Back to Journals » ImmunoTargets and Therapy » Volume 13
Clinical Significance and Molecular Annotation for PD-L1 Negative Advanced Non-Small Cell Lung Cancer with Sensitivity to Responsive to Dual PD-1/CTLA-4 Blockade
Authors Wang L, Liu L, Zhao J, Yu X, Su C
Received 29 April 2024
Accepted for publication 4 September 2024
Published 6 September 2024 Volume 2024:13 Pages 435—445
DOI https://doi.org/10.2147/ITT.S476040
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Shurin
Li Wang, Li Liu, Jing Zhao, Xin Yu, Chunxia Su
Department of Medical Oncology, Shanghai Pulmonary Hospital & Thoracic Cancer Institute, Tongji University School of Medicine, Shanghai, 200433, People’s Republic of China
Correspondence: Chunxia Su, Department of Medical Oncology, Shanghai Pulmonary Hospital & Thoracic Cancer Institute, Tongji University School of Medicine, Shanghai, 200433, People’s Republic of China, Email [email protected]
Background: Immunotherapy has become the standard treatment for driving gene-negative advanced non-small cell lung cancer (NSCLC). However, compared to PD-L1-positive patients, the efficacy of Anti-PD-(L)1 monotherapy is suboptimal in PD-L1-negative advanced NSCLC. In this study, we aim to analyze the optimal immunotherapy approach for PD-L1-negative NSCLC patients and develop a new nomogram to enhance the clinical predictability of immunotherapy for NSCLC patients.
Methods: In this study, we retrieved clinical information and genomic data from cBioPortal for NSCLC patients undergoing immunotherapy. Cox regression analyses were utilized to screen the clinical information and genomic data that related to survival. The prognostic-relate genes function was studied by comprehensive bioinformatics analyses. The Kaplan-Meier plot method was employed for survival analysis.
Results: A total of 199 PD-L1-negative NSCLC patients were included in this study. Among them, 165 patients received Anti-PD-(L)1 monotherapy, while 34 patients received Anti-PD-(L)1+Anti-CTLA-4 combination therapy. The Anti-PD-(L)1+Anti-CTLA-4 combination therapy demonstrated significantly higher PFS compared to the Anti-PD-(L)1 monotherapy. The mutation status of KRAS, ANO1, COL14A1, LTBP1. ERBB4 and PCSK5 were found to correlate with PFS. Utilizing the clinicopathological parameters and genomic data of the patients, a novel nomogram was developed to predict the prognosis of Anti-PD-(L)1+Anti-CTLA-4 combination therapy.
Conclusion: Our study revealed that KRAS, ANO1, COL14A1, LTBP1. ERBB4 and PCSK5 mutation could serve as predictive biomarkers for patients with Anti-PD-(L)1+Anti-CTLA-4 combination therapy. Our systematic nomogram demonstrates significant potential in predicting the prognosis for NSCLC patients with responsive to dual PD-1/CTLA-4 blockade.
Keywords: NSCLC, immunotherapy, immune checkpoint inhibitors, nomogram, cBioPortal
Introduction
The incidence and mortality rates of lung cancer have been steadily increasing, making it the deadliest malignancy globally.1 NSCLC comprises roughly 85% of all lung cancer cases, with more than half diagnosed at an advanced stage.2 In the past decade, immunotherapy has emerged as a significant breakthrough in the field of cancer treatment. Immune checkpoint inhibitors (ICIs) have demonstrated convincing efficacy and tolerable safety profiles in both monotherapy and combination therapy approaches in NSCLC.3–6 Based on tumor tissue PD-L1 expression, NSCLC patients can be categorized into PD-L1-negative and PD-L1-positive populations. KEYNOTE-189 and KEYNOTE-407 clinical trials indicate that the first-line treatment of immunotherapy of 1-year PFS rate of around 26% in the PD-L1-negative population, is significantly lower than the 38% in the PD-L1-positive population.7,8 Therefore, there is an urgent need for new treatment modalities and drugs to improve efficacy and enhance survival in PD-L1-negative advanced NSCLC patients.
In immunotherapy, the most used combination strategies with PD-(L)1 antibodies include chemotherapy, CTLA-4 inhibitors, and VEGF/R targeted drugs. Meanwhile, the dual immunotherapy combination of anti-PD-1 antibodies and anti-CTLA-4 antibodies has shown excellent efficacy in multiple cancer types.9–11 CheckMate 9LA study demonstrates that the dual immunotherapy combined with chemotherapy significantly prolonged PFS and OS compared to chemotherapy, regardless of PD-L1 expression and tumor tissue type.12 Moreover, CheckMate 227 study further demonstrated that compared to chemotherapy, the combination of Nivolumab and ipilimumab significantly improved OS in PD-L1 negative advanced NSCLC patients (median 17.2 months vs 12.2 months, HR=0.62).13 However, these Phase III clinical trials primarily investigated OS endpoints in the PD-L1-positive population, hence requiring more evidence to support their efficacy. Meanwhile, a meta-analysis including 16 studies involving 8278 patients with first-line treatment of NSCLC systematically compared the efficacy and safety of 10 immunotherapy combination treatment strategies. The median OS of Nivolumab combined with ipilimumab was superior to Pembrolizumab combined with chemotherapy in PD-L1-negative patients.14 Hence, there is still a lack of direct clinical evidence to conclusively demonstrate the superiority of Anti-PD-(L)1+Anti-CTLA-4 combination therapy over Anti-PD-(L)1 monotherapy.
At present, the expression of PD-L1 is extensively employed in clinical settings to select patients suitable for immunotherapy.15 However, PD-L1-negative NSCLC patients face a more pronounced challenge due to the absence of biomarkers. Nomograms have garnered increasing attention in cancer research, offering a more interpretable and visually intuitive representation of predictive models. The growing interest in nomograms arises from their capacity to seamlessly integrate a range of predictive markers, thereby enhancing their importance as valuable graphical tools in the field of cancer research.16–19 The cBioPortal was used to download data from NSCLC patients treated with ICIs in this study.20 Novel nomogram was created based on clinicopathological and genome data to predict the prognosis for PD-L1 negative advanced NSCLC with ICIs treatment.
Materials and Methods
Data Download and Processing
The cBio Cancer Genomics Portal (http://cbioportal.org) is an open-access resource for interactive exploration of multidimensional cancer genomics data sets.20 Four cohorts of PD-L1-negative advanced NSCLC were obtained from The cBio Cancer Genomics Portal. PD-L1 negative was defined as the PD-L1 expression less than 1%. The first cohort (MSK Mind, Nature Cancer 2022) consisted of 126 PD-L1-negative advanced NSCLC patients at Memorial Sloan Kettering (MSK) Cancer Center who received immunotherapy therapy.21 The second cohort (MSK, Cancer Cell 2018) comprised 25 PD-L1-negative NSCLC patients treated with anti-PD-1 and anti–CTLA–4.22 This cohort also performed whole-exome sequencing (WES) on tumor tissue and paired blood. The third cohort (MSK, J Clin Oncol 2018) consisted of 42 PD-L1-negative NSCLC patients treated with with anti–PD-(L)1 monotherapy or in combination with anti–CTLA-4.23 These tumors from these patients also were analyzed by WES. The four cohort (MSK, Science 2015) comprised 6 PD-L1-negative NSCLC patients treated with anti-PD-1 therapy.24 The clinical information of ICI cohorts includes age, gender, treatment type, tumor mutational burden (TMB), and so on. Durable clinical benefit (DCB) was characterized by PFS for more than 6 months, and Non-durable benefit (NDB) was defined as PFS that lasted 6 months or less.25 The lung cancer patients underwent PD-L1 testing and targeted next-generation sequencing (using MSK-IMPACT).
Bioinformatic Analysis
To identify biomarkers predictive of immunotherapy efficacy, we utilized the R package “GenVisR“ to plot the top 25 gene alterations in the DCB and NDB groups. The R package ”GenVisR” is an R language software package designed for generating bioinformatics visualizations.26 It offers functions for creating high-quality, customizable graphics, suitable for visualizing genomic, mutational, structural variation, and Copy Number Variation (CNV) data.
Gene ontology (GO) and Kyoto Encyclopedia of Genes and Genomes (KEGG) analyses were commonly used methods in bioinformatics for functional enrichment analysis, aiming to interpret the biological significance and pathways of gene sets. In this study, GO and KEGG analyses were employed to annotate the functional significance of the top 20 mutation genes in the DCB and NDB groups by the R package “clusterProfiler”.27
Development of Nomogram
Cox regression analyses were utilized to screen mutation genes that related to survival. Utilizing the patient’s clinical data and genomic data, nomograms can forecast the probability of PFS. The R package “rms“ offers a comprehensive set of functions tailored to streamline and enhance various facets of regression modeling.28,29 It establishes scoring criteria by assessing the magnitude of regression coefficients associated with all variables in the model. For each patient, the cumulative score is calculated by summing the individual scores of all variables. Subsequently, a transformation function, associated with the probability of PFS, is applied to estimate the survival probability for each patient. The concordance index (C-index) and calibration curve served as the primary metrics for evaluating the predictive accuracy of the nomogram. We also constructed the Dynamic nomogram using The R package ”DynNom”. An easy-to-use web-based nomogram model was developed at https://shinyapps.io/, and the latest version will also be accessible online.
Statistical Analyses
Statistical analyses were conducted using GraphPad Prism 9.0 and R 4.2.2. The Cox proportional hazard model was applied for multivariate analysis. The explanatory factors utilized in this analysis include smoking, treatment, treatment line, TMB, and histology. The Fisher’s exact test or Pearson chi-square was used to compare proportions. Survival analyses were performed employing the Kaplan-Meier plot method and compared using the Log rank test, where a P <0.05 was deemed statistically significant.
Result
The Combination Therapy of Anti-PD-(L)1+anti-CTLA-4 Demonstrated Superior Survival Benefits Compared to Anti-PD-(L)1 Monotherapy in PD-L1-Negative NSCLC Patients
A total of 199 PD-L1-negative NSCLC patients were included in this study, with a median age of 65.4 years (range: 31–86 years). There were 59 patients for first-line treatment, 101 patients for second-line treatment, and 39 patients for third or more-line treatment. 165 patients received anti-PD-(L)1 monotherapy without concurrent chemotherapy combination, and 34 patients received anti-PD-(L)1+anti-CTLA-4 combination therapy. The baseline demographic and disease characteristics of the patients are provided in Table 1.
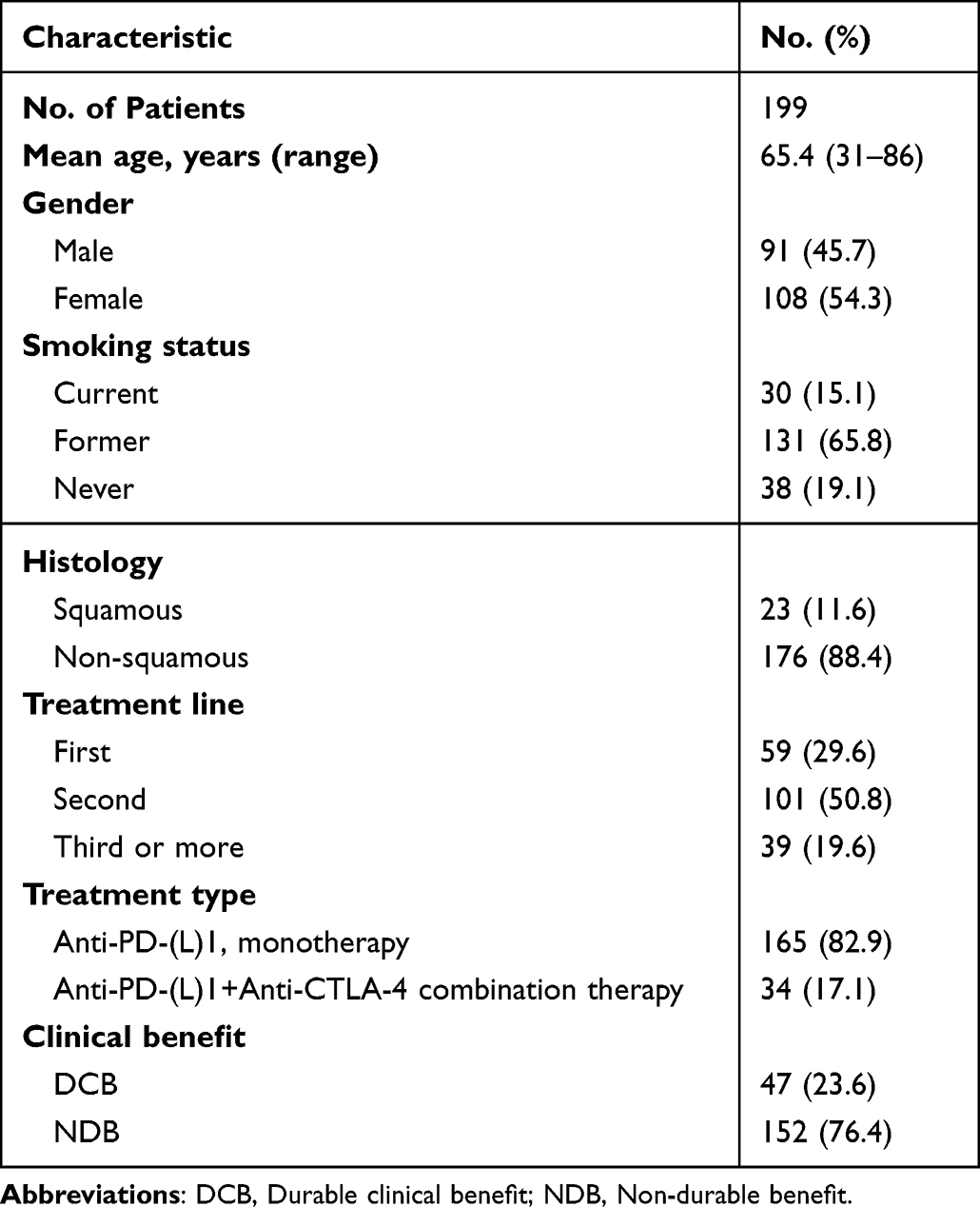 |
Table 1 PD-L1 Negative NSCLC Patient Characteristics |
We investigated the therapeutic advantages of the combination therapy of anti-PD-(L)1+anti-CTLA-4 in PD-L1-negative NSCLC patients. In univariate analysis, the variables influencing NSCLC survival included treatment (P = 0.002), treatment line (P < 0.001), and TMB (P = 0.003). Multivariate analysis confirmed the independent impact of treatment (P = 0.009) and TMB (P < 0.001) on PFS. The results of univariate and multivariate analyses are shown in Figure 1A and B. The anti-PD-(L)1+anti-CTLA-4 group demonstrated significantly higher PFS compared to the anti-PD-(L)1 monotherapy group (HR 0.5109 (95% CI, 0.3609–0.7233), P = 0.0021) (Figure 1C). Besides that, we also observed the same results in the first-line population (P = 0.0427) (Figure 1D). Overall, anti-PD-(L)1+anti-CTLA-4 options are significantly more effective than anti-PD-(L)1 monotherapy in PD-L1-negative NSCLC patients. TMB is suitable as a biomarker for screening PD-L1-negative NSCLC patients for immunotherapy.
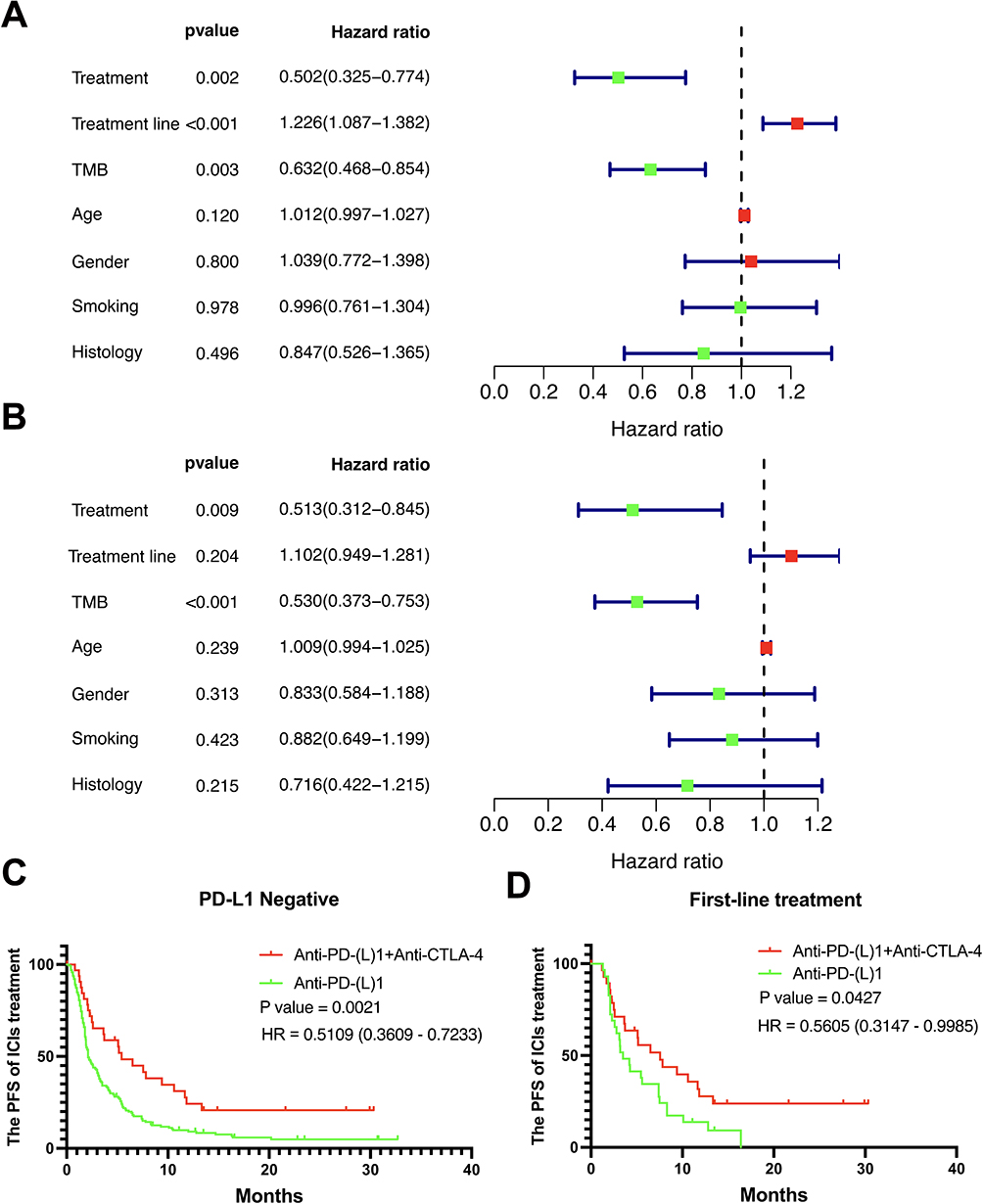 |
Figure 1 The therapeutic advantages of anti-PD-(L)1+anti-CTLA-4 in PD-L1-negative NSCLC patients. (A) Univariate analysis for PFS; (B) multivariate analysis for PFS; (C) The Kaplan-Meier plot of Anti-PD-(L)1+Anti-CTLA-4 combination therapy in PD-L1-negative NSCLC patients; (D) The Kaplan-Meier plot of Anti-PD-(L)1+Anti-CTLA-4 combination therapy in PD-L1-negative NSCLC patients with first-line treatment. |
Top 25 Gene Alterations of PD-L1-Negative NSCLC Patients Who Received the Combination Therapy of Anti-PD-(L)1+anti-CTLA-4
Next, we generated the mutation landscape for PD-L1-negative NSCLC patients who underwent first-line treatment with anti-PD-(L)1+anti-CTLA-4 therapy. A total of 30 patients were included in this cohort. There were 16 patients for the NDB group, and 14 patients for the DCB group. Detailed patient and treatment characteristics can be found in Table 2. There were no significant differences in other clinical and pathological characteristics between these groups.
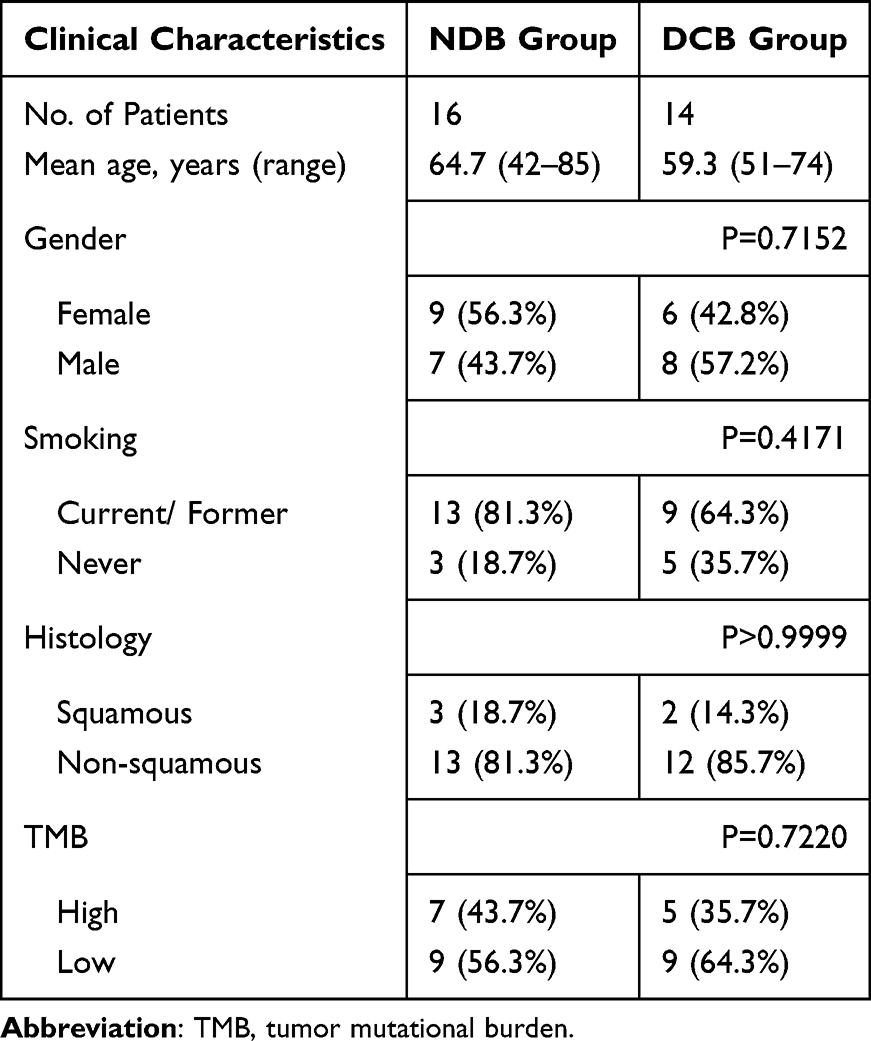 |
Table 2 PD-L1 Negative NSCLC Patients with Anti-PD-(L)1 Combination with Anti–CTLA-4 Characteristics with NDB and DCB Groups |
Top 25 gene alterations in DCB group were TP53, RYR2, OBSCN, ANO1, VPS13B, USH2A, TTN, TOX, TENM3, SMARCA4, PRIM2, PAPPA2, OTOGL, NEB, NCOA6, MACF1, LTBP1, LRP1B, KIAA1109, KEAP1, HERC2, ERBB4, CSMD3, COL14A1 and ZFHX4 (Figure 2A). We also investigated top 25 gene alterations in NDB (Figure 2B). We found common genes alterations in both groups including TP53, RYR2, OBSCN, USH2A, TTN, SMARCA4, LRP1B, and KEAP1 (Figure 2C). The mutation of KRAS (P = 0.0004) and ANO1 (P = 0.0004) were closely associated with the PFS of anti-PD-(L)1+anti-CTLA-4 therapy (Figure 2D and E). In summary, we identified high-frequency mutation genes from the genomic data of PD-L1-negative patients that can predict patient prognosis, which will be used for subsequent bioinformatics analysis and construction of a nomogram.
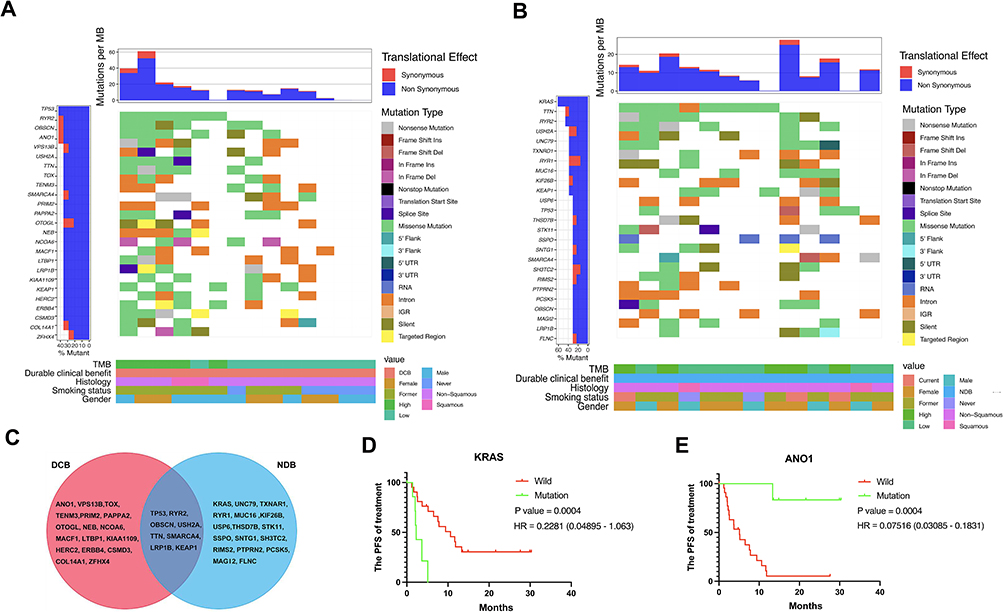 |
Figure 2 Summary of genomic landscape in PD-L1-negative NSCLC patients with dual immunotherapy. (A and B) Top 25 gene alterations in the DCB group and NDB group; (C) Venn plot of common top 25 genes; (D) The Kaplan-Meier plot of KRAS mutation; (E) The Kaplan-Meier plot of ANO1 mutation. |
GO and KEGG Enrichment Analyses of the Top 25 Gene Alterations
The results of GO analysis suggested that the significant enrichment of the top 25 genes was mainly associated with extracellular matrix component, anchoring collagen complex, and transmembrane receptor protein kinase activity in the DCB group (Figure 3A). Four pathways were particularly enriched including ErbB signaling pathway, DNA replication, Proteoglycans in cancer, and Protein digestion and absorption in DCB group (Figure 3B). Besides that, sarcoplasm, ryanodine receptor complex, and LRR domain binding were main enrichments in NDB group (Figure 3C). Autophagy animal, FoxO signaling pathway, proteoglycans in cancer, and long-term depression were main enrichments in NDB group (Figure 3D).
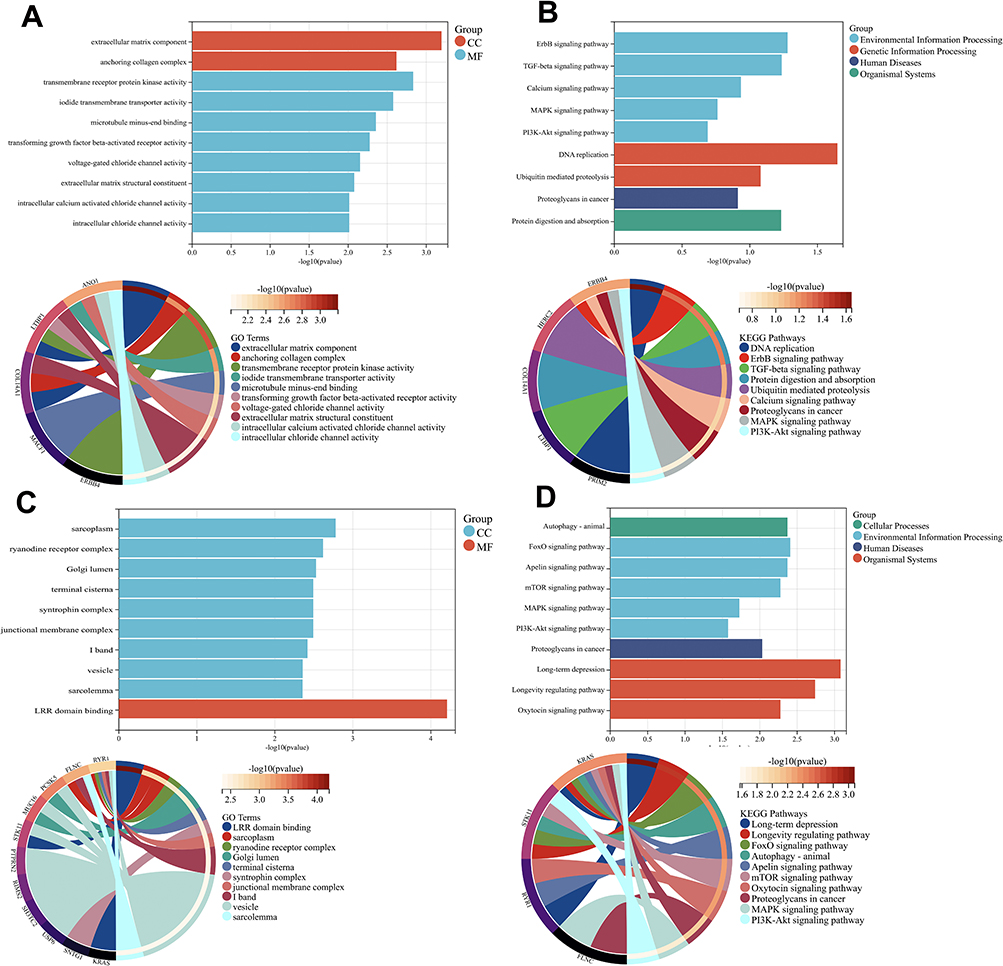 |
Figure 3 GO and KEGG enrichment analysis. (A) GO analysis of DCB; (B) KEGG analysis of DCB; (C) GO analysis of NDB; (D) KEGG analysis of NDB. |
Identification of Independent Prognostic Mutation Genes
We then conducted Univariate Cox regression analyses on the top 25 mutation genes within the NDB and DCB groups to further refine our selection of genes influencing prognosis. We observed that the mutation of KRAS (P = 0.0019), ANO1 (P = 0.0056), COL14A1 (P = 0.0238), LTBP1 (P = 0.0331), ERBB4 (P = 0.0383), and PCSK5 (P = 0.0465) could serve as independent prognostic factors in PD-L1-negative NSCLC treated with anti-PD-(L)1+anti-CTLA-4 therapy. The results of the univariate Cox regression analysis of gene alterations in the DCB and NDB groups are presented in Table 3. The identified independent prognostic mutation genes, in conjunction with the patient’s clinical data, were utilized for constructing subsequent nomograms.
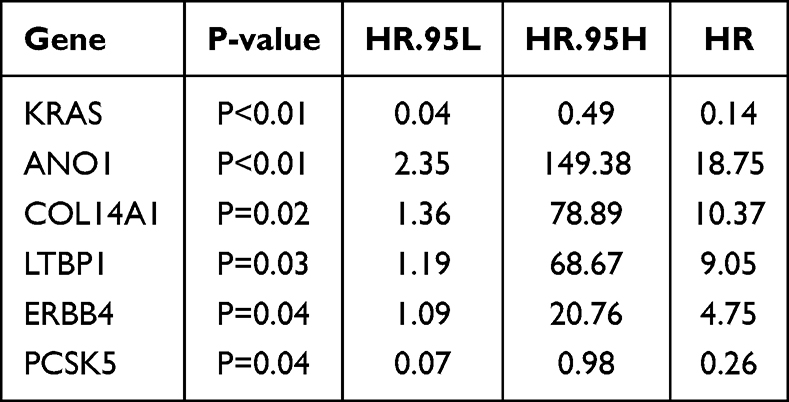 |
Table 3 Univariate COX Regression |
Construction of Nomogram for PD-L1 Negative Advanced NSCLC Treated with Combination Anti-PD-(L)1 and Anti–CTLA-4 Therapy
In this study, we integrated patient clinical information with the identified independent prognostic mutation genes (KRAS, ANO1, COL14A1, LTBP1, ERBB4, and PCSK5) to construct a novel nomogram for predicting the 6-month and 1-year PFS of PD-L1-negative advanced NSCLC patients receiving combination anti-PD-(L)1 and anti-CTLA-4 therapy. Using the Cox method, we established a nomogram to assess the prognostic significance of these features in the sample (Figure 4A). An online version of the dynamic nomogram to assist researchers and clinicians could be accessed at https://shphwl.shinyapps.io/DynNomapp/. The C-index of our nomogram was 0.880 (95% CI 0.811 to 0.949). The calibration plot demonstrated great predictive performance of our nomograms (Figure 4B–C). Based on our nomograms, clinical physicians can calculate the total points based on all variable points and subsequently assess the PFS of each PD-L1-negative advanced NSCLC patient who received the combination therapy of anti-PD-(L)1 + anti-CTLA-4.
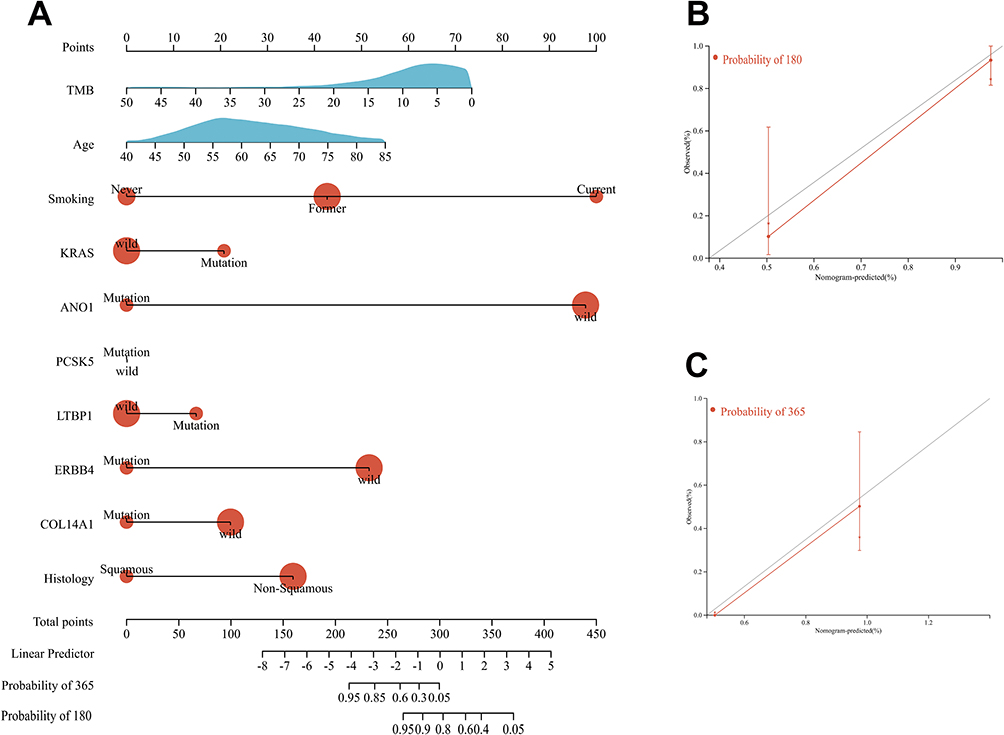 |
Figure 4 Development of nomograms for the PFS of PD-L1-negative NSCLC with dual immunotherapy. (A) Systematic nomogram to predict the 6-month and 1-year PFS. (B) The calibration plot for the chance of surviving 6-month PFS. (C) The calibration plot for the chance of surviving 1-year PFS. |
Discussion
In recent years, there has been rapid progress in immunotherapy. PD-L1-negative NSCLC without driver mutations remains a challenging subgroup in cancer treatment. PD-L1-negative NSCLC accounts for 50– 75% of all lung cancer cases.30 Therefore, the significance of exploring immunotherapy combination strategies for this subgroup is highly important. Based on results from the KEYNOTE-189 and KEYNOTE-407 clinical trials, the preferred treatment regimen for PD-L1-negative NSCLC patients is immunotherapy combined with chemotherapy as the standard first-line treatment.7,8 Moreover, the CheckMate227 clinical trial indicates that patients with PD-L1 expression below 1% treated with nivolumab plus ipilimumab achieved a median OS of 17.2 months, compared to 15.2 months with nivolumab plus chemotherapy, and 12.2 months with chemotherapy alone.13 However, the primary target population and endpoints of these phase III clinical studies were not initially intended for PD-L1-negative patients or their associated clinical indicators. There are ongoing clinical trials for various novel anti-tumor drugs specifically tailored for PD-L1-negative patients, including cadonilimab (PD-1/CTLA-4 bi-specific antibody).31 However, these trials are still in the recruitment phase and lack mature clinical data. In summary, PD-L1-negative advanced NSCLC patients represent a unique population, and data from multiple clinical trials suggest that immunotherapy combined with chemotherapy or dual immunotherapy are promising treatment strategy.
In this study, we found that the combination therapy of anti-PD-(L)1 and anti-CTLA-4 is more effective than anti-PD-(L)1 monotherapy in the PD-L1 negative NSCLC. Furthermore, to selectively identify patients who would benefit from dual immunotherapy, we conducted further analysis of patients’ genomic data. We discovered that mutations in genes such as KRAS, ANO1, COL14A1, LTBP1, ERBB4, and PCSK5 may serve as predictive biomarkers for the efficacy of dual immunotherapy in PD-L1-negative patients. Some studies have demonstrated that KRAS mutations are associated with the prognosis of NSCLC patients treated with immunotherapy32。Additionally, overexpression of ANO1 and COL14A1 has been linked to the survival of NSCLC patients.33,34 Several studies have shown that mutations or increased expression of members of the ErbB family are associated with various malignancies, including lung cancer.35 Finally, we combined patients’ clinical data and genomic data to construct a novel nomogram for predicting the PFS of such patients.
Presently, many nomograms focusing on immunotherapy for NSCLC have been published.36,37 However, there is currently a lack of a nomogram for dual immunotherapy in PD-L1-negative patients. Through reviewing relevant literature, our study is the first to specifically design a nomogram for this population. Certainly, there remain some limitations in our study. Firstly, some specific details and clinical pathological data regarding NSCLC are unclear or lacking. Secondly, there may be heterogeneity among the four studies, and the sample size of patients receiving dual immunotherapy is relatively small. Furthermore, due to the lack of data on adverse effects/side effects during treatment, this study did not discuss the potential impact of adverse reactions on treatment outcomes. Besides that, given the lack of research on such populations in public databases, our nomograms have not undergone external validation. To enhance the credibility of our findings, we aim to pursue additional external datasets in future research to validate the robustness and practicality of our models. This validation process is essential to confirm the reliability of our study and strengthen the credibility of our models. Finally, the molecular mechanisms behind these correlations must still undergo validation via both in vivo and in vitro experiments.
Conclusion
In conclusion, our study demonstrated that KRAS, ANO1, COL14A1, LTBP1, ERBB4, and PCSK5 mutation could serve as a prognostic biomarker in PD-L1 negative NSCLC patients with the combination therapy of anti-PD-(L)1 and anti-CTLA-4. Additionally, our systematic nomograms demonstrated promising potential for clinical application in predicting the prognosis of NSCLC patients undergoing dual immunotherapy. These findings help to identify biomarkers that can assist in personalized treatment decision-making, enhancing patient outcomes in the era of dual immunotherapy for PD-L1 negative advanced NSCLC.
Data Sharing Statement
All data included in this study are available including cBioPortal of Cancer Genomics ([MSK Mind, Nature Cancer 2022], [MSK, Cancer Cell 2018], [MSK, J Clin Oncol 2018]) and [MSK, Science 2015].
Ethics Approval and Consent to Participate
As all clinical data utilized in this study were obtained from publicly available clinical databases, this study was conducted under the principles outlined in the Declaration of Helsinki and was approved by the Ethics Committee of Shanghai Pulmonary Hospital (Approval number: L24-369). The hospital ethics committee has granted an exemption from obtaining informed consent for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the National Natural Science Foundation of China (grant numbers: 82072568, 82373320), Shanghai Shenkang Hospital Development Center (grant number: SHDC12024125), Shanghai Shen kang development research physician project (grant number: SHDC2022CRD048), Shanghai Pulmonary Hospital National Nature Cultivation Project (grant number: fkzr2403), and National Key R&D Program of China (grant number:2023YFC2508600, 2023YFC2508604, 2023YFC2508605).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Miller K, et al. Cancer treatment and survivorship statistics, 2019.. CA. 2019;69
2. Herbst RS, Morgensztern D, Boshoff C. The biology and management of non-small cell lung cancer. Nature. 2018;553(7689):446–454. doi:10.1038/nature25183
3. Mok TSK, Wu Y-L, Kudaba I, et al. Pembrolizumab versus chemotherapy for previously untreated, PD-L1-expressing, locally advanced or metastatic non-small-cell lung cancer (KEYNOTE-042): a randomised, open-label, controlled, Phase 3 trial. Lancet. 2019;393(10183):1819–1830. doi:10.1016/S0140-6736(18)32409-7
4. Reck M, Rodríguez-Abreu D, Robinson AG, et al. Five-year outcomes with pembrolizumab versus chemotherapy for metastatic non-small-cell lung cancer with pd-l1 tumor proportion score ≥ 50. J Clin Oncol. 2021;39(21):2339–2349. doi:10.1200/JCO.21.00174
5. Gadgeel S, Rodríguez-Abreu D, Speranza G, et al. Updated Analysis From KEYNOTE-189: pembrolizumab or placebo plus pemetrexed and platinum for previously untreated metastatic nonsquamous non-small-cell lung cancer. J Clin Oncol. 2020;38(14):1505–1517. doi:10.1200/JCO.19.03136
6. Novello S, Kowalski DM, Luft A et al. Pembrolizumab plus chemotherapy in squamous non-small-cell lung cancer: 5-year update of the phase III KEYNOTE-407 study.. J Clin Oncol. 2023;Jco2201990.
7. Novello S, Kowalski DM, Luft A, et al. Pembrolizumab plus chemotherapy in squamous non-small-cell lung cancer: 5-year update of the phase III KEYNOTE-407 study.. J Clin Oncol. 2023;41(11):1999–2006. doi:10.1200/JCO.22.01990
8. Garassino MC, Gadgeel S, Speranza G, et al. Pembrolizumab plus pemetrexed and platinum in nonsquamous non-small-cell lung cancer: 5-year outcomes from the phase 3 KEYNOTE-189 study. J Clin Oncol. 2023;41(11):1992–1998. doi:10.1200/JCO.22.01989
9. Larkin J, Chiarion-Sileni V, Gonzalez R, et al. Five-year survival with combined nivolumab and ipilimumab in advanced melanoma. N Engl J Med. 2019;381(16):1535–1546. doi:10.1056/NEJMoa1910836
10. Yau T, Kang Y-K, Kim T-Y, et al. Efficacy and safety of nivolumab plus ipilimumab in patients with advanced hepatocellular carcinoma previously treated with sorafenib: the checkmate 040 randomized clinical trial. JAMA Oncol. 2020;6(11):e204564. doi:10.1001/jamaoncol.2020.4564
11. Hellmann MD, Paz-Ares L, Bernabe Caro R, et al. Nivolumab plus ipilimumab in advanced non-small-cell lung cancer. N Engl J Med. 2019;381(21):2020–2031. doi:10.1056/NEJMoa1910231
12. Paz-Ares L, Ciuleanu T-E, Cobo M, et al. First-line nivolumab plus ipilimumab combined with two cycles of chemotherapy in patients with non-small-cell lung cancer (CheckMate 9LA): an international, randomised, open-label, phase 3 trial. Lancet Oncol. 2021;22(2):198–211. doi:10.1016/S1470-2045(20)30641-0
13. Paz-Ares LG, Ramalingam SS, Ciuleanu T-E, et al. First-line nivolumab plus ipilimumab in advanced NSCLC: 4-Year outcomes from the randomized, open-label, phase 3 checkmate 227 part 1 trial. J Thorac Oncol. 2022;17(2):289–308. doi:10.1016/j.jtho.2021.09.010
14. Liu L, Bai H, Wang C, et al. Efficacy and safety of first-line immunotherapy combinations for advanced NSCLC: a systematic review and network meta-analysis. J Thorac Oncol. 2021;16(7):1099–1117. doi:10.1016/j.jtho.2021.03.016
15. Doroshow DB, Bhalla S, Beasley MB, et al. PD-L1 as a biomarker of response to immune-checkpoint inhibitors. Nat Rev Clin Oncol. 2021;18(6):345–362. doi:10.1038/s41571-021-00473-5
16. Wang L, Dong T, Xin B, et al. Integrative nomogram of CT imaging, clinical, and hematological features for survival prediction of patients with locally advanced non-small cell lung cancer. Eur Radiol. 2019;29(6):2958–2967. doi:10.1007/s00330-018-5949-2
17. Tanadini-Lang S, Rieber J, Filippi AR, et al. Nomogram based overall survival prediction in stereotactic body radiotherapy for oligo-metastatic lung disease. Radiother Oncol. 2017;123(2):182–188. doi:10.1016/j.radonc.2017.01.003
18. Oberije C, De Ruysscher D, Houben R, et al. A validated prediction model for overall survival from stage III non-small cell lung cancer: toward survival prediction for individual patients. Int J Radiat Oncol Biol Phys. 2015;92(4):935–944. doi:10.1016/j.ijrobp.2015.02.048
19. Tang XR, Li Y-Q, Liang S-B, et al. Development and validation of a gene expression-based signature to predict distant metastasis in locoregionally advanced nasopharyngeal carcinoma: a retrospective, multicentre, cohort study. Lancet Oncol. 2018;19(3):382–393. doi:10.1016/S1470-2045(18)30080-9
20. Cerami E, Gao J, Dogrusoz U, et al. The cBio cancer genomics portal: an open platform for exploring multidimensional cancer genomics data. Cancer Discov. 2012;2(5):401–404. doi:10.1158/2159-8290.CD-12-0095
21. Vanguri RS, Luo J, Aukerman AT, et al. Multimodal integration of radiology, pathology and genomics for prediction of response to PD-(L)1 blockade in patients with non-small cell lung cancer. Nat Cancer. 2022;3(10):1151–1164. doi:10.1038/s43018-022-00416-8
22. Hellmann MD, Nathanson T, Rizvi H, et al. Genomic features of response to combination immunotherapy in patients with advanced non-small-cell lung cancer. Cancer Cell. 2018;33(5):843–852.e4. doi:10.1016/j.ccell.2018.03.018
23. Rizvi H, Sanchez-Vega F, La K, et al. Molecular determinants of response to anti-programmed cell death (PD)-1 and anti-programmed death-ligand 1 (PD-L1) blockade in patients with non-small-cell lung cancer profiled with targeted next-generation sequencing. J Clin Oncol. 2018;36(7):633–641. doi:10.1200/JCO.2017.75.3384
24. Rizvi NA, Hellmann MD, Snyder A, et al. Cancer immunology. Mutational landscape determines sensitivity to PD-1 blockade in non-small cell lung cancer. Science. 2015;348(6230):124–128. doi:10.1126/science.aaa1348
25. Kuhl CK, Alparslan Y, Schmoee J, et al. Validity of RECIST version 1.1 for response assessment in metastatic cancer: a prospective, multireader study. Radiology. 2019;290(2):349–356. doi:10.1148/radiol.2018180648
26. Skidmore ZL, Wagner AH, Lesurf R, et al. GenVisR: genomic visualizations in R. Bioinformatics. 2016;32(19):3012–3014. doi:10.1093/bioinformatics/btw325
27. Wu T, Hu E, Xu S, et al. clusterProfiler 4.0: a universal enrichment tool for interpreting omics data. Innovation. 2021;2(3):100141. doi:10.1016/j.xinn.2021.100141
28. Liu TT, Li R, Huo C, et al. Identification of CDK2-related immune forecast model and ceRNA in Lung adenocarcinoma, a pan-cancer analysis. Front Cell Dev Biol. 2021;9:682002. doi:10.3389/fcell.2021.682002
29. Sun D, Zhu Y, Zhao H, et al. Loss of ARID1A expression promotes lung adenocarcinoma metastasis and predicts a poor prognosis. Cell Oncol. 2021;44(5):1019–1034. doi:10.1007/s13402-021-00616-x
30. Schoenfeld AJ, Rizvi H, Bandlamudi C, et al. Clinical and molecular correlates of PD-L1 expression in patients with lung adenocarcinomas. Ann Oncol. 2020;31(5):599–608. doi:10.1016/j.annonc.2020.01.065
31. Pang X, Huang Z, Zhong T, et al. Cadonilimab, a tetravalent PD-1/CTLA-4 bispecific antibody with trans-binding and enhanced target binding avidity. MAbs. 2023;15(1):2180794. doi:10.1080/19420862.2023.2180794
32. Ricciuti B, Alessi JV, Elkrief A, et al. Dissecting the clinicopathologic, genomic, and immunophenotypic correlates of KRAS(G12D)-mutated non-small-cell lung cancer. Ann Oncol. 2022;33(10):1029–1040. doi:10.1016/j.annonc.2022.07.005
33. He Y, Li H, Chen Y, et al. Expression of anoctamin 1 is associated with advanced tumor stage in patients with non-small cell lung cancer and predicts recurrence after surgery. Clin Transl Oncol. 2017;19(9):1091–1098. doi:10.1007/s12094-017-1643-0
34. Li H, LEI Y, LI G, et al. Identification of tumor-suppressor genes in lung squamous cell carcinoma through integrated bioinformatics analyses. Oncol Res. 2023;32(1):187–197. doi:10.32604/or.2023.030656
35. Roskoski R Jr. The ErbB/HER family of protein-tyrosine kinases and cancer. Pharmacol Res. 2014;79:34–74. doi:10.1016/j.phrs.2013.11.002
36. Wang L, Ren Z, Yu B, et al. Development of nomogram based on immune-related gene FGFR4 for advanced non-small cell lung cancer patients with sensitivity to immune checkpoint inhibitors. J Transl Med. 2021;19(1):22. doi:10.1186/s12967-020-02679-0
37. Zeng H, Huang -W-W, Liu Y-J, et al. Development and validation of a nomogram for predicting prognosis to immune checkpoint inhibitors plus chemotherapy in patients with non-small cell lung cancer. Front Oncol. 2021;11:685047. doi:10.3389/fonc.2021.685047
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Establishment and Validation of a Predictive Nomogram for Postoperative Survival of Stage I Non-Small Cell Lung Cancer
Wang ZH, Deng L
International Journal of General Medicine 2022, 15:7287-7298
Published Date: 14 September 2022
Molecular Characteristics and the Effect of KRAS Mutation on the Prognosis of Immunotherapy in Non-Small Cell Lung Cancer in Xinjiang, China
Gu G, Yu B, Wan H, Lu S, Zhu X, Zhao Y, Fuxi Y, Liu C
OncoTargets and Therapy 2022, 15:1021-1032
Published Date: 21 September 2022
Immunotherapy for Urothelial Carcinoma: Focus on Clinical Utility of Nivolumab
Chiang RS, Glover MJ, Khaki AR, Srinivas S
OncoTargets and Therapy 2022, 15:1259-1269
Published Date: 20 October 2022
The Extended Surgical Concepts for Hepatocellular Carcinoma in the Era of Immune Checkpoint Inhibitors
Hsu HM, Tsai HI, Lee WC, Wang CC, Yu MC, Lin SM, Lin CY, Wu CH, Lee CW
Journal of Hepatocellular Carcinoma 2023, 10:1873-1880
Published Date: 24 October 2023
Development and Validation of a Novel Nomogram Integrated with Hypoxic and Lactate Metabolic Characteristics for Prognosis Prediction in Hepatocellular Carcinoma
Qiu X, Dong L, Wang K, Zhong X, Xu H, Xu S, Guo H, Wei X, Chen W, Xu X
Journal of Hepatocellular Carcinoma 2024, 11:241-255
Published Date: 2 February 2024