Back to Journals » Cancer Management and Research » Volume 18

Association Between Blood Transfusion and Survival Outcomes in Metastatic Cutaneous Melanoma Treated with Nivolumab
Authors Coskun A ![]() , Cavdar E, Sali S, Odabasi Bukun H, Sali M, Sahin AB, Deligonul A, Cubukcu E, Evrensel T
, Cavdar E, Sali S, Odabasi Bukun H, Sali M, Sahin AB, Deligonul A, Cubukcu E, Evrensel T
Received 22 March 2026
Accepted for publication 26 May 2026
Published 5 June 2026 Volume 2026:18 611126
DOI https://doi.org/10.2147/CMAR.S611126
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Harikrishna Nakshatri
Alper Coskun,1 Eyyup Cavdar,2 Seda Sali,1 Hulya Odabasi Bukun,1 Mursel Sali,1 Ahmet Bilgehan Sahin,1 Adem Deligonul,1 Erdem Cubukcu,1 Turkkan Evrensel1
1Department of Medical Oncology, Bursa Uludağ University Faculty of Medicine, Bursa, Turkey; 2Department of Medical Oncology, Namık Kemal University Faculty of Medicine, Tekirdağ, Turkey
Correspondence: Alper Coskun, Department of Medical Oncology, Bursa Uludağ University Faculty of Medicine, Bursa, Turkey, Email [email protected]
Objective: Immune checkpoint inhibitors (ICIs) are a cornerstone in the treatment of metastatic cutaneous malignant melanoma (cMM). Blood transfusions exert immunomodulatory effects that may impair antitumor immunity; however, their impact on survival outcomes in patients receiving ICIs remains unclear. This study evaluated the association between blood transfusion and survival outcomes in patients with metastatic cMM treated with nivolumab.
Methods: In this retrospective cohort study, 57 patients with metastatic cMM who received nivolumab as second-line therapy between January 2018 and December 2023 were analyzed. Blood transfusion exposure during the metastatic stage and survival outcomes, including progression-free survival (PFS) and overall survival (OS), were assessed.
Results: The median age was 60.0 years (range, 25.0– 87.0). Median follow-up was 55.0 months. Median PFS was 10.23 months (95% confidence interval [CI], not estimable to 21.53), and median OS was 31.93 months (95% CI, not estimable to 66.31). Kaplan-Meier analysis demonstrated significantly worse PFS and OS among patients who received red blood cell (RBC) transfusions (Log Rank, p = 0.024, p = 0.016, respectively). In univariate Cox regression analysis, melanoma localization, brain metastases at metastatic onset, shorter nivolumab duration, and RBC transfusion exposure were associated with poorer survival outcomes.
Conclusion: Blood transfusion during the metastatic stage was associated with reduced survival in patients with metastatic cMM receiving nivolumab. These findings suggest that transfusion-related immunomodulation may be associated with reduced immunotherapy efficacy and highlight RBC transfusion as a clinically relevant and potentially modifiable factor in patient management.
Keywords: blood transfusion, immune checkpoint inhibitors, immunotherapy, melanoma, nivolumab, survival
Introduction
Cutaneous malignant melanoma (cMM) is responsible for nearly 80% of deaths attributable to skin cancer, despite accounting for only approximately 4% of all cutaneous malignancies.1 Although relatively uncommon compared with other skin cancers, cMM represents a major challenge in oncology due to its high metastatic potential and poor prognosis in advanced stages. According to cancer statistics from the United States, the 5-year survival rate exceeds 99% in patients with localized disease; however, this rate decreases markedly to around 35% once distant metastases develop.2
Over the past decade, immune checkpoint inhibitors (ICIs) have emerged as the foundation of treatment for metastatic cMM, providing substantial improvements in response rates and survival compared with conventional chemotherapy (CT) regimens. The clinical efficacy of ICIs in metastatic cMM has been consistently demonstrated across multiple studies.3–8 These agents enhance antitumor immunity by inhibiting key immune regulatory receptors expressed on T lymphocytes, including cytotoxic T-lymphocyte–associated antigen-4, programmed cell death-1 (PD-1), and lymphocyte activation gene-3.6,9 As the therapeutic activity of ICIs depends on effective immune activation, factors that compromise immune function, particularly those affecting T-cell activity, may negatively influence treatment outcomes.
Anemia represents the most frequent hematologic abnormality in patients with cancer and may, in some cases, constitute the only clinical manifestation of the disease.10 Its pathogenesis is multifactorial and includes anemia of chronic disease, hemorrhage, immune- or mechanically mediated hemolysis, CT-induced myelosuppression, and bone marrow infiltration by malignant cells.11 Red blood cell (RBC) transfusion is commonly used to manage cancer-related anemia, treatment-associated toxicities, and perioperative blood loss.12 Nevertheless, RBC transfusion has been shown to exert immunosuppressive effects that may promote tumor recurrence and progression. These effects are largely attributed to transfusion-related immunomodulation (TRIM), mediated by residual leukocytes, apoptotic cells, and biologically active mediators present in RBC, resulting in impaired immune surveillance.12,13 Consequently, RBC transfusion may negatively influence the efficacy of ICI therapy through TRIM effects. Supporting this concept, a systematic review demonstrated poorer survival outcomes among patients receiving blood transfusions during curative-intent surgery, a phenomenon attributed to TRIM.14
In addition to RBCs, other blood products such as platelets (PLT), fresh frozen plasma (FFP), and cryoprecipitate are frequently administered in cancer patients with coagulation abnormalities.15 Platelet-driven tumor progression has been linked to elevated levels of thromboxane, serotonin, and other metabolites, increased release of growth factors including vascular endothelial growth factor, and the presence of platelet-derived microparticles (PMPs).16–19 PMPs are known to facilitate tumor growth and dissemination by promoting tumor microenvironment formation through growth factor release and by inducing proangiogenic and proinflammatory signaling. Experimental and observational studies have suggested that FFP-related inflammatory and growth mediators may contribute to tumor progression in certain settings.12 These observations suggest that non-RBC blood products may also influence immune responses and potentially affect ICI efficacy.
Given that ICIs are widely used in the treatment of metastatic cMM, factors that impair immune function may negatively affect treatment efficacy. Prior studies have shown that concomitant exposure to agents such as antibiotics and corticosteroids can attenuate the antitumor activity of ICIs.20,21 Recent studies have also emphasized the evolving prognostic landscape and immunotherapy-related factors in advanced cutaneous skin cancers.22 Given the highly immunogenic nature of cMM and the central role of T-cell-mediated antitumor activity in ICI efficacy, TRIM may be particularly relevant in this patient population. In light of the well-documented immunosuppressive properties of blood transfusions, reducing transfusion exposure in patients with cMM receiving ICIs may represent a rational clinical approach. Accordingly, the present study aimed to investigate the association between blood transfusion during the metastatic stage, including RBC, PLT, and/or FFP, and treatment efficacy and toxicity outcomes in patients with metastatic cMM treated with nivolumab, an anti PD-1 ICI. In addition to transfusion-related variables, exploratory analyses of selected clinicopathological and inflammatory parameters were also performed to better characterize factors potentially associated with survival outcomes.
Materials and Methods
Study Design and Patient Population
This study was conducted as a clinical, observational cohort study with a retrospective design. Adult patients (≥ 18 years) diagnosed with metastatic (stage IV) cMM, who were followed at our tertiary oncology center and initiated nivolumab as second-line therapy in the metastatic setting between January 1, 2018, and December 31, 2023, were eligible for inclusion. All available clinical data were retrospectively retrieved and analyzed.
Data Collection
Demographic and clinicopathological data were obtained from physical patient charts and the institutional electronic medical record system. Collected variables included age, sex, primary melanoma skin localization, metastatic status at diagnosis, metastatic sites at diagnosis (when applicable), performance of optimal surgical resection in patients without metastatic disease at diagnosis, prior treatments received before metastatic progression, dates and sites of recurrence or metastasis, treatments administered before nivolumab in the metastatic stage, baseline laboratory parameters prior to nivolumab initiation (hemoglobin, neutrophil count, lymphocyte count, platelet count, albumin, and C-reactive protein levels), ABO and Rhesus (Rh) blood groups, duration of nivolumab therapy, history and timing of blood transfusions before, during, and after nivolumab treatment, type and volume of transfused blood products (when applicable), follow-up duration, treatment response, and survival outcomes.
For exposure classification, only blood transfusions administered during the metastatic stage were considered. Pre-nivolumab transfusion exposure was defined as blood transfusions given within six months prior to the initiation of second-line nivolumab.
Inflammatory and Nutritional Indices
Based on baseline hematological and biochemical parameters, several inflammatory and nutritional prognostic indices previously reported to have prognostic relevance across different malignancies were calculated. These included the neutrophil-to-lymphocyte ratio (NLR), platelet-to-lymphocyte ratio (PLR), systemic immune-inflammation index (SII), C-reactive protein-to-albumin ratio (CAR), and hemoglobin–albumin–lymphocyte–platelet score (HALP).23–28 The conduct and reporting of this study followed the Reporting Recommendations for Tumor Marker Prognostic Studies (REMARK) guidelines. In addition, study design and reporting complied with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational cohort studies.29,30
Outcome Definitions
Progression-free survival (PFS) was defined as the interval from the initiation of nivolumab treatment to documented disease progression, death from any cause, or the date of last follow-up. Overall survival (OS) was defined as the time from nivolumab initiation to death from any cause or last follow-up. Second progression-free survival (PFS2) was defined as the time from the start of subsequent-line therapy following progression on nivolumab to disease progression, death, or last follow-up. Patients without documented progression or death at the time of analysis were censored at the date of their last recorded follow-up for PFS, OS, and PFS2.
Time-Dependent Cox Regression Analysis
To account for the timing of RBC exposure after nivolumab initiation and minimize immortal time bias, a time-dependent Cox proportional hazards model was additionally performed for OS. RBC transfusions occurring after nivolumab initiation and before death or last follow-up were modeled as time-dependent covariates. Patients were considered unexposed until the first post-nivolumab RBC transfusion and exposed thereafter. Exploratory landmark analyses for PFS were also considered; however, the number of patients receiving RBC transfusion within predefined landmark periods was too limited for meaningful comparative analyses.
Treatment Response and Safety Assessment
Tumor response to nivolumab therapy was assessed according to the Response Evaluation Criteria in Solid Tumours (RECIST), version 1.1, and categorized as complete response (CR), partial response (PR), stable disease (SD), or progressive disease (PD). Treatment-related adverse events of any grade were evaluated and graded in accordance with the Common Terminology Criteria for Adverse Events (CTCAE), version 5.0.
Ethics Approval and Informed Consent
The study protocol was approved by the Bursa Uludağ University Health Research Ethics Committee (Decision No: 2025/4-20, Date: February 19, 2025). All procedures were conducted in accordance with institutional regulations and applicable local legislation. Written informed consent was waived by the Ethics Committee due to the retrospective nature of the study and the use of fully anonymized data. Patient information was de-identified prior to analysis, and no personally identifiable data were collected or disclosed. The study adhered to the ethical principles of the Declaration of Helsinki (1975), as revised in 2024.
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics version 25.0. Categorical variables were summarized as frequencies and percentages, whereas continuous variables were reported as mean ± standard deviation, median, and range (minimum–maximum). Data distribution was assessed using the Kolmogorov–Smirnov and Shapiro–Wilk tests. Comparisons between two groups for continuous variables were conducted using the Mann–Whitney U-test, irrespective of distribution characteristics. Categorical variables were compared using the Chi-square test. Survival analyses were performed using the Kaplan–Meier method, and survival curves were compared with the Log Rank test. Univariate Cox proportional hazards regression analyses were used to identify potential factors associated with PFS and OS. These analyses were considered exploratory, whereas transfusion exposure represented the primary variable of interest. Multivariable Cox regression analysis was not performed to avoid model overfitting, considering the limited number of events relative to the number of clinically relevant covariates. Continuous variables were categorized using predefined or distribution-based thresholds when appropriate. RBC transfusion exposure was classified into three predefined groups (0 units, 1–3 units, and ≥4 units) to evaluate potential dose–response relationships. Missing data were managed using a complete-case analysis approach. All statistical tests were two-sided, and a p value < 0.05 was considered statistically significant.
Results
During the study period, 86 patients were identified as having received nivolumab for cMM. After retrospective screening, patients were excluded for the following reasons: nivolumab use in the adjuvant setting (n = 7), incomplete or missing data (n = 6), administration of nivolumab as third-line or later therapy in the metastatic setting (n = 5), diagnosis of mucosal malignant melanoma (n = 5), diagnosis of uveal malignant melanoma (n = 4), and initiation of nivolumab as first-line therapy in the metastatic setting (n = 2). Following these exclusions, 57 patients were included in the final analysis.
The median age of the study population was 60.0 years (range, 25.0–87.0), and 37 patients (64.9%) were male. At the time of initial diagnosis, 30 patients (52.6%) presented with metastatic disease. Among patients without metastasis at diagnosis, 16 (28.1%) had undergone optimal surgical resection. Pathological subtype information was unavailable in 20 patients (35.1%); among those with known subtypes, nodular cMM was the most frequently observed, identified in 18 patients (31.6%). All patients received nivolumab as second-line therapy in the metastatic setting. As first-line treatment for metastatic disease, temozolomide was administered to 50 patients (87.7%), while seven patients (12.3%) received combined dabrafenib and trametinib therapy. The median duration of nivolumab treatment was 4.0 months (range, 0.5–71.0). BRAF mutations were detected in 14 patients (24.6%), including isolated V600E mutations in 10 patients (17.5%), combined V600E/V600D mutations in two patients, combined V600E/V600K mutations in one patient, and an isolated V600K mutation in one patient. Baseline demographic and clinicopathological characteristics are summarized in Table 1.
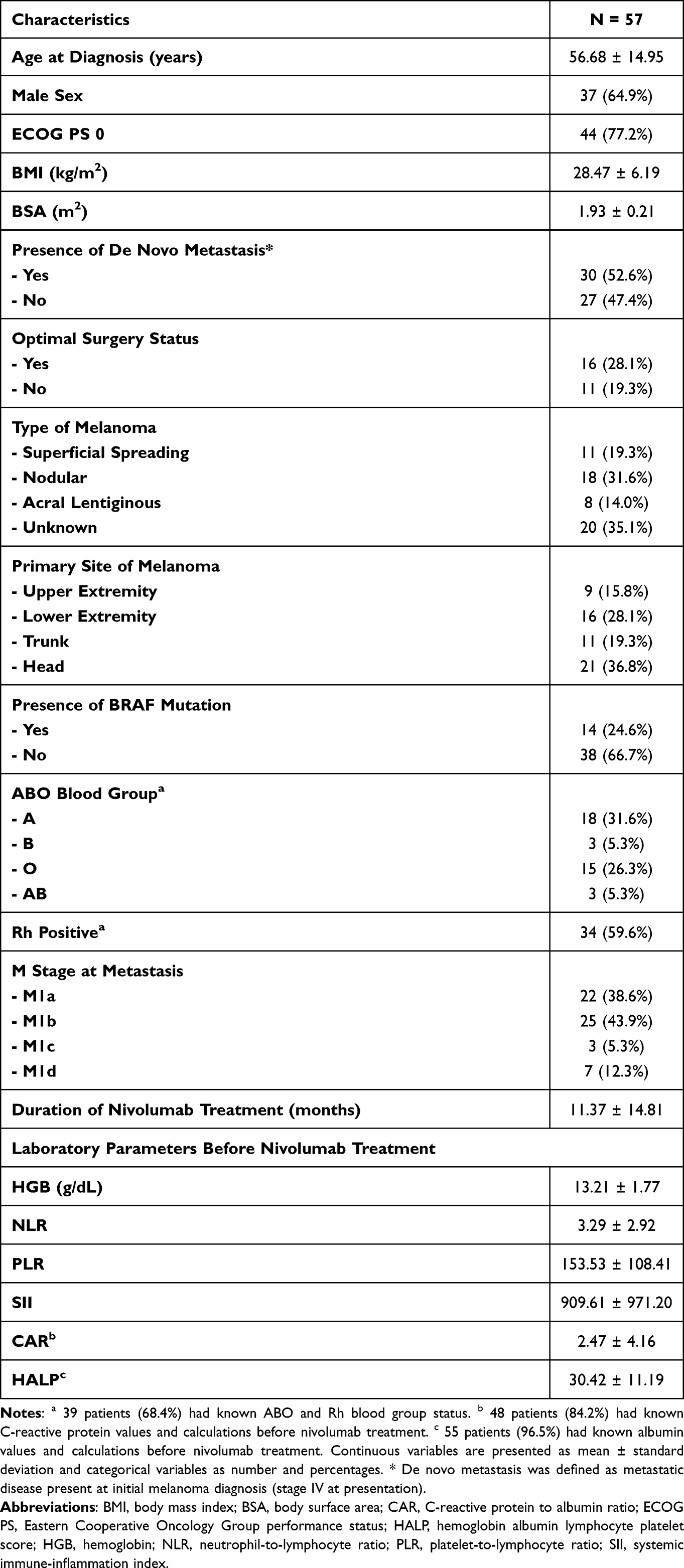 |
Table 1 General Characteristics of the Patients |
In the metastatic setting, blood transfusions were administered to 16 patients (28.1%). RBC was transfused in 13 patients (22.8%), FFP in four patients (7.0%), and PLT in two patients (3.5%). With respect to transfusion timing, two patients (3.5%) received transfusions exclusively before nivolumab treatment, two patients (3.5%) during treatment only, eight patients (14.0%) after treatment only, two patients (3.5%) both before and during nivolumab treatment, and two patients (3.5%) both during and after nivolumab treatment. There was a statistically significant difference in age at diagnosis between the transfusion and non-transfusion groups (p = 0.008). Comparative demographic and clinicopathological characteristics according to transfusion status are presented in Table 2.
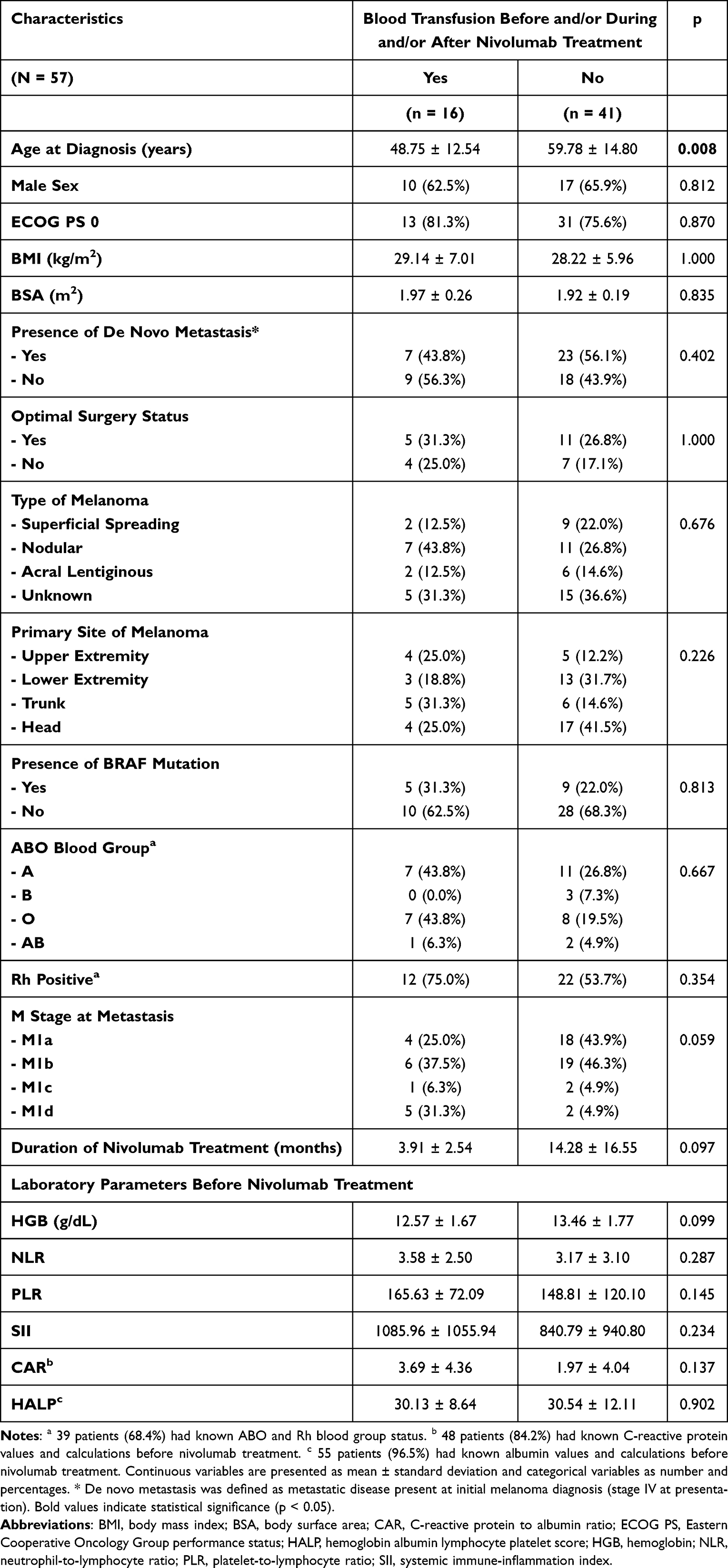 |
Table 2 Comparison of Clinical Features Between Transfused and Non-Transfused Patients |
For the entire cohort, the median follow-up was 55.00 months (95% confidence interval [CI], 47.33–62.67), estimated using the reverse Kaplan-Meier method. The median PFS was 10.23 months (95% CI, not estimable to 21.53). The median OS was 31.93 months (95% CI, not estimable to 66.31). Patients who received RBC transfusions had a median PFS of 5.26 months (95% CI, 2.48–8.04), compared with 16.36 months (95% CI, 2.01–30.71) among those who did not receive transfusions. Similarly, median OS was 9.30 months (95% CI, 5.54–13.06) in the RBC transfusion group and 45.60 months (95% CI, 27.05–64.15) in the non-transfusion group. Kaplan-Meier survival analysis demonstrated significantly inferior PFS (Log Rank, p = 0.024) and OS (Log Rank, p = 0.016) in patients who received RBC transfusions. A clear separation of PFS and OS curves was observed early and remained consistent over time. Kaplan–Meier curves for PFS and OS are shown in Figures 1 and 2.
 |
Figure 1 Kaplan–Meier curves for progression-free survival (PFS). (A) PFS in the entire cohort. (B) PFS according to RBC transfusion status. The number at risk is shown below the curves. Abbreviation: RBC, red blood cell. |
 |
Figure 2 Kaplan–Meier curves for overall survival (OS). (A) OS in the entire cohort. (B) OS according to RBC transfusion status. The number at risk is shown below the curves. Abbreviation: RBC, red blood cell. |
Univariate Cox proportional hazards regression analyses were performed to identify factors associated with PFS and OS. For PFS, primary melanoma localization outside the head region, M1c and M1d disease at metastatic onset, nivolumab treatment duration of ≤ 4 months, receipt of any blood transfusion during the metastatic stage, and receipt of RBC transfusion were significantly associated with poorer outcomes (p = 0.013, p = 0.009, p = 0.002, p < 0.001, p = 0.005, and p = 0.028, respectively). In addition, receipt of ≥ 4 units of RBC transfusion was significantly associated with worse PFS compared with no transfusion (p = 0.012).
For OS, primary melanoma localization outside the head region, brain metastases at the time of metastatic disease diagnosis (M1d disease), nivolumab treatment duration of ≤ 4 months, receipt of any blood transfusion during the metastatic stage, and receipt of RBC transfusion were significantly associated with poorer survival outcomes (p = 0.018, p = 0.007, p = 0.002, p = 0.014, and p = 0.019, respectively). Moreover, receipt of ≥ 4 units of RBC transfusion was significantly associated with worse OS compared with no transfusion (p = 0.028). Detailed results of the univariate Cox regression analyses for PFS and OS are presented in Tables 3 and 4, respectively.
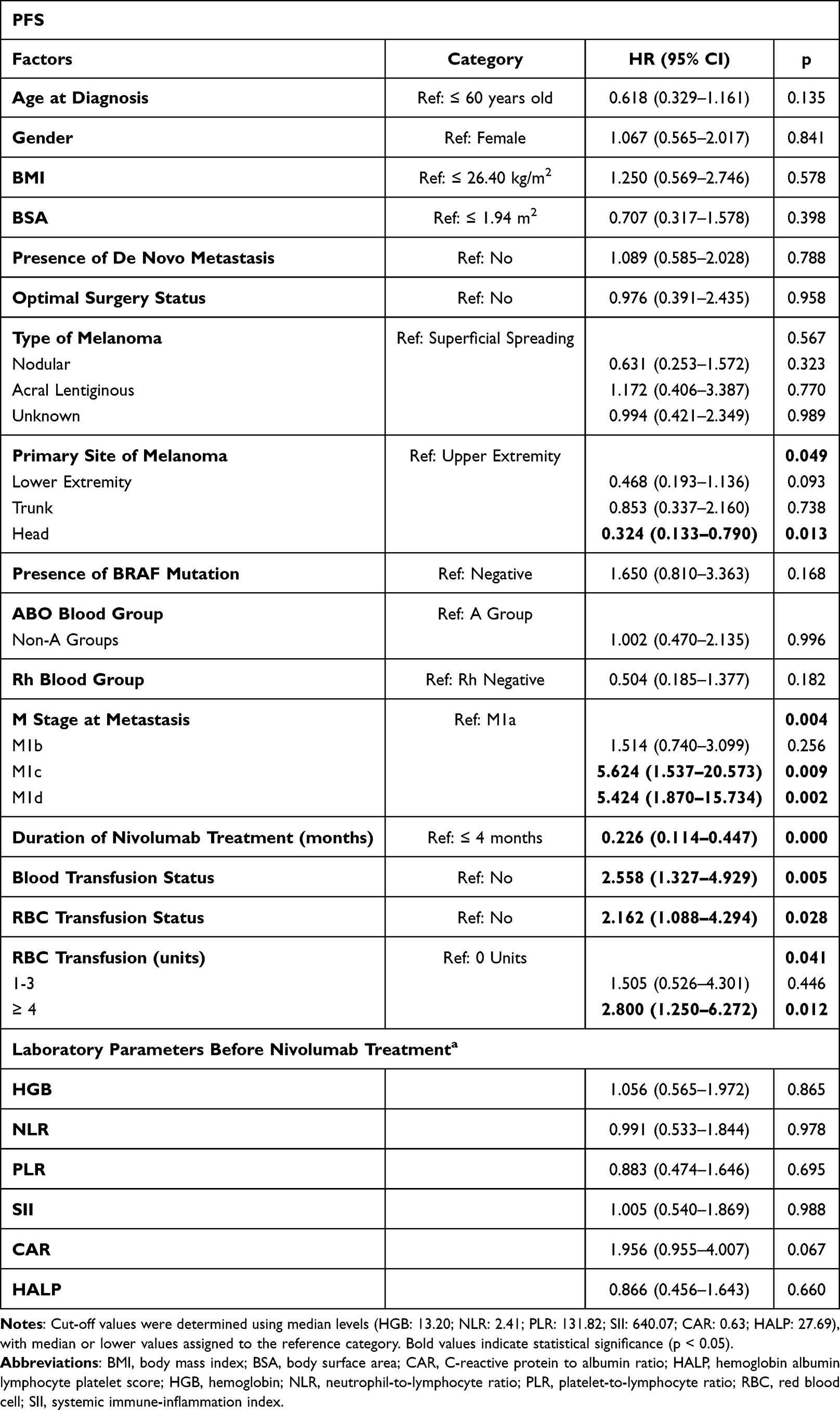 |
Table 3 Univariate Cox Regression Analysis of Clinical and Laboratory Factors Associated With Progression-Free Survival (PFS) |
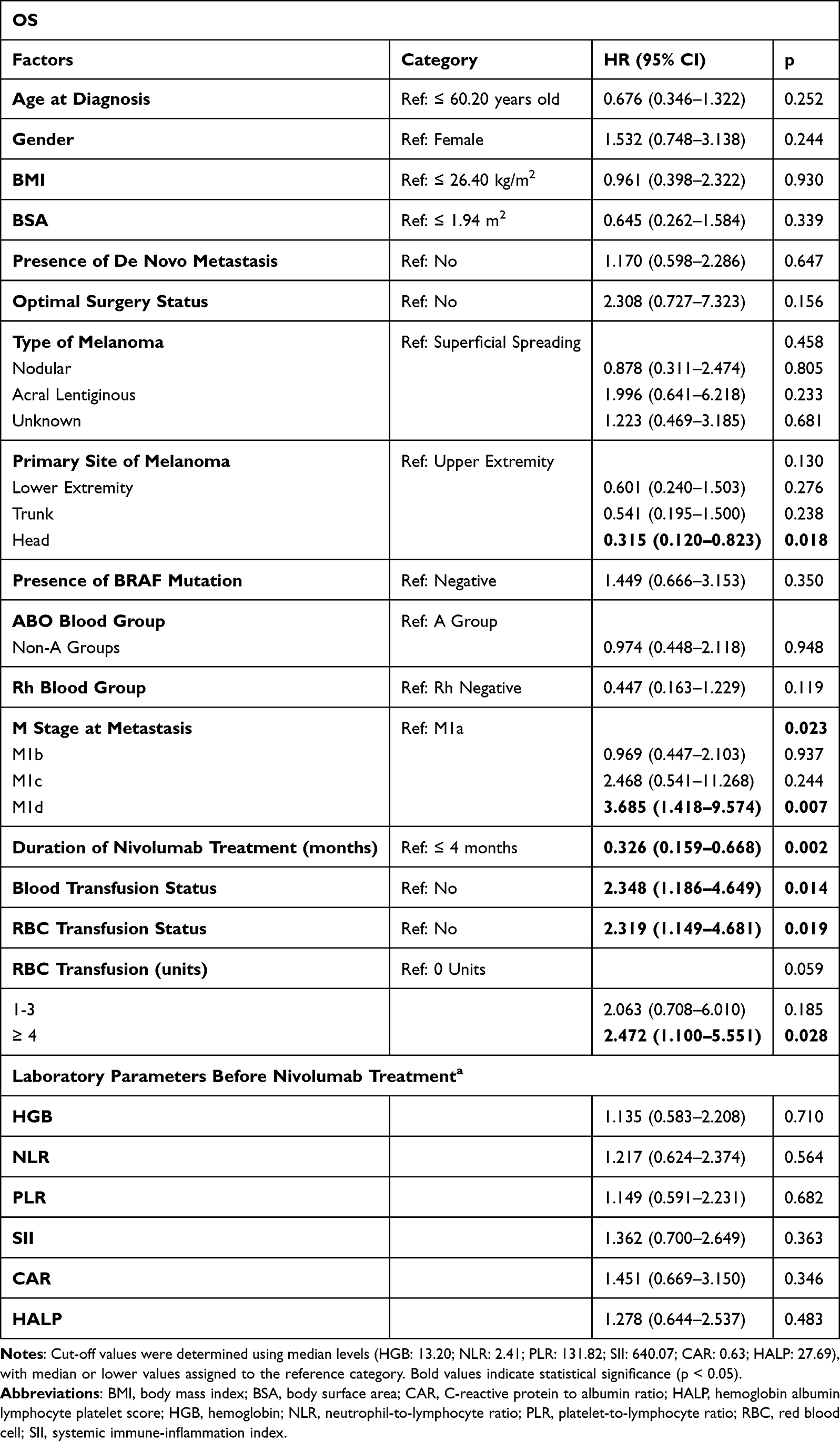 |
Table 4 Univariate Cox Regression Analysis of Clinical and Laboratory Factors Associated With Overall Survival (OS) |
To further account for immortal time bias, in the time-dependent Cox regression analysis, post-nivolumab-initiation RBC transfusion was significantly associated with inferior OS (HR 2.77, 95% CI 1.35–5.70; p = 0.006). Landmark analyses for PFS were explored but were not feasible because only one patient received RBC transfusion within the predefined 3-month landmark period.
Assessment of best response (BR), according to RECIST version 1.1, demonstrated CR in eight patients (14.0%), PR in 16 patients (28.1%), SD in 12 patients (21.1%), and PD in 21 patients (36.8%). At the time of last radiological assessment, CR was observed in five patients (8.8%), PR in nine patients (15.8%), SD in three patients (5.3%), and PD in 40 patients (70.2%).
After progression on nivolumab, 20 patients (35.1%) received subsequent systemic therapy. Ipilimumab monotherapy was the most commonly administered subsequent treatment, given to 10 patients (17.5%). Other subsequent therapies included carboplatin plus paclitaxel (n = 5), temozolomide (n = 4), and combined dabrafenib and trametinib therapy (n = 1). The median PFS2 was 3.16 months (95% CI, 2.84–3.48). Among patients who received blood transfusions, the median PFS2 was 2.60 months (95% CI, 1.98–3.22), whereas it was 4.16 months (95% CI, 2.52–5.80) in those who did not receive transfusions; this difference was not statistically significant (Log Rank, p = 0.151).
Among the 16 patients who received blood transfusions during the metastatic stage, 10 received RBC alone, three received FFP alone, two received a combination of RBC and PLT, and one received both RBC and FFP. The overall median number of transfused units per patient was 4 (range, 1–41). Among patients who received RBC transfusions, the median number of RBC units administered was 4 (range, 1–16).
In addition to survival outcomes, treatment-related adverse events were descriptively evaluated to provide an overall assessment of nivolumab treatment characteristics in the study cohort. Immune-related adverse events (irAEs) of any grade were documented in 17 patients (29.8%) following nivolumab therapy. The most frequently observed irAEs were maculopapular rash and hepatitis, each occurring in five patients (8.8%). Grade 1–2 irAEs were reported in 12 patients (21.1%), while grade 3–4 irAEs were observed in six patients (10.5%). No grade 5 irAEs were recorded.
Discussion
In this study evaluating the association between nivolumab efficacy and blood transfusion in patients with cMM, receipt of blood transfusion during the metastatic stage was associated with significantly inferior PFS and OS. These findings suggest a possible association between blood transfusion and poorer long-term survival outcomes in patients receiving ICIs.
TRIM has been reported to affect immune function through multiple mechanisms that may be relevant in patients receiving ICIs. Transfusion-related soluble mediators and immunomodulatory factors may alter T-cell, monocyte, and natural killer-cell activity, potentially impairing antitumor immune responses and contributing to poorer oncologic outcomes.31–34 These effects may be particularly important in the setting of ICI therapy, which depends on intact cellular immunity. In our cohort, the observed dose-response pattern, especially among patients receiving ≥ 4 units of RBC transfusion, further supports a possible biological interaction between transfusion exposure and ICI efficacy.
Previous studies evaluating RBC transfusion in patients receiving ICIs have similarly suggested an association between transfusion exposure and poorer treatment outcomes. Mispelbaum et al reported that RBC transfusion administered shortly after immunotherapy initiation was associated with reduced treatment response, whereas pre-immunotherapy transfusion was not.35 Likewise, D’Avella et al demonstrated inferior survival outcomes among transfused patients receiving ICIs for solid tumors.36 Although these studies included heterogeneous solid tumor populations and limited or no representation of cMM, their findings are generally consistent with the results of the present study and support a potential negative interaction between RBC transfusion and ICI efficacy.
To further address the potential for immortal time bias, a time-dependent Cox regression model was additionally performed. The association between post-nivolumab-initiation RBC transfusion and inferior OS remained significant, supporting the robustness of the findings. Nevertheless, the possibility of residual confounding by indication cannot be excluded, as patients requiring transfusion may have had more advanced disease burden or poorer clinical status.
Several limitations of this study should be acknowledged. First, blood transfusion may represent a surrogate marker of more advanced disease, poorer performance status, or a more aggressive clinical course, potentially contributing to the observed survival differences. The numerically higher proportion of M1d disease in the transfusion group may also have contributed to poorer survival outcomes. In addition, the younger age observed among transfused patients may reflect more aggressive disease biology, higher treatment intensity, or increased transfusion requirements related to disease burden; however, this finding should be interpreted cautiously given the limited sample size. In addition, detailed data regarding the specific clinical indications for transfusion, including active bleeding, disease-related anemia burden, or treatment-related hematologic toxicity, were not uniformly available and therefore could not be fully incorporated into the analyses. Although time-dependent Cox regression analysis was performed to minimize immortal time bias, residual confounding related to transfusion timing and clinical indication may still have influenced the findings. Second, the retrospective single-center design may limit the generalizability of the results. Furthermore, the relatively small sample size and limited number of events reduced the statistical power of the analyses and precluded construction of a fully adjusted multivariable model without risking overfitting. Third, due to national reimbursement restrictions during the study period, nivolumab was reimbursed only as second-line monotherapy for metastatic cMM in our healthcare system, precluding evaluation of other ICI regimens. In addition, landmark analyses for PFS could not be robustly performed because only a very small number of patients received RBC transfusions within the predefined landmark periods, limiting interpretability. Finally, incomplete adverse event data may have been present in some cases.
To the best of our knowledge, this is the first study specifically evaluating the impact of blood transfusion on survival outcomes in patients with cMM treated with PD-1 inhibitor therapy. These findings may support a more restrictive transfusion strategy in patients receiving immunotherapy.
Given the increasing use of ICIs in metastatic cMM and other solid tumors, identification of potentially modifiable factors associated with reduced treatment efficacy is clinically important. Although causality cannot be established from the present study, our findings suggest that transfusion exposure may represent a clinically relevant variable in patients receiving immunotherapy and warrant further investigation in larger prospective cohorts.
Conclusions
In this study, blood transfusion during nivolumab treatment in patients with cMM was associated with worse PFS and OS. These findings suggest a possible association between transfusion-related immunomodulation (TRIM) and reduced immunotherapy efficacy and highlight blood transfusion as a clinically relevant and potentially modifiable factor in patient management. Larger multicenter studies are warranted to validate these findings and to further clarify the impact of blood transfusion on immunotherapy efficacy and survival outcomes in this patient population.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
Ethics Approval and Informed Consent
The study protocol was approved by the Bursa Uludağ University Health Research Ethics Committee (Decision No: 2025/4-20, Date: February 19, 2025). All procedures were conducted in accordance with institutional regulations and applicable local legislation. Written informed consent was waived by the Ethics Committee due to the retrospective nature of the study and the use of fully anonymized data. Patient information was de-identified prior to analysis, and no personally identifiable data were collected or disclosed. The study adhered to the ethical principles of the Declaration of Helsinki (1975), as revised in 2024.
Consent for Publication
No individual patient data, images, or videos are presented in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors disclosed that they did not receive any grants or contracts during the conduction or writing of this manuscript.
Disclosure
The authors declare that they have no conflicts of interest related to this work.
References
1. Giblin AV, Thomas JM. Incidence, mortality and survival in cutaneous melanoma. J Plast Reconstr Aesthet Surg. 2007;60(1):32–14. doi:10.1016/j.bjps.2006.05.008
2. Siegel RL, Kratzer TB, Giaquinto AN, Sung H, Jemal A. Cancer statistics, 2025. CA Cancer J Clin. 2025;75(1):10–45. doi:10.3322/caac.21871
3. Robert C, Long GV, Brady B, et al. Nivolumab in previously untreated melanoma without BRAF mutation. N Engl J Med. 2015;372(4):320–330. doi:10.1056/NEJMoa1412082
4. Wolchok JD, Chiarion-Sileni V, Gonzalez R, et al. Overall survival with combined nivolumab and ipilimumab in advanced melanoma. N Engl J Med. 2017;377(14):1345–1356. doi:10.1056/NEJMoa1709684
5. Livingstone E, Zimmer L, Hassel JC, et al. Adjuvant nivolumab plus ipilimumab or nivolumab alone versus placebo in patients with resected stage IV melanoma with no evidence of disease (IMMUNED): final results of a randomised, double-blind, Phase 2 trial. Lancet. 2022;400(10358):1117–1129. doi:10.1016/S0140-6736(22)01654-3
6. Tawbi HA, Schadendorf D, Lipson EJ, et al. Relatlimab and nivolumab versus nivolumab in untreated advanced melanoma. N Engl J Med. 2022;386(1):24–34. doi:10.1056/NEJMoa2109970
7. Long GV, Carlino MS, McNeil C, et al. Pembrolizumab versus ipilimumab for advanced melanoma: 10-year follow-up of the Phase III KEYNOTE-006 study. Ann Oncol. 2024;35(12):1191–1199. doi:10.1016/j.annonc.2024.08.2330
8. Acar C, Yüksel HÇ, Şahin G, et al. Efficacy and prognostic factors of anti-PD1 and nivolumab-ipilimumab therapy in advanced melanoma patients resistant to prior ICI treatment. Discov Oncol. 2024;15(1):813. doi:10.1007/s12672-024-01702-w
9. Pauken KE, Dougan M, Rose NR, Lichtman AH, Sharpe AH. Adverse Events Following Cancer Immunotherapy: obstacles and Opportunities. Trends Immunol. 2019;40(6):511–523. doi:10.1016/j.it.2019.04.002
10. Gaspar BL, Sharma P, Das R. Anemia in malignancies: pathogenetic and diagnostic considerations. Hematology. 2015;20(1):18–25. doi:10.1179/1607845414Y.0000000161
11. Dunn A, Carter J, Carter H. Anemia at the end of life: prevalence, significance, and causes in patients receiving palliative care. J Pain Symptom Manag. 2003;26(6):1132–1139. doi:10.1016/j.jpainsymman.2003.04.001
12. Iqbal N, Haider K, Sundaram V, et al. Red blood cell transfusion and outcome in cancer. Transfus Apher Sci. 2017;56(3):287–290. doi:10.1016/j.transci.2017.05.014
13. Remy KE, Hall MW, Cholette J, et al. Mechanisms of red blood cell transfusion-related immunomodulation. Transfusion. 2018;58(3):804–815. doi:10.1111/trf.14488
14. Goubran H, Sheridan D, Radosevic J, Burnouf T, Seghatchian J. Transfusion-related immunomodulation and cancer. Transfus Apher Sci. 2017;56(3):336–340. doi:10.1016/j.transci.2017.05.019
15. Cata JP, Gottumukkala V. Blood transfusion practices in cancer surgery. Ind J Anaesth. 2014;58(5):637–642. doi:10.4103/0019-5049.144675
16. Cathcart MC, Gately K, Cummins R, Kay E, O’Byrne KJ, Pidgeon GP. Examination of thromboxane synthase as a prognostic factor and therapeutic target in non-small cell lung cancer. Mol Cancer. 2011;10:25. doi:10.1186/1476-4598-10-25
17. Lee HK, Eom CS, Kwon YM, Ahn JS, Kim S, Park SM. Meta-analysis: selective serotonin reuptake inhibitors and colon cancer. Eur J Gastroenterol Hepatol. 2012;24(10):1153–1157. doi:10.1097/MEG.0b013e328355e289
18. Sullivan LA, Brekken RA. The VEGF family in cancer and antibody-based strategies for their inhibition. MAbs. 2010;2(2):165–175. doi:10.4161/mabs.2.2.11360
19. Goubran H, Sabry W, Kotb R, Seghatchian J, Burnouf T. Platelet microparticles and cancer: an intimate cross-talk. Transfus Apher Sci. 2015;53(2):168–172. doi:10.1016/j.transci.2015.10.014
20. Meriggi F, Zaniboni A. Antibiotics and steroids, the double enemies of anticancer immunotherapy: a review of the literature. Cancer Immunol Immunother. 2021;70(6):1511–1517. doi:10.1007/s00262-020-02786-3
21. Cortellini A, Di Maio M, Nigro O, et al. Differential influence of antibiotic therapy and other medications on oncological outcomes of patients with non-small cell lung cancer treated with first-line pembrolizumab versus cytotoxic chemotherapy. J Immunother Cancer. 2021;9(4):e002421. doi:10.1136/jitc-2021-002421
22. Di Guardo A, Trovato F, Cantisani C, et al. Advanced cutaneous squamous cell carcinoma: biology, immunotherapy, and evolving prognostic factors. Biomedicines. 2025;13(12):3010. doi:10.3390/biomedicines13123010
23. Tan S, Zheng Q, Zhang W, Zhou M, Xia C, Feng W. Prognostic value of inflammatory markers NLR, PLR, and LMR in gastric cancer patients treated with immune checkpoint inhibitors: a meta-analysis and systematic review. Front Immunol. 2024;15:1408700. doi:10.3389/fimmu.2024.1408700
24. Ou Y, Liang S, Gao Q, et al. Prognostic value of inflammatory markers NLR, PLR, LMR, dNLR, ANC in melanoma patients treated with immune checkpoint inhibitors: a meta-analysis and systematic review. Front Immunol. 2024;15:1482746. doi:10.3389/fimmu.2024.1482746
25. Wang E, Huang H, Tang L, et al. Prognostic significance of platelet lymphocyte ratio in patients with melanoma: a meta-analysis. Medicine. 2021;100(38):e27223. doi:10.1097/MD.0000000000027223
26. Zhang Y, Chen Y, Guo C, Li S, Huang C. Systemic immune-inflammation index as a predictor of survival in non-small cell lung cancer patients undergoing immune checkpoint inhibition: a systematic review and meta-analysis. Crit Rev Oncol Hematol. 2025;210:104669. doi:10.1016/j.critrevonc.2025.104669
27. Öztop H, Hunutlu FÇ, Ekizoğlu Sİ, Gül ÖÖ, Cander S, Şahin AB. Effect of hemoglobin, albumin, lymphocyte count, and platelet (HALP) score on survival of patients with metastatic thyroid cancer treated with tyrosine kinase inhibitors. J Clin Med. 2025;14(4):1306. doi:10.3390/jcm14041306
28. Dai M, Wu W. Prognostic role of C-reactive protein to albumin ratio in cancer patients treated with immune checkpoint inhibitors: a meta-analysis. Front Oncol. 2023;13:1148786. doi:10.3389/fonc.2023.1148786
29. McShane LM, Altman DG, Sauerbrei W, et al. REporting recommendations for tumour MARKer prognostic studies (REMARK). Br J Cancer. 2005;93(4):387–391. doi:10.1038/sj.bjc.6602678
30. von Elm E, Altman DG, Egger M, et al. Strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. BMJ. 2007;335(7624):806–808. doi:10.1136/bmj.39335.541782.AD
31. Ghio M, Contini P, Negrini S, Mazzei C, Zocchi MR, Poggi A. Down regulation of human natural killer cell-mediated cytolysis induced by blood transfusion: role of transforming growth factor-β(1), soluble Fas ligand, and soluble Class I human leukocyte antigen. Transfusion. 2011;51(7):1567–1573. doi:10.1111/j.1537-2995.2010.03000.x
32. Hod EA, Spitalnik SL. Stored red blood cell transfusions: iron, inflammation, immunity, and infection. Transfus Clin Biol. 2012;19(3):84–89. doi:10.1016/j.tracli.2012.04.001
33. Vamvakas EC, Blajchman MA. Transfusion-related immunomodulation (TRIM): an update. Blood Rev. 2007;21(6):327–348. doi:10.1016/j.blre.2007.07.003
34. Muszynski JA, Spinella PC, Cholette JM, et al. Transfusion-related immunomodulation: review of the literature and implications for pediatric critical illness. Transfusion. 2017;57(1):195–206. doi:10.1111/trf.13855
35. Mispelbaum R, Hattenhauer ST, Brossart P, Heine A. Red blood cell transfusions impact response rates to immunotherapy in patients with solid malignant tumors. Front Immunol. 2022;13:976011. doi:10.3389/fimmu.2022.976011
36. D’Avella C, Devarajan K, Edelman M, Daniel, Geynisman D. The effect of packed red blood cell transfusions on the clinical efficacy of immunotherapy. J Immunother Cancer. 2020;8(Suppl 3):A180.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The DPY30-H3K4me3 Axis-Mediated PD-L1 Expression in Melanoma
Zhang Z, Han Y, Sun Q, Wang Y, Sun L
Journal of Inflammation Research 2022, 15:5595-5609
Published Date: 26 September 2022
Immunotherapy for Urothelial Carcinoma: Focus on Clinical Utility of Nivolumab
Chiang RS, Glover MJ, Khaki AR, Srinivas S
OncoTargets and Therapy 2022, 15:1259-1269
Published Date: 20 October 2022
Ability of Blood Cell Parameters to Predict Clinical Outcomes of Nivolumab Monotherapy in Advanced Esophageal Squamous Cell Carcinoma
Hamai Y, Emi M, Ibuki Y, Kurokawa T, Yoshikawa T, Ohsawa M, Hirohata R, Kitasaki N, Okada M
OncoTargets and Therapy 2023, 16:263-273
Published Date: 10 April 2023
The Extended Surgical Concepts for Hepatocellular Carcinoma in the Era of Immune Checkpoint Inhibitors
Hsu HM, Tsai HI, Lee WC, Wang CC, Yu MC, Lin SM, Lin CY, Wu CH, Lee CW
Journal of Hepatocellular Carcinoma 2023, 10:1873-1880
Published Date: 24 October 2023
NOTCH1 Mutations Predict Superior Outcomes of Immune Checkpoint Blockade in Non-Small Cell Lung Cancer
Huang Q, Cao H, Yao Q, Zhou X, Li H, Bai Q, Hu H
ImmunoTargets and Therapy 2023, 12:165-173
Published Date: 5 December 2023