Back to Journals » Therapeutics and Clinical Risk Management » Volume 21
Early Phase Thrombolysis and Functional Outcome for Acute Ischemic Stroke Treated with Endovascular Thrombectomy After Intravenous Thrombolysis
Authors Sun S, Yuan K ![]() , Huang H, Xie M, Huo S, Deng K, Liu R, Liu X
, Huang H, Xie M, Huo S, Deng K, Liu R, Liu X ![]()
Received 16 August 2025
Accepted for publication 15 November 2025
Published 2 December 2025 Volume 2025:21 Pages 1637—1644
DOI https://doi.org/10.2147/TCRM.S554227
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Siyu Sun,1,* Kang Yuan,2,* Hui Huang,3,* Mengdi Xie,2,4 Shuxian Huo,2 Kejia Deng,2 Rui Liu,2 Xinfeng Liu1,2
1Department of Neurology, Jinling Clinical Medical College, Nanjing Medical University, Nanjing, 210002, People’s Republic of China; 2Department of Neurology, Nanjing Jinling Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, 210002, People’s Republic of China; 3Department of Neurology, Linquan Country People’s Hospital, Anhui, 236400, People’s Republic of China; 4Department of Neurology, Linyi People’s Hospital, Shangdong, 276000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xinfeng Liu, Department of Neurology, Jinling Hospital, Nanjing Medical University, No. 305 East Zhongshan Road, Nanjing, Jiangsu Province, 210002, People’s Republic of China, Tel +86 2584801861, Fax +86 2584805169, Email [email protected]
Background: The efficacy of intravenous thrombolysis (IVT) in treating acute ischemic stroke (AIS) has shown a rapid decline with time; however, the impact of this trend on IVT prior to endovascular thrombectomy (EVT) remains uncertain.
Methods: This study retrospectively analyzed patients from multicenter trials who received EVT after IVT in the anterior circulation. The endpoints included unfavorable outcomes (defined as a 90-day modified Rankin Scale score of 3– 6) and hemorrhagic complications. Patients were stratified into two groups based on onset-to-needle time (ONT), with a 2-hour threshold. ONT was defined as the interval from the first observed stroke symptoms (or the last known well state) to the initiation of IVT. Multivariate logistic regression and propensity score matching (PSM) were used to compare outcomes.
Results: Among the 176 patients following PSM (with a median age of 67.5 years and 60.8% being female), the median ONT was 120 minutes (85 minutes vs 176 minutes in early and late phase group), with 88 patients in each group. Multivariate analysis revealed that late phase IVT (ONT > 2 hours) was significantly associated with unfavorable outcomes (odds ratio [OR] = 2.213; 95% confidence interval [CI] = 1.078– 4.646; P = 0.032). No significant differences were observed in mortality and hemorrhagic complications between the groups. Subgroup analysis revealed no significant disparities among the predefined subgroups.
Conclusion: Early phase IVT (ONT ≤ 2 hours) before EVT was linked to reduced unfavorable outcomes for AIS. No significant differences were observed among predefined subgroups.
Keywords: ischemic stroke, thrombolysis, thrombectomy, therapeutic window, hemorrhage, prognosis
Introduction
Endovascular thrombectomy (EVT) has emerged as the gold standard for anterior circulation acute ischemic stroke (AIS) patients since 2015.1 Clinical trials demonstrated that EVT after intravenous thrombolysis (IVT) was non-inferior to using monotherapy.2–5 A randomized study noted that, using the combined approach, 46.6% (vs 54.3% EVT alone) achieved independence at 3 months, with similar mortality (17.8% vs 17.2%) and hemorrhage rates (6.8% vs 6.1%).3 Therefore, the American and European guidelines all recommended this strategy in eligible patients.6,7 Specifically, EVT after IVT benefited certain groups, and even caused harm in some cases. Identifying optimal patients was complex, with challenges including occlusion site, stroke type, and thrombus features.8 Further investigation into the potential influencing factors was warranted.
Early administration was associated with proportionally greater benefits in AIS, making the timing of EVT after IVT crucial to functional outcomes.9,10 The deformability and softness of thrombi on the early stage boosted the probability of complete recanalization.11 Onset-to-needle (ONT) has been recognized as the potential factor that influences the outcomes of EVT after IVT.12 The improving reperfusion strategies in Ischemic Stroke (IRIS) collaborators emphasized that ONT of less than 2 hours 20 minutes, followed by EVT after IVT, was statistically associated with functional outcomes.12 An observational study found a 21.4–39.4% complete recanalization rate with an ONT of 1 hour.9 A meta-analysis of six trials indicated improved outcomes with IVT within 2 hours.13
Based on previous research, Our study hypothesized that early phase IVT (ONT ≤ 2 hours) after EVT was associated with reduced unfavorable outcomes, potentially being more pronounced in specific subgroups. We aimed to help refine patient selection or optimize emergency decision-making for EVT after IVT.
Methods
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Study Design and Participants
We included patients from two multicenter prospective studies, the Captor trial (ChiCTR1900025256, https://www.chictr.org.cn) and SINOMED SR trial (NCT04973332, clinicaltrials.gov), and a multicenter retrospective registry between January 2019 and January 2020. Meanwhile, most of the other inclusion and exclusion criteria aligned closely with the detailed explanations in the Chinese guidelines for EVT of AIS. The inclusion criteria were 1) age ≥ 18 years; 2) the National Institutes of Health Stroke Scale (NIHSS) ≥ 6 at enrollment; 3) pre-stroke modified Rankin Scale (mRS) < 2; 4) AIS due to large-vessel occlusion in the anterior circulation confirmed by CT angiography, MR angiography, or digital subtraction angiography; and 5) treatment of EVT after IVT within the thrombolysis time window. The exclusion criteria were 1) CT or MR imaging evidence of intracranial hemorrhage; 2) pre-stroke mRS ≥ 2; 3) presence of active bleeding and known bleeding tendency; 4) with heart, lung, liver, kidney function failure or other severe diseases to interventional surgery; 5) no available data on ONT and follow-up information; and 6) with contraindications for IVT. Our study was approved by the Medical Ethics Committee of Linyi People’s Hospital (YX200655) to exempt informed consent, as it was a retrospective analysis using existing medical records, with no risk to participant identities, privacy, or safety. Our study was performed in adherence to the ethical standards of the 1964 Helsinki Declaration and its later amendments.
Clinical and Imaging Data
Demographic details, medical history, laboratory tests, and radiological images were collected in a standard process. Stroke severity was measured with NIHSS score at baseline and 24–48 hours after admission. Stroke subtypes were classified according to Trial of Org 10172 in Acute Stroke Treatment (TOAST). Radiological images were independently reviewed by two experienced neurologists who were blinded to treatment allocation and outcomes. Early ischemic changes were evaluated using the Alberta Stroke Program Early CT score (ASPECTS). Cerebral reperfusion was assessed with the modified Thrombolysis in Cerebral Infarction (mTICI).
Treatment and Time Parameters
All patients enrolled received EVT after IVT. IVT was administered within the therapeutic window based on the thrombolysis agents as determined by neurologists, including recombinant tissue-plasminogen activator (rt-PA), urokinase, and Tenecteplase (TNK). The subsequent EVT frequently relied on thrombectomy with retrievers, as well as rescue procedures such as stent implantation, balloon angioplasty, intra-atrial thrombolysis, or tirofiban when recanalization failed. EVT was initiated as soon as possible without waiting for clinical responses from IVT.
In all trials, the time of stroke onset was recorded as either the moment the symptoms of AIS were first noticed or the last known time of the participants’ normal condition. The time point of IVT administration, arterial access, and cerebral reperfusion for thrombectomy was registered by the local investigators of each center for recording time parameters such as ONT, onset to puncture time (OTP), and puncture to recanalization time (PTR).
Clinical Outcome
The unfavorable outcome was defined as mRS score of 3–6 at 90 days after stroke. The score ranged from 0–6, where larger values indicated a higher degree of disability and 6 represented death. Successful recanalization was defined as a final mTICI grade of 2b or 3 at the end of the endovascular procedure – corresponding to reperfusion of at least 50% of the affected vascular territory. Symptomatic intracranial hemorrhage (SICH) was defined as the occurrence of intracranial hemorrhage (ICH) confirmed by CT or MRI, accompanied by an increase in the NIHSS score of at least 4 points. Hemorrhagic complications included ICH, as well as extracranial bleeding, such as at puncture sites, the gastrointestinal tract, and the urinary tract.
Statistical Analysis
Data on baseline characteristics were summarized using frequencies and proportions for categorical variables and means (or medians) with standard deviations (or interquartile range) as appropriate for continuous variables. Differences in baseline characteristics were analyzed using the Fisher exact test or χ2 test for categorical variables and the t-test or Mann–Whitney U-test for continuous outcomes.
Propensity score-matching (PSM) was used to minimize the potential effect of between-group differences in key variables. The propensity score was generated with variables with a P < 0.1 in univariable analyses or with variables known to impact clinical outcomes. Patients were then matched in a 1:1 ratio based on the nearest-neighbor algorithm without replacement within the caliper distance of 0.2. We used multiple imputation for missing data.
Restricted cubic splines (RCS) were performed to evaluate the potential nonlinear relationship between ONT and unfavorable outcomes, with four knots at the 5th, 35th, 65th, and 95th percentiles. We divided the ONT into the early phase (≤ 2 hours) and the late phase (> 2 hours). The RCS revealed a significant increase in the risk of unfavorable outcomes when ONT > 2 hours (Supplementary Figure 1). Moreover, previous clinical trials and meta-analyses have indicated a striking reduction in the time benefit after approximately 120 minutes.9,12–14
Univariable logistic regression was performed to explore the predictors of the unfavorable outcomes. Differences between the early phase group and late phase group in clinical outcomes were reported separately using unadjusted (Model 1) and adjusted (Model 2) multivariable logistic analysis (adjusted for age, gender, hypertension, diabetes mellitus, atrial fibrillation, hyperlipidemia, smoking status, NIHSS score, ASPECTS score, glucose (GLU), OTP, and PTR). Furthermore, we did a prespecified subgroups analysis to test the heterogeneity of treatment effect on unfavorable outcomes by relevant variables, including age, gender, hypertension, diabetes, AF, and NIHSS score. Odds ratio and associated P values of each interaction term were estimated from separate logistic regression models across the prespecified subgroups.
All reported P values were two-sided, with P < 0.05 considered statistically significant. Statistical analysis was performed using R studio (version 4.4.1 R Foundation).
Results
Study Population
We obtained data of 215 patients treated with EVT after IVT (median age was 68 years, and 60.5% of patients were female) from three trials after excluding 430 patients due to missing related data.
Of 215 patients, 99 received IVT in the early phase (≤ 2 hours) when the median ONT was 1 hour 25 mins vs 116 in the late phase (> 2 hours) when the median ONT was 3 hours. In total, 71.6% of patients had a history of hypertension, 15.8% had diabetes, 19.5% had hyperlipidemia, and 39.1% had atrial fibrillation (AF) (Supplement Table 1). Patients in the ONT ≤ 2 hours group had higher ASPECTS scores, lower mRS at 90 days, shorter OTP, and less unfavorable outcomes (all P <0.05, Supplement Table 1).
After PSM, 176 participants remained for evaluation, and 88 patients in the ONT ≤ 2 hours group were matched to 88 patients in the ONT > 2 hours group. The differences in the two groups were reduced with an absolute mean difference ≤ 0.20 for variables that were included in the propensity score formula, except ASPECT score (Supplementary Figure 2). Patients in the ONT ≤ 2 hours group had a shorter period of OTP, lower mRS at 90 days, lower proportions of MCA artery occlusion and less unfavorable outcome (all P <0.05, Table 1).
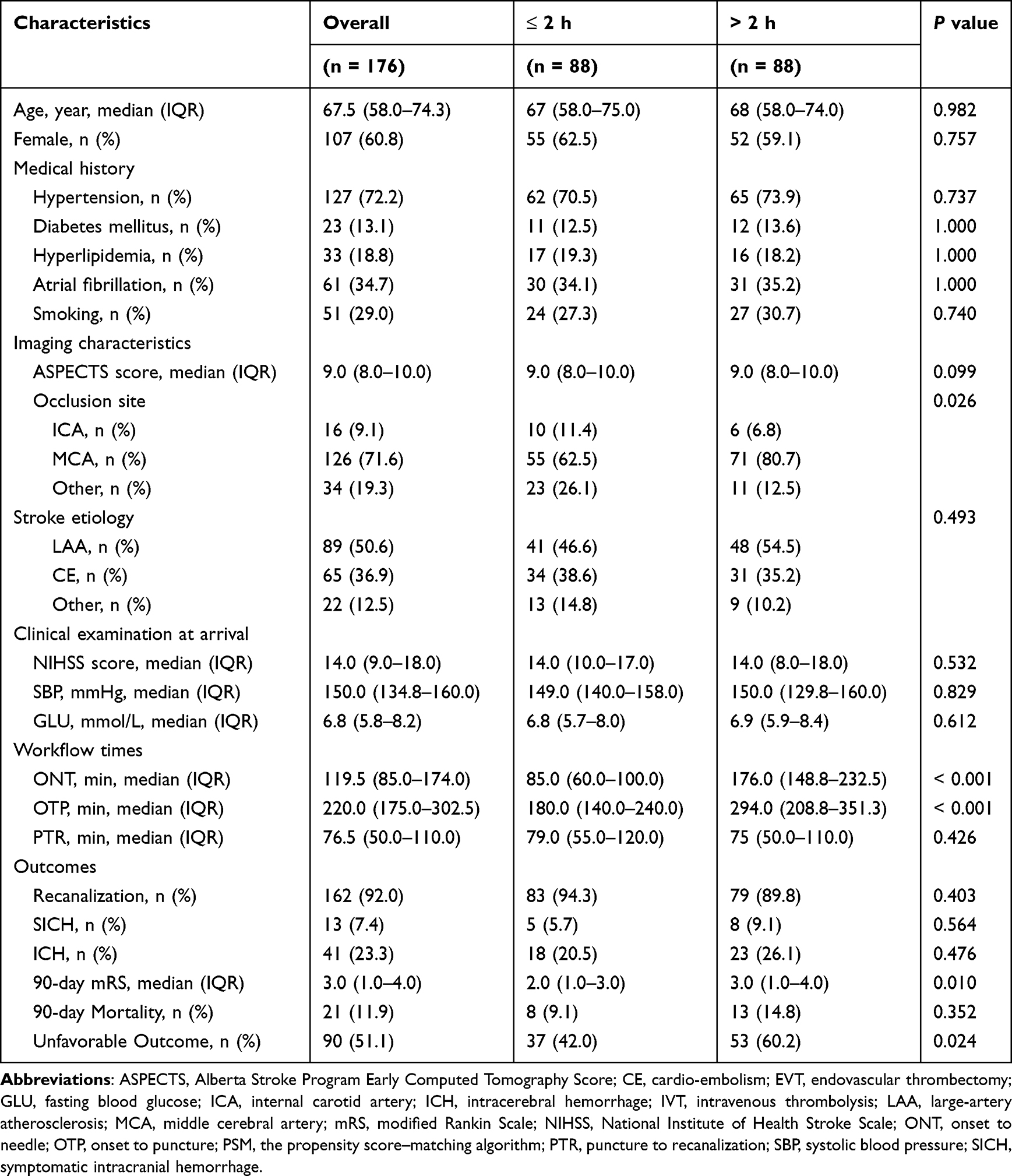 |
Table 1 Baseline characteristics of patients accepting EVT after IVT according to ONT after PSM |
Clinical Outcomes
After PSM, the rates of unfavorable outcomes were 42% in the early phase group and 60.2% in the late phase group, with an absolute risk reduction (ARR) of 18.2% and a number needed to treat (NNT) of six. The rates of SICH (9.1% vs 5.7%) and ICH (26.1% vs 20.5%) were also higher in the late phase group (Table 1).
The RCS revealed a nonlinear relationship between ONT and unfavorable outcomes, indicating that the risk of unfavorable outcomes decreased when ONT was between 70 and 120 hours. Conversely, the risk increased when ONT > 2 hours (Supplementary Figure 1). In univariable analysis, age, AF, high NIHSS score, low ASPECT score, and GLU were the independent predictors of unfavorable outcomes (all P < 0.05, Supplement Table 3).
In multivariable analysis, the late phase IVT had a significant association with unfavorable outcomes in model 1 (OR = 2.087; 95% CI = 1.149–3.833; P = 0.016) and model 2 (OR = 2.213; 95% CI = 1.078–4.646; P = 0.032; Table 2). We did not observe a significant relationship between ONT and successful recanalization, ICH, SICH, and mortality before and after PSM (Supplement Table 2). At 90 days, the early phase IVT was linked with a shift in the distribution of mRS score toward better outcomes (Figure 1).
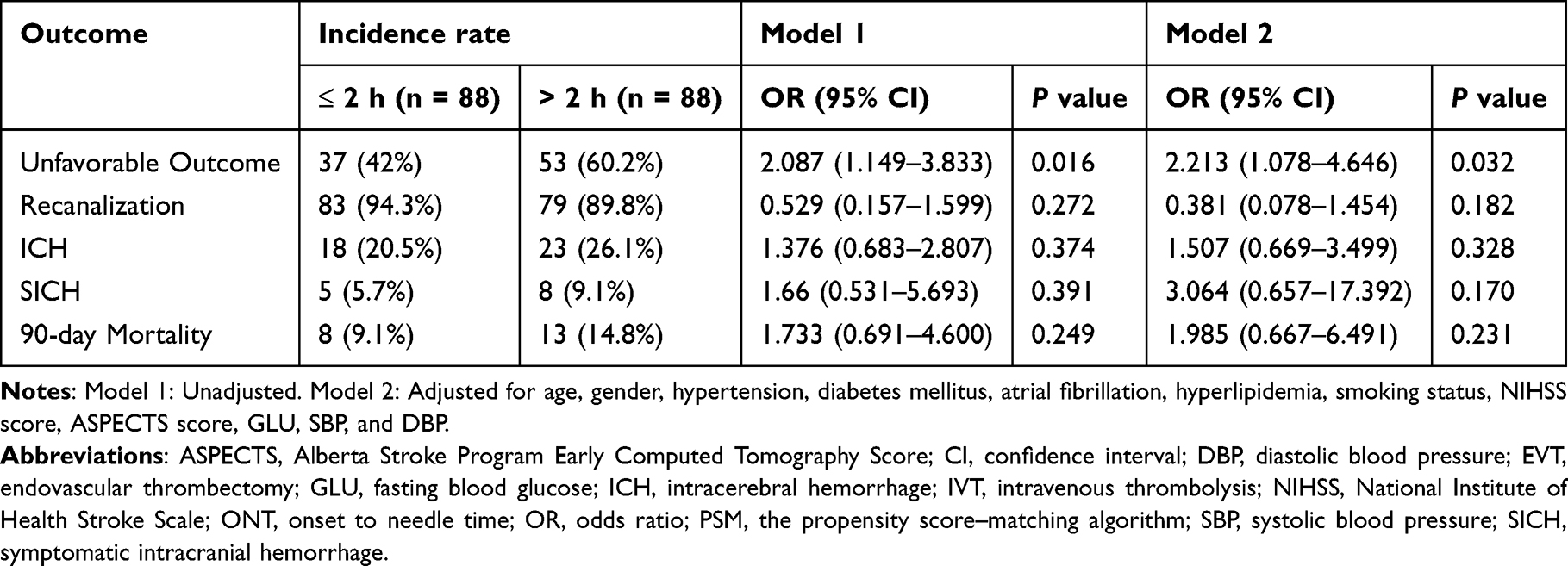 |
Table 2 Odds ratio (95% CI) for outcomes accepting EVT after IVT according to ONT after PSM |
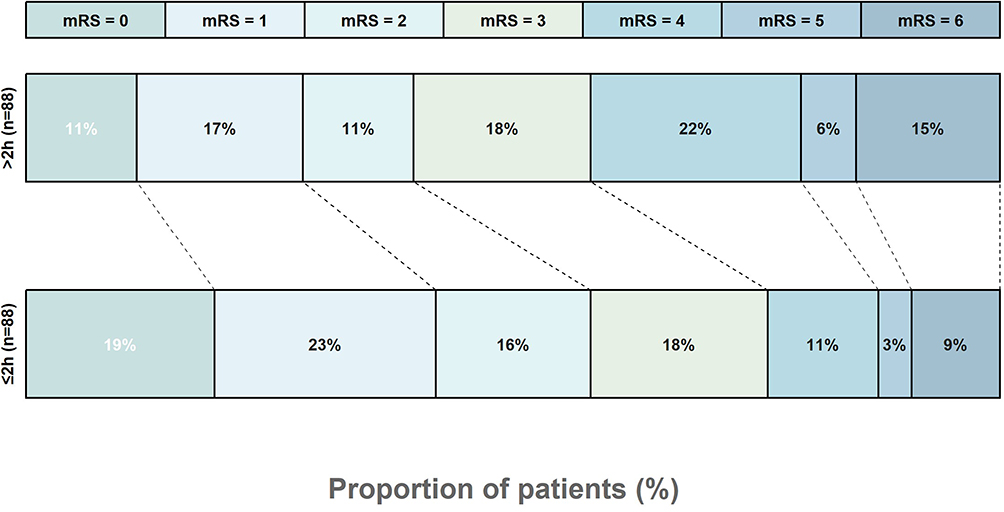 |
Figure 1 Scores on the modified Rankin Scale at 90 days. Distribution of mRS scores at 90 days in the early phase and late phase groups. Abbreviations: EVT, endovascular thrombectomy; IVT; intravenous thrombolysis; mRS, modified Rankin Scale. |
In subgroup analysis, there was no statistical evidence of heterogeneity in treatment effect on unfavorable outcomes. Although the P value for males indicated statistical significance, the broad 95% CI suggested a low precision in the estimated true effect (OR = 3.603; 95% CI = 1.644–8.165, P = 0.033, Figure 2).
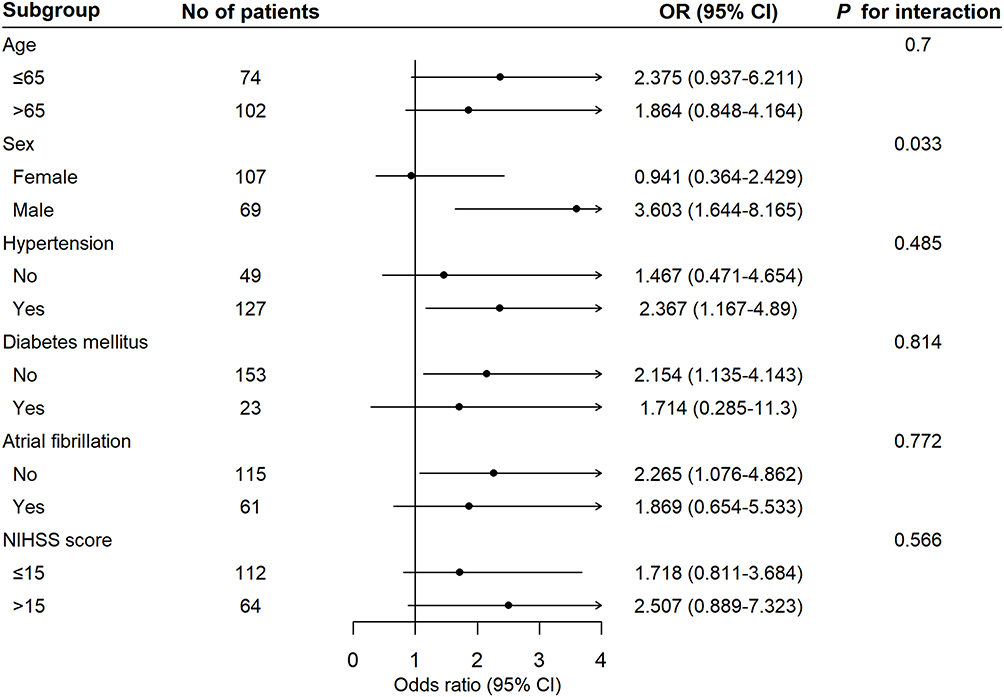 |
Figure 2 Forest plot showing adjusted treatment effect for unfavorable outcomes in prespecified subgroups with P values for heterogeneity across subgroups. Abbreviations: CI, confidence interval; OR, odds ratio; NIHSS, National Institutes of Health Stroke Scale. |
Discussion
In AIS patients treated with EVT after IVT, IVT administrated within 2 hours was significantly associated with the reduction in unfavorable outcomes at 90 days. There was no significant difference in the rates of SICH, ICH, and mortality between patients receiving IVT in the early phase and those in the late phase.
Time was identified as a determinant factor of outcomes in AIS patients. In a recent meta-analysis, Kaesmacher et al reported EVT after IVT lost benefits at about 2 hours from stroke symptom onset.13 Hence, we chose 2 hours as the ONT threshold to classify in our study. Another meta-analysis suggested that the benefit of EVT after IVT was statistically significant only when ONT was short, with the magnitude of benefit decreasing as ONT extended.12 In addition, Gregg et al observed that shorter door to needle time (DNT) was linked with better outcomes and lower mortality.14 Obviously, our findings were consistent with the previous researches.
The abovementioned finding appeared meaningful for clinical routine. The median ONT reported in recent clinical trials varied. In a Dutch registry,15 the median ONT was 1 hour and 22 mins for patients directly admitted to endovascular-capable centers; An American study16 reported 1 hour and 29 mins, and Japan’s17 was 1 hour and 57 mins. We reported the median ONT was 2 hours. Therefore, despite geographical variations, up to approximately 50% of patients were eligible for early phase IVT that showed a significant association with functional outcome.
Our study suggested that the NNT was 6, implying that early phase IVT provided significant clinical advantages. We observed a rapid increase in NNT with treatment delay in similar trails.18 The predicted absolute risk difference (ARD) varied from 9% at 1 hour, to 5% at 2 hours, and 1% at 3 hours, when comparing EVT following IVT with EVT alone.12 Therefore, we recommended that patients selected the nearest endovascular-capable hospital, physicians initiated IVT as soon as possible for ONT ≤ 2 hours, and chose direct EVT for ONT > 2 hours, while carefully weighing the economic pressures, bleeding risks, and clinical benefits.
No evidence of treatment effect heterogeneity was detected in the six prespecified subgroups, except for gender. The moderate sample size constrained the analysis’s power. However, the 95% CI for males (1.644–8.165) was excessively broad, indicating a very low precision in the estimated true effect. Previous studies have conducted analysis of subpopulations. Grossberg et al pointed out that AF patients receiving EVT after IVT suffered more hemorrhagic complications and less functional outcomes.19 Diabetes impacted the sensitivity to the time window and was associated with a higher incidence of ICH.20 Males had higher rates of effective reperfusion, while females had more cases of futile reperfusion.21 However, these findings were merely the results of subgroup analysis, and further randomized controlled trials targeting specific populations such as AF and diabetes status were required.
The observed inconsistency between functional outcomes and successful recanalization rates prompted us to further investigate the underlying mechanism. The “no-reflow” phenomenon, characterized by reduced microvascular reperfusion after complete recanalization, could be the rationale behind this.22 A pooled analysis of three RCTs showed that cerebral “no-reflow” was common and linked to poor prognosis.23 The formation of microthrombi was an important factor. Recent research indicated that administering alteplase to dissolve microthrombi in patients with complete recanalization after EVT improved outcomes.24 The deformability and softness of thrombi on the early stage led to an increased risk of microthrombi.25,26
Our study had several limitations. First, our study combined the data from two prospective studies, and a retrospective registry. Merging the three datasets might generate potential biases because of the different inclusion and exclusion criteria. The retrospective study, prone to selection bias and missing data, was the main source, potentially affecting causality and follow-up. Second, our study lacked data on variables that might influence clinical outcomes due to the original study design, such as post-operative ASPECTS score and collateral status due to study design. Two prospective studies only contributed 54/215 subjects (38/176 post-PSM) due to extensive missing ONT. Third, the statistical power of our findings might be reduced due to the relatively small sample size, especially subgroup analysis. Board 95% CI for unfavorable outcomes (OR = 2.213; 95% CI = 1.078–4.646; P = 0.032) might suggest a degree of uncertainty. Fourth, the potential superiority of EVT following early-phase IVT VS alone EVT was not explored.
In conclusion, our study suggested that early phase IVT was associated with a lower risk of unfavorable outcomes than those in the late phase, without increasing hemorrhagic risk and mortality. ONT was a crucial factor for physicians to consider when selecting optimal candidates for EVT after IVT, physicians should initiate IVT as soon as possible for ONT ≤ 2 hours, and chose direct EVT for ONT > 2 hours. Larger prospective studies were warranted to validate these findings and explore the underlying mechanisms.
Funding
The project is supported by the National Natural Science Foundation of China (NSFC-82471341, and NSFC-U22A20341).
Disclosure
The authors have declared no conflicts of interest with respect to the authorship or publication of this article.
References
1. Campbell BCV, Mitchell PJ, Kleinig TJ, et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N Engl J Med. 2015;372:1009–1018. doi:10.1056/NEJMoa1414792
2. Saver JL, Goyal M, Bonafe A, et al. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA Alone in stroke. N Engl J Med. 2015;372:2285–2295. doi:10.1056/NEJMoa1415061
3. Zi W, Qiu Z, Li F, et al. Effect of endovascular treatment alone vs intravenous alteplase plus endovascular treatment on functional independence in patients with acute ischemic stroke: the DEVT randomized clinical trial. JAMA. 2021;325:234–243. doi:10.1001/jama.2020.23523
4. Coutinho JM, Liebeskind DS, Slater L-A, et al. Combined intravenous thrombolysis and thrombectomy vs thrombectomy alone for acute ischemic stroke: a pooled analysis of the SWIFT and STAR studies. JAMA Neurol. 2017;74:268–274. doi:10.1001/jamaneurol.2016.5374
5. Bracard S, Ducrocq X, Mas JL, THRACE investigators, et al. Mechanical thrombectomy after intravenous alteplase versus alteplase alone after stroke (THRACE): a randomised controlled trial. Lancet Neurol. 2016;15:1138–1147. doi:10.1016/S1474-4422(16)30177-6
6. Powers WJ, Rabinstein AA, Ackerson T, et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 update to the 2018 Guidelines for the early management of acute ischemic stroke: a guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2019;50:e344–e418. doi:10.1161/STR.0000000000000211
7. Turc G, Tsivgoulis G, Audebert HJ, et al. European Stroke Organisation (ESO)–European Society for Minimally Invasive Neurological Therapy (ESMINT) expedited recommendation on indication for intravenous thrombolysis before mechanical thrombectomy in patients with acute ischemic stroke and anterior circulation large vessel occlusion. J NeuroIntervent Surg. 2022;14:209–227. doi:10.1136/neurintsurg-2021-018589.
8. Joundi RA, Menon BK. Thrombus composition, imaging, and outcome prediction in acute ischemic stroke. Neurology. 2021;97:S68–S78. doi:10.1212/WNL.0000000000012796.
9. Tsivgoulis G. Intravenous thrombolysis for ischemic stroke in the golden hour: propensity-matched analysis from the SITS-EAST registry. J Neurol. 2017;264:912–920. doi:10.1007/s00415-017-8461-8
10. Tsivgoulis G, Saqqur M, Sharma VK, et al. Timing of recanalization and functional recovery in acute ischemic stroke. J Stroke. 2020;22:130–140. doi:10.5853/jos.2019.01648
11. Cines DB, Lebedeva T, Nagaswami C, et al. Clot contraction: compression of erythrocytes into tightly packed polyhedra and redistribution of platelets and fibrin. Blood. 2014;123:1596–1603. doi:10.1182/blood-2013-08-523860
12. Kaesmacher J, Cavalcante F, Kappelhof M, et al. Time to treatment with intravenous thrombolysis before thrombectomy and functional outcomes in acute ischemic stroke: a meta-analysis. JAMA. 2024;331:764. doi:10.1001/jama.2024.0589
13. Sebastian IA, Hill MD. In ischemic stroke, adding IV thrombolysis ≤2 h after symptom onset to thrombectomy was associated with benefit. Ann Intern Med. 2024;
14. Man S, Solomon N, Mac Grory B, et al. Shorter door-to-needle times are associated with better outcomes after intravenous thrombolytic therapy and endovascular thrombectomy for acute ischemic stroke. Circulation. 2023;148:20–34. doi:10.1161/CIRCULATIONAHA.123.064053
15. Venema E, Groot AE, Lingsma HF, et al. Effect of interhospital transfer on endovascular treatment for acute ischemic stroke. Stroke. 2019;50:923–930. doi:10.1161/STROKEAHA.118.024091
16. Froehler MT, Saver JL, Zaidat OO, et al. Interhospital transfer before thrombectomy is associated with delayed treatment and worse outcome in the STRATIS registry (systematic evaluation of patients treated with neurothrombectomy devices for acute ischemic stroke). Circulation. 2017;136:2311–2321. doi:10.1161/CIRCULATIONAHA.117.028920
17. Ueda T, Hasegawa Y, Takeuchi M, et al. Primary results of mechanical thrombectomy for acute ischemic stroke: the K-NET registry in the Japanese metropolitan area. Int J Stroke. 2023;18:607–614. doi:10.1177/17474930221138014
18. Emberson J, Lees KR, Lyden P, et al. Effect of treatment delay, age, and stroke severity on the effects of intravenous thrombolysis with alteplase for acute ischaemic stroke: a meta-analysis of individual patient data from randomised trials. Lancet. 2014;384:1929–1935. doi:10.1016/S0140-6736(14)60584-5
19. Akbik F, Alawieh A, Dimisko L, et al. Bridging thrombolysis in atrial fibrillation stroke is associated with increased hemorrhagic complications without improved outcomes. J NeuroIntervent Surg. 2022;14:979–984. doi:10.1136/neurintsurg-2021-017954
20. Zhou Y, Zhang L, Cavalcante F, et al. Intracranial hemorrhage in patients with stroke after endovascular treatment with or without iv alteplase: an individual participant data meta-analysis. JAMA Neurol. 2025;82:1031. doi:10.1001/jamaneurol.2025.2610
21. Shen H, Killingsworth MC, Bhaskar SMM. Comprehensive meta-analysis of futile recanalization in acute ischemic stroke patients undergoing endovascular thrombectomy: prevalence, factors, and clinical outcomes. Life. 2023;13:1965. doi:10.3390/life13101965
22. Zhang Y, Jiang M, Gao Y, et al. “No-reflow” phenomenon in acute ischemic stroke. J Cereb Blood Flow Metab. 2024;44:19–37. doi:10.1177/0271678X231208476
23. Ng FC, Churilov L, Yassi N, et al. Prevalence and significance of impaired microvascular tissue reperfusion despite macrovascular angiographic reperfusion (no-reflow). Neurology. 2022;22:98. doi:10.1186/s12883-022-02607-3
24. Renú A, Millán M, San Román L, et al. Effect of intra-arterial alteplase vs placebo following successful thrombectomy on functional outcomes in patients with large vessel occlusion acute ischemic stroke: the CHOICE randomized clinical trial. JAMA. 2022;327:826. doi:10.1001/jama.2022.1645
25. Maekawa K, Shibata M, Nakajima H, et al. Erythrocyte-rich thrombus is associated with reduced number of maneuvers and procedure time in patients with acute ischemic stroke undergoing mechanical thrombectomy. Cerebrovasc Dis Extra. 2018;8:39–49. doi:10.1159/000486042
26. Sporns PB, Jeibmann A, Minnerup J, et al. Histological clot composition is associated with preinterventional clot migration in acute stroke patients. Stroke. 2019;50:2065–2071. doi:10.1161/STROKEAHA.118.023314
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Relationship Between Neuron-Specific Enolase and Clinical Outcomes in Patients Undergoing Mechanical Thrombectomy
Peng Q, Chen W, E Y, Deng Y, Xu Z, Wang S, Fu X, Wei B, Wang M, Hou J, Zhang Y, Duan R
Neuropsychiatric Disease and Treatment 2023, 19:709-719
Published Date: 4 April 2023
Correlation of Atherosclerotic Dyslipidemia with Long-Term Stroke Recurrence in Patients Undergoing Intravenous Thrombolysis for Acute Ischemic Stroke
Cheng Y, Wang Q, Niu G, Luo C
International Journal of General Medicine 2023, 16:1621-1629
Published Date: 2 May 2023
Association Between Inflammatory Burden Index and Unfavorable Prognosis After Endovascular Thrombectomy in Acute Ischemic Stroke
Du M, Xu L, Zhang X, Huang X, Cao H, Qiu F, Lan W, Jiang H
Journal of Inflammation Research 2023, 16:3009-3017
Published Date: 19 July 2023
Glial Fibrillary Acidic Protein Levels in Post-Stroke Depression: A Prospective Ischemic Stroke Cohort
Shan W, Zhao J, Qiu C, Xu G, Feng J
Neuropsychiatric Disease and Treatment 2023, 19:2171-2178
Published Date: 18 October 2023
A Novel Nomogram to Predict Symptomatic Intracranial Hemorrhage in Ischemic Stroke Patients After Intravenous Thrombolysis
Jiang Z, Xu D, Li H, Wu X
Therapeutics and Clinical Risk Management 2023, 19:993-1003
Published Date: 29 November 2023