Back to Journals » Patient Preference and Adherence » Volume 16
Basic Determinants of Disease Knowledge in COPD Patients: Results from COSYCONET
Authors Fischer C ![]() , Jörres RA
, Jörres RA ![]() , Alter P
, Alter P ![]() , Trudzinski FC
, Trudzinski FC ![]() , Yildirim, Bals R, Vogelmeier CF, Kauffmann-Guerrero D
, Yildirim, Bals R, Vogelmeier CF, Kauffmann-Guerrero D ![]() , Behr J, Watz H, Holle R
, Behr J, Watz H, Holle R ![]() , Kahnert K
, Kahnert K
Received 1 April 2022
Accepted for publication 16 June 2022
Published 26 July 2022 Volume 2022:16 Pages 1759—1770
DOI https://doi.org/10.2147/PPA.S367284
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Carolina Fischer,1 Rudolf A Jörres,1 Peter Alter,2 Franziska C Trudzinski,3 Önder Yildirim,4 Robert Bals,5 Claus F Vogelmeier,2 Diego Kauffmann-Guerrero,6 Jürgen Behr,6 Henrik Watz,7 Rolf Holle,8 Kathrin Kahnert6 And members of the COSYCONET study group
1Institute and Outpatient Clinic for Occupational, Social and Environmental Medicine, University Hospital, LMU Munich, Comprehensive Pneumology Center Munich (CPC-M), Munich, Germany; 2Department of Medicine, Pulmonary and Critical Care Medicine, University of Marburg (UMR), Germany, Marburg, Germany; 3Department of Pneumology and Critical Care Medicine, Thoraxklinik, University of Heidelberg, Translational Lung Research Center Heidelberg (TLRC-H), Heidelberg, Germany; 4Institute of Lung Biology and Disease (ILBD), Comprehensive Pneumology Center Munich (CPC-M), Munich, Germany; 5Department of Internal Medicine V - Pulmonology, Allergology, Intensive Care Medicine, Saarland University Hospital, Homburg, Germany; 6Department of Medicine V, University Hospital, LMU Munich, Comprehensive Pneumology Center Munich (CPC-M), Munich, Germany; 7Pulmonary Research Institute at LungenClinic Grosshansdorf, Airway Research Center North (ARCN), Grosshansdorf, Germany; 8Institute for Medical Informatics, Biometry and Epidemiology, University Hospital, LMU Munich, Munich, Germany
Correspondence: Kathrin Kahnert, Department of Medicine V, University Hospital, LMU Munich, Comprehensive Pneumology Center Munich (CPC-M), Ziemssenstraße 1, Munich, 80336, Germany, Email [email protected]
Introduction: In many chronic diseases, including COPD, the patients’ basic knowledge of the disorder has been shown to be relevant for the course of the disease. We studied which clinical and functional characteristics were related to this knowledge as well as the patients’ satisfaction with their knowledge about COPD.
Methods: The study population comprised 645 patients of GOLD grades 1– 4 who participated in Visit 6 of the COSYCONET cohort (COPD and Systemic Consequences - Comorbidities Network). The assessments covered a broad panel of clinical and functional characteristics, including generic and disease-specific quality of life and the COPD Assessment Test (CAT). The study aim was addressed by two questions, referring to patients’ knowledge of the meaning of FEV1 and the overall satisfaction with their knowledge of COPD.
Results: Knowledge of FEV1 was higher in patients of higher spirometric GOLD grades or exacerbation risk, in males, with higher educational level, and after participation in a prior educational training on COPD. Patients with more detailed knowledge showed a higher satisfaction with their knowledge. Satisfaction was associated with higher generic quality of life and a lower CAT score. Furthermore, satisfaction was higher in patients with a treatment plan but lower in patients with cardiac comorbidities. It appeared that females with basic education, high burden from COPD and low quality of life had the greatest knowledge deficits.
Discussion: The results suggest room for education programs adapted to the educational level of the participants. They also emphasize the major role of a disease management plan for the patients.
Keywords: chronic obstructive pulmonary disease, knowledge, education, satisfaction
Introduction
Patients with chronic obstructive pulmonary disease (COPD) show a large heterogeneity of their clinical condition that is commonly described by the categorization into GOLD grades 1–4 based on spirometry, and GOLD groups A to D based on symptoms and exacerbation history.1 The respiratory condition and the frequent presence of comorbidities lead to extensive therapy.2 It is reasonable to assume that the therapeutic success depends on patients’ cooperation and possibly their understanding of the disease, both of which can be promoted by education and disease management programs. Indeed, self-management programs have been designed to improve patients’ clinical status3 through behavioral changes, optimized social, emotional and physical impairments.4,5 Although _ENREF_6we did not find clinical status to be a major determinant of the adherence to medication in a previous analysis,6 this might be different with respect to the acquired knowledge about the disease and the need for further information expressed by the patients. This study aimed to investigate the relationship between disease-specific knowledge and clinical and functional characteristics of COPD patients. In an analogous manner, we analyzed patient satisfaction with COPD-specific knowledge to identify potential needs for action. To elucidate such associations and potential needs, we analyzed the responses to two basic questions on patients’ knowledge and their satisfaction with their knowledge of the disease, using data from the large, multi-center German COPD study COSYCONET (COPD and Systemic Consequences - Comorbidities Network) addressing different aspects of COPD research.7–11 These data comprised information on anthropometric, clinical and lung function characteristics, time since diagnosis, education level, participation in a disease management program, availability of a treatment plan and whether the treating physician was a pneumologist.
Materials and Methods
Assessments
The observational German COPD cohort study COSYCONET (“COPD and SYstemic consequences-COmorbidities NETwork”) investigates the interaction of lung disease, comorbidities and systemic inflammation and n=2741 patients with COPD were included into visit 1 of COSYCONET.12 Details of the COSYCONET study have been published previously12. Inclusion criteria comprised aged 40 years and older, diagnosis of COPD (according to GOLD criteria) or chronic bronchitis, availability for repeated study visits over at least 18 months and exclusion criteria comprised having undergone major lung surgery, moderate or severe exacerbation within the last 4 weeks, having a lung tumor, physical or cognitive impairment resulting in an inability to walk or to understand the intention of the project.12 Follow-up visits were performed after 6, 18, 36, 54 and 72 months. At the time of the 72-month visit, 776 patients still participated in the study. At this point in time, questions “Do you know the term FEV1 (forced expiratory volume in one second)” and “How satisfied are you with your knowledge and understanding regarding COPD?” were introduced into the COSYCONET questionnaires. Only patients of spirometric GOLD grades 1–41 were included in visit 6 (see Figure 1). At each visit, the assessments of COSYCONET comprised a detailed clinical history, anthropometric data, lung function, time since COPD diagnosis, comorbidities based on patients’ reports of physician-based diagnoses, symptoms, exacerbation history, physical activity by the International Physical Activity Questionnaire (IPAQ), and quality of life via the visual analogue scale (VAS) of the EQ-5D-3L and the disease-specific St George’s Respiratory Questionnaire (SGRQ). All visits followed standard operating procedures (SOP).12 Education level was grouped into three categories based on the number of years of education completed (basic education ≤9 years, secondary education 10 to 11 years, higher education >11 years).13 Moreover, patients were questioned regarding participation in a disease management program, availability of a treatment plan and whether the treating physician was a pneumologist.
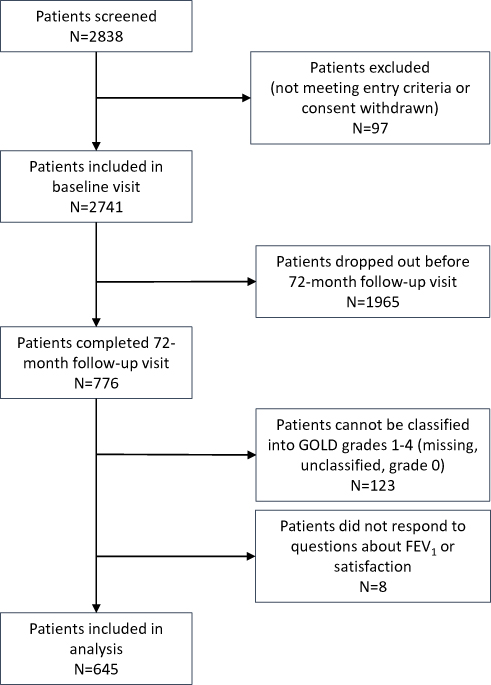 |
Figure 1 Flow-chart diagram of the study population. |
The assumed basic knowledge of COPD was assessed based on the question “Do you know the term FEV1 (forced expiratory volume in one second)”; the answers were either yes or no. This was considered relevant as FEV1 plays a fundamental role in the categorization of COPD and could be assumed to be known to patients who had already performed a considerable number of lung function tests. The level of further information desired by patients was assessed by the question “How satisfied are you with your knowledge and understanding regarding COPD?”; answers were given on a Likert scale ranging from 0 (not at all) to 6 (very satisfied).
The COSYCONET study was approved by the Ethical Committee of the coordinating center (University of Marburg) and those of all study centers, as well as the respective data security authorities (data security agency of the federal states of Hesse, Baden-Württemberg, Lower-Saxony and Saarland). Moreover, it followed the declaration of Helsinki and Good Clinical Practice Guidelines. All patients gave their written informed consent. Clinical Trial registration: NCT01245933.
Data Analysis
For descriptive purposes, median values [quartiles] and numbers or percentages were computed, depending on the type of data. Statistical comparisons between groups were performed using contingency tables and the chi-square statistics, or the Mann–Whitney-U-Test, depending on the type of data and comparison. As only few patients showed low score points in the satisfaction with COPD knowledge, we defined a new binary variable comprising 0–4 versus 5–6 points based on ROC (receiver operator characteristics) analysis with knowledge as outcome. This simplification was done in order to make the analyses of satisfaction and knowledge more comparable.
Multiple binary logistic regression analysis was employed to identify statistically independent predictors of knowledge and satisfaction. The predictors used were age, sex, GOLD grades, symptoms (GOLD BD vs AC), exacerbations (GOLD CD vs AB), IPAQ, CAT, EQ-5D-3L VAS, patients’ education category, participation in COPD education, participation in a COPD disease management program, a COPD treatment plan and the specialty of the treating physician (pneumologist vs others) as well as the comorbidities coronary artery disease (CAD), myocardial infarction (MI), heart failure (HF), hypertension, peripheral artery disease (PAD), diabetes, hyperlipidemia, hyperuricemia, osteoporosis, mental disorders, sleep apnea and asthma. The comorbidities were analyzed through four sum scores comprising the number of respiratory, cardiac, vascular and metabolic disorders, whereby osteoporosis was counted separately due to its special relation to COPD resulting from corticosteroid therapy. GOLD grades 1–4 were treated as categorical variables relative to grade 1. We omitted the SGRQ from the analysis due to its high collinearity with CAT and VAS. In case of knowledge, satisfaction was included as additional predictor, in case of satisfaction, knowledge. Analyses were performed using inclusion of all predictors and repeated with forward and backward selection to confirm that the set of predictors identified as significant was the same and thus the result could be considered as statistically reliable. For the sake of brevity, only the significant predictors are shown in the graphs, and the presented estimates refer to analyses restricted to these predictors. Statistical significance was assumed for p<0.05. All analyses were performed using the software package SPSS (IBM SPSS Statistics for Macintosh, Version 28.0., Armonk, NY, USA).
Results
Study Population
In total, 645 patients of GOLD grades 1–4 participated in the 72-month follow-up visit and answered the questions regarding COPD knowledge and satisfaction (Table 1). Of these, 235 (36.4%) stated to be familiar with the term FEV1. Satisfaction with COPD knowledge at Likert points 0–6 was reported by 1.2, 3.4, 7.6, 26.4, 23.7, 24.0 and 13.6% of patients, respectively, resulting in 243 patients (37.7%) in the category of ≥5 points.
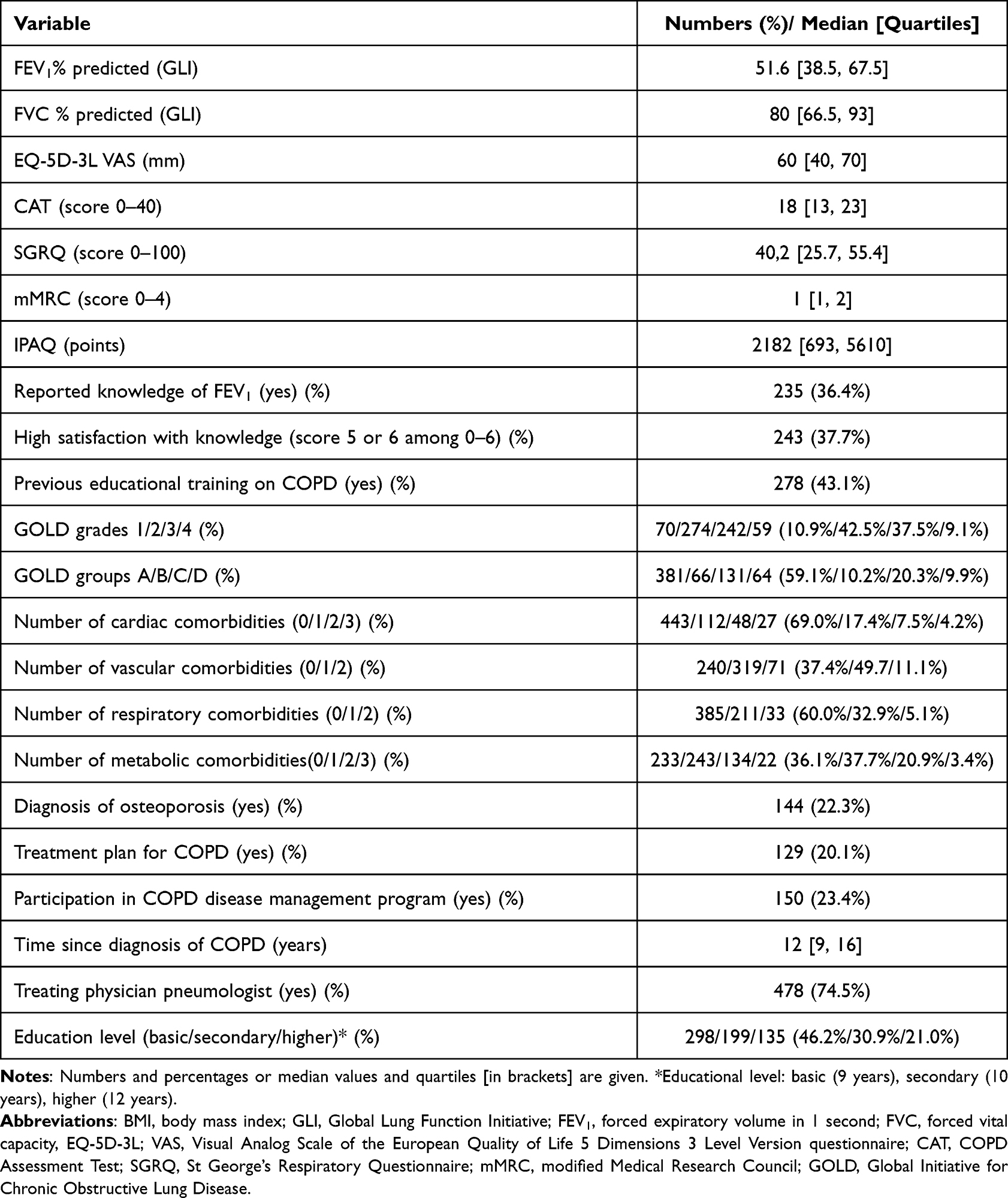 |
Table 1 Patient Characteristics (n=645) of the Study Cohort |
Associations of Reported Knowledge of FEV1
The results of univariate analyses using contingency tables and the Mann–Whitney-U-Test are summarized in Tables 2 and 3. There were associations with multiple variables that were checked in multiple logistic regression analyses for being statistically independent predictors. Male sex, GOLD grades 3 and 4 compared to grade 1, higher exacerbation score, previous education on COPD, osteoporosis, participation in a COPD disease management program, secondary and high compared to low education as well as satisfaction with knowledge were significant simultaneous predictors of greater knowledge (p<0.05 each), while CAT, EQ-5D-3L VAS, IPAQ and other comorbidity scores were not relevant. This was confirmed by forward and backward selection. The results are shown in Figure 2 in terms of odds ratios.
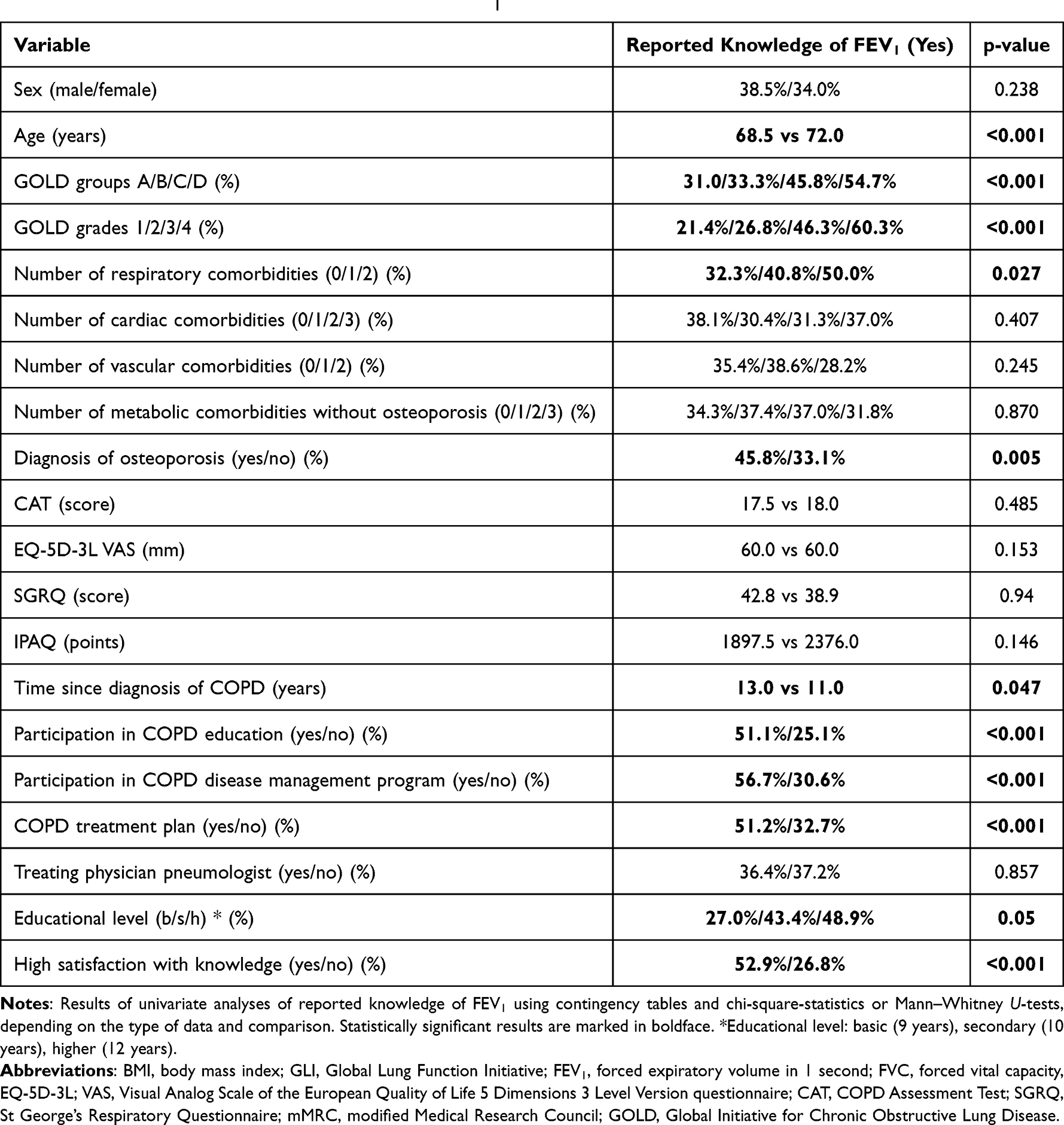 |
Table 2 Associations of Reported Knowledge of FEV1 |
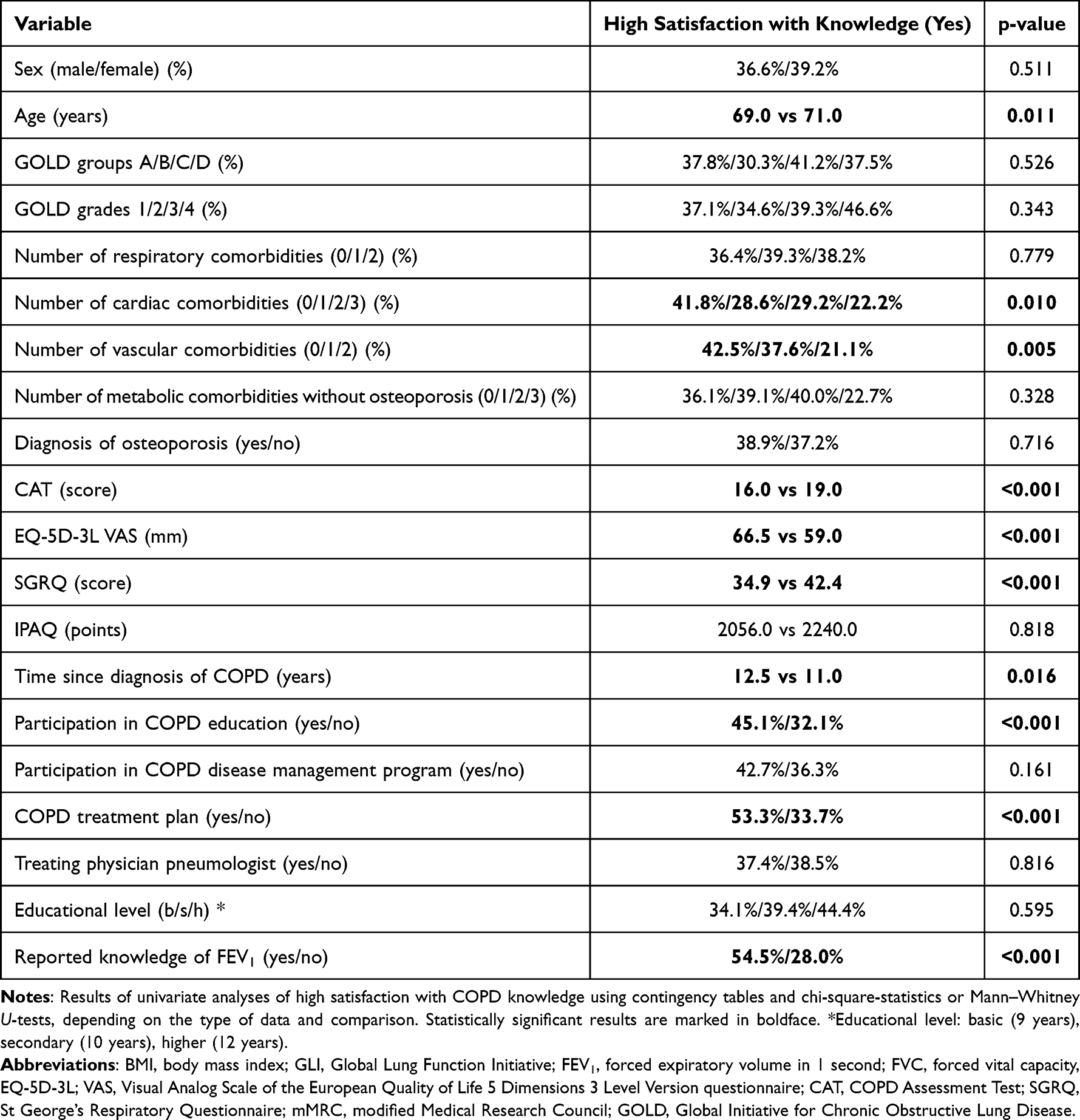 |
Table 3 Associations of High Satisfaction with Knowledge on COPD |
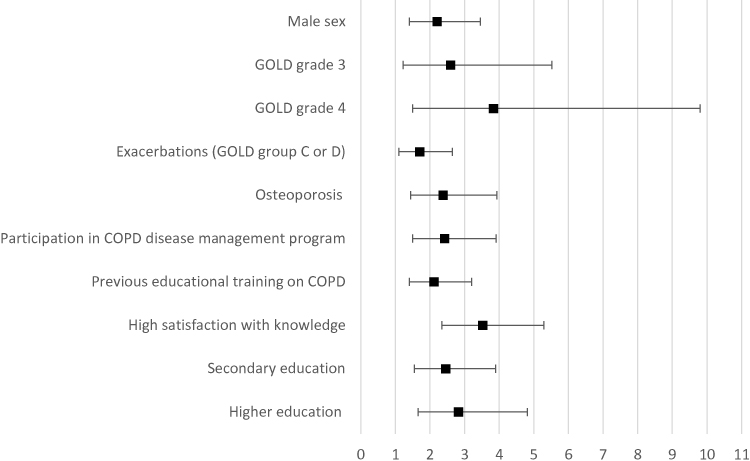 |
Figure 2 Odds ratios and 95% confidence intervals obtained from logistic regression analysis of the reported knowledge of FEV1 versus a comprehensive set of predictors (see Methods). The figure shows the result restricted to those predictors that were consistently found significant with inclusion as well as forward and backward selection. The effects of GOLD grades 3 and 4 were relative to grade 1. |
To elucidate whether the effect of educational training on the knowledge of FEV1 was dependent on education, we repeated the analysis separately in patients with either basic education (N=298; 46.2%) or secondary/higher education (N=344; 53.3%). In both groups, GOLD grade 4, participation in a disease management program and satisfaction with COPD knowledge remained as predictors (p<0.05 each). In the group of basic education, exacerbations were additional predictors, in the group with secondary/higher education, osteoporosis, male sex and previous education on COPD (p<0.05 each). For the corresponding odds ratios see the Supplemental Table S1. The differences between groups were small, but the highest GOLD grades were linked to more detailed knowledge, primarily in patients with basic education.
In patients without previous educational training, GOLD grade 3, exacerbations and satisfaction with knowledge were significant predictors (p<0.05 each). In patients with previous educational training, GOLD grade 4, secondary/higher education level, participation in a disease management program and satisfaction with COPD knowledge were significant predictors (p<0.05 each). For the corresponding odds ratios see the Supplemental Table S1. Differences were small, but participation in a disease management program was relevant only in patients with prior educational training.
Associations of Satisfaction with COPD Knowledge
Univariate analyses using contingency tables and the Mann–Whitney-U-Test yielded the results summarized in Table 2. These associations were checked in multiple logistic regression analysis for statistically independent predictors. The results showed statistical significance (p<0.05 each) for higher exacerbations, higher EQ-5D-3L VAS, lower CAT, the existence of a treatment plan, longer time since the diagnosis of COPD, lower cardiac comorbidities and reported knowledge. The corresponding odds ratios are shown in Figure 3.
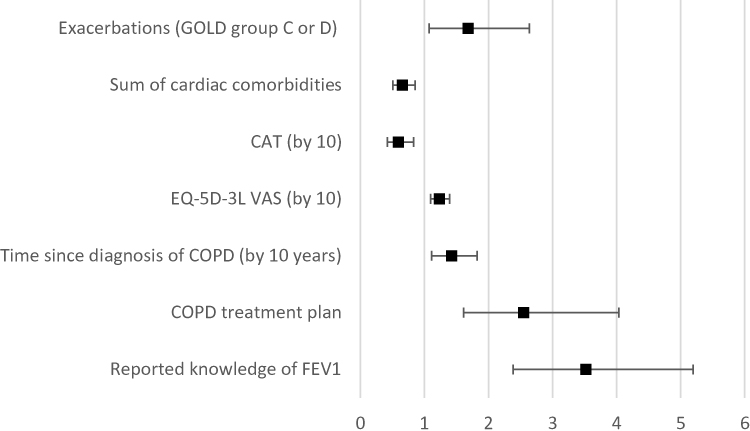 |
Figure 3 Odds ratios and 95% confidence intervals obtained from logistic regression analysis of the reported higher satisfaction with COPD knowledge versus a comprehensive set of predictors (see Methods). The figure shows the result restricted to those predictors that were consistently found significant with inclusion as well as forward and backward selection. For better readability, the effects of CAT, EQ-5D-3L VAS and the duration of COPD since diagnosis are given for changes in 10 units of the respective variable. |
In patients with basic education a higher EQ-5D-3L VAS, the existence of a treatment plan and knowledge of FEV1 were linked to more satisfaction (p<0.05). In patients with secondary/higher education, a higher EQ-5D-3L VAS, the existence of a treatment plan, lower cardiac comorbidities and knowledge of FEV1 were associated with higher satisfaction (p<0.05). In patients without previous educational training, a lower CAT, the presence of a treatment plan, lower cardiac comorbidities and the knowledge of FEV1 were significant predictors of satisfaction (p<0.05 each). In patients with previous educational training, higher EQ-5D-3L VAS, the presence of a treatment plan, longer time since COPD diagnosis and the knowledge of FEV1 were significant predictors of satisfaction (p<0.05 each). From the Supplemental Table S2 it can be seen that for both subcategorizations the differences in odds ratios were small irrespective of statistical significance.
Discussion
The present analysis addressed COPD-relevant knowledge and satisfaction with this knowledge in relation to basic characteristics of patients including educational level and previous participation in educational programs on COPD. The aim was to get hints on the characteristics of patients who lack information and conversely benefit most from educational training. For this purpose, we used two simple questions that had been introduced into the COSYCONET cohort at one of the follow-up visits; these questions referred to the knowledge of the meaning of FEV1 and to the overall satisfaction with the knowledge about COPD.
As expected, the reported knowledge depended on the educational level and the participation in a prior educational training on COPD. Interestingly, it also was higher in patients of higher spirometric GOLD grades or exacerbation risk, as well as in males. Additionally, patients who participated in a disease management program as well as patients with the diagnosis of osteoporosis reported better knowledge. Neither the clinical state as measured by the CAT, nor generic quality of life, reported daily activity, nor the presence of comorbidities played a role. Patients with reported knowledge of FEV1 were also more satisfied with their general knowledge about COPD, suggesting that the specific knowledge regarding FEV1 was considered a relevant part of knowledge.
Satisfaction with the knowledge showed a different pattern of predictors. It depended on the reported knowledge as well as a higher exacerbation score but not on GOLD grades or sex or age. Conversely, it was associated with less COPD complaints in terms of the CAT and higher generic quality of life. Moreover, the presence of cardiac comorbidities was associated with less satisfaction with the knowledge about COPD. Additionally, the presence of a COPD treatment plan as well a longer time since the diagnosis of COPD had a positive effect on the patients’ satisfaction.
These results are in line with the known positive effect of disease knowledge on the course of COPD.4 They furthermore provide insight into which particular patients lack knowledge and suggest that these are females with basic education, high burden from COPD, low quality of life and cardiac disease. Lower educational level is a proxy of socioeconomic status that has been shown to be associated with poorer COPD outcomes,13,14 therefore these patients might benefit from COPD education.
The fact that the estimated effect of previous education on COPD was low in patients with basic education also points towards education programs that are adapted to the needs and understanding of these patients. Thus, different courses might be offered for different levels of education. This could easily be implemented in online courses which not only could help to reconcile the participation with work but also might avoid problems arising from a slower rate of understanding in a group.
Previous studies already investigated the distribution of patients’ disease-specific knowledge in COPD15–17 or other chronic diseases such as diabetes.18,19 These studies often used extensive panels designed for covering a broad spectrum of knowledge. In the present study, we used only two questions. The reason was that the extensive study protocol of COSYCONET12 and the restrictions of time prevented the introduction of more detailed assessments or specific tests to verify the claimed knowledge.
Despite these limitations, the results seem plausible and the questions suitable FEV1 is the basic variable used to categorize COPD into GOLD categories 1–4. These categories are known to the great majority of patients and treating physicians including non-specialists. Moreover, patients are commonly monitored over time involving repeated assessments of lung function and often ask doctors and technicians for the measured values. It therefore appeared reasonable to utilize the knowledge of FEV1 as a proxy of basic knowledge on the disease, similarly to that of HbA1c or glucose levels in diabetes.20 Knowledge on COPD was also related to the presence of osteoporosis. This is known to many patients as a risk of treatment with corticosteroids and of advanced age which is relevant as COPD is primarily a disease of the elderly. Indeed, a great number of patients in COSYCONET are treated with corticosteroids, irrespective of the conformity with treatment recommendations.2
The question regarding satisfaction with the knowledge of COPD did not address a specific topic and covered the whole area of COPD. It is therefore plausible that high satisfaction correlated with other broad-band measures such as CAT and generic quality of life. Satisfaction was lower in patients with a history of cardiac diseases. Experience shows that such diseases are considered as a threat21 which is also reflected in the high adherence to cardiac medication.6 In view of the close link between COPD and cardiac diseases, the feeling of insufficient knowledge seems understandable as patients may put their primary focus on the cardiac disease rather than COPD. Conversely, higher exacerbations and longer duration of COPD seemed to favor satisfaction with COPD knowledge, possibly based on more experience with the successful management of the disease. Another interesting finding was that while the existence of a COPD treatment plan was associated with higher satisfaction, this was not true for the mere participation in a disease management program.
Limitations
This is a cross-sectional study, as the question on knowledge about FEV1 and the question on satisfaction with knowledge was introduced in the course of the COSYCONET study. In the study population, a total of 40% of COPD patients received disease-specific education. This number is likely to be higher than in real-life situations, since participation in an intensive observational study such as COSYCONET should have a selection effect. It can therefore be assumed that COPD-specific knowledge in the general population is lower. Moreover, the single question regarding FEV1 was considered as indicator question for the level of COPD knowledge; this was probably justified as it is a simple, intuitive parameter and many patients are aware of lung function being used for COPD grading. The advantage of this study is the detailed knowledge about the clinical characteristics, thus it was possible to identify patients with the largest gaps of knowledge.
Conclusion
We found that patients with greater disease-specific knowledge in terms of FEV1 had higher satisfaction with their knowledge. Satisfaction was lower in patients with cardiac comorbidities and higher in patients with a treatment plan. Higher satisfaction corresponded to a higher generic quality of life and a lower score in the COPD Assessment Test. It appeared that females with basic education, high burden from COPD and low quality of life had the greatest deficits in knowledge. The results suggest room for education programs that take into account the educational level of the participants and emphasize the role of a disease management plan for the patients.
COSYCONET Study Group
Andreas, Stefan (Lungenfachklinik, Immenhausen); Bals, Robert Universitätsklinikum des Saarlandes); Behr, Jürgen and Kahnert, Kathrin (Klinikum der Ludwig-Maximilians-Universität München); Bahmer, Thomas (Universitätsklinikum Schleswig Holstein) and Bewig, Burkhard (Städtisches Krankenhaus Kiel); Ewert, Ralf and Stubbe, Beate (Universitätsmedizin Greifswald); Ficker, Joachim H. (Klinikum Nürnberg, Paracelsus Medizinische Privatuniversität Nürnberg); Grohé, Christian (Ev. Lungenklinik Berlin); Held, Matthias (Klinikum Würzburg Mitte gGmbH, Standort Missioklinik); Behr, Jürgen and Henke, Markus (Asklepios Fachkliniken München-Gauting); Herth, Felix (Thoraxklinik Heidelberg gGmbH); Kirsten, Anne-Marie and Watz, Henrik (Pneumologisches Forschungsinstitut an der Lungenclinic Grosshansdorf GmbH); Koczulla, Rembert (Schön Klinik Berchtesgadener Land); Kronsbein, Juliane (Berufsgenossenschaftliches Universitätsklinikum Bergmannsheil, Bochum); Kropf-Sanchen, Cornelia (Universitätsklinikum Ulm); Herzmann, Christian (Forschungszentrum Borstel); Pfeifer, Michael (Klinik Donaustauf); Randerath, Winfried J. (Wissenschaftliches Institut Bethanien e. V., Solingen); Seeger, Werner (Justus-Liebig-Universität Gießen); Studnicka, Michael (Uniklinikum Salzburg); Taube, Christian (Ruhrlandklinik gGmbH Essen); Timmermann, Hartmut (Hamburger Institut für Therapieforschung GmbH); Alter, Peter; Schmeck, Bernd and Vogelmeier, Claus (Universitätsklinikum Gießen und Marburg GmbH, Standort Marburg); Welte, Tobias (Medizinische Hochschule Hannover); Wirtz, Hubert (Universitätsklinikum Leipzig) The study was based on 2741 patients recruited within the COSYCONET framework (ClinicalTrials.gov, Identifier: NCT01245933). For further information see Karch A, Vogelmeier C, Welte T, Bals R, Kauczor HU, Biederer J, Heinrich J, Schulz H, Glaser S, Holle R et al.: The German COPD cohort COSYCONET: Aims, methods and descriptive analysis of the study population at baseline. Respir Med 2016, 114:27–37.
Data Sharing Statement
The basic data are part of the German COPD cohort COSYCONET (www.asconet.net) and available upon request. The website of the network provides a detailed procedure for respective applications. The data can be obtained after submission of a proposal that is evaluated by the steering committee. All results to which the manuscript refers, are documented appropriately in the text, figures or tables.
Statement of Ethics
All assessments were approved by the central (Marburg [Ethikkommission FB Medizin Marburg]) and local (Bad Reichenhall [Ethikkommission bayerische Landesärztekammer]); Berlin (Ethikkommission Ärztekammer Berlin); Bochum (Ethikkommission Medizinische Fakultät der RUB); Borstel (Ethikkommission Universität Lübeck); Coswig (Ethikkommission TU Dresden); Donaustauf (Ethikkommission Universitätsklinikum Regensburg); Essen (Ethikkommission Medizinische Fakultät Duisburg-Essen); Gießen (Ethikkommission Fachbereich Medizin); Greifswald (Ethikkommission Universitätsmedizin Greifswald); Großhansdorf (Ethikkommission Ärztekammer Schleswig-Holstein); Hamburg (Ethikkommission Ärztekammer Hamburg); MHH Hannover/Coppenbrügge (MHH Ethikkommission); Heidelberg Thorax/Uniklinik (Ethikkommission Universität Heidelberg); Homburg (Ethikkommission Saarbrücken); Immenhausen (Ethikkommission Landesärztekammer Hessen); Kiel (Ethikkommission Christian-Albrechts-Universität zu Kiel); Leipzig (Ethikkommission Universität Leipzig); Löwenstein (Ethikkommission Landesärztekammer Baden-Württemberg); Mainz (Ethikkommission Landesärztekammer Rheinland-Pfalz); München LMU/Gauting (Ethikkommission Klinikum Universität München); Nürnberg (Ethikkommission Friedrich-Alexander-Universität Erlangen Nürnberg); Rostock (Ethikkommission Universität Rostock); Berchtesgadener Land (Ethikkommission Land Salzburg); Schmallenberg (Ethikkommission Ärztekammer Westfalen-Lippe); Solingen (Ethikkommission Universität Witten-Herdecke); Ulm (Ethikkommission Universität Ulm); Würzburg (Ethikkommission Universität Würzburg) ethical committees and written informed consent was obtained from all patients. The ethics application for the COSYCONET study which was approved by all of the above mentioned central and local committees, includes the consent of the patients that their data may be used for further future analyses of any kind. The current study is a secondary analysis of COSYCONET and therefore the study did not require separate ethical approval. The following statement (translated from the original patient informed consent), which was approved by all of the above mentioned ethical committees, confirms that the patient informed consent includes the consent to have their data used in any future study based on COSYCONET data.
I also consent to the recording of disease data as part of the study and to its storage and disclosure in accordance with Patient Information IV.
I agree that blood samples, respiratory samples and urine samples may be taken for research purposes as part of my participation in the study and that these samples may be used for current and future research into COPD and may also be passed on to other researchers outside COSYCONET in an anonymous form in this context I consent to my data and biomaterial samples being used for an indefinite period.
I am aware that my data and biomaterial samples can be used for a very long time. The right to use my data and biomaterial samples persists after my death.
I also agree that in the event of death, an independent committee consisting of three experts and appointed by the management of the Asthma/COPD Competence Network may view my medical records and contact the treating physicians to determine the cause of death. In this case, I release my treating doctor from his duty of confidentiality.”The study was based on 2741 patients recruited within the COSYCONET framework (ClinicalTrials.gov, Identifier: NCT01245933). For further information see Karch A, Vogelmeier C, Welte T, Bals R, Kauczor HU, Biederer J, Heinrich J, Schulz H, Glaser S, Holle R et al: The German COPD cohort COSYCONET: Aims, methods and descriptive analysis of the study population at baseline. Respir Med 2016, 114:27–37.
For further information see:
Karch A, Vogelmeier C, Welte T, Bals R, Kauczor HU, Biederer J, Heinrich J, Schulz H, Glaser S, Holle R et al: The German COPD cohort COSYCONET: Aims, methods and descriptive analysis of the study population at baseline. Respir Med. 2016;114:27-37.
Consent for Publication
Within the ethical approval of COSYCONET, the participants of the study gave their consent to publish the data collected without reference to their person.
Acknowledgments
We are grateful to all COSYCONET study centers, especially to all study nurses, for their excellent and enduring work in data collection, as well as to all patients who were willing to participate in this study. COSYCONET is supported by the German Federal Ministry of Education and Research (BMBF) Competence Network Asthma and COPD (ASCONET) and performed in collaboration with the German Center for Lung Research (DZL). The project is funded by the BMBF with grant number 01 GI 0881, and is supported by unrestricted grants from AstraZeneca GmbH, Bayer Schering Pharma AG, Boehringer Ingelheim Pharma GmbH & Co. KG, Chiesi GmbH, GlaxoSmithKline, Grifols Deutschland GmbH, MSD Sharp & Dohme GmbH, Mundipharma GmbH, Novartis Deutschland GmbH, Pfizer Pharma GmbH, Takeda Pharma Vertrieb GmbH & Co. KG, Teva GmbH for patient investigations and laboratory measurements. The funding body had no involvement in the design of the study, or the collection, analysis or interpretation of the data.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Professor Robert Bals reports grants from BMBF, during the conduct of the study; grants, personal fees from Various, outside the submitted work. Dr Claus F Vogelmeier reports grants from German Ministry of Education and Science (BMBF), during the conduct of the study; personal fees from Aerogen, grants, personal fees from AstraZeneca, grants, personal fees from Boehringer Ingelheim, grants, personal fees from Chiesi, grants, personal fees from CSL Behring, grants, personal fees from GlaxoSmithKline, grants, personal fees from Grifols, personal fees from Menarini, grants, personal fees from Novartis, personal fees from Nuvaira, outside the submitted work. The authors declare that they have no other competing interests with regard to this study.
References
1. Vogelmeier CF, Criner GJ, Martinez FJ, et al. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease 2017 report: GOLD executive summary. Eur Respir J. 2017;49:3. doi:10.1183/13993003.00214-2017
2. Graf J, Jorres RA, Lucke T, Nowak D, Vogelmeier CF, Ficker JH. Medical treatment of COPD. Dtsch Arztebl Int. 2018;155(37):599–605. doi:10.3238/arztebl.2018.0599
3. Cameron-Tucker HL, Wood-Baker R, Owen C, Joseph L, Walters EH. Chronic disease self-management and exercise in COPD as pulmonary rehabilitation: a randomized controlled trial. Int J Chron Obstruct Pulmon Dis. 2014;9:513–523. doi:10.2147/COPD.S58478
4. Cannon D, Buys N, Sriram KB, Sharma S, Morris N, Sun J. The effects of chronic obstructive pulmonary disease self-management interventions on improvement of quality of life in COPD patients: a meta-analysis. Respir Med. 2016;121:81–90. doi:10.1016/j.rmed.2016.11.005
5. O’Conor R, Muellers K, Arvanitis M, et al. Effects of health literacy and cognitive abilities on COPD self-management behaviors: a prospective cohort study. Respir Med. 2019;160:105630. doi:10.1016/j.rmed.2019.02.006
6. Konigsdorfer N, Jorres RA, Sohler S, et al. Adherence to respiratory and nonrespiratory medication in patients with COPD: results of the German COSYCONET cohort. Patient Prefer Adherence. 2019;13:1711–1721. doi:10.2147/PPA.S223438
7. Wacker ME, Kitzing K, Jorres RA, et al. The contribution of symptoms and comorbidities to the economic impact of COPD: an analysis of the German COSYCONET cohort. Int J Chron Obstruct Pulmon Dis. 2017;12:3437–3448. doi:10.2147/COPD.S141852
8. Byng D, Lutter JI, Wacker ME, et al. Determinants of healthcare utilization and costs in COPD patients: first longitudinal results from the German COPD cohort COSYCONET. Int J Chron Obstruct Pulmon Dis. 2019;14:1423–1439. doi:10.2147/COPD.S201899
9. Lutter JI, Jorres RA, Kahnert K, et al. Health-related quality of life associates with change in FEV1 in COPD: results from the COSYCONET cohort. BMC Pulm Med. 2020;20(1):148. doi:10.1186/s12890-020-1147-5
10. Kahnert K, Lucke T, Huber RM, et al. Relationship of hyperlipidemia to comorbidities and lung function in COPD: results of the COSYCONET cohort. PLoS One. 2017;12(5):e0177501. doi:10.1371/journal.pone.0177501
11. Wacker ME, Jorres RA, Schulz H, et al. Direct and indirect costs of COPD and its comorbidities: results from the German COSYCONET study. Respir Med. 2016;111:39–46. doi:10.1016/j.rmed.2015.12.001
12. Karch A, Vogelmeier C, Welte T, et al. The German COPD cohort COSYCONET: aims, methods and descriptive analysis of the study population at baseline. Respir Med. 2016;114:27–37. doi:10.1016/j.rmed.2016.03.008
13. Lutter JI, Jorres RA, Welte T, et al. Impact of education on COPD severity and all-cause mortality in lifetime never-smokers and longtime ex-smokers: results of the COSYCONET cohort. Int J Chron Obstruct Pulmon Dis. 2020;15:2787–2798. doi:10.2147/COPD.S273839
14. Gershon AS, Dolmage TE, Stephenson A, Jackson B. Chronic obstructive pulmonary disease and socioeconomic status: a systematic review. COPD. 2012;9(3):216–226. doi:10.3109/15412555.2011.648030
15. White R, Walker P, Roberts S, Kalisky S, White P. Bristol COPD Knowledge Questionnaire (BCKQ): testing what we teach patients about COPD. Chron Respir Dis. 2006;3(3):123–131. doi:10.1191/1479972306cd117oa
16. Ray SM, Helmer RS, Stevens AB, Franks AS, Wallace LS. Clinical utility of the chronic obstructive pulmonary disease knowledge questionnaire. Fam Med. 2013;45(3):197–200.
17. Raptis DG, Rapti GG, Papathanasiou IV, Papagiannis D, Gourgoulianis KI, Malli F. Level of knowledge about COPD among patients and caregivers. Adv Exp Med Biol. 2021;1337:299–305.
18. Dawson AZ, Walker RJ, Egede LE. Differential relationships between diabetes knowledge scales and diabetes outcomes. Diabetes Educ. 2017;43(4):360–366. doi:10.1177/0145721717713316
19. Broos B, Charleer S, Bolsens N, et al. Diabetes knowledge and metabolic control in type 1 diabetes starting with continuous glucose monitoring: FUTURE-PEAK. J Clin Endocrinol Metab. 2021;106(8):e3037–e3048. doi:10.1210/clinem/dgab188
20. Gopalan A, Kellom K, McDonough K, Schapira MM. Exploring how patients understand and assess their diabetes control. BMC Endocr Disord. 2018;18(1):79. doi:10.1186/s12902-018-0309-4
21. Lindsay GM, Smith LN, Hanlon P, Wheatley DJ. Coronary artery disease patients’ perception of their health and expectations of benefit following coronary artery bypass grafting. J Adv Nurs. 2000;32(6):1412–1421. doi:10.1046/j.1365-2648.2000.01621.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Awareness of COPD and Its Risk Factors Among the Adult Population of the Aseer Region, Saudi Arabia
Esam Mahmood S, A Alqahtani AT, Alghamdi BAA, Gazzan MA, A Alqahtani MY, Y Alfaifi NA, Alsaleem SA, Riaz F, Tauheed Ahmad M, Ahmad A, Suhail Khan M, Saquib Abullais S
International Journal of Chronic Obstructive Pulmonary Disease 2023, 18:23-35
Published Date: 9 January 2023
The Efficacy of a Preoperative Occupational Therapy Educational Session for Saudi Patients Undergoing a Lower Extremity Joint Replacement
Al-Heizan MO, Shoman A, Tawffeq A, Banamah A, Balkhair F, Filimban S, Alsinan W, Batouk O, Turkistani T
Journal of Multidisciplinary Healthcare 2023, 16:31-38
Published Date: 10 January 2023
Comparing Knowledge Acquisition and Retention Between Mobile Learning and Traditional Learning in Teaching Respiratory Therapy Students: A Randomized Control Trial
Alhamad BR, Agha S
Advances in Medical Education and Practice 2023, 14:333-342
Published Date: 6 April 2023
The Effect of Family Planning Education on Knowledge, Attitude and Practice Toward Family Planning Methods Among Married Couples in Kersa and Goma Districts of Jimma Zone, South West Ethiopia
Yadassa F, Debelew GT, Birhanu Z
Risk Management and Healthcare Policy 2023, 16:2051-2062
Published Date: 2 October 2023
Comparison Between Game-Based Learning and Traditional Learning Methods in Traumatic Dental Management Among Dental Interns at KAUFD
Dardeer FM, Areesh RM, Alnafisi AA, Alzain I, Andijani BM, Abudawood SN, Abdullah AM, Ainousa AM, Alulaiyan M
Clinical, Cosmetic and Investigational Dentistry 2025, 17:381-390
Published Date: 25 August 2025