")
Back to Journals » OncoTargets and Therapy » Volume 15
Immunotherapy for Urothelial Carcinoma: Focus on Clinical Utility of Nivolumab
Authors Chiang RS, Glover MJ, Khaki AR, Srinivas S
Received 1 April 2022
Accepted for publication 27 September 2022
Published 20 October 2022 Volume 2022:15 Pages 1259—1269
DOI https://doi.org/10.2147/OTT.S369043
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Sanjeev K. Srivastava
Ryan S Chiang,1 Michael J Glover,1 Ali Raza Khaki,2 Sandy Srinivas2
1Department of Medicine, Stanford University, Stanford, CA, USA; 2Division of Oncology, Department of Medicine, Stanford University, Stanford, CA, USA
Correspondence: Sandy Srinivas, Division of Oncology, Department of Medicine, Stanford University, 875 Blake Wilbur Drive, Clinic E, Stanford, CA, 94305, USA, Tel +1 650-725-2078, Email [email protected]
Abstract: Over the past decade, the emergence of immune checkpoint inhibitors has brought about significant change to the treatment landscape of bladder cancer. Nivolumab is an immune checkpoint inhibitor that has shown favorable results resulting in FDA approval for treatment of platinum-refractory locally advanced or metastatic urothelial carcinoma. More recently, it was the first (and only) immune checkpoint inhibitor to receive FDA approval for the treatment of urothelial carcinoma in the adjuvant setting after radical surgery. Multiple trials are now actively underway to further understand the nuances in which immune checkpoint inhibitors such as nivolumab can be beneficial. In this review, we explore the development of nivolumab in terms of its mechanism of action, its growing indications in the treatment of urothelial carcinoma, and potential future directions for clinical trials. Immune checkpoint inhibitors are a promising treatment for bladder cancer, but further work is needed to continue to improve outcomes for patients.
Keywords: immune checkpoint inhibitors, immunotherapy, nivolumab, urothelial carcinoma, bladder cancer
Introduction to Bladder Cancer
The treatment landscape for urothelial carcinoma (UC) has undergone a renaissance. Since 2017, eight new medications have received approval from the US Food and Drug Administration (FDA) for the treatment of this disease. These new therapies include five immune checkpoint inhibitors (ICIs), though one (durvalumab) subsequently withdrew its UC indication, two antibody-drug conjugates (enfortumab vedotin, sacituzumab govitecan) and one tyrosine kinase inhibitor (erdafitinib).
ICIs have improved outcomes for patients with UC with multiple agents showing efficacy in different treatment settings. Currently, there is level 1 evidence to support the use of ICIs for patients previously treated with platinum-based chemotherapy, either as switch-maintenance therapy (avelumab) for those with non-progressive disease or some response to platinum chemotherapy or for platinum-refractory disease as a second line or salvage therapy. Additional treatment indications include for treatment-naive patients with locally advanced, unresectable or metastatic UC who are cisplatin-ineligible with high PD-L1 expression, or for patients who are platinum-ineligible (irrespective of PD-L1 expression), for BCG-refractory non-muscle invasive bladder cancer (NMIBC) with carcinoma in situ and as an adjuvant therapy after extirpative surgery. Clinical trials are ongoing further exploring additional perioperative approaches and combination therapies.
Nivolumab is one of the ICIs that has shown efficacy in UC treatment. While the earliest indications for nivolumab included FDA approval for the treatment of metastatic melanoma, metastatic non-small cell lung cancer, and advanced renal cell carcinoma, it also received FDA accelerated approval for patients with platinum-refractory locally advanced or metastatic UC based on findings from Checkmate 275.1 More recently through the phase III double-blind Checkmate 274 clinical trial, nivolumab became the first FDA approved ICI for use in the adjuvant setting for patients with UC treated with radical surgery who are at high risk of recurrence.2
In this narrative review, we discuss the mechanism of action, current indications in different UC disease settings, and potential future directions for the use of the PD-1 inhibitor nivolumab in the treatment of UC. We reviewed the available trials on clinicaltrials.gov as part of our search methodology.
Mechanism of Action of Nivolumab
Immune checkpoint inhibitors (ICIs) are monoclonal antibodies that block programmed cell death protein 1 (PD-1) and its ligand (PD-L1) to enhance intrinsic antitumor mechanisms. They have been estimated to be a therapeutic option for many cancers and have become standard of care in several types of solid organ malignancies including UC.3 In UC, five ICIs received FDA approval (nivolumab, atezolizumab, pembrolizumab, durvalumab, and avelumab), though one (durvalumab) has since withdrawn this indication after a subsequent negative confirmatory trial.4
Nivolumab is a fully human anti-PD-1 IgG4 monoclonal antibody. Compared to cytotoxic chemotherapy, which primarily interferes with cell growth or division to inhibit tumor growth, immunotherapies focus on enhancement of one’s native immune defenses. Specifically, nivolumab and other ICIs can restore vital T-cell activity, which is the predominant method for elimination of cancer cells.5 This T-cell environment is intricate and involves elimination of regulatory T cells, recruiting CD4+ T cell support, and an interplay of various immune-related cytokines designed to assist CD8+ T cells in the destruction of tumor cells.
Immune checkpoints such as PD-1 and CTLA-4 are cell surface receptors expressed by T cells, B cells, and natural killer (NK) cells, which all normally assist in modulation of immune responses. This complex interplay creates a delicate balance between preventing autoimmunity from excessive surveillance and preventing cancerous growth. Cancer biology can often exploit this key aspect of the immune system through aberrant upregulation of PD-L1 in tumor cells, which can then neuter natural immune-mediated destruction. One additional proposed mechanism is that the upregulation of PD-1 may assist regulatory T cells to further suppress the immune response by inhibiting T cell proliferation and inflammatory cytokine production.5 Nivolumab and other anti-PD-1 antibodies inhibit the PD-1 mediated T-cell inhibition to rescue the effector function of T cells and prevent escape from immune cell recognition and allow natural cytolysis of cancer cells.
By tilting the immunoprofile towards greater recognition of self-antigens, this can result in greater risk for non-specific inflammation and autoimmunity in nearly any organ in the body. Therefore, it is paramount to provide close monitoring with interval clinic visits and routine lab work prior to each administration to monitor for immune-related adverse events such as thyroiditis, colitis, or immune injury to other organ systems. Fortunately, among those on ICI monotherapy, most of adverse events are low grade and can be managed without cessation of the treatment with strategies such as hormone replacement.
Clinical Evidence of Nivolumab
Non-Muscle Invasive Bladder Cancer
The majority of patients with UC present with hematuria and are found to have non-muscle invasive disease, which is generally associated with better outcomes given its earlier stage. However, for high-risk non-muscle invasive bladder cancer (NMIBC), patients have a greater risk of progression to muscle-invasive bladder cancer (MIBC) or metastatic disease. Therefore, these high-risk patients are treated with intravesical Bacillus Calmette-Guérin (BCG), an attenuated strain of Mycobacterium bovis, that has been the primary immunotherapy treatment option for several decades. For patients with BCG unresponsive disease, guidelines suggest pursuing radical cystectomy, which can result in increased risk of mortality from major surgery or increased morbidity and a lower quality of life.6 Bladder sparing options in this clinical scenario have historically been limited and have relied upon the use of intravesical chemotherapy, including mitomycin, gemcitabine, valrubicin and more recently sequential gemcitabine and docetaxel. However, investigations into ICIs have also begun demonstrating activity in the NMIBC clinical setting.
While no data from nivolumab has been shown in this setting, clinical trials are ongoing and there is precedence for ICI therapy in NMIBC, as pembrolizumab received FDA approval based on KEYNOTE-057, which showed a clinically complete response for patients with BCG unresponsive NMIBC with carcinoma in situ at a rate of 41% at 3 months and 19% at 1 year.7 There are several active clinical trials using nivolumab and other ICIs in the treatment of NMIBC (Table 1).8 For example, CheckMate 9UT is an ongoing phase II clinical trial assessing the use of combination nivolumab with BCG, indoleamine 2,3-dioxygenase, or both for patients with BCG unresponsive, high-risk NMIBC (NCT03519256).9
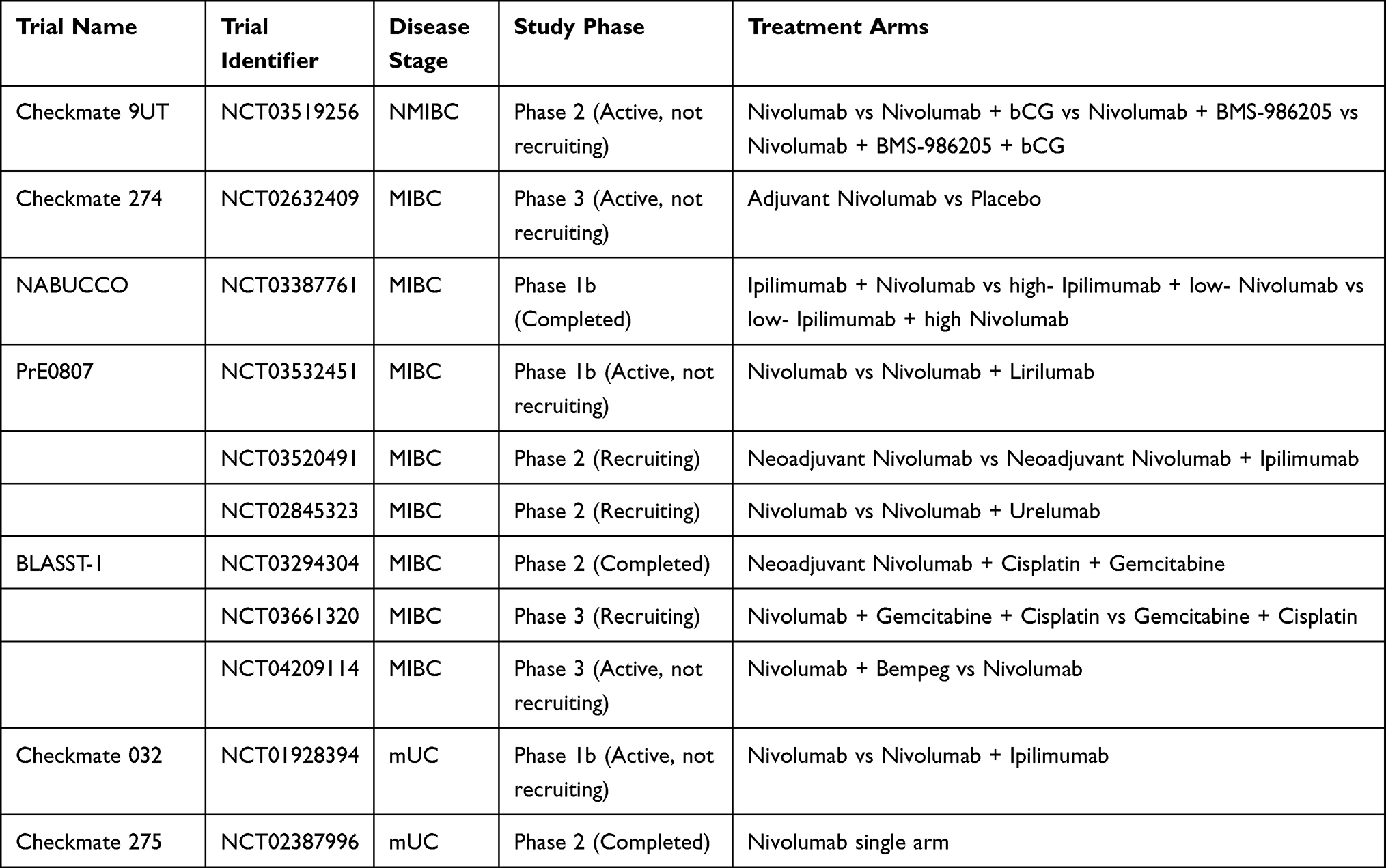 |
Table 1 Overview of Nivolumab Clinical Trials in Urothelial Carcinoma |
Muscle Invasive Bladder Cancer
Nearly 20% of patients with UC present with MIBC. The standard of care therapy for MIBC is neoadjuvant cisplatin-based chemotherapy followed by radical cystectomy with pelvic lymph node dissection, which has improved survival rates since its adoption.10,11 However, not all patients with MIBC are cisplatin chemotherapy candidates and many are also hesitant about undergoing a radical cystectomy given the associated morbidity and quality of life decrements. An alternate therapy for MIBC includes bladder-preservation with chemoradiation, which has been shown to improve outcomes compared with radiation alone.12 ICI treatment options for MIBC have been actively studied in recent years in both the neoadjuvant and adjuvant setting, including in patients who are cisplatin-ineligible. With the advent of ICIs, there may also be increased possibilities for bladder preservation strategies using a variety of different combinations including chemotherapy and/or ICIs with radiation therapy.13
Studies have been investigating the use of ICIs in the adjuvant setting after radical cystectomy for treatment of MIBC. A phase 3 clinical trial (Checkmate 274) found that, with the intention to treat population, the median survival free from recurrence was 22.9 months with nivolumab compared to 13.7 months with placebo regardless of PD-L1 status or nodal status. Patients with PD-L1 expression of 1% or more who received adjuvant nivolumab had improved median disease-free survival (DFS) compared to placebo (20.8 months vs.10.8 months), and the percentage of patients alive at 6 months was 74.9% with adjuvant nivolumab compared to 60.3% with placebo.2
Conversely, the IMvigor010 (NCT02450331) investigating a similar role as adjuvant therapy for atezolizumab was a negative study. In this study, patients with MIBC with high risk of recurrence after radical surgery were randomized to atezolizumab or observation.14 Atezolizumab did not show statistically significant benefit in DFS (HR 0.89, P = 0.245) in the overall population or in those with IC2/3 (defined as PD-L1 expressing tumor-infiltrating immune cells covering ≥5% of the tumor area). One notable difference in study design between IMvigor010 and Checkmate 274 was the use of observation rather than an active placebo control, which may have changed surveillance patterns or initiation of subsequent therapy and contributed to the difference in study results between studies. In addition, the PD-L1 assays used in the two studies were also different from the IMvigor study using the Ventana SP142 assay staining for PD-L1 expression on tumor-infiltrating immune cells, whereas Checkmate 274 used the pharmDx 28–8 assay staining for PD-L1 expression on tumor cells. Notably, an exploratory analysis of the trial population stratified by circulating tumor DNA (ctDNA) positivity immediately after surgery suggests that atezolizumab may have a role in patients who are ctDNA positive, as this subpopulation had improved DFS (HR 0.58, P = 0.0024) and OS (HR 0.59) with atezolizumab treatment when compared to observation.15 A follow-up study, IMvigor011, is underway to further evaluate this hypothesis and validate ctDNA as a potentially predictive biomarker (NCT04660344). A similar approach may also have utility with nivolumab and warrants further investigation to possibly spare patients in the future unnecessary therapies.
In addition to adjuvant therapy, there are several clinical trials evaluating the use of nivolumab as neoadjuvant therapy either as monotherapy or in combination with chemotherapy, other targeted therapies or immunotherapies. In patients with stage III UC, the NABUCCO trial showed a 46% pathologic complete response (pCR) rate in patients who received neoadjuvant ipilimumab (3mg/kg × 2 doses) plus nivolumab (1mg/kg × 1 and 3mg/kg × 1) followed by radical cystectomy.16 This pCR rate was numerically higher than what has been observed with neoadjuvant cisplatin chemotherapy and other ICI monotherapy studies.17–20 The ABACUS study of two cycles of neoadjuvant atezolizumab in 95 patients with MIBC had a pCR of 31%, and the PURE-01 study with three cycles of neoadjuvant pembrolizumab in 114 patients had a pCR of 37%.21,22
There are many ongoing neoadjuvant trials including nivolumab as monotherapy or in combination with other immunotherapies. Similar to the NABUCCO study, there is an ongoing phase 1b study (NCT03387761) and phase 2 study (NCT03520491) exploring the use of preoperative nivolumab and ipilimumab prior to radical cystectomy, with the phase 2 study also including a nivolumab monotherapy arm. In addition, other trials are investigating nivolumab with other potential immunotherapy agents. One phase 2 clinical trial is assessing the use of neoadjuvant nivolumab alone or in combination with urelumab, an anti-CD137 monoclonal antibody, in patients with MIBC who are cisplatin-ineligible or who decline chemotherapy (NCT02845323). Another phase 1b study plans to compare neoadjuvant nivolumab monotherapy and neoadjuvant combination of nivolumab with lirilumab, an anti-KIR2DL1/2L3 monoclonal antibody, in patients with cisplatin-ineligible MIBC (NCT03532451). Another phase 3 study is assessing outcomes between neoadjuvant nivolumab monotherapy, a combination of nivolumab and bempeg, and standard of care (radical cystectomy alone) in patients with cisplatin-ineligible MIBC (NCT04209114).
In addition to neoadjuvant immunotherapy combinations, nivolumab has also been investigated in combination with chemotherapy. BLASST-1 is a multicenter phase II trial, which assessed the efficacy of combining nivolumab with gemcitabine-cisplatin as neoadjuvant therapy in patients with MIBC. Initial analysis shows 65.8% (24/41) of patients had a pathologic response (defined as ≤pT1, N0) with 51.8% with pCr without significantly added toxicities or delays to cystectomy.23 In another phase 3 study, patients with MIBC are randomized to neoadjuvant gemcitabine cisplatin chemotherapy with nivolumab or with nivolumab and BMS-986205, an indoleamine 2,3-dioxygenase (IDO) inhibitor, as prior studies have shown those who receive cisplatin often have higher rates of PD-L1 and INO expression (NCT03661320).
Finally, nivolumab is also being investigated in some trials with bladder-sparing approaches. In a trial from the Hoosier Network (HCRN GU16-257), patients with MIBC were treated with four cycles of gemcitabine, cisplatin and nivolumab and 31 of 64 (48%) patients had a clinically complete response (defined as no abnormalities on imaging and urine cytology and bladder biopsy ≤ low-grade Ta) and were given the option of cystectomy or surveillance (30/31 elected for surveillance; six ultimately underwent delayed cystectomy due to recurrence).24 Another similar risk-enabled study with nivolumab and accelerated MVAC neoadjuvant chemotherapy is ongoing (NCT04506554). There are also multiple studies investigating the role of nivolumab either as induction therapy prior to chemoradiation (Indi-Blade, NCT05200988) with chemoradiation (NCT03993249) or as adjuvant therapy after chemoradiation (NEXT, NCT03171025).
Metastatic Urothelial Carcinoma
As many as 50% of patients will develop metastasis following cystectomy for clinically localized disease. Although considered a chemosensitive malignancy, the survival for patients with metastatic urothelial carcinoma remains poor with median survival of approximately 15 months.
Platinum-based therapy with cisplatin (or carboplatin if cisplatin-ineligible) and gemcitabine or dose-dense MVAC (methotrexate, vinblastine, doxorubicin, and cisplatin) is the standard of care first-line treatment for metastatic urothelial cancer.25 Similar to other ICIs, nivolumab first received accelerated FDA approval in 2017 for the treatment of metastatic urothelial cancer after progression on platinum-based regimen.
The FDA approval for platinum-refractory disease is based on the results from multicenter, single-arm, phase II Checkmate 275 study.1 In this study, 265 patients with metastatic or surgically unresectable urothelial carcinoma were treated with nivolumab 3mg/kg every 2 weeks until disease progression or clinical deterioration. The primary outcome was objective response rate (ORR), which was identified in 52 (19.6%) of the 265 patients. ORR was 28.4% in the 81 patients with PD-L1 expression of 5% or greater, 23.8% in patients with PD-L1 greater than 1%, and 16% of patients with PD-L1 of less than 1%. The prespecified threshold of historical control was 10% ORR, and so the study was considered positive for all PD-L1 subgroups.
Galsky et al published an extended analysis of the Checkmate 275 that further evaluated PD-L1 and tumor mutational burden (TMB) relationship to nivolumab response.26 In the analysis, higher TMB (>170 missense somatic mutations per tumor) was significantly associated with ORR, PFS, and OS. Using TMB combined with PD-L1 better predicted ORR, OFS, and OS than use of PD-L1 status alone.
A phase I/Ib trial Checkmate 032 explored the use of nivolumab single agent with and without ipilimumab in several tumor types, including patients with previously treated metastatic urothelial cancer.27 The cohorts included a nivolumab monotherapy (nivolumab 3 mg/kg every 2 weeks) or one of two nivolumab plus ipilimumab combinations (nivolumab 3mg/kg plus ipilimumab 1mg/kg for four doses with nivolumab maintenance and nivolumab 1mg/kg and ipilimumab 1mg/kg for four doses with nivolumab maintenance). ORRs were 25.6% with nivolumab monotherapy, and 26.9 and 38% in the combination therapies, respectively.
Given the high toxicity profile with nivolumab and ipilimumab combinations, one approach that has been investigated is a tailored immunotherapy intensification based on initial response to nivolumab monotherapy. In the TITAN-TCC study, patients with locally advanced or metastatic UC were treated with four doses of biweekly nivolumab 240mg induction. Patients with treatment response were continued on nivolumab monotherapy but for those patients with stable or progressive disease, therapy was intensified to nivolumab 3mg/kg and ipilimumab 1mg/kg every 3 weeks for two doses and if still without a response, nivolumab 1mg/kg and ipilimumab 3mg/kg every 3 weeks for two doses. Overall, this approach improved the ORR with treatment from 26% with nivolumab monotherapy to 36% with intensification.28 In addition, there are also studies evaluating combination therapy with nivolumab and other agents for those who have progressed on initial lines of ICI therapy. Recent results from a 30-patient phase I trial with a combination of nivolumab and tyrosine kinase inhibitor cabozantinib showed clinical activity (ORR 16%) and favorable tumor microenvironment profile in patients who had progressed on prior ICI therapy. There are ongoing trials to better understand the efficacy of this combination.
As previously stated, in addition to nivolumab, four other ICIs have been investigated for treatment of locally advanced or metastatic UC. Atezolizumab, a PD-L1 inhibitor, initially received FDA accelerated approval in 2016 based on the platinum-refractory cohort of the multi-cohort phase II trial, IMvigor 210.29 The trial showed an ORR of 15%, which was considered higher than historical control (~10%), with median duration of response of 59 months. A larger phase III trial, IMvigor211, randomly assigned patients with mUC who had progressed on platinum-based chemotherapy to either atezolizumab or chemotherapy (vinflunine, paclitaxel, or docetaxel).30 There was no significant improvement in OS or ORR, but median duration of response was longer with atezolizumab. The study did show higher response rates in patients with increased PD-L1 expression. In 2021, an extended analysis of the trial showed longer OS with atezolizumab (24-mo OS rate 23% vs 13%).31 Additionally, IMvigor130 was another phase III trial evaluating atezolizumab in a frontline setting for patients with locally advanced or metastatic UC.32 This trial compared patients with chemotherapy (gemcitabine plus either carboplatin or cisplatin) and atezolizumab to patients with atezolizumab monotherapy to patients with chemotherapy alone. The addition of atezolizumab to platinum-based chemotherapy prolonged PFS (median 8.2 vs 6.3 months, HR 0.82) compared to chemotherapy alone. However, no significant prolongation of OS was observed, so the current FDA-approved indications for atezolizumab are limited to patients with metastatic UC who are cisplatin-ineligible with high (>5%) PD-L1 expression or for those who are platinum-ineligible (irrespective of PD-L1 expression). This indication is based on a second cohort from the IMvigor 210 study, which included previously untreated, cisplatin-ineligible patients with locally advanced or metastatic UC and found a 23% ORR with median OS of 16.3 months.33
Pembrolizumab, a PD-1 inhibitor, was approved by the FDA in the second-line setting in patients with mUC based on data from KEYNOTE-045, which demonstrated a median OS of 10.3 months with pembrolizumab compared with 7.4 months for with chemotherapy.34 A subsequent accelerated approval was granted for pembrolizumab in the first-line setting for cisplatin-ineligible patients with mUC based on the phase II KEYNOTE-052 study, which noted an ORR of 24%, with higher objective responses found in those patients with a PD-L1 expression combined positive score (CPS) of ≥10% (n = 110) than in patients with CPS scores of <10%.35 This label was subsequently limited to platinum-ineligible patients only as the KEYNOTE-361 study showed inferior outcomes with pembrolizumab monotherapy compared to carboplatin-based chemotherapy.36 Pembrolizumab also has an FDA-approved indication for NMIBC with CIS based on the KEYNOTE-057 study reviewed above.
Avelumab is a PD-L1 inhibitor that was initially approved by the FDA in the platinum-refractory setting in patients with previously treated metastatic urothelial carcinoma based on the results from the Javelin Solid Tumor study.4 The FDA indication was then expanded to the switch-maintenance setting for patients with metastatic urothelial carcinoma through the JAVELIN Bladder 100 study.37 This study showed for patients without progression after 4–6 cycles of first-line platinum-based chemotherapy who then receive maintenance avelumab, they had significantly improved OS compared with patients who only received supportive care.
Durvalumab is another ICI viable for use in platinum-refractory mUC as the STRONG trial found that the overall safety and efficacy are similar to other ICIs.38 This had a prior FDA accelerated approval that was subsequently withdrawn after the confirmatory DANUBE trial did not show improved OS for durvalumab alone or with anti-CTLA-4 tremelimumab when compared with platinum chemotherapy.4
In addition to ICIs, there has been an increased effort to move cancer directed therapy away from traditional cytotoxic chemotherapies and towards targeted agents.39 In urothelial carcinoma, there are several over-expressed proteins/targets that have been identified for drug development. Currently, there are three molecular targets with cytotoxic drugs approved by the FDA for locally advanced or metastatic bladder cancer: Nectin-4, Fibroblast Growth Factor Receptor (FGFR2, FGFR3), and Trop-2.40–42
Nectin-4 is a cell-adhesion molecule that is ubiquitously expressed in urothelial carcinoma and contributes to cell proliferation.43 Enfortumab vedotin (EV) is an antibody–drug conjugate (ADC) designed against Nectin-4 that received FDA approval in patients with metastatic urothelial cancer who have previously been on PD-1/PDL-1 inhibition and platinum-based chemotherapy or patients who are platinum ineligible and received at least one line of therapy. EV initially received FDA accelerated approval in 2019 based on the first cohort of a single-arm, multi-cohort phase II EV-201 study that showed an overall response rate of 44% in heavily pretreated patients.44 Later, it received regular approval in 2021 based on the confirmatory data from the randomized phase III EV-301 study. At this same time, it also received label expansion to include cisplatin-ineligible patients treated with one prior line of therapy based on cohort 2 (cisplatin-ineligible) from EV-201.45 In the EV-301 study, patients were randomized to EV vs investigators' choice of single-agent chemotherapy (taxane or vinflunine), and patients in EV arm had significantly increased OS (median 12.9 vs 9.0 mo; hazard ratio [HR] 0.70), PFS (median 5.6 vs 3.7 mo; HR 0.62) and ORR (41% vs 18%). EV is also being studied in combination with pembrolizumab, an ICI, in the first-line setting, with early trial results from a cisplatin-ineligible population showing ORR 71%.46 A phase III study comparing the combination to traditional chemotherapy and other studies investigating EV’s role in earlier treatment settings (perioperative and NMIBC) are ongoing (NCT04223856).
FGFRs are receptor tyrosine kinases that act along the PI3K/MAPK pathway stimulating cell growth, differentiation, survival, and angiogenesis.47 FGFR aberrations are found in 7% of all cancers, most commonly gene amplification and mutations.48 They are found in almost all types of cancer but with high prevalence in urothelial cancers (32% FGFR aberrant). Erdafitinib is an FGFR 1–4 inhibitor that received FDA accelerated approval in 2019 for patients with susceptible FGFR2 or FGFR3 mutated locally advanced or metastatic UC that progressed on platinum chemotherapy. The approval was based on the phase II BLC2001 study that showed an ORR of 40%.49 Studies are ongoing to confirm efficacy of erdafitinib for metastatic urothelial carcinoma and investigating this agent in combination with ICIs or EV in earlier lines of therapy, while several other FGFR receptors are also in phase I–III trials for use in UC. Upper tract urothelial carcinoma (UTUC) is a difficult to treat form of UC that tends to be associated with high tumor mutational burden (TMB) and FGFR3 mutations.50,51 Immune checkpoint inhibitors are a potential second-line option for treating patients with this rare malignancy.52 The higher prevalence of FGFR3 mutation also invites further exploration of treatment with targeted therapies such as erdafitinib.
Trop-2 is a membrane glycoprotein involved in intracellular signaling that is overexpressed in several cancer types.53 Because of its overexpression in urothelial carcinoma as well as its extracellular domain, it has become a target of interest for drug development. The data from TROPHY-U-01 lead to the 2021 FDA accelerated approval of Sacituzumab govitecan, an ADC comprised humanized anti-trop-2 monoclonal antibody conjugated with the active metabolite of irinotecan (SN-38).54 In the trial, patients with locally advanced or unresectable or metastatic UC who had progressed after prior platinum and immune checkpoint inhibitors (ICI) had an ORR of 27% and median OS of 5.4 months in a heavily pretreated cohort. Confirmatory studies are also underway for these agents as monotherapy or in combinations and in earlier treatment settings.
Biomarkers
An emerging area of interest is the utility of predictive biomarkers for identification of targetable mutations, patient stratification, and selection of patients who may benefit from immunotherapy and targeted therapies in UC. Relevant biomarkers for immune checkpoint inhibitors include immunohistochemical staining of PD-L1 and tumor mutational burden. In addition, ctDNA is also an interesting biomarker that could help improve evaluation of residual disease after surgery as well as monitoring for progression in the metastatic disease setting.
One of the earliest biomarkers investigated related to immune checkpoint inhibitors was immunohistochemical staining for PD-L1. Multiple different assays have been investigated with different ICIs and used variably as a stratification factor or as part of a nested primary endpoint. However, the assays have been limited by lack of reproducibility and variable definitions (eg, which cells measured, what type of scoring) and cutoffs, which ultimately limited further development.
Tumor mutational burden has been a more consistent biomarker that has been used to identify patients that may benefit from ICIs. TMB >10 has been used for a tumor-agnostic approval of pembrolizumab based on the multi-cohort Keynote-158 trial, which suggested the benefit of using this threshold in multiple tumor types.55 In mUC, higher TMB was associated with higher ORR with nivolumab in an exploratory analysis of Checkmate-275.26 Further, in a recent exploratory real-world study, patients who were cisplatin-ineligible with TMB >10 had longer PFS and OS with first-line ICIs vs first-line carboplatin-based chemotherapy.56
Liquid biopsy using circulating tumor DNA (ctDNA) in plasma or urine may provide a minimally invasive method of data acquisition. Several studies have found that metastatic relapse and treatment failure were associated with significantly higher ctDNA levels compared to those that did not. As previously mentioned, in an exploratory study of IMvigor010, the presence of ctDNA after radical cystectomy seemed to identify patients with MIBC who may benefit from adjuvant atezolizumab, thus suggesting that this could be a useful predictive biomarker for adjuvant ICI selection. In addition, high levels of ctDNA have been identified as an independent prognostic indicator for overall survival in patients with metastatic UC. Further work is needed to best identify the disease settings to implement this as a useful biomarker to improve patient outcomes.
In addition to these immunotherapy-specific biomarkers, additional molecular biomarkers are in various stages of development as pertaining to other novel therapies. Erdafitinib was approved in conjunction with a companion diagnostic to identify FGFR 2/3 alterations that predict treatment response. In addition, there is ongoing work to identify if immunohistochemical staining for nectin-4 or trop-2 would help predict response to EV or SG, respectively. Circulating tumor cells, HER-2 IHC, and other molecular alterations (eg, ERCC2, TP53, etc.) are also in various stages of ongoing investigation.
Future Directions for Nivolumab
Overall, nivolumab and other ICIs have expanded therapeutic options for UC beyond conventional cytotoxic chemotherapy and improved outcomes for patients. However, response rates remain modest and further work is needed to develop biomarkers and new agents.57 As we look towards the future, there still remain multiple questions to be answered.
There is growing interest towards trialing combination regimens with ICIs and other targeted agents in an attempt to achieve greater therapeutic responses for patients with advanced disease. Some of the early combinations have been mentioned here including nivolumab with ipilimumab and pembrolizumab with EV. One potential interesting combination not under investigation is the combination of nivolumab, ipilimumab and EV. This combination of agents has shown promising activity in patients with UC and based on the preliminary EV and pembrolizumab data, may have synergy, though toxicity may be a concern.
There is good clinical evidence for the activity of nivolumab in patients with mUC, but the FDA approval in this setting is not biomarker specific. Based on trials in nivolumab and other ICIs, the effect of ICIs on bladder cancer seems to be related to TMB and PD-L1 status, though neither biomarker has been reliably shown to be predictive. Clinical factors like metastatic disease sites, performance status or risk scores can also help inform clinical decisions.58–60 Clinicians should consider this data when considering nivolumab or other ICIs against other lines of treatment. From a biomarker standpoint, there remains more work to be done.
One question still being answered is the duration of therapy for patients receiving nivolumab for treatment of UC. In previous trials, there has been no clear end date for patients who are responding to ICIs. The alliance A031901 trial (IMAGINE; NCT04637594) is a study in the recruitment phase designed to identify the current duration of therapy for patients on ICIs for mUC. The study is a non-inferiority study that randomizes patients with stable disease on ICIs for 12–15 to ICI discontinuation vs continued therapy with the primary endpoint of OS.
ICIs and other targeted therapies have improved outcomes and expanded treatment options for patients with UC, but some key principles in ongoing drug development also warrant consideration. First, as clinical trials include patients from across the globe and move toward earlier treatment settings, it is important to ensure that patients receive appropriate post-protocol therapy (eg, ICIs for platinum-refractory disease) that is in line with US standards (if seeking FDA drug approval). It may be possible that sequential therapy has similar benefit to combinations, but this can only be accurately assessed if appropriate post-protocol therapy is delivered. Second, although there remain multiple settings where ICIs warrant further investigation, some consideration is needed regarding trial redundancy as highlighted by Beaver et al61 The influx of redundant agents may limit the amount of intellectual and financial resources available and have not included randomized trials with direct comparisons against existing FDA approved ICIs, nor has the market redundancy led to any price competition to reduce financial toxicity.
In conclusion, nivolumab and other ICIs have truly revolutionized the treatment landscape for UC across a wide array of treatment settings. These agents and other targeted therapies are expanding treatment options for patients, improving or preserving patient’s quality of life and extending overall survival. Further work is needed and ongoing in biomarker development, investigations in earlier treatment settings and as combination therapies to continue to improve outcomes for all patients with urothelial carcinoma.
Disclosure
Dr Ali Raza Khaki reports Research collaborations with Tempus Labs and Natera. The authors have no other conflict of interests to declare.
References
1. Sharma P, Retz M, Siefker-Radtke A, et al. Nivolumab in metastatic urothelial carcinoma after platinum therapy (checkmate 275): a multicentre, single-arm, phase 2 trial. Lancet Oncol. 2017;18(3):312–322. doi:10.1016/S1470-2045(17)30065-7.
2. Bajorin DF, Witjes JA, Gschwend JE, et al. Adjuvant nivolumab versus placebo in muscle-invasive urothelial carcinoma. N Engl J Med. 2021;384(22):2102–2114. doi:10.1056/NEJMoa2034442.
3. Simsek M, Tekin SB, Bilici M. Immunological agents used in cancer treatment. Eurasian J Med. 2019;51(1):90–94. doi:10.5152/eurasianjmed.2018.18194.
4. Powles T, van der Heijden MS, Castellano D, et al. Durvalumab alone and durvalumab plus tremelimumab versus chemotherapy in previously untreated patients with unresectable, locally advanced or metastatic urothelial carcinoma (Danube): a randomised, open-label, multicentre, phase 3 trial. Lancet Oncol. 2020;21(12):1574–1588. doi:10.1016/S1470-2045(20)30541-6.
5. Wei SC, Duffy CR, Allison JP. Fundamental mechanisms of immune checkpoint blockade therapy. Cancer Discov. 2018;8(9):1069–1086. doi:10.1158/2159-8290.CD-18-0367.
6. Sari Motlagh R, Pradere B, Mori K, Miura N, Abufaraj M, Shariat SF. Bladder-preserving strategies for Bacillus Calmette-Guérin unresponsive non-muscle invasive bladder cancer; where are we and what will be expected? Curr Opin Urol. 2020;30(4):584–593. doi:10.1097/MOU.0000000000000792.
7. Balar AV, Kamat AM, Kulkarni GS, et al. Pembrolizumab monotherapy for the treatment of high-risk non-muscle-invasive bladder cancer unresponsive to BCG (KEYNOTE-057): an open-label, single-arm, multicentre, phase 2 study. Lancet Oncol. 2021;22(7):919–930. doi:10.1016/S1470-2045(21)00147-9.
8. Califano G, Ouzaid I, Verze P, Stivalet N, Hermieu JF, Xylinas E. New immunotherapy treatments in non-muscle invasive bladder cancer. Nuevos tratamientos de immunoterapia en cáncer de vejiga no musculoinvasivo. Arch Esp Urol. 2020;73(10):945–953.
9. Witjes JA, Gschwend J, Palou J, et al. A phase 2, randomized study of nivolumab or nivolumab plus BMS-986205 with or without intravesical bacillus Calmette-Guerin in patients with bacillus Calmette-Guerin-unresponsive, high-risk, nonmuscle invasive bladder cancer: checkMate 9UT. Eur Urol Suppl. 2019;18:e1833–e1834. doi:10.1016/S1569-9056(19)31328-4
10. Grossman HB, Natale RB, Tangen CM, et al. Neoadjuvant chemotherapy plus cystectomy compared with cystectomy alone for locally advanced bladder cancer. N Engl J Med. 2003;349(9):859–866. doi:10.1056/NEJMoa022148
11. Vale CL; Advanced Bladder Cancer (ABC) Meta-analysis Collaboration. Neoadjuvant chemotherapy in invasive bladder cancer: update of a systematic review and meta-analysis of individual patient data advanced bladder cancer (ABC) meta-analysis collaboration. Eur Urol. 2005;48(2):202–206. doi:10.1016/j.eururo.2005.04.006
12. James ND, Hussain SA, Hall E, et al. Radiotherapy with or without chemotherapy in muscle-invasive bladder cancer. N Engl J Med. 2012;366(16):1477–1488. doi:10.1056/NEJMoa1106106.
13. van Hattum JW, de Ruiter BM, Oddens JR, Hulshof MCCM, de Reijke TM, Bins AD. Bladder-sparing chemoradiotherapy combined with immune checkpoint inhibition for locally advanced urothelial bladder cancer-a review. Cancers. 2021;14(1):38. doi:10.3390/cancers14010038.
14. Bellmunt J, Hussain M, Gschwend JE, et al. Adjuvant atezolizumab versus observation in muscle-invasive urothelial carcinoma (IMvigor010): a multicentre, open-label, randomised, phase 3 trial. Lancet Oncol. 2021;22(4):525–537. doi:10.1016/S1470-2045(21)00004-8.
15. Powles T, Assaf ZJ, Davarpanah N, et al. ctDNA guiding adjuvant immunotherapy in urothelial carcinoma. Nature. 2021;595(7867):432–437. doi:10.1038/s41586-021-03642-9.
16. van Dijk N, Gil-Jimenez A, Silina K, et al. Preoperative ipilimumab plus nivolumab in locoregionally advanced urothelial cancer: the NABUCCO trial. Nat Med. 2020;26(12):1839–1844. doi:10.1038/s41591-020-1085-z
17. Pfister C, Gravis G, Fléchon A, et al. Dose-Dense Methotrexate, Vinblastine, Doxorubicin, and Cisplatin or Gemcitabine and Cisplatin as perioperative chemotherapy for patients with nonmetastatic muscle-invasive bladder cancer: results of the GETUG-AFU V05 VESPER. J Clin Oncol. 2022:JCO2102051. doi:10.1200/JCO.21.02051
18. Choueiri TK, Jacobus S, Bellmunt J, et al. Neoadjuvant dose-dense methotrexate, vinblastine, doxorubicin, and cisplatin with pegfilgrastim support in muscle-invasive urothelial cancer: pathologic, radiologic, and biomarker correlates. J Clin Oncol. 2014;32(18):1889–1894. doi:10.1200/JCO.2013.52.4785
19. Plimack ER, Hoffman-Censits JH, Viterbo R, et al. Accelerated methotrexate, vinblastine, doxorubicin, and cisplatin is safe, effective, and efficient neoadjuvant treatment for muscle-invasive bladder cancer: results of a multicenter phase II study with molecular correlates of response and toxicity. J Clin Oncol. 2014;32(18):1895–1901. doi:10.1200/JCO.2013.53.2465
20. Flaig TW, Tangen CM, Daneshmand S, et al. A randomized phase II study of Coexpression Extrapolation (COXEN) with neoadjuvant chemotherapy for bladder cancer (SWOG S1314; NCT02177695). Clin Cancer Res. 2021;27(9):2435–2441. doi:10.1158/1078-0432.CCR-20-2409
21. Powles T, Kockx M, Rodriguez-Vida A, et al. Clinical efficacy and biomarker analysis of neoadjuvant atezolizumab in operable urothelial carcinoma in the ABACUS trial. Nat Med. 2019;25(11):1706–1714. doi:10.1038/s41591-019-0628-7
22. Necchi A, Anichini A, Raggi D, et al. Pembrolizumab as neoadjuvant therapy before radical cystectomy in patients with muscle-invasive urothelial bladder carcinoma (PURE-01): an open-label, single-arm, phase ii study. J Clin Oncol. 2018;36(34):3353–3360. doi:10.1200/JCO.18.01148
23. Gupta S, Sonpavde G, Weight CJ, et al. Results from BLASST-1 (bladder cancer signal seeking trial) of nivolumab, gemcitabine, and cisplatin in muscle invasive bladder cancer (MIBC) undergoing cystectomy. J Clin Oncol. 2020;38:439. doi:10.1200/JCO.2020.38.6_suppl.439.
24. Galsky MD, Siamak D, Chan KG, et al. Phase 2 trial of gemcitabine, cisplatin, plus nivolumab with selective bladder sparing in patients with muscle- invasive bladder cancer (MIBC): HCRN GU 16–257. J Clin Oncol. 2021;39:4503. doi:10.1200/JCO.2021.39.15_suppl.4503
25. Lenis AT, Lec PM, Chamie K, Mshs MD. Bladder cancer: a review. JAMA. 2020;324(19):1980–1991. doi:10.1001/jama.2020.17598
26. Galsky MD, Saci A, Szabo PM, et al. Nivolumab in patients with advanced platinum-resistant urothelial carcinoma: efficacy, safety, and biomarker analyses with extended follow-up from checkMate 275. Clin Cancer Res. 2020;26(19):5120–5128. doi:10.1158/1078-0432.CCR-19-4162
27. Sharma P, Siefker-Radtke A, de Braud F, et al. Nivolumab Alone and with ipilimumab in previously treated metastatic urothelial carcinoma: checkmate 032 nivolumab 1 mg/kg plus ipilimumab 3 mg/kg expansion cohort results. J Clin Oncol. 2019;37(19):1608–1616. doi:10.1200/JCO.19.00538
28. Grimm MO, Schmitz-Dräger BJ, Zimmermann U, et al. Tailored immunotherapy approach with nivolumab in advanced transitional cell carcinoma. J Clin Oncol. 2022:JCO2102631. doi:10.1200/JCO.21.02631
29. Rosenberg JE, Hoffman-Censits J, Powles T, et al. Atezolizumab in patients with locally advanced and metastatic urothelial carcinoma who have progressed following treatment with platinum-based chemotherapy: a single-arm, multicentre, phase 2 trial. Lancet. 2016;387(10031):1909–1920. doi:10.1016/S0140-6736(16)00561-4
30. Powles T, Durán I, van der Heijden MS, et al. Atezolizumab versus chemotherapy in patients with platinum-treated locally advanced or metastatic urothelial carcinoma (IMvigor211): a multicentre, open-label, phase 3 randomised controlled trial [published correction appears in Lancet. Lancet. 2018;391(10122):748–757. doi:10.1016/S0140-6736(17)33297-X
31. van der Heijden MS, Loriot Y, Durán I, et al. Atezolizumab versus chemotherapy in patients with platinum-treated locally advanced or metastatic urothelial carcinoma: a long-term overall survival and safety update from the phase 3 IMvigor211 clinical trial. Eur Urol. 2021;80(1):7–11. doi:10.1016/j.eururo.2021.03.024
32. Galsky MD, Arija JÁA, Bamias A, et al. Atezolizumab with or without chemotherapy in metastatic urothelial cancer (IMvigor130): a multicentre, randomised, placebo-controlled phase 3 trial. Lancet. 2020;395(10236):1547–1557. doi:10.1016/S0140-6736(20)30230-0
33. Balar AV, Galsky MD, Rosenberg JE, et al. Atezolizumab as first-line treatment in cisplatin-ineligible patients with locally advanced and metastatic urothelial carcinoma: a single-arm, multicentre, phase 2 trial. Lancet. 2017;389(10064):67–76. doi:10.1016/S0140-6736(16)32455-2
34. Bellmunt J, de Wit R, Vaughn DJ, et al. Pembrolizumab as second-line therapy for advanced urothelial carcinoma. N Engl J Med. 2017;376(11):1015–1026. doi:10.1056/NEJMoa1613683
35. Vuky J, Balar AV, Castellano D, et al. Long-term outcomes in KEYNOTE-052: phase ii study investigating first-line pembrolizumab in cisplatin-ineligible patients with locally advanced or metastatic urothelial cancer. J Clin Oncol. 2020;38(23):2658–2666. doi:10.1200/JCO.19.01213
36. Powles T, Csőszi T, Özgüroğlu M, et al. Pembrolizumab alone or combined with chemotherapy versus chemotherapy as first-line therapy for advanced urothelial carcinoma (KEYNOTE-361): a randomised, open-label, phase 3 trial. Lancet Oncol. 2021;22(7):931–945. doi:10.1016/S1470-2045(21)00152-2
37. Apolo AB, Ellerton JA, Infante JR, et al. Avelumab as second-line therapy for metastatic, platinum-treated urothelial carcinoma in the phase Ib JAVELIN Solid Tumor study: 2-year updated efficacy and safety analysis. J Immunother Cancer. 2020;8(2):e001246. doi:10.1136/jitc-2020-001246
38. Sonpavde GP, Sternberg CN, Loriot Y, et al. Primary results of STRONG: an open-label, multicenter, phase 3b study of fixed-dose durvalumab monotherapy in previously treated patients with urinary tract carcinoma. Eur J Cancer. 2022;163:55–65. doi:10.1016/j.ejca.2021.12.012
39. Baudino TA. Targeted cancer therapy: the next generation of cancer treatment. Curr Drug Discov Technol. 2015;12(1):3–20. doi:10.2174/1570163812666150602144310
40. Research, C. for D. E. FDA grants regular approval to enfortumab vedotin-ejfv for locally advanced or metastatic urothelial cancer. FDA; 2021.
41. Research, C. for D. E. FDA grants accelerated approval to erdafitinib for metastatic urothelial carcinoma. FDA; 2019.
42. Research, C. for D. E. FDA grants accelerated approval to sacituzumab govitecan for advanced urothelial cancer. FDA; 2021.
43. Challita-Eid PM, Satpayev D, Yang P, et al. Enfortumab vedotin antibody-drug conjugate targeting nectin-4 is a highly potent therapeutic agent in multiple preclinical cancer models. Cancer Res. 2016;76(10):3003–3013. doi:10.1158/0008-5472.CAN-15-1313
44. Rosenberg JE, O’Donnell PH, Balar AV, et al. Pivotal trial of enfortumab vedotin in urothelial carcinoma after platinum and anti-programmed death 1/programmed death ligand 1 therapy. J Clin Oncol. 2019;37(29):2592–2600. doi:10.1200/JCO.19.01140
45. Powles T, Rosenberg JE, Sonpavde GP, et al. Enfortumab vedotin in previously treated advanced urothelial carcinoma. N Engl J Med. 2021;384(12):1125–1135. doi:10.1056/NEJMoa2035807
46. Rosenberg JE, Flaig TW, Friedlander TW, et al. Study EV-103: durability results of enfortumab vedotin plus pembrolizumab for locally advanced or metastatic urothelial carcinoma. J Clin Oncol. 2020;38:5044. doi:10.1200/JCO.2020.38.6_suppl.441.
47. Casadei C, Dizman N, Schepisi G, et al. Targeted therapies for advanced bladder cancer: new strategies with FGFR inhibitors. Ther Adv Med Oncol. 2019;11:1758835919890285. doi:10.1177/1758835919890285
48. Helsten T, Elkin S, Arthur E, Tomson BN, Carter J, Kurzrock R. The FGFR landscape in cancer: analysis of 4853 tumors by next-generation sequencing. Clin Cancer Res. 2016;22(1):259–267. doi:10.1158/1078-0432.CCR-14-3212
49. Loriot Y, Necchi A, Park SH, et al. Erdafitinib in locally advanced or metastatic urothelial carcinoma. N Engl J Med. 2019;381(4):338–348. doi:10.1056/NEJMoa1817323
50. Califano G, Ouzaid I, Laine-Caroff P, et al. Current advances in immune checkpoint inhibition and clinical genomics in upper tract urothelial carcinoma: state of the art. Curr Oncol. 2022;29(2):687–697. doi:10.3390/curroncol29020060
51. Califano G, Ouzaid I, Verze P, Hermieu JF, Mirone V, Xylinas E. Immune checkpoint inhibition in upper tract urothelial carcinoma. World J Urol. 2021;39(5):1357–1367. doi:10.1007/s00345-020-03502-7
52. Esagian SM, Khaki AR, Diamantopoulos LN, et al. Immune checkpoint inhibitors in advanced upper and lower tract urothelial carcinoma: a comparison of outcomes. BJU Int. 2021;128(2):196–205. doi:10.1111/bju.15324
53. Zaman S, Jadid H, Denson AC, Gray JE. Targeting Trop-2 in solid tumors: future prospects. Onco Targets Ther. 2019;12:1781–1790. doi:10.2147/OTT.S162447
54. Tagawa ST, Balar AV, Petrylak DP, et al. TROPHY-U-01: a phase ii open-label study of sacituzumab govitecan in patients with metastatic urothelial carcinoma progressing after platinum-based chemotherapy and checkpoint inhibitors. J Clin Oncol. 2021;39(22):2474–2485. doi:10.1200/JCO.20.03489
55. Marabelle A, Fakih M, Lopez J, et al. Association of tumour mutational burden with outcomes in patients with advanced solid tumours treated with pembrolizumab: prospective biomarker analysis of the multicohort, open-label, phase 2 KEYNOTE-158 study. Lancet Oncol. 2020;21(10):1353–1365. PMID: 32919526. doi:10.1016/S1470-2045(20)30445-9
56. Graf RP, Fisher V, Huang RSP, et al. Tumor mutational burden as a predictor of first-line immune checkpoint inhibitor versus carboplatin benefit in cisplatin-unfit patients with urothelial carcinoma. JCO Precis Oncol. 2022;6:e2200121. doi:10.1200/PO.22.00121.
57. Dietrich B, Siefker-Radtke AO, Srinivas S, Yu EY. Systemic therapy for advanced urothelial carcinoma: current standards and treatment considerations. Am Soc Clin Oncol Educ Book. 2018;38:342–353. doi:10.1200/EDBK_201193
58. Makrakis D, Diamantopoulos LN, Koshkin VS, et al. Association between sites of metastases (mets) and outcomes with immune checkpoint inhibitor (ICI) therapy for advanced urothelial carcinoma (aUC). J Clin Oncol. 2021;39. doi:10.1200/JCO.2021.39.6_suppl.445.
59. Khaki AR, Li A, Diamantopoulos LN, et al. Impact of performance status on treatment outcomes: a real-world study of advanced urothelial cancer treated with immune checkpoint inhibitors. Cancer. 2020;126(6):1208–1216. doi:10.1002/cncr.32645
60. Khaki AR, Li A, Diamantopoulos LN, et al. A new prognostic model in patients with advanced urothelial carcinoma treated with first-line immune checkpoint inhibitors. Eur Urol Oncol. 2021;4(3):464–472. doi:10.1016/j.euo.2020.12.006
61. Beaver JA, Pazdur R. The wild west of checkpoint inhibitor development. N Engl J Med. 2021. doi:10.1056/NEJMp2116863.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.