Back to Journals » ImmunoTargets and Therapy » Volume 14
Anti-GAD65 Antibodies Related Refractory Epilepsy Successfully Treated with Tocilizumab: A Case Report and Systematic Literature Review
Authors Chen S, Kessi M, Tan J, He F, Zhang C, Yin F, Yang L ![]() , Peng J
, Peng J ![]()
Received 14 February 2025
Accepted for publication 11 April 2025
Published 18 April 2025 Volume 2025:14 Pages 491—500
DOI https://doi.org/10.2147/ITT.S520026
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Shurin
Shimeng Chen,1 Miriam Kessi,1 Jielu Tan,1– 3 Fang He,1– 3 Ciliu Zhang,1– 3 Fei Yin,1– 3 Lifen Yang,1– 3 Jing Peng1– 3
1Department of Pediatrics, Xiangya Hospital, Central South University, Changsha, People’s Republic of China; 2Hunan Intellectual and Developmental Disabilities Research Center, Pediatrics, Changsha, People’s Republic of China; 3Clinical Research Center for Children Neurodevelopmental Disabilities of Hunan Province, Xiangya Hospital, Central South University, Changsha, People’s Republic of China
Correspondence: Lifen Yang, Department of Pediatrics, Xiangya Hospital, Central South University, Changsha, Hunan, 410008, People’s Republic of China, Tel +86-1367435745, Fax +86-731-84327332, Email [email protected]
Background: Although anti-GAD65 related epilepsy is rare, it needs more attention because it is refractory to the conventional therapies, has poor outcome and high relapse rate. In this study, we intended to report the efficacy of tocilizumab in the treatment of anti-GAD65 antibodies related refractory epilepsy based on our center’s experience and literature review.
Methods: The clinical data of the patients managed with tocilizumab at Xiangya Hospital and those from the literature was collected and analysed.
Results: A female child presented at our center with neuropsychiatric symptoms and generalized tonic-clonic seizures (including status epilepticus) at the age of 3 years. She had positive anti-GAD65 autoantibodies. Her initial electroencephalograph showed multi-focal epileptic discharges and an early brain magnetic resonance imaging demonstrated increased intensity in the bilateral hippocampi and right insular cortex. She received several anti-seizures medications (ASMs) and immunotherapies without significant improvement; however, she experienced significant clinical, electrographic and radiological improvement after receiving four cycles of the tocilizumab. Literature review unveiled two more female cases. The mean age of seizure onset for three cases was 7.72 years, and they presented with refractory seizures (n=3), neuropsychiatric symptoms (n=3), ataxia (n=2), and anti-GAD autoantibodies were elevated in both the serum and cerebrospinal fluid (n=3). All three cases tried several combinations of ASMs and immunotherapies before tocilizumab but they remained with refractory epilepsy. Following several cycles of the tocilizumab, all cases had significant positive changes: seizure freedom (n=1), seizure control (n=2), improved-normal cognition (n=3), improved neuropsychiatry symptoms (n=2) and controlled ataxia (n=2).
Conclusion: Tocilizumab seems to be an effective therapy for the refractory anti-GAD65 related epilepsy as it can control seizures, improve cognition and neuropsychiatric symptoms.
Keywords: anti-GAD65 autoantibodies, epilepsy, tocilizumab, efficacy, safety, review
Introduction
Gamma-aminobutyric acid (GABA) is a neurotransmitter produced by the enzyme known as glutamic acid decarboxylase-65 (GAD65).1 Anti-GAD65 antibodies can cause several neurological disorders such as epilepsy, cognitive impairment, limbic encephalitis, Stiff-person spectrum disorders, cerebellar ataxia, myelopathy and brainstem dysfunction.1 Despite the fact that anti-GAD65 antibodies are considered as a cause of aforementioned syndromes, high serum titers do not associate with disease severity or response to therapies.2 Thus, it is still unclear if anti-GAD65 antibodies are pathogenic or only serve as a marker for autoimmune disorders induced by cytotoxic T cells.2 For the anti-GAD related epilepsy, patients can present with epilepsia partialis continua, refractory status epilepticus,3 segmental myoclonus and epilepsy4 and adult onset temporal lobe epilepsy (TLE).5 There are some evidences from human and animal models suggesting the role of the interneurons (including GABAergic interneurons, which have connection with GAD) in the occurrence of epilepsy.6,7 The loss of principal cells and interneurons and neuroinflammation are among the histopathological features of TLE.6 There are some evidences that GABAergic interneurons are reduced in the dentate gyrus of patients with TLE and rodent models, therefore, their loss can lower seizure threshold.6 Moreover, spontaneous recurrent seizures can reduce interneurons during epileptogenesis.6 Of concern, most of the GAD epileptic manifestations are refractory to the combinations of therapies including immunotherapies and antiseizure medications (ASMs).2,5,8–11 A recent review also revealed that the prognosis of patients diagnosed with anti-GAD65 related epilepsy is poor, more prone to relapse and can cause more central nervous system (CNS) morbidities than other anti-GAD65 related syndromes.2,12,13 Recently, tocilizumab was reported as an effective therapy for the epilepsy in two patients.14,15
Although anti-GAD65 related epilepsy is rare, it needs more attention because it is refractory to the conventional therapies, has poor outcome and high relapse rate. Therefore, we provide more evidence that tocilizumab is effective and safe therapy for this condition by sharing our treatment experience. To the best of our knowledge, this is the third report about the treatment of the anti-GAD65 related epilepsy with tocilizumab worldwide, and the first case ever in Asia. Along with our cases, we have summarized the information of all reported patients who were treated with this therapy to provide more robust evidence to advocate its use in similar situations.
Case Report
A normally developed female child presented with status epilepticus and neuropsychiatric symptoms at the age of 3 years and 2 months. She was attended in another hospital two weeks prior to the admission in our unit. The initial manifestations included aggression, biting of people, bad mood, confusion, occasional vomiting, and intermittent low fever. One month later, she experienced fever-related (39.3°C) tonic-clonic seizures for the first time that lasted for 30 minutes (status epilepticus); consequently, she was admitted to the local hospital for 2 weeks. Unfortunately, she developed cognitive decline after seizures and only received symptomatic treatment at this hospital. She experienced a second episode of frequent seizures 13 days later. These seizures continued to the next day, were accompanied with tremor of the upper extremities, and altered level of consciousness during post-ictal phase. She was then transferred to our hospital on the second day of repeated seizures. Initial investigations’ results from the first hospital and ours were similar; brain magnetic resonance images (MRIs) showed increased intensity in the bilateral hippocampi and right insular cortex (Figure 1A). The electroencephalographs (EEGs) showed multi-focal epileptic discharges and subclinical seizures (Figure 2A–F). Cerebrospinal fluid (CSF) analysis revealed normal levels of the white blood cells (WBC), protein and glucose. Serum levels of the thyroperoxidase autoantibodies (TPO-A) and thyroglobulin autoantibodies (TGA) were elevated significantly (both > 1000 IU/mL). The whole body screening for tumors via computed tomography (CT) scan was non-remarkable. There was no evidence of pathogenic infection or metabolic disease. Both CSF and serum were screened for the autoantibodies via indirect immunofluorescence on cell-based assays in an independent laboratory (KingMed Diagnostic, Changsha, Hunan). Autoantibodies checked included anti-NMDAR, -GAD65, -LGI1, -CASPR2, -GABABR, -AMPAR1, -AMPAR2, -IgLON5, -DPPX,-mGluR5, -MOG, -GFAP, -GABAAR, -AQP4 and -mGluR1, consequently, there were anti-GAD65 positive antibodies in both serum and CSF (both 1:100). Therefore, the diagnosis of the anti-GAD65 antibodies related encephalitis was reached.
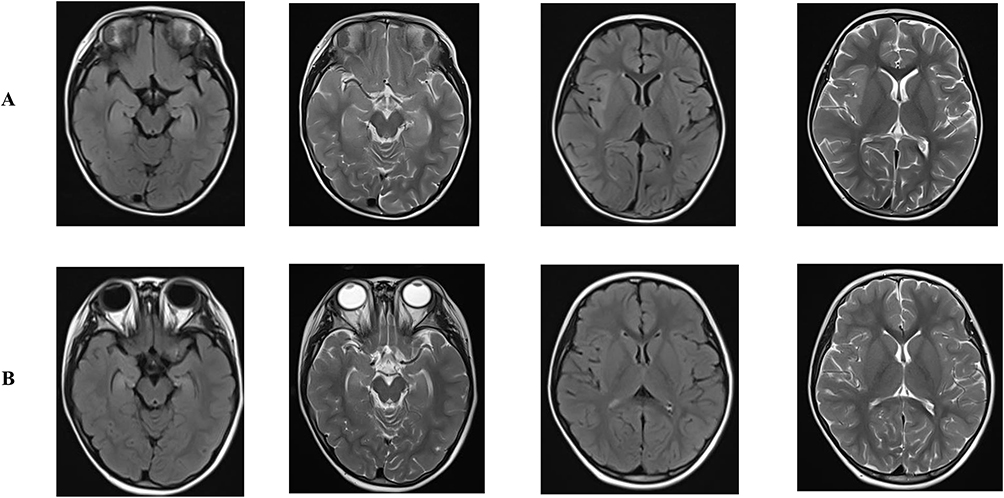 |
Figure 1 Brain magnetic resonance imaging (MRI) results. (A) The initial brain MRI taken on the 2nd month of the disease course; there is an increased intensity and edema in the bilateral hippocampi and right insular cortex. (B) The brain MRI taken at last follow up on the 22nd month of the disease course, the edema and lesions in the bilateral hippocampi and right insular cortex improved. |
 |
Figure 2 Electroencephalographic findings during the acute phase of the disease. (A) Background showing α rhythm in the occipital regions. (B) Typical inter-ictal discharges: bilateral multifocal sharp and spike-slow wave complexes of medium-high amplitude, more prominent in the right anterior region. (C–F) Compound consecutive figures showing one of the subclinical seizures: low-amplitude sharp wave bursts in the right anterior regions evolving into sharp slow wave complexes of medium-high amplitude bursts in the right hemisphere evolving to low-amplitude sharp and spike slow wave complexes bursts mainly in the right frontal and temporal regions with a duration of 81seconds. The arrows indicate the starting and ending of this subclinical seizure, respectively. |
After the admission to our hospital, she was given intravenous immunoglobulin (IVIG, 2g/kg in total) and intravenous methylprednisolone (IVMP pulse, 15 mg/kg/day for 5 continuous days), followed by oral prednisone (2 mg/kg/day) which was tapered off within the following six months. Levetiracetam (LEV) and other symptomatic treatments were prescribed. She got some relief; however, she still had experienced abnormal behavior (hyperactivity and poor cognition), occasional clinical seizures and frequent subclinical seizures according to the EEG monitoring. As a result, within the following 14 months, she took combined immunotherapies as described below. Monthly to bimonthly IVIG (2 g/kg, 10 times); rituximab (750 mg/m2 twice in 2 weeks interval shortly after the first IVIG plus IVMP pulse; 750 mg/m2 once, half a year later and 700 mg/m2 once, one year later). Besides, mycophenolate mofetil (MMF) was added shortly after the first round of rituximab since the improvement of the patient was not satisfactory; IVMP pulse was repeated again in the 9th month of treatment (15 mg/kg/day for five continuous days, which was followed by oral prednisone (1 mg/kg/d) and then tapered off within 1 month). Moreover, lacosamide (LCM) was added in the 14th month of treatment. Despite this long duration of repetitive and continuous aggressive therapies, she still presented with abnormal behavior (mostly hyperactivity), poor cognition and uncontrolled seizures (her EEG once became normal in the 7th month of the treatment but it became worse later with occasional clinical seizures and frequent subclinical seizures according to the EEG monitoring) (Figure 3A–F).
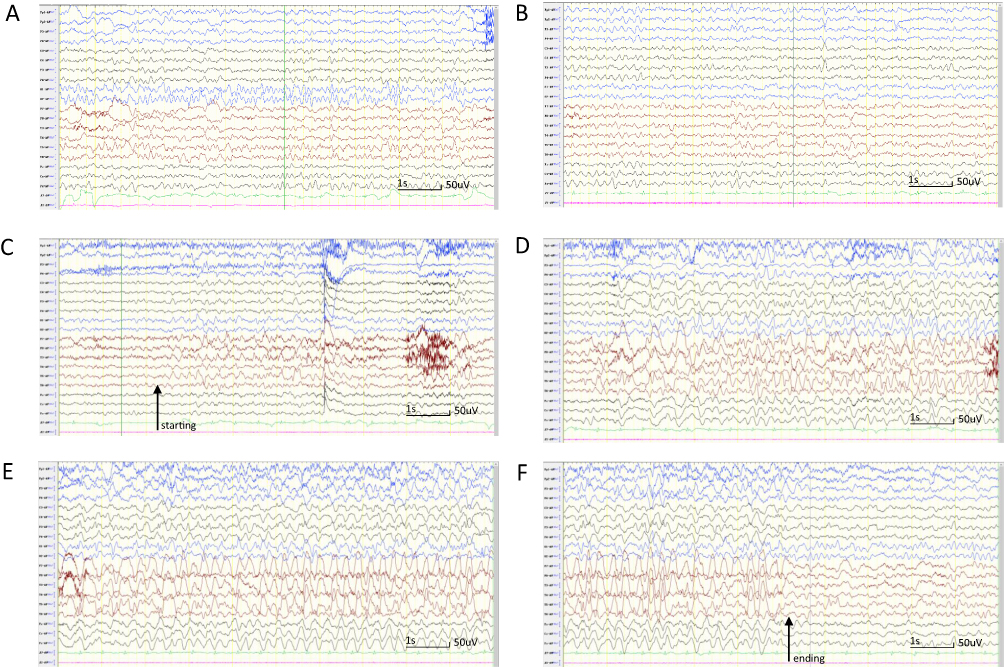 |
Figure 3 Electroencephalographic findings before tocilizumab treatment. (A) Background showing α rhythm in the occipital regions. (B) Typical inter-ictal discharges; multifocal sharp and spike-slow wave complexes prominent in the frontal and temporal lobes. (C–F) Compound consecutive figures showing one of the subclinical seizures: low-medium amplitude sharp or sharp-slow wave complex rhythms located in either left or right temporal regions, which spread to ipsilateral frontal region or hemisphere with a duration of 44 seconds. The arrows indicate the starting and ending of this subclinical seizure, respectively. |
In the 15th month of treatment, we gave her the first dose of tocilizumab (10 mg/kg), tapered off LCM due to the complained itchy rashes, added clobazam (CLB, 5mg bid) and repeated IVIG (1.5 g/kg in total) once. Her mental status improved obviously after the first dosage of the tocilizumab. Then in the following six months, we gave her another 5 cycles of tocilizumab (10–12 mg/kg), tapered down MMF, maintained the dosage of LEV and CLB and repeated IVIG (1 g/kg in total) once. Her cognition became better and better with the use of the tocilizumab, however, she got an upper respiratory tract infection once in between (after the 3rd cycle of tocilizumab) and regressed a little bit. We continued with tocilizumab and other therapies in the following months. At the end of the 20th month of treatment, she had no clinical seizures or subclinical seizures and the EEG was normal (Figure 4). In the 21st month of treatment, her behavior and cognition had improved significantly. Besides, brain MRI (Figure 1B) was improved too. She got mild side effects (upper respiratory tract infection and reduced Ig levels in the serum) after the third tocilizumab dose.
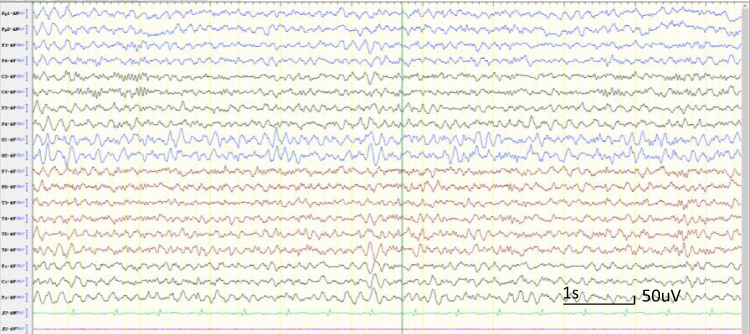 |
Figure 4 Electroencephalograph findings after 4 cycles of tocilizumab; the background with θ and α rhythm in the occipital regions without inter-ictal discharges. |
Written informed consent was obtained from the parents to have the case details and any accompanying image published and the study was approved by the ethical committee of Xiangya Hospital, Central South University according to the tenets of the Declaration of Helsinki. The institutional approval from the ethical committee of Xiangya Hospital, Central South University (approval number 202310892) was given to publish the case details.
Literature Review
A literature search was carried out in the PubMed. The key words for searching included: GAD AND (encephalitis OR epilepsy OR tocilizumab). Two published reports were retrieved.12,13 Two cases with anti-GAD antibodies encephalitis treated with tocilizumab have been reported so far. Thus, we now have three cases if we add our patient. All three cases were females and the mean age of seizure onset was 7.72 years. They all presented with refractory seizures including status epilepticus in two cases, and altered mental status. Two cases presented with ataxia. Anti-GAD autoantibodies were elevated in both the serum and CSF for all cases. Two cases had abnormal brain MRI findings. All three cases had tried several combined ASMs and immunotherapies before tocilizumab but patients remained with refractory AE. ASMs tried included LEV, LCM, CLB: clobazam, phenytoin (PHT), clonazepam (CZP), sodium valproate (VPA), midazolam (MDZ), topiramate (TPM), ketogenic diet (KD), perampanel, phenobarbital (PB), intravenous propofol and ketamine. Immunotherapies used included several cycles of long-term use of IVIG, IVMP, rituximab, plasma exchange (PE) and MMF. Following several cycles of the tocilizumab, all cases had significant improvement; seizure freedom (n=1), seizure control (n=2), improved-normal cognition (n=3), improved neuropsychiatry symptoms (n=2) and controlled ataxia (n=2). Table 1 summarizes the clinical data of our case and patients from the literature.
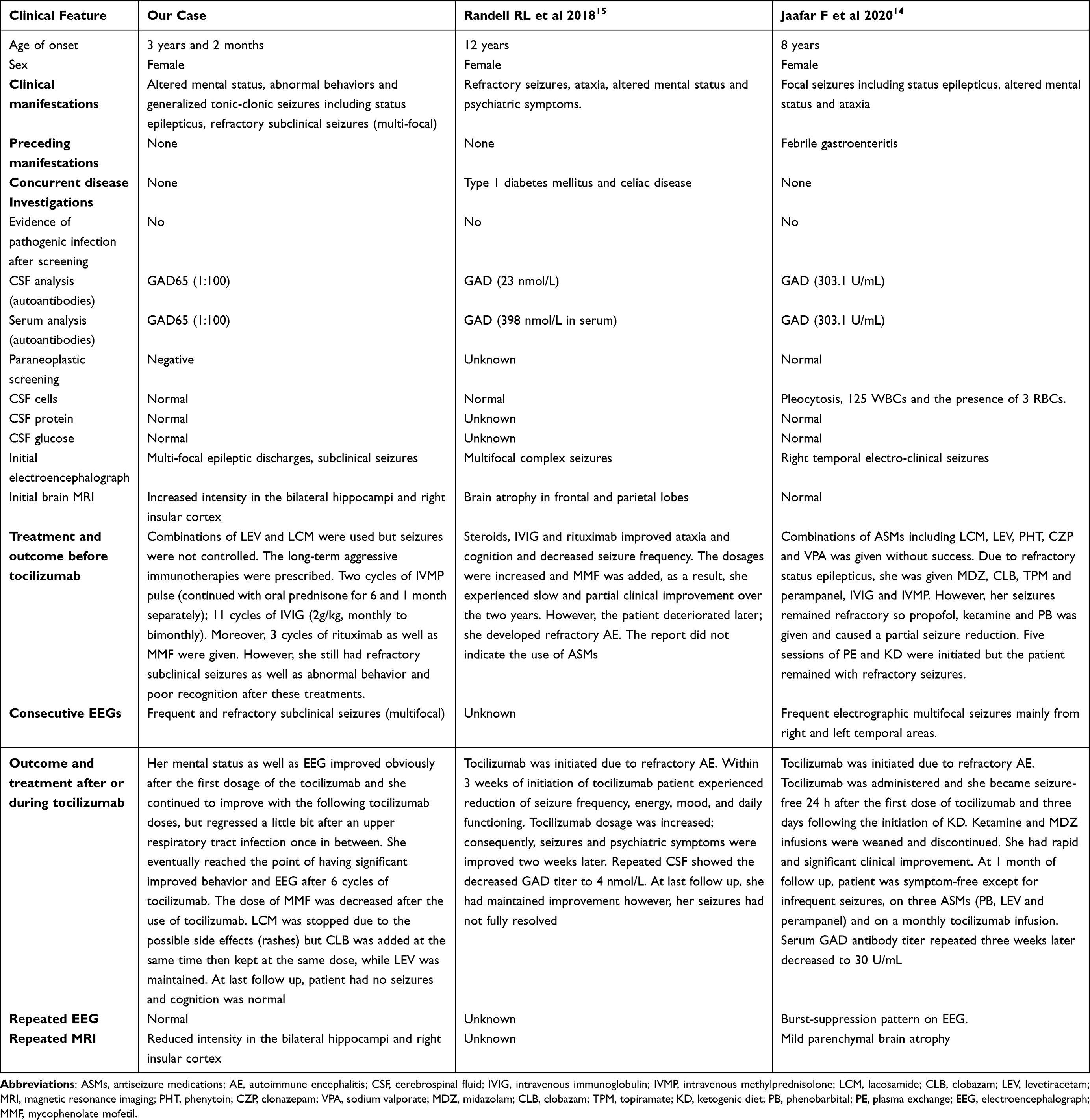 |
Table 1 Demographics, Clinical and Treatment Information of the Patients Before After Receiving Tocilizumab |
Discussion
Our patient along with the two previous reported cases14,15 provide more evidences that tocilizumab is effective and safe for the refractory anti-GAD antibodies related epilepsy. Our patient is the youngest in comparison to the other two. She presented with altered mental status and generalized tonic-clonic seizures, which started as status epilepticus, which is somehow similar to the presentation of one of the two reported cases.14 Likewise, other studies of the anti-GAD related epilepsy treated with other therapies unveiled that patients can present with epilepsia partialis continua and refractory status epilepticus.3 Prior to the use of tocilizumab, all three cases (including ours) received several combinations of ASMs, steroids and other immunotherapies, which led to temporary seizure control without improvement of other associated symptoms which concur with the current understanding of this condition.2,5,8–11 However, the introduction of the tocilizumab to all cases led to the quick control of seizures as well as improvement of cognition, neuropsychiatric symptoms and ataxia. Tocilizumab has been reported as an effective therapy for other types of the refractory autoimmune encephalitis (AE) including anti-CASPR2 encephalitis,16,17 anti-NMDAR encephalitis18 as well as anti-LGI1 encephalitis.19 In addition, there are some evidences that tocilizumab is effective to some refractory epileptic syndromes including new-onset refractory status epilepticus (NORSE)20–24 and febrile infection-related epilepsy syndrome (FIRES).25–27
Tocilizumab is an interleukin-6 (IL-6) inhibitor. IL-6 is a molecule produced by T cells and is vital for the modulation of the antibodies’ synthesis by B cells.28 Besides, IL-6 can also be produced by astrocytes and neurons29 and there is an evidence that high levels of the IL-6 in the brain can cause astrocytosis and neurodegeneration.30 It has been reported that that high serum anti-GAD65 antibodies titers do not associate with disease severity or response to therapies.2 However, the two previous reported cases14,15 treated with tocilizumab showed the reduction of the antibodies. It is unfortunate that we did not monitor the antibodies titer changes in our case since she recovered well. Currently, it is still unclear if anti-GAD65 antibodies are causative or only serve as a marker for AE induced by cytotoxic T cells,2 nevertheless, based on the reported two cases, we speculate them to be pathogenic. Although we could not check and monitor IL-6 levels in the serum and CSF, we speculate that this cytokine might play a role in the pathogenesis of this type of AE as evidenced by the improvement of the three cases following the use of tocilizumab. Notably, a recent report showed that elevated plasma IL-6 are related with high GAD titers in epileptic patients.31 Future studies are needed to explore the signaling pathways involved in the pathogenesis of anti-GAD65 related encephalitis connecting production of cytokines, chemokines and synthesis of autoantibodies. Epilepsy in children represents an important problem and is associated with significant morbidities such as cognitive impairment, mood disorders (anxiety and depression) and attention deficit/hyperactivity disorder.32,33 Therefore, it is crucial to identify therapies that can control seizures and minimize the comorbidities.
Conclusively, although anti-GAD65 antibodies related epilepsy is rare, it is a complex disease because it is difficult to manage even with multiple combinations of the ASMs, steroids and other immunotherapies. However, tocilizumab seems to be an effective therapy for the refractory anti-GAD65 related epilepsy as it can control seizures, improve cognition and neuropsychiatric symptoms. This case report supports the treatment with interleukin-6 inhibitors in similar cases of autoimmune encephalitis.
Study Limitations
We assessed our patient retrospectively hence; the study might be prone to the information bias. It is hard to tell the long-term outcome of the patient since we have followed her for a short period.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval and Consent to Participate
The study including all methods adhered to the tenets of the Declaration of Helsinki and received approval from the Institutional Review Board and Research Ethics Committee of Xiangya Hospital, Central South University, Changsha, Hunan. Written consent was obtained from the parents of the subject, which were approved by the Institutional Ethics Committee of Xiangya Hospital, Central South University.
Consent to Publication
The consent for publication was obtained from the parents of the subject.
Acknowledgments
We thank the participating patients and their families.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Natural Science Foundation of Hunan province 2021JJ40986.
Disclosure
None of the authors has any conflict of interest to disclose for this work.
References
1. McKeon A, Tracy JA. GAD65 neurological autoimmunity. Muscle Nerve. 2017;56(1):15–27. doi:10.1002/mus.25565
2. Li X, Guo Q, Zheng Z, Wang X, Liu S. Immune-mediated epilepsy with GAD65 antibodies. J Neuroimmunol. 2020;341:577189. doi:10.1016/j.jneuroim.2020.577189
3. Triplett J, Vijayan S, MacDonald A, et al. Fulminant Anti-GAD antibody encephalitis presenting with status epilepticus requiring aggressive immunosuppression. J Neuroimmunol. 2018;323:119–124. doi:10.1016/j.jneuroim.2018.06.013
4. Salman MS, Xu Q, Bunge M, Ilse W, Gerhold K, Udow SJ. Segmental Myoclonus and Epilepsy in a Child with GAD 65 Antibodies. Can J Neurol Sci Le J Can des Sci Neurol. 2022;49(1):136–139. doi:10.1017/cjn.2021.21
5. Daif A, Lukas RV, Issa NP, et al. Antiglutamic acid decarboxylase 65 (GAD65) antibody-associated epilepsy. Epilepsy Behav. 2018;80:331–336. doi:10.1016/j.yebeh.2018.01.021
6. Curia G, Lucchi C, Vinet J, et al. Pathophysiogenesis of mesial temporal lobe epilepsy: is prevention of damage antiepileptogenic? Curr Med Chem. 2014;21(6):663–688. doi:10.2174/0929867320666131119152201
7. Gualtieri F, Marinelli C, Longo D, et al. Hypoxia markers are expressed in interneurons exposed to recurrent seizures. Neuromolecular Med. 2013;15(1):133–146. doi:10.1007/s12017-012-8203-0
8. Saiz A, Blanco Y, Sabater L, et al. Spectrum of neurological syndromes associated with glutamic acid decarboxylase antibodies: diagnostic clues for this association. Brain. 2008;131(Pt 10):2553–2563. doi:10.1093/brain/awn183
9. Khawaja AM, Vines BL, Miller DW, Szaflarski JP, Amara AW. Refractory status epilepticus and glutamic acid decarboxylase antibodies in adults: presentation, treatment and outcomes. Epileptic Disord. 2016;18(1):34–43. doi:10.1684/epd.2016.0797
10. Serrano-Castro PJ, Rodríguez-Uranga JJ, Cabezudo-García P, et al. Cenobamate and Clobazam Combination as Personalized Medicine in Autoimmune-Associated Epilepsy With Anti-Gad65 Antibodies. Neurol Neuroimmunol Neuroinflam. 2023;10(6). doi:10.1212/NXI.0000000000200151
11. Li TR, Zhang YD, Wang Q, Shao XQ, Li ZM, Lv RJ. Intravenous methylprednisolone or immunoglobulin for anti-glutamic acid decarboxylase 65 antibody autoimmune encephalitis: which is better? BMC Neurosci. 2020;21(1):13. doi:10.1186/s12868-020-00561-9
12. Joubert B, Belbezier A, Haesebaert J, et al. Long-term outcomes in temporal lobe epilepsy with glutamate decarboxylase antibodies. J Neurol. 2020;267(7):2083–2089. doi:10.1007/s00415-020-09807-2
13. Chengyu L, Weixiong S, Chao C, et al. Clinical features and immunotherapy outcomes of anti-glutamic acid decarboxylase 65 antibody-associated neurological disorders. J Neuroimmunol. 2020;345:577289. doi:10.1016/j.jneuroim.2020.577289
14. Jaafar F, Haddad L, Koleilat N, Sharara-Chami R, Shbarou R. Super refractory status epilepticus secondary to anti-GAD antibody encephalitis successfully treated with aggressive immunotherapy. Epilepsy Behav Rep. 2020;14:100396. doi:10.1016/j.ebr.2020.100396
15. Randell RL, Adams AV, Van Mater H. Tocilizumab in Refractory Autoimmune Encephalitis: a Series of Pediatric Cases. Pediatr Neurol. 2018;86:66–68. doi:10.1016/j.pediatrneurol.2018.07.016
16. Krogias C, Hoepner R, Müller A, Schneider-Gold C, Schröder A, Gold R. Successful treatment of anti-Caspr2 syndrome by interleukin 6 receptor blockade through tocilizumab. JAMA Neurol. 2013;70(8):1056–1059. doi:10.1001/jamaneurol.2013.143
17. Benucci M, Tramacere L, Infantino M, et al. Efficacy of Tocilizumab in Limbic Encephalitis with Anti-CASPR2 Antibodies. Case Rep Neurol Med. 2020;2020:5697670. doi:10.1155/2020/5697670
18. Zhang YX, Cai MT, Li EC, Xu YF. Efficacy of tocilizumab in anti- N -methyl-d-asparate receptor encephalitis with Graves’ hyperthyroidism and positive anti-glial fibrillary acidic protein antibodies. CNS Neurosci Ther. 2022;28(11):1898–1900. doi:10.1111/cns.13949
19. Jang S, Kim SY, Kim WJ, Chae JH, Kim KJ, Lim BC. A case of pediatric anti-leucine-rich glioma inactivated 1 encephalitis with faciobrachial dystonic seizure. Brain Dev. 2023;45(6):348–353. doi:10.1016/j.braindev.2023.02.003
20. Jun JS, Lee ST, Kim R, Chu K, Lee SK. Tocilizumab treatment for new onset refractory status epilepticus. Ann Neurol. 2018;84(6):940–945. doi:10.1002/ana.25374
21. Kwack DW, Kim DW. The Increased Interleukin-6 Levels Can Be an Early Diagnostic Marker for New-Onset Refractory Status Epilepticus. J Epilepsy Res. 2022;12(2):78–81. doi:10.14581/jer.22015
22. Wadayama T, Shimizu M, Yata T, et al. Cryptogenic new-onset refractory status epilepticus responded to anti-interleukin-6 treatment. J Neuroimmunol. 2022;363:577789. doi:10.1016/j.jneuroim.2021.577789
23. Nakamura Y, Ueda M, Kodama S, et al. Treatment of Cryptogenic New-onset Refractory Status Epilepticus (C-NORSE) with Tocilizumab. Intern Med. 2024;63(24):3377–3382. doi:10.2169/internalmedicine.3392-23
24. Donnelly JP, Kasatwar N, Hafeez S, et al. Resolution of cryptogenic new onset refractory status epilepticus with tocilizumab. Epilepsy Behav Rep. 2021;15:100431. doi:10.1016/j.ebr.2021.100431
25. Wan L, Liu J, Wang J, et al. Favorable outcomes and FDG-PET changes following tocilizumab treatment for febrile infection-related epilepsy syndrome in a child. Int Immunopharmacol. 2025;146:113872. doi:10.1016/j.intimp.2024.113872
26. Cantarín-Extremera V, Jiménez-Legido M, Duat-Rodríguez A, et al. Tocilizumab in pediatric refractory status epilepticus and acute epilepsy: experience in two patients. J Neuroimmunol. 2020;340:577142. doi:10.1016/j.jneuroim.2019.577142
27. Aledo-Serrano A, Hariramani R, Gonzalez-Martinez A, et al. Anakinra and tocilizumab in the chronic phase of febrile infection-related epilepsy syndrome (FIRES): effectiveness and safety from a case-series. Seizure. 2022;100:51–55. doi:10.1016/j.seizure.2022.06.012
28. Choy EH, De Benedetti F, Takeuchi T, Hashizume M, John MR, Kishimoto T. Translating IL-6 biology into effective treatments. Nat Rev Rheumatol. 2020;16(6):335–345. doi:10.1038/s41584-020-0419-z
29. Ma J, Zhang FL, Zhou G, Bao YX, Shen Y, Qian ZM. Different Characteristics of Hepcidin Expression in IL-6+/+ and IL-6-/- Neurons and Astrocytes Treated with Lipopolysaccharides. Neurochem Res. 2018;43(8):1624–1630. doi:10.1007/s11064-018-2577-9
30. Garbers C, Heink S, Korn T, Rose-John S. Interleukin-6: designing specific therapeutics for a complex cytokine. Nat Rev Drug Discov. 2018;17(6):395–412. doi:10.1038/nrd.2018.45
31. Basnyat P, Peltola M, Raitanen J, et al. Elevated IL-6 plasma levels are associated with GAD antibodies-associated autoimmune epilepsy. Front Cell Neurosci. 2023;17:1129907. doi:10.3389/fncel.2023.1129907
32. Operto FF, Pastorino GMG, Viggiano A, et al. Epilepsy and Cognitive Impairment in Childhood and Adolescence: a Mini-Review. Curr Neuropharmacol. 2023;21(8):1646–1665. doi:10.2174/1570159X20666220706102708
33. Wei SH, Lee WT. Comorbidity of childhood epilepsy. J Formos Med Assoc. 2015;114(11):1031–1038. doi:10.1016/j.jfma.2015.07.015
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Relative Safety and Efficacy of Two Doses of Tandospirone Citrate for Generalized Anxiety Disorder: A Multicenter Randomized Controlled Trial
Li Q, Zhang H, Lin G, Shi S, Zhang Y, Ji J, Yang L, Yao J, Wu W
Neuropsychiatric Disease and Treatment 2022, 18:1653-1664
Published Date: 8 August 2022
Biosimilars: Science, Implications, and Potential Outlooks in the Middle East and Africa
Batran RA, Elmoshneb M, Hussein AS, Hussien OM, Adel F, Elgarhy R, Morsi MI
Biologics: Targets and Therapy 2022, 16:161-171
Published Date: 6 October 2022
Clinical Evaluation of Risankizumab in the Treatment of Adults with Moderately to Severely Active Crohn’s Disease: Patient Selection and Reported Outcomes
Horst S, Cross RK
Drug Design, Development and Therapy 2023, 17:273-282
Published Date: 31 January 2023
Clinical Analysis of Lacosamide Monotherapy in the Treatment of Self-Limited Epilepsy with Centrotemporal Spikes
Feng J, Zhang L, Tang J, Zhang B, Xiao X, Shi X
Neuropsychiatric Disease and Treatment 2024, 20:459-467
Published Date: 4 March 2024
The Effectiveness and Safety of Acupuncture for Mammary Hyperplasia: A Systematic Review and Meta-Analysis
Li J, Zhang D, Hu J, Cui J, Mansoor KM
Journal of Pain Research 2024, 17:1761-1772
Published Date: 17 May 2024