Back to Journals » Clinical Ophthalmology » Volume 19
A Systematic Review of the PAUL Glaucoma Implant
Authors Tan N ![]() , Summers S, Alryalat SA, Patnaik JL
, Summers S, Alryalat SA, Patnaik JL ![]() , Lazcano-Gomez GS
, Lazcano-Gomez GS ![]() , Seibold LK, Kahook MY
, Seibold LK, Kahook MY
Received 3 June 2025
Accepted for publication 18 August 2025
Published 5 September 2025 Volume 2025:19 Pages 3255—3271
DOI https://doi.org/10.2147/OPTH.S544440
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Nicholas Tan, Steven Summers, Saif Aldeen Alryalat, Jennifer L Patnaik, Gabriel S Lazcano-Gomez, Leonard K Seibold, Malik Y Kahook
Department of Ophthalmology, The University of Colorado, Aurora, CO, USA
Correspondence: Malik Y Kahook, Department of Ophthalmology, The University of Colorado, 1675 Aurora Ct, Aurora, CO, 80045, USA, Tel +1 720 848-2500, Fax +1 720 848-5079, Email [email protected]
Abstract: The PAUL Glaucoma Implant (PGI) is a novel, valveless glaucoma drainage device that is distinguished from prevailing tube shunts by its compact plate and small lumen. However, clinical consensus is lacking on its real-world advantages. Thus, we conducted a systematic review to assess PGI surgical approaches, safety, and efficacy. A comprehensive literature search was performed using PubMed, Embase, Web of Science, and ClinicalTrials.gov. Single case reports were excluded. Twenty-six studies comprising 1143 eyes were included. The most common duration of follow-up was one year, and five studies were prospective. Median IOP reduction by last follow-up was 53.4% (range 27.7– 66.2%), and glaucoma medication use decreased by 71.8% (42.3– 94.6%). At an intraocular pressure (IOP) upper threshold of 21 mmHg, the median qualified success rate was 92.0% (80.0– 100.0%), and complete success was 48.0% (24.0– 73.3%); though criteria varied between studies. The most frequently reported complications were hyphema (10.0%), numerical hypotony (9.7%), and shallow anterior chamber (5.9%). Tube erosion occurred in 5.0% of cases overall, and in 9.8% of eyes in prospective studies. A single randomized controlled trial comparing the PGI to the Ahmed Glaucoma Valve in pediatric patients found noninferiority at 12 months, but was limited by sample size and generalizability. Four additional retrospective comparative studies (three versus Baerveldt, one versus Ahmed) showed no consistent advantages of the PGI. Substantial variation was also reported in PGI surgical techniques, including ripcord use, graft material, and adjunctive antifibrotics. While the PGI appears effective in lowering IOP and medication burden, current evidence is limited by retrospective designs, small cohorts, heterogeneous protocols, and short follow-up. Tube erosions were reported more often than historically seen with Baerveldt and Ahmed devices. Higher-quality, prospective comparative studies are needed to determine the long-term safety, efficacy, and optimal surgical approach for the PGI.
Keywords: glaucoma drainage device, tube shunt, safety, efficacy, outcomes
Introduction
Glaucoma is a progressive optic neuropathy with an increasing global burden. For primary open-angle glaucoma (POAG) alone, the number of affected patients is projected to climb to 79.8 million by 2040 compared to 52.7 million in 2020.1 Intraocular pressure (IOP) reduction constitutes the principal approach to treatment. In cases of advanced disease, maximal reduction in IOP can be achieved through a trabeculectomy or glaucoma drainage device (GDD) implantation.2 The most commonly used GDDs are the Ahmed and Baerveldt tube shunts.3 The Ahmed Glaucoma Valve (AGV, New World Medical, Rancho Cucamonga, CA, USA) utilizes a valved system to reduce the flow of aqueous humor when IOP is low, reducing the risk of hypotony. Frequently used models of the AGV include the FP7 (endplate surface area of 184 mm2) and FP8 (102 mm2). The Baerveldt Glaucoma Implant (BGI, Abbott Medical Optics, Santa Ana, CA, USA) differs in that it features both a wider endplate (250 or 350 mm2) and a valveless reservoir to allow for maximum IOP reduction. In multicenter randomized controlled trials (RCTs), the BGI was found to have greater success rates, while the AGV demonstrated fewer side-effects, particularly in the early postoperative period.4–6
Though both tube shunts possess advantages, there has been interest in developing GDDs that may improve upon their designs. One such example is the valveless Ahmed ClearPath (ACP, New World Medical, Rancho Cucamonga, CA, USA). Like the BGI, it exists in 250 mm2 and 350 mm2 plate sizes. Its key differences include an alternatively contoured plate and more anteriorly positioned eyelets.7 The compact ACP 250 endplate allows it to be implanted without manipulating extraocular muscles.8 The PAUL Glaucoma Implant (PGI, Advanced Ophthalmic Innovations, Singapore) is another valveless GDD that incorporates some aspects of the Baerveldt implant. By using a 342.1 mm2 endplate with compact wings, it can more easily be tucked between the recti.9 The smaller profile is hypothesized to reduce device interference with motility in a manner similar to the ACP. It further differs from the BGI by including a smaller diameter tube, theoretically reducing flow rate without requiring a valve. Combined, these features aim to achieve sustained IOP reduction with fewer hypotony-associated complications.9
Though the United States Food and Drug Administration (FDA) approved the ACP in 2019, the PGI has not yet gained equivalent status. Most American glaucoma specialists have not trialed the PGI, and there is growing anecdotal interest in its effects. No systematic review of the PGI has been published at the time of writing. Therefore, we sought to review the existing retrospective and prospective literature on PGI clinical outcomes. It was our aim to provide a comprehensive assessment of current PGI findings in order to better inform tube shunt surgeons.
Methods
PRISMA 2020 guidelines were followed.10 Pubmed, Embase, Web of Science, and clinicaltrials.gov were each queried with the search terms “PAUL Glaucoma Implant.” The period of extraction was from 4/1/2025 – 4/7/2025. Prospective studies and retrospective case series that examined primary clinical outcomes of the PAUL Glaucoma Implant were included. The following publication types were excluded: reviews, commentaries, replies, individual case reports, imaging or histologic studies, abstracts with data published in a separate paper, and articles lacking an English full text.
After initial identification from the aforementioned databases and register, Microsoft EndNote was used to remove duplicate records. The remaining records were then screened by abstract. At this stage, records were excluded for having no data or being unrelated to the PGI. The subsequent reports were then sought for full text retrieval with the remaining exclusion criteria applied to determine the final studies.
Data from the final selected studies were compiled onto Excel spreadsheets. Data entries were recorded and cross-verified by three authors (NT, SS, SAA). Three sheets were assembled: 1) baseline and outcomes; 2) surgical techniques; and 3) complications. Demographics data included country or countries of study, retrospective or prospective study design, PGI sample size, mean duration of follow-up, surgical comparison group (if any), sample size of comparison group, mean age, % female, racial/ethnic breakdown of PGI sample, % with prior glaucoma surgery, glaucoma types, mean baseline IOP, and mean baseline glaucoma medications. Outcome measures recorded included mean final IOP, mean final medications, % reduction in IOP and medications from baseline to last follow-up, definitions of success, and qualified and complete success rates. For surgical techniques, patch graft type, ripcord suture use, mitomycin-C use, 5-fluorouracil use, and combination with cataract surgery were evaluated. Lastly, for complications, the full list was based off those reported in the Ahmed Baerveldt Comparison (ABC) and Ahmed Versus Baerveldt (AVB) studies.11,12
Sample sizes were enumerated using the eye as the unit of measurement. In cases where descriptive statistics were extracted, the native measures of dispersion (eg standard deviation, range) were reported without conversion. In cases where two comparison groups were involved and both groups received the PGI implant, study values were computed for the combined sample. Summative metrics were pooled accordingly between groups. For studies that reported multiple success rates, percentages of qualified successes at a given IOP target were counted inclusive of the complete successes. The central tendency and dispersion of study-level means were described using the median and range. Percentage reduction metrics were averaged across all studies. Complications were tallied across all studies and assigned a cumulative percentage. Per study, a complication was coded as zero percent when the authors indicated that the complication was monitored for and did not occur. Otherwise, if a complication was not reported in a study, that complication was assigned a null value to avoid underestimation.
Results
Demographics and Baseline Characteristics
The PRISMA diagram for this review is shown in Figure 1. At the completion of screening, 26 studies were selected for full analysis (Table 1). Five were prospective,9,13–16 of which one was a randomized controlled trial.13 All others were retrospective. Comparison groups with differing surgical techniques were included in 6 studies.13,17–21,22 Second arms included the AGV (N = 2), BGI (N = 3), and PGI with mitomycin-C (MMC; N = 1). Mean follow-up for all studies ranged from 2 months to 35.8 months. Twelve studies had mean follow-up between 11 and 13 months, and five studies followed patients for 2–3 years. Eighteen studies were based solely in Europe, most commonly Germany (N = 5).14–31 Three publications were specific to Asian nations.32–34 Two studies were performed exclusively in the United Arab Emirates (UAE).35,36 Two studies involved sites in two nations, while a third publication described international collaborations across five nations.9,13,37 No patients were recruited from the United States.
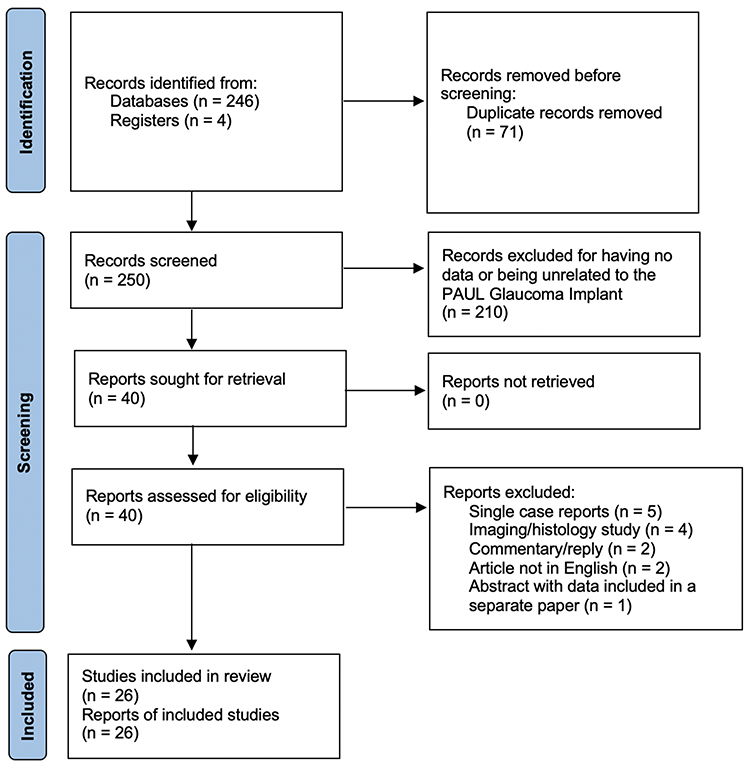 |
Figure 1 PRISMA Diagram for PAUL Glaucoma Implant Studies. Notes: PRISMA figure adapted from Page MJ, McKenzie JE, Bossuyt PM et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71.10 |
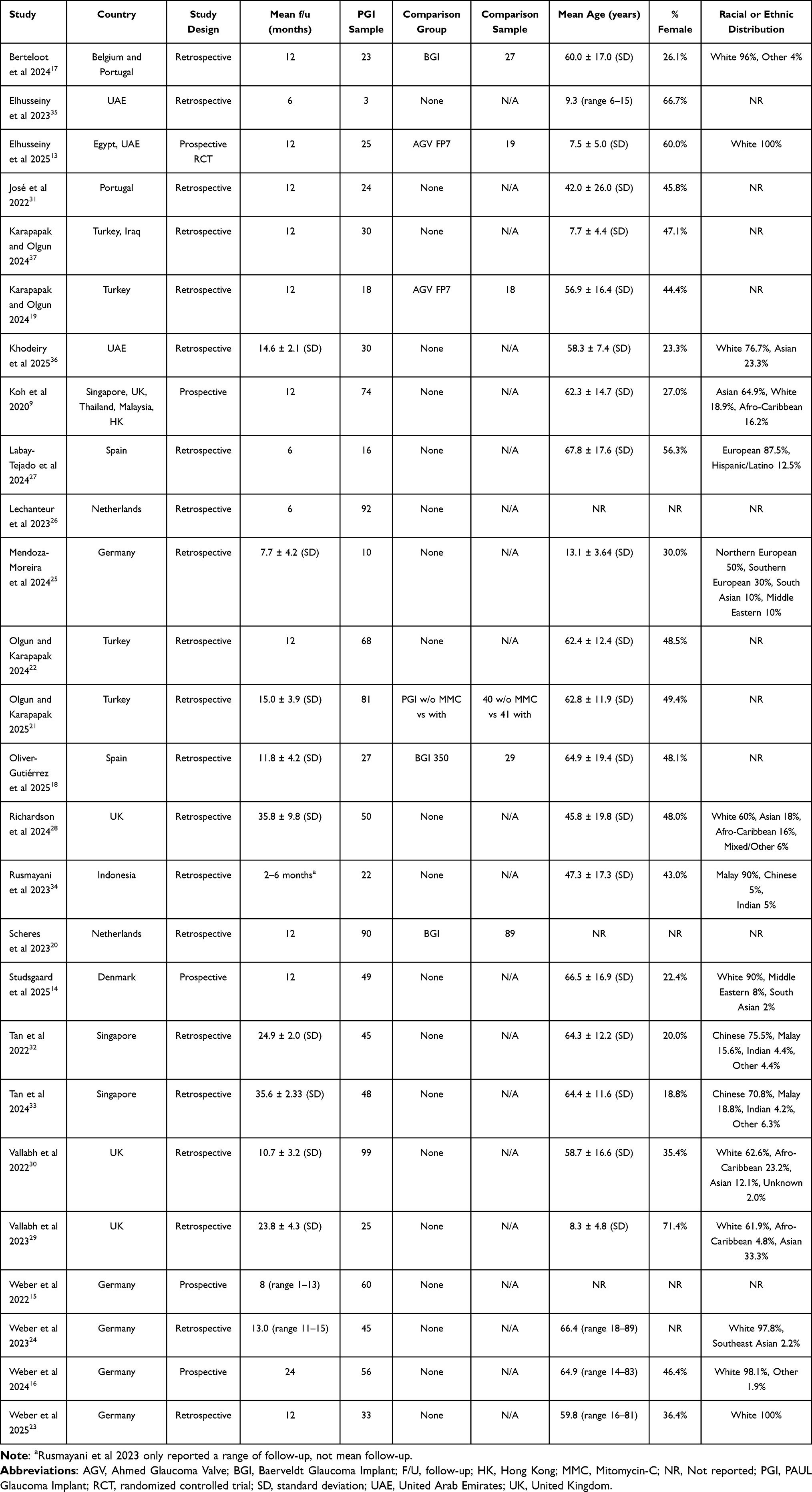 |
Table 1 Baseline Data in Studies of the PAUL Glaucoma Implant |
There were four first authors and one pair of authors who contributed multiple PGI publications. Marcus Tan, Abdelrahman Elhusseiny, and Neeru Vallabh each published two studies as first authors, and Constance Weber published four studies.13,15,16,23,24,29,30,32,33,35 The duo of Ali Olgun and Murat Karapapak published four studies.19,21,22,37 In total, 14/26 (53.8%) of the reviewed publications had Tan, Elhusseiny, Vallabh, Weber, or Olgun plus Karapapak listed.
Per-study sample sizes of PGI recipients ranged from 3 to 99. The median N was 39, and the total number of PAUL device implantations across all reviewed publications was 1143. The median age across studies was 59.8 years, with reported mean ages ranging from 7.5 to 67.8 years. Five protocols examined PGI use specifically in pediatric patients.13,25,29,35,37 Twelve studies were comprised of a 60% or greater proportion of white patients, while four had 65% or greater Asian representation. The remaining ten publications did not report race or ethnicity.18–22,26,30,31,35,37 Six studies specified PGI use for only a single classification of glaucoma; all others that described the glaucoma subtypes of their samples included multiple classes (Table 2). Previous glaucoma surgeries, where reported, were relatively common (522/901, 57.9%).
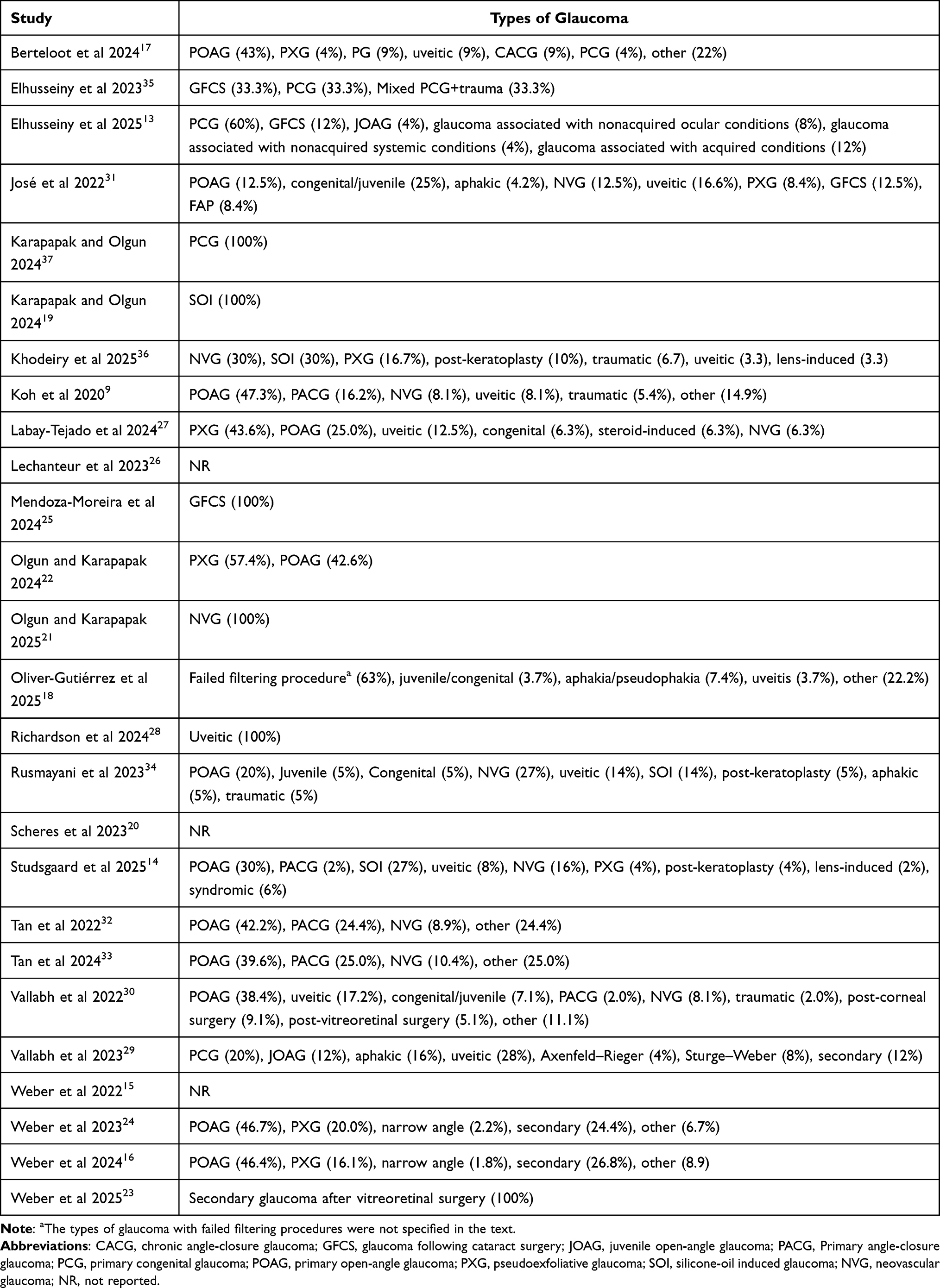 |
Table 2 Types of Glaucoma Included in Studies of the PAUL Glaucoma Implant |
Surgical Technique
Koh et al 2020 were the first to describe a PGI surgical technique.9 Conjunctiva and Tenon’s fascia are dissected in the quadrant of choice, with the end plate of the device tucked between the adjacent recti muscles and sutured 9–10 mm posterior to the limbus. A tract into the anterior chamber, parallel to iris, is then made using a 25- or 27-gauge needle. The tube is then trimmed, tunneled into the AC, and covered with a donor patch graft. Beyond these general steps, several factors were left to surgeon discretion in Koh et al’s protocol. Patch graft type, ligation sutures, suture tube occlusion (“ripcord”), viscoelastic filling, use of mitomycin-C (MMC), and extent of postoperative topical antibiotics and steroids were all operator-dependent.
This variability in surgical approach extended to subsequent studies (Table 3). Twenty papers (76.9%) described use of a 6–0 polypropylene ripcord suture threaded into the PGI lumen. The principle is that the suture obstructs some outflow in the early postoperative period to limit hypotony, whilst allowing for later removal to facilitate further IOP reduction. Criteria designating when the polypropylene stent would be removed were not uniform across studies, and often not specified. Rates of retained versus extracted ripcords accordingly varied. Furthermore, the ripcord was reported to cause a few cases of conjunctival erosion.14 Where specified, pericardial patch grafts were most commonly employed to reduce tube erosion risk (17/26 studies, 65.4%). Three studies used exclusively corneal grafts.14,35,36 Six studies utilized a mix of grafts, including various combinations of pericardium, cornea, sclera and fascia lata (Table 3).
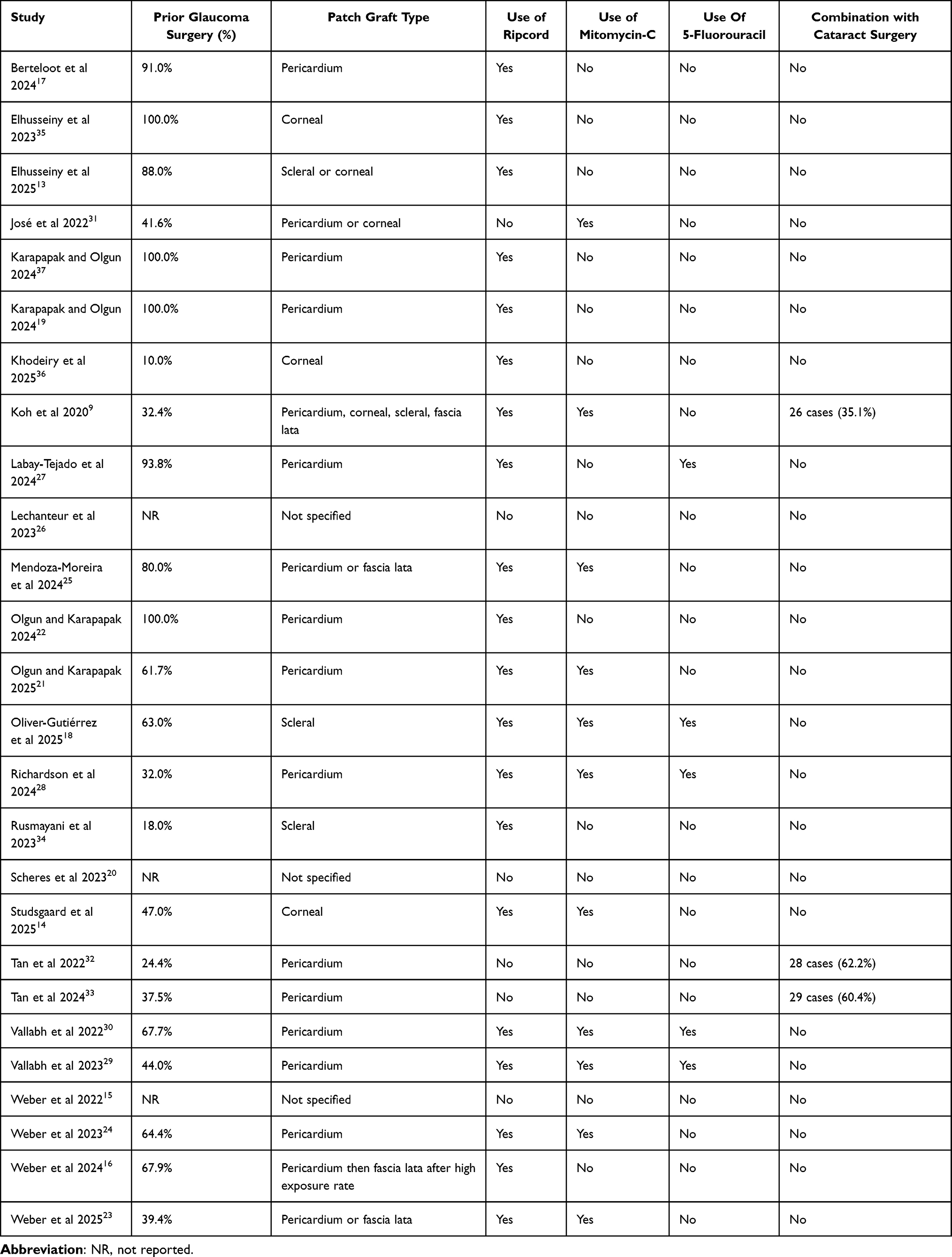 |
Table 3 PAUL Glaucoma Implant Surgical Data |
In terms of antifibrotics, 12 studies (46.2%) used MMC and/or 5-Fluorouracil (5-FU) with the goal of reducing bleb fibrosis rates. MMC was more frequently employed (N = 11). One study by Olgun and Karapapak 2025 retrospectively compared the PGI with MMC (N = 41) to no MMC (N = 40) in neovascular glaucoma patients through a year of follow-up.21 At baseline, the MMC arm had numerically more prior trabeculectomies (70.7% MMC (+) vs 52.5% MMC (-); p = 0.09). At postop month 1, IOP was lower in the MMC group (20.2 ± 7.7 MMC (-) vs 15.0 ± 3.7 mmHg MMC (+); p < 0.001). Regarding postoperative glaucoma medications, means were lower at every timepoint in the MMC group (p < 0.05 for all). The non-MMC group required significantly more cycloablative procedures in the follow-up period (25.0% (-) MMC vs 2.4% (+) MMC; p = 0.003). There were no statistically significant differences in success rates, month 12 IOP, vision changes, or complications. Mean time to ripcord suture removal was earlier in the non-MMC group (43.1 ± 44.1 days (-) MMC vs 158.4 ± 102.3 days (+) MMC; p < 0.001).
Three studies included patients who received concurrent cataract surgery.9,32,33 Of those, only Tan et al 2024 compared phaco (+) and phaco (-), finding no differences in rates of hypotony.33 Moreover, the two publications by Tan and et al described a unique approach to shielding the plate. An additional pericardial patch graft, undermined by viscoelastic, was placed between the plate and the subconjunctival space.32,33
Efficacy and Safety Outcomes
Twenty-two publications (84.6%) described surgical success as an endpoint (Table 4). Certain criteria for success were shared across many studies: an IOP 6 or above, no loss of light perception, no reoperation for glaucoma, and no explantation. The most commonly used IOP maximum threshold was ≤ 21 mmHg, followed by ≤ 18 mmHg. Minimum expected reduction from preop IOP was usually 20%, with a few protocols citing higher targets. Ten out of 22 studies (45.5%) did not include any percentage reduction requirement (Table 4). Most also distinguished between “complete” and “qualified” success. The former excluded postoperative ocular hypotensive use. At an IOP limit of 21 mmHg, the median qualified success rate was 92.0% (range 80.0–100.0%) and the median complete success rate was 48.0% (range 24.0–73.3%) (Table 5). At a limit of 18 mmHg, the median rates were 83.3% (75.0–94.0%) and 46.0% (30.0–75.0%), respectively.
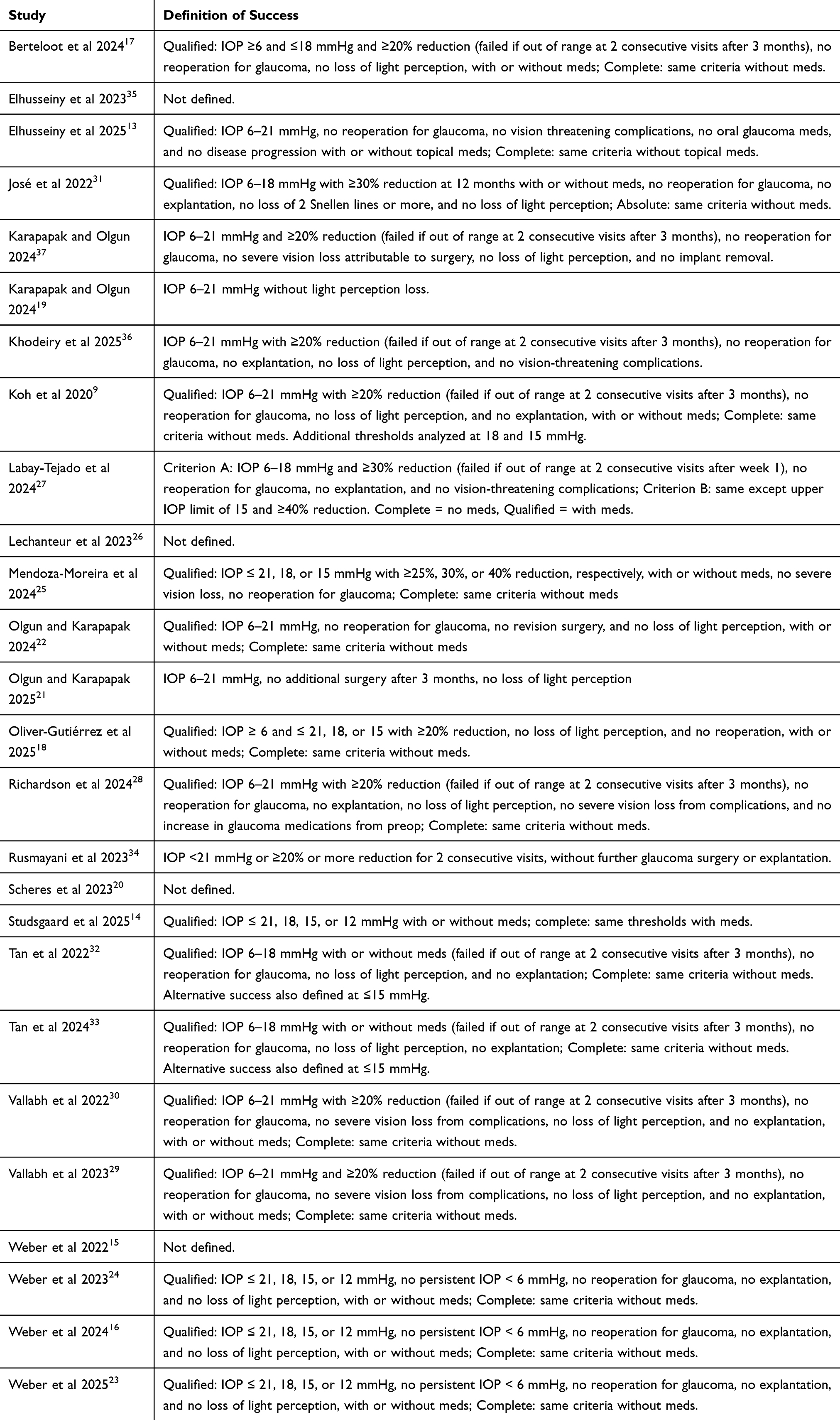 |
Table 4 PAUL Glaucoma Implant Success Criteria by Study |
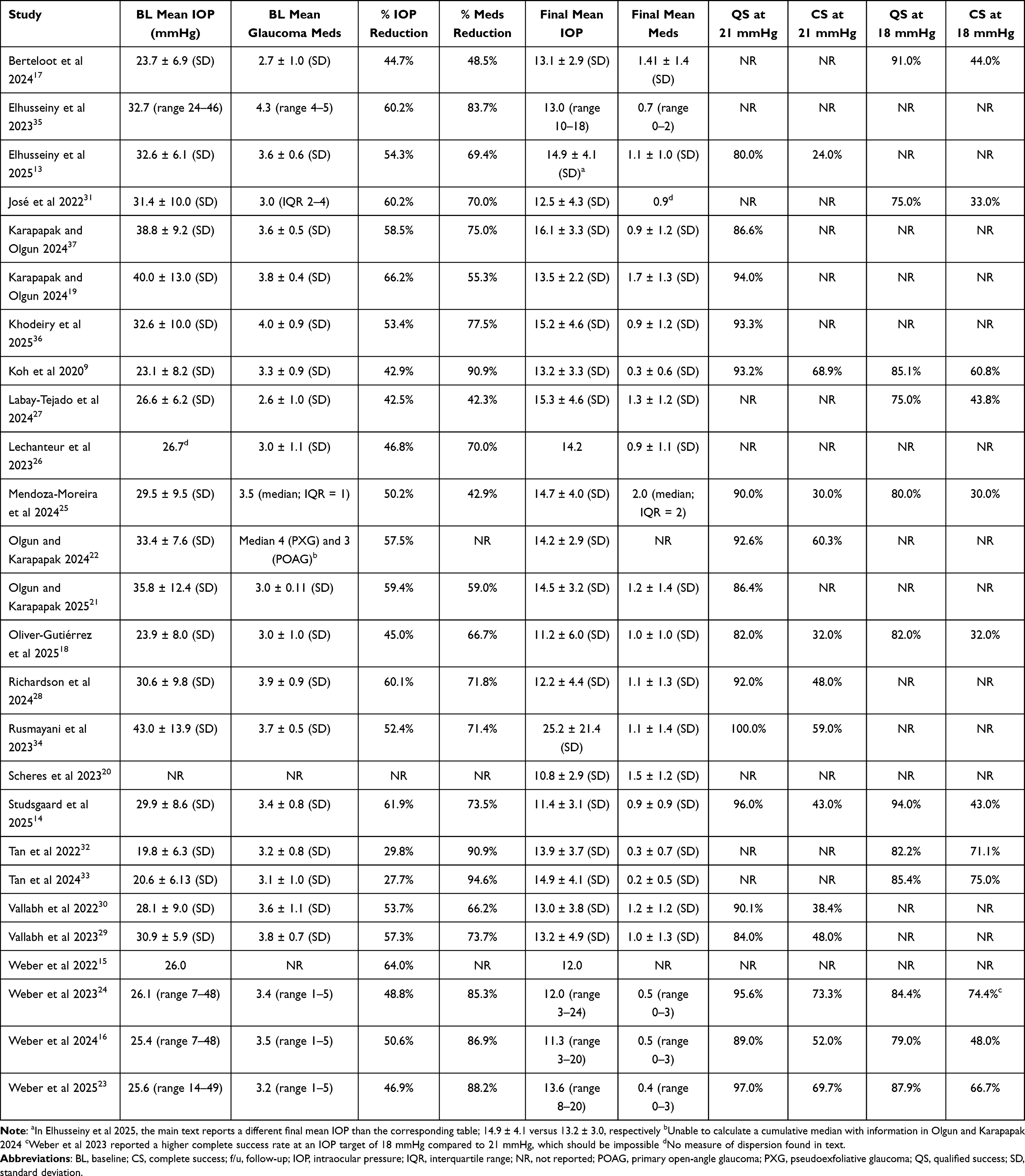 |
Table 5 Outcomes of the PAUL Glaucoma Implant |
From a median baseline IOP of 29.5 mmHg (range 19.8–43.0 mmHg), median IOP at last follow-up was 13.4 (range 10.8–25.2 mmHg) (Table 5). Median percentage IOP reduction was 53.4% (range 27.7–66.2%). From a median baseline 3.5 glaucoma medications (range 2.6–4.3), median meds at last follow-up was decreased to 1.0 (range 0.2–2.0). Median percentage reduction in medications was 71.8% (range 42.3–94.6%).
Complications for the PGI summed across all reporting studies are shown in Table 6. Though each publication reported individual complications, only eight studies specified the cumulative percentage of the sample with any complications.13,16,18,19,21,23–25 The summed complication rate across those eight papers was 28.8% (85/295 eyes). The most common individual complication was hyphema, occurring in 10.0% (76/759) of implantations. Numerical hypotony (IOP < 6 for at least one follow-up visit), where reported, occurred for 9.7% (68/701) of eyes. In terms of hypotony-related issues, maculopathy occurred at a rate of 1.8% (10/545), shallow anterior chamber at 5.9% (38/646), and choroidal effusions at 3.4% (27/805). Corneal decompensation occurred in 3.0% (7/230) of cases. Tube/plate issues varied; erosions were documented in 5.0% (45/900) of eyes, obstructions in 4.5% (27/599), tube-corneal touch in 2.3% (8/349), diplopia in 3.1% (16/523), and encapsulated blebs in 3.6% (7/196). Of note, tube erosion was reported more frequently in prospective studies (9.8%, 20/204 eyes prospective vs 3.6%, 25/696 eyes retrospective). A single case of endophthalmitis was reported (0.2%, 1/469). Complication-related reoperation rate was 8.3% (75/908).
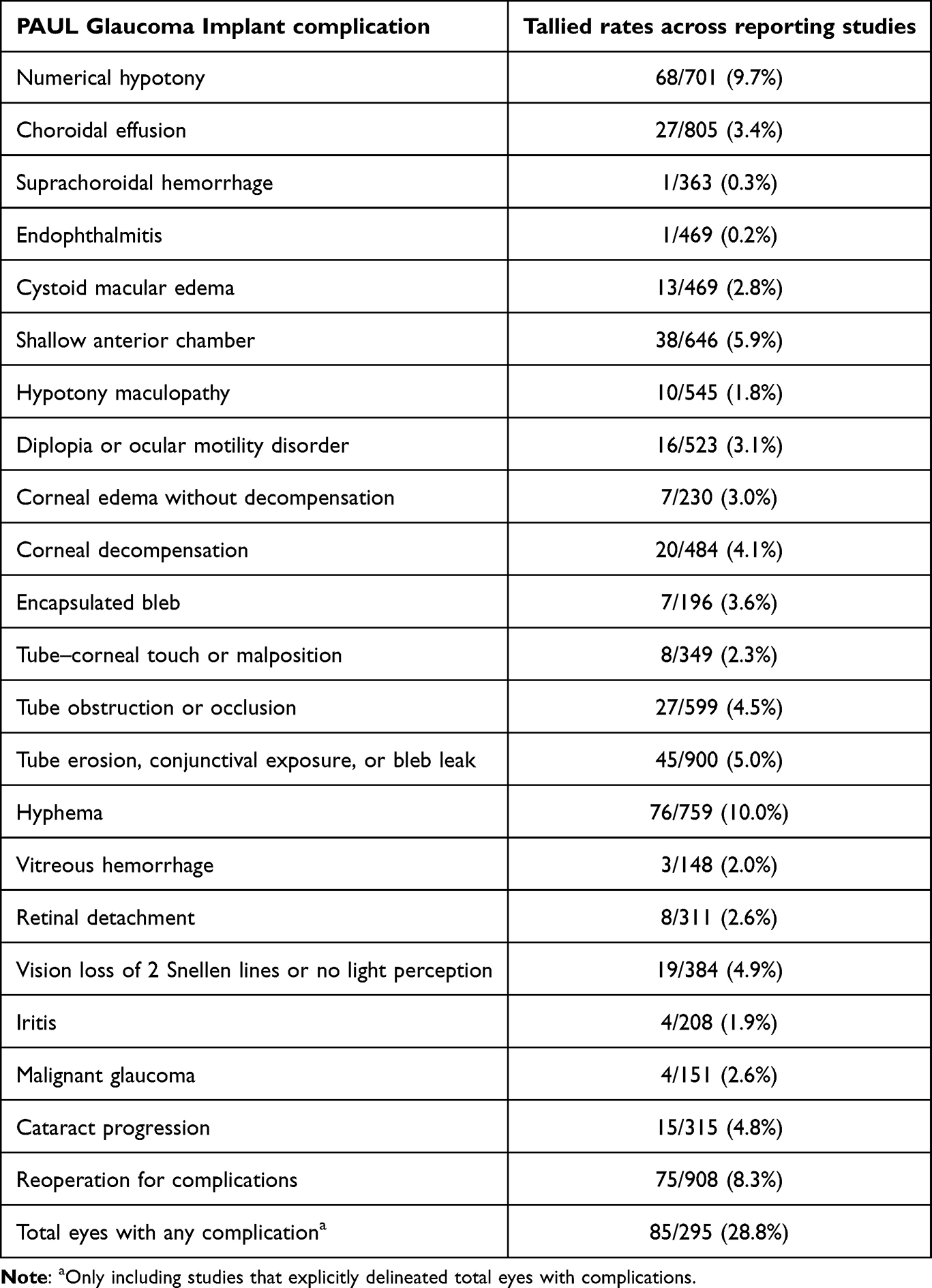 |
Table 6 PAUL Glaucoma Implant Complications aOnly Including Studies That Explicitly Delineated Total Eyes with Complications |
Comparative Studies Against the AGV and BGI
The sole RCT reviewed, the PAUL Ahmed Comparison study (PAC), compared 25 pediatric patients who received the PGI to 19 pediatric patients who received the AGV FP7.13 Antifibrotic agents were not used. Participants were followed for a year at sites in Egypt and the UAE. The study followed a per-protocol approach, with the two eyes that dropped out in the AGV group being excluded from analysis. At baseline, none of the metrics compared between groups were significantly different. The AGV group contained numerically more patients with glaucoma following cataract surgery (3 PGI vs 7 AGV), while the PGI group contained more patients who had glaucoma associated with ocular, systemic, or acquired conditions (6 PGI vs 0 AGV). IOPs were averaged from three rebound measurements. Mean IOP at postop month 1 was 5.6 mmHg greater in the PGI group compared to the AGV group (p = 0.003). At months 3, 6, and 12, there were no statistically significant differences in IOP, and the PGI group met prespecified noninferiority criteria. There were no statistically significant differences in medications or success rates at any time point. Complication rates were 12.0% in the PGI cohort and 15.7% for the AGV. The three complications for the PGI were tube extrusion, tube exposure, and flat anterior chamber. The three AGV complications included two cases of hypotony requiring AC reformation, and one event of endophthalmitis.
An additional four studies that compared the PGI to another tube were all retrospective. Karapapak and Olgun 2024 compared outcomes of the PGI (N = 18) to the AGV FP7 (N = 18) for silicone oil glaucoma.19 Antifibrotics were not used and baseline characteristics were similar. Success rates, IOP, and medication endpoints were similar between groups through one year of follow-up. Though the complication rate was higher for the AGV (44.4%) compared to the PGI (22.2%), this difference did not achieve statistical significance (p > 0.05).
The remaining three studies used the BGI as the second arm. Oliver-Gutierrez et al 2025 compared 27 PGI eyes to 29 BGI eyes, both implanted using MMC sponges and topical 5-FU, followed for an average period of 15.3 months.18 Two statistically significant baseline differences were noted: the PGI group more frequently had failed previous filtering surgery (63.0% PGI vs 31.0% BGI; p = 0.04) and more frequently had the tube placed in the anterior chamber (81.5% PGI vs 24.1% BGI; p < 0.01). No statistically significant differences were found for IOP at 1 year, medications at 1 year, success rates, complication rates, or vision changes. However, complete success rates at 12 months with an upper IOP threshold of 21 mmHg were lower for the PGI group (32.0% PGI vs 56.0% BGI, p = 0.22) and complication rates were higher (48.2% PGI vs 31% BGI, p = 0.15), but neither difference was significant. In the conference abstract from Scheres et al 2023, 90 PGI eyes were compared to 89 BGI eyes and followed for 1 year.20 At baseline, the BGI group had a higher mean IOP (p = 0.003) and a greater proportion of eyes with uveitic glaucoma (p = 0.02). Day 1 and week 1 IOPs were lower in the PGI group compared to the BGI (10.5 ± 8.7 and 11.7 ± 6.2 mmHg PGI vs 16.8 ± 12.5 and 13.7 ± 6.8 mmHg BGI; p < 0.05), however there were no significant differences in IOP at year one (p = 0.92). Numbers of medications and complications were similar. Berteloot et al 2024 examined 23 PGI eyes and 27 BGI eyes with 1 year of follow up.17 No statistically significant differences were noted in baseline characteristics, year 1 meds, success rates, vision changes, slit lamp interventions, or complications. The PGI group had lower IOP at week 1 (13.6 ± 6.1 PGI vs 20.1 ± 7.4 mmHg BGI, p = 0.002) and month 1 (14.6 ± 3.8 PGI vs 21.2 ± 5.8 mmHg BGI, p < 0.001), and furthermore required fewer medications at month 1 (1.6 ± 1.5 PGI vs 2.5 ± 1.2 BGI; p = 0.02). However, at 1 year the IOP trend reversed, with the BGI group having lower IOP (13.1 ± 2.9 PGI vs 10.4 ± 4.9 mmHg BGI; p = 0.02).
Discussion
In this review of 26 studies containing 1143 PGI implantations, efficacy outcomes were generally positive. Median complete and qualified success rates at an IOP upper limit of 21 were 48.0% and 92.0%, respectively; at a limit of 18 mmHg, they were 46.0% and 83.3%. Median reductions in IOP and glaucoma medications were 53.4% and 71.8%, respectively. Given that the most frequent length of PGI follow-up was a year, one can compare against the ABC and AVB studies at 1 year.11,12 The ABC study targeted a 21 mmHg upper threshold for success, while the AVB set a more aggressive 18 mmHg goal; other criteria were largely shared. The ABC study’s AGV group had a 19% complete success rate and an 84% qualified success rate. The BGI group had a 31% complete success rate and an 86% qualified rate. By comparison, the AVB study reported complete and qualified success for the AGV at 8% and 57%, respectively, while for the BGI rates were 17% and 72%.
Though it appears that the PGI success rates compare reasonably well to the BGI data from the ABC and AVB trials, such comparisons should be viewed with caution. Definitions of success across reviewed studies varied and in several instances were less stringent than the seminal tube trials (Table 4). For instance, only 54.5% (12/22) of PGI studies with success criteria required a reduction in IOP of 20% or more, and the number of visits during which IOP needed to remain within range was only occasionally specified. In both the ABC and AVB studies, success required two consecutive visits at or after 6 months with IOP in range. The AVB study had especially demanding complete criteria: not only no meds, but also a lack of vision loss of 2 Snellen lines or more and IOP targets met at every study visit from 3 months onwards. No PGI study replicated this full standard. Furthermore, four PGI studies that reported success had follow-up of less than a year, possibly contributing to inflated success rates.25,27,30,34
Regarding safety, the cumulative PGI complication rate across reporting studies was 28.8%. The most frequent individual complications were hyphema (10.0%), numeric hypotony (9.7%), shallow anterior chamber (5.9%), and tube erosion (5.0%). Hypotony-related sequelae such as maculopathy (1.8%), choroidal effusion (3.4%), and suprachoroidal hemorrhage (0.3%) were rare. Vision loss of two Snellen lines or more occurred in 4.9% of eyes in reporting studies. Only a single eye (0.2%) experienced endophthalmitis. Reoperation rate for complications was 8.3%. In the ABC study’s 1-year findings, overall complication rates were 43% for the AGV and 58% for the BGI.12 In the AVB study, rates were 45% for the AGV and 54% for the BGI.11 For most individual complications, the reported PGI data appears to compare favorably to both the AGV and BGI. A key exception is tube erosions. Overall tube erosion rates in both the ABC and AVB studies were 1% and 2%, respectively.11,12 In contrast, rates for the PGI were higher, particularly among prospective studies (9.8%). This difference may be reflective of the greater tendency to utilize MMC in PGI implantation (no tubes in the ABC or AVB studies received MMC) and/or differences in plate design.
However, just as with success rates, comparing complication rates has its limitations. For the current review, complications were tallied from a source only when the study at least alluded to monitoring the complications in question. This rule was used to avoid underestimation. Regardless, certain complications may still have been underrepresented. For instance, corneal changes were typically only reported when there was decompensation, not edema. Vision in the postop period was often reported as average or median changes rather than tallied into eyes that lost 2 lines or more. Most studies failed to disclose reoperation and overall complication rates. On the other hand, certain other complications may have been overestimated by the current study’s methodology. Serious adverse events, such as endophthalmitis, would presumably be monitored for in any study even if not made explicit.
It would thus be more optimal to have high-quality, prospective comparative studies of the PGI. At the time of writing, there has been just a single RCT of the PGI published, the PAC study.13 Though the PAC study found noninferiority for the PGI arm, it had several limitations: small sample size, just one year of follow-up, a purely pediatric sample recruited from Egypt and the UAE, per-protocol design, baseline differences in glaucoma types that approached statistical significance, and IOP levels that were only averaged from three rebound measurements. Aside from that RCT, the four studies that directly compared the PGI to an AGV or BGI were each retrospective and in adult populations. The one comparison of the PGI and AGV occurred in the very specific clinical circumstance of silicone oil glaucoma, with a trend towards fewer complications in the PGI arm that did not reach statistical significance.19 For the three PGI vs BGI studies, few meaningful differences in outcomes were seen between groups. However, two of the three retrospective studies had significant differences in baseline characteristics between treatment arms, with clinical implications for the outcome measures.18,20 Thus, for surgeons weighing the PGI against the current standard of care, the utility of the few comparative studies is limited. At best, they point to no definitive benefits of the PGI.
PGI surgical techniques varied widely, with 76.9% of studies using a ripcord technique (with minimal uniformity in the timing of removal), 65.4% using pericardial patch grafts, and 46.2% employing antifibrotic agents. Each of these variations could have affected rates of events such as hypotonous sequelae and tube exposure. Weber et al 2024 remarked that after an inordinately high exposure rate with pericardium, their practice switched to facia lata grafts with improvement in outcomes.16 No other study remarked on similar adjustments. As for antifibrotics, the one retrospective study comparing MMC to no MMC use in neovascular glaucoma patients found generally better outcomes for the MMC group.21 Better IOP control overall likely was reflected in the lower medication use, later removal of the ripcord, and less need for follow-up cycloablation. However, the MMC group did have more tube exposure events (9.8% vs 0.0%), possibly reflecting increased conjunctival thinning from the antifibrotic. There has been some interest in using MMC to reduce the rates of the hypertensive phase in AGV surgeries, so further research into its use in PGIs may be beneficial.38
In sum, the reviewed studies were heterogenous with several limitations. Over half of the reviewed studies listed one of six researchers (Tan, Elhusseiny, Vallabh, Weber, Olgun, or Karapapak) as a first author. With multiple studies from the same clinicians, risks of bias and sample overlap are increased. No study contained more than 99 eyes that received the PGI. The median number of PGI surgeries was only 39. Merely five studies were prospective, with the remainder suffering from retrospective bias risks. The most common follow-up duration was just one year, with the longest period of follow-up being a single study at 3 years. Most studies looked at implantations in a potpourri of glaucoma subtypes, without sufficient power to determine which subtypes the device may be most efficacious for. Five studies focused on purely pediatric patients, whereas the ABC and AVB studies each excluded pediatric patients. Patient populations were predominantly White or Asian, limiting applicability to other groups. Significant heterogeneity of included studies and lack of robust comparative evidence limit the utility of this article for guiding clinical practice. As for the current review’s methodology, it is principally limited by a lack of rigorous meta-analysis and a lack of formal bias assessment. Querying additional databases may have yielded further studies. And for any large-scale data extraction, risks for coding errors exist, even with multiple reviewers.
Conclusion
The PGI was conceptualized in part to combine the strengths of two popular tube shunts. In an ideal scenario, it would provide efficacy at or above the level of the BGI, whilst offering a safety profile comparable or even favorable to the AGV. On one hand, the PGI’s reported success rates were high, and complications in general appeared relatively infrequent. On the other, with the many methodologic limitations of the currently published data that bias towards pro-PGI outcomes, it is difficult to reliably assess how the novel device compares to the current standard of care. The sole RCT available has poor generalizability and certain protocol challenges. The remaining retrospective comparative studies provide minimal compelling evidence to choose the PGI over other tubes. Moreover, a possible safety signal was seen in prospective PGI studies that reported high tube erosion rates, which may relate to antifibrotic use. Overall, there is need for high-quality RCTs in adults that compare the PGI against mainstream tubes and that compare different PGI surgical approaches.
Disclosure
Malik Kahook and Leonard K. Seibold are consultants to New World Medical, which produces the Ahmed Glaucoma Valve. Also, Leonard K. Seibold is a consultant to Abbvie and Thea. The other authors have no relevant conflicts of interest to declare.
References
1. Gedde SJ, Vinod K, Wright MM, et al. Primary open-angle glaucoma preferred practice pattern®. Ophthalmology. 2021;128(1):P71–p150. doi:10.1016/j.ophtha.2020.10.022
2. Gedde SJ, Schiffman JC, Feuer WJ, Herndon LW, Brandt JD, Budenz DL. treatment outcomes in the tube versus trabeculectomy (tvt) study after five years of follow-up. Am J Ophthalmol. 2012;153(5):789–803.e782. doi:10.1016/j.ajo.2011.10.026
3. Tseng VL, Coleman AL, Chang MY, Caprioli J. Aqueous shunts for glaucoma. Cochrane Database Syst Rev. 2017;7(7):Cd004918. doi:10.1002/14651858.CD004918.pub3
4. Christakis PG, Kalenak JW, Tsai JC, et al. The Ahmed versus Baerveldt study five-year treatment outcomes. Ophthalmology. 2016;123(10):2093–2102. doi:10.1016/j.ophtha.2016.06.035
5. Christakis PG, Zhang D, Budenz DL, Barton K, Tsai JC, Ahmed IIK. Five-year pooled data analysis of the Ahmed Baerveldt comparison study and the ahmed versus baerveldt study. Am J Ophthalmol. 2017;176:118–126. doi:10.1016/j.ajo.2017.01.003
6. Budenz DL, Barton K, Gedde SJ, et al. Five-year treatment outcomes in the Ahmed Baerveldt comparison study. Ophthalmology. 2015;122(2):308–316. doi:10.1016/j.ophtha.2014.08.043
7. Grover DS, Kahook MY, Seibold LK, et al. Clinical outcomes of Ahmed clearpath implantation in glaucomatous eyes: a novel valveless glaucoma drainage device. J Glaucoma. 2022;31(5):335–339. doi:10.1097/IJG.0000000000002013
8. Shalaby WS, Reddy R, Wummer B, et al. Ahmed clearpath vs. baerveldt glaucoma implant: a retrospective noninferiority comparative study. Ophthalmol Glaucoma. 2024;7(3):251–259. doi:10.1016/j.ogla.2023.12.006
9. Koh V, Chew P, Triolo G, Lim KS, Barton K, PGIS G. Treatment outcomes using the PAUL glaucoma implant to control intraocular pressure in eyes with refractory glaucoma. Ophthalmol Glaucoma. 2020;3(5):350–359. doi:10.1016/j.ogla.2020.05.001
10. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
11. Christakis PG, Kalenak JW, Zurakowski D, et al. The Ahmed versus baerveldt study one-year treatment outcomes. Ophthalmology. 2011;118(11):2180–2189. doi:10.1016/j.ophtha.2011.05.004
12. Budenz DL, Barton K, Feuer WJ, et al. Treatment outcomes in the Ahmed baerveldt comparison study after 1 year of follow-up. Ophthalmology. 2011;118(3):443–452. doi:10.1016/j.ophtha.2010.07.016
13. Elhusseiny AM, Khaled OM, Chauhan MZ, Sayed MS, Shaarawy T. Initial results of the Paul Ahmed Comparison (PAC) study in refractory childhood glaucoma. Am J Ophthalmol. 2025;271:71–78. doi:10.1016/j.ajo.2024.10.024
14. Studsgaard A, Nielsen SE, Telinius N. One tube for all: 1-year outcomes after transition to Paul glaucoma implant at a tertiary centre. Acta Ophthalmologica. 2025;103:461–468. doi:10.1111/aos.17443
15. Weber C, Liegl R, Holz FG, Mercieca K. Real-world outcomes following Paul Glaucoma Implant (PGI) surgery. Invest Ophthalmol Visual Sci. 2022;63(7).
16. Weber C, Hundertmark S, Stasik I, Holz FG, Mercieca K. Two-year clinical outcomes of the PAUL glaucoma implant in white patients with refractory glaucoma. J Glaucoma. 2024;33(10):808–814. doi:10.1097/IJG.0000000000002457
17. Berteloot S, Barao RC, Pinto LA, Vandewalle E, Stalmans I, Lemmens S. treatment outcomes comparing the paul and baerveldt glaucoma implants after one year of follow-up. J Glaucoma. 2024;33(8):594–600. doi:10.1097/IJG.0000000000002366
18. Oliver-Gutiérrez D, Segura-Duch G, Ávila-Marrón E, Arciniegas-Perasso CA, Duch-Tuesta S. Paul versus Baerveldt 350 glaucoma drainage implants: one-year comparative analysis. Indian J Ophthalmol. 2025;73(Suppl 2):S317–S323. doi:10.4103/IJO.IJO_2595_24
19. Karapapak M, Olgun A. One-year outcomes of the PAUL glaucoma implant compared with the Ahmed glaucoma valve for the treatment of silicone oil glaucoma. J Glaucoma. 2024;33(5):310–316. doi:10.1097/IJG.0000000000002360
20. Scheres LMJ, Komljanc EP, Berendschot T, Beckers HJM. One year outcomes of the PAUL glaucoma implant in comparison to the Baerveldt glaucomaimplant for glaucoma. Acta Ophthalmologica. 2023;101:17.
21. Olgun A, Karapapak M. Impact of mitomycin C on surgical outcomes of PAUL glaucoma implant in neovascular glaucoma: 12-month follow-up results. Eur J Ophthalmol. 2025;35:1305–1313. doi:10.1177/11206721251313835
22. Olgun A, Karapapak M. Assessing the Efficacy of the PAUL glaucoma implant in pseudoexfoliative glaucoma. Beyoglu Eye J. 2024;9(1):26–32. doi:10.14744/bej.2024.96729
23. Weber C, Schipper P, Walz W, et al. Clinical outcomes of the PAUL® glaucoma implant for secondary glaucoma after vitreoretinal surgery. Ophthalmologica;2025. 1–23. doi:10.1159/000543748
24. Weber C, Hundertmark S, Liegl R, et al. Clinical outcomes of the PAUL® glaucoma implant: one-year results. Clin Exp Ophthalmol. 2023;51(6):566–576. doi:10.1111/ceo.14235
25. Mendoza-Moreira AL, Voigt AM, Stingl JV, et al. Paul glaucoma implant following congenital cataract surgery in a pediatric cohort. J Clin Med. 2024;13(10):2914. doi:10.3390/jcm13102914
26. Lechanteur YTE, Nobacht S, Kersten E. Six-month treatment outcomes using the PAUL glaucoma implant at radboud university medical center. Acta Ophthalmologica. 2023;101:19–20.
27. Labay-Tejado S, Ventura-Abreu N, Porto-Castro S, et al. Early safety and efficacy outcomes of the PAUL glaucoma implant in a Spanish population: a retrospective study. Saudi J Ophthalmol. 2024;38(4):368–373. doi:10.4103/sjopt.sjopt_164_24
28. Richardson J, Tacea F, Yu JAT, Yau K, Fenerty C, Au L. The PAUL Glaucoma Implant in the management of uveitic glaucoma-3-year follow-up. Eye. 2024;39:931–937. doi:10.1038/s41433-024-03527-x
29. Vallabh NA, Mohindra R, Drysdale E, Mason F, Fenerty CH, Yau K. The PAUL® glaucoma implant: 1-year results of a novel glaucoma drainage device in a paediatric cohort. Graefes Arch Clin Exp Ophthalmol. 2023;261(8):2351–2358. doi:10.1007/s00417-023-06000-9
30. Vallabh NA, Mason F, JTS Y, et al. Surgical technique, perioperative management and early outcome data of the PAUL® glaucoma drainage device. Eye. 2022;36(10):1905–1910. doi:10.1038/s41433-021-01737-1
31. José P, Barão RC, Teixeira FJ, et al. One-Year efficacy and safety of the PAUL glaucoma implant using a standardized surgical protocol. J Glaucoma. 2022;31(3):201–205. doi:10.1097/IJG.0000000000001969
32. Tan MCJ, Choy HYC, Chang VKT, et al. Two-year outcomes of the Paul glaucoma implant for treatment of glaucoma. J Glaucoma. 2022;31(6):449–455. doi:10.1097/IJG.0000000000001998
33. Tan MCJ, Ong CW, Aquino MC, et al. Three-year outcomes of the Paul glaucoma implant for treatment of glaucoma. J Glaucoma. 2024;33(7):478–485. doi:10.1097/IJG.0000000000002369
34. Rusmayani E, Viona V, Soebijantoro I, et al. Early experience with the novel glaucoma shunt device: Paul glaucoma implant in the Indonesian populations. Int Eye Sci. 2023;23(10):1603–1608.
35. Elhusseiny AM, Khodeiry MM, Lee RK, Shaarawy T, Waqar S, Sayed MS. Early experience with the Paul glaucoma implant in childhood glaucoma: a case series. Clin Ophthalmol. 2023;17:1939–1944. doi:10.2147/OPTH.S414183
36. Khodeiry MM, Hassan AK, Elhusseiny AM, Lee RK, Sayed MS. Outcomes of the Paul glaucoma implant in refractory secondary glaucoma. Clin Ophthalmol. 2025;19:167–174. doi:10.2147/OPTH.S505220
37. Karapapak M, Olgun A. Efficacy and safety of the Paul glaucoma implant in the treatment of refractory primary congenital glaucoma. Japanese J Ophthalmol. 2024;68(5):571–577. doi:10.1007/s10384-024-01076-0
38. Perez CI, Verdaguer S, Khaliliyeh D, Maul EA, Ou Y, Han Y. Subconjunctival injections of mitomycin C are associated with a lower incidence of hypertensive phase in eyes with Ahmed glaucoma valve. Ophthalmol Glaucoma. 2021;4(3):322–329. doi:10.1016/j.ogla.2020.10.004
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Efficacy and Safety of Anlotinib in Extensive-Stage Small Cell Lung Cancer: A Multicenter Real-World Study
Zheng HR, Jiang AM, Gao H, Liu N, Zheng XQ, Fu X, Zhang R, Ruan ZP, Tian T, Liang X, Yao Y
Cancer Management and Research 2022, 14:2273-2287
Published Date: 2 August 2022
Relative Safety and Efficacy of Two Doses of Tandospirone Citrate for Generalized Anxiety Disorder: A Multicenter Randomized Controlled Trial
Li Q, Zhang H, Lin G, Shi S, Zhang Y, Ji J, Yang L, Yao J, Wu W
Neuropsychiatric Disease and Treatment 2022, 18:1653-1664
Published Date: 8 August 2022
Biosimilars: Science, Implications, and Potential Outlooks in the Middle East and Africa
Batran RA, Elmoshneb M, Hussein AS, Hussien OM, Adel F, Elgarhy R, Morsi MI
Biologics: Targets and Therapy 2022, 16:161-171
Published Date: 6 October 2022
Efficacy and Safety of Empagliflozin in Patients with Type 2 Diabetes Mellitus Fasting During Ramadan: A Real-World Study from Bangladesh
Pathan MF, Akter N, Selim S, Saifuddin M, Qureshi NK, Kamrul-Hasan ABM, Hannan MA, Ahmed MAU, Mustari M, Chakraborty AK
Diabetes, Metabolic Syndrome and Obesity 2022, 15:4011-4021
Published Date: 22 December 2022
Clinical Evaluation of Risankizumab in the Treatment of Adults with Moderately to Severely Active Crohn’s Disease: Patient Selection and Reported Outcomes
Horst S, Cross RK
Drug Design, Development and Therapy 2023, 17:273-282
Published Date: 31 January 2023