Back to Journals » Breast Cancer: Targets and Therapy » Volume 18
Advancing Germline Genetic Testing for Breast Cancer in Resource-Restricted Settings: Evidence, Barriers, and a Practical Roadmap for Implementation
Authors Abdel-Razeq H ![]()
Received 18 April 2026
Accepted for publication 18 June 2026
Published 24 June 2026 Volume 2026:18 618067
DOI https://doi.org/10.2147/BCTT.S618067
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Harikrishna Nakshatri
Hikmat Abdel-Razeq1,2
1Department of Internal Medicine, King Hussein Cancer Center, Amman, 11941, Jordan; 2School of Medicine, The University of Jordan, Amman, 11942, Jordan
Correspondence: Hikmat Abdel-Razeq, Department of Internal Medicine, King Hussein Cancer Center, Amman, 11941, Jordan, Tel +962 6 530 0460, Ext: 1000, Email [email protected]
Abstract: Germline genetic testing (GGT) is increasingly integrated in breast cancer management, yet its implementation, particularly in resource-restricted settings, remains a challenge. This narrative review addresses current evidence and international guideline recommendations regarding GGT in breast cancer, with emphasis on clinical utility, evolving testing criteria and implementation challenges, drawing partly on the experience and demographic characteristics of Jordan as an example of a resource-restricted setting. Approximately 10% of patients with breast cancer carry germline pathogenic variants, mostly involving BRCA1 and BRCA2. GGT guides systemic therapy including PARP inhibitors, informs surgical decisions and enables cascade testing for at-risk relatives to support prevention and early detection. Recent guideline updates from major international societies have expanded eligibility, with recommendations supporting testing up to age 65 and some advocating universal testing. In low- and middle-income countries, these expanded criteria render a large proportion of patients eligible but raise concerns regarding infrastructure, cost and variant of uncertain significance (VUS) interpretation. While expanded testing increases detection of actionable variants and may improve outcomes, universal GGT remains controversial, and context-adapted strategies are required to balance benefit, feasibility, and sustainability. Overall, integrating GGT into routine breast cancer care represents a key component of precision oncology and hereditary cancer prevention strategies worldwide, especially in early-onset disease populations. Implementation requires multidisciplinary coordination and equitable access to testing services.
Keywords: breast cancer, genetic testing, genetic counselling, BRCA1, BRCA2, resource-restricted countries
Introduction
Breast cancer continues to be the most common cancer diagnosed in women worldwide and remains a leading cause of cancer-related deaths.1 While most breast cancer cases are sporadic with environmental and lifestyle factors contribute significantly to its prevalence, genetic mutations in cancer predisposing genes contribute to 5–15% of newly-diagnoses cases.2,3
The discovery of pathogenic variants in high-risk genes like BRCA1 and BRCA2 has revolutionized the understanding of breast cancer genetics. These alterations significantly increase the lifetime risk of breast cancer, making them key targets for early screening, prevention, and personalized therapy.4
Identification of specific genetic mutations allows clinicians to tailor preventive and therapeutic strategies, such as the use of poly (ADP-ribose) polymerase (PARP) inhibitors for BRCA1/2-mutated cancers or risk-reducing surgeries including bilateral salpingo-oophorectomy and contralateral mastectomy.5–7 Preventive measures can also be extended to at-risk family members who may carry the same genetic alterations that predispose them to the similar risk of inherited cancers including, but not limited to, breast and ovarian cancers.
However, despite the potential advantages of genetic testing, its implementation remains limited in low- and middle-income countries (LMICs), where shortage of genetic counseling professionals, infrastructure limitations and resource constraints pose substantial barriers to widespread adoption.8
Many international professional societies have issued guidelines on when, how and whom to test for germline mutations. The National Comprehensive Cancer Network (NCCN) guidelines are widely used in daily practice,9 however, these guidelines are a little complex and frequently updated, making adherence a challenge. More recently, The American society of Clinical Oncology (ASCO) has expanded testing to include all breast cancer patients aged 65 years or younger,10–12 while the American Society of Breast Surgeon recommends genetic testing for all patients with breast cancer, regardless of age or other risk factors.13,14
This review aims to evaluate the evidence supporting expanded and universal germline genetic testing in breast cancer while critically examining the unique challenges faced by resource-restricted healthcare systems. Emphasis is placed on financial constraints, workforce limitations, laboratory infrastructure, management of variants of uncertain significance, access to downstream interventions, and implementation strategies relevant to LMICs. In addition, we propose a practical phased framework that may facilitate the gradual transition from guideline-based testing toward broader and potentially universal testing as local resources and infrastructure evolve.
Methods
We conducted a literature search using multiple scientific databases, including Scopus, PubMed, and Google Scholar. We searched for published research between 1990 and 2025, using the following keywords: Universal germline genetic testing, Lower middle-income countries, Low-income countries, LMIC, resource restricted countries, BRCA1, BRCA2, carrier, prophylactic mastectomy, risk-reducing surgery, oophorectomy, surveillance and bilateral salpingo-oopherectomy (BSO). Articles were considered for inclusion if they were published in peer-reviewed journals, written in English and relevant to germline genetic testing. Titles and abstracts were screened for relevance to breast cancer germline genetic testing, implementation strategies, clinical utility, health-economic analyses, genetic counseling delivery models, and healthcare system integration. Particular emphasis was placed on studies originating from LMICs or addressing resource-restricted settings. Such studies were identified through targeted searches incorporating geographic descriptors and LMIC-specific terminology. When direct evidence from LMICs was unavailable, evidence from high-income countries was included and critically appraised for transferability. Findings were synthesized narratively and organized into thematic domains relevant to implementation of germline testing programs in resource-constrained environments.
Data was extracted from selected studies including study design, sample size, main findings, and methodologies. Data were then synthesized into common themes, allowing for a comparison across different research efforts.
Our review is subject to certain limitations, including the possibilities of language bias (only English-language papers were included), publication bias, and excluding non-peer-reviewed sources.
Genetic Basis of Breast Cancer
Breast cancer is a heterogeneous disease influenced by both environmental and genetic factors. Breast cancer cases may also be attributed to inherited mutations in high-penetrance genes such as BRCA1 and BRCA2, which are tumor suppressor genes that, when mutated, significantly increase the risk of developing breast and ovarian cancers.15,16 Other genes, such as ATM, PALB2, TP53, and CHEK2, have also been identified as playing roles in hereditary breast cancer risk.17,18
BRCA1 and BRCA2 mutations increase the risk of breast cancer through their role in maintaining the integrity of DNA. These genes are known as tumor suppressor genes, meaning they normally help prevent the formation of tumors by repairing damaged DNA. Specifically, BRCA1 and BRCA2 are involved in the repair of double-strand DNA breaks through a process called homologous recombination repair (HRR).19 When either of these genes are mutated, this repair mechanism becomes faulty, allowing for the accumulation of genetic mutations in critical regions of the genome. This accumulation of mutations can lead to uncontrolled cell growth and, over time, cancer.20,21 In individuals with inherited BRCA1/2 mutations, the risk of having breast cancer is significantly higher because the defective gene is present in all cells. For women with a BRCA1/2 mutation, the lifetime risk of developing breast cancer can be as high as 70%, much greater than the risk of the general population (about 12%).22 The mutations also increase the risk of other cancers, such as ovarian, prostate and pancreatic cancer.23
Clinical Implications of Germline Genetic Testing
The clinical benefits of diagnosing germline pathogenic variants in patients with breast cancer are numerous. The presence of a BRCA1 or BRCA2 mutation may lead to recommendations for risk-reducing surgeries, such as mastectomy or oophorectomy, to reduce the risk of developing additional cancers.24,25 Additionally, patients with these mutations may benefit from therapies targeting DNA repair mechanisms, such as PARP inhibitors, which have shown promise in clinical trials for patients with BRCA-mutated breast cancers.26 Moreover, knowing genetic risk allows healthcare providers to offer personalized surveillance strategies, such as more frequent mammograms or MRI screening, to detect cancer at an earlier stage.27
Beyond the individual patient, genetic testing has profound implications for the family members of those tested. Identifying a pathogenic mutation in a patient can have cascading effects, as relatives may also be at risk. Genetic counseling and testing can help at-risk family members make informed decisions regarding their own cancer prevention strategies, ultimately improving overall health outcomes in these families.28
PARP Inhibitors
The OlympiA trial has demonstrated that patients with early-stage, Human Epidermal growth factor Receptor-2 (HER2)-negative breast cancer who have germline BRCA1 or BRCA2 pathogenic variants and are at high risk of recurrence benefit significantly from adjuvant therapy olaparib, a PARP inhibitor. This patient population showed improved invasive disease-free survival (iDFS) and distant disease-free survival (dDFS) when treated with olaparib compared to placebo, following the completion of local treatment and adjuvant or neoadjuvant chemotherapy.29 Olaparib was associated with a 3-year iDFS rate of 85.9% compared to 77.1% in the placebo group, with a hazard ratio of 0.58, indicating a 42% reduction in the risk of invasive disease or death. Additionally, the trial reported a significant improvement in overall survival (OS) with a hazard ratio of 0.68, further supporting the benefit of olaparib in this high-risk group.30 The study was updated recently with similar promising outcomes.31,32
Olaparib and talazoparib, another PARP inhibitor, were also tested in patients with HER2-negative metastatic breast cancer (MBC) who harbor germline BRCA1/2 mutations. Both drugs have demonstrated significant improvements in PFS and OS compared to standard chemotherapy options. The OlympiAD trial, a pivotal phase-3 randomized trial, compared olaparib with standard chemotherapy (eribulin, capecitabine, or vinorelbine) in patients with HER2-negative MBC and germline BRCA mutations. The trial showed that olaparib significantly prolonged median PFS (7.0 months vs. 4.2 months) and improved response rates (59.9% vs. 28.8%) compared to chemotherapy, with a hazard ratio (HR) for progression or death of 0.58.33–35 Additionally, olaparib was associated with a lower incidence of grade 3 or higher adverse events compared to chemotherapy, and it improved health-related quality of life measures.
The EMBRACA trial, another phase-3 study, evaluated talazoparib in a similar patient population and also demonstrated a meaningful PFS benefit over standard chemotherapy.36 These findings support the use of PARP inhibitors as a standard treatment option for patients with BRCA1/2-mutated metastatic breast cancer.37,38
Current International Guidelines
International guidelines for germline genetic testing (GGT) testing in breast cancer emphasize the importance of genetic testing for individuals with a family or personal history suggestive of hereditary breast and ovarian cancer syndromes. The guidelines from various organizations provide specific criteria for when GGT testing should be considered:
NCCN Guidelines
The NCCN guidelines for germline genetic testing are based on age, gender, ancestry, tumor pathology and family history. All patients who are 50 years or younger, regardless of their family or personal history, all male patients and all Ashkenazi Jewish breast cancer patients to be tested. Several other recommendations are based on breast cancer pathology like those with triple negative disease and those with lobular breast cancer with personal or family history of diffuse gastric cancer. Additionally, patients at any age with significant family history of breast, ovarian, pancreatic or metastatic/high-risk prostate cancer are recommended to be tested (Table 1).9
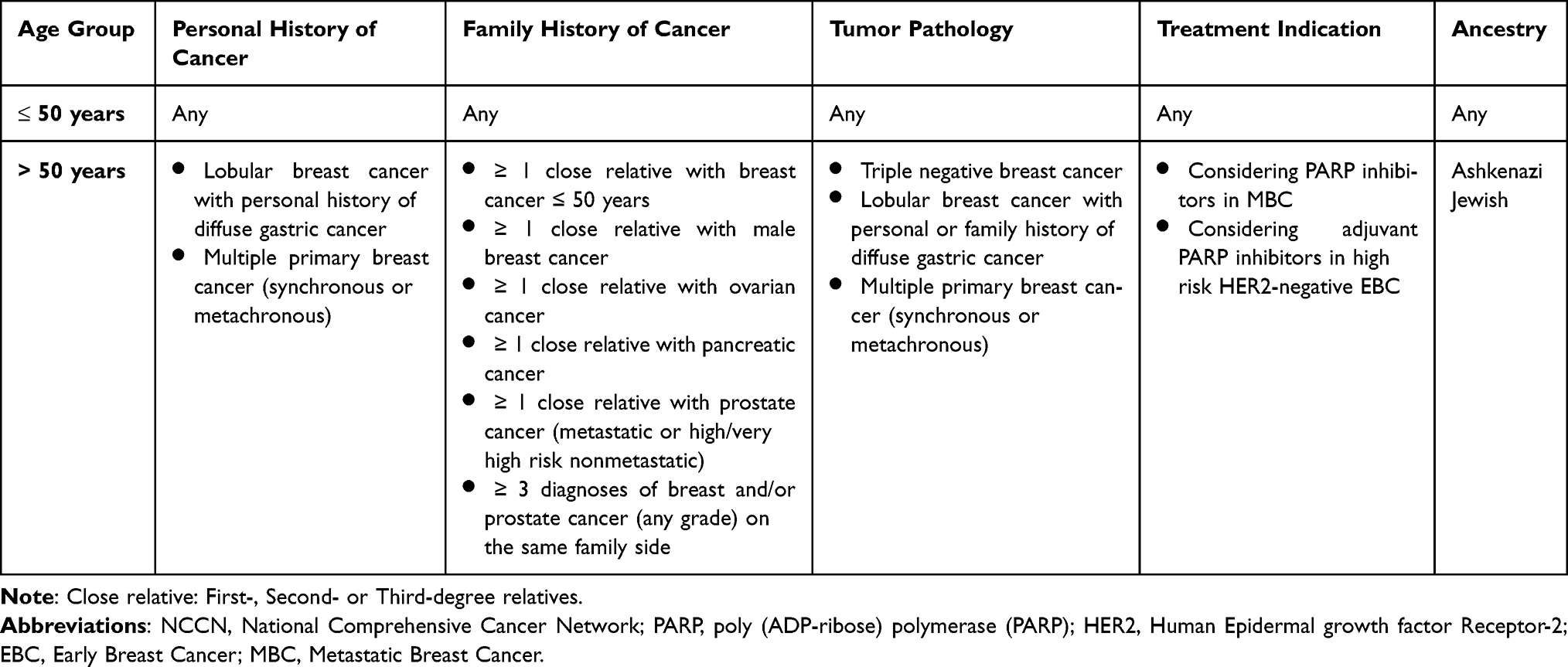 |
Table 1 Summary of NCCN Guidelines for Germline Genetic Testing |
National Institute for Health and Care Excellence (NICE), United Kingdom
NICE guidelines recommend genetic testing in specialty genetic clinics to individuals with breast or ovarian cancer if their combined BRCA1 and BRCA2 mutation carrier probability ≥ 10%. They also suggest that families with one relative with ovarian cancer on the same side of the family should be referred to a specialist genetic clinic.39
The American Society of Breast Surgeons (ASBrS)
Since 2019, the American Society of Breast Surgeon recommends genetic testing for all women with breast cancer, irrespective of age or other risk factors, to increase the identification of pathogenic variants that could influence treatment and management decisions.13,40 This approach aims to address the limitations of traditional criteria, such as those from the NCCN, which may miss a significant number of patients with PVs.
The American Society of Clinical Oncology-Society of Surgical Oncology (ASCO-SSO)
These guidelines, which were recently updated, suggest a more targeted approach, recommending BRCA1 and BRCA2 testing for all patients newly diagnosed with breast cancer who are 65 years or younger, particularly if the results will inform personal risk management or family risk assessment. This age-based criterion is designed to balance the benefits of genetic testing with considerations of cost-effectiveness and the potential for identifying VUS.10 These guidelines reflect differing perspectives on the scope of genetic testing, with the ASBrS advocating for a universal approach and the ASCO-SSO supporting age-based criteria to optimize the clinical utility of GGT in breast cancer management.
Challenges to Universal Genetic Testing in Resource-Restricted Countries
While germline genetic testing offers clear clinical advantages, the widespread implementation of this practice in resource-limited settings is not without challenges. These challenges range from financial constraints to insufficient healthcare infrastructure and the lack of genetic counseling services. Strategies to overcome some of these challenges are summarized below:
- Global collaboration and funding
- Partnership between institutions, governmental and non-governmental organizations (NGOs)
- Global funding initiatives
- Grants for genetic research and testing
- Establishment of subsidized insurance programs or special funds
- Active contribution of manufactures of genetic tests or international laboratories to low-income countries
- Capacity Building and Training
- Educate and train healthcare providers
- Incorporating genetic education into medical training
- Create regional genetic centers of excellence
- Technological Innovation
- Develop rapid, accurate and affordable genetic tests
- Use digital platforms to facilitate telemedicine consultations and remote genetic counseling
- Mobile health initiatives
- Education and community outreach
- Increase public awareness
- Community outreach programs
Economic Barriers
High cost of genetic tests remains one of the major obstacles to its widespread adoption in LMICs. Advanced genetic testing, particularly for multiple gene panels, can be prohibitively expensive for patients, at-risk relatives and healthcare systems. While genetic testing in high-income countries may be covered by insurance or publicly funded healthcare systems, the lack of such financial support in many LMICs means that only a small proportion of patients can access testing. Furthermore, the cost of follow-up care, including counseling and subsequent treatment, adds significantly to the financial burden for patients in these countries.41,42
One study attempted to estimate the incremental lifetime effects and cost-effectiveness of multigene testing of all unselected breast cancer patients (strategy A), compared with the current practice of genetic testing based on clinical criteria or family history (Strategy B). The study was conducted in in United Kingdom (UK) and US populations. Data were obtained from almost 12,000 patients in population-based BC cohorts. All breast cancer patients in strategy A underwent BRCA1/BRCA2/PALB2 testing. In strategy B, only eligible patients for testing based on family history or clinical criteria underwent genetic testing. Patients with BRCA/PALB2 pathogenic variants could undertake contralateral preventive mastectomy while BRCA carriers could choose risk-reducing salpingo-oophorectomy (RRSO). The cost analysis also factored cascaded testing for relatives of affected patients along with associated risk reducing strategy including surveillance with magnetic resonance imaging (MRI) or mammography screening, chemoprevention, or risk-reducing mastectomy and RRSO. This study concludes that unselected, high-risk multigene testing for all patients with BC, regardless of their personal or family history, to be extremely cost-effective compared with testing based on FH or clinical criteria for UK and US health systems. These findings support changing current policy to expand genetic testing to all women with BC.43 Other investigators have looked into the cost effectiveness of population-based testing which will not be detailed here since we do not endorse it.44,45
Healthcare Infrastructure
In many low-resource settings, healthcare infrastructure remains underdeveloped, and this lack of infrastructure impedes the effective implementation of genetic testing. Genetic testing requires specialized laboratory facilities and trained personnel to perform and interpret the tests. Unfortunately, in many LMICs, such laboratory infrastructure is either inadequate or nonexistent. Moreover, even in countries where testing services exist, these services may be concentrated in urban centers, making access difficult for individuals living in rural areas.46
Additionally, the shortage of healthcare professionals with expertise in genetics exacerbates the problem. Genetic counseling, which is essential for explaining test results and their implications to patients, is often unavailable. Without adequate counseling, patients may be unable to fully comprehend the meaning of their test results or make informed decisions regarding their healthcare options.47,48
Cultural and Ethical Considerations
The cultural context in which genetic testing is introduced also plays a significant role in its acceptance and utilization. In some societies, genetic testing may be met with skepticism or fear due to misconceptions about genetics, the potential for discrimination, or concerns about the stigma associated with knowing one’s genetic risk. For example, individuals in certain cultures may be reluctant to undergo genetic testing because they fear that a positive result could lead to stigmatization or reduced social standing.49
Ethical dilemmas also arise in the context of genetic testing, particularly in how to manage the information obtained. Genetic testing can reveal incidental findings, such as variants of uncertain significance or mutations linked to other conditions, which may complicate decision-making. Furthermore, genetic information is not only relevant to the individual being tested but also to their family members, raising concerns about the privacy and confidentiality of genetic data.50
Variants of Uncertain Significance (VUS)
Variants of Uncertain Significance (VUS) are genetic variants identified through genetic testing that cannot be classified as benign or pathogenic. A VUS might be identified in genes known to be associated with a specific cancer, but there is not enough evidence to confirm whether such variants contribute to the disease.51 Rates of VUS varied with population tested, significantly higher with expanded panels and indications for testing.52 Dealing of patients with VUS should be done with extreme caution as these variants are not clinically actionable and as such should not alter clinical management based on the VUS result alone. Patients and relatives should be informed that VUS may be reclassified over time, and periodic follow-up is necessary to reassess the variant’s classification.53
Genetic counseling plays a vital role in managing VUS, as it helps patients understand the implications of their genetic test results and the potential for reclassification. Family history and other risk factors should guide clinical decisions rather than the VUS itself.54
Efforts to improve the interpretation of VUS include subclassifying them based on the likelihood of pathogenicity and conducting routine family-based evaluations. These strategies aim to mitigate the potential harms associated with VUS, such as unnecessary treatments and psychological distress.52
In the context of hereditary cancer, studies have shown that individuals with VUS do not typically undergo inappropriate clinical management compared to those with pathogenic variants. However, there is a need for appropriate counseling to make sure that patients understand the non-actionable nature of VUS and the importance of follow-up.55
Overall, the management of VUS requires a balanced approach that incorporates genetic counseling, consideration of family history, and ongoing re-evaluation of the variant’s classification as more data becomes available.
Population Demographics
Jordan exhibits a distinct demographic profile compared to that of the Western societies, as reflected in their population pyramids. Jordan’s population pyramid is characterized by a broad base, indicating a high proportion of young individuals, with 31.2% under 15 years of age. As of 2023, less than 5% of Jordan’s population is aged 65 and above.56 In comparison, the United States has a higher proportion of elderly individuals, with over 18% of its population is ≥ 65 years.57 This youthful demographic structure suggests a high fertility rate and a growing population. Conversely, the United States, as an example, has a more uniform population distribution, with a median age of 38.9 years, reflecting a more balanced age structure and a lower fertility rate. These differences are further highlighted by life expectancy figures; in 2023, Jordan’s life expectancy is 78.0 years, while the United States has a higher life expectancy of 79.76 years. Additionally, Jordan’s birth rate stands at 21.62 births per 1000 people, significantly higher than the US rate of 11.00 births per 1000 people. These demographic disparities are influenced by various factors, including healthcare systems, economic conditions, and cultural norms.58
Strategies to Overcome Barriers to Universal Genetic Testing
Challenges to universal genetic testing do exist. However, several strategies may help overcome these challenges and barriers and make genetic testing more accessible in resource-restricted settings.
Global Collaboration and Funding
International partnerships between healthcare institutions, governmental and non-governmental organizations (NGOs), and the private sector are essential to address the economic barriers to genetic testing in LMICs. Global funding initiatives, such as grants for genetic research and testing programs, could help subsidize the costs of genetic testing. By pooling resources and expertise, international collaborations could establish sustainable genetic testing programs that increase access for patients in underserved areas. King Hussein Cancer Center can be a model to follow in this regard.59,60 Our cancer genetics program was launched after we secured several research grants to help fund germline genetic testing and counselling.61–63
The establishment of subsidized insurance programs or a special fund that can cover the cost of testing, counselling and risk-reducing strategies can reduce the financial burden on patients and ensure that testing is available to those who need it most. Additionally, multinational firms that manufacture genetic tests or international laboratories that perform testing may be encouraged to reduce their prices in LMICs to improve accessibility.64
Technological Innovation
The development of affordable, rapid, and accurate genetic testing technologies holds great promise for improving access to genetic screening. Recent advances in next-generation sequencing (NGS) have dramatically reduced the cost of testing, making it more affordable for LMICs to incorporate genetic screening into their healthcare systems. NGS can simultaneously analyze multiple genes in a single test, enabling comprehensive testing at a fraction of the cost of traditional sequencing methods.65,66
Furthermore, the use of platforms to enable telemedicine consultations and remote genetic counseling could improve accessibility for patients in rural or remote areas.67 Mobile health initiatives that offer genetic education, counseling, and even remote testing could also increase access to genetic services in under-resourced regions.68
Education and Community Outreach
Increasing public understanding and awareness of the benefits of germline genetic testing is crucial in overcoming cultural and societal barriers. Community outreach programs that educate individuals about genetic risk factors for breast cancer, the benefits of early detection, and the options available for prevention and treatment can help reduce stigma and encourage greater acceptance of genetic testing. These programs should also involve healthcare providers, ensuring that they have the skills and knowledge necessary to educate their patients.69
Moreover, incorporating genetic education into medical training can help healthcare professionals understand the value of genetic testing and how to effectively integrate it into clinical practice.
Capacity Building and Training
Building local capacity is critical for ensuring the sustainability of genetic testing programs. This includes training local healthcare professionals, such as genetic counselors, laboratory technicians, and clinicians, to effectively conduct genetic testing and interpret the results.70 Additionally, creating regional genetic centers of excellence that can provide training, guidance, and resources to surrounding areas can help distribute expertise throughout the country.71
In countries with limited resources, it may also be beneficial to develop tiered models of genetic testing, where basic testing is available to a broad population, and more advanced testing is available in specialized centers. This approach would help ensure that even those in low-resource areas could benefit from genetic testing, while still providing the opportunity for advanced genetic screening when necessary.
Ethical and Legal Considerations in Genetic Testing
Informed Consent
Informed consent is very essential for ethical genetic testing, and it is crucial that patients fully understand the potential benefits, risks, and limitations of testing.72 In LMICs, where literacy levels and access to health education may vary, informed consent procedures must be tailored to ensure that patients comprehend the information provided.73–75 This could involve the use simplified language, visual aids and culturally sensitive communication strategies.76,77
Genetic Discrimination
In many countries, genetic data may be used inappropriately for discriminatory purposes, such as denying individuals access to insurance or employment.78,79 The potential for genetic discrimination makes it essential for countries to enact strong legal protections to prevent misuse of genetic data.80 Laws that prohibit discrimination based on genetics, such as the Genetic Information Nondiscrimination Act (GINA) in the United States, should be considered as models for countries seeking to introduce genetic testing programs.81 Canada passed the Genetic Non-Discrimination Act (GNA) in 2017, which is quite similar to GINA.82 It prohibits discrimination based on genetic test results in the areas of employment, insurance, and other areas of public life. This legislation ensures that individuals are not compelled to undergo genetic testing and cannot be discriminated against based on their genetic information.83
Several Western countries have enacted laws or policies that aim to protect individuals from discrimination based on genetic information, similar to GINA act in the United States.84 Although not specifically targeted at genetic information, the General Data Protection Regulation (GDPR), which regulates data privacy in the EU, includes provisions that protect sensitive information including genetic data.85,86 The regulation classifies genetic data as a special category of personal data, and its processing is subject to strict conditions. This offers a level of protection for genetic information, including against discrimination based on that data.85
In Jordan, there are growing discussions about bioethics and genetic counseling within medical practice.87 Ethical guidelines in medicine, particularly in genetic counseling, aim to ensure that genetic information is used responsibly and not to discriminate against individuals based on their genetic test results.88 While there is no dedicated law in Jordan that mirrors GINA specifically, there are a range of legal protections that might offer indirect safeguards against genetic discrimination, especially in terms of broader anti-discrimination provisions, privacy protections for sensitive medical data, and ethical medical practices.89 However, the legal framework could benefit from more specific legislation addressing genetic information and its potential misuse in areas such as employment and insurance.90
Privacy and Confidentiality
Genetic data is deeply personal, and patients must be assured that their genetic information will be protected. Data security protocols must be established to safeguard genetic information from unauthorized access or misuse. This is particularly important in LMICs, where data privacy laws may be underdeveloped or weak.80,91
Counselling
Uncertainties surrounding gene penetrance, inconclusive results, the varying effectiveness of screening and surgical interventions make risk communication with patients and at-risk relatives a challenge.92 The general lack of awareness about clinical genetics adds to the above problems. While interventions to address patients’ psychological needs and strategies for scalable and efficient clinical risk communication are commonly used and usually successful.93 Effective clinical risk communication strategies, decision support tools, psychosocial support resources and written educational materials may significantly address the supportive needs of BRCA carriers.94,95
The Psychological Impact
The psychological impacts of receiving breast cancer gene test results, particularly for BRCA1 and BRCA2, can be significant and multifaceted including higher levels of psychological distress, depression and anxiety compared to non-carriers.96–98 This is attributed to the heightened perceived risk of developing cancer and the consequences for family members. However, the distress levels can vary based on individual coping mechanisms and the availability of psychological support.99,100 Individuals with better coping self-efficacy tend to experience less symptoms of anxiety and depression following the disclosure of genetic test results. This suggests that enhancing coping skills could be a protective factor against psychological morbidity.101 However, despite initial negative emotions upon receiving a positive test result, some studies suggest that the overall quality of life may not be significantly impaired in the long term. This is particularly true when adequate counseling and support are provided, which can help individuals adjust to their genetic risk status.102
On a positive note, receiving a positive test result can lead to an improved understanding of personal cancer risk, which may positively influence health behavior intentions, such as increased surveillance and consideration of preventive measures.103,104 The disclosure of genetic test results can affect family dynamics, with significant barriers to communication noted. The transfer of information to at-risk relatives is high, but genetic testing among them remains low, indicating potential psychological barriers.28
Overall, the psychological impact of breast cancer gene testing is complex and influenced by various factors, including the quality of genetic counseling, individual psychological resilience and family support systems. It is crucial to provide comprehensive pre- and post-test counseling to mitigate adverse psychological effects and support informed decision-making. This counseling should be conducted by qualified genetic professionals and include discussions on the implications of test results, potential outcomes, and the limitations of genetic testing.
Overall, a multidisciplinary approach involving genetic counseling, psychosocial support, and educational resources is essential to address the psychological impacts of BRCA testing and to support patients in making informed decisions about their health.
Practical Framework for Implementing Expanded Germline Testing
Low- versus High-Income Countries
Although the majority of evidence supporting expanded or universal germline testing originates from high-income countries, direct extrapolation to resource-restricted settings should be approached cautiously. Cost-effectiveness estimates may vary substantially according to local healthcare financing models, testing costs, workforce availability, and access to downstream interventions. Similarly, shortages of trained genetic counselors, limited laboratory infrastructure, and challenges related to interpretation of variants of uncertain significance may affect implementation. Broader testing strategies should therefore be adapted to local realities rather than adopted uniformly across all healthcare systems.
A Phased Implementation Strategy
Phase 1 should focus on guideline-based testing of patients meeting established hereditary cancer criteria. This strategy offers the highest immediate diagnostic yield while minimizing financial burden. Phase 2 may expand eligibility to all patients aged 65 years or younger, consistent with contemporary recommendations, once counseling capacity and testing infrastructure become established. Phase 3 may ultimately consider universal testing for all patients with breast cancer when sustainable funding, laboratory infrastructure, variant interpretation systems, and access to downstream preventive and therapeutic interventions are available. This phased approach balances clinical benefit with healthcare system readiness and may represent the most realistic pathway for many LMICs.
Lessons from Jordan – A Real-World Model
Jordan provides an illustrative example of how cancer genetics services can be progressively developed within a resource-constrained healthcare environment. Over the last decade, structured investment in genetic counseling services, multigene panel testing, patient education, and multidisciplinary collaboration has facilitated the establishment of one of the largest hereditary cancer programs in the region.105 The experience demonstrates that successful implementation requires institutional commitment, workforce development, patient engagement, and sustainable funding mechanisms. Importantly, the Jordanian experience highlights the feasibility of expanding access to germline testing despite financial and logistical barriers and provides practical lessons that may be applicable to other resource-restricted settings.
Conclusion
Germline genetic testing has become an increasingly important component of modern breast cancer care, influencing treatment selection, surgical decision-making, surveillance recommendations, and familial risk assessment. While growing evidence supports broader testing strategies and recent guidelines have expanded eligibility criteria, implementation in resource-restricted settings remains challenging. Financial limitations, shortages of trained personnel, laboratory infrastructure requirements, management of VUS, and unequal access to downstream interventions must all be considered when translating evidence generated in high-income countries to LMICs. Rather than viewing universal testing as an immediate objective, resource-restricted healthcare systems may benefit from a phased implementation strategy that progresses from guideline-based testing to expanded eligibility and ultimately universal testing as local capacity evolves. Such a pragmatic and context-specific approach may provide the most realistic pathway toward equitable access to germline genetic testing worldwide.
Funding
This project did not receive funding; however, the Article Processing Charges (APC) is covered by King Hussein Cancer Center (KHCC).
Disclosure
The author declares no competing interests in this work.
References
1. Kim J, Harper A, McCormack V, et al. Global patterns and trends in breast cancer incidence and mortality across 185 countries. Nat Med. 2025;31(4):1154–13. doi:10.1038/s41591-025-03502-3
2. Winters S, Martin C, Murphy D, Shokar NK. Breast cancer epidemiology, prevention, and screening. In: Progress in Molecular Biology and Translational Science. Vol. 151. Elsevier; 2017:1–32.
3. Manna EDF, Serrano D, Cazzaniga L, et al. Hereditary breast cancer: comprehensive risk assessment and prevention strategies. Genes. 2025;16:82. doi:10.3390/genes16010082
4. Lux MP, Fasching PA. Breast cancer and genetic BRCA1/2 testing in routine clinical practice: why, when and for whom? Geburtshilfe Frauenheilkd. 2023;83:310–320. doi:10.1055/a-1929-2629
5. Miglietta F, Cinquini M, Dieci MV, et al. PARP-inhibitors for BRCA1/2-related advanced HER2-negative breast cancer: a meta-analysis and GRADE recommendations by the italian association of medical oncology. Breast. 2022;66:293–304. doi:10.1016/j.breast.2022.10.014
6. Taylor AM, Chan DLH, Tio M, et al. PARP (Poly ADP-Ribose Polymerase) inhibitors for locally advanced or metastatic breast cancer. Cochrane Database Syst Rev. 2021;4:CD011395. doi:10.1002/14651858.CD011395.pub2
7. Muñante B, Paz-Manrique R, Pinto JA, Gomez HL. Clinical management in BRCA carriers with early breast cancer. Cancer Control. 2025;32:10732748251377864. doi:10.1177/10732748251377864
8. Abdel-Razeq H, Sharaf B, Tamimi F, et al. Establishment of a clinical cancer genetics program for breast cancer in a resource-limited country; challenges and opportunities. Front Oncol. 2024;14:1431985. doi:10.3389/fonc.2024.1431985
9. National Comprehensive Cancer Network (NCCN). Genetic/Familial high-risk assessment: breast, ovarian, pancreatic, and prostate (Version 2.2026). NCCN clinical practice guidelines in oncology. Available from: https://www.nccn.org/guidelines/guidelines-detail?category=2&id=1545.
10. Bedrosian I, Somerfield MR, Achatz MI, et al. Germline testing in patients with breast cancer: ASCO–society of surgical oncology guideline. JCO. 2024;42:584–604. doi:10.1200/JCO.23.02225
11. Whitworth PW, Beitsch PD, Patel R, et al. Clinical utility of universal germline genetic testing for patients with breast cancer. JAMA Network Open. 2022;5:e2232787. doi:10.1001/jamanetworkopen.2022.32787
12. De Silva DL, Stafford L, Skandarajah AR, et al. Universal genetic testing for women with newly diagnosed breast cancer in the context of multidisciplinary team care. Med J Aust. 2023;218:368–373. doi:10.5694/mja2.51906
13. Manahan ER, Kuerer HM, Sebastian M, et al. Consensus guidelines on genetic` testing for hereditary breast cancer from the American Society of Breast Surgeons. Ann Surg Oncol. 2019;26:3025–3031. doi:10.1245/s10434-019-07549-8
14. Samadder NJ, Riegert-Johnson D, Boardman L, et al. Comparison of universal genetic testing vs guideline-directed targeted testing for patients with hereditary cancer syndrome. JAMA Oncol. 2021;7:230–237. doi:10.1001/jamaoncol.2020.6252
15. Miki Y, Swensen J, Shattuck-Eidens D, et al. A strong candidate for the breast and ovarian cancer susceptibility gene BRCA1. Science. 1994;266:66–71. doi:10.1126/science.7545954
16. Meijers-Heijboer H, van den Ouweland A, Klijn J, et al. Low-penetrance susceptibility to breast cancer due to CHEK2(*)1100delC in noncarriers of BRCA1 or BRCA2 mutations. Nat Genet. 2002;31:55–59. doi:10.1038/ng879
17. Antoniou AC, Casadei S, Heikkinen T, et al. Breast-cancer risk in families with mutations in PALB2. N Engl J Med. 2014;371:497–506. doi:10.1056/NEJMoa1400382
18. Thompson D, Duedal S, Kirner J, et al. Cancer risks and mortality in heterozygous ATM mutation carriers. J Natl Cancer Inst. 2005;97:813–822. doi:10.1093/jnci/dji141
19. Roy R, Chun J, Powell SN. BRCA1 and BRCA2: different roles in a common pathway of genome protection. Nat Rev Cancer. 2011;12:68–78. doi:10.1038/nrc3181
20. Mahdavi M, Nassiri M, Kooshyar MM, et al. Hereditary breast cancer; genetic penetrance and current status with BRCA. J Cell Physiol. 2019;234:5741–5750. doi:10.1002/jcp.27464
21. Venkitaraman AR. How do mutations affecting the breast cancer genes BRCA1 and BRCA2 cause cancer susceptibility? DNA Repair. 2019;81:102668. doi:10.1016/j.dnarep.2019.102668
22. Siegel RL, Miller KD, Wagle NS, Jemal A. Cancer Statistics, 2023. CA Cancer J Clin. 2023;73:17–48. doi:10.3322/caac.21763
23. Kuchenbaecker KB, Hopper JL, Barnes DR, et al. Risks of breast, ovarian, and contralateral breast cancer for BRCA1 and BRCA2 mutation carriers. JAMA. 2017;317:2402–2416. doi:10.1001/jama.2017.7112
24. Vargason AB, Turner CE, Shriver CD, Ellsworth RE. Influence of germline test results on surgical decision making in women with invasive breast cancer. Cancer Genet. 2022;266–267,81–85. doi:10.1016/j.cancergen.2022.07.003
25. Abdel-Razeq H. Surgical options for patients with early-stage breast cancer and pathogenic germline variants: an oncologist perspectives. Front Oncol. 2023;13:1265197. doi:10.3389/fonc.2023.1265197
26. Edaily S, Abdel-Razeq H. Management strategies of breast cancer patients with BRCA1 and BRCA2 pathogenic germline variants. Onco Targets Ther. 2022;15:815–826. doi:10.2147/OTT.S369844
27. Abdel-Razeq H, Tamimi F, Iweir S, et al. Genetic counseling and genetic testing for pathogenic germline mutations among high-risk patients previously diagnosed with breast cancer: a traceback appRoach. Sci Rep. 2024;14:12820. doi:10.1038/s41598-024-63300-8
28. Abdel-Razeq H, Mustafa R, Abdel-Razeq S, et al. Pathogenic germline variants in patients with breast cancer: conversations across generations, practices and patients’ attitude. Front Genet. 2023;14:1194075. doi:10.3389/fgene.2023.1194075
29. Tutt ANJ, Garber JE, Kaufman B, et al. Adjuvant olaparib for patients with BRCA1- or BRCA2-mutated breast cancer. N Engl J Med. 2021;384:2394–2405. doi:10.1056/NEJMoa2105215
30. Geyer CE, Garber JE, Gelber RD, et al. Overall survival in the olympiA Phase III trial of adjuvant olaparib in patients with germline pathogenic variants in BRCA1/2 and high-risk, early breast cancer. Ann Oncol. 2022;33:1250–1268. doi:10.1016/j.annonc.2022.09.159
31. Garber JE, et al. Pre-specified analyses of IDFS, DDFS and OS 10 years from first patient In (FPI) in the olympia trial of adjuvant olaparib in germline BRCA1/2 mutation-associated breast cancer. In:
32. Morganti S, Bychkovsky BL, Poorvu PD, et al. Adjuvant olaparib for germline BRCA carriers with HER2-negative early breast cancer: evidence and controversies. Oncologist. 2023;28:565–574. doi:10.1093/oncolo/oyad123
33. Robson M, Im S-A, Senkus E, et al. Olaparib for metastatic breast cancer in patients with a germline BRCA mutation. N Engl J Med. 2017;377:523–533. doi:10.1056/NEJMoa1706450
34. Henry NL, Somerfield MR, Dayao Z, et al. Biomarkers for systemic therapy in metastatic breast cancer: ASCO guideline update. JCO. 2022;40:3205–3221. doi:10.1200/JCO.22.01063
35. Burstein HJ, Somerfield MR, Barton DL, et al. Endocrine treatment and targeted therapy for hormone receptor–positive, human epidermal growth factor receptor 2–negative metastatic breast cancer: ASCO guideline update. JCO. 2021;39:3959–3977. doi:10.1200/JCO.21.01392
36. Litton JK, Rugo HS, Ettl J, et al. Talazoparib in patients with advanced breast cancer and a germline BRCA mutation. N Engl J Med. 2018;379:753–763. doi:10.1056/NEJMoa1802905
37. Schettini F, Giudici F, Bernocchi O, et al. Poly (ADP-Ribose) polymerase inhibitors in solid tumours: systematic review and meta-analysis. Eur. J. Cancer. 2021;149:134–152. doi:10.1016/j.ejca.2021.02.035
38. Walsh EM, Mangini N, Fetting J, et al. Olaparib use in patients with metastatic breast cancer harboring somatic BRCA1/2 mutations or mutations in non-BRCA1/2, DNA damage repair genes. Clinical Breast Cancer. 2022;22:319–325. doi:10.1016/j.clbc.2021.12.007
39. National Institute for Health and Care Excellence (NICE). Familial breast cancer: classification, care and managing breast cancer and related risks in people with a family history of breast cancer (CG164). Available from: https://www.nice.org.uk/guidance/cg164/ifp/chapter/Early-detection-of-breast-cancer-by-surveillance.
40. Culver JO, Freiberg Y, Ricker C, et al. Integration of universal germline genetic testing for all new breast cancer patients. Ann Surg Oncol. 2023;30:1017–1025. doi:10.1245/s10434-022-12595-w
41. Goh SP, Ong SC, Chan JE. Economic evaluation of germline genetic testing for breast cancer in low- and middle-income countries: a systematic review. BMC Cancer. 2024;24:316. doi:10.1186/s12885-024-12038-7
42. Erfani P, Bhangdia K, Stauber C, Mugunga JC, Pace LE, Fadelu T. Economic evaluations of breast cancer care in low- and middle-income countries: a scoping review. Oncologist. 2021;26:e1406–e1417. doi:10.1002/onco.13841
43. Sun L, Brentnall A, Patel S, et al. A cost-effectiveness analysis of multigene testing for all patients with breast cancer. JAMA Oncol. 2019;5:1718–1730. doi:10.1001/jamaoncol.2019.3323
44. Guo F, Adekanmbi V, Hsu CD, Berenson AB, Kuo Y-F, Shih Y-C. Cost-effectiveness of population-based multigene testing for breast and ovarian cancer prevention. JAMA Network Open. 2024;7:e2356078. doi:10.1001/jamanetworkopen.2023.56078
45. Sun L, Wei X, Fierheller CT, et al. Economic evaluation of population-based BRCA1 and BRCA2 testing in Canada. JAMA Network Open. 2024;7:e2432725. doi:10.1001/jamanetworkopen.2024.32725
46. Delikurt T, Williamson GR, Anastasiadou V, Skirton H. A systematic review of factors that act as barriers to patient referral to genetic services. Eur J Hum Genet. 2015;23:739–745. doi:10.1038/ejhg.2014.180
47. Raspa M, Moultrie R, Toth D, Haque SN. Barriers and facilitators to genetic service delivery models: scoping review. Interact J Med Res. 2021;10:e23523. doi:10.2196/23523
48. Boothe E, Greenberg S, Delaney CL, Cohen SA. Genetic counseling service delivery models: a study of genetic counselors’ interests, needs, and barriers to implementation. J Genet Couns. 2021;30:283–292. doi:10.1002/jgc4.1319
49. Zhong A, Darren B, Loiseau B, et al. Ethical, social, and cultural issues related to clinical genetic testing and counseling in low- and middle-income countries: a systematic review. Genet Med. 2021;23:2270–2280. doi:10.1038/s41436-018-0090-9
50. Thong M-K, See-Toh Y, Hassan J, Ali J. Medical genetics in developing countries in the Asia-Pacific region: challenges and opportunities. Genet Med. 2018;20:1114–1121. doi:10.1038/s41436-018-0135-0
51. Burke W, Parens E, Chung WK, Berger SM, Appelbaum PS. The challenge of genetic variants of uncertain clinical significance: a narrative review. Ann Intern Med. 2022;175:994–1000. doi:10.7326/M21-4109
52. Abdel-Razeq H, Tamimi F, Abujamous L, et al. Rates of variants of uncertain significance among patients with breast cancer undergoing genetic testing: regional perspectives. Front Oncol. 2022;12:673094. doi:10.3389/fonc.2022.673094
53. Welsh JL, Hoskin TL, Day CN, et al. Clinical decision-making in patients with variant of uncertain significance in BRCA1 or BRCA2 genes. Ann Surg Oncol. 2017;24:3067–3072. doi:10.1245/s10434-017-5959-3
54. Chang J, Seng S, Yoo J, Equivel P, Lum SS. Clinical management of patients at risk for hereditary breast cancer with variants of uncertain significance in the era of multigene panel testing. Ann Surg Oncol. 2019;26:3389–3396. doi:10.1245/s10434-019-07595-2
55. Makhnoon S, Bednar EM, Krause KJ, Peterson SK, Lopez-Olivo MA. Clinical management among individuals with variant of uncertain significance in hereditary cancer: a systematic review and meta-analysis. Clin Genet. 2021;100:119–131. doi:10.1111/cge.13966
56. PopulationPyramid.net. Population Pyramid of Jordan 2024. Available from: https://www.populationpyramid.net/jordan/2024/.
57. PopulationPyramid.net. Population pyramid of the United States of America 2024. Available from: https://www.populationpyramid.net/united-states-of-america/2024/.
58. World Health Organization. Country data: jordan. Available from: https://data.who.int/countries/400.
59. Adombire S, Baiden D, Puts M, Puchalski Ritchie LM, Ani-Amponsah M, Cranley L. Knowledge, skills, attitudes, beliefs, and implementation of evidence-based practice among nurses in low- and middle-income countries: a scoping review. Worldviews Evid Based Nurs. 2024;21:542–553. doi:10.1111/wvn.12734
60. Walters S, Aldous C, Malherbe H. Knowledge, attitudes, and practices of primary healthcare practitioners in low- and middle-income countries: a scoping review on genetics. J Community Genet. 2024;15:461–474. doi:10.1007/s12687-024-00721-y
61. Abdel-Razeq H, Al-Omari A, Zahran F, Arun B. Germline BRCA1/BRCA2 mutations among high risk breast cancer patients in Jordan. BMC Cancer. 2018;18:152. doi:10.1186/s12885-018-4079-1
62. Ullah E, Abdel-Razeq H, Bentebbal S, et al. Comprehensive genomic analysis of Non-BRCA familial breast cancer in an Arab population. Npj Breast Cancer. 2026. doi:10.1038/s41523-026-00926-z
63. Abdel-Razeq H, Abujamous L, Al-Azzam K, et al. Guideline-based, multi-gene panel germline genetic testing for at-risk patients with breast cancer. Breast Cancer. 2023;15:1–10. doi:10.2147/BCTT.S394092
64. Tekola-Ayele F, Rotimi CN. Translational genomics in low- and middle-income countries: opportunities and challenges. Public Health Genomics. 2015;18:242–247. doi:10.1159/000433518
65. Zalis M, Viana Veloso GG, Aguiar PN, et al. Next-generation sequencing impact on cancer care: applications, challenges, and future directions. Front Genet. 2024;15:1420190. doi:10.3389/fgene.2024.1420190
66. Yadav D, Patil-Takbhate B, Khandagale A, Bhawalkar J, Tripathy S, Khopkar-Kale P. Next-generation sequencing transforming clinical practice and precision medicine. Clin Chim Acta. 2023;551:117568. doi:10.1016/j.cca.2023.117568
67. Vrečar I, Hristovski D, Peterlin B. Telegenetics: an update on availability and use of telemedicine in clinical genetics service. J Med Syst. 2017;41:21. doi:10.1007/s10916-016-0666-3
68. Gorrie A, Gold J, Cameron C, Krause M, Kincaid H. Benefits and Limitations of Telegenetics: a Literature Review. J Genet Couns. 2021;30:924–937. doi:10.1002/jgc4.1418
69. Atsumi H, Damdinsuren A, Asai S, et al. A local community outreach educational program on genetic testing: a pilot study. Tokai J Exp Clin Med. 2024;49:67–72.
70. Berninger T, Nusbaum R, Redlinger-Grosse K, Davis C, Reiser C. A narrative literature review: growing the workforce through increased fieldwork capacity in genetic counseling training programs. J Genet Couns. 2021;30:574–587. doi:10.1002/jgc4.1346
71. Calabrò GE, Tognetto A, Mazzaccara A, et al. Capacity building of health professionals on genetics and genomics practice: evaluation of the effectiveness of a distance learning training course for Italian physicians. Front Genet. 2021;12:626685. doi:10.3389/fgene.2021.626685
72. Botkin JR. Informed consent for genetic and genomic research. Curr Protoc Hum Genet. 2020;108:e104. doi:10.1002/cphg.104
73. Ochieng J, Kwagala B, Barugahare J, Möller M, Moodley K. Awareness, experiences and perceptions regarding genetic testing and the return of genetic and genomics results in a hypothetical research context among patients in Uganda: a qualitative study. J Med Ethics. 2024;50:829–834. doi:10.1136/jme-2022-108885
74. Wright GEB, Koornhof PGJ, Adeyemo AA, Tiffin N. Ethical and legal implications of whole genome and whole exome sequencing in African populations. BMC Med Ethics. 2013;14:21. doi:10.1186/1472-6939-14-21
75. Mubarak S, Ashraf M. Ethics considerations for precision medicine research and genetic testing in low- and middle-income countries. East Mediterr Health J. 2024;30:455–460. doi:10.26719/2024.30.6.455
76. Nankya H, Alibu VP, Wamala E, Matovu E, Barugahare J. Understanding of key considerations for effective community engagement in genetics and genomics research: a qualitative study of the perspectives of research ethics committee members and national research regulators in a low resource setting. J Empir Res Hum Res Ethics. 2024;19:197–207. doi:10.1177/15562646241289015
77. Li Y, Bowen DJ, Yu J-H. Informed consent in genetic and genomic studies in sub-saharan Africa: a systematic review of bioethical issues. BMC Med Ethics. 2025;26:99. doi:10.1186/s12910-025-01170-z
78. Gostin L. Genetic discrimination: the use of genetically based diagnostic and prognostic tests by employers and insurers. Am J Law Med. 1991;17:109–144. doi:10.1017/S0098858800007942
79. Ellis AM. Genetic justice: discrimination by employers and insurance companies based on predictive genetic information. Tex Tech Law Rev. 2003;34:1071–1099.
80. Clayton EW, Evans BJ, Hazel JW, Rothstein MA. The law of genetic privacy: applications, implications, and limitations. J Law Biosci. 2019;6:1–36. doi:10.1093/jlb/lsz007
81. Prince AER, Uhlmann WR, Suter SM, Scherer AM. Genetic testing and insurance implications: surveying the us general population about discrimination concerns and knowledge of the Genetic Information Nondiscrimination Act (GINA). Risk Manag Insur Rev. 2021;24:341–365. doi:10.1111/rmir.12195
82. Bombard Y, Heim-Myers B. The genetic non-discrimination act: critical for promoting health and science in Canada. CMAJ. 2018;190:E579–E580. doi:10.1503/cmaj.180298
83. Lenartz A, Scherer AM, Uhlmann WR, Suter SM, Anderson Hartley C, Prince AER. The persistent lack of knowledge and misunderstanding of the Genetic Information Nondiscrimination Act (GINA) more than a decade after passage. Genet Med. 2021;23:2324–2334. doi:10.1038/s41436-021-01268-w
84. Shabani M, Borry P. Rules for processing genetic data for research purposes in view of the new EU general data protection regulation. Eur J Hum Genet. 2018;26:149–156. doi:10.1038/s41431-017-0045-7
85. McGeveran W, Schmitz C. General-purpose privacy regulation and translational genomics. J Law Med Ethics. 2020;48:142–150. doi:10.1177/1073110520917002
86. Staunton C, Slokenberga S, Parziale A, Mascalzoni D. Appropriate safeguards and article 89 of the GDPR: considerations for biobank, databank and genetic research. Front Genet. 2022;13:719317. doi:10.3389/fgene.2022.719317
87. Ahram M, Soubani M, Abu salem L, Saker H, Ahmad MK. Attitudes, and practice regarding genetic testing and genetic counselors in jordan: a population-based survey. J Genet Couns. 2015;24:1001–1010. doi:10.1007/s10897-015-9839-3
88. Shenbagam S, Taylor A, Jain R, Fakhro K, Alkuraya F, Abou Tayoun A. Genetic counseling in the middle east: provider perspectives of patient attitudes and cultural challenges. Hum Genomics. 2025;19:59. doi:10.1186/s40246-025-00770-5
89. NSAIRS. Data protection and privacy (Jordan). Available from: https://nsairs.com/wp-content/uploads/2023/07/2024-Data-Protection-Privacy-Jordan.pdf.
90. Khdair SI, Al-Qerem W, Jarrar W. Knowledge and attitudes regarding genetic testing among jordanians: an approach towards genomic medicine. Saudi J Biol Sci. 2021;28:3989–3999. doi:10.1016/j.sjbs.2021.04.004
91. Stiles D, Appelbaum PS. Cases in precision medicine: concerns about privacy and discrimination after genomic sequencing. Ann Intern Med. 2019;170:717–721. doi:10.7326/M18-2666
92. Makhnoon S, Arun B, Bedrosian I. Helping patients understand and cope with BRCA mutations. Curr Oncol Rep. 2022;24:733–740. doi:10.1007/s11912-022-01254-8
93. Gietel-Habets JJG, de Die-Smulders CEM, Derks-Smeets IA, et al. Awareness and attitude regarding reproductive options of persons carrying a BRCA mutation and their partners. Hum Reprod. 2017;32:588–597. doi:10.1093/humrep/dew352
94. McGarrigle SA, Prizeman G, Spillane C, et al. Decision aids for female BRCA mutation carriers: a scoping review. BMJ Open. 2024;14:e076876. doi:10.1136/bmjopen-2023-076876
95. Starkings R, Shilling V, Jenkins V, Fallowfield L. A systematic review of communication interventions to help healthcare professionals discuss genetic testing for breast cancer. Breast Cancer Res Treat. 2020;183:9–21. doi:10.1007/s10549-020-05741-z
96. Meiser B, Butow P, Friedlander M, et al. Psychological impact of genetic testing in women from high-risk breast cancer families. Eur J Cancer. 2002;38:2025–2031. doi:10.1016/s0959-8049(02)00264-2
97. Mella S, Muzzatti B, Dolcetti R, Annunziata MA. Emotional impact on the results of BRCA1 and BRCA2 genetic test: an observational retrospective study. Hered Cancer Clin Pract. 2017;15:16. doi:10.1186/s13053-017-0077-6
98. Hamilton JG, Lobel M, Moyer A. Emotional distress following genetic testing for hereditary breast and ovarian cancer: a meta-analytic review. Health Psychol. 2009;28:510–518. doi:10.1037/a0014778
99. Blomen CL, Pott A, Volk AE, Budäus L, Witzel I. Communication processes about predictive genetic testing within high-risk breast cancer families: a two-phase study design. Sci Rep. 2021;11:20178. doi:10.1038/s41598-021-98737-8
100. Lombardi L, Bramanti SM, Babore A, et al. Psychological aspects, risk and protective factors related to BRCA genetic testing: a review of the literature. Support Care Cancer. 2019;27:3647–3656. doi:10.1007/s00520-019-04918-7
101. Isselhard A, Lautz Z, Töpper M, et al. Coping self-efficacy and its relationship with psychological morbidity after genetic test result disclosure: results from cancer-unaffected BRCA1/2 mutation carriers. Int J Environ Res Public Health. 2023;20:1684. doi:10.3390/ijerph20031684
102. Qiu J, Guan J, Yang X, et al. Quality of life and psychological state in chinese breast cancer patients who received BRCA1/2 genetic testing. PLoS One. 2016;11:e0158531. doi:10.1371/journal.pone.0158531
103. Padmanabhan H, Hassan NT, Wong S-W, et al. Psychosocial outcome and health behaviour intent of breast cancer patients with BRCA1/2 and PALB2 pathogenic variants unselected by a priori risk. PLoS One. 2022;17:e0263675. doi:10.1371/journal.pone.0263675
104. Brédart A, Kop JL, Depauw A, et al. Short-term psychological impact of the BRCA1/2 test result in women with breast cancer according to their perceived probability of genetic predisposition to cancer. Br J Cancer. 2013;108:1012–1020. doi:10.1038/bjc.2012.599
105. Abdel-Razeq H, Tamimi F, Abdel-Razeq S, et al. Universal vs. ASCO guidelines-based germline genetic testing for newly diagnosed breast cancer patients in resource-restricted settings. Oncol Rev. 2026;19:1638255. doi:10.3389/or.2025.1638255
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Management Strategies of Breast Cancer Patients with BRCA1 and BRCA2 Pathogenic Germline Variants
Edaily S, Abdel-Razeq H
OncoTargets and Therapy 2022, 15:815-826
Published Date: 27 July 2022
Guideline-Based, Multi-Gene Panel Germline Genetic Testing for at-Risk Patients with Breast Cancer
Abdel-Razeq H, Abujamous L, Al-Azzam K, Abu-Fares H, Bani Hani H, Alkyam M, Sharaf B, Elemian S, Tamimi F, Abuhijla F, Edaily S, Salama O, Abdulelah H, Daoud R, Abubaker M, Al-Atary A
Breast Cancer: Targets and Therapy 2023, 15:1-10
Published Date: 13 January 2023
Association Between Germline BRCA1/2 Gene Variants and Clinicopathological Features of Ovarian Cancer
Luo Y, Pan R, Rao H, Chen X, Yang H
International Journal of General Medicine 2024, 17:75-84
Published Date: 11 January 2024
Functional Analysis of BRCA1 3’UTR Variants Predisposing to Breast Cancer
Sierra-Díaz DC, Cabrera R, Gonzalez-Vasquez LA, Angulo-Aguado M, Llinás-Caballero K, Fonseca-Mendoza DJ, Contreras-Bravo NC, Restrepo CM, Ortega-Recalde O, Morel A
The Application of Clinical Genetics 2024, 17:57-62
Published Date: 23 May 2024
The Frequency and Reclassification of Variants Uncertain Significance in Hereditary Breast and Ovarian Cancer Among Levantine Patients
Assaf N, Sharab SJ, Monsef C, El Saghir NS
Cancer Management and Research 2025, 17:2503-2512
Published Date: 27 October 2025