Back to Journals » Cancer Management and Research » Volume 18

Baseline Nutritional Indices as Prognostic Indicators in Patients with Recurrent or Metastatic Nasopharyngeal Carcinoma Treated with the PD-L1 Inhibitor KL-A167: A Secondary Analysis of the KL-A167 Trial
Authors Li H, Liu Z, Li J ![]() , Wei Z, Li R, Pei Y, Min Y, Song G, Gao K, Qin Z, Ge J, Qing Y, Wei Y, Zhou J, Peng X
, Wei Z, Li R, Pei Y, Min Y, Song G, Gao K, Qin Z, Ge J, Qing Y, Wei Y, Zhou J, Peng X ![]()
Received 30 March 2026
Accepted for publication 19 June 2026
Published 24 June 2026 Volume 2026:18 611346
DOI https://doi.org/10.2147/CMAR.S611346
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Harikrishna Nakshatri
Huilin Li,1,* Zheran Liu,1,* Jiacheng Li,2,* Zhigong Wei,1 Ruidan Li,1 Yiyan Pei,1 Yu Min,1 Ge Song,1 Kun Gao,1,3 Zijian Qin,1 Junyou Ge,4 Yan Qing,4 Youneng Wei,4 Jitao Zhou,5 Xingchen Peng1,6
1Department of Biotherapy, Cancer Center, West China Hospital, Sichuan University, Chengdu, Sichuan, People’s Republic of China; 2College of Medical and Life Sciences, Chengdu University of Traditional Chinese Medicine, Chengdu, Sichuan, People’s Republic of China; 3Department of Radiation Oncology, Cancer Center, West China Hospital, Sichuan University, Chengdu, Sichuan, People’s Republic of China; 4Sichuan Kelun-Biotech Biopharmaceutical Co., Ltd, Chengdu, Sichuan, People’s Republic of China; 5Department of Abdominal Oncology, Cancer Center, West China Hospital, Sichuan University, Chengdu, Sichuan, People’s Republic of China; 6Nuclear Physics and Medical Research Key Laboratory of Sichuan Province, Sichuan University, Chengdu, Sichuan, People’s Republic of China
*Huilin Li, Zheran Liu and Jiacheng Li contributed equally to this work
Correspondence: Xingchen Peng, Department of Biotherapy, Cancer Center, West China Hospital, Sichuan University, Chengdu, Sichuan, People’s Republic of China, Email [email protected]; [email protected] Jitao Zhou, Department of Abdominal Oncology, Cancer Center, West China Hospital, Sichuan University, Chengdu, Sichuan, People’s Republic of China, Email [email protected]
Background: Nutritional status is a recognized prognostic factor in oncology. However, its impact on patients with recurrent or metastatic nasopharyngeal carcinoma (R/M NPC) treated with the PD-L1 inhibitor KL-A167 remains unclear.
Methods: We conducted a secondary exploratory analysis of the KL-A167 trial, which included 153 patients with R/M NPC who had progressed after at least two lines of chemotherapy. Baseline nutritional status was assessed using the Controlling Nutritional Status (CONUT) score, Nutritional Risk Index (NRI), and Prognostic Nutritional Index (PNI). The associations between these indices and survival outcomes, including overall survival (OS) and progression-free survival (PFS), were analyzed using Kaplan-Meier methods and Cox regression models.
Results: Baseline nutritional status was associated with survival outcomes. In multivariable Cox analyses as continuous variables, higher CONUT, lower NRI, and lower PNI were all independently associated with worse OS (all p < 0.01), while higher CONUT and lower PNI were independently associated with worse PFS (both p < 0.01). In categorical analyses, high CONUT and low PNI were independently associated with worse OS, and high CONUT, low NRI, and low PNI were independently associated with worse PFS.
Conclusion: Baseline nutritional indices, particularly PNI, were associated with OS and PFS in patients with R/M NPC treated with the PD-L1 inhibitor KL-A167. Routine baseline nutritional screening may help identify high-risk patients before immunotherapy, although the clinical benefits of early nutritional interventions remain to be confirmed.
Keywords: nasopharyngeal carcinoma, immunotherapy, immune checkpoint inhibitors, nutritional indices
Introduction
Nasopharyngeal carcinoma (NPC) is an epithelial malignancy of the nasopharynx associated with Epstein–Barr virus (EBV) infection. It is endemic to Southeast Asia, with an incidence of 4 to 25 cases per 100,000 people.1 While treatments like imaging, radiotherapy, and systemic therapies have improved survival,1–3 many patients still experience relapse or metastasis. Around 15% of patients present with metastatic disease, and 20% to 40% will eventually recur, which is associated with poor outcomes.4
Programmed death-1 ligand (PD-L1) is often overexpressed in NPC, which suppresses T-cell activity. This provides a rationale for using immune checkpoint inhibitors.2 Clinical trials have demonstrated survival benefits for anti-PD-L1 therapy in patients with chemotherapy-refractory recurrent or metastatic disease.5,6
Malnutrition is common in oncology and negatively impacts treatment response, toxicity, and quality of life.7 The Patient-Generated Subjective Global Assessment (PG-SGA) is a standard tool, but simpler laboratory-based indices are frequently used. The Controlling Nutritional Status (CONUT) score, Nutritional Risk Index (NRI), and Prognostic Nutritional Index (PNI) are examples that have shown prognostic value in various cancers.8–12
Recent studies suggest a link between baseline nutrition and immunotherapy outcomes.13,14 However, most data involve PD-1 rather than PD-L1 inhibitors, and the prognostic role of these indices in R/M NPC remains uncertain. For instance, our prior work demonstrated that anatomical tumor burden, specifically baseline liver metastasis, was an independent adverse prognostic factor for survival.15 However, evaluating the host’s systemic state offers a complementary and potentially modifiable dimension compared to fixed anatomical characteristics. In this study, we selected three widely used nutritional indices – CONUT, NRI, and PNI. These indices combine different biological parameters (serum albumin, lymphocyte count, total cholesterol, and body weight/height) that collectively reflect visceral protein reserves, systemic inflammation, metabolic status, and host anti-tumor immunity. Therefore, we conducted a secondary exploratory analysis of the KL-A167 trial to clarify the prognostic significance of these baseline nutritional indices in patients with R/M NPC treated with the PD-L1 inhibitor KL-A167.
Methods
Study Population
This is a secondary exploratory analysis of the open-label, multicenter, Phase II KL-A167 trial (NCT03848286). We included 153 patients with non-keratinizing R/M NPC. All patients had disease progression after at least two prior chemotherapy regimens, including at least one platinum-based treatment. The primary trial methods have been previously reported.16 Over the follow-up period, a total of 102 death events (66.67%) and 139 PFS events (90.85%) occurred. The median follow-up time was 27.7 months (95% CI: 26.9–28.6) for the intention-to-treat (ITT) population. The primary clinical outcomes were progression-free survival (PFS) and overall survival (OS). PFS was calculated from the date of the first dose of KL-A167 to the first occurrence of documented disease progression or death from any cause. OS was calculated from the date of the first dose of KL-A167 to death from any cause. Patients without progressive disease or death at the data cutoff were censored at the date of their last evaluable efficacy assessment. Efficacy was evaluated by investigators according to the Response Evaluation Criteria in Solid Tumors (RECIST) version 1.1. Radiographic tumor assessments (computed tomography or magnetic resonance imaging of the nasopharynx, head, neck, chest, abdomen, and pelvis) were performed at baseline, every 6 weeks during the first 24 months of treatment, and every 12 weeks thereafter until disease progression.
Evaluation of Nutrition Status
The CONUT score was derived from serum albumin, total cholesterol, and lymphocyte count.17 This composite index has been applied as a nutritional and prognostic marker in several diseases, including cancer, cardiovascular conditions, and liver disorders.18 The NRI, originally proposed by Buzby et al,19 was determined by: NRI = 1.489 × serum albumin (g/L) + 41.7 × (current body weight/usual body weight). However, because usual body weight (UBW) is often difficult to obtain objectively and typically relies on patient recall or estimation in clinical practice (which introduces memory/recall bias), ideal body weight (IBW) is commonly used as a substitute. In our study, current body weight and height were successfully obtained for all 153 patients (100%), and NRI was calculated for all patients using the IBW-based modified formula: NRI = 1.489 × serum albumin (g/L) + 41.7 × (current weight/ideal weight), where ideal weight was calculated using the Lorentz equations:20 Men: ideal weight = height (cm) - 100 - (height (cm) - 150)/4; Women: ideal weight = height (cm) - 100 - (height (cm) - 150)/2.5. The PNI, as defined by Onodera et al21 incorporated serum albumin and total lymphocyte count: PNI = 10 × albumin (g/dL) + 0.005 × lymphocyte count (/mm3). A summary of the definitions and thresholds for these indices is presented in Figure 1.
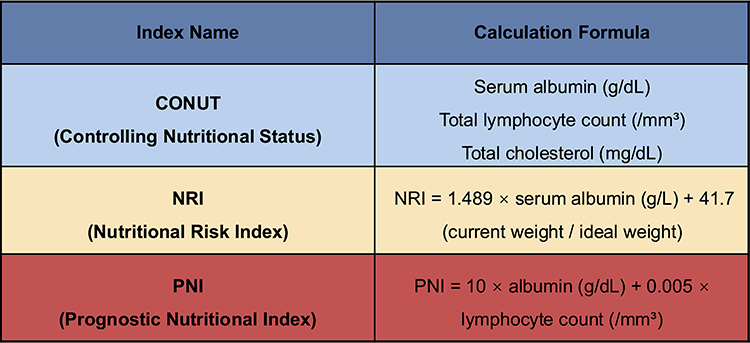 |
Figure 1 The definition, calculation formula, and scoring criteria of three nutritional indices. |
Statistical Methods
The outcome measures were OS and PFS. Survival was estimated using the Kaplan–Meier method and compared with Log rank tests. To identify independent prognostic factors, multivariable Cox proportional hazards regression models were constructed. Because the CONUT score, NRI, and PNI share variables (eg., serum albumin) and are highly correlated, they were entered into separate multivariable Cox regression models to prevent severe multicollinearity. The multivariable models were adjusted for baseline covariates including age, gender, T stage, N stage, smoking history, alcohol history, past radiotherapy history, Eastern Cooperative Oncology Group Performance Status (ECOG PS), and baseline liver metastasis. The proportional hazards assumption was tested using the Schoenfeld residuals method. Multicollinearity among the adjusted covariates within each separate model was evaluated using the Variance Inflation Factor (VIF). Analyses were performed in R (version 4.3.1), with a two-sided p-value < 0.05 considered statistically significant.
Results
Patient Characteristics
The study included 153 patients (mean age 47.6 ± 9.8 years; 81.7% male). By body mass index (BMI), 60.8% were normal weight, 19.0% were underweight and 20.3% were overweight. Baseline characteristics are detailed in Table 1.
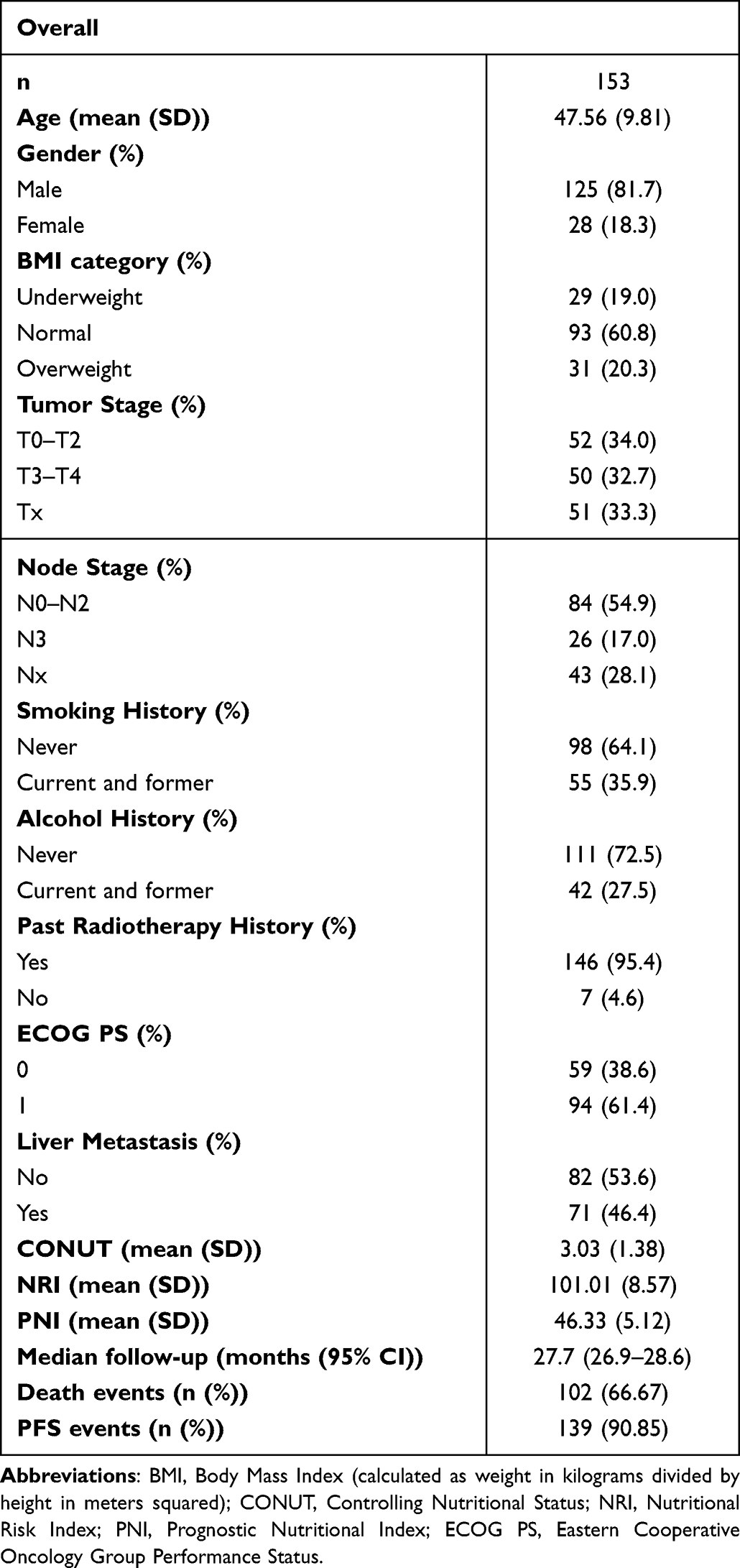 |
Table 1 Clinical and Demographic Characteristics of the KL-A167 Cohort |
Nutritional Indices Measurements and Correlations
Two patients were excluded from the CONUT analysis due to missing total cholesterol data; thus, CONUT was calculated for 151 patients, and NRI and PNI for 153 patients. Mean values were 3.03 ± 1.38 for CONUT, 101.01 ± 8.57 for NRI, and 46.33 ± 5.12 for PNI. Although clinical thresholds for these indices exist in the literature, they were developed for surgical or non-oncological populations. To maintain statistical power and reflect the specific distribution characteristics of this heavily pretreated R/M NPC cohort, patients were divided into high and low groups based on median values: CONUT = 3, NRI = 101.19, and PNI = 46.4. Spearman correlation analysis showed that NRI and PNI were strongly positively correlated, while CONUT was negatively correlated with both NRI and PNI (Figure 2).
 |
Figure 2 Correlation coefficients of three nutritional indices were calculated using Spearman’s rank correlation. Statistical significance is indicated as follows: * p < 0.05, ** p < 0.01, and *** p < 0.001; ns indicates not significant (p ≥ 0.05). Abbreviations: CONUT, Controlling Nutritional Status; NRI, Nutritional Risk Index; PNI, Prognostic Nutritional Index. |
The global test p-values for the multivariable models of CONUT, NRI, and PNI were 0.708, 0.740, and 0.640 for the continuous models, and 0.767, 0.780, and 0.760 for the categorical models, respectively, for OS; for PFS, the global test p-values were 0.408, 0.420, and 0.448 for the continuous models, and 0.520, 0.210, and 0.190 for the categorical models, respectively, indicating that the proportional hazards assumption was satisfied for all models. Additionally, the maximum equivalent VIF across all models was 2.01 (all VIFs < 5.0), indicating no significant multicollinearity.
Associations with Survival
Baseline nutritional indices were significantly associated with PFS, whereas only NRI and PNI were significantly associated with OS (Figure 3). There was no significant difference in OS between the high and low CONUT groups (p = 0.110), but the low CONUT group had a longer median PFS (93 vs 46 days, p = 0.012). The high-NRI group had better OS (500 vs 355 days, p = 0.010) and PFS (126 vs 40 days, p = 0.010) compared to the low-NRI group. The high-PNI group also showed longer OS (607 vs 322 days, p < 0.001) and PFS (130 vs 46 days, p = 0.018) than the low-PNI group.
 |
Figure 3 Kaplan-Meier curves of patients with high and low groups of nutritional indices. (A) Kaplan-Meier curve showing overall survival (i) and progression-free survival (ii) of patients with high and low CONUT; (B) Kaplan-Meier curve showing overall survival (i) and progression-free survival (ii) of patients with high and low NRI; (C) Kaplan-Meier curve showing overall survival (i) and progression-free survival (ii) of patients with high and low PNI. |
Multivariable Cox regression analyses (Tables 2 and 3) assessed the independent prognostic value of these indices. As continuous variables for OS, higher CONUT scores were associated with an increased risk of mortality (HR 1.28, 95% CI 1.09–1.49; p = 0.002), while higher NRI (HR 0.96, 95% CI 0.94–0.99; p = 0.002) and PNI (HR 0.92, 95% CI 0.88–0.96; p < 0.001) were protective. In the categorical analyses, high CONUT (HR 1.61, 95% CI 1.02–2.57; p = 0.043) and high PNI (HR 0.61, 95% CI 0.39–0.95; p = 0.030) remained independent prognostic factors for OS, whereas categorical NRI did not exhibit a statistically significant association with OS (p = 0.179).
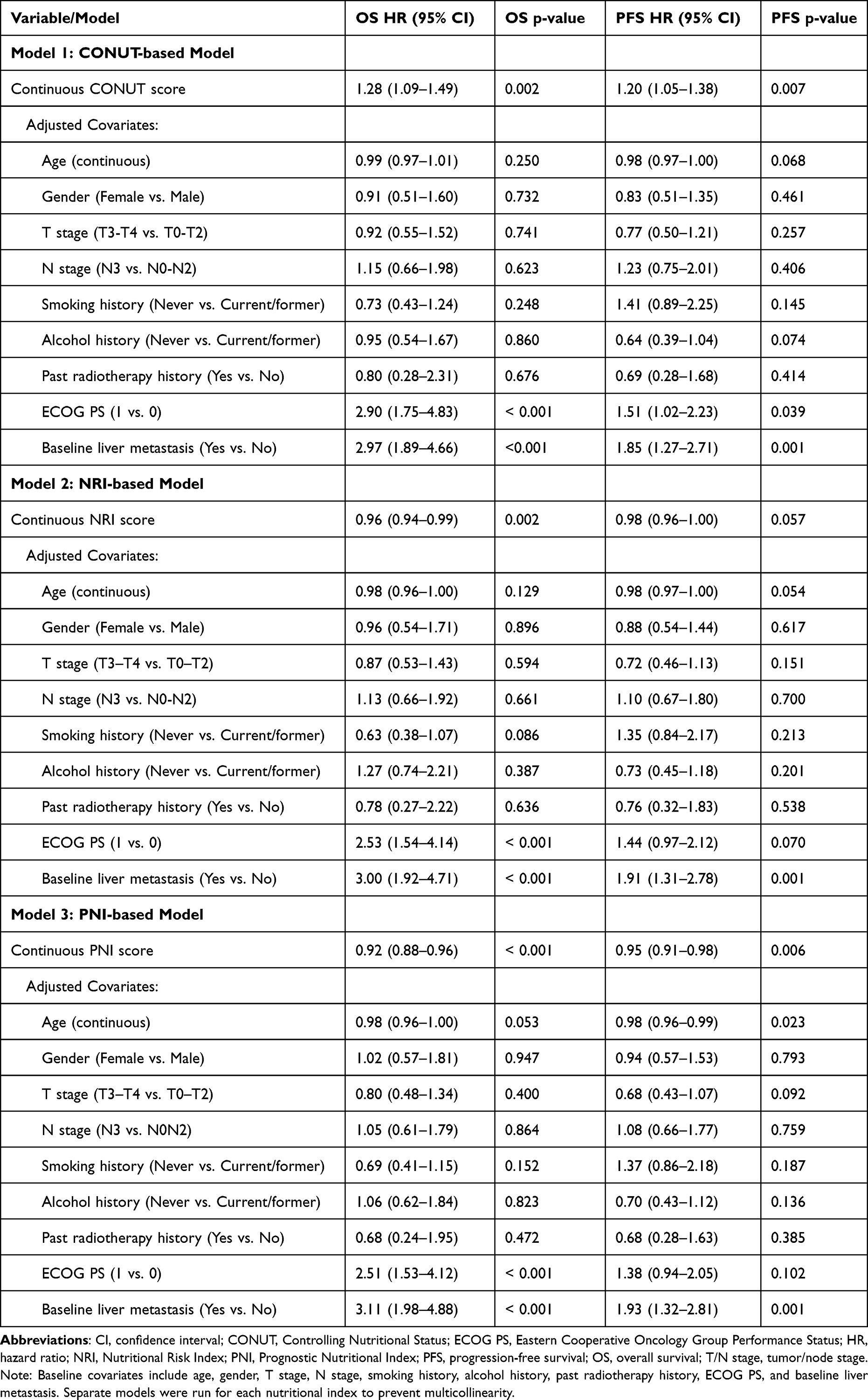 |
Table 2 Multivariable Cox Proportional Hazards Regression Analyses of Baseline Nutritional Indices (Continuous) for Overall Survival (OS) and Progression-Free Survival (PFS) in Separate Models |
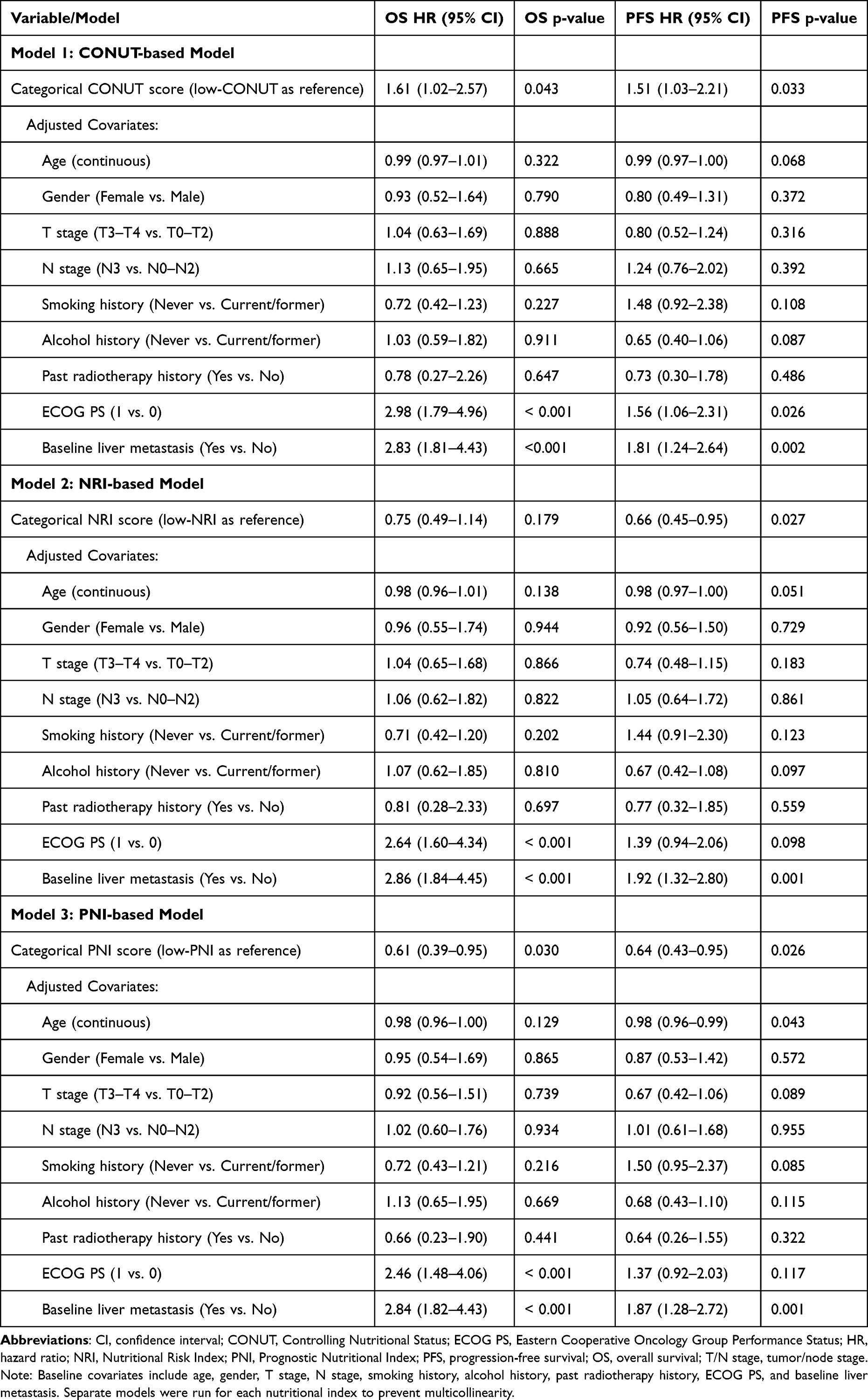 |
Table 3 Multivariable Cox Proportional Hazards Regression Analyses of Baseline Nutritional Indices (Categorical) for Overall Survival (OS) and Progression-Free Survival (PFS) in Separate Models |
For PFS, continuous CONUT was associated with increased progression risk (HR 1.20, 95% CI 1.05–1.38; p = 0.007). Continuous NRI was borderline associated with decreased risk of progression (HR 0.98, 95% CI 0.96–1.00; p = 0.057), and continuous PNI was associated with decreased risk (HR 0.95, 95% CI 0.91–0.98; p = 0.006). Categorical analyses showed significant associations with PFS for high CONUT (HR 1.51, 95% CI 1.03–2.21; p = 0.033), high NRI (HR 0.66, 95% CI 0.45–0.95; p = 0.027), and high PNI (HR 0.64, 95% CI 0.43–0.95; p = 0.026). All multivariable hazard ratios, confidence intervals, and p-values for the nutritional indices and adjusted covariates are detailed in Tables 2 and 3.
Discussion
This secondary exploratory analysis evaluated the prognostic value of baseline nutritional status in patients with R/M NPC receiving the PD-L1 inhibitor KL-A167. While our previous analysis of the identical KL-A167 trial cohort established the prognostic impact of anatomical tumor burden, specifically identifying baseline liver metastasis as an independent adverse factor,15 the present study explores the dataset from a complementary host-centric dimension. This is consistent with other immunotherapeutic settings, where combining anatomical indices (such as tumor burden score) with biochemical markers (such as alpha-fetoprotein) has been shown to effectively predict survival outcomes in patients treated with anti-PD-1 antibodies.22 We demonstrated that baseline nutritional indices are independently associated with survival outcomes: continuous CONUT, NRI, and PNI are associated with OS, while continuous CONUT and PNI are associated with PFS. In categorical analyses, CONUT and PNI are independent prognostic factors for OS, and all three indices (CONUT, NRI, and PNI) are independent prognostic factors for PFS. It is important to distinguish between prognostic and predictive biomarkers: our findings indicate a prognostic association (correlating baseline host status with survival outcomes) rather than a predictive capacity to determine specific therapeutic benefit from PD-L1 inhibitors compared to other agents. Given the rapid evolution of cancer immunotherapy, including immune checkpoint inhibitors and novel therapeutic vaccines,23 identifying reliable prognostic biomarkers is crucial to optimize treatment outcomes in advanced settings. Unlike fixed anatomical characteristics, these blood-based nutritional indices (CONUT, NRI, and PNI) represent modifiable host factors, supporting further evaluation of baseline nutritional screening as a risk-stratification tool.
The prognostic value of these indices lies in their integration of key physiological parameters reflecting protein reserves, systemic inflammation, and host immunity. Serum albumin is a classic marker of visceral protein reserves. Hypoalbuminemia reflects systemic inflammation and cancer-associated malnutrition, which impairs drug metabolism and increases systemic toxicity. Lymphocytes are the cellular cornerstones of host anti-tumor immunity. Lymphopenia compromises the immune system’s capacity to mount an effective response against tumor antigens, thereby limiting the efficacy of immune checkpoint inhibitors. This is particularly relevant in patients who have undergone prior radiotherapy, as exposure of peripheral blood lymphocytes to X-rays can induce significant DNA damage and alter their immune function.24 Total cholesterol reflects cellular membrane integrity and lipid metabolism; low cholesterol is associated with advanced cachexia and impaired antigen-presenting cell function. Finally, weight loss, captured by body weight changes in the NRI, is a hallmark of cancer cachexia, reflecting systemic metabolic derangement and predicting shortened survival across diverse cancer types.25 Together, these markers reflect the host’s physiological resilience and immune competence.
Several potential clinical confounders could influence the relationship between baseline nutritional status and survival. For instance, baseline liver metastasis (present in 46.4% of this cohort) can impair hepatic albumin synthesis and cholesterol metabolism, acting as a major confounder. Other factors, such as high EBV DNA load, elevated lactate dehydrogenase (LDH), and C-reactive protein (CRP), represent high tumor burden and systemic inflammatory status, which are intrinsically linked to malnutrition. Additionally, active infections or the use of systemic corticosteroids (which was restricted in the trial to <=10 mg daily prednisone equivalent within 14 days of the first dose) can cause lymphopenia or alter weight. Prior heavy treatment lines (all patients failed ≥2 lines of chemotherapy) also accumulate hematological and nutritional toxicity. While our multivariable Cox models adjusted for several major baseline confounders—including age, sex, tumor/node stage, prior radiotherapy, ECOG PS, and liver metastasis—residual confounding from unmeasured inflammatory factors (like CRP or cytokines) cannot be completely excluded.
In our cohort, 19.0% of patients were underweight, reflecting the long-term radiotherapy-induced toxicities (eg., dysphagia, xerostomia, open mouth difficulty) common in R/M NPC patients (95.4% of our cohort had prior radiotherapy) that impair oral intake and lead to progressive malnutrition. These results align with findings in other immunotherapy settings, such as advanced lung and head and neck cancers, where baseline PNI and NRI predict outcomes.13,14 The strong correlation among CONUT, NRI, and PNI is expected due to shared parameters (eg., albumin and lymphocytes); in clinical practice, PNI may be the most practical because it requires only blood-based albumin and lymphocyte counts, bypassing height and weight data that are frequently missing or inaccurate in databases. Based on our findings, we hypothesize that early dietary counseling and multidisciplinary nutritional support prior to immunotherapy might preserve host physiological reserves and may help preserve nutritional status and deserves prospective evaluation, consistent with ASCO clinical guidelines.26
Malnutrition affects more than half of patients with advanced cancer, contributing to approximately 20% of cancer-related deaths and reducing treatment tolerance while increasing complication risks.9,22,23 This impairment is closely linked to chronic systemic inflammation, which drives cancer cachexia via cytokine pathways (such as IL-6 and TNF-α) in a bidirectional manner—malnutrition suppresses immune function, while inflammation accelerates muscle wasting.27,28 Consequently, routine baseline nutritional screening combined with early anti-inflammatory and dietary support may help identify patients who require closer nutritional assessment before immunotherapy; prospective trials are needed to test whether intervention changes outcomes.9,22,23,27,28
This study has limitations that should be acknowledged. First, it is a post-hoc secondary exploratory analysis of a single-arm phase II trial, which limits the level of evidence. Second, we lacked an independent external validation cohort to confirm the generalizability of our findings, the median cutoffs were data-driven and have not been externally validated. Third, the sample size (n=153) is relatively small, which limits the statistical power of subgroup analyses. Fourth, nutritional status was only assessed at baseline, and we lacked longitudinal, dynamic nutritional data during immunotherapy to evaluate whether nutritional changes correlate with survival. Fifth, despite adjusting for multiple baseline variables, there remains a potential for residual confounding from unmeasured factors, such as C-reactive protein, interleukin-6, and other systemic inflammatory cytokines. Lastly the use of ideal body weight instead of usual body weight for the entire cohort alters the standard clinical definition of the NRI, making it behave closer to a modified NRI index.
In conclusion, baseline nutritional indices, particularly PNI, were associated with OS and PFS in patients with R/M NPC treated with the PD-L1 inhibitor KL-A167. These markers may help identify high-risk patients before immunotherapy. Prospective studies are needed to determine whether nutritional or anti-inflammatory interventions can improve treatment outcomes in this population.
Abbreviations
PD-L1, Programmed death-1 ligand; R/M NPC, Recurrent or metastatic nasopharyngeal carcinoma; CONUT, Controlling Nutritional Status; NRI, Nutritional Risk Index; PNI, Prognostic Nutritional Index; OS, Overall survival; PFS, Progression-free survival; NPC, Nasopharyngeal carcinoma; EBV, Epstein–Barr virus; PG-SGA, Patient-Generated Subjective Global Assessment; HR, Hazard ratio; CI, Confidence interval; ECOG, Eastern Cooperative Oncology Group; BMI, Body mass index; SD, Standard deviation; IL-6, Interleukin-6; TNF-α, Tumor necrosis factor-alpha.
Data Sharing Statement
The data utilized in our study, derived from the KL-A167 cohort, are subject to privacy regulations and institutional policies that protect participant confidentiality. Consequently, the complete data set is not publicly accessible. Requests should include a detailed research proposal and demonstrate compliance with ethical standards. Approval from the respective institutional review boards will be required inquiries should be directed to XP (West China Hospital).
Ethics Approval and Consent to Participate
The study adhered to the principles of the Declaration of Helsinki and the International Council for Harmonization’s guidelines for Good Clinical Practice. The study protocol was approved by the Ethics Committee on Clinical Trial, West China Hospital of Sichuan University (Approval Number: HX-IRB-AF-12-V4.0). Prior to enrollment, all participants provided written informed consent.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The work was supported by the Noncommunicable Chronic Diseases-National Science and Technology Major Project (2023ZD0503000, 2023ZD0503004), Fundamental and Interdisciplinary Disciplines Breakthrough Plan of the Ministry of Education of China (JYB2025XDXM607), the Institutional Joint Innovation Fund from Sichuan University and Nuclear Power Institute of China (LHCX-2024-JJ), Sichuan Science and Technology Program (2025YFHZ0087), Science and Technology Project of Sichuan Provincial Health Commission (Clinical Research Special Project JH2023082), the International Science and Technology Cooperation Program of Chengdu Science and Technology Bureau (2024-YF06-00011-HZ and 2022-GH03-00004-HZ), the Health Research Project of Chengdu Eastern New Area Management Committee (202304), 1.3.5 project for disciplines of excellence from West China Hospital of Sichuan University (ZYYC23006), Clinical Research Incubation Project of West China Hospital (23HXFH001), Clinical Research Youth Fund of West China Hospital (2025HXFH028), West China Hospital “Qimingxing” Research Fund for Young Talents (HXQMX0184), Yunnan Province Key Laboratory of Precision Diagnosis and Treatment for Thoracic Diseases (202449CE340026), National Key R&D·Program of China (2023YFC3403200) and the Ministry of Education University-Industry Collaborative Education Program (230720523707281). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
Junyou Ge, Yan Qing, and Youneng Wei are employees of Sichuan Kelun-Biotech Biopharmaceutical Co., Ltd. (the sponsor of the KL-A167 trial). Their roles in the trial were limited to trial coordination. They had no role in the design of this secondary analysis, the statistical modeling of the nutritional indices, or the decision to submit the manuscript. The authors report no other conflicts of interest in this work.
References
1. Wong KCW, Hui EP, Lo KW, et al. Nasopharyngeal carcinoma: an evolving paradigm. Nat Rev Clin Oncol. 2021;18(11):11. doi:10.1038/s41571-021-00524-x
2. Chen YP, Chan ATC, Le QT, Blanchard P, Sun Y, Ma J. Nasopharyngeal carcinoma. Lancet. 2019;394(10192):64–13. doi:10.1016/S0140-6736(19)30956-0
3. Liu X, Shen H, Zhang L, Huang W, Zhang S, Zhang B. Immunotherapy for recurrent or metastatic nasopharyngeal carcinoma. Npj Precis Oncol. 2024;8(1):101. doi:10.1038/s41698-024-00601-1
4. Zhang L, Huang Y, Hong S, et al. Gemcitabine plus cisplatin versus fluorouracil plus cisplatin in recurrent or metastatic nasopharyngeal carcinoma: a multicentre, randomised, open-label, Phase 3 trial. Lancet Lond Engl. 2016;388(10054):1883–1892. doi:10.1016/S0140-6736(16)31388-5
5. Adkins DR, Haddad RI. Clinical trial data of Anti–PD-1/PD-L1 therapy for recurrent or metastatic nasopharyngeal Carcinoma: a review. Cancer Treat Rev. 2022;109:102428. doi:10.1016/j.ctrv.2022.102428
6. Chong WQ, Low JL, Tay JK, et al. Pembrolizumab with or without bevacizumab in platinum-resistant recurrent or metastatic nasopharyngeal carcinoma: a randomised, open-label, Phase 2 trial. Lancet Oncol. 2025;26(2):175–186. doi:10.1016/S1470-2045(24)00677-6
7. Bossi P, Delrio P, Mascheroni A, Zanetti M. The spectrum of malnutrition/cachexia/sarcopenia in oncology according to different cancer types and settings: a narrative review. Nutrients. 2021;13(6):6. doi:10.3390/nu13061980
8. Sun H, Chen L, Huang R, et al. Prognostic nutritional index for predicting the clinical outcomes of patients with gastric cancer who received immune checkpoint inhibitors. Front Nutr. 2022:9. doi:10.3389/fnut.2022.1038118.
9. Przekop Z, Szostak-Węgierek D, Milewska M, Panczyk M, Zaczek Z, Sobocki J. Efficacy of the Nutritional Risk Index, Geriatric Nutritional Risk Index, BMI, and GLIM-Defined Malnutrition in Predicting Survival of Patients with Head and Neck Cancer Patients Qualified for Home Enteral Nutrition. Nutrients. 2022;14(6):6. doi:10.3390/nu14061268
10. Chen L, Qi Y, Kong X, et al. Nutritional risk index predicts survival in patients with breast cancer treated with neoadjuvant chemotherapy. Front Nutr. 2022:8. doi:10.3389/fnut.2021.786742.
11. Luan CW, Tsai YT, Yang HY, Chen KY, Chen PH, Chou HH. Pretreatment prognostic nutritional index as a prognostic marker in head and neck cancer: a systematic review and meta-analysis. Sci Rep. 2021;11(1):17117. doi:10.1038/s41598-021-96598-9
12. Takagi K, Buettner S, Ijzermans JNM. Prognostic significance of the controlling nutritional status (CONUT) score in patients with colorectal cancer: a systematic review and meta-analysis. Int J Surg. 2020;78:91–96. doi:10.1016/j.ijsu.2020.04.046
13. Haas M, Lein A, Fuereder T, et al. The Geriatric Nutritional Risk Index (GNRI) as a Prognostic Biomarker for Immune Checkpoint Inhibitor Response in Recurrent and/or Metastatic Head and Neck Cancer. Nutrients. 2023;15(4):4. doi:10.3390/nu15040880
14. Johannet P, Sawyers A, Qian Y, et al. Baseline prognostic nutritional index and changes in pretreatment body mass index associate with immunotherapy response in patients with advanced cancer. J Immunother Cancer. 2020;8(2):e001674. doi:10.1136/jitc-2020-001674
15. Li Y, Min Y, Wei Z, et al. Metastatic sites of baseline as predictors in recurrent or metastatic nasopharyngeal carinoma treated with PD-L1 inhibitor: a secondary analysis of multicenter, single-arm, phase II study (KL-A167). Cancer Immunol Immunother. 2025;74(2):72. doi:10.1007/s00262-024-03905-0
16. Shi Y, Qin X, Peng X, et al. Efficacy and safety of KL-A167 in previously treated recurrent or metastatic nasopharyngeal carcinoma: a multicenter, single-arm, phase 2 study. Lancet Reg Health West Pac. 2022;31:100617. doi:10.1016/j.lanwpc.2022.100617
17. de Ulíbarri JI, González-Madroño A, de Villar NG, et al. CONUT: a tool for Controlling Nutritional Status. First validation in a hospital population. Nutr Hosp.
18. Kheirouri S, Alizadeh M. Prognostic Potential of the Preoperative Controlling Nutritional Status (CONUT) Score in Predicting Survival of Patients with Cancer: a Systematic Review. Adv Nutr. 2021;12(1):234–250. doi:10.1093/advances/nmaa102
19. Buzby GP, Williford WO, Peterson OL, et al. A randomized clinical trial of total parenteral nutrition in malnourished surgical patients: the rationale and impact of previous clinical trials and pilot study on protocol design. Am J Clin Nutr. 1988;47(2 Suppl):357–365. doi:10.1093/ajcn/47.2.357
20. Bouillanne O, Morineau G, Dupont C, et al. Geriatric Nutritional Risk Index: a new index for evaluating at-risk elderly medical patients2. Am J Clin Nutr. 2005;82(4):777–783. doi:10.1093/ajcn/82.4.777
21. Onodera T, Goseki N, Kosaki G. Prognostic nutritional index in gastrointestinal surgery of malnourished cancer patients. Nihon Geka Gakkai Zasshi. 1984;85(9):1001–1005.
22. Molfino A, Imbimbo G, Laviano A. Current screening methods for the risk or presence of malnutrition in cancer patients. Cancer Manag Res. 2022;14:561–567. doi:10.2147/CMAR.S294105
23. Marshall KM, Loeliger J, Nolte L, Kelaart A, Kiss NK. Prevalence of malnutrition and impact on clinical outcomes in cancer services: a comparison of two time points. Clin Nutr. 2019;38(2):644–651. doi:10.1016/j.clnu.2018.04.007
24. Sioen S, D’Hondt L, Van Houte F, et al. Peripheral blood lymphocytes differ in DNA damage response after exposure to X-rays with different physical properties. Int J Radiat Biol. 2024;100(2):236–247. doi:10.1080/09553002.2023.2261525
25. Martin L, Senesse P, Gioulbasanis I, et al. Diagnostic criteria for the classification of cancer-associated weight loss. J Clin Oncol. 2015;33(1):90–99. doi:10.1200/JCO.2014.56.1894
26. Ligibel JA, Bohlke K, May AM, et al. Exercise, Diet, and Weight Management During Cancer Treatment: ASCO Guideline. J Clin Oncol. 2022;40(22):2491–2507. doi:10.1200/JCO.22.00687
27. Greten FR, Grivennikov SI. Inflammation and Cancer: triggers, Mechanisms, and Consequences. Immunity. 2019;51(1):27–41. doi:10.1016/j.immuni.2019.06.025
28. Xie H, Ruan G, Ge Y, et al. Inflammatory burden as a prognostic biomarker for cancer. Clin Nutr. 2022;41(6):1236–1243. doi:10.1016/j.clnu.2022.04.019
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Immunotherapy for Urothelial Carcinoma: Focus on Clinical Utility of Nivolumab
Chiang RS, Glover MJ, Khaki AR, Srinivas S
OncoTargets and Therapy 2022, 15:1259-1269
Published Date: 20 October 2022
The Extended Surgical Concepts for Hepatocellular Carcinoma in the Era of Immune Checkpoint Inhibitors
Hsu HM, Tsai HI, Lee WC, Wang CC, Yu MC, Lin SM, Lin CY, Wu CH, Lee CW
Journal of Hepatocellular Carcinoma 2023, 10:1873-1880
Published Date: 24 October 2023
Lethal Immune Myocarditis and Myasthenia Gravis Due to Anti-PD-1 Treatment for a Bladder Cancer Patient: A Case Report and Possible Treatment Inspiration
Gao P, Li X, He Z, Zhang H, Zhang Z, Liu Z
International Medical Case Reports Journal 2024, 17:359-365
Published Date: 18 April 2024
Recent Advances in Immunotherapy for Breast Cancer: A Review
Wen QE, Li L, Feng RQ, Li DH, Qiao C, Xu XS, Zhang YJ
Breast Cancer: Targets and Therapy 2024, 16:497-516
Published Date: 27 August 2024
Clinical Significance and Molecular Annotation for PD-L1 Negative Advanced Non-Small Cell Lung Cancer with Sensitivity to Responsive to Dual PD-1/CTLA-4 Blockade
Wang L, Liu L, Zhao J, Yu X, Su C
ImmunoTargets and Therapy 2024, 13:435-445
Published Date: 6 September 2024