Back to Journals » Neuropsychiatric Disease and Treatment » Volume 21
Efficacy and Safety of Remote Ischemic Conditioning for Depression Insufficiently Responsive to Antidepressant: A Randomized Controlled Trial
Authors Wang J, Shuai Y ![]() , Ren M, Li N, Li X, Li W, Jiang B, Wang L, Huang L
, Ren M, Li N, Li X, Li W, Jiang B, Wang L, Huang L ![]() , Ji X, Wang Z
, Ji X, Wang Z ![]()
Received 2 June 2025
Accepted for publication 18 September 2025
Published 8 October 2025 Volume 2025:21 Pages 2279—2291
DOI https://doi.org/10.2147/NDT.S536528
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Yu-Ping Ning
Jun Wang,1,* Yu Shuai,1,* Ming Ren,2,* Ningning Li,3 Xujuan Li,4 Wenfei Li,5 Binxun Jiang,4 Linlin Wang,4 Leping Huang,3 Xunming Ji,6,7 Zuowei Wang3,8
1Division of Mood Disorders, Shanghai Yangpu Mental Health Center, Shanghai, 200093, People’s Republic of China; 2Department of Neurology, Shanghai Blue Cross Brain Hospital, Tongji University, Shanghai, 200086, People’s Republic of China; 3Division of Mood Disorders, Shanghai Hongkou Mental Health Center, Shanghai, 200083, People’s Republic of China; 4Division of Mood Disorders, Shulan (Hangzhou) Hospital Affiliated to Zhejiang Shuren University Shulan International Medical College, Hangzhou, 310022, People’s Republic of China; 5Division of Mood Disorders, Anhui Mental Health Center, Hefei. Anhui, 230022, People’s Republic of China; 6Department of Neurosurgery, Xuanwu Hospital, Capital Medical University, Beijing, 100053, People’s Republic of China; 7Beijing Key Laboratory of Hypoxic Conditioning Translational Medicine, Xuanwu Hospital, Capital Medical University, Beijing, 100053, People’s Republic of China; 8Clinical Research Center for Mental Health, School of Medicine, Shanghai University, Shanghai, 200083, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zuowei Wang, Division of Mood Disorders, Shanghai Hongkou Mental Health Center, Shanghai, 200083, People’s Republic of China, Email [email protected] Xunming Ji, Department of Neurosurgery, Xuanwu Hospital, Capital Medical University, Beijing, 100053, People’s Republic of China, Email [email protected]
Background: Physical therapies are recommended for individuals who are insufficiently responsive to pharmacotherapy and psychotherapy. But most physical therapy needs to be done in a hospital, so finding a physical therapy that can be done at home is very meaningful. This study intends to explore the efficacy and safety of remote ischemic preconditioning (RIPC) as an add-on therapy for depression.
Methods: A total of 60 major depressive disorder patients with inadequate response to escitalopram in this study were randomly assigned to sham or active RIPC group. The clinical symptoms, side-effects and physical examination were evaluated and recorded once every 2 weeks until the end of 8th week. The clinical symptoms were evaluated using the 16-item Quick Inventory of Depressive Symptomatology (Self-Report) (QIDS-16-SR) and the Generalized Anxiety Disorder 7-item scale (GAD-7). Side-effects included skin ecchymosis, risk of manic episodes, and RIPC-related serious adverse events. Physical examination included heart rate and blood pressure.
Results: No significant difference in QIDS-16-SR and GAD-7 scores between the two groups was found at baseline, week 2, week 4, week 6 and week 8 (P > 0.05). There were no significant differences in heart rate and blood pressure (including systolic and diastolic blood pressure) at any time point between the active group and the sham group (P > 0.05). There were no manic or hypomanic episodes associated with the study.
Conclusion: For depression patients with poor response to antidepressant therapy, the efficacy of RIPC as adjuvant therapy was not observed in this study. In general, RIPC adjuvant therapy is relatively safe, and has no significant effect on cardiovascular system, nor does it increase the risk of manic episode.
Keywords: depression patient, efficacy, physical therapy, remote ischemic, safety
Introduction
Major depressive disorder (MDD), characterized by its high incidence rates, relapsing nature, and increased suicide risk, puts great strain on individuals, families, and societies, making it a prominent global medical and social issue. The World Health Organization (WHO) stated that around 350 million people worldwide were affected by MDD, which was roughly equivalent to one in every twenty people having had or being afflicted with the disorder at the time of the report.1,2 Chinese epidemiological survey data showed that the lifetime prevalence rate for depressive disorders in China was 6.8%, and that for MDD was 3.4%.3 Nevertheless, a large number of MDD patients, especially in low- and lower-middle-income countries, did not get proper treatment.4,5 Consequently, depression rose to be the second leading cause of the global disease burden, coming after cardiovascular diseases, and was expected to become the main cause of disease burden and disability by 2030.1–3
Even though a great many effective treatments have been identified, quite a large number of patients suffering from depression show inadequate response or tolerance to antidepressants and/or psychotherapy.6 The Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study showed that more than half of depression patients did not respond to the first-line therapeutic methods and about one-third failed to attain long-lasting clinical remission after a four-step sequential treatment plan.7–9 A recent systematic review and network meta-analysis covering 522 trials of 21 antidepressants with 116,477 adult participants found out that all antidepressants were better than placebos in adults with Major Depressive Disorder (MDD), but the overall effect size was rather small (~0.30).10 Furthermore, even though the pharmacological treatment of depression had grown extensively since the 1970s, epidemiological data indicated that there was no decrease in the prevalence rates of MDD.11 The difference between the availability of treatment and the actual treatment rates implied that there were still considerable obstacles to getting depression treatment.12 In order to reduce the prevalence of MDD, it was crucial to find effective alternative treatments, close the treatment gaps, make it easier to get timely interventions, guarantee high-quality therapeutic services, and do away with waiting times for care.11
Physiotherapeutic methods like electroconvulsive therapy (ECT) and repetitive transcranial magnetic stimulation (rTMS) are suggested for patients showing poor reactions to drug therapy and/or psychosocial interventions.13,14 Even though these approaches are the most effective treatment plan for people with treatment-resistant depression (TRD) and might be seen as a first-choice option in some acute situations, the use of ECT is restricted because of its related negative effects, high costs, and bureaucratic difficulties.15,16 rTMS, a non-invasive technique that stimulates specific areas of the cortex, has moderate effectiveness and few safety issues for patients with major depressive disorder (MDD) who have not responded to or cannot tolerate antidepressant medications during both acute attacks and maintenance periods.17 Based on the clinical guidelines of the Canadian Network for Mood and Anxiety Treatments (CANMAT) for dealing with adult MDD, patients who do not show early progress after 2–4 weeks of initial first- line antidepressant treatment were advised to get additional rTMS before switching to another antidepressant or adding more drug therapies.13,14 Just like ECT, rTMS needs advanced equipment and special setups and its application demands skilled therapists.18 The possibility of side effects like headaches and the danger of causing epilepsy reduces the acceptability of rTMS as a treatment alternative.
As a result, it was essential to pursue methodologies that were more user-friendly and economical and had a narrower range of both immediate and long-term negative side effects. Remote ischemic preconditioning (RIPC) seemed potentially to meet these requirements and thus its effectiveness and safety in treating depression became a highly interesting area for research.18 Remote Ischemic Preconditioning (RIPC) is a protective strategy that induces ischemic tolerance in distant vital organs (such as the heart, brain, and kidneys) by performing brief, non-lethal ischemia-reperfusion treatments on tissues or limbs far from the target organ. It has currently been applied as an adjuvant therapy for diseases including coronary heart disease, acute myocardial infarction, and ischemic stroke.19–21 For RIPC entailed inducing short-term ischemic incidents that could activate numerous built-in protective reactions to lessen ischemic harm and improve the malfunction of far-away organs caused by a sudden drop in blood flow.22 It might also have neuroprotective impacts via various reasonable ways like regulating neural routes and signal transmission, restraining inflammatory and immune reactions, decreasing oxidative stress and excessive calcium levels, moderating glutamate-induced toxicity, and stopping cell death.22–27 Previous studies have shown that the neuroprotective ability of RIPC might reduce the occurrence of different neuropsychiatric and neurological problems such as cognitive decline, dementia, insomnia, and depression among patients with intracranial arterial stenosis (ICAS) and carotid artery stenosis (CAS).28–32
We know that the pathogenesis of depression is closely related to factors such as neurotransmitter imbalance and immune inflammatory responses.33,34 Thus, it can be seen that the brain protection mechanism of RIPC matches the pathogenesis of depression, and may combine with antidepressants and augment their effects to alleviate depressive symptoms.35–37 Our previous study, a single-arm, open-label trial, had shown the safety and acceptability of RIPC as an additional treatment for Major Depressive Disorder (MDD).18 The aim of the present research was to carry out a multi-center randomized controlled trial to assess the therapeutic effectiveness and safety of RIPC in people with MDD who had not responded well enough to standard antidepressant treatment and the intention was to offer initial evidence supporting RIPC as a practical, safe, and effective intervention for treatment- resistant depression, so as to make way for a later large-scale, randomized, double-blind, sham-controlled study to strictly test this hypothesis.
Materials and Methods
Study Design
This was a randomized, sham-controlled, double-blind and multicenter study registered at Chinese Clinical Trial Registry (http://www.chictr.org.cn/,identifier: ChiCTR2000029729, date of registration: February 10, 2020). This study used a two-stage design consisting of run-in period and randomized intervention phase. In the run-in period, eligible patients received escitalopram monotherapy as usual as in clinical practice for 4 weeks. In the randomized intervention phase, the patients who were with inadequate response were randomly assigned to active RIPC or sham with their ongoing escitalopram for 8 weeks. The overview of the study design is presented in Figure 1.
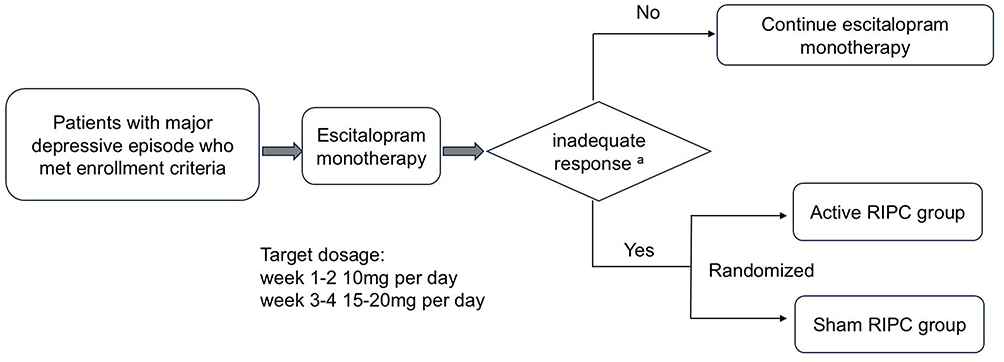 |
Figure 1 An overview of study design. Abbreviation: RIPC, remote ischemic preconditioning. Notes: a < 50% reduction in QIDS-16-SR score from baseline or a total score ≥16 points at the end of week 4. |
Study Setting and Personnel
The research was carried out in four different places: Shanghai Hongkou Mental Health Centre, Shanghai Yangpu Mental Health Centre, Shulan (Hangzhou) Hospital which belongs to Zhejiang Shuren University, and Anhui Mental Health Centre. Shanghai Hongkou Mental Health Centre acted as the coordinating place being in charge of overseeing the training of all research staff and the conduct of the trial. The study’s plan received ethical approval from the Institutional Review Board (IRB) of Shanghai Hongkou Mental Health Center (protocol approval number: 2019D04). Subsequently, the IRBs at other participating sites reviewed and approved the protocol from the coordinating center. Prior to initiating any study-related procedures, written informed consent was obtained from each participant.
Inclusion Criteria
Subjects could be included in the initial stage of the study if they met the following criteria: (1) were aged between 18 and 65 years old; (2) met the diagnostic standards for a major depressive episode (MDE) as specified in the International Classification of Diseases and Related Health Problems, Tenth Edition (ICD-10); (3) scored no less than 16 on the 16-item Quick Inventory of Depressive Symptomatology (Self-Report) (QIDS-16-SR) during the screening visit; (4) had not taken any psychotropic drugs in past one month; (5) had an education level equal to or higher than middle school; and (6) had sufficient audiovisual and cognitive abilities to understand and sign the informed consent form.
Exclusion Criteria
Subjects were not eligible to be included in the study if they fulfilled any of the following exclusion criteria: (1) having a previous medical history of (hypo) manic episodes or other mental health conditions like schizophrenia, bipolar disorder, schizoaffective disorder, substance use disorder, neurodegenerative diseases, and personality disorders; (2) women who were pregnant or breastfeeding, or were planning for pregnancy; (3) had a high risk of suicide (QIDS-16-SR item 12 score ≥3 or judged by a study psychiatrist); (4) previously not response or intolerant to escitalopram; (5) had ECT or rTMS in past 6 months; (6) had psychotherapy such as cognitive behavioral therapy, psychoanalysis and other forms of psychotherapeutic interventions in past 2 months; (7) participated in other clinical trials in past 3 months.
Methods of Study
Initial Treatment of Escitalopram in the Run-In Period
Subjects meeting the inclusion criteria and lacking any exclusion criteria were started on escitalopram alone at 10 mg per day for two weeks. Those showing tolerance to this dose became eligible for a dose increase to 15–20mg daily starting from the third or fourth week. Participants who could not tolerate at least 10 mg of escitalopram daily were withdrawn from the study and referred for standard clinical treatment. For patients who met the adequate response criterion, ie, ≥50% reduction in QIDS-16-SR from baseline or a total score of QIDS-16-SR <16 points at the end of week 4, they wound end the study and continue escitalopram monotherapy at the same dose and move to routine clinical care.
Randomization and Blinding
Patients with an inadequate response to escitalopram (ie, a < 50% reduction in QIDS-16-SR score from baseline or a total score ≥16 points at the end of week 4) entered the RIPC-assisted therapeutic intervention stage. Simple random grouping was conducted using a computer-generated random number table Patients who met the inclusion criteria were assigned to the true RIPC group (experimental group) and the sham RIPC group (control group) in a 1:1 ratio. The random sequence was generated by the statistician, and the grouping results were sealed in an opaque envelope, which was opened and administered by the research assistant. As a double-blinded study, both participants and members of the study teams blinded to group assignment. The clinical research coordinators (CRCs) from each site were responsible independently for managing and distributing the random numbers and the ischemic preconditioning devices. The ischemic preconditioning (IPC) devices were pre-set to the fixed treatment pressures for active RIPC or sham RIPC treatments. Once a patient pressed the start button of an IPC device he/she received, the pressure of cuffs on both upper arms would rise automatically to 200 mmHg or 60 mmHg. Researchers responsible for clinical symptom assessment did not participate in grouping or intervention implementation and were unaware of the patients’ group assignments (assessors were blinded) to reduce assessment bias.
Intervention in Randomized Phase
The RIPC was provided with an electric autocontrol IPC device (model IPC-906) designed and manufactured by Beijing Renqiao Cardio-cerebrovascular Disease Prevention Research Nantong Co., Ltd, China (patent number ZL201410834305.2, China). The RIPC was administered by patients at home. The data were spontaneously uploaded to the terminal of the device for monitoring. Patients could consult the CRCs by phone if they had any question or concern about the use of the device.
The location of the pressure cuff for the ischemic preconditioning was fixed on both upper arms, which was similar to the position of blood pressure measurement. The treatment mode was twice a day (once in the morning and once in the afternoon or evening at the patient’s convenient time) for at least 5 days a week. When patients pressed the start button on a device, the treatment pressure was automatically on for 5 minutes, then off for 5 minutes, and automatically stopped after 5 cycles. The treatment pressure was 200 mmHg for the active group and 60 mmHg for the sham group.
Research staff monitored the use of RIPC equipment by patients through an online management system provided by the manufacturer of the IPC device. A mobile electronic database platform recorded the use of the RIPC device. If the IPC use data indicated that a patient did not use it one day apart, a coordinator would alert the patient by phone or text message to ensure that the patient followed the research protocol.
During the randomized treatment phase, patients continued on-going dose of escitalopram. The non-benzodiazepine or short half-life benzodiazepine sedative hypnotic drugs for insomnia (such as lorazepam, zopiclone, zolpidem, estazolam, alprazolam, etc.) were permitted as well as medications for adverse reactions related to study or physical diseases. However, concomitant psychotherapy, use of antipsychotics and other psychotropic drugs or interventional therapy (ECT, rTMS, etc.) were prohibited.
Diagnosis and Assessments
Demographic and clinical data at baseline and efficacy and safety data during the study period were collected through clinical research forms that included demographic information, physical disease history, diagnosis of mental disorder(s), inclusion and exclusion criteria, treatment records, and reasons for study termination. The Chinese version of Mini-International Neuropsychiatric Interview (M.I.N.I.) was used to ascertain the diagnosis of a major depressive episode according to the ICD-10 criteria. The QIDS-16-SR scale covers the core symptoms of depressive episodes (such as low mood, reduced interest, sleep disorders, changes in appetite, fatigue, self-blame, etc.) and can comprehensively reflect the multi-dimensional manifestations of depression. Previous studies have shown that the correlation among its items is relatively high, with Cronbach’s α coefficient typically ranging from 0.80 to 0.90, and the test-retest correlation coefficient is usually between 0.70 and 0.85. The correlation coefficients with other commonly used depression assessment tools (such as the Hamilton Depression Scale (HAMD), the Beck Self-Rating Depression Scale (BDI), PHQ-9, etc.) are usually between 0.60 and 0.85.38–40 Because of its high reliability and validity, the QIDS-16-SR was used to evaluate the severity of depressive symptoms. The Generalized Anxiety Disorder 7-item (GAD-7) and Altman Self-Rating Mania Scale (ASRM) were used to evaluate the severity of anxiety and manic symptoms, respectively.
During the run-in period, the QIDS-16-SR were self-rated at screening, at the end of week 2 and at the end of week 4. In the randomized intervention phase, QIDS-16-SR, GAD-7 and ASRM were completed at the randomization, and at the week 2, week 4, week 6 and week 8 after randomization. If a patient had suspected an adverse reaction(s) related to drugs or RIPC, an additional unplanned follow-up visit(s) would be provided as appropriate. A follow up visit was provided when the study was terminated for various reasons. Adverse event (AE) and serious adverse event (SAE) forms were used to monitor treatment-related adverse reactions.
Sample Size
The sample size for this study was calculated with regard to the comparison of sample rates between two groups. The starting hypothesis is a 25% response rate in the control group in accordance with rTMS for TRD and STAR*D trials, and 60% in the study group based on the pilot study.18,41,42 Assuming a 5% (bilateral) type I error and a power of 80%, a total of 60 subjects is required (calculated according to the following formula, p1 = 0.60 and p2 = 0.25). Sixty participants will be recruited and randomly assigned in a 1:1 ratio to the two experimental groups, with 30 subjects in each group.
Statistical Analysis
The dataset was subjected to statistical analysis by means of SPSS version 25.0. For demographic and clinical characteristics at baseline, continuous variables (eg, age, scale score, RIPC related to heart rate and blood pressure.) were described using means ± standard deviations and categorical variables (eg, gender, education level, etc.) using frequencies and percentages and analyzed with chi-square test or independent sample T-test. The primary outcome QIDS-16-SR scores and secondary outcome GAD-7 scores of the two groups at each time node were compared by Paired sample t-test (Intra-group) or independent sample t-test (Inter-group). The secondary outcomes, clinical remission rates (QIDS-16-SR total score ≤ 5) and dropout rates were conducted according to the intent-to-treat (ITT) and per-protocol (PP) principle. The clinical remission rates and dropout rates were compared by chi-squared test. The safety measures, skin ecchymosis and occurrence of (hypo) manic symptoms (scored ≥5 points in ASRM at any follow-up visit) were used with descriptive analysis. All statistical tests were two-sided at α level of 0.05. Because of explorative nature of the study, no adjustment for multiple comparisons was performed.
Results
Demographics and Clinical Correlates
Of 328 patients screened, 259 patients received escitalopram monotherapy 10–20mg per day for 4 weeks. There were 199 patients did not enter the following RIPC randomized intervention phase. Of the 199 cases who were not randomized, 122 cases met the adequate response criterion, 39 cases could not tolerate the minimum dose of escitalopram 10 mg per day, and 38 cases withdrew from the study due to concerns about the efficacy and adverse reactions of RIPC adjuvant therapy.
Of the 60 patients were randomized, 32 were in the active RIPC group and 28 were in the sham RIPC group. Twenty-eight patients in active group and twenty-three patients in the sham group completed the 8-week randomized phase. The flow chat of participants’ disposition was presented in Figure 2.
 |
Figure 2 The flow chat of research participants. Abbreviations: MDD: Major depressive disorder; RIPC, remote ischemic preconditioning; ASRM: Altman Self-Rating Mania Scale. |
Table 1 shows demographic traits and historical associations, and the analysis showed that there were no statistically noteworthy distinctions between the two groups regarding demographic factors, historical connections, or the severity of depressive, anxious, and manic/hypomanic symptoms at the time of randomization, as is clearly stated in Table 1.
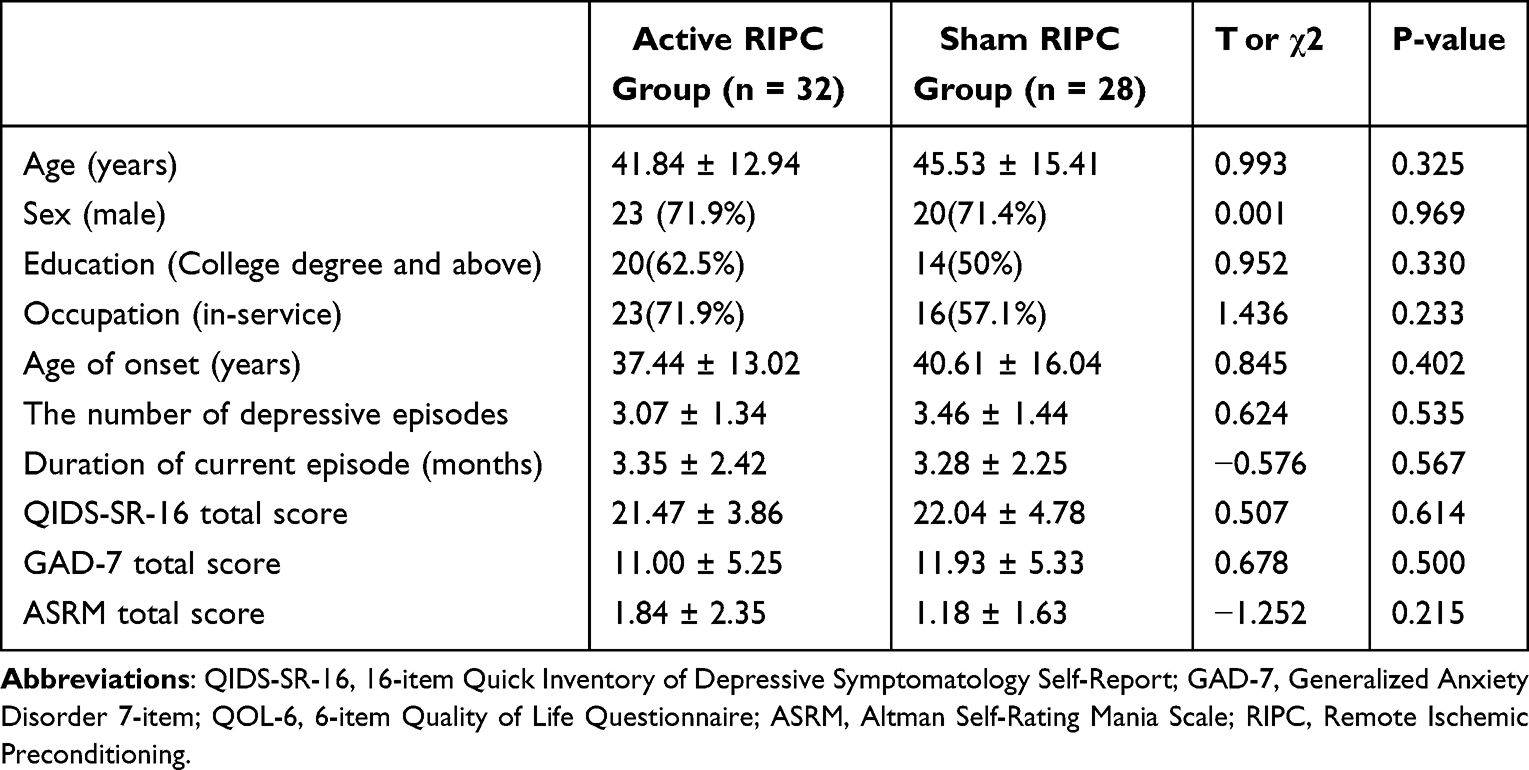 |
Table 1 Comparison of Baseline Demographic and Clinical Characteristics Between Study Group and Control Group |
Primary Outcome
The QIDS-16-SR scores at each time node between the two groups were not significantly different (Table 2). However, the QIDS-16-SR scores between the two groups at the end of week 8 had a trend lower the active RIPC treatment over the sham with a p value of 0.14 (Table 2). The effect size suggested that the mean difference between follow-up and baseline score changes between the two groups was not significant (d < 0.5) (Table 2).
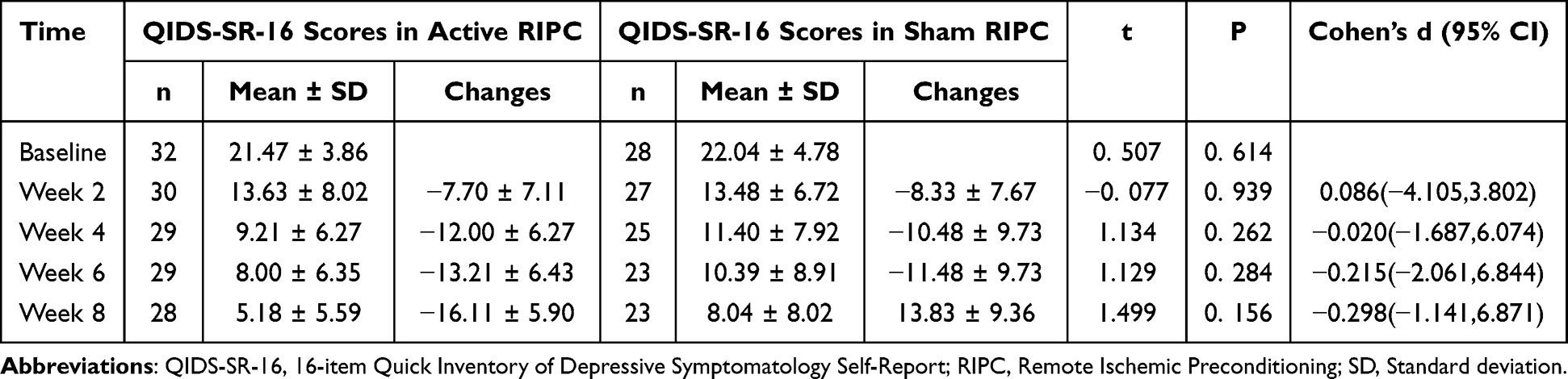 |
Table 2 Comparison of QIDS-SR-16 Scores Between the Two Groups at Different Time Nodes |
Secondary Outcomes
Remission Rates and Dropout Rates
At the end of eight-week RIPC intervention, there were 18 patients in the active RIPC group and 12 patients in the sham group whose QIDS-16-SR total scores were ≤5. The ITT analysis showed that the remission rate was 56.3% (18/32) in the active RIPC group and 42.9% (12/28) in the sham RIPC group, with no significant difference between the two groups (X2 = 1.070, P > 0.05) (Figure 3). The PP analysis showed that the remission rate was 64.3% (18/28) in the active RIPC group and 52.2% (12/23) in the sham RIPC group, with no significant difference between the two groups (X2 = 0.765, P > 0.05) (Figure 3). The dropout rates were 12.5% (4/32) in the active RIPC group and 17.9% (5/28) in the sham RIPC group, with no significant difference between the two groups (X2 = 0.336, P > 0.05) (Figure 3).
 |
Figure 3 The remission rates and dropout rates. Abbreviations: ITT, Intent-to-treat; PP, per-protocol. |
Change in Anxiety Symptoms
The GAD-7 scores at each time point between the two groups were not significantly different (Table 3). However, the GAD-7scores between the two groups at the end of week 8 had a trend lower the active RIPC treatment over the sham with a p value of 0.053 (Table 3). The effect size suggested that the mean difference between follow-up and baseline score changes between the two groups was not significant (d < 0.6) (Table 3).
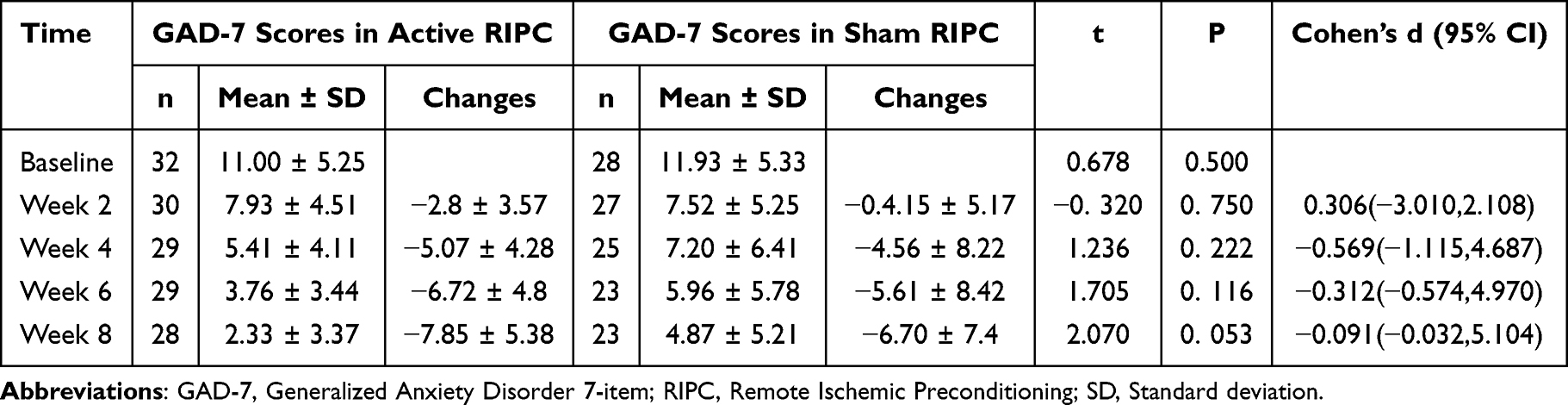 |
Table 3 Comparison of GAD-7 Scores Between the Two Groups at Different Time Nodes |
Safety Outcomes
During the 8-week intervention, all patients in both groups did not experience serious adverse reactions. Three patients in the active RIPC group had scattered skin ecchymosis compressed by RIPC cuffs within 2 weeks, among which two patients withdrew from the study and one patient continued to complete the study. The skin ecchymosis disappeared in all 3 patients within 1 week. No skin ecchymosis was reported in the sham RIPC group. In the active RIPC group, two patients dropped out of the study at the second week of follow-up because of skin ecchymosis, one patient dropped out of the study at the fourth week of follow-up due to a positive life event that resulted in a score of 5 on the ASRM scale, one patient dropped out of the study after the sixth week of follow-up because he wanted to participate in psychotherapy and rated the ASRM scale as a 6. In the sham RIPC group, one patient dropped out of the study at the second week of follow-up due to a positive life event that resulted in a score of 6 on the ASRM scale, two patients dropped out of the study at the fourth week of follow-up because they were receiving psychotherapy, two patients dropped out of the study at the sixth week of follow-up due to a 6 score on the ASRM scale after drinking alcohol.
The heart rate and blood pressure (including systolic and diastolic blood pressure) at any time node between the two groups were not significantly different (P > 0.05, see Tables 4 and 5).
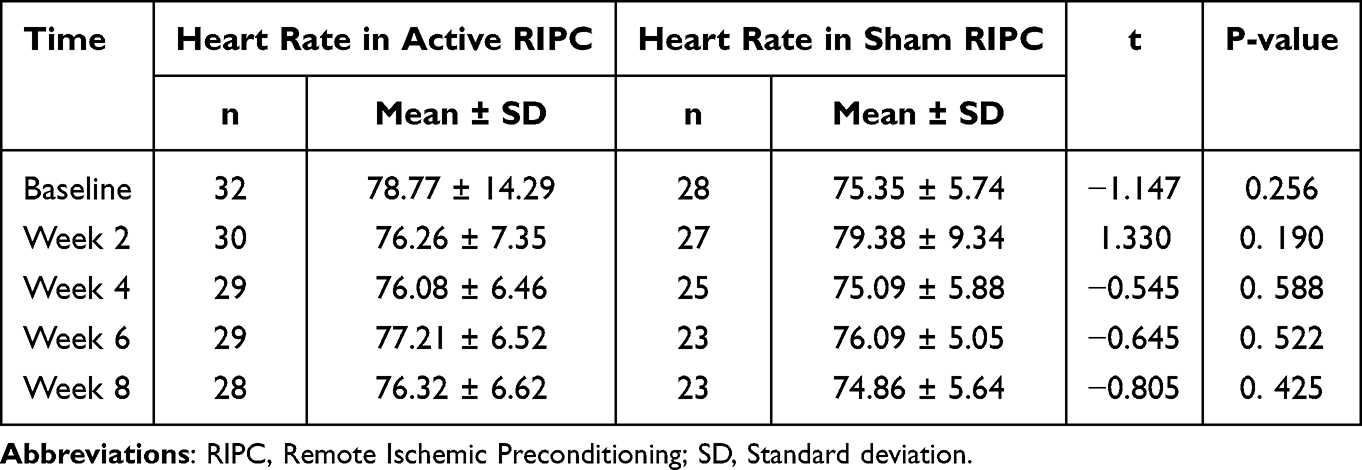 |
Table 4 Comparison of Heart Rate Between the Two Groups at Different Time Nodes |
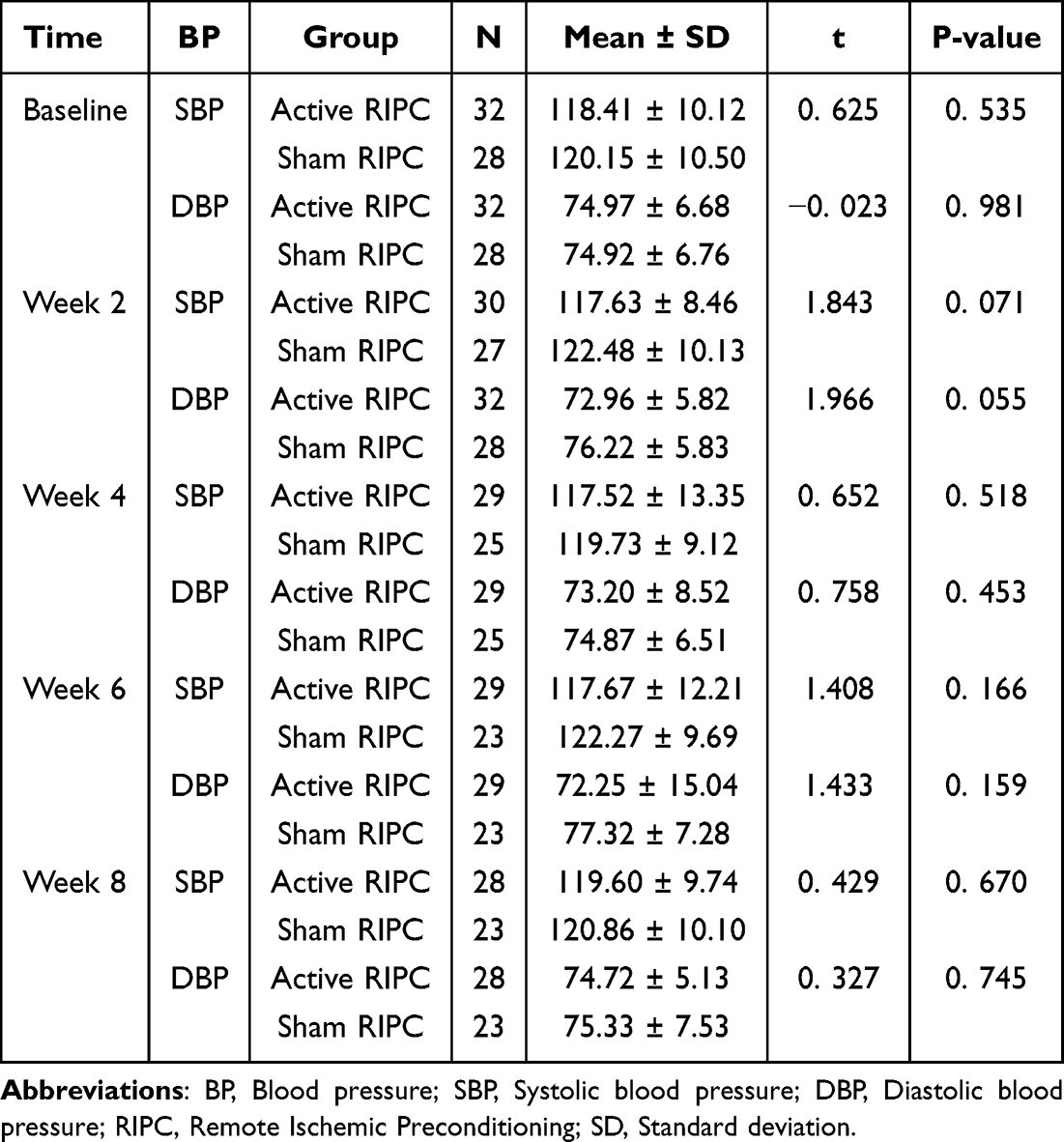 |
Table 5 Comparison of Blood Pressure Between the Two Groups at Different Time Nodes |
Discussion
Main Findings
To date to our knowledge, this was the first randomized, double-blind, sham controlled trial to explore the efficacy and safety of RIPC in patients who were diagnosed with MDD and did not have adequate response to the initial treatment with escitalopram. We found that RIPC was well tolerated Except of depressive symptom, we also investigate the influence of anxiety symptoms, quality of life, and the risk of treatment-emergent mania. The principal findings of the current study were that RIPC adjuvant therapy does not increase significantly the efficacy for patients with depression who do not respond well to escitalopram monotherapy. In addition, the improvement of anxiety symptoms and quality of life, and remission rate in patients with RIPC adjunctive therapy are not better than that in patients without RIPC adjunctive therapy. While RIPC adjuvant therapy is generally relatively safe and tolerable.
Although the exact mechanism of RIPC has not been fully elucidated, previous studies have suggested that it may involve the following aspects: (1) RIPC can trigger a series of endogenous protective mechanisms, including anti-oxidative stress, anti-inflammatory response, anti-apoptosis, etc. These protective mechanisms can alleviate tissue damage caused by ischemia-reperfusion; (2) RIPC can activate a variety of signal transduction pathways, such as protein kinase C (PKC), mitogen-activated protein kinase (MAPK), etc. Activation of these pathways can promote cell survival and adaptive responses, thereby mitigating ischemic injury; and (3) RIPC can induce adaptive responses in cells, such as increasing vascular permeability and promoting the formation of collateral circulation. These adaptive responses can improve tissue tolerance and resistance to combat ischemic injury.43–45 At present, RIPC has been confirmed to have a certain protective effect in heart disease, stroke, organ transplantation and other fields.46–48 Baranova et al performed RIPC on depressed rats, and the results showed that RIPC completely prevented depression-like behavior and caused excessive activation of the pituitary-adrenal hormone axis.49 They also conducted RIPC experiments on the rat model of post-traumatic stress disorder, and found that RIPC could improve the anxiety symptoms of PTSD rats.50 These findings indicate that RIPC has potential anxiolytic and antidepressant effects. At present, there is still a lack of research on its clinical efficacy and safety in patients with depression and anxiety.
However, our study had not shown significant difference in the improvement of depressive symptoms between the active RIPC group and the sham RIPC group. There are several possible reasons to be considered. Firstly, the sample size was insufficient. The sample size directly affects the statistical power of the experimental results. If the sample size is too small, differences between the experimental and control groups may not be detected, even if these differences are real. Secondly, a reduction of less than 50% on the QIDS-SR16 scale score may be too wide for a poor response to escitalopram. The results showed that both the experimental group and the control group had significant improvement in depressive symptoms at the second week of enrollment, suggesting that some of the enrolled patients may have a good response to escitalopram treatment, but the treatment time is insufficient. It may be more appropriate to set the reduction rate of QIDS-SR16 scale score to 30% as the enrollment criterion. Thirdly, RIPC treatment may simply not be effective in physically healthy patients with depression. Previous clinical studies have confirmed that RIPC therapy has a protective effect on ischemic diseases such as myocardial infarction and cerebral infarction.46–48 Whether RIPC has a benefit in people without ischemic risk is unknown. RIPC adjuvant therapy may be effective for patients with depression who are at risk for ischemic disease. The patients with risk for ischemic disease had been excluded from our study.
The results of our study showed no significant difference in anxiety symptoms between the experimental and control groups. We mainly enrolled patients with depression, and the anxiety symptoms of the enrolled patients were not very severe at Baseline (GAD-7 score median 10.0 in the active and 13.5 in the sham RIPC group), which could attribute to the non-significant difference in efficacy of anxiety symptoms. As mentioned earlier, there was no significant difference in improvement in depressive symptoms between the two groups. Although without significant differences, the remission rate in the active RIPC group was 13.4% (ITT analysis) or 12.1% (PP analysis) higher than the sham RIPC group, RIPC as an adjunctive treatment for depression still has certain clinical advantages and worth further research.
In terms of treatment safety assessment, from the results of our study, RIPC as an adjuvant treatment is relatively safe, with no significant effect on heart rate and blood pressure, and no increase in the risk of (hypo) manic episodes, except for a few patients with local skin ecchymosis (which relieved spontaneously within 1 week). The RIPC treatment was well tolerated by MDD patients without a significant increase in study discontinuation, instead the dropout rate decreased by 5.4% in the active RIPC group compared with that in the sham RIPC group.
Some promising intervention strategies have demonstrated antidepressant effects in patients with major depressive disorder (MDD). Among them, deep transcranial magnetic stimulation (dTMS) enhances neural plasticity by focusing on deep brain regions such as the dorsolateral prefrontal cortex.51 Its efficacy in treatment-resistant MDD has been supported by multiple randomized controlled trials, and it has higher target specificity than traditional repetitive TMS.52,53 Continuous theta burst stimulation (cTBS), which modulates cortical excitability through a high-frequency pulse pattern, takes effect more quickly (usually within 1–2 weeks) and is suitable for MDD patients who need rapid symptom relief.54 Stanford Neuro Modulation Therapy (SNT), based on individualized brain imaging localization, achieves rapid antidepressant effects in a short course (5 days) through intensive high-frequency rTMS, and shows particular potential for severe or suicidal MDD patients.55 Unlike these neuroregulatory strategies that directly act on brain regions, the remote ischemic preconditioning (RIPC) explored in this study, as a peripheral intervention method, complements the mechanism by which it affects the central nervous system through the neuro-immune-endocrine pathway, providing a new perspective for the multi-target intervention measures of MDD.43–45 Meanwhile, RIPC, as a non-invasive treatment measure, is easy to operate, highly safe, and can be carried out in a non-medical environment. If further research can prove its antidepressant efficacy, it will provide patients with an additional clinical treatment option.
Limitations
There are two main limitations in this study. Firstly, the definition of a poor response to escitalopram monotherapy was too liberal in this study. Enrolled patients did not necessarily have a complete poor response to escitalopram. This leads to an increase in the inaccuracy of the experimental results. Secondly, a small sample size may affect statistical power, as a result, the desired therapeutic advantage cannot be demonstrated. The results of this study should be replicated in a larger sample. The sample size estimation for future research on the effects of remote ischemic preconditioning was conducted using GPower3.1.9.7 software (Universität Düsseldorf, Düsseldorf, Germany). An effect size of 0.298 was determined based on the difference in QIDS-SR-16 scores between the two groups from baseline to Week 8. The level of significance (α) was set at 0.05 and the power (1-β) at 0.8, with a group allocation ratio of 1.14:1. Considering a 20% loss to follow-up, a total of 430 patients will need to be recruited. If the sample size is enlarged and the recruitment criteria for research subjects are stricter, the experiment proves that the adjunctive treatment effect of RIPC on depression is not significant, the experiment can be carried out in patients with specific subtypes of depression (eg, depression with anxiety characteristics) to find out the patients who may be suitable for it.
Conclusion
Overall, RIPC was not effective as an adjunctive treatment for depression, but to a certain extent it can increase the clinical remission rate and reduce the dropout rate, with good safety and tolerability. However, our study enrolled patients with limited sample size, further research to address these limitations is required. Despite all this, to date, this study is a first attempt and preliminary investigation of the efficacy of RIPC intervention by a randomized controlled trial in patients with depression. It has certain reference significance for subsequent research and clinical practice. In terms of follow-up research, given the limitation of the sample size in this study, its results can provide a direction for further exploration in this field. Subsequent research can expand the sample size of patients, conduct multi-center, large-sample randomized controlled trials to more accurately verify the effect of RIPC in the adjuvant treatment of depression, and clarify its applicability in different populations and patients with different severity of the disease. At the same time, it can also deeply explore the mechanism by which RIPC exerts its effect, providing a theoretical basis for optimizing the treatment plan. Although this study indicates that RIPC is not highly effective as an adjuvant treatment for depression, its ability to improve clinical remission rates, reduce dropout rates, and demonstrate good safety and tolerability still provides clinicians with certain references. Given its safety and convenience, if subsequent studies can further verify its clinical efficacy, it could provide clinicians with an additional treatment option.
Data Sharing Statement
Due to patient data and ethical restrictions, the current research data is not publicly accessible. If necessary, please send an Email to [email protected] to apply to the corresponding author.
Ethics and Consent Statements
This study complies with the Declaration of Helsinki and was approved by the Ethics Committee of Shanghai Hongkou Mental Health Center (2019/D04), and was registered with the Chinese Clinical Trial Registry on February 10, 2020 (ChiCTR2000029729). Participants gave informed consent.
Acknowledgments
Prof. Xunming Ji is one of the inventors of the electric autocontrol IPC device (model IPC-906) that has been patented in China (patent number ZL201410834305.2, China) who supplied freely all devices in this study. Thank him for the equipment support of this study. We would like to thank all the subjects who agreed to participate in this study. Gratitude to all researchers for their dedicated efforts.
Funding
This work was supported by Health System Key Discipline of Shanghai (2024ZDXK0013), Scientific Research Project of Shanghai Municipal Health Commission (202040318), Shanghai Yangpu District Health Commission Foundation (22YPZB10), Shanghai University of Medicine & Health Sciences Foundation (20MC2020005), and Shanghai University of Medicine & Health Sciences/Shanghai Yangpu District Mental Health Center Foundation (YJYPI202401).
Disclosure
The authors declare no competing interests related to this study.
References
1. Lam RW, McIntosh D, Wang J, et al. Canadian Network For Mood And Anxiety Treatments (CANMAT) 2016 Clinical guidelines for the management of adults with major depressive disorder: section 1. Can J Psychiatry. 2016;61:510–523. doi:10.1177/0706743716659416
2. World Health Organization WHO. Depression and other common mental disorders.Global Health Estimates. Geneva:World Health Organization. Available from. https://creativecommons.org/licenses/by-nc-sa/3.0/igo/.
3. Huang Y, Wang Y, Wang H, et al. Prevalence of mental disorders in China: cross-sectional epidemiological study. Lancet Psychiatry. 2019;6(3):211–224. doi:10.1016/S2215-0366(18)30511-X
4. Thornicroft G, Chatterji S, Evans-Lacko S, et al. Undertreatment of people with major depressive disorder in 21 countries. Br J Psychiatry. 2017;210(2):119–124. doi:10.1192/bjp.bp.116.188078
5. Phillips MR, Zhang J, Shi Q, et al. Prevalence, treatment, and associated disability of mental disorders in four provinces in China during 2001-05: an epidemiological survey. Lancet. 2009;373(9680):2041–2053. doi:10.1016/S0140-6736(09)60660-7
6. McIntyre RS, Filteau MJ, Martin L, et al. Treatment-resistant depression: definitions, review of the evidence, and algorithmic approach. J Affect Disord. 2014; 156:1–7. doi:10.1016/j.jad.2013.10.043
7. Rush AJ, Fava M, Wisniewski SR, et al. Sequenced treatment alternatives to relieve depression (STAR*D): rationale and design. Control Clin Trials. 2004;25(1):119–142. doi:10.1016/S0197-2456(03)00112-0
8. Trivedi MH, Rush AJ, Wisniewski SR, et al. Evaluation of outcomes with citalopram for depression using measurement-based care in STAR*D: implications for clinical practice. Am J Psychiatry. 2006;163(1):28–40. doi:10.1176/appi.ajp.163.1.28
9. Rush AJ, Trivedi MH, Wisniewski SR, et al. Acute and longer-term outcomes in depressed outpatients requiring one or several treatment steps: a STAR*D report. Am J Psychiatry. 2006;163(11):1905–1917. doi:10.1176/ajp.2006.163.11.1905
10. Andrea C, Toshi AF, Georgia S, et al. Comparative efficacy and acceptability of 21 antidepressant drugs for the acute treatment of adults with major depressive disorder: a systematic review and network meta-analysis. Lancet. 2018;391(10128):1357–1366. doi:10.1016/S0140-6736(17)32802-7
11. Ormel J, Kessler RC, Schoevers R. Depression: more treatment but no drop in prevalence: how effective is treatment? And can we do better? Curr Opin Psychiatry. 2019;32(4):348–354. doi:10.1097/YCO.00000000000000505
12. Jason M, Joski P, Yarbrough C, et al. Trends in treatment and spending for patients receiving outpatient treatment of depression in the United States, 1998-2015. JAMA Psychiatry. 2019;76(8):810–817. doi:10.1001/jamapsychiatry.2019.0633
13. Kennedy SH, Lam RW, McIntyre RS, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 3. Can J Psychiatry. 2016;61(9):540–560. doi:10.1177/0706743716659417
14. Milev RV, Giacobbe P, Kennedy SH, et al. Canadian Network for Mood and Anxiety Treatments (CANMAT) 2016 clinical guidelines for the management of adults with major depressive disorder: section 4. Can J Psychiatry. 2016;61(9):561–575. doi:10.1177/0706743716660033
15. Heijnen WT, Birkenhäger TK, Wierdsma AI, van den Broek WW. Antidepressant pharmacotherapy failure and response to subsequent electroconvulsive therapy: a meta-analysis. J Clin Psychopharmacol. 2010;30(5):616–619. doi:10.1097/JCP.0b013e3181ee0f5f
16. Mi Z, Biswas K, Fairchild JK, et al. Repetitive transcranial magnetic stimulation (rTMS) for treatment-resistant major depression (TRMD) Veteran patients: study protocol for a randomized controlled trial. Trials. 2017;18(1):409. doi:10.1186/s13063-017-2125-y
17. Levkovitz Y, Isserles M, Padberg F, et al. Efficacy and safety of deep transcranial magnetic stimulation for major depression: a prospective multicenter randomized controlled trial. World Psychiatry. 2015;14(1):64–73. doi:10.1002/wps.20199
18. Wang Z, Li X, Li N, et al. Safety and tolerability of both arm ischemic conditioning in patients with major depression: a proof of concept study. Front Psychiatry. 2020;11:570. doi:10.3389/fpsyt.2020.00570
19. Xu Y, Yu Q, Yang J, et al. Acute hemodynamic effects of remote ischemic preconditioning on coronary perfusion pressure and coronary collateral blood flow in coronary heart disease. Acta Cardiol Sin. 2018;34(4):299–306. doi:10.6515/ACS.201807_34(4).20180317A
20. Lv J, Guan W, You Q, et al. RIPC provides neuroprotection against ischemic stroke by suppressing apoptosis via the mitochondrial pathway. Sci Rep. 2020;10(1):5361. doi:10.1038/s41598-020-62336-w
21. Cao B, Wang H, Zhang C, Xia M, Yang X. Remote Ischemic Postconditioning (RIPC) of the upper arm results in protection from cardiac ischemia-reperfusion injury following primary percutaneous coronary intervention (PCI) for acute ST-Segment Elevation Myocardial Infarction (STEMI). Med Sci Monit. 2018;24:1017–1026. doi:10.12659/msm.908247
22. You J, Feng L, Bao L, Xin M, Ma D, Feng J. Potential applications of remote limb ischemic conditioning for chronic cerebral circulation insufficiency. Front Neurol. 2019;10:467. doi:10.3389/fneur.2019.00467
23. Dirnagl U, Simon RP, Hallenbeck JM. Ischemic tolerance and endogenous neuroprotection. Trends Neurosci. 2003;26(5):248–254. doi:10.1016/S0166-2236(03)00071-7
24. Meng R, Ding Y, Asmaro K, et al. Ischemic conditioning is safe and effective for octo- and nonagenarians in stroke prevention and treatment. Neurotherapeutics. 2015;12(3):667–677. doi:10.1007/s13311-015-0358-6
25. Hausenloy DJ, Yellon DM. Ischaemic conditioning and reperfusion injury. Nat Rev Cardiol. 2016;13(4):193–209. doi:10.1038/nrcardio.2016.5
26. Ren C, Wang P, Wang B, et al. Limb remote ischemic per-conditioning in combination with post-conditioning reduces brain damage and promotes neuroglobin expression in the rat brain after ischemic stroke. Restor Neurol Neurosci. 2015;33(3):369–379. doi:10.3233/RNN-140413
27. Ren C, Li S, Wang B, et al. Limb remote ischemic conditioning increases Notch signaling activity and promotes arteriogenesis in the ischemic rat brain. Behav Brain Res. 2018;340:87–93. doi:10.1016/j.bbr.2016.10.036
28. Meng R, Asmaro K, Meng L, et al. Upper limb ischemic preconditioning prevents recurrent stroke in intracranial arterial stenosis. Neurology. 2012;79(18):1853–1861. doi:10.1212/WNL.0b013e318271f76a
29. Li S, Ma C, Shao G, et al. Safety and feasibility of remote limb ischemic preconditioning in patients with unilateral middle cerebral artery stenosis and healthy volunteers. Cell Transplant. 2015;24(9):1901–1911. doi:10.3727/096368914X683520
30. Zhao W, Meng R, Ma C, et al. Safety and efficacy of remote ischemic preconditioning in patients with severe carotid artery stenosis before carotid artery stenting: a Proof-of-Concept, randomized controlled trial. Circulation. 2017;135(14):1325–1335. doi:10.1161/CIRCULATIONAHA.116.024807
31. Zhao W, Zhang J, Sadowsky MG, Meng R, Ding Y, Ji X. Remote ischaemic conditioning for preventing and treating ischaemic stroke. Cochrane Database Syst Rev. 2018;7:CD012503.
32. Zhou D, Ding J, Ya J, et al. Efficacy of remote ischemic conditioning on improving WMHs and cognition in very elderly patients with intracranial atherosclerotic stenosis. Aging. 2019;11(2):634–648. doi:10.18632/aging.101764
33. Nutt DJ. Relationship of neurotransmitters to the symptoms of major depressive disorder. J Clin Psychiatry. 2008;69(E1):4–7.
34. Beurel E, Toups M, Nemeroff CB. The bidirectional relationship of depression and inflammation: double trouble. Neuron. 2020;107(2):234–256. doi:10.1016/j.neuron.2020.06.002
35. Cai S, Huang S, Hao W. New hypothesis and treatment targets of depression: an integrated view of key findings. Neurosci Bull. 2015;31(1):61–74. doi:10.1007/s12264-014-1486-4
36. Milenkovic VM, Stanton EH, Nothdurfter C, Rupprecht R, Wetzel CH. The role of chemokines in the pathophysiology of major depressive disorder. Int J Mol Sci. 2019;20:2283. doi:10.3390/ijms20092283
37. Etherton MR, Siddiqui KA, Schwamm LH. Prestroke selective serotonin reuptake inhibitor use and functional outcomes after ischaemic stroke. Stroke Vasc Neurol. 2018;3(1):9–16. doi:10.1136/svn-2017-000119
38. Rush AJ, Trivedi MH, Ibrahim HM, et al. The 16-item Quick Inventory Of Depressive Symptomatology (QIDS), clinician rating (QIDS-C), and self-report (QIDS-SR): a psychometric evaluation in patients with chronic major depression. Biol. Psychiatry. 2003;54(5):573–583. doi:10.1016/s0006-3223(02)01866-8
39. Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. doi:10.1046/j.1525-1497.2001.016009606.x
40. Roniger A, Späth C, Schweiger U, Klein JP. A psychometric evaluation of the german version of the Quick Inventory of Depressive Symptomatology (QIDS-SR16) in outpatients with depression. Psychother Psychosomatics. 2015;83:17–22. doi:10.1055/s-0041-110203
41. Trivedi MH, Fava M, Wisniewski SR, et al. Medication augmentation after the failure of SSRIs for depression. N Engl J Med. 2006;354(12):1243–1252. doi:10.1056/NEJMoa052964
42. Bulteau S, Sébille V, Fayet G, et al. Efficacy of intermittent Theta Burst Stimulation (iTBS) and 10-Hz high-frequency repetitive transcranial magnetic stimulation (rTMS) in treatment-resistant unipolar depression: study protocol for a randomised controlled trial. Trials. 2017;18(1):17. doi:10.1186/s13063-016-1764-8
43. Baranova K, Nalivaeva N, Rybnikova E. Neuroadaptive biochemical mechanisms of remote ischemic conditioning. Int J Mol Sci. 2023;24(23):17032. doi:10.3390/ijms242317032
44. Hao Y, Xin M, Feng L, et al. Review cerebral ischemic tolerance and preconditioning: methods, mechanisms, clinical applications, and challenges. Front Neurol. 2020;11:812. doi:10.3389/fneur.2020.00812
45. Keevil H, Phillips BE, England TJ. Remote ischemic conditioning for stroke: a critical systematic review. Int J Stroke. 2024;19(3):271–279. doi:10.1177/17474930231191082
46. Mollet I, Pedro Marto J, Mendonça M, et al. Remote but not distant: a review on experimental models and clinical trials in remote ischemic conditioning as potential therapy in ischemic stroke. Vieira Mol Neurobiol. 2022;59(1):294–325. doi:10.1007/s12035-021-02585-6
47. Ferdinandy P, Andreadou I, Baxter GF, et al. Interaction of cardiovascular nonmodifiable risk factors, comorbidities and comedications with ischemia/reperfusion injury and cardioprotection by pharmacological treatments and ischemic conditioning. Pharmacol Rev. 2023;75(1):159–216. doi:10.1124/pharmrev.121.000348
48. Czigany Z, Bleilevens C, Beckers C, et al. Limb remote ischemic conditioning of the recipient protects the liver in a rat model of arterialized orthotopic liver transplantation. PLoS One. 2018;13(4):e0195507. doi:10.1371/journal.pone.0195507
49. Baranova KA, Zenko MY. Applying remote ischemic pre- and postconditioning for the correction of experimental depression. Zh Nevrol Psikhiatr Im S S Korsakova. 2019;119(6):72–80. doi:10.17116/jnevro201911906172
50. Baranova KA, Pivina SG, Rybnikova EA. The anxiolytic effects of moderate hypoxia and remote ischemia in the posttraumatic stress disorder model are accompanied by modification of functioning of the hypothalamic–pituitary–adrenal axis. Neurochem J. 2018;12(2):130–134. doi:10.1134/S1819712418020022
51. Lan XJ, Yang XH, Mo Y, et al. Deep transcranial magnetic stimulation for treatment-resistant depression: a systematic review and meta-analysis of randomized controlled studies. Asian J Psychiatr. 2024;96:104032. doi:10.1016/j.ajp.2024.104032
52. Bouhassira D, Jazat-Poindessous F, Farnes N, et al. Comparison of the analgesic effects of “superficial” and “deep” repetitive transcranial magnetic stimulation in patients with central neuropathic pain: a randomized sham-controlled multicenter international crossover study. Pain. 2024;165(4):884–892. doi:10.1097/j.pain.0000000000003082
53. Valero-Cabré A, Amengual JL, Stengel C, et al. Transcranial magnetic stimulation in basic and clinical neuroscience: a comprehensive review of fundamental principles and novel insights. Neurosci Biobehav Rev. 2017;83:381–404. doi:10.1016/j.neubiorev.2017.10.006
54. Cai DB, Qin XD, Qin ZJ, et al. Adjunctive continuous theta burst stimulation for major depressive disorder or bipolar depression: a meta-analysis of randomized controlled studies. J Affect Disord. 2024;346:266–272. doi:10.1016/j.jad.2023.10.161
55. Lan XJ, Cai DB, Liu QM, et al. Stanford neuromodulation therapy for treatment-resistant depression: a systematic review. Front Psychiatry. 2023;14:1290364. doi:10.3389/fpsyt.2023.1290364
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Efficacy and Safety of Anlotinib in Extensive-Stage Small Cell Lung Cancer: A Multicenter Real-World Study
Zheng HR, Jiang AM, Gao H, Liu N, Zheng XQ, Fu X, Zhang R, Ruan ZP, Tian T, Liang X, Yao Y
Cancer Management and Research 2022, 14:2273-2287
Published Date: 2 August 2022
Relative Safety and Efficacy of Two Doses of Tandospirone Citrate for Generalized Anxiety Disorder: A Multicenter Randomized Controlled Trial
Li Q, Zhang H, Lin G, Shi S, Zhang Y, Ji J, Yang L, Yao J, Wu W
Neuropsychiatric Disease and Treatment 2022, 18:1653-1664
Published Date: 8 August 2022
Biosimilars: Science, Implications, and Potential Outlooks in the Middle East and Africa
Batran RA, Elmoshneb M, Hussein AS, Hussien OM, Adel F, Elgarhy R, Morsi MI
Biologics: Targets and Therapy 2022, 16:161-171
Published Date: 6 October 2022
Efficacy and Safety of Empagliflozin in Patients with Type 2 Diabetes Mellitus Fasting During Ramadan: A Real-World Study from Bangladesh
Pathan MF, Akter N, Selim S, Saifuddin M, Qureshi NK, Kamrul-Hasan ABM, Hannan MA, Ahmed MAU, Mustari M, Chakraborty AK
Diabetes, Metabolic Syndrome and Obesity 2022, 15:4011-4021
Published Date: 22 December 2022
Clinical Evaluation of Risankizumab in the Treatment of Adults with Moderately to Severely Active Crohn’s Disease: Patient Selection and Reported Outcomes
Horst S, Cross RK
Drug Design, Development and Therapy 2023, 17:273-282
Published Date: 31 January 2023