Back to Journals » Biologics: Targets and Therapy » Volume 16
Biologic Therapy for Refractory Immune Checkpoint Inhibitor Colitis
Authors Alorfi NM ![]() , Alourfi MM
, Alourfi MM
Received 23 March 2022
Accepted for publication 8 July 2022
Published 5 August 2022 Volume 2022:16 Pages 119—127
DOI https://doi.org/10.2147/BTT.S367675
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Shein-Chung Chow
Nasser M Alorfi,1 Mansour Marzouq Alourfi2,3
1Department of Pharmacology and Toxicology, College of Pharmacy, Umm Al-Qura University, Makkah, Saudi Arabia; 2Internal Medicine Department, King Faisal Medical City for Southern Region, Abha, Saudi Arabia; 3Internal Medicine Department, Khamis Mushait General Hospital, Khamis Mushait, Saudi Arabia
Correspondence: Nasser M Alorfi, Umm Al Qura University, Al Abdeyah, Mecca, 24381, Saudi Arabia, Tel +966500644261, Email [email protected]
Abstract: Immune checkpoint inhibitors (ICI) are treatments for several cancer types. Pathogenesis of ICI-induced colitis is not yet clearly explained as it can be disguised as another form such as inflammatory bowel disease or IBD. Recent studies revealed that ICI-induced colitis is a unique form of colitis wherein the synergy of regulatory T cells with the gut microbiome is involved. Diagnosis of colitis can be done via endoscopic lesions and histopathological methods. A patient with colitis can be compared with someone who has IBD. Initial treatment is a corticosteroid. Cooperation between gastroenterologists and oncologists is required to understand further the complete diagnosis and management of different behaviors of ICI-induced colitis. Although immunotherapy provides breakthroughs in treating cancer, adverse effects cannot be prevented and have to be carefully addressed. This study aimed to discuss different biologic therapeutic perspectives in treating refractory immune checkpoint inhibitor-induced colitis. This review provided guidelines, challenges, and suggested protocols for drug immunosuppression.
Keywords: biologics, colitis, immune checkpoint inhibitors, inflammatory bowel movement, diarrhea, oncology, gastroenterology
Introduction: Disease Definition, Epidemiology, and Risk Factors
Definition
Diarrhea, as defined by the American Society of Clinical Oncology (ASCO), is associated with a symptomatic presentation of more than three moist bowel activities in 24 hours. On the other hand, colitis was established as a disease characterized by persistent abdominal pain, blood in the rectum, and mucus in the stool.1–4 Immune-mediated colitis, on the other hand, can disguise as a regular inflammatory bowel disease due to their resemblance with each other. But it is actually considered an uncommon type of colitis with acute onset characterized by accelerated growth that could potentially lead to further adverse effects like bowel perforation and fatality.1
Epidemiology
Colitis is oncologically defined by clinical manifestation, which poses a significant challenge for gastroenterologists since these symptoms do not necessarily demonstrate colonic inflammation. Colonic inflammation is mucosal ulceration detected endoscopically or showed as white blood cells in feces, increased lactoferrin, or calprotectin in stool. With this confusion, it is essential to identify these emerging disorders to improve treatment and enhance overall survival.1
The prevalence of immune-mediated colitis (IMC) or diarrhea may depend on the drug regimen and dosage. Some studies have identified a 12.1–13.7% occurrence of diarrhea in patients that were treated using anti- PD-1 (program cell death protein-1). On the other hand, there was a 30.2–35.4% incidence for patients administered with anti-CTLA-4 (cytotoxic T-lymphocyte-associated protein-4), while patients that used a combination of both experienced prevalences at 9.4–10.6. Colitis was found to have a prevalence of 0.7–1.6%, 5.7–9.1%, and 13.6% for anti PD-1 treatment, anti-CTLA-4, and combination therapy, respectively.5–8
Immuno-Checkpoint Inhibitors (ICIs)
An anti-CTLA-4 drug, Ipilimumab, is an immuno-checkpoint inhibitor that provides dose-dependent occurrence for both colitis and diarrhea, with 5% and 10% prevalence, respectively, for 10 mg/kg dosage. On the other hand, a 3mg/kg dose obtained a prevalence of 6% and 2% for diarrhea and colitis, respectively. Ipilimumab intends to prolong survival in advanced melanoma. Anti-PD-1 drugs Nivolumab and Pembrolizumab treat melanoma and metastatic NSCLC (non-small cell lung cancer). Metastatic melanoma can also be treated using both ipilimumab and nivolumab. Anti-programmed death-1 drugs Atezolizumab and Durvalumab were also approved to treat NSCLC, SCLC, Triple-negative breast cancer (TNBC), and transitional cell carcinoma (urothelial cancer). These ICIs were found to improve antitumor T-cell activity and demonstrate activation of global T-cell responses that cause gastrointestinal (GI) immune-related adverse events or irAE. ICI-induced colitis, also termed immune-mediated colitis (IMC), is the most pertinent type of irAEs.9
Risk Factors
There have not been any well-established biomarkers that can predict the commencement of ipilimumab-induced colitis. The increased risk of diarrhea and severe colitis was found to be correlated with increased levels of baseline serum IL-17.10 On the other hand, there were increased risks of GI irAEs found with high peripheral eosinophil values during ipilimumab treatments.10
At the introduction of ipilimumab, detection on patients undergoing colonoscopy 1–2 weeks subsequently demonstrated that first abnormal endoscopic findings could not be predicted for grade 2 or higher colitis. Even elevated focal neutrophilic cryptitis, infiltration of neutrophils, excess plasma in the lamina propria, and cryptitis by the lymphocytes predicted the commencement of symptoms in a span of three weeks for grade 2 or higher diarrhea, they were found to be a not quite dependable biomarker in determining IMC. Lastly, calprotectin on feces can be associated with inflammation of the intestines. However, its baseline levels still cannot predict GI irAEs onset.11 Another risk factor that can be associated as a risk factor for IMCs is nonsteroidal anti-inflammatory drugs. They were also found to induce an increased risk of IMC in patients that have pre-existing autoimmune diseases such as IBD or Inflammatory Bowel Disease, with a 30% prevalence for those treated with ipilimumab. Three of nine patients with ulcerative colitis (UC) incurred IMC or relapsed UC or Crohn's disease (CD). Another study showed that in 5 patients with a past record using the anti-PD-1 inhibitor, treatment for IBD was found pertinent with no recorded flares. They also found that anti-PD-1 therapy had a higher tolerance in patients with IBD than therapy using ipilimumab. In terms of dosage, there were increased rates of cases of IMC for those with increased doses of ipilimumab and its combination with nivolumab.12 The possibility of immune-mediated colitis with PD-1 inhibitors may also come from tumor histology since they may increase melanoma incidence, compared with NSCLC and renal cell carcinoma (RCC).13
Diagnosis of ICI-Induced Colitis
The overall survival rates and duration of treatment of patients for previously almost untreatable malignant diseases have generally increased through the years. Nonetheless, there has been an incidence of “non-classical” oncology adverse events brought about by immunotherapy agents like ICI-induced diarrhea or colitis. Diarrhea with sustained pain with rectal bleeding is termed colitis, which is usually exhibited as an IBD flare and is resistant to supportive treatment.
Immune-Related Side Effects of ICI Therapy
Immune checkpoint proteins, activated by T lymphocytes like PD-1 and CTLA-4, are common immunosuppressive receptors. Their role is to obstruct the endogenous immune system against cancer cells. ICI drugs, ie, ipilimumab (CTLA-4), pembrolizumab and nivolumab (PD-1), and atezolizumab (PD-L1) are drugs that have been already widely prescribed to treat higher forms of aggressive melanoma, lung cancer, and RCC. Under regulatory consideration are some indications such as urothelial cancer, head and neck SCC, stomach cancer, colon cancer, cancer of the ovaries, Merkel cell carcinoma, and Hodgkin’s disease.14
ICI can therefore cause immune-mediated adverse events such as colitis but still cannot be associated with tumor response. There were only reported mild cases of adverse events, but grade 2 or 4 toxicity levels can also be exhibited in up to 10% of patients that have undergone immunotherapy.15
ICI-Induced Diarrhea and Colitis
The occurrence of diarrhea was found to be higher in patients that received treatment with CTLA-4 obstructing antibodies in comparison to those with PD-1 receptor inhibitors. Its level was associated with the amount of dosage for ipilimumab. During the second phase of dose findings, the severity of diarrhea was elevated up to 10mg/kg rate compared to 3mg/kg at 10 to 1%, respectively.14
Physical signs and symptoms of colitis are exhibited by diarrhea with pain in the abdomen, colorectal bleeding, or mucus in the stool. There were 0.3% to 7% of patients that acquired immune-related colitis and then proceeded to further complications such as reflex ileus (abnormal to lack of muscle contractions in the intestine), distension of the colon (colectasia), or perforation on the intestines that may eventually need emergency surgery and worse, can lead to death. Further studies also showed that excess use of ipilimumab in stage 3 melanoma could lead to grade III–IV adverse effects such as GI (16%). Lastly, three patients out of 475 died with colitis upon treatment with ipilimumab.16 It was found that diarrhea and colitis may emerge within six weeks, or later upon introduction to ICI treatment. This suggests that the risk of getting immune-mediated colitis in the first few months of treatment is high.
ICI-mediated colitis has a remarkable similarity with IBD in terms of its physiopathology. UC and CD are very multi-faceted and considered a relapsing-remitting inflammatory disorders. Factors such as genetics largely cause aggression in T cell response to microbiota and dysbiosis. On the other hand, melanoma patients subjected to ipilimumab treatment exhibited a response with unique baseline gut microbiota.16 On the other hand, with the use of endoscopy, the similarity between ICI-induced colitis and inflammatory colitis was also observed with their absence of blood vessel patterns, frank friability, casual bleeding, and ulcerations. They also possess similar histological properties such as cryptitis, lympho-plasmocytic, and polynuclear epithelial infiltration. Granuloma was also found in ICI-induced colitis, akin to Crohn’s disease.17
Assessment of ICI-Induced Colitis
Endoscopy assessment is the best tool to verify and identify the extent of mucosal inflammation. Studies have shown that the formation of ulcers in the colon may indicate steroid-refractory in patients with enterocolitis induced by ipilimumab. Prognosis via endoscopy is possible in identifying future steroid-refractory patients.
A colonoscopy with biopsy is necessary for prevalent NCI Common Terminology Criteria for Adverse events (NCI CTCAE) v4 grade I–II, III–IV diarrhea, or rectal bleeding – including confirmation of colitis prior to infliximab therapy. Primary lesions observed via endoscopy were the absence of vascular patterns, erythema, and ulcerations.17
Another option that can be considered aside from colonoscopy is rectosigmoidoscopy as an exploratory technique. While the former mostly may require effective cleansing of the colon and general anesthesia, the latter proposes a very simple enema preparation, providing faster diagnosis.
Management of ICI-Induced Colitis
For proper diagnosis, recurrence of bowel movement, colorectal bleeding, the intensity of pain, dehydration, and inflammation of the abdomen or peritonitis must be carefully examined. From Lichtiger scores, severe ICI colitis is relative to severe acute colitis brought by IBD. Intense flares can cause distension of the colon and perforation. It is important to assess the extent of the level of adverse effects during the IMC. This can be obtained from general condition evaluation, recurrence of stool, occurrence of stool at night, colorectal bleeding, abdominal pain, and use of therapy for diarrhea. With these, clinical scores can be determined.18 See Table 1 of criteria for evaluation of severe acute colitis that is determined by obtaining a score of greater than or equal to 10.
 |
Table 1 Evaluation of Acute Severe Colitis via Lichtiger Score of Colitis Severity in Inflammatory Bowel Diseases |
Meanwhile, ambulatory treatment is possible if there were less than six bowel movements per day over baseline (grade 1 or 2 diarrhea). For grade 1 diarrhea, a continuation of treatment is possible with close medical supervision. If symptoms persist, ICI treatment shall be halted. Outpatient care management must be done in terms of biological and bacteriological assessments. Supported care therapy can be done by taking racecadotril 100mg thrice a day with oral rehydration and strict monitoring.19 Corticosteroids are taken at an exact dosage of 1 mg/kg per day up to 2mg/kg per day in refractory cases. This can be followed by a progressive corticosteroid decrease after two to five days when symptoms have already been controlled, for a period of 1-to 2 months alongside prophylaxis treatment with trimethoprim and sulphamethoxazole.20 If symptoms persist and there is no progress over a 24-h period, hospitalization may follow, with an intravenous corticosteroid, and rehydration. At this stage, loperamide and opioids must be avoided even with abdominal pain and diarrhea.21 At a Lichtiger score of >10, most cases proceed to the hospitalization in a colitis-specialized unit. ICI must be discontinued. Further abdominal symptoms such as peritonitis, and abdominal computed tomography must be done to identify colonic perforation. This is followed by an endoscopic assessment to evict any other differential diagnosis. Alongside this stage is an infusion of corticosteroid of 1 mg/kg/day dosage for 1–2 months. If the case proceeds to deterioration, infliximab (an anti-TNF-alpha) may be considered at a single dosage (5mg/kg). TNF-alpha is responsible for inflammatory colitis. It is used in corticosteroid-resistant SAC (severe acute colitis) or as a continuance for corticosteroid-reliant or severe IBD. On the other hand, infliximab maintains overall survival.22
No preventive treatment displayed a promising efficacy yet. Moreover, antibiotics positively affect severe colitis in IBD, but no sufficient information regarding immune checkpoint inhibitor-induced colitis is parallel to IBD. There is also no data regarding systemic preventive anti-coagulation, local therapy, or Ciclosporin. Diagnosis, management, and treatment of ICI-induced colitis are still based on its similarity with IBD.
Refractory Immune Checkpoint Inhibitors Colitis and Rule of Biologic Therapy
Only a few studies discussed handling challenging cases such as ICI-induced colitis. Basic guidelines for treatment always start with a high dose of steroids, followed by an increase in drug immune suppression. This process will continue without proven biomarkers that determine the steroid-refractory disease. For patients with severe irARs, adding cytokine-directed mAb at the beginning provides presumptive convenience of preventing immuno-pathophysiological process also avoiding exposure to extended courses of immune suppression. Table 2 shows several new advancements of therapies for the control of irAEs.23
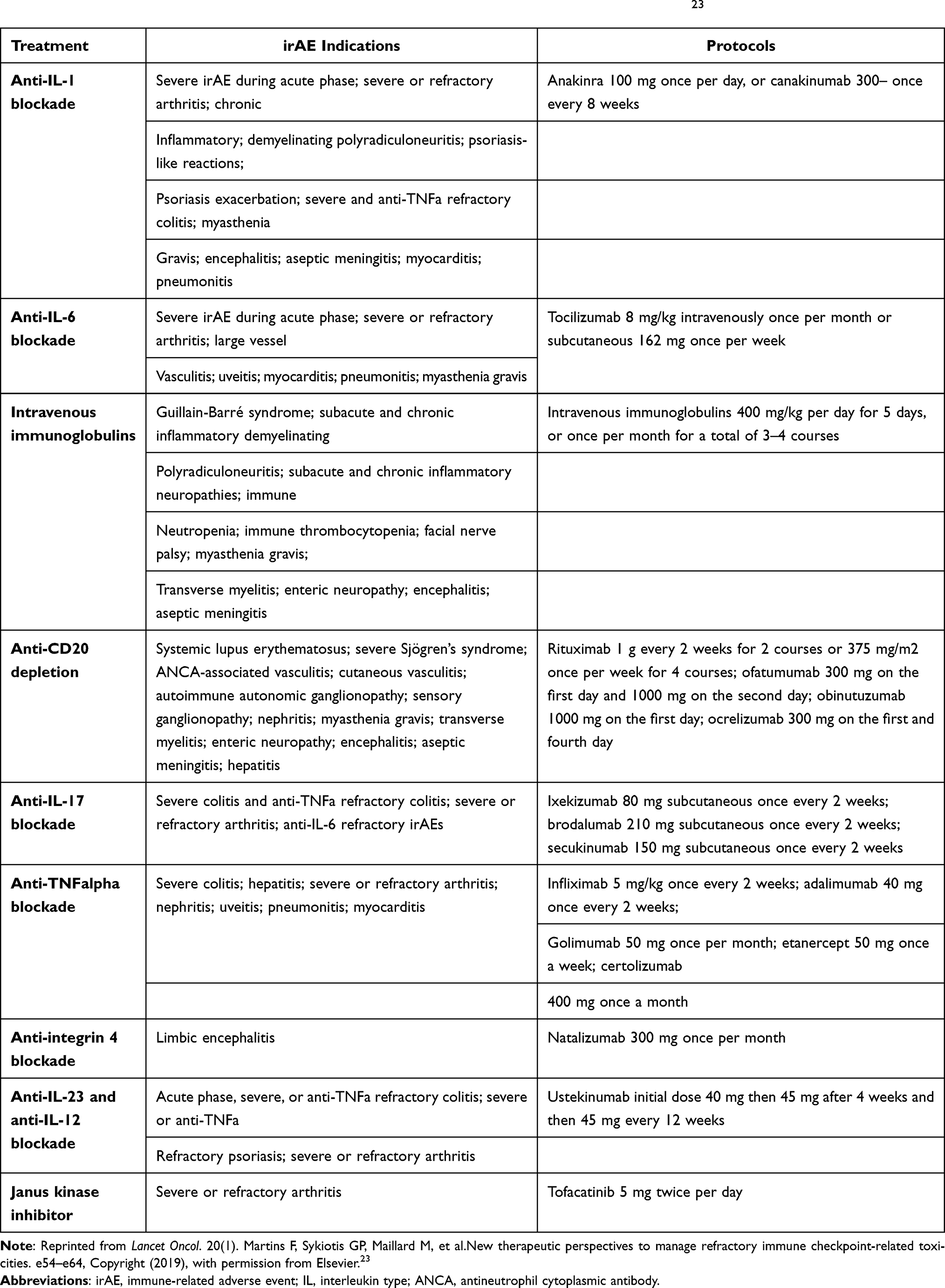 |
Table 2 New Therapeutic Perspectives for the Management of Immune-Related Adverse Events23 |
ICI-related myocarditis is an aggressive drug immune-suppression, reportedly associated with high morbidity and mortality rate with a high risk of adverse effects when subjected to lower doses of steroids compared to higher dose therapy, as affirmed by a meta-analysis in 2018 wherein there was a 0.6% prevalence in patients subjected to ICIs.24 Upon treatment initiation with monotherapy, severe irAEs start to appear, while it arises with ICI combination at median two weeks. Mortality-contributing factors are seen from unusual clinical presentations with diagnosis delay.
Dominant autoimmune diseases related to irAEs also vary with factors such as disease phenotype, treatment response, and pathophysiological activities. Another factor considered is the uniqueness of steroid efficiency in AI diseases in comparison to most ICI-induced diseases. Also, the costings and economical value on healthcare providers affect the use of different therapeutic strategies, which are amortized depending on decreasing patient morbidity. With this, clinical trials of toxicities are also essential due to the growing need for cancer immunotherapy.
Corticosteroids
The usual first line of treatment is corticosteroids due to their fast action and ease of use. Oral prednisone at 1–2 mg/kg or parenteral methylprednisolone at 125–1000mg is the common doses. High-dose corticosteroids may result in other infectious complications and metabolic disturbances. Narrowing duration up to 4–6 weeks is recommended to avoid flares.25
Calcineurin Inhibitors and Anti-TNF Alpha Therapies
Due to their similarities, treatments used in IBD and autoimmune hepatitis are also utilized in ICI-related colitis. Colitis brought about by refractory irAEs respond positively with a one dose of 5 mg per kilogram of infliximab, the same as the treatment for Crohn’s disease.26 Infliximab treatment provided high efficacy for corticosteroid-refractory colitis, with a response as quick as one to three days. Patients with recidivism or non-response may require a second dose after 14 days. Consequently, maintenance must be done for long-term and recurring cases. This treatment has good efficiency towards steroid-refractory pneumonitis. Thus, anti-TNF alpha therapy may also provide a better option compared to other former known immuno-suppressive drugs.
Anti-Interleukin (IL)-1 Blockade
At the acute phase of inflammation, IL-1 is present and preclinical data determined that the IL-1 beta pathway is responsible for tumor progression via tumor-linked macrophages, myeloid suppressive cells, and upregulation of PD-L1 in cancer cells. Anakinra is an anti-IL-1 receptor that treats rheumatoid arthritis and is used for other autoinflammatory disorders. Blocking IL-1 does not affect cancer response.27
Anti-Interleukin (IL)-6 Blockade
Interleukin-6 comes alongside IL-1 with TNF alpha in acute inflammation phase that causes cancer progression and metastasis. An anti- Interleukin-6 treatment can also be efficient for severe IBD when there is no response to standard treatment as it also targets TNF alpha. Consequently, this can be an alternative as anti-TNF alpha or anti-IL-1. Tocilizumab at 8mg/kg per month dosage can be administered via intravenous therapy or 162mg subcutaneously one dosage every seven days. This must be appropriately administered in patients with refractory ICI colitis as it poses higher chances of lower GI tract perforation.28
Anti-Interleukin (IL)-23 and Anti-Interleukin(IL)-12 Therapy
Ustekinumab can be a significant treatment for cutaneous psoriasis and arthritis. A trial was conducted- in which it was administered in an initiation of anti-TNF alpha refractory Crohn’s disease, wherein one-third of the patients had a response at six weeks. However, concerns on opposite functions of IL-23 and IL-12 are raised, but there is no found higher risk of cancer in approved indications. The protocol is 6 mg per kilogram IV treatment followed by 90mg for two to three months.29
Anti-Integrin 4
Typically, natalizumab serves as a treatment for multiple sclerosis. A study showed positive results with combined checkpoint inhibition therapy from a patient with stage 4 lung cancer with a relapse of limbic encephalitis. Vedolizumab is also an anti-integrin with alpha-4-beta-7 antibody with gut-selective anti-inflammatory activity and can be used as a treatment for refractory IBD.30 Two to four administrations of this drug can be used to prevent steroid reduction in their cohort with no other side effects.
Janus Kinase Inhibition
Tofacitinib is a Janus Kinase (JAK)-1 and JAK3 inhibitor that treats refractory rheumatoid arthritis and UC. However, this therapy is correlated with lower GI tract perforation, requiring to follow-up check-ups upon treatment of ICI-induced colitis. The dosage suggested is 5mg or 10 mg 2 times per day.31
Anti-B-Cell
B-cell reduction in patients with melanoma that are unresponsive to therapy was administered with ofatumumab and apparently showed positive results for immunosuppression and a median of 1-year survival for metastatic melanoma upon treatments with rituximab. Two rounds of rituximab may be administered, 1 g per 14 days or 375 mg/m2 per week for one month. Another anti-B-cell therapy used was belimumab, which showed a promising response to severe and refractory auto-mAb irAEs.32
Immune-mediated colitis can be typically recognized as an ordinary kind of bowel disease, but the complexity behind it is underestimated, along with its accelerated growth that can potentially lead to worse adverse effects like bowel perforation and, worse, fatality. The disease’s prevalence may vary from different types of drug regimens and doses. In this study, researchers were able to identify immuno-checkpoint inhibitors in the likes of Ipilimumab, a drug that causes the dose-dependent occurrence of diarrhea and colitis. Risk factors must also be considered as there have not been established biomarkers to detect induced colitis. Diagnosis determines the chance of survival and duration of treatment. In this study, immune-related side effects were also discussed and assessed using endoscopy, recognized as the best tool to verify the extent of the disease. To manage, proper condition evaluation, assessment of recurrence of stool, occurrence of stool at night, colorectal bleeding, and abdominal pain must be monitored. Dominant autoimmune diseases related to irAEs also vary with factors such as disease phenotype, treatment response, and pathophysiological activities. Another factor considered is the uniqueness of steroid efficiency in AI diseases in comparison to most ICI-induced conditions.
Funding
This research did not receive any specific funding from any agencies in the public, commercial, or non-profit sectors.
Disclosure
The authors have no declared conflict of interest for this study.
References
1. Bellaguarda E, Hanauer S. Checkpoint inhibitor-induced colitis. Am J Gastroenterol. 2020;115(2):202–210. doi:10.14309/ajg.0000000000000497
2. Burdine L, Lai K, Laryea JA. Ipilimumab-induced colonic perforation. J Surg Case Rep. 2014;2014(3):rju010–rju010. doi:10.1093/jscr/rju010
3. Dilling P, Walczak J, Pikiel P, Kruszewski WJ. Multiple colon perforation as a fatal complication during treatment of metastatic melanoma with ipilimumab - case report. Pol Przegl Chir. 2014;86(2):94–96. doi:10.2478/pjs-2014-0017
4. Shah R, Witt D, Asif T, Mir FF. Ipilimumab as a cause of severe pan-colitis and colonic perforation. Cureus. 2017;9(4):e1182. doi:10.7759/cureus.1182
5. Larkin J, Chiarion-Sileni V, Gonzalez R, et al. Combined nivolumab and ipilimumab or monotherapy in untreated melanoma. N Engl J Med. 2015;373(1):23–34. doi:10.1056/NEJMoa1504030
6. Myers G. Immune-related adverse events of immune checkpoint inhibitors: a brief review. Curr Oncol. 2018;25(5):342–347. doi:10.3747/co.25.4235
7. Tandon P, Bourassa-Blanchette S, Bishay K, Parlow S, Laurie SA, McCurdy JD. The risk of diarrhea and colitis in patients with advanced melanoma undergoing immune checkpoint inhibitor therapy: a systematic review and meta-analysis. J Immunother. 2018;41(3):101–108. doi:10.1097/CJI.0000000000000213
8. Wang DY, Ye F, Zhao S, Johnson DB. Incidence of immune checkpoint inhibitor-related colitis in solid tumor patients: a systematic review and meta-analysis. Oncoimmunology. 2017;6(10):e1344805. doi:10.1080/2162402X.2017.1344805
9. Postow MA, Callahan MK, Wolchok JD. Immune checkpoint blockade in cancer therapy. J Clin Oncol. 2015;33(17):1974–1982. doi:10.1200/JCO.2014.59.4358
10. Soularue E, Lepage P, Colombel JF, et al. Enterocolitis due to immune checkpoint inhibitors: a systematic review. Gut. 2018;67(11):2056–2067. doi:10.1136/gutjnl-2018-316948
11. Berman D, Parker SM, Siegel J, et al. Blockade of cytotoxic T-lymphocyte antigen-4 by ipilimumab results in dysregulation of gastrointestinal immunity in patients with advanced melanoma. Cancer Immun. 2010;10:11.
12. Menzies AM, Johnson DB, Ramanujam S, et al. Anti-PD-1 therapy in patients with advanced melanoma and preexisting autoimmune disorders or major toxicity with ipilimumab. Ann Oncol. 2017;28(2):368–376. doi:10.1093/annonc/mdw443
13. Khoja L, Day D, Wei-Wu Chen T, Siu LL, Hansen AR. Tumour- and class-specific patterns of immune-related adverse events of immune checkpoint inhibitors: a systematic review. Ann Oncol. 2017;28(10):2377–2385. doi:10.1093/annonc/mdx286
14. Prieux-Klotz C, Dior M, Damotte D, et al. Immune checkpoint inhibitor-induced colitis: diagnosis and management. Target Oncol. 2017;12(3):301–308. doi:10.1007/s11523-017-0495-4
15. Hofmann L, Forschner A, Loquai C, et al. Cutaneous, gastrointestinal, hepatic, endocrine, and renal side-effects of anti-PD-1 therapy. Eur J Cancer. 2016;60:190–209. doi:10.1016/j.ejca.2016.02.025
16. Chaput N, Lepage P, Coutzac C, et al. Baseline gut microbiota predicts clinical response and colitis in metastatic melanoma patients treated with ipilimumab. Ann Oncol. 2017;28(6):1368–1379. doi:10.1093/annonc/mdx108
17. Rastogi P, Sultan M, Charabaty AJ, Atkins MB, Mattar MC. Ipilimumab associated colitis: an IpiColitis case series at MedStar Georgetown University Hospital. World J Gastroenterol. 2015;21(14):4373–4378. doi:10.3748/wjg.v21.i14.4373
18. Dignass A, Eliakim R, Magro F, et al. Second European evidence-based consensus on the diagnosis and management of ulcerative colitis part 1: definitions and diagnosis. J Crohn's Colitis. 2012;6(10):965–990. doi:10.1016/j.crohns.2012.09.003
19. Fischbach W, Andresen V, Eberlin M, Mueck T, Layer P. A comprehensive comparison of the efficacy and tolerability of racecadotril with other treatments of acute diarrhea in adults. Front Med. 2016;3:44. doi:10.3389/fmed.2016.00044
20. Cooley L, Dendle C, Wolf J, et al. Consensus guidelines for diagnosis, prophylaxis and management of Pneumocystis jirovecii pneumonia in patients with haematological and solid malignancies, 2014. Intern Med J. 2014;44(12b):1350–1363. doi:10.1111/imj.12599
21. Tarhini A. Immune-mediated adverse events associated with ipilimumab ctla-4 blockade therapy: the underlying mechanisms and clinical management. Scientifica. 2013;2013:857519. doi:10.1155/2013/857519
22. Arriola E, Wheater M, Karydis I, Thomas G, Ottensmeier C. Infliximab for IPILIMUMAB-related colitis-letter. Clin Cancer Res. 2015;21(24):5642–5643. doi:10.1158/1078-0432.CCR-15-2471
23. Martins F, Sykiotis GP, Maillard M, et al. New therapeutic perspectives to manage refractory immune checkpoint-related toxicities. Lancet Oncol. 2019;20(1):e54–e64. doi:10.1016/S1470-2045(18)30828-3
24. Wang DY, Salem JE, Cohen JV, et al. Fatal toxic effects associated with immune checkpoint inhibitors: a systematic review and meta-analysis. JAMA Oncol. 2018;4(12):1721–1728. doi:10.1001/jamaoncol.2018.3923
25. Thompson JA, Schneider BJ, Brahmer J, et al. Management of immunotherapy-related toxicities, version 1.2019. J Natl Compr Canc Netw. 2019;17(3):255–289. doi:10.6004/jnccn.2019.0013
26. Cheng R, Cooper A, Kench J, et al. Ipilimumab-induced toxicities and the gastroenterologist. J Gastroenterol Hepatol. 2015;30(4):657–666. doi:10.1111/jgh.12888
27. Harrison SR, McGonagle D, Nizam S, et al. Anakinra as a diagnostic challenge and treatment option for systemic autoinflammatory disorders of undefined etiology. JCI Insight. 2016;1(6):e86336. doi:10.1172/jci.insight.86336
28. Strangfeld A, Richter A, Siegmund B, et al. Risk for lower intestinal perforations in patients with rheumatoid arthritis treated with tocilizumab in comparison to treatment with other biologic or conventional synthetic DMARDs. Ann Rheum Dis. 2017;76(3):504–510. doi:10.1136/annrheumdis-2016-209773
29. Teng MW, Vesely MD, Duret H, et al. Opposing roles for IL-23 and IL-12 in maintaining occult cancer in an equilibrium state. Cancer Res. 2012;72(16):3987–3996. doi:10.1158/0008-5472.CAN-12-1337
30. Singh H, Grewal N, Arora E, Kumar H, Kakkar AK. Vedolizumab: a novel anti-integrin drug for treatment of inflammatory bowel disease. J Nat Sci Biol Med. 2016;7(1):4–9. doi:10.4103/0976-9668.175016
31. Sandborn WJ, Su C, Panes J. Tofacitinib as induction and maintenance therapy for ulcerative colitis. N Engl J Med. 2017;377(5):496–497.
32. Tai YT, Mayes PA, Acharya C, et al. Novel anti-B-cell maturation antigen antibody-drug conjugate (GSK2857916) selectively induces killing of multiple myeloma. Blood. 2014;123(20):3128–3138. doi:10.1182/blood-2013-10-535088
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Fidaxomicin Use in the Pediatric Population with Clostridioides difficile
Oliver MB, Vaughn BP
Clinical Pharmacology: Advances and Applications 2022, 14:91-98
Published Date: 23 September 2022
Risk Factors and Prognostic Analysis of Immune Checkpoint Inhibitor-Related Colitis in Lung Cancer
Wang S, Tian B, Wang H
Journal of Inflammation Research 2024, 17:7535-7542
Published Date: 21 October 2024
C-Reactive Protein in Immune Checkpoint Inhibitor-Associated Colitis: A Scoping Review of Evidence and Knowledge Gaps
Ohta R, Ryu Y, Tanaka K, Sano C, Hayashi H
Cancer Management and Research 2025, 17:2631-2641
Published Date: 7 November 2025
Intestinal Stenosis Related to Immune Checkpoint Inhibitors Caused by Sintilimab: A Case Report
Li HY, Liu Y, Hu SL, Li YQ, Tang TY
Journal of Inflammation Research 2026, 19:556800
Published Date: 10 January 2026