Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
The Efficacy of a Preoperative Occupational Therapy Educational Session for Saudi Patients Undergoing a Lower Extremity Joint Replacement
Authors Al-Heizan MO ![]() , Shoman A, Tawffeq A, Banamah A, Balkhair F, Filimban S, Alsinan W, Batouk O
, Shoman A, Tawffeq A, Banamah A, Balkhair F, Filimban S, Alsinan W, Batouk O ![]() , Turkistani T
, Turkistani T
Received 25 October 2022
Accepted for publication 4 January 2023
Published 10 January 2023 Volume 2023:16 Pages 31—38
DOI https://doi.org/10.2147/JMDH.S394761
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Muhammad O Al-Heizan,1 Amna Shoman,2 Abdullah Tawffeq,3 Ansam Banamah,4 Fanar Balkhair,5 Shahd Filimban,4 Walla Alsinan,3 Omar Batouk,6 Taghreed Turkistani7
1Department of Rehabilitation Sciences, College of Applied Medical Sciences, King Saud University, Riyadh, Saudi Arabia; 2Saudi Autistic Society, Jeddah, Saudi Arabia; 3King Khalid National Guard Hospital, King Abdulaziz Medical City, Jeddah, Saudi Arabia; 4Sinad City for Special Education, Makkah, Saudi Arabia; 5Children with Disability Association, Makkah, Saudi Arabia; 6College of Medicine, King Saud bin Abdulaziz University for Health Sciences, Jeddah, Saudi Arabia; 7Occupational Therapy Department, Armed Forces Center for Health Rehabilitation, Taif, Saudi Arabia
Correspondence: Muhammad O Al-Heizan, Department of Rehabilitation Sciences, College of Applied Medical Sciences, King Saud University, Riyadh, 11433, Saudi Arabia, Tel +966 503483618, Email [email protected]
Purpose: Prior to a lower extremity joint replacement, many surgical candidates participate in a preoperative occupational therapy educational program that is meant to increase patient awareness, promote positive health behaviors, and improve health outcomes after surgery. With the limited number of occupational therapists in Saudi Arabia, patients may only receive one preoperative educational session. The objective of the study was to explore the efficacy of one preoperative occupational therapy educational session for patients undergoing a lower extremity joint replacement.
Methods: A total of 19 participants were included in the study, 7 participants to the intervention and 12 participants to the control groups. Participants underwent either a total knee or total hip replacement. The intervention group received one preoperative educational session prior to the surgery and the control group received usual care. After the surgery, both groups were assessed on pain (SF-MPQ), Satisfaction (SPSQ), Quality of life (QOLS), functional performance (FIM). Mann–Whitney U-tests were used to compare between groups.
Results: The findings showed significant improvements in both pain (12.14 ± 7.22 vs 21.25 ± 8.60; p=0.02) and satisfaction (106.28 ± 25.17 vs 78.08 ± 31.49; p=0.03) when compared to usual care. Although both FIM and QOLS scores indicated improvements when compared to usual care, these results were not statistically significant. Effect sizes showed moderate and large effects for score differences on both the SF-MPQ and SPSQ (r= 0.47, r=0.52) respectively. Whereas effect sizes for score differences on both the FIM and QOLS were small.
Conclusion: An occupational therapy preoperative education session shows promise for patients undergoing lower extremity joint replacement; however, further research is needed to confirm these findings.
Keywords: joint replacement, education, occupational therapy, pain, satisfaction, quality of life, FIM
Introduction
The number of people living with complete hip or knee replacement is significantly high. In the United States alone, the number of people impacted by either a hip or knee replacement is reported to be equivalent to those impacted by stroke and myocardial infarction, and rates are projected to increase in the upcoming years.1,2 In Saudi Arabia, there has not been any published literature on the prevalence of a hip or knee replacement. However, public knowledge of these type of issues is high.3 These numbers highlight the importance of finding efficient and effective approaches to address the associated issues that impact people with hip or knee replacement.
In order to avoid negative side effects or a decline in function, many surgical candidates participate in preoperative educational programs.4 The rehabilitation team, including occupational therapists facilitate education programs to increase patient awareness, facilitate positive health behaviors, and improve medical and functional outcomes after surgery. The occupational therapist role in the team typically includes training on activities of daily living, and postoperative pain management.5 An educational program may include anxiety management, pain management, educating about post-operation management such as providing the needed assistive device, providing educational session for the provided assistive device, and home modification to prevent falls.6
An important topic that is discussed during an educational program includes the potential stress and psychosocial complications associated with surgery. These psychosocial factors can negatively impact a patient’s functional outcomes, and pain after surgery.7 Moreover, it has been found that increasing patient awareness, and education about the prognosis significantly reduces pain, increases function, which in turn decreases length of hospital stay post-surgery.8,9 It has been demonstrated that this educational preparation is most effective when presented in the form of handouts, photos, videos, slide shows, and patient group discussion.10,11
In addition to psychosocial factors, preoperative education programs have also had a positive impact on functional performance factors. A recent study reported that patients that underwent a total knee replacement (TKR) and received preoperative education had a decrease in number of falls postoperatively.12 This reduction in falls has been reported to increase patient’s functional performance in daily life, improve overall safety, decrease the risk of reinjury, and improve overall quality of life.13,14
Pain is another important factor that has also been addressed in previous research that explored educational programs with mixed findings. A recent study demonstrated no significant differences between groups in pain level, length of stay, and complication rate, despite experiencing less anxiety before the surgery and reported ability to manage the pain after surgery.15 On the contrary, a preoperative educational program showed better physical functioning, pain relief and greater satisfaction,16 and more awareness of the precautions with ADLs and satisfaction, which decreased anxiety and improved pain management as well as having a positive impact on performance outcomes and quality of life in postoperative patients.17 These factors support the viability of preoperative education for surgical candidates. To our knowledge, there are currently no studies that explored the impact of a pre-operative occupational therapy educational program or session in Saudi Arabia. This study is the first study that combines all factors that have been discussed above.
In Saudi Arabia, occupational therapy is a relatively new profession with a limited number of occupational therapists working in clinical settings.18 This increases the ratio of therapist per patient which in turn reduces the number of time/sessions a therapist can have with a patient. This increase in ratio and reduction in time and/or amount of therapy sessions may also impact the conditions that have priority for occupational therapy services. For these reasons, patients undergoing a Total Knee or Hip Replacement may not have the ability to be seen by occupational therapy prior to surgery, with some having only one session with occupational therapy prior to surgery. This warrants the need for exploring whether only one preoperative occupational therapy session can improve patient level of function in ADLs, and management of pain after surgery which may lead to overall satisfaction and better quality of life.
The purpose of this study was to examine the feasibility of implementing one preoperative occupational therapy educational session for patients undergoing a lower extremity joint replacement. We hypothesized that the use of a preoperative occupational therapy educational session would improve functional outcomes, the ability to manage pain, satisfaction and overall quality of life post-surgery.
Materials and Methods
Study Design
This study used an experimental posttest-only control group design. Researchers considered this design to be appropriate due to the limited amount of time occupational therapists have with lower extremity joint replacement patients and the impracticality of administering outcome measures at pretest due to the possibility of sensitizing participants to the outcome measures which might influence their scores at posttest.19 The study was approved by the National Guard Hospital Affairs Institutional Review Board (JED-19-427780-120282). In addition, the study complies with the Declaration of Helsinki.
Participants
A total of 19 patients undergoing a knee or hip replacement surgery at the department of Orthopedic surgery were recruited for this study. Participants that agreed to participate provided an informed consent prior to their surgery.
The inclusion criteria were as follows: (1) 50 years of age or older and (2) a diagnosis with a condition that requires a total hip replacement (THR) or total knee replacement (TKR). Exclusion criteria were as follows: (1) required only a partial knee or hip replacement and (2) had any cognitive deficits that might prevent full participation and understanding of the educational session.
Procedures
This study was conducted over the course of 3 months at the Rehabilitation Center located at the National Guard Hospital Affairs (NGHA) in Jeddah, Saudi Arabia, from July 2019 to December 2019. Participants were allocated to either an intervention or control group using a convenient sampling method from a list of patients admitted to the orthopedic surgery unit by one of the researchers that was not involved in the administration of the outcome measures or the educational sessions. Those that we were able to administer the educational session on were allocated to the intervention group and those that we could not be allocated to the control group. This was due to the relatively short time between admission and surgery and researchers had limited time to recruit and allocate patients given the limited number of occupational therapists at the facility at the time the study was conducted. Therefore, participants were not blinded to group allocation. Educational sessions were conducted by trained occupational therapy students under the supervision of an experienced occupational therapist. The control group received their usual care from their orthopedic doctors and did not receive any preoperative occupational therapy education prior to their respective surgery.
The intervention group received usual care in addition to the preoperative educational program conducted by a trained occupational therapy student under the supervision of occupational therapist 1 day prior to surgery, then underwent their respective orthopedic surgery. Occupational therapy students applied the same educational methods with all patients, which was approved by the occupational therapist supervisor. Instructions included information on postoperative rehabilitation including care after surgery, managing complications, precautions, use of adaptive equipment for participation in activities of daily living (ADLs), as well as stress and pain management.20 The occupational therapists also provided a physical demonstration of how to perform ADLs while using adaptive equipment in the patients’ room at the orthopedic ward. The format of the education consisted of handouts, photos, videos, and patient/therapist discussion.
After surgery, researchers conducted the outcome measures with both the intervention and control groups 4–6 days post-surgery. All outcome measures were administered by trained occupational therapy students in the same order: the Functional Independence Measure, the short-form McGill Pain Questionnaire, Quality of Life Scale, then the Satisfaction with Performance Scaled Questionnaire.
Outcome Measures
Functional Independence Measure (FIM).21 The FIM is therapist-rated measure of an individual’s functional performance during daily tasks. The FIM assesses the individual’s degree of disability and need for assistance during these tasks on a scale of 0 to 7. Scoring was completed by a trained occupational therapist. Scores range from 0 to 126. Higher scores indicate better performance on the FIM. The FIM has established reliability and validity.22–25
The short-form McGill Pain Questionnaire (SF-MPQ).26 The SF-MPQ is a self-report measure used to measure level of pain after surgery. The SF-MPQ was developed as a short form of the McGill Pain Questionnaire (MPQ) which is a participant self-report scale that describes the nature and intensity of perceived pain and how this pain changes over time. Scores range from 0 to 45. Higher scores on the SF-MPQ indicate higher pain. The SF-MPQ has established reliability and validity with a variety of patient populations including patients with musculoskeletal conditions.27–31
The Quality of Life Scale (QOLS)32 is a self-report measure that was implemented to measure the physical, psychological, and social aspects of the participant’s quality of life. These factors were considered an important determinant in the individual’s success and positive outcomes during their postoperative course. Scores range from 7 to 112. A higher score indicates better quality of life. The QOLS has established reliability and validity.33,34
Satisfaction with Performance Scaled Questionnaire (SPSQ).35 The SPSQ is a self-report measure designed to determine the participants’ level of satisfaction with their performance of daily life activities. This assessment was used to measure how the individual perceives his or her own performance of occupations regardless of their actual performance in daily occupations. Scores range from 0 to 120. Higher scores indicate higher satisfaction. The measurement properties of the SPSQ have been established.35
Data Analysis
Descriptive statistics and frequency analysis were performed to describe the general characteristics of the study participants. A comparison between the two groups on age and gender was conducted to assure equivalency among the two groups. Given the small unequal sample size of the two groups, and the violation of the assumptions of normality and homogeneity of variance, the non-parametric Mann–Whitney U-test was used to compare the two groups on the four outcome measures. The level of significance was set at p < 0.05. To examine practical significance, effect sizes were calculated using the correlation coefficient (r).19 Cohen suggests effect sizes for r: small = 0.10, medium = 0.30, large = 0.50.36 All analyses were performed using R statistical software.37
Results
A total of 19 participants met the inclusion criteria for the study, 7 of which were in the intervention group, and 12 were in the control group. Most of the sample were female, and the two groups were similar in age. The two groups were not significantly different on both age and gender. Most participants underwent a unilateral or bilateral total knee replacement surgery with only one participant that underwent a total hip replacement surgery in the intervention group. See Table 1 for a detailed description of the characteristics of the two groups.
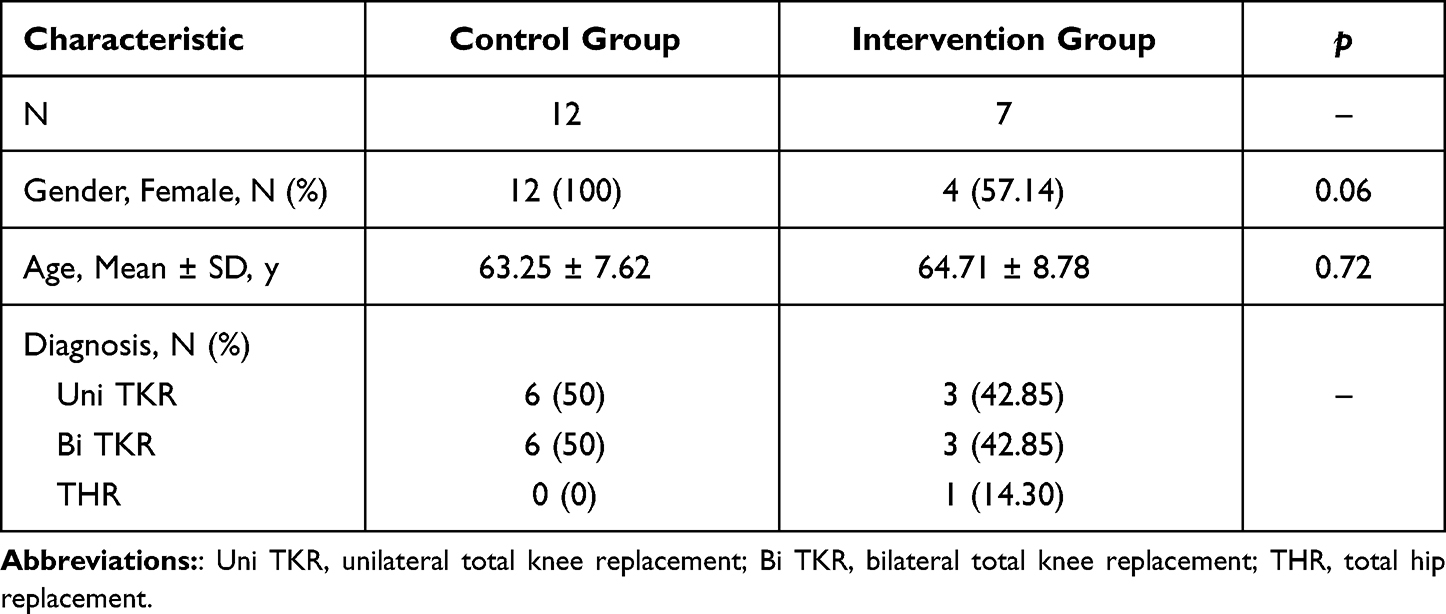 |
Table 1 General Characteristics of Subjects (N=19) |
The analyses demonstrated statistically significant differences among groups on both pain and satisfaction. The intervention group had a better mean MPQ score (M = 12.14 ± 7.22) than the control group (M = 21.25 ± 8.60). Similarly, the intervention group also had a higher mean SPSQ score (M = 106.28 ± 25.17) than the control group (M = 78.08 ± 31.49). The effect size for both the MPQ and the SPSQ score differences were moderate (r = 0.47) and large (r = 0.52), respectively.
On the other hand, comparison of the two groups on both functional and quality of life measures did not yield statistically significant results. The effect sizes for both the FIM and the QOLS score differences were small. See Table 2 for the full results of the comparison of the two groups on the four outcome measures.
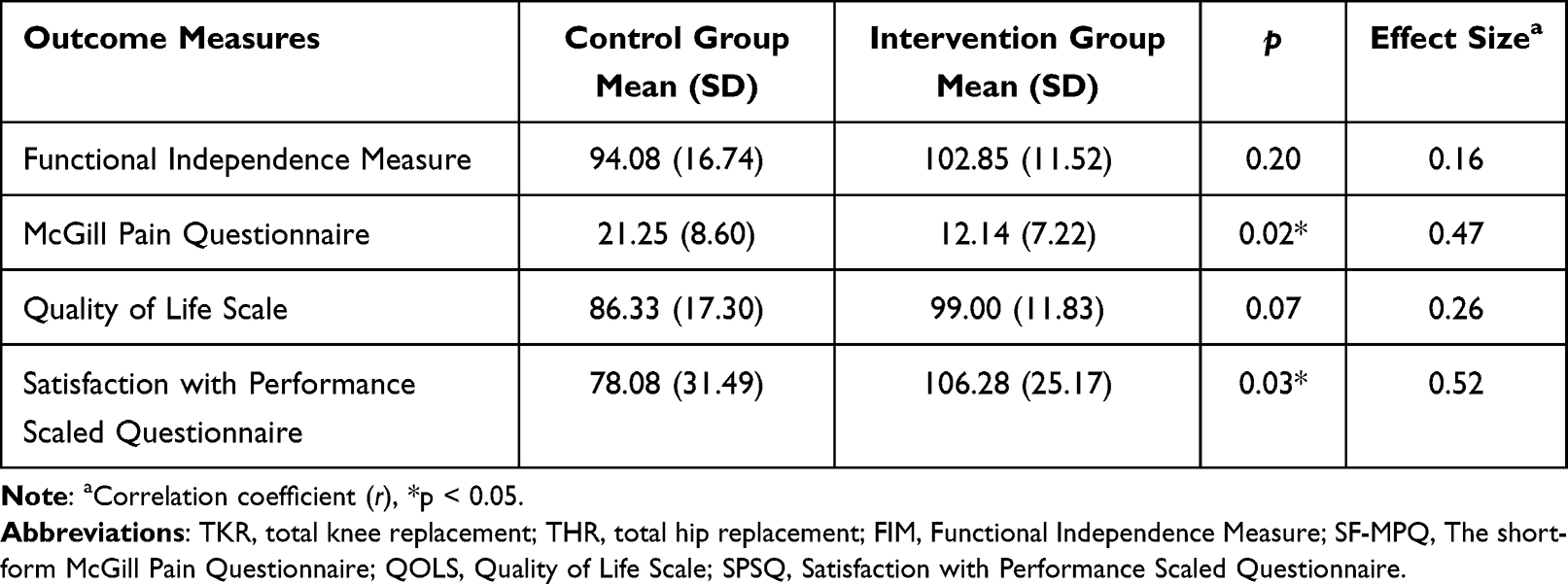 |
Table 2 Comparison of Groups on Outcome Measures Using Mann–Whitney U-Tests |
Discussion
This study aimed to explore the efficacy of a preoperative occupational therapy educational session to improve functional independence, pain, satisfaction, and overall quality of life post-surgery for patients with lower extremity joint replacement. The results of this study indicated that when compared to a control group, the implementation of a preoperative occupational therapy educational session significantly improved pain and satisfaction in patients after lower extremity joint replacement surgery. Whereas functional performance and QOLS did not show significant improvements.
The results of the current study indicated that patients that received a single occupational therapy educational session had improved pain and self-perceived satisfaction in occupational performance after a TKR or THR. In addition, the effect sizes indicated medium-to-large effects for both pain and satisfaction. A recent systematic review found that preoperative education particularly by occupational therapy improved pain and self-reported outcomes after TKR, specifically interventions targeting psychological distress.38 The intervention group in our study received methods to manage stress which may have had an impact on pain and satisfaction. Further, McDonald et al report that pain may also be improved as a result of preoperative education compared to no education.11 However, their results indicated that improvements in pain may be more apparent after hip replacement surgeries than knee replacement surgeries. Further, Chen et al39 reported that a preoperational educational intervention reduced the level of pain in patients who undergone a TKR. To our knowledge, our study is the first to show the impact of a preoperative occupational therapy educational session on self-perceived satisfaction during occupational performance after a lower extremity joint replacement, which we deemed necessary to explore given that the study investigated the impact of an occupational therapy educational session. A previous study showed that preoperative intervention may improve patient anticipated satisfaction after a lower extremity joint replacement surgery.9
Our results also did indicate that the intervention group had better functional independence on the FIM and QOLS, however these differences were not statistically significant. However, the effect sizes showed small-to-medium effect suggesting possible practical/clinical significance. Similar results were found by Moulton et al,40 preoperative education did not impact function post-operation in patients with a TKR as much as patients with a THR. These findings are consistent with the results of the current study given that our sample had only one participant who has undergone a THR. In addition, function did not seem to be affected by preoperative rehabilitation that focused on exercise and education in patients with TKR or THR.41 A possible explanation for these findings is the impact of Saudi culture on functional performance outcomes. Similar to other Middle Eastern and Islamic cultures, Saudi culture focuses on family support and provision of assistance rather than the ability to be functionally independent.42 The care for sick relatives was viewed as a central part of Islamic teaching and a duty of care grounded in a family-oriented society,43 which may have impacted the results of our study regarding functional independence. Nonetheless, the effect sizes that were found in our study indicate that preoperative occupational therapy education may still be effective in improving functional independence although these findings did not indicate statistical significance.
The results also indicated that patients that received preoperative occupational therapy had improved quality of life on the QOLS than patients that did not. Although these results were not statistically significance, the effect size suggests a low-to-medium effect supporting the clinical utility of the intervention. Similarly, preoperative support was connected to improved post-operative quality of life in patients that have undergone a knee or hip replacement.44 On the contrary, Beaupre and others found that preoperative exercise and education did not result in improved post-operative quality of life following a TKR.45 However, pre-operative occupational therapy may still be feasible in improving post-operative quality of life after a lower extremity joint replacement.46 It is not surprising however that the results regarding quality of life are consistent with functional independence in our study. Research suggests that improvements in quality of life are directly related to improvements in functional independence.47,48
The current study is to our knowledge the first to explore the efficacy of a single occupational therapy session on postoperative outcomes in patients that have undergone a TKR or THR. Occupational therapy is a relatively young profession in Saudi Arabia, and there is dire need for exploring the impact of occupational therapy services in a variety of clinical settings and populations including individuals with a lower extremity joint replacement.49 Given the small number of currently practicing occupational therapists in the country,18 the results indicate that one preoperative occupational therapy session may have a positive impact on important postoperative outcomes. In fact, this may also result in shorter length of stay and reduced postoperative costs.50 This is particularly important given that the limited time and resources occupational therapists have with such conditions combined with the lack of awareness of occupational therapy51 may reduce the number of times an occupational therapist can see a lower extremity joint replacement patient prior to their surgery.
Limitations and Future Studies
The results of the current study should be used with caution. Although the results indicate a positive impact of a preoperative occupational therapy educational session on some postoperative outcomes, the study had limitations that should be considered and improved upon. Despite our efforts to control and account for other education that the patients may have received, we cannot assure that other disciplines did not provide education to patients in a formal or informal method. Future studies should make efforts to account for other educational methods from other disciplines. In fact, studies should work towards implementing multidisciplinary preoperative education for patients prior to undergoing a TKR or THR.52,53 There were group differences between the intervention and control groups in the current study as a result of the limited time between admission and surgery, which resulted in lower number of patients being allocated into the intervention group due to the small number of occupational therapists during the time of the study. Future research should aim to have more evenly distributed groups. In addition, the current study had a small sample size that was limited to a specific clinical setting. Future studies should aim to explore the impact of preoperative occupational therapy education with a larger sample and within a variety of clinical settings and outcomes. Gender, age, and condition bias could also be a limitation in this study, most participants in the study were female and with a TKR. Future research should explore these findings in samples with higher younger male participants and patients with THR.
Conclusion
The current study shows promising results supporting the use of a single preoperative occupational therapy educational session prior to patients undergoing a lower extremity joint replacement. These results have important clinical implications for clinical settings with limited number of occupational therapists and with priority given to other conditions. In addition, further research should be done with larger and more diverse samples to confirm the current findings.
Acknowledgments
The authors wish to acknowledge all the participants in this study for their valuable time.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Maradit Kremers H, Larson DR, Crowson CS, et al. Prevalence of total hip and knee replacement in the United States. J Bone Joint Surg Am. 2015;97(17):1386–1397. doi:10.2106/JBJS.N.01141
2. Edwards RR, Campbell C, Schreiber KL, et al. Multimodal prediction of pain and functional outcomes 6 months following total knee replacement: a prospective cohort study. BMC Musculoskelet Disord. 2022;23(1):1–17. doi:10.1186/s12891-022-05239-3
3. Al-Mohrej OA, Alshammari FO, Aljuraisi AM, Bin Amer LA, Masuadi EM, Al-Kenani NS. Knowledge and attitude towards total knee arthroplasty among the public in Saudi Arabia: a nationwide population-based study. Int Orthop. 2018;42(4):819–827. doi:10.1007/s00264-017-3743-4
4. Kim KY, Anoushiravani AA, Chen KK, et al. Perioperative orthopedic surgical home: optimizing total joint arthroplasty candidates and preventing readmission. J Arthroplasty. 2019;34(7):S91–S96. doi:10.1016/j.arth.2019.01.020
5. Steultjens EE, Dekker JJ, Bouter LM, Schaardenburg DD, Kuyk MM, Van den Ende EC. Van den Ende EC. Occupational therapy for rheumatoid arthritis. Cochrane Database Syst Rev. 2004;(1). doi:10.1002/14651858.CD003114.pub2
6. Causey-Upton R, Howell D, Kitzman P, Custer M, Pre-Operative DE. Education for total knee replacement: a pilot survey. Internet J Allied Health Sci Pract. 2018;16(4):1–12.
7. Wylde V, Trela-Larsen L, Whitehouse MR, Blom AW. Preoperative psychosocial risk factors for poor outcomes at 1 and 5 years after total knee replacement: a cohort study of 266 patients. Acta orthopaedica. 2017;88(5):530–536. doi:10.1080/17453674.2017.1334180
8. Giraudet-Le Quintrec JS, Coste J, Vastel L, et al. Positive effect of patient education for hip surgery: a randomized trial. Clin Orthop Relat Res. 2003;414:112–120. doi:10.1097/01.blo.0000079268.91782.bc
9. McGregor AH, Rylands H, Owen A, Doré CJ, Hughes SPF. Does preoperative Hip rehabilitation advice improve recovery and patient satisfaction? J Arthroplasty. 2004;19(4):464–468. doi:10.1016/j.arth.2003.12.074
10. Huber EO, de Bie RA, Roos EM, Bischoff-Ferrari HA. Effect of pre-operative neuromuscular training on functional outcome after total knee replacement: a randomized-controlled trial. BMC Musculoskelet Disord. 2013;14(1):157. doi:10.1186/1471-2474-14-157
11. McDonald S, Page MJ, Beringer K, Wasiak J, Sprowson A. Preoperative education for Hip or knee replacement. Cochrane Database Syst Rev. 2014;(5). doi:10.1002/14651858.CD003526.pub3
12. Clarke HD, Timm VL, Goldberg BR, Hattrup SJ. Preoperative patient education reduces in-hospital falls after total knee arthroplasty. Clin Orthop Relat Res. 2012;470(1):244–249. doi:10.1007/s11999-011-1951-6
13. Bjerk M, Brovold T, Skelton DA, Bergland A, N M D, Devi Sagili K. A falls prevention programme to improve quality of life, physical function and falls efficacy in older people receiving home help services: study protocol for a randomised controlled trial. BMC Health Serv Res. 2017;17(1):1–9. doi:10.1186/s12913-016-1943-z
14. Vukomanović A, Popović Z, Đurović A, Krstić L. The effects of short-term preoperative physical therapy and education on early functional recovery of patients younger than 70 undergoing total Hip arthroplasty. Vojnosanit Pregl. 2008;65(4):291–297. doi:10.2298/VSP0804291V
15. Kearney M, Jennrich MK, Lyons S, Robinson R, Berger B. Effects of preoperative education on patient outcomes after joint replacement surgery. Orthop Nurs. 2011;30(6):391–396. doi:10.1097/NOR.0b013e31823710ea
16. Soever LJ, MacKay C, Saryeddine T, et al. Educational needs of patients undergoing total joint arthroplasty. Physiother Can. 2010;62(3):206–214. doi:10.3138/physio.62.3.206
17. Mahomed NN, Liang MH, Cook EF, et al. The importance of patient expectations in predicting functional outcomes after total joint arthroplasty. J Rheumatol. 2002;29(6):1273–1279.
18. Meny AH, Hayat AA. Knowledge about occupational therapy in Makkah, Saudi Arabia. Where do health care professionals stand. Int Ann Med. 2017;1(11):6. doi:10.24087/IAM.2017.1.11.351
19. Portney LG. Foundations of Clinical Research: Applications to Evidence-Based Practice. FA Davis; 2020.
20. Pendleton HM, Schultz-Krohn W. Pedretti’s Occupational Therapy - E-Book: Practice Skills for Physical Dysfunction. Elsevier Health Sciences; 2017.
21. Keith RA. The Functional Independence Measure: a new tool for rehabilitation. Adv Clin Rehabil. 1987;2:6–18.
22. Aitken DM, Bohannon RW. Functional independence measure versus short form-36: relative responsiveness and validity. Int J Rehabil Res. 2001;24(1):65–68. doi:10.1097/00004356-200103000-00009
23. Kidd D, Stewart G, Baldry J, et al. The functional independence measure: a comparative validity and reliability study. Disabil Rehabil. 1995;17(1):10–14. doi:10.3109/09638289509166622
24. Ottenbacher KJ, Hsu Y, Granger CV, Fiedler RC. The reliability of the functional Independence measure: a quantitative review. Arch Phys Med Rehabil. 1996;77(12):1226–1232. doi:10.1016/S0003-9993(96)90184-7
25. Shields RK, Enloe LJ, Evans RE, Smith KB, Steckel SD, Reliability V. Responsiveness of functional tests in patients with total joint replacement. Phys Ther. 1995;75(3):169–176. doi:10.1093/ptj/75.3.169
26. Melzack R. The short-form McGill pain questionnaire. Pain. 1987;30(2):191–197. doi:10.1016/0304-3959(87)91074-8
27. Grafton KV, Foster NE, Wright CC. Test-retest reliability of the short-form McGill pain questionnaire: assessment of intraclass correlation coefficients and limits of agreement in patients with osteoarthritis. Clin J Pain. 2005;21(1):73–82. doi:10.1097/00002508-200501000-00009
28. Melzack R. The McGill Pain Questionnaire: major properties and scoring methods. PAIN. 1975;1(3):277–299. doi:10.1016/0304-3959(75)90044-5
29. Strand LI, Ljunggren AE, Bogen B, Ask T, Johnsen TB. The short-form McGill pain questionnaire as an outcome measure: test–retest reliability and responsiveness to change. Eur J Pain. 2008;12(7):917–925. doi:10.1016/j.ejpain.2007.12.013
30. Turner KV, Moreton BM, Walsh DA, Lincoln NB. Reliability and responsiveness of measures of pain in people with osteoarthritis of the knee: a psychometric evaluation. Disabil Rehabil. 2017;39(8):822–829. doi:10.3109/09638288.2016.1161840
31. Wright KD, Asmundson GJG, McCreary DR. Factorial validity of the short-form McGill pain questionnaire (SF-MPQ). Eur J Pain. 2001;5(3):279–284. doi:10.1053/eujp.2001.0243
32. Flanagan JC. A research approach to improving our quality of life. Am Psychol. 1978;33:138–147. doi:10.1037/0003-066X.33.2.138
33. Burckhardt CS, Woods SL, Schultz AA, Ziebarth DM. Quality of life of adults with chronic illness: a psychometric study. Res Nurs Health. 1989;12(6):347–354. doi:10.1002/nur.4770120604
34. Burckhardt CS, Anderson KL. The Quality of Life Scale (QOLS): reliability, validity, and utilization. Health Qual Life Outcomes. 2003;1(1):60. doi:10.1186/1477-7525-1-60
35. Yerxa EJ, Burnett-Beaulieu S, Stocking S, Azen SP. Development of the Satisfaction with Performance Scaled Questionnaire (SPSQ). Am J Occup Ther. 1988;42(4):215–221. doi:10.5014/ajot.42.4.215
36. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
37. R Core Team. R: a language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing; 2021. Available from: http://wwwR-project.org/.
38. Sorel JC, Overvliet GM, Gademan MGJ, den Haan C, Honig A, Poolman RW. The influence of perioperative interventions targeting psychological distress on clinical outcome after total knee arthroplasty. Rheumatol Int. 2020;40(12):1961–1986. doi:10.1007/s00296-020-04644-y
39. Chen S, Chen C, Lin P. The effect of educational intervention on the pain and rehabilitation performance of patients who undergo a total knee replacement. J Clin Nurs. 2014;23(1–2):279–287. doi:10.1111/jocn.12466
40. Moulton LS, Evans PA, Starks I, Smith T. Preoperative education prior to elective knee arthroplasty surgery does not change patient outcomes. Musculoskelet Care. 2017;15(4):341–344. doi:10.1002/msc.1177
41. Moyer R, Ikert K, Long K, Marsh J. The value of preoperative exercise and education for patients undergoing total hip and knee arthroplasty: a systematic review and meta-analysis. JBJS Rev. 2017;5(12):e2. doi:10.2106/JBJS.RVW.17.00015
42. Malkawi SH, Alqatarneh NS, Fehringer EK. The influence of culture on occupational therapy practice in Jordan. Occup Ther Int. 2020;2020:e1092805. doi:10.1155/2020/1092805
43. Al Busaidy NS, Borthwick A. Occupational therapy in Oman: the impact of cultural dissonance. Occup Ther Int. 2012;19(3):154–164. doi:10.1002/oti.1332
44. Fitzgerald JD, Orav EJ, Lee TH, et al. Patient quality of life during the 12 months following joint replacement surgery. Arthritis Care Res. 2004;51(1):100–109. doi:10.1002/art.20090
45. Beaupre LA, Lier D, Davies DM, Johnston DBC. The effect of a preoperative exercise and education program on functional recovery, health related quality of life, and health service utilization following primary total knee arthroplasty. J Rheumatol. 2004;31(6):1166–1173.
46. Jepson P, Sands G, Beswick AD, Davis ET, Blom AW, Sackley CM. A feasibility randomised controlled trial of pre-operative occupational therapy to optimise recovery for patients undergoing primary total Hip replacement for osteoarthritis (PROOF-THR). Clin Rehabil. 2016;30(2):156–166. doi:10.1177/0269215515576811
47. Araujo ILA, Castro MC, Daltro C, Matos MA. Quality of life and functional independence in patients with osteoarthritis of the knee. Knee Surg Relat Res. 2016;28(3):219–224. doi:10.5792/ksrr.2016.28.3.219
48. Papakostidou I, Dailiana ZH, Papapolychroniou T, et al. Factors affecting the quality of life after total knee arthroplasties: a prospective study. BMC Musculoskelet Disord. 2012;13(1):116. doi:10.1186/1471-2474-13-116
49. Sheth M, Simone R, Shimoda B, Dalusung D, Peralta J. Role of OT in an interdisciplinary team care approach, used to rehabilitate elective hip and knee arthroplasties: a systematic review. AJOT. 2020;74(S1):NA–NA.
50. National Guideline Centre (UK). Evidence review for preoperative rehabilitation: joint replacement (primary): hip, knee and shoulder: evidence review C. National Institute for Health and Care Excellence (UK); 2020. Available from: http://www.ncbi.nlm.nih.gov/books/NBK561392/.
51. Meny AH, Hayat AA, Ain QU, et al. Knowledge about occupational therapy among people in Saudi Arabia. J Evol Med Dent Sci. 2021;10(22):1703–1708. doi:10.14260/jemds/2021/352
52. Kennedy D, Wainwright A, Pereira L, et al. A qualitative study of patient education needs for hip and knee replacement. BMC Musculoskelet Disord. 2017;18(1):413. doi:10.1186/s12891-017-1769-9
53. Nguyen C, Boutron I, Roren A, et al. Effect of prehabilitation before total knee replacement for knee osteoarthritis on functional outcomes: a randomized clinical trial. JAMA network open. 2022;5(3):e221462–e221462. doi:10.1001/jamanetworkopen.2022.1462
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Basic Determinants of Disease Knowledge in COPD Patients: Results from COSYCONET
Fischer C, Jörres RA, Alter P, Trudzinski FC, Yildirim, Bals R, Vogelmeier CF, Kauffmann-Guerrero D, Behr J, Watz H, Holle R, Kahnert K
Patient Preference and Adherence 2022, 16:1759-1770
Published Date: 26 July 2022
The Burden of Metastatic Cancer–Induced Bone Pain: A Narrative Review
Colosia A, Njue A, Bajwa Z, Dragon E, Robinson RL, Sheffield KM, Thakkar S, Richiemer SH
Journal of Pain Research 2022, 15:3399-3412
Published Date: 25 October 2022
A Systematic Review and Meta-Analysis of the Effects of Rehabilitation Using Digital Healthcare on Musculoskeletal Pain and Quality of Life
Jang S, Lee B, Lee E, Kim J, Lee JI, Lim JY, Hwang JH, Jang S
Journal of Pain Research 2023, 16:1877-1894
Published Date: 31 May 2023
The Effect of Virtual Reality Glasses Applied During the Episiotomy On Pain and Satisfaction: A Single Blind Randomized Controlled Study
Orhan M, Bülez A
Journal of Pain Research 2023, 16:2227-2239
Published Date: 29 June 2023
Physical Activity, Depression and Quality of Life in COPD – Results from the CLARA II Study
Horner A, Olschewski H, Hartl S, Valipour A, Funk GC, Studnicka M, Merkle M, Kaiser B, Wallner EM, Brecht S, Lamprecht B
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:2755-2767
Published Date: 29 November 2023