Back to Journals » Cancer Management and Research » Volume 17

C-Reactive Protein in Immune Checkpoint Inhibitor-Associated Colitis: A Scoping Review of Evidence and Knowledge Gaps
Authors Ohta R ![]() , Ryu Y, Tanaka K
, Ryu Y, Tanaka K ![]() , Sano C, Hayashi H
, Sano C, Hayashi H ![]()
Received 23 July 2025
Accepted for publication 7 October 2025
Published 7 November 2025 Volume 2025:17 Pages 2631—2641
DOI https://doi.org/10.2147/CMAR.S555819
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Harikrishna Nakshatri
Ryuichi Ohta,1– 3 Yoshinori Ryu,1,3 Kaoru Tanaka,2 Chiaki Sano,3 Hidetoshi Hayashi2
1Department of Community Care, Unnan City Hospital, Unnan, Shimane, Japan; 2Department of Medical Oncology, Kindai University Faculty of Medicine, Sayama, Osaka, Japan; 3Community Medicine Management, Shimane University Faculty of Medicine, Izumo, Shimane, Japan
Correspondence: Ryuichi Ohta, Department of Community Care, Unnan City Hospital, Unnan, Shimane, Japan, Email [email protected]
Background: Immune checkpoint inhibitors (ICIs) have transformed cancer care but frequently cause immune-mediated diarrhea and colitis (IMDC), a clinically significant immune-related adverse event. Prompt diagnosis and severity assessment are essential but often rely on invasive endoscopic procedures. C-reactive protein (CRP), a widely available biomarker of systemic inflammation, has been suggested as a potential adjunct in evaluating IMDC. However, its diagnostic utility and clinical relevance remain unclear.
Methods: We conducted a scoping review in accordance with the PRISMA-ScR guideline to map existing evidence and identify knowledge gaps regarding the association between CRP and IMDC. A comprehensive literature search was performed across PubMed, Embase, and Web of Science (January 2010–April 2025). Eligible studies included adult patients receiving ICIs who developed gastrointestinal immune-related adverse events, with reported CRP levels. Data were extracted on study design, patient population, CRP measurement, and its relationship with IMDC diagnosis, severity, or outcomes.
Results: Of 538 records screened, five observational studies comprising 583 patients were included. Only one study specifically analyzed CRP levels in histologically confirmed IMDC, demonstrating a positive correlation with clinical and endoscopic severity but no validated diagnostic thresholds. The remaining studies assessed CRP as a general marker for immune-related adverse events without gastrointestinal-specific analyses or diagnostic accuracy metrics. No study provided sufficient data to establish sensitivity, specificity, or predictive values for CRP in IMDC.
Conclusion: This scoping review highlights the limited and heterogeneous evidence linking CRP to IMDC and underscores the absence of validated thresholds or diagnostic performance data. For generalist physicians, CRP may serve as a supportive marker to prompt further evaluation but cannot replace established diagnostic pathways. Future prospective studies should integrate CRP with organ-specific biomarkers and standardized endpoints to clarify its role in triage and severity assessment of IMDC.
Keywords: C-reactive protein, colitis, immune checkpoint inhibitors, biomarkers, immune-related adverse events, scoping review
Introduction
Immune checkpoint inhibitors (ICIs), including monoclonal antibodies targeting programmed death-1 (PD-1), programmed death-ligand 1 (PD-L1), and cytotoxic T lymphocyte antigen-4 (CTLA-4), have revolutionized the treatment of various malignancies such as melanoma, lung cancer, renal cell carcinoma, and hepatocellular carcinoma.1 By disrupting inhibitory pathways in T-cell activation, ICIs restore anti-tumor immune responses and provide durable clinical benefits for a substantial subset of patients.2
As the use of ICIs expands into community oncology and general practice settings, non-specialist physicians are increasingly expected to recognize and triage immune-related adverse events (irAEs), including immune-mediated colitis, resulting from nonspecific immune activation against self-antigens.3 Gastrointestinal irAEs, particularly immune-mediated diarrhea and colitis (IMDC), occur in up to 30% of patients, especially with anti-CTLA-4 agents or combination ICI therapy.4 While mild cases may resolve spontaneously, moderate to severe IMDC can be life-threatening and often requires immunosuppressive treatment, such as corticosteroids or biologics like infliximab or vedolizumab.4,5 Prompt diagnosis and grading of severity are therefore essential to avoid complications, reduce morbidity, and allow safe continuation of cancer therapy when possible. Recent studies further support the importance of colitis as a high-risk irAE subtype. For example, a recent publication reported that patients who developed colitis during ICI therapy had a higher risk of irAE recurrence upon ICI reinitiation compared to patients with other irAEs.6 This underscores the clinical significance of IMDC in the management of ICI-related toxicities.
Current diagnostic strategies rely heavily on clinical assessment, endoscopic evaluation, and histologic confirmation.7 However, endoscopy is invasive, resource-intensive, and may not be readily available in all clinical settings, particularly for acutely ill patients. Consequently, there is increasing interest in identifying reliable, non-invasive biomarkers that can aid in the early detection and monitoring of IMDC.2
C-reactive protein (CRP), an acute-phase reactant produced by hepatocytes in response to interleukin-6 (IL-6), is commonly used in routine oncology practice to evaluate systemic inflammation and infection.8 Several studies have suggested that CRP levels may be elevated during irAEs, including gastrointestinal manifestations, and could correlate with disease severity.9,10 However, most of these studies have focused on CRP as a general marker of irAE risk rather than organ-specific events, and only a limited number have examined gastrointestinal manifestations directly. This underscores the importance of clarifying CRP’s potential role in IMDC within the broader context of its use as a biomarker in ICI therapy.
Given the widespread availability of CRP and its rapid turnaround time, clarifying its potential role in IMDC could have significant clinical implications. If better understood, CRP might be used as a triage tool to prioritize patients for endoscopy, guide early treatment decisions, or monitor disease progression and response to therapy.11 This scoping review aims to map the existing literature on serum CRP in the context of immune checkpoint inhibitor-associated colitis, summarize the extent and nature of available evidence, and identify key knowledge gaps to guide future research.
Methods
Protocol and Registration
This scoping review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) guideline.12 The review protocol was prospectively registered in the International Prospective Register of Systematic Reviews (PROSPERO; Registration ID: CRD420251054606). The protocol specified the research objectives, eligibility criteria, data charting process, and synthesis approach.
Eligibility Criteria and Search Strategy
We included original peer-reviewed research articles reporting adult patients (≥18 years) treated with ICIs—specifically agents targeting PD-1, PD-L1, or CTLA-4—who developed gastrointestinal immune-related adverse events (irAEs), particularly immune-mediated diarrhea and colitis (IMDC). Studies were eligible if they reported serum CRP levels in relation to:
- The diagnosis or presence of IMDC,
- Assessment of disease severity (clinical, endoscopic, or histologic), or
- Clinical outcomes such as treatment response or recurrence.
We included retrospective and prospective observational cohort studies, case–control studies, interventional trials, and case series with ≥5 patients. No restrictions were placed on tumor type, ICI regimen (monotherapy vs combination), or line of therapy.
We excluded studies that:
- Did not report CRP levels separately for IMDC,
- Focused solely on irAEs involving other organs (eg, hepatitis, pneumonitis, endocrinopathies),
- Were reviews, commentaries, conference abstracts, or letters to the editor, or
- Were unavailable in English.
A comprehensive literature search was conducted on April 23, 2025, across PubMed (MEDLINE), Embase, and Web of Science. Search terms combined Medical Subject Headings (MeSH) and free-text terms related to ICIs, gastrointestinal irAEs, and biomarkers (eg, “immune checkpoint inhibitor”, “immune-related colitis”, “immune-mediated diarrhea”, “C-reactive protein”, “biomarker”). Boolean operators (AND, OR) were used to combine terms appropriately. The search covered publications from January 2010 to April 2025, reflecting the clinical adoption timeline of ICIs. Reference lists of included articles and relevant reviews were manually screened to identify additional eligible studies. Detailed database-specific search strategies and the number of records retrieved per database are provided in Supplementary Material 1.
Study Selection and Data Charting
All search results were imported into a reference management tool, and duplicate records were removed automatically and manually. Two reviewers (RO and YR) independently screened titles and abstracts according to predefined eligibility criteria. Full texts of potentially eligible studies were retrieved and assessed for inclusion. Disagreements were resolved by discussion or, if necessary, by a third reviewer (KT).
A standardized data charting form (Microsoft Excel) was developed and pilot-tested prior to full implementation. The following key information was extracted from each included study:
- General study characteristics (first author, publication year, country, study design),
- Cancer type(s) and ICI regimens,
- Number of patients and proportion with IMDC,
- Timing and method of CRP measurement,
- Reported CRP levels (mean, median, range) and any proposed diagnostic cut-off values,
- Main findings related to CRP and IMDC diagnosis, severity, or outcomes.
When studies included multiple cohorts or subgroups, data were extracted separately when possible.
Methodological Quality
Since the objective of this review was to map the extent and nature of evidence rather than appraise study quality for meta-analysis, formal risk-of-bias assessment was not mandatory. However, to provide context on the robustness of the evidence, we briefly summarized study design features and potential limitations (eg, retrospective design, lack of standardized IMDC definitions, small sample size).
Synthesis of Results
As this scoping review aimed to describe and map the existing evidence rather than statistically synthesize findings, no quantitative meta-analysis was performed.
- We summarized the number and type of studies available,
- Mapped the reported associations between CRP and IMDC presence or severity,
- Highlighted any proposed CRP thresholds for predicting IMDC or other irAEs,
- Identified key knowledge gaps and directions for future research.
Due to heterogeneity in study designs, patient populations, ICI regimens, timing of CRP measurement, and outcome reporting, diagnostic accuracy metrics (eg, sensitivity, specificity, ROC curves) could not be pooled.
Results
Study Selection
Database searches identified 538 records (205 from Embase, 167 from PubMed, 166 from Web of Science). After removing 129 duplicates, 409 unique records remained for title and abstract screening. During initial screening, 390 studies were excluded as unrelated to the review objectives. Of the remaining 19 full-text articles, 14 were excluded due to wrong outcomes (n = 7), inappropriate study design (n = 5), unrelated intervention (n = 1), or mismatched patient population (n = 1).
Ultimately, five studies were included in this scoping review, comprising observational cohort analyses across multiple cancer types. Only one study specifically focused on IMDC, while the others reported CRP in the broader context of immune-related adverse events (irAEs). Figure 1 presents the PRISMA-ScR flow diagram for study selection.
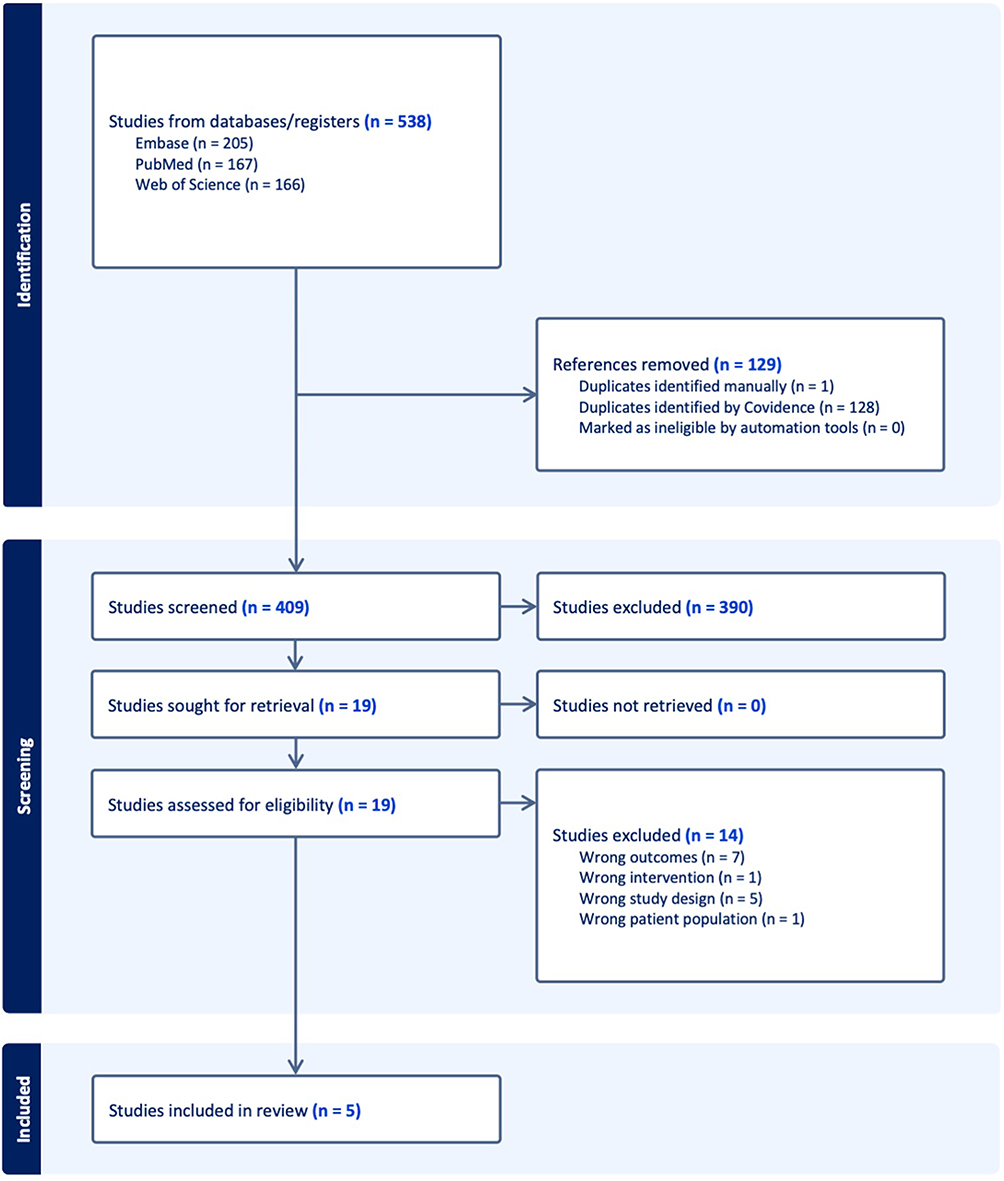 |
Figure 1 PRISMA-ScR flow diagram inserted here. Flow diagram outlining the identification, screening, eligibility assessment, and inclusion of studies in the scoping review. The diagram illustrates the number of records identified through database searches, the number of duplicates removed, the records screened and excluded, the full-text articles assessed for eligibility, and the studies included in the final qualitative synthesis. |
Study Characteristics
The five included studies encompassed a total of 583 patients treated with ICIs, of whom a subset developed gastrointestinal irAEs, including IMDC. Four studies were retrospective cohorts, and one was a prospective observational study. Cancer types included melanoma, non-small cell lung cancer (NSCLC), hepatocellular carcinoma (HCC), and mixed solid tumors. No randomized trials or prospective biomarker validation studies were identified. A descriptive summary of study characteristics and key findings is presented in Table 1.
 |
Table 1 Summary of Studies Included in the Systematic Review Assessing the Association Between C-Reactive Protein and Immune-Related Colitis |
Mapping of CRP Evidence in IMDC
Only one study (Liu et al, 2023) specifically analyzed CRP levels in histologically confirmed IMDC. In this cohort of 128 patients, CRP levels measured at diagnosis correlated significantly with diarrhea grade (p = 0.015), colitis grade (p = 0.013), and endoscopic severity (p = 0.016). However, no associations were found between baseline CRP and clinical or endoscopic remission or recurrence after immunosuppressive therapy. Importantly, no validated diagnostic thresholds or formal diagnostic accuracy metrics (sensitivity, specificity, ROC curves) were reported. This finding suggests CRP may reflect initial disease burden in IMDC but lacks discriminatory value for predicting treatment response or long-term outcomes (Table 2).
 |
Table 2 Association Between Serum CRP Levels and IMDC Parameters in Liu et al (2023) |
CRP as a General Biomarker for irAE Risk
Several included studies evaluated CRP as a baseline predictor of overall irAE risk rather than organ-specific events. For example, Onodera et al (2023) found that baseline CRP > 1.0 mg/dL predicted irAE development (OR = 2.41) and poorer survival in NSCLC patients, whereas Yu et al (2022) proposed a threshold of ≥0.82 mg/dL for predicting irAEs in HCC patients treated with ICIs plus TKIs. However, neither study provided gastrointestinal-specific analyses nor validated diagnostic thresholds. Similarly, Husain et al (2021) observed dynamic CRP increases during irAE onset (0.7 → 1.77 mg/dL), but subgroup analyses for GI-irAEs were not performed (Table 3).
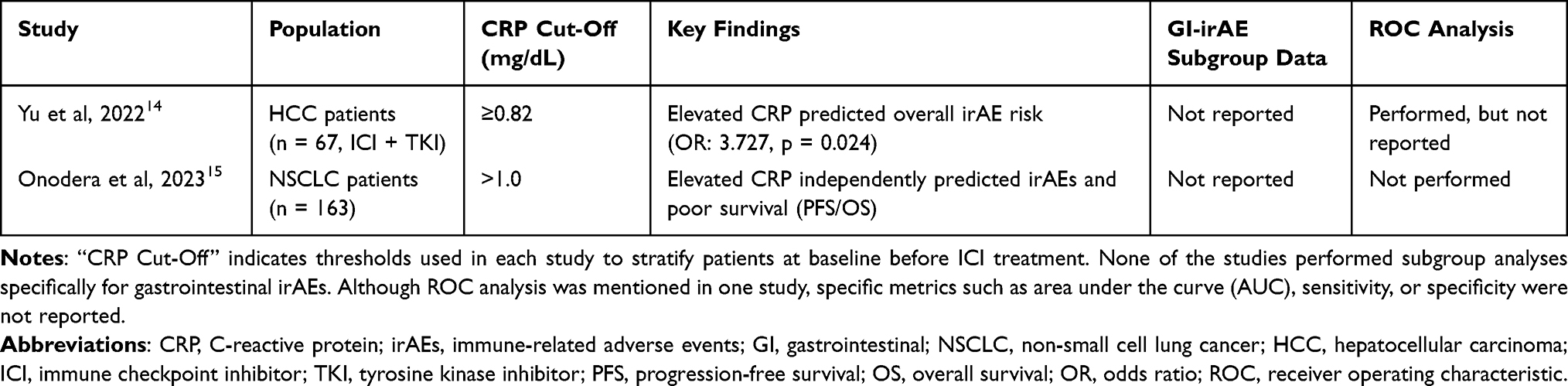 |
Table 3 Summary of Studies Evaluating Baseline CRP as a Predictor of General irAE Risk |
Knowledge Gaps on CRP Thresholds and Diagnostic Performance
Across all included studies, proposed CRP thresholds ranged from 0.82 mg/dL to 1.0 mg/dL for predicting general irAEs, but no validated cut-off specific to IMDC was identified. Furthermore, none of the studies reported complete 2×2 diagnostic data to allow calculation of sensitivity, specificity, or predictive values for IMDC.
This lack of validated diagnostic performance data highlights a critical gap and underscores the need for prospective studies focused on gastrointestinal-specific irAEs (Table 4).
 |
Table 4 Summary of Dynamic Changes in Serum CRP During irAE Onset in Husain et al (2021) |
Methodological Limitations
Most included studies were small retrospective cohorts with heterogeneous populations and varied definitions of irAEs. None was designed as prospective biomarker validation studies. Standardized timing of CRP measurement, organ-specific endpoints, and blinded outcome assessments were lacking. These methodological gaps limit the interpretability of current evidence and emphasize the need for prospective, multicenter validation of CRP in IMDC (Table 5).
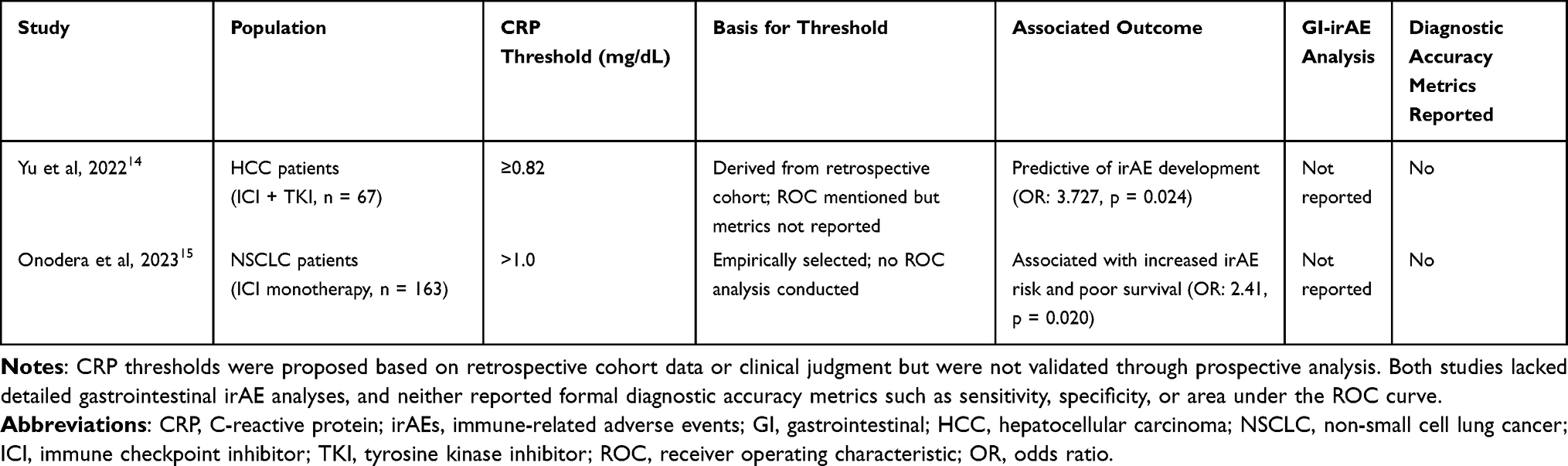 |
Table 5 Reported CRP Thresholds and Associated Diagnostic Contexts for Predicting Immune-Related Adverse Events |
Key Takeaway from Evidence Mapping
This scoping review identified only one IMDC-specific study and four broader irAE studies evaluating CRP. Collectively, current evidence is sparse, heterogeneous, and insufficient to inform clinical decision-making for IMDC. Future research should prioritize organ-specific analyses, standardized diagnostic criteria, and integration of CRP with fecal and endoscopic biomarkers.
Discussion
Summary of Main Findings
This scoping review mapped the available evidence on serum C-reactive protein (CRP) in the context of immune checkpoint inhibitor-associated colitis (IMDC). Across five observational studies involving 583 patients, only one directly examined CRP in histologically confirmed IMDC. This study demonstrated a significant correlation between elevated CRP levels and IMDC severity, including diarrhea grade, colitis grade, and endoscopic findings.13 However, no associations were observed with treatment response or recurrence.
The remaining studies evaluated CRP as a general biomarker for immune-related adverse events (irAEs) without gastrointestinal-specific analyses. Two studies proposed thresholds for predicting irAEs (≥0.82 mg/dL and >1.0 mg/dL),14,15 but none validated a colitis-specific cut-off or reported robust diagnostic accuracy metrics such as sensitivity, specificity, or AUC.
Collectively, these findings indicate that current evidence is sparse, heterogeneous, and insufficient to inform the diagnostic role of CRP in IMDC. Beyond its potential diagnostic application, recent literature has also emphasized the prognostic utility of CRP in the context of ICI therapy. For example, a recent study demonstrated that serial CRP measurements may provide prognostic information regarding treatment outcomes.17 This broader perspective suggests that while CRP lacks specificity for IMDC, it may still have clinical value when integrated into dynamic biomarker strategies to monitor systemic inflammation and therapeutic trajectories during ICI therapy.
Comparison with Previous Literature
These findings are consistent with prior reports showing that systemic inflammatory markers, including CRP, often rise during irAE onset, likely reflecting activation of pro-inflammatory cytokine pathways. Husain et al demonstrated a significant increase in CRP from a baseline of 0.7 mg/dL to 1.77 mg/dL during irAE onset, a change paralleled by increased IL-6 concentrations.16 This supports the mechanistic role of IL-6–driven hepatic CRP synthesis during immune activation induced by checkpoint blockade.18 Similar CRP elevations have been observed in other immunotherapy settings, reinforcing its biological plausibility as a marker of systemic immune activation.9,19
However, the literature remains inconclusive regarding CRP’s diagnostic specificity for IMDC. Unlike fecal biomarkers such as calprotectin or lactoferrin, which directly reflect gastrointestinal mucosal inflammation, CRP is a systemic marker elevated in diverse conditions—including infections, tumor progression, and irAEs affecting other organs (eg, pneumonitis or hepatitis).20,21 This lack of organ specificity limits CRP’s ability to distinguish IMDC from other inflammatory processes in ICI-treated patients.
Additionally, most studies failed to use standardized endoscopic or histopathological confirmation of colitis, making it unclear whether elevated CRP reliably reflects true mucosal inflammation. Without validated scoring systems for gastrointestinal pathology—such as mucosal ulceration or histologic infiltration—CRP cannot be confidently interpreted as a surrogate for colonic activity.22,23 Heterogeneity in study design, timing of CRP measurement, ICI regimens, and outcome definitions further impedes comparability and integration into clinical diagnostic algorithms.22,24
Knowledge Gaps and Implications for Research
This review highlights key knowledge gaps:
- Scarcity of IMDC-specific evidence: Only one study focused exclusively on CRP in confirmed IMDC.14
- No validated gastrointestinal-specific CRP thresholds: Proposed cut-offs for general irAEs14,15 lack organ-specific validation.
- Absence of diagnostic accuracy metrics: No included study provided sensitivity, specificity, ROC analyses, or predictive values.
- Limited biomarker integration: No studies combined CRP with fecal or endoscopic biomarkers to enhance specificity.
Addressing these gaps requires prospective multicenter studies with harmonized definitions of IMDC, standardized timing of CRP measurement, and organ-specific subgroup analyses. Future research should explore CRP as part of a multimodal biomarker panel—integrating fecal calprotectin, lactoferrin, and cytokine profiling—to improve diagnostic precision.
Clinical Implications
CRP is inexpensive, widely available, and routinely measured in oncology practice, making it a potentially useful supportive marker for evaluating suspected IMDC.25,26 Its correlation with colitis severity in Liu et al suggests it could prompt more urgent investigation when gastrointestinal symptoms arise.13,27 For generalist physicians, CRP may help prioritize patients for endoscopy or early immunosuppressive treatment when invasive testing is delayed or contraindicated.28
However, current evidence does not support CRP as a standalone diagnostic tool. Its low specificity for gastrointestinal inflammation and lack of validated thresholds prevent it from replacing established diagnostic pathways, which should continue to rely on clinical, endoscopic, and histopathological evaluation. Consistent with this observation, a recent publication demonstrated that CRP did not predict irAE recurrence, underscoring its limitations as a biomarker in the longitudinal management of ICI-related toxicities.6 Together, these findings suggest that although CRP may serve as a supportive marker of acute disease severity, its utility in predicting recurrence or guiding reinitiation of ICI therapy remains limited.
Limitations of the Evidence Base
The evidence mapped in this scoping review has several limitations. Only one study addressed histologically confirmed IMDC directly. None of the included studies systematically evaluated diagnostic accuracy or reported sensitivity, specificity, or likelihood ratios. Most were small retrospective cohorts with heterogeneous patient populations, variable definitions of outcomes, and inconsistent timing of CRP measurements. Publication bias may also favor studies reporting positive associations. This limitation is further underscored by the fact that only one of the five included studies specifically assessed CRP in histologically confirmed IMDC. In contrast, the remaining studies evaluated CRP in the broader context of irAEs without gastrointestinal-specific analyses. As such, our review contributes to understanding the narrow evidence base for CRP in IMDC but should be interpreted within the broader literature that shows CRP as a nonspecific marker of systemic immune activation during ICI therapy.
As a scoping review, we aimed to map the extent and nature of available evidence rather than formally appraise study quality or perform meta-analysis, so these findings should be interpreted as an overview of the current evidence landscape rather than definitive conclusions on diagnostic performance.
Future Directions
Future research should prioritize prospective validation studies with standardized CRP measurement timing and harmonized IMDC diagnostic criteria, integration of CRP with fecal biomarkers and cytokine profiling to improve specificity for gastrointestinal irAEs, establishment of validated IMDC-specific CRP thresholds using ROC analyses and stratification by severity grade, and development of multivariable diagnostic models combining CRP with clinical, endoscopic, and histologic findings to guide triage and management in ICI-treated patients.
Conclusions
This scoping review reveals a substantial evidence gap regarding CRP’s diagnostic and prognostic utility in ICI-associated colitis. While CRP appears to correlate with IMDC severity in one study, its lack of organ specificity and the absence of validated thresholds limit its clinical utility. Mapping this limited and heterogeneous evidence underscores the need for prospective organ-specific biomarker studies to define CRP’s role within a multimodal diagnostic strategy for IMDC.
Data Sharing Statement
This study is a systematic review based on previously published articles. No new data were generated or analyzed.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
Dr Kaoru Tanaka reports personal fees from Astrazeneca, Bristol-Myers Squibb, ONO PHARMACEUTICAL, MSD, CHUGAI PHARMACEUTICAL, Eisai, Novartis Pharma, Taiho Pharmaceutical, outside the submitted work. Professor Hidetoshi Hayashi reports grants/personal fees from Ono Pharmaceutical Co., Ltd., Eli Lilly Japan K.K., Merck Biopharma Co., Ltd., Daiichi Sankyo Co., Ltd., AstraZeneca K.K., MSD K.K., Sysmex Corporation, AbbVie Inc., Kyowa Kirin Co., Ltd, Reno. Medical K.K., Nippon Kayaku Co., Ltd., 3H Clinical Trial Inc., Novartis Pharma K.K., Pfizer Japan Inc., Amgen Inc., Eisai Co., Ltd., CareNet, Inc., Novocure K.K, Bristol Myers Squibb Company, Takeda Pharmaceutical Co., Ltd., Chugai Pharmaceutical Co., Ltd, Nippon Boehringer Ingelheim Co., Ltd., Janssen Pharmaceutical K.K., Taiho Pharmaceutical Co., Ltd., Hisamitsu Pharmaceutical Co., Inc., IQVIA Services JAPAN K.K., SYNEOS HEALTH CLINICAL K.K., EPS Corporation, CMIC CO., Ltd., Pfizer R&D Japan G.K., Labcorp Development Japan K.K., Kobayashi Pharmaceutical Co., Ltd., A2 Healthcare Corp., Medpace Japan KK, PPD-SNBL K.K, Mochida Pharmaceutical Co., Ltd., EP-CRSU CO., LTD., Shionogi & Co., Ltd., Otsuka Pharmaceutical Co., Ltd., GlaxoSmithKline K.K., Sanofi K.K., SRL Medisearch Inc., PRA Health Sciences Inc., Astellas Pharma Inc., Ascent Development Services, Eisai Inc., Bayer Yakuhin, Ltd, ICON Japan K.K., Clinical Research Support Center Kyushu, Public Health Research Foundation, Japanese Gastric Cancer Association, Aichi Cancer Network, Japan Clinical Cancer Research Organization, Kyushu Study group of Clinical Cancer, Thoracic Oncology Research Group, West Japan Oncology Group, Comprehensive Support Project for Oncological Research of Breast Cancer, outside the submitted work. The other authors declare no conflicts of interest for this article.
References
1. Pardoll DM. The blockade of immune checkpoints in cancer immunotherapy. Nat Rev Cancer. 2012;12(4):252–264. doi:10.1038/nrc3239
2. Schneider BJ, Naidoo J, Santomasso BD, et al. Management of immune-related adverse events in patients treated with immune checkpoint inhibitor therapy: ASCO guideline update. J Clin Oncol. 2021;39(36):4073–4126. doi:10.1200/JCO.21.01440
3. Shatila M, Zhang HC, Shirwaikar Thomas A, et al. Systematic review of immune checkpoint inhibitor-related gastrointestinal, hepatobiliary, and pancreatic adverse events. J Immunother Cancer. 2024;12(11):e009742. doi:10.1136/jitc-2024-009742
4. Sleiman J, Wei W, Shah R, Faisal MS, Philpott J, Funchain P. Incidence of immune checkpoint inhibitor-mediated diarrhea and colitis (imDC) in patients with cancer and preexisting inflammatory bowel disease: a propensity score-matched retrospective study. J Immunother Cancer. 2021;9(6):e002567. doi:10.1136/jitc-2021-002567
5. Zoghbi M, Burk KJ, Haroun E, Saade M, Carreras MTC. Immune checkpoint inhibitor-induced diarrhea and colitis: an overview. Support Care Cancer. 2024;32(10):680. doi:10.1007/s00520-024-08889-2
6. Acar C, Yüksel H, Şahin G, Açar FP, Karaca B. Immune checkpoint inhibitor resumption after discontinuation due to immune-related adverse events: a nomogram-based analysis of risk factors and outcomes. Expert Rev Anticancer Ther. 2025;25(8):983–991. doi:10.1080/14737140.2025.2517274
7. Giesler S, Riemer R, Lowinus T, Zeiser R. Immune-mediated colitis after immune checkpoint inhibitor therapy. Trends Mol Med. 2025;31(3):265–280. doi:10.1016/j.molmed.2024.09.009
8. Lauwyck J, Beckwée A, Santens A, et al. C-reactive protein as a biomarker for immune-related adverse events in melanoma patients treated with immune checkpoint inhibitors in the adjuvant setting. Melanoma Res. 2021;31(4):371–377. doi:10.1097/CMR.0000000000000748
9. Mouliou DS. C-reactive protein: pathophysiology, diagnosis, false test results and a novel diagnostic algorithm for clinicians. Diseases. 2023;11(4).
10. Yeung SJ, Qdaisat A, Bischof JJ, Caterino JM, Kyriacou DN, Coyne Md C. A case series of adrenal insufficiency (likely due to hypophysitis) in cancer patients treated with immune checkpoint inhibitors. Am J Emerg Med. 2024;80:227.e1–e5. doi:10.1016/j.ajem.2024.04.046
11. Abolhassani AR, Schuler G, Kirchberger MC, Heinzerling L. C-reactive protein as an early marker of immune-related adverse events. J Cancer Res Clin Oncol. 2019;145(10):2625–2631. doi:10.1007/s00432-019-03002-1
12. Matthew JP, Joanne EM, Patrick MB, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
13. Liu C, Shatila M, Mathew A, et al. Role of C-reactive protein in predicting the severity and response of immune-mediated diarrhea and colitis in patients with cancer. J Cancer. 2023;14(10):1913–1919. doi:10.7150/jca.84261
14. Yu Y, Wang S, Su N, et al. Increased circulating levels of CRP and IL-6 and decreased frequencies of T and B lymphocyte subsets are associated with immune-related adverse events during combination therapy with PD-1 inhibitors for liver cancer. Front Oncol. 2022;12:906824. doi:10.3389/fonc.2022.906824
15. Onodera R, Chiba S, Nihei S, et al. High level of C-reactive protein as a predictive factor for immune-related adverse events of immune checkpoint inhibitors in non-small cell lung cancer: a retrospective study. J Thorac Dis. 2023;15(8):4237–4247. doi:10.21037/jtd-23-85
16. Husain B, Kirchberger MC, Erdmann M, et al. Inflammatory markers in autoimmunity induced by checkpoint inhibitors. J Cancer Res Clin Oncol. 2021;147(6):1623–1630. doi:10.1007/s00432-021-03550-5
17. Acar C, Yüksel H, Şahin G, et al. C-reactive protein kinetics as prognostic biomarkers in advanced melanoma treated with immune checkpoint inhibitors. Melanoma Res. 2025;35(4):232–241. doi:10.1097/CMR.0000000000001039
18. Naqash AR, McCallen JD, Mi E, et al. Increased interleukin-6/C-reactive protein levels are associated with the upregulation of the adenosine pathway and serve as potential markers of therapeutic resistance to immune checkpoint inhibitor-based therapies in non-small cell lung cancer. J Immunother Cancer. 2023;11(10):e007310. doi:10.1136/jitc-2023-007310
19. Enocsson H, Karlsson J, Li HY, et al. The complex role of C-reactive protein in systemic lupus erythematosus. J Clin Med. 2021;10(24):5837. doi:10.3390/jcm10245837
20. Rubio MG, Amo-Mensah K, Gray JM, et al. Fecal lactoferrin accurately reflects mucosal inflammation in inflammatory bowel disease. World J Gastrointest Pathophysiol. 2019;10(5):54–63. doi:10.4291/wjgp.v10.i5.54
21. Jia X-H, Geng L-Y, Jiang -P-P, et al. The biomarkers related to immune related adverse events caused by immune checkpoint inhibitors. J Exp Clin Cancer Res. 2020;39(1):284. doi:10.1186/s13046-020-01749-x
22. Rosenberg L, Nanda KS, Zenlea T, et al. Histologic markers of inflammation in patients with ulcerative colitis in clinical remission. Clin Gastroenterol Hepatol. 2013;11(8):991–996. doi:10.1016/j.cgh.2013.02.030
23. Vespa E, D’Amico F, Sollai M, et al. Histological scores in patients with inflammatory bowel diseases: the state of the art. J Clin Med. 2022;11(4):939. doi:10.3390/jcm11040939
24. Stares M, Ding TE, Stratton C, et al. Biomarkers of systemic inflammation predict survival with first-line immune checkpoint inhibitors in non-small-cell lung cancer. ESMO Open. 2022;7(2):100445. doi:10.1016/j.esmoop.2022.100445
25. Koch A, Fohlin H, Sörenson S. Prognostic significance of C-reactive protein and smoking in patients with advanced non-small cell lung cancer treated with first-line palliative chemotherapy. J Thorac Oncol. 2009;4(3):326–332. doi:10.1097/JTO.0b013e31819578c8
26. Asegaonkar SB, Asegaonkar BN, Takalkar UV, Advani S, Thorat AP. C-reactive protein and breast cancer: new insights from old molecule. Int J Breast Cancer. 2015;2015:145647. doi:10.1155/2015/145647
27. Li F, He M, Zhou M, et al. Association of C-reactive protein with mortality in Covid-19 patients: a secondary analysis of a cohort study. Sci Rep. 2023;13(1):20361. doi:10.1038/s41598-023-47680-x
28. Reyes-Gibby CC, Caterino JM, Coyne CJ, et al. Immune-related adverse event in the emergency department: methodology of the immune-related emergency disposition index (IrEDi). Emerg Cancer Care. 2024;3(1):1. doi:10.1186/s44201-023-00023-y
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Biologic Therapy for Refractory Immune Checkpoint Inhibitor Colitis
Alorfi NM, Alourfi MM
Biologics: Targets and Therapy 2022, 16:119-127
Published Date: 5 August 2022
A Case of Hepatocellular Carcinoma Successfully Resumed Atezolizumab and Bevacizumab After Associated Grade 3 Diarrhea and Grade 2 Colitis: Case Report and Literature Review
Fuji T, Arai J, Otoyama Y, Nio Y, Sugiura I, Nakajima Y, Kajiwara A, Ichikawa Y, Uozumi S, Shimozuma Y, Uchikoshi M, Sakaki M, Nozawa H, Momo K, Sasaki T, Yoshida H
OncoTargets and Therapy 2022, 15:1281-1288
Published Date: 25 October 2022
Onychopathy Following Durvalumab Treatment for Extensive-Stage Small-Cell Lung Cancer: A Case Report
Zhang C, Wang K, Zhang H, Liu J, Zheng C, Tao J, Lin L, Zhai L
Clinical, Cosmetic and Investigational Dermatology 2023, 16:2429-2432
Published Date: 5 September 2023
Upper Tract Urothelial Carcinoma (UTUC): Prevalence, Impact and Management Challenge
Nally E, Young M, Chauhan V, Wells C, Szabados B, Powles T, Jackson-Spence F
Cancer Management and Research 2024, 16:467-475
Published Date: 17 May 2024
Biological Markers of Musculoskeletal Pain: A Scoping Review
Djade CD, Diorio C, Laurin D, Hessou SPH, Toi AK, Gogovor A, Sidibe A, Ekanmian G, Porgo TV, Zomahoun HTV, Dionne CE
Journal of Pain Research 2024, 17:3355-3369
Published Date: 11 October 2024