS and 3-year RMST than PD-L1high/CTLA-4low and PD-L1low/CTLA-4high (group II) and PD-L1low/CTLA-4low (group III) (3-year OS: 30% vs 50% vs 90%; P < 0.001) (Figure 2G and H). Importantly, age, gender, and European Leukemia Network (ELN) risk stratification were included in univariate and multivariate Cox regression analyses to balance confounding factors, and the results suggested that age and increased co-expression of PD-L1 and CTLA-4 are independent OS predictors for AML patients (group III vs I: HR = 26.89, 95% CI: 2.84–254.18, P = 0.004; Table 1). Because MRD assessment helps refining prognosis and can support the adoption of post-transplant therapeutic modalities, MRD and PD-L1/CTLA-4 were combined for survival analysis. A total of 34 AML patients who received allo-HSCT had MRD data were collected, and the results indicated that positive MRD or high PD-L1/CTLA4 expression predicted poor OS in patients, especially when they occurred simultaneously (P < 0.001, Figure 2I).
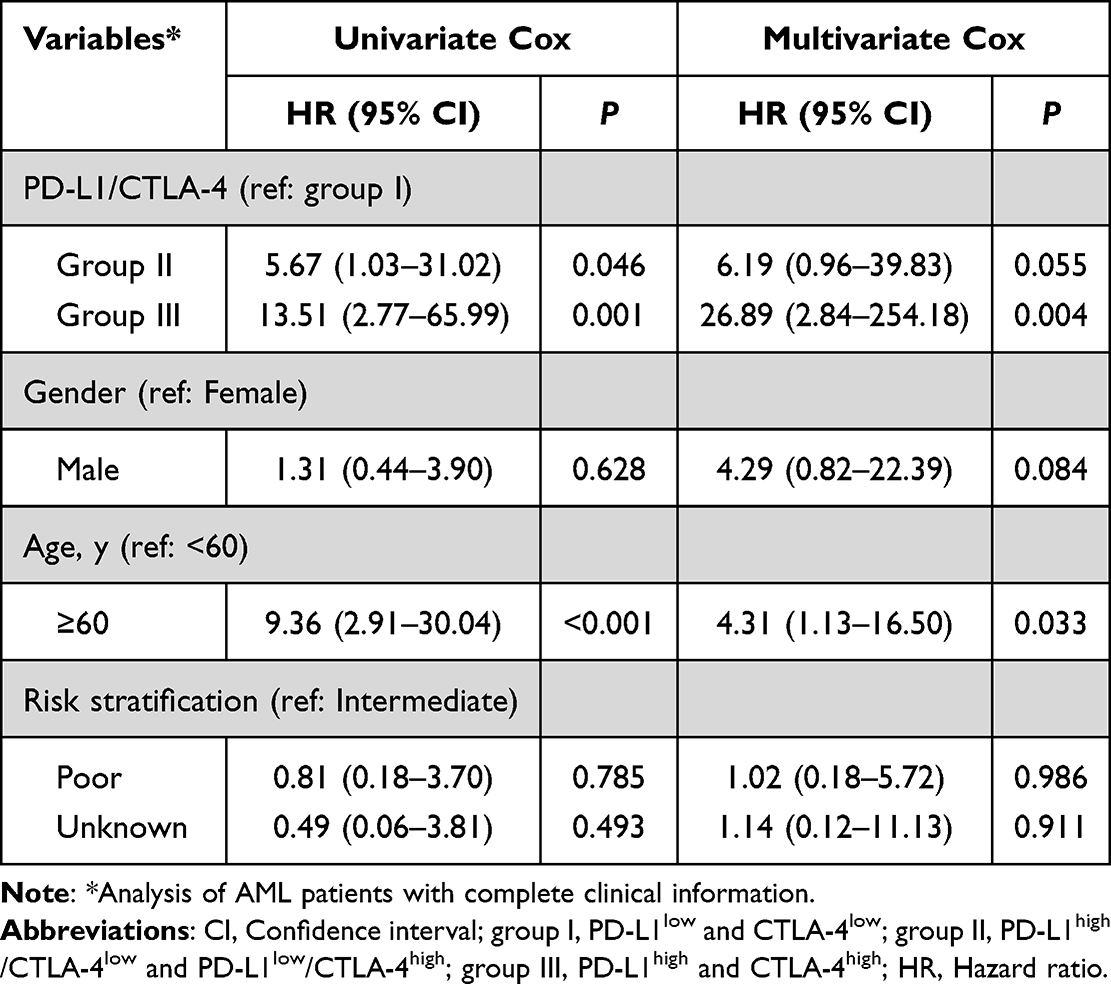 |
Table 1 Univariate and Multivariate Cox Regression Analysis in AML Patients Following allo-HSCT |
Construction of Risk Stratification for AML Patients Following allo-HSCT
As shown in Table 1, age and PD-L1/CTLA-4 are independent OS predictors for AML patients following allo-HSCT; thus, PD-L1, CTLA-4 and age were used to construct a nomogram model to visualize 5-year OS rates for AML patients (Figure 3A). Then, AML patients were divided into two subgroups according to the total risk score derived from the nomogram model, and the high-risk score was significantly associated with poor OS in AML patients (HR = 17.17, 95% CI: 2.22–132.60, P < 0.001; Figure 3B, left panel and Figure S2). However, ELN risk stratification cannot predict the OS of AML patients following allo-HSCT (P = 0.566; Figure 3B, right panel). The receiver operating characteristic curve (ROC) was used to further evaluate the performance of two different risk stratification in predicting prognosis, and we found that the risk stratification based on the nomogram model was better than ELN in predicting poor OS in patients following allo-HSCT [nomogram: area under the curve (AUC) = 0.82, 95% CI: 0.70–0.94, P = 0.002; ELN: AUC = 0.55, 95% CI: 0.36–0.75, P = 0.602] (Figure 3C).
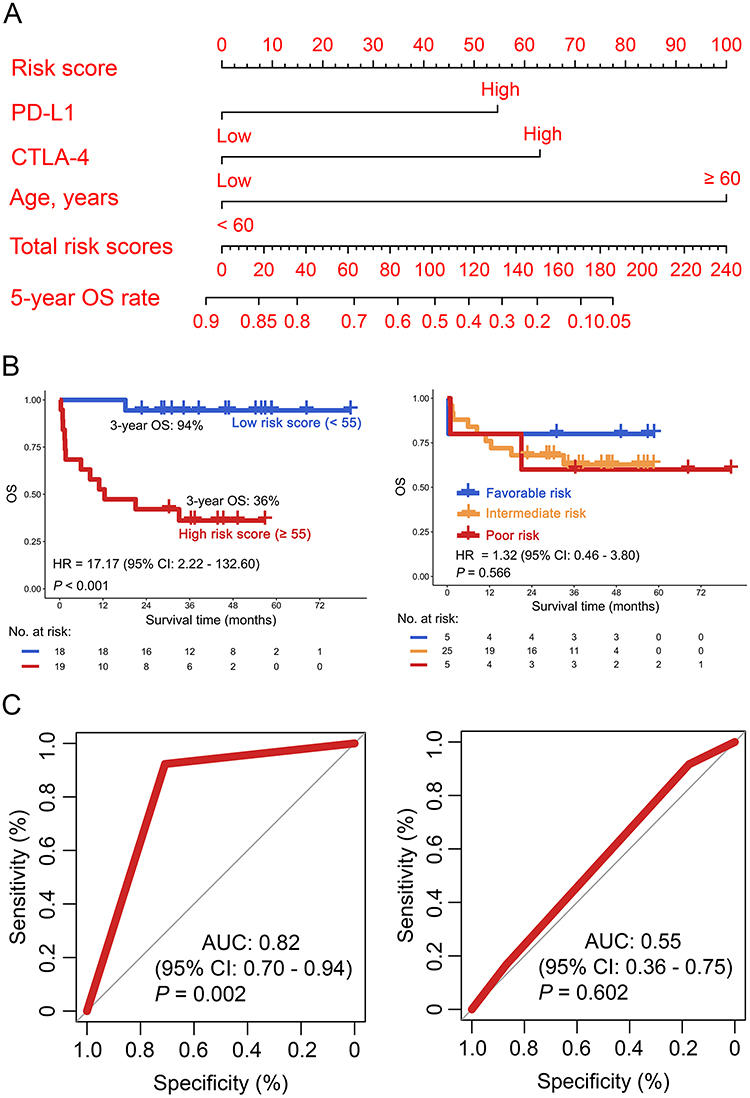 |
Figure 3 Risk stratification for AML receiving allo-HSCT. (A) The nomogram model was constructed by PD-L1, CTLA-4, and age. (B) Kaplan–Meier curves of new risk stratification based on risk score (left panel) and European Leukemia Net (ELN) risk stratification (right panel) were plotted. (C) The Receiver Operating Characteristic (ROC) curve was used for assessing the performance of new (left panel) and ELN risk stratification (right panel). |
Discussion
The intricate interplay between ICs, which are critical regulators of immune responses, underscores the importance of considering their combined expression patterns in the context of cancer and other immune-mediated diseases.23–25 Our previous studies have revealed that the simultaneous expression of multiple ICs, such as PD-1, PD-L1, PD-L2, CTLA-4, and LAG-3, was significantly associated with adverse clinical outcomes of AML patients.4,14,15,23 By analyzing the co-expression patterns of ICs, researchers have discovered that certain combinations of these molecules are more predictive of patient prognosis than individual markers.23 This finding suggests that the interplay between these immune regulators is complex and that a holistic approach, considering their collective influence, is necessary for accurate prognostication.24,25 In this study, high expression of PD-1, PD-L1, PD-L2, CTLA-4, and LAG-3, which play the role in the key immune suppression, was associated with poor OS in AML patients receiving allo-HSCT. Importantly, PD-L1/CTLA-4 was the best combination model for predicting poor OS in AML patients following allo-HSCT. This result is similar to our previous findings that increased co-expression of PD-1/CTLA-4 and PD-L2/CTLA-4 correlated with poor AML prognosis.4 Meanwhile, the different combination may indicate the special marker in subgroup of AML patients with allo-HSCT. Notably, previous reports have shown that AML patients with positive MRD have a higher recurrence rate and also predict poor OS,26–28 which might provide evidence that MRD assessment could help refining prognosis and support the adoption of post-transplant therapeutic modalities. Positive MRD after receiving allo-HSCT may lead to T cell exhaustion, and they might need other treatment options for consolidation, such as chemotherapy, ICIs or secondary transplantation.
In the context of AML transplantation, ICIs may offer several potential benefits.11–13 First, they may improve the graft-versus-leukemia (GVL) effect, where donor T cells attack residual AML cells, thereby reducing the risk of relapse. Second, ICIs may modulate the immune microenvironment, creating a more favorable landscape for the engraftment and function of donor immune cells. Lastly, ICIs may help restore immune homeostasis, reducing the risk of graft-versus-host disease (GVHD).11–13 However, the overall response rate of AML patients who relapse after allo-HSCT using ICI alone is limited.11 Therefore, combining two ICIs under allo-HSCT may improve the prognosis of AML patients, and further exploration with clinical trials is needed. This study may provide a reference that the co-expression pattern of PD-L1/CTLA-4 may be a potential immune biomarker for designing ICIs combined allo-HSCT for AML.
It is well known that AML is a complex and heterogeneous hematological malignancy and necessitates a tailored therapeutic approach tailored to individual patient characteristics. ELN risk stratification, achieved through a meticulous evaluation of cytogenetic profiles, molecular mutations, and clinical factors, allows for the categorization of patients into distinct risk groups.29,30 This stratification is crucial for guiding treatment regimens, prognostic assessment, and clinical trial design.30,31 However, the ELN-2022 and ELN-2017 systems have limited prognostic utility for AML patients following allo-HSCT,32 which was consistent with this study that ELN risk stratification cannot predict the OS of AML patients following allo-HSCT. It is thought that allo-HSCT can overcome adverse genetic alterations or chromosomal abnormalities.33 Notably, various studies have demonstrated the efficacy and utility of nomogram models in risk stratification across various medical specialties. For example, in oncology, nomograms have been developed to predict survival outcomes and guide treatment decisions for various cancer types, including T-cell lymphoma, esophageal cancer, and AML.21,34,35 Altogether, risk stratification based on nomogram models represents a significant advancement in medical practice. By providing accurate and personalized risk assessments, these models enable clinicians to make more informed decisions, optimize patient management, and ultimately improve patient outcomes.36 In this study, the nomogram model based on age and PD-L1/CTLA-4 was used to divide AML patients receiving allo-HSCT into high- and low-risk subgroups, which better evaluated the prognosis of AML patients than ELN risk stratification. However, the nomogram model and risk stratification lack validation from a large cohort and dataset from another clinical center.
Conclusion
High expression of PD-1, PD-L1, PD-L2, CTLA-4, and LAG-3 was associated with poor OS in AML patients receiving allo-HSCT, with PD-L1/CTLA-4 being the optimal combination to predict the clinical outcomes of patients, especially combined with MRD. Moreover, PD-L1/CTLA-4 might be potential immune biomarkers to supplement the risk stratification for AML patients treated with allo-HSCT.
Abbreviations
allo-HSCT, allogeneic hematopoietic stem cell transplantation; AML, Acute myeloid leukemia; BM, Bone marrow; CI, Confidence interval; CTLA-4, Cytotoxic T-lymphocyte associated protein 4; ELN, European Leukemia Network; HR, Hazard ratio; IC, Immune checkpoint; LAG-3, Lymphocyte activation gene-3; OS, Overall survival; PD-1, Programmed cell death 1; PD-L1, Programmed cell death 1 ligand 1; PD-L2, Programmed cell death 1 ligand 2; qRT-PCR, Quantitative real-time PCR; RMST, Restricted mean survival time.
Data Sharing Statement
All supporting data are included in the manuscript and supplemental files. Additional data are available upon reasonable request to the corresponding author.
Ethics Approval and Informed Consent
This study complies with the Declaration of Helsinki and was approved by the Ethics Committee of Guangzhou First People’s Hospital (No. K-2021-202-01). All participants provided written informed consent.
Funding
This study was supported by grants from the National Natural Science Foundation of China (Nos. 82300176, 82293632, 82293630, 82070152), Guangdong Natural Science Foundation (No. 2022A1515012478), Frontier Medical Technique Project of Guangzhou First People’s Hospital (No. QY-C02) and the Fundamental Research Funds for the Central Universities (No. 2024ZYGXZR029).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Gournay V, Vallet N, Peux V, et al. Immune landscape after allo-HSCT: TIGIT- and CD161-expressing CD4 T cells are associated with subsequent leukemia relapse. Blood. 2022;140(11):1305–1321. doi:10.1182/blood.2022015522
2. McDonald GB, Sandmaier BM, Mielcarek M, et al. Survival, nonrelapse mortality, and relapse-related mortality after allogeneic hematopoietic cell transplantation: comparing 2003–2007 versus 2013–2017 cohorts. Ann Intern Med. 2020;172(4):229–239. doi:10.7326/M19-2936
3. Deng DX, Ma XH, Wu ZH, et al. Pre-transplantation levels of lysine (K)-specific methyltransferase 2A (KMT2A) partial tandem duplications can predict relapse of acute myeloid leukemia patients following haploidentical donor hematopoietic stem cell transplantation. Blood Sci. 2024;6(4):e00207. doi:10.1097/BS9.0000000000000207
4. Chen C, Liang C, Wang S, et al. Expression patterns of immune checkpoints in acute myeloid leukemia. J Hematol Oncol. 2020;13(1):28. doi:10.1186/s13045-020-00853-x
5. Tan J, Chen S, Lu Y, et al. Higher PD-1 expression concurrent with exhausted CD8+ T cells in patients with de novo acute myeloid leukemia. Chin J Cancer Res. 2017;29(5):463–470. doi:10.21147/j.issn.1000-9604.2017.05.11
6. Liu L, Chang YJ, Xu LP, et al. T cell exhaustion characterized by compromised MHC class I and II restricted cytotoxic activity associates with acute B lymphoblastic leukemia relapse after allogeneic hematopoietic stem cell transplantation. Clin Immunol. 2018;190:32–40. doi:10.1016/j.clim.2018.02.009
7. Wang P, Zhang Y, Cai Q, et al. Optimal combination of immune checkpoint and senescence molecule predicts adverse outcomes in patients with acute myeloid leukemia. Ann Med. 2023;55(1):2201507. doi:10.1080/07853890.2023.2201507
8. Wang P, Cai Q, Peng X, et al. Increased co-expression of CTLA4/LAG3 predicted adverse clinical outcomes in patients with T-cell malignancies. Cell Investigation. 2025;1(1):100004. doi:10.1016/j.clnves.2024.100004
9. Li S, Shen Y, Dong C, et al. The molecular and immune microenvironmental landscape of brain metastases: implications for novel treatment options. Cell Investigation. 2025;1(1):100005. doi:10.1016/j.clnves.2024.100005
10. Wang J, Zhao Y, Liao P, et al. Immune checkpoint expression patterns on T cell subsets in light-chain amyloidosis: vista, PD-1, and TIGIT as potential therapeutic targets. Blood Sci. 2024;6(1):e00181. doi:10.1097/BS9.0000000000000181
11. Apostolova P, Kreutmair S, Toffalori C, et al. Phase II trial of hypomethylating agent combined with nivolumab for acute myeloid leukaemia relapse after allogeneic haematopoietic cell transplantation-immune signature correlates with response. Br J Haematol. 2023;203(2):264–281. doi:10.1111/bjh.19007
12. Garcia JS, Flamand Y, Penter L, et al. Ipilimumab plus decitabine for patients with MDS or AML in posttransplant or transplant-naïve settings. Blood. 2023;141(15):1884–1888. doi:10.1182/blood.2022017686
13. Saberian C, Abdel-Wahab N, Abudayyeh A, et al. Post-transplantation cyclophosphamide reduces the incidence of acute graft-versus-host disease in patients with acute myeloid leukemia/myelodysplastic syndromes who receive immune checkpoint inhibitors after allogeneic hematopoietic stem cell transplantation. J Immunother Cancer. 2021;9(2).
14. Pan S, Cai Q, Wei Y, et al. Increased co-expression of ICOS and PD-1 predicts poor overall survival in patients with acute myeloid leukemia. Immunobiology. 2024;229(3):152804. doi:10.1016/j.imbio.2024.152804
15. Chen C, Xu L, Gao R, et al. Transcriptome-based co-expression of BRD4 and PD-1/PD-L1 predicts poor overall survival in patients with acute myeloid leukemia. Front Pharmacol. 2020;11:582955. doi:10.3389/fphar.2020.582955
16. Núñez-Torrón Stock C, Jiménez Chillón C, Martín Moro F, et al. Patients with secondary acute myeloid leukemia undergoing allogeneic stem-cell transplant have inferior outcomes than de novo acute myeloid leukemia regardless minimal residual disease level by flow cytometry. Hematol Oncol. 2023;41(4):753–761. doi:10.1002/hon.3160
17. Heuser M, Freeman SD, Ossenkoppele GJ, et al. 2021 update on MRD in acute myeloid leukemia: a consensus document from the European LeukemiaNet MRD working party. Blood. 2021;138(26):2753–2767. doi:10.1182/blood.2021013626
18. Chen C, Liu SM, Chen Y, et al. Predictive value of TCR Vβ-Jβ profile for adjuvant gefitinib in EGFR mutant NSCLC from ADJUVANT-CTONG 1104 trial. JCI Insight. 2022;7(1):e152631. doi:10.1172/jci.insight.152631
19. Zeng C, Nie D, Wang X, et al. Combined targeting of GPX4 and BCR-ABL tyrosine kinase selectively compromises BCR-ABL+ leukemia stem cells. Mol Cancer. 2024;23(1):240. doi:10.1186/s12943-024-02162-0
20. Zheng X, Jin Y, Zhang C, et al. RNA-binding protein Roq modulates the Drosophila STING antiviral immune response. Cell Investigation. 2025;1(1):100002. doi:10.1016/j.clnves.2024.100002
21. Wang P, Chen Y, Long Q, et al. Increased coexpression of PD-L1 and TIM3/TIGIT is associated with poor overall survival of patients with esophageal squamous cell carcinoma. J Immunother Cancer. 2021;9(10):e002836. doi:10.1136/jitc-2021-002836
22. Chen C, Liu SM, Chen Y, et al. Poor prognosis of intra-tumoural TRBV6-6 variants in EGFR-mutant NSCLC: results from the ADJUVANT-CTONG1104 trial. Clin Transl Med. 2022;12(4):e775. doi:10.1002/ctm2.775
23. Chen C, Li Y. Predictive value of co-expression patterns of immune checkpoint molecules for clinical outcomes of hematological malignancies. Chin J Cancer Res. 2023;35(3):245–251. doi:10.1158/1538-7445.AM2023-LB245
24. Palermo B, Franzese O, Frisullo G, et al. CD28/PD1 co-expression: dual impact on CD8(+) T cells in peripheral blood and tumor tissue, and its significance in NSCLC patients’ survival and ICB response. J Exp Clin Cancer Res. 2023;42(1):287. doi:10.1186/s13046-023-02846-3
25. Ma J, Yan S, Zhao Y, et al. Blockade of PD-1 and LAG-3 expression on CD8+ T cells promotes the tumoricidal effects of CD8+ T cells. Front Immunol. 2023;14:1265255. doi:10.3389/fimmu.2023.1265255
26. Walter RB, Gyurkocza B, Storer BE, et al. Comparison of minimal residual disease as outcome predictor for AML patients in first complete remission undergoing myeloablative or nonmyeloablative allogeneic hematopoietic cell transplantation. Leukemia. 2015;29(1):137–144. doi:10.1038/leu.2014.173
27. Buckley SA, Wood BL, Othus M, et al. Minimal residual disease prior to allogeneic hematopoietic cell transplantation in acute myeloid leukemia: a meta-analysis. Haematologica. 2017;102(5):865–873. doi:10.3324/haematol.2016.159343
28. Araki D, Wood BL, Othus M, et al. Allogeneic hematopoietic cell transplantation for acute myeloid leukemia: time to move toward a minimal residual disease-based definition of complete remission? J Clin Oncol. 2016;34(4):329–336. doi:10.1200/JCO.2015.63.3826
29. Döhner H, Estey EH, Amadori S, et al. Diagnosis and management of acute myeloid leukemia in adults: recommendations from an international expert panel, on behalf of the European LeukemiaNet. Blood. 2010;115(3):453–474. doi:10.1182/blood-2009-07-235358
30. Papaemmanuil E, Gerstung M, Bullinger L, et al. Genomic classification and prognosis in acute myeloid leukemia. N Engl J Med. 2016;374(23):2209–2221. doi:10.1056/NEJMoa1516192
31. Grimwade D, Hills RK, Moorman AV, et al. Refinement of cytogenetic classification in acute myeloid leukemia: determination of prognostic significance of rare recurring chromosomal abnormalities among 5876 younger adult patients treated in the United Kingdom Medical Research Council trials. Blood. 2010;116(3):354–365. doi:10.1182/blood-2009-11-254441
32. Zhang H, Zheng X, Guo W, et al. Outcomes of acute myeloid leukemia patients undergoing allogeneic hematopoietic stem cell transplantation: validation, comparison and improvement of 2022 ELN genetic risk system. Exp Hematol Oncol. 2024;13(1):16. doi:10.1186/s40164-024-00487-6
33. Wang H, Chu TT, Han SY, et al. FLT3-ITD and CEBPA mutations predict prognosis in acute myelogenous leukemia irrespective of hematopoietic stem cell transplantation. Biol Blood Marrow Transplant. 2019;25(5):941–948. doi:10.1016/j.bbmt.2018.11.031
34. Chen C, Huang L, Chen Z, et al. Higher 13-gene-estimated TMB detected from plasma ctDNA is associated with worse outcome for T-cell lymphoma patients. Adv Biol. 2023;7:e2300042. doi:10.1002/adbi.202300042
35. Yu X, Chen C, Hu Y, et al. High expression of LOC541471, GDAP1, SOD1, and STK25 is associated with poor overall survival of patients with acute myeloid leukemia. Cancer Med. 2023;12(7):9055–9067. doi:10.1002/cam4.5644
36. Yang Y, Zhang YJ, Zhu Y, et al. Prognostic nomogram for overall survival in previously untreated patients with extranodal NK/T-cell lymphoma, nasal-type: a multicenter study. Leukemia. 2015;29(7):1571–1577. doi:10.1038/leu.2015.44
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
A Novel Risk Score (P-score) Based on a Three-Gene Signature, for Estimating the Risk of Prostate Cancer-Specific Mortality
Söderdahl F, Xu LD, Bring J, Häggman M
Research and Reports in Urology 2022, 14:203-217
Published Date: 11 May 2022
Serum NOX4 as a Promising Prognostic Biomarker in Association with 90-Day Outcome of Severe Traumatic Brain Injury
Jiang F, Chen Z, Hu J, Liu Q
International Journal of General Medicine 2022, 15:5307-5317
Published Date: 30 May 2022
Identification of KRBA1 as a Potential Prognostic Biomarker Associated with Immune Infiltration and m6A Modification in Hepatocellular Carcinoma
Liu Y, Fu B, Yu Z, Song G, Zeng H, Gong Y, Ding Y, Huang D
Journal of Hepatocellular Carcinoma 2022, 9:497-516
Published Date: 31 May 2022
Expression, Clinical Significance, Immune Infiltration, and Regulation Network of miR-3940-5p in Lung Adenocarcinoma Based on Bioinformatic Analysis and Experimental Validation
Lin Z, Huang W, Xie Z, Yi Y, Li Z
International Journal of General Medicine 2022, 15:6451-6464
Published Date: 6 August 2022
NUP62CL as an Immunological and Prognostic Biomarker of Oral Squamous Cell Carcinoma
Yu X, Xu L, Zhou Y, Zhou X, Yang L, Zhou Y
Journal of Inflammation Research 2023, 16:3799-3809
Published Date: 29 August 2023