Back to Journals » OncoTargets and Therapy » Volume 15
A Case of Hepatocellular Carcinoma Successfully Resumed Atezolizumab and Bevacizumab After Associated Grade 3 Diarrhea and Grade 2 Colitis: Case Report and Literature Review
Authors Fuji T, Arai J ![]() , Otoyama Y, Nio Y, Sugiura I, Nakajima Y, Kajiwara A, Ichikawa Y, Uozumi S, Shimozuma Y
, Otoyama Y, Nio Y, Sugiura I, Nakajima Y, Kajiwara A, Ichikawa Y, Uozumi S, Shimozuma Y ![]() , Uchikoshi M, Sakaki M, Nozawa H, Momo K
, Uchikoshi M, Sakaki M, Nozawa H, Momo K ![]() , Sasaki T, Yoshida H
, Sasaki T, Yoshida H
Received 26 July 2022
Accepted for publication 10 September 2022
Published 25 October 2022 Volume 2022:15 Pages 1281—1288
DOI https://doi.org/10.2147/OTT.S383769
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Arseniy Yuzhalin
Takahiro Fuji,1 Jun Arai,1 Yumi Otoyama,1 Yuta Nio,2,3 Ikuya Sugiura,1 Yoko Nakajima,1 Atsushi Kajiwara,1 Yuki Ichikawa,1 Shojiro Uozumi,1 Yuu Shimozuma,1 Manabu Uchikoshi,1 Masashi Sakaki,1 Hisako Nozawa,1 Kenji Momo,2 Tadanori Sasaki,3 Hitoshi Yoshida1
1Department of Medicine, Division of Gastroenterology, Showa University School of Medicine, Tokyo, Japan; 2Department of Hospital Pharmaceutics, School of Pharmacy, Showa University Hospital, Tokyo, Japan; 3Department of Pharmacy, Showa University Hospital, Tokyo, Japan
Correspondence: Jun Arai, Department of Medicine, Division of Gastroenterology, Showa University School of Medicine, 1-5-8 Hatanodai, Shinagawa-ku, Tokyo, 142-8666, Japan, Tel +81-3-3784-8535, Fax +81-3-3784-7553, Email [email protected]
Abstract: Systemic chemotherapy has shown a significant survival benefit in patients with hepatocellular carcinoma (HCC). However, it is associated with various immune-related adverse events (irAEs). We report a case with grade 3 diarrhea and grade 2 colitis following systemic chemotherapy, successfully treated with prednisolone. An 89-year-old man was incidentally detected with a 140-mm hypervascular intrahepatic nodule on contrast-enhanced computed tomography (CECT). Washout of the contrast medium was also detected, and protein induced by vitamin K deficiency or antagonists-II (PIVKA-II) was elevated. Since the Albumin–Bilirubin (ALBI) grade was 2a without any distant metastasis, transarterial chemoembolization (TACE) was performed to treat the HCC, but several intrahepatic nodules were seen in both lobes. Therefore, the patient was treated with lenvatinib for 1 year and 4 months. A complete response according to modified Response Evaluation Criteria in Solid Tumors (mRECIST) criteria was achieved in 2 months; however, multiple hypervascular nodules were detected again. Since the ALBI grade was 1, a second round of chemotherapy with atezolizumab and bevacizumab was initiated. Although a complete response was achieved, the therapy was discontinued due to grade 3 diarrhea and grade 2 colitis after the sixth course. Based on the stool analysis and culture, CECT, and colonoscopy, the diagnosis was atezolizumab-associated colitis. Diarrhea was controlled following the oral administration of 0.5 mg/kg/day of prednisolone, and atezolizumab-bevacizumab therapy was successfully reinitiated without recurrence of colitis. The management of irAEs is important for a significant survival benefit. Systemic chemotherapy with atezolizumab and bevacizumab can be resumed despite a grade 3 irAE due to atezolizumab.
Keywords: hepatocellular carcinoma, immune checkpoint inhibitors, immune-related adverse events, ICI-mediated colitis, IL-17, PIVKA-II
Introduction
Hepatocellular carcinoma (HCC) is the most common primary liver cancer; it is the fifth most common cancer in men and the seventh most common in women worldwide.1 HCC usually occurs in patients with chronic hepatitis or liver cirrhosis due to infection with hepatitis B virus or hepatitis C virus, non-alcoholic fatty liver disease (NAFLD), nonalcoholic steatohepatitis (NASH), alcoholic liver disease, autoimmune liver disease, congestive liver disease, and liver disease of unknown etiology.2,3 The incidence rates of HCC and its recurrence are significantly higher in patients with Child–Pugh (CP)-C than in those with CP-A or CP-B despite the administration of direct-acting antivirals.4 As of July 2022, there are five molecular targeted agents and one combination immunotherapy approved in Japan for HCC: atezolizumab plus bevacizumab as first-line treatment.5,6 There are also possible sequential systemic therapies as second-line and later-line therapy, which target a variety of kinases implicated in angiogenic and tumor.5,7 Recent evidence has shown that its antitumor efficacy is due to a comprehensive spectrum of tumor neo-angiogenesis, enhancement of immunosurveillance by natural killer cells, and immunomodulatory effects on the tumor microenvironment, which plays a crucial role in tumor development and growth-promoting pathways.7,8
However, immune checkpoint inhibitors (ICIs) potentially cause an imbalance in the immune system, leading to immune-related adverse events (irAEs). In particular, ICI-mediated colitis (IMC) is the most frequent cause of discontinuation of ICI therapy.9,10 In a meta-analysis of 34 studies including 8863 patients, the overall incidence of colitis grade 3 or higher during ipilimumab monotherapy was 6.8%, and that of diarrhea grade 3 or higher was 7.9%. The incidence was lowest with programmed cell death protein 1 (PD-1)/programmed death-ligand 1 (PD-L1) inhibitor monotherapy, being 0.9% for colitis grade 3 or higher and 1.2% for diarrhea grade 3 or higher, while the combination therapy of ipilimumab and nivolumab resulted in the highest incidences of 9.4% and 9.2% for colitis and diarrhea, respectively, among ICIs.11 While the antitumor mechanisms of ICIs have been widely studied, large studies to determine the mechanisms involved in irAEs are still lacking. There are several guidelines about the ideal treatment of IMC; however, there is no consensus regarding the resumption of treatment with ICI after IMC.12–14
We report a rare case of a patient with HCC who developed atezolizumab-associated grade 3 diarrhea and grade 2 colitis. These adverse events were successfully treated with prednisolone, and atezolizumab plus bevacizumab therapy was re-initiated with no recurrent IMC.
Case Presentation
An 89-year-old Japanese man with no relevant past medical history was referred to our hospital from a community hospital in 2018 for the investigation of an accidentally detected intrahepatic nodule on plain computed tomography (CT); which was not suggestive of liver cirrhosis or fatty liver disease (Figure 1A). Contrast-enhanced CT (CECT) showed a hypervascular intrahepatic nodule 140 mm in diameter in the arterial phase (Figure 1B). Later, washout of the contrast medium was also detected in the portal phase (Figure 1C). Based on the vascular pattern seen on the CT imaging, the intrahepatic nodule was diagnosed as HCC with no distant metastasis. Blood examination revealed a low platelet count (11.8×104 /μL), slightly elevated AST level (54 IU/L), elevated protein induced by vitamin K deficiency or antagonists-II (PIVKA-II) (1057.2 mAU/mL), and normal α-fetoprotein (Supplemental Table 1). His HbA1c level was 5.7%, and HBV surface antigen and anti-HCV antibody were negative. Since the Albumin–Bilirubin (ALBI) grade was 2a without any distant metastasis, it was classified as early stage (A) HCC according to the American Association for the Study of Liver Diseases (AASLD) guidelines.15 Four cycles of transarterial chemoembolization (TACE) were effectively performed to HCC without significant adverse events, and the patient achieved complete response according to modified Response Evaluation Criteria in Solid Tumors (mRECIST) criteria (Figure 1D and E). The PIVKA-II level decreased to less than the upper limit of normal as shown in Figure 2. During the follow-up after the fourth-TACE, several intrahepatic hypervascular nodules were seen in both lobes on CECT (Figure 1F). At that time, atezolizumab and bevacizumab therapy had not been approved, and the HCC was classified as intermediate stage (B) without worsening ALBI grade. Therefore, considering his age, the patient was treated with lenvatinib 4 mg daily. No significant adverse events occurred, and the complete response evaluated according to the mRECIST criteria was achieved in 2 months, as seen on CECT (Figure 3A). However, a year and 4 months after initiating lenvatinib, multiple hypervascular nodules were detected (Figure 3B). Within the up-to-seven criteria, TACE was performed twice. However, it did not stop the progression of HCC (Figure 3C). Since the ALBI grade was 1, a second cycle of chemotherapy with atezolizumab 1200 mg and bevacizumab 15 mg/kg body weight was initiated every 3 weeks. Although a complete response was achieved (Figure 3D), after the sixth cycle, he complained of increased frequency of stool to more than ten times daily. There was mucus in the stool but no blood or abdominal pain. The therapy was discontinued due to grade 3 diarrhea and grade 2 colitis. Based on the results of the stool culture, CECT, and colonoscopy, it was diagnosed as atezolizumab and bevacizumab-associated colitis. No pathogenic bacteria were found in the stool culture, and Clostridium difficile toxin was negative. There were no findings indicative of peritonitis, such as ascites, swelling of the colonic wall, or dirty fat sign surrounding the colon (Supplementary Figure 1A–C). Furthermore, the serum anti-cytomegalovirus IgM antibody was negative, and cytomegalovirus antigen was not detected. Colonoscopy revealed friability and loss of vascular pattern from the rectum to the cecum (Figure 3E). Furthermore, the pathological result of the colonic specimen revealed mild cryptitis, but there was no diffuse mononuclear cell infiltration or basal plasmacytosis (Figure 3F). The diarrhea was promptly controlled after the oral administration of prednisolone at a dose of 20 mg/day (0.5 mg/kg/day). One week later, it was reduced to 10 mg/day, and after 2 more weeks, it was changed to 5 mg/day, after which atezolizumab and bevacizumab were reinitiated carefully after taking informed consent from the patient. He was treated with 5 mg/day of prednisolone for 6 weeks, and the dose of prednisolone was gradually reduced by 1 mg every 3 weeks to 1 mg/day. Fortunately, atezolizumab at 1200 mg and bevacizumab at 15 mg/kg body weight were continued until 14 courses while continuing 1 mg of oral prednisolone daily without recurrence of diarrhea or colitis. During the treatment, the patient’s IL-17 level was measured multiple times using the IL-17 ELISA Kit (R&D Systems, Minneapolis, MN). As shown in (Figure 2), the baseline serum IL-17 level was very low and did not increase during the systemic treatment. This case report was approved by a suitably constituted Ethics Committee of our institution, and it complied with the provisions of the Declaration of Helsinki. Written informed consent was obtained from the patient for publication of this case report and any accompanying images.
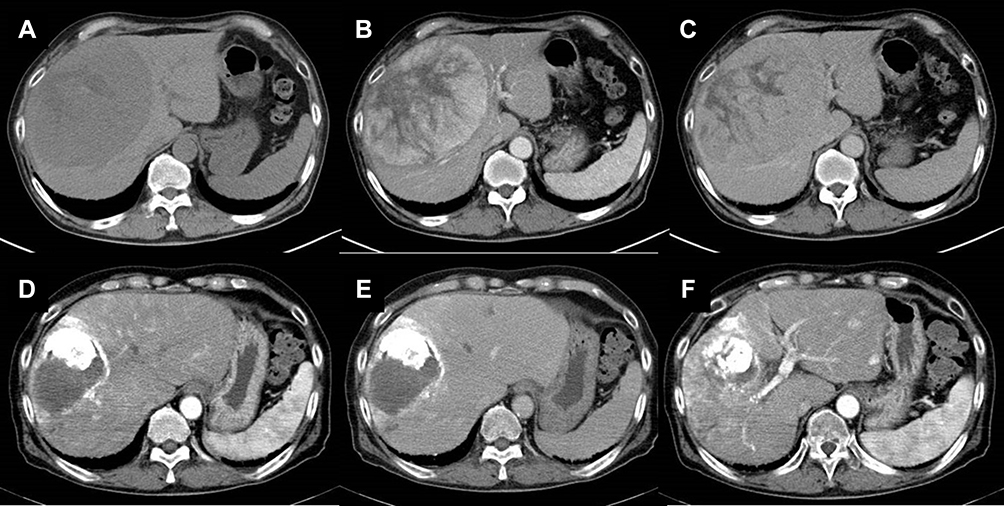 |
Figure 1 Clinical images of hepatocellular carcinoma in an 89-year-old man. (A) The intrahepatic lesion shown in the plain CT. The contrast-enhanced CT showing the intrahepatic nodule (B) in the arterial phase and (C) in the portal phase at the initial diagnosis. (D and E) CT findings after TACE showing the complete response according to mRECIST criteria, and (F) later, several intrahepatic nodules were seen in both lobes. |
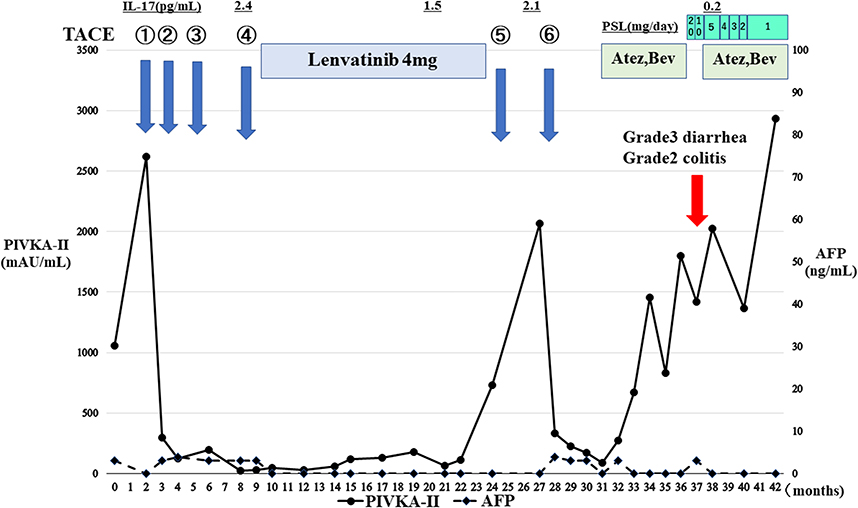 |
Figure 2 Changes in tumor markers and IL-17 level in this case are shown. |
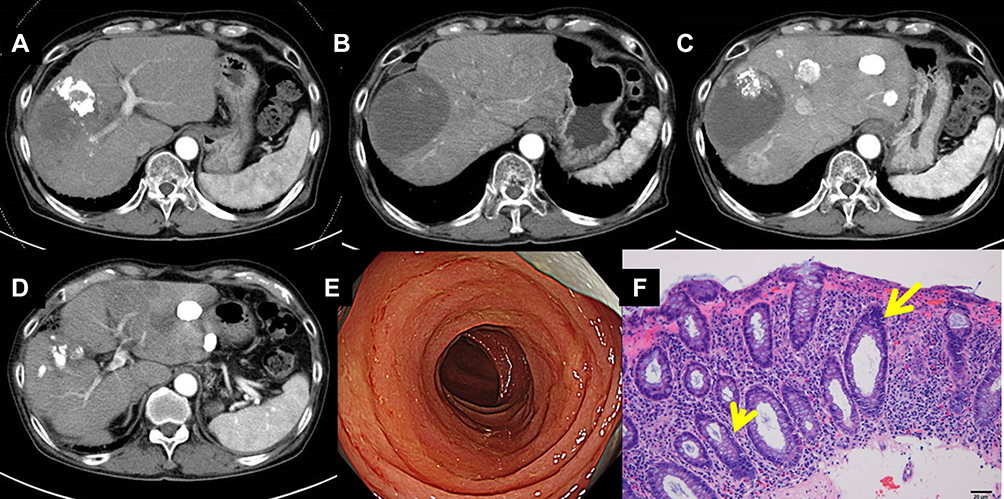 |
Figure 3 Clinical images of hepatocellular carcinoma during the treatment. (A) The contrast-enhanced CT after lenvatinib therapy showing the complete response according to mRECIST criteria, and (B) later, multiple intrahepatic nodules were seen in both lobes. (C) After TACE was performed, intrahepatic nodules were exacerbated in both lobes in the contrast-enhanced CT. (D) CT findings after chemotherapy with atezolizumab and bevacizumab showing the complete response according to mRECIST criteria. (E) Colonoscopy showing friability and loss of vascular pattern from the rectum to the cecum. (F) Microscopic findings of the colonic specimen showing mild cryptitis described with arrows, but there was no diffuse mononuclear cell infiltration or basal plasmacytosis. |
Discussion
ICI therapy as first-line treatment has significantly changed the prognosis of HCC; however, the occurrence of adverse events, including frequent IMC often leads to discontinuation of ICI therapy.9,10 Interestingly, the development of irAEs was associated with better clinical outcome for HCC patients who were treated with ICIs, although the sample size was small.16 Corticosteroid therapy is often indicated in the management of cancer-related symptoms such as cachexia, anorexia, edema in the central nervous system, or pain and is recommended by guidelines as first-line therapy for most irAEs.17,18 Recently, Pinato et al reported that there is inadequate evidence about corticosteroid therapy before or during ICI therapy being associated with overall survival and progression-free survival in patients with HCC even at a dose of more than 10 mg/day.18 We experienced a case of atezolizumab and bevacizumab-associated grade 3 diarrhea and grade 2 colitis in which the adverse events were controlled with corticosteroids, and ICI could be resumed. Patients who experience persistent diarrhea of grade 2 or higher or abdominal pain should undergo investigations to rule out infections and colonoscopy with biopsies.19 In our case, the diagnosis could be established as IMC based on stool culture, CECT, and colonoscopy. Endoscopic features of IMC range from normal appearing mucosa to erosions, erythema, and loss of vascular pattern, to ulcerations.19,20 Biopsies typically show features of acute colitis, such as increased cellularity of the lamina propria, intraepithelial neutrophilic infiltrates, and crypt abscesses, rather than characteristics of chronic colitis such as intraepithelial or basal lymphocytes and crypt architecture distortion.21 Since the findings on colonoscopy showed friability, loss of vascular pattern from the rectum to the cecum, without ulcerations (Figure 3E), and pathological analysis showed inflammation with mild cryptitis (Figure 3F), the patient was treated with oral prednisolone 0.5 mg/kg/day at the outpatient clinic. The diarrhea stopped on the day after initiating prednisolone. Hayashi et al reported eight cases of ICI-induced grade 2/3 gastroenterocolitis treated with prednisolone.22 Among them, only one patient with melanoma, who suffered from ipilimumab-associated grade 3 diarrhea, was reinitiated with nivolumab. Usually, continuing the same ICI is suggested for patients who develop a less severe grade 1 colitis.23 The risk of recurrent IMC was found to be almost 30% with most regimens, but this risk was higher in patients who were switched from PD-1/PD-L1 inhibitors to cytotoxic T lymphocyte-associated antigen (CTLA-4) inhibitors.23,24 In cases of anti-CTLA-4- related grade 3 toxicity, it is recommended to immediately and permanently discontinue the medication. These patients can be considered for anti-PD-1/PD-L1 agents once the irAE has resolved.21 In a survey of 93 patients who resumed the ICI treatment, among five patients experienced IMC after anti-PD-1 or anti-PD-L1, three patients experienced the recurrence of IMC after anti-PD-1 or anti-PD-L1 resumption. However, there was no information about the grade of colitis during the first irAEs, and patients treated for HCC were not included.25 Nine cases of IMC who reinitiated ICI have been reported in the English literature (Table 1). Badran et al also reported five cases with Grade 1 and 2 IMC, all of which were initially treated with corticosteroid therapy and infliximab (IFX).26 In four cases, IFX was continuously administered even after the resumption of ICIs, which were the same as the initial regimen.26 Two case reports with melanoma discussed the discontinuation of ICI due to IMC followed by and re-initiation of ICI after the resolution of IMC.27,28 Six cases, including our own, provided IFX or corticosteroid administration when reinitiating ICI. Among the total nine cases, one patient experienced the recurrence of IMC after resuming ICI despite corticosteroid administration.28
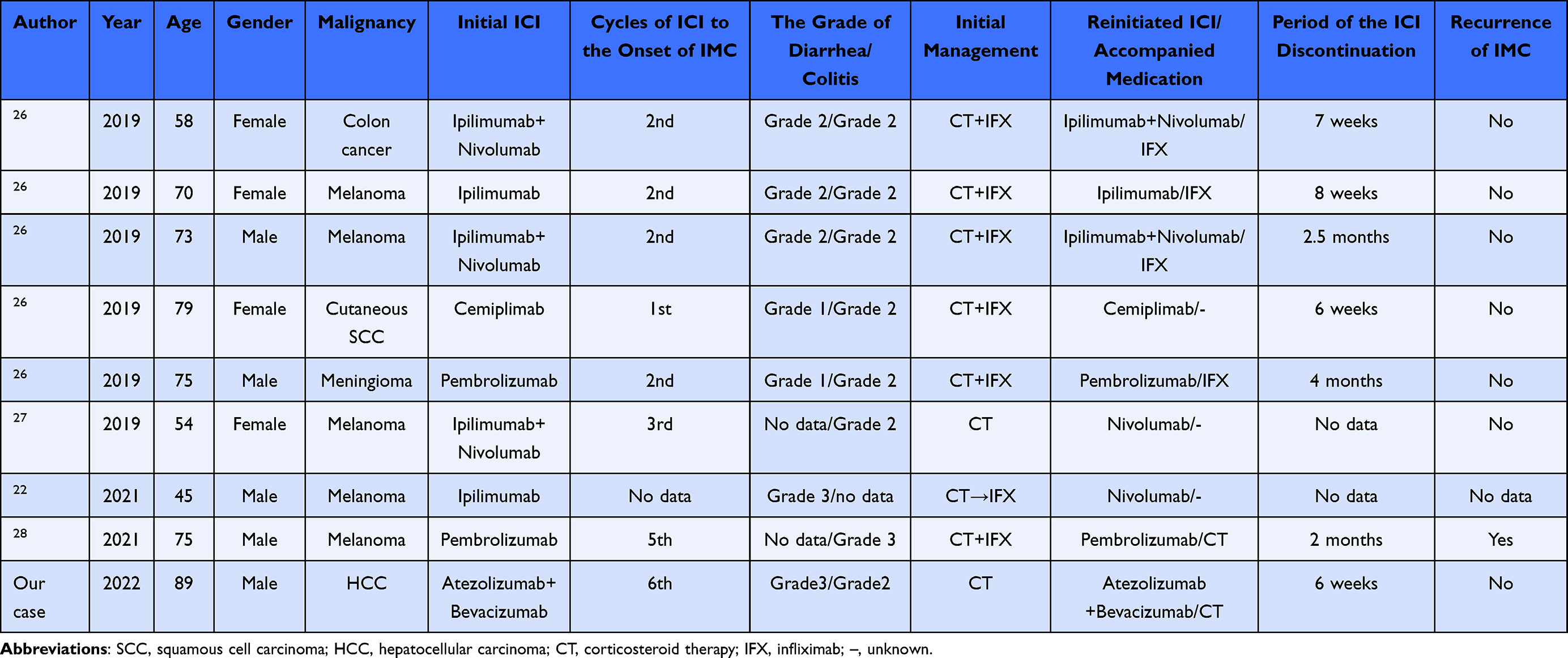 |
Table 1 The Clinical Characteristics of Nine HCC Cases with IMC Re-Initiated with ICI are Shown |
In unresectable HCC, ICI combination therapy with tremelimumab plus durvalumab is likely to be approved soon, in which more careful monitoring of IMC would be necessary for patients with HCC.29 Recently, it was reported that Th17/IL-17 axis is responsible for the production of chemokines CXCL8 and GM-CSF by the intestinal epithelial cells, which attract neutrophils leading to IMC.10 Importantly, blood IL-17 levels at baseline were found to correlate significantly with the incidence of grade 3 diarrhea/colitis among patients with melanoma treated with ipilimumab.30 The average baseline IL-17 level in patients with grade 3 diarrhea/colitis was more than 50 (pg/mL), while among patients with grade 0–2 diarrhea/colitis, the average level was approximately 10 (pg/mL).30 IL-17 is one of the principal inflammatory cytokines and is known to be upregulated in patients with inflammatory bowel disease.30 Therefore, the evaluation of IL-17 in patients with IMC is rational. A previous study demonstrated that Th17/IL-17 might be associated with toxicities after administration of anti-CTLA-4 antibodies because the cells producing IL-17 on non-specific ex vivo stimulation were found to be increased in post-dosing blood samples from patients.31 To the best of our knowledge, there are no previous reports about IL-17 levels in patients with IMC treated with PD-1/PD-L1 inhibitors. In our case, the baseline serum IL-17 level was very low as shown in Figure 2, and did not increase during the follow-up. Since this is a single-case report and the patient did not receive anti-CTLA-4 antibodies, further investigation into the correlation between the serum IL-17 level and IMC is necessary, including in the upcoming combination therapy for HCC.
Since the colonoscopy findings indicated mild colitis, and the therapeutic response was complete response, atezolizumab and bevacizumab were resumed carefully. Despite gradually decreasing the dose of prednisolone to 1 mg/day, the systemic chemotherapy with atezolizumab and bevacizumab was safely continued without recurrence of gastrointestinal symptoms. The National Comprehensive Cancer Network (NCCN) Guidelines 2020 suggest that in patients with grade 3 diarrhea or colitis associated with PD-1/PD-L1 inhibitors, therapy should be withheld and resumed after improvement of symptoms to below grade 1.13
Finally, the HCC got worse, and the patient did not hope to take further systemic chemotherapy. He was introduced to his general practitioner for taking care according to his proposal. The patient has been alive for approximately 4 years with systemic chemotherapy and TACE, although he was incidentally detected with HCC at an advanced age. The reasons for the good prognosis include non-worsening of the liver function during treatment and no metastases to lymph nodes or other organs. To the best of our knowledge, this is the first case in which ICI therapy was successfully resumed after atezolizumab and bevacizumab-associated grade 3 diarrhea and grade 2 colitis. With the increase in clinical experience of ICI as the first-line treatment of HCC, more evidence for safely reinitiating ICI after irAEs is necessary.
Abbreviations
HCC, hepatocellular carcinoma; NAFLD, non-alcoholic fatty liver disease; NASH, nonalcoholic steatohepatitis; CP, Child–Pugh; ICIs, immune checkpoint inhibitors; irAEs, immune-related adverse events; IMC, ICI-mediated colitis; PD-1, programmed cell death protein 1; PD-L1, programmed death-ligand 1; CT, computed tomography; CECT, contrast-enhanced CT; PIVKA-II, protein induced by vitamin K deficiency or antagonists-II; ALBI, Albumin–Bilirubin; AASLD, American Association for the Study of Liver Diseases; TACE, transarterial chemoembolization; mRECIST, modified Response Evaluation Criteria in Solid Tumors; CTLA-4, cytotoxic T lymphocyte-associated antigen; IFX, infliximab; NCCN, National Comprehensive Cancer Network.
Ethics Approval and Consent to Participate
The research has been performed in accordance with the Declaration of Helsinki.
Not applicable for consent to participate. Publication of this case report was approved by a suitably constituted Ethics Committee of our institution.
Consent for Publication
Written informed consent was obtained from the patient for publication of this case report and any accompanying images. A copy of the written consent is available for review by the Editor of this journal.
Acknowledgments
J.A. was supported by Grants-in-Aid for Scientific Research from the Ministry of Education, Culture, Sports, Science, and Technology (19K08412). We thank Editage for English language editing.
Disclosure
TS received an honorarium for presentation at AstraZeneca, and Daiichi-Sankyo. KM reports personal fees from AbbVie and Nippon Kayaku; grants from Taiho, Nippon Kayaku, Daiichi Sankyo, and Shionogi, outside the submitted work. The other authors have disclosed that they have no significant relationships with, or financial interest in any commercial companies in this work.
References
1. El-Serag HB. Epidemiology of viral hepatitis and hepatocellular carcinoma. Gastroenterology. 2012;142:1264–1273.e1. doi:10.1053/j.gastro.2011.12.061
2. Nagaoki Y, Hyogo H, Aikata H, et al. Recent trend of clinical features in patients with hepatocellular carcinoma. Hepatol Res. 2012;42:368–375. doi:10.1111/j.1872-034X.2011.00929.x
3. Nishikawa H, Osaki Y. Non-B, non-C hepatocellular carcinoma (Review). Int J Oncol. 2013;43:1333–1342. doi:10.3892/ijo.2013.2061
4. Tahata Y, Hikita H, Mochida S, et al. Liver-related events after direct-acting antiviral therapy in patients with hepatitis C virus-associated cirrhosis. J Gastroenterol. 2022;57:120–132. doi:10.1007/s00535-021-01845-5
5. Kudo M, Kawamura Y, Hasegawa K, et al. Management of hepatocellular carcinoma in Japan: JSH consensus statements and recommendations 2021 update. Liver Cancer. 2021;10:181–223. doi:10.1159/000514174
6. Tsuchiya K, Kurosaki M, Sakamoto A, et al. The real-world data in Japanese patients with unresectable hepatocellular carcinoma treated with lenvatinib from a nationwide Multicenter Study. Cancers. 2021;13:2608. doi:10.3390/cancers13112608
7. Granito A, Forgione A, Marinelli S, et al. Experience with regorafenib in the treatment of hepatocellular carcinoma. Therap Adv Gastroenterol. 2021;14:17562848211016959. doi:10.1177/17562848211016959
8. Arai J, Goto K, Stephanou A, et al. Predominance of regorafenib over sorafenib: restoration of membrane-bound MICA in hepatocellular carcinoma cells. J Gastroenterol Hepatol. 2018;33:1075–1081. doi:10.1111/jgh.14029
9. Dolladille C, Ederhy S, Sassier M, et al. Immune checkpoint inhibitor rechallenge after immune-related adverse events in patients with cancer. JAMA Oncol. 2020;6:865–871. doi:10.1001/jamaoncol.2020.0726
10. Westdorp H, Sweep MWD, Gorris MAJ, et al. Mechanisms of immune checkpoint inhibitor-mediated colitis. Front Immunol. 2021;12:768957. doi:10.3389/fimmu.2021.768957
11. Wang DY, Ye F, Zhao S, Johnson DB. Incidence of immune checkpoint inhibitor-related colitis in solid tumor patients: a systematic review and meta-analysis. Oncoimmunology. 2017;6:e1344805. doi:10.1080/2162402X.2017.1344805
12. Haanen JBAG, Carbonnel F, Robert C, et al. Management of toxicities from immunotherapy: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2017;28(suppl_4):iv119–iv142. doi:10.1093/annonc/mdx225
13. Thompson JA, Schneider BJ, Brahmer J, et al. NCCN guidelines insights: management of immunotherapy-related toxicities, version 1.2020. J Natl Compr Canc Netw. 2020;18:230–241. doi:10.6004/jnccn.2020.0012
14. CTCAE ver5.0 National Cancer Institute, Division of Cancer Treatment & Diagnosis. Common terminology criteria for adverse events (CTCAE), version 5.0. Bethesda, MD: US Department of Health and Human Services; 2017. Available from: https://ctep.cancer.gov/protocolDevelopment/.
15. Llovet JM, Villanueva A, Marrero JA, et al. Trial Design and endpoints in hepatocellular carcinoma: AASLD consensus conference. Hepatology. 2021;73(Suppl 1):158–191. doi:10.1002/hep.31327
16. Xu S, Lai R, Zhao Q, Zhao P, Zhao R, Guo Z. Correlation between immune-related adverse events and prognosis in hepatocellular carcinoma patients treated with immune checkpoint inhibitors. Front Immunol. 2021;12:794099. doi:10.3389/fimmu.2021.794099
17. Michot JM, Bigenwald C, Champiat S, et al. Immune-related adverse events with immune checkpoint blockade: a comprehensive review. Eur J Cancer. 2016;54:139–148. doi:10.1016/j.ejca.2015.11.016
18. Pinato DJ, Kaseb A, Wang Y, et al. Impact of corticosteroid therapy on the outcomes of hepatocellular carcinoma treated with immune checkpoint inhibitor therapy. J Immunother Cancer. 2020;8:e000726. doi:10.1136/jitc-2020-000726
19. Som A, Mandaliya R, Alsaadi D, et al. Immune checkpoint inhibitor-induced colitis: a comprehensive review. World J Clin Cases. 2019;7:405–418. doi:10.12998/wjcc.v7.i4.405
20. Nishida T, Iijima H, Adachi S. Immune checkpoint inhibitor-induced diarrhea/colitis: endoscopic and pathologic findings. World J Gastrointest Pathophysiol. 2019;10:17–28. doi:10.4291/wjgp.v10.i2.17
21. Kröner PT, Mody K, Farraye FA. Immune checkpoint inhibitor-related luminal GI adverse events. Gastrointest Endosc. 2019;90:881–892. doi:10.1016/j.gie.2019.09.009
22. Hayashi Y, Hosoe N, Takabayashi K, et al. Clinical, endoscopic, and pathological characteristics of immune checkpoint inhibitor-induced gastroenterocolitis. Dig Dis Sci. 2021;66:2129–2134. doi:10.1007/s10620-020-06441-w
23. Hashash JG, Francis FF, Farraye FA. Diagnosis and management of immune checkpoint inhibitor colitis. Gastroenterol Hepatol. 2021;17:358–366.
24. Abu-Sbeih H, Ali FS, Naqash AR, et al. Resumption of immune checkpoint inhibitor therapy after immune-mediated colitis. J Clin Oncol. 2019;37:2738–2745. doi:10.1200/JCO.19.00320
25. Simonaggio A, Michot JM, Voisin AL, et al. Evaluation of readministration of immune checkpoint inhibitors after immune-related adverse events in patients with cancer. JAMA Oncol. 2019;5:1310–1317. doi:10.1001/jamaoncol.2019.1022
26. Badran YR, Cohen JV, Brastianos PK, Parikh AR, Hong TS, Dougan M. Concurrent therapy with immune checkpoint inhibitors and TNFα blockade in patients with gastrointestinal immune-related adverse events. J Immunother Cancer. 2019;7:226. doi:10.1186/s40425-019-0711-0
27. Norwood TG, Wang MJ, Huh WK. Combination checkpoint inhibitor therapy induces multiple immune major related adverse events in the treatment of vaginal melanoma: a cautionary case report. Gynecol Oncol Rep. 2019;30:100508. doi:10.1016/j.gore.2019.100508
28. Moradi LA, Clark CA, Schneider CS, Deshane AS, Dobelbower MC. Durable metastatic melanoma remission following pembrolizumab and radiotherapy: a case report of prophylactic immunosuppression in a patient with myasthenia gravis and immune-mediated colitis. Front Immunol. 2021;12:788499. doi:10.3389/fimmu.2021.788499
29. Kelley RK, Sangro B, Harris W, et al. Safety, efficacy, and pharmacodynamics of tremelimumab plus durvalumab for patients with unresectable hepatocellular carcinoma: randomized expansion of a phase I/II study. J Clin Oncol. 2021;39:2991–3001. doi:10.1200/JCO.20.03555
30. Tarhini AA, Zahoor H, Lin Y, et al. Baseline circulating IL-17 predicts toxicity while TGF-β1 and IL-10 are prognostic of relapse in ipilimumab neoadjuvant therapy of melanoma. J Immunother Cancer. 2015;3:39. doi:10.1186/s40425-015-0081-1
31. von Euw E, Chodon T, Attar N, et al. CTLA4 blockade increases Th17 cells in patients with metastatic melanoma. J Transl Med. 2009;7:35. doi:10.1186/1479-5876-7-35
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Simultaneous and Sequential Use of Molecular Targeted Agents Plus Immune Checkpoint Inhibitors for Advanced Hepatocellular Carcinoma: A Real-World Practice in China
Li J, Huang L, Ge C, Zhu X, Qiu M, Chen C, Wei S, Yan Y
Journal of Hepatocellular Carcinoma 2023, 10:949-958
Published Date: 20 June 2023
Onychopathy Following Durvalumab Treatment for Extensive-Stage Small-Cell Lung Cancer: A Case Report
Zhang C, Wang K, Zhang H, Liu J, Zheng C, Tao J, Lin L, Zhai L
Clinical, Cosmetic and Investigational Dermatology 2023, 16:2429-2432
Published Date: 5 September 2023
The Extended Surgical Concepts for Hepatocellular Carcinoma in the Era of Immune Checkpoint Inhibitors
Hsu HM, Tsai HI, Lee WC, Wang CC, Yu MC, Lin SM, Lin CY, Wu CH, Lee CW
Journal of Hepatocellular Carcinoma 2023, 10:1873-1880
Published Date: 24 October 2023
Transarterial Chemoembolization Combined with Tyrosine Kinase Inhibitors Plus Immune Checkpoint Inhibitors for Advanced Hepatocellular Carcinoma: A Propensity Score Matching Analysis
Gao B, Yang F, Zheng D, Hu S, Liu J, Liu H, Liu Y, Liu L, Wang R, Zhao Y, Cui C, Fang C, Yang J, Su S, Han Y, Yang X, Li B
Journal of Hepatocellular Carcinoma 2023, 10:2265-2276
Published Date: 13 December 2023
Immune Checkpoint Inhibitor-Associated Systemic Sclerosis in the Treatment of a Small Cell Lung Cancer Patient with Durvalumab: A Case Report
Li DH, Xiong XZ
Clinical, Cosmetic and Investigational Dermatology 2024, 17:663-669
Published Date: 18 March 2024