")
Back to Journals » Journal of Pain Research » Volume 15
The Burden of Metastatic Cancer–Induced Bone Pain: A Narrative Review
Authors Colosia A, Njue A, Bajwa Z, Dragon E, Robinson RL , Sheffield KM, Thakkar S , Richiemer SH
Received 19 April 2022
Accepted for publication 1 September 2022
Published 25 October 2022 Volume 2022:15 Pages 3399—3412
DOI https://doi.org/10.2147/JPR.S371337
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Amitabh Gulati
Ann Colosia,1 Annete Njue,2 Zahid Bajwa,3 Erika Dragon,4 Rebecca L Robinson,5 Kristin M Sheffield,5 Sheena Thakkar,6 Steven H Richiemer7
1Department of Market Access and Outcomes Strategy, RTI Health Solutions, Research Triangle Park, NC, USA; 2Department of Market Access and Outcomes Strategy, RTI Health Solutions, Manchester, UK; 3Medical Affairs, Eli Lilly and Company, Indianapolis, IN, USA; 4Medical Affairs, Pfizer, Ltd, Budapest, Hungary; 5Value, Evidence, and Outcomes, Eli Lilly and Company, Indianapolis, IN, USA; 6Patient Health & Impact, Pfizer Inc, New York, NY, USA; 7Division of Pain Medicine, Keck School of Medicine, University of Southern California, Los Angeles, CA, USA
Correspondence: Rebecca L Robinson, Eli Lilly and Company, Lilly Corporate Center, Indianapolis, IN, 46285, USA, Tel +1 3174331323, Fax +1 3172777444, Email [email protected]
Abstract: Bone pain is one of the most common forms of pain reported by cancer patients with metastatic disease. We conducted a review of oncology literature to further understand the epidemiology of and treatment approaches for metastatic cancer–induced bone pain and the effect of treatment of painful bone metastases on the patient’s quality of life. Two-thirds of patients with advanced, metastatic, or terminal cancer worldwide experience pain. Cancer pain due to bone metastases is the most common form of pain in patients with advanced disease and has been shown to significantly reduce patients’ quality of life. Treatment options for cancer pain due to bone metastases include nonsteroidal anti-inflammatory drugs, palliative radiation, bisphosphonates, denosumab, and opioids. Therapies including palliative radiation and opioids have strong evidence supporting their efficacy treating cancer pain due to bone metastases; other therapies, like bisphosphonates and denosumab, do not. There is sufficient evidence that patients who experience pain relief after radiation therapy have improved quality of life; however, a substantial proportion are nonresponders. For those still requiring pain management, even with available analgesics, many patients are undertreated for cancer pain due to bone metastases, indicating an unmet need. The studies in this review were not designed to determine why cancer pain due to bone metastases was undertreated. Studies specifically addressing cancer pain due to bone metastases, rather than general cancer pain, are limited. Additional research is needed to determine patient preferences and physician attitudes regarding choice of analgesic for moderate to severe cancer pain due to bone metastases.
Keywords: cancer, pain, bone, metastasis, quality of life, cancer patients
Introduction
Bone metastases are a significant contributor to the cancer-induced pain felt by over half of patients with metastatic cancer.1,2 In fact, bone pain is often the initial symptom of bone metastasis.3,4 The pain may come and go at first, becoming constant and gradually intensifying with time.5 Patients often experience worsening background pain in the months leading up to a diagnosis of bone metastasis.6 After a bone metastasis diagnosis, the proportion of patients experiencing pain may continue to rise at a slower rate than before diagnosis, likely as a result of more intensive patient management, including the introduction or intensification of pain medications.6 Severe spontaneous (ie breakthrough) pain occurs frequently, with acute and unpredictable occurrence and severity.5 Higher pain levels correlate with greater functional impairment.7
Metastatic cancer–induced bone pain (mCIBP) is caused by inflammation and bone remodeling (nociceptive pain) or by damage to or dysfunction of the nervous system (neuropathic pain) due to tumor invasion.8,9 Increasingly, research indicates that cancer-induced bone pain is often a combination of neuropathic and nociceptive pain, rather than distinct neurochemical events.10 Pain from persistent nerve activation or damage from bone metastases may result in peripheral or central sensitization.9 Cancer pain due to bone metastases may be background (tonic) pain, spontaneous at rest, related to movement (incident pain), or breakthrough pain, defined as a transitory flare of pain superimposed on an otherwise stable pattern under opioid therapy.7,11 These types of pain may be present alone or in combination. Incident pain can be managed by increasing the opioid dose above that which is effective for controlling pain at rest.11 Breakthrough pain is often unpredictable, sudden in onset (< 5 minutes from start of pain escalation until maximum pain), of short duration (often < 15 minutes), and particularly debilitating for patients.7,12,13
In this review, we describe the epidemiology of bone metastases by cancer type, the prevalence and severity of pain associated with bone metastases, the impact of this pain on health-related quality of life (HRQOL), and the effectiveness of current treatments on cancer pain due to bone metastases and on patients’ HRQOL. While many patients find some pain relief through current therapeutic methods and improvement in HRQOL from radiation treatment, our findings also identify patients’ unmet needs, with the hopes of providing guidance for future research.
We conducted a targeted literature review using search terms for cancer pain and epidemiology, HRQOL, practice patterns, and treatment guidelines to search literature databases (PubMed, Embase, Cochrane Library, and EconLit) for publications in the last 10 years; the search was conducted on August 20, 2020. We also searched the 2018–2020 meeting abstracts from key congresses (American Society of Clinical Oncology, European Society for Medical Oncology, European Pain Federation, International Society for Pharmacoeconomics and Outcomes Research, and National Comprehensive Care Network). We included reviews or primary studies of cancer pain due to bone metastases in adults.
Epidemiology of Cancer Pain
According to Smith et al’s systematic review of 122 cancer pain studies across disease subtypes, cancer pain is a prevalent issue for cancer patients, as 66.4% of patients with advanced, metastatic, or terminal cancer experienced pain related to their cancer.14 Further analysis showed that 51.9% of all patients with advanced, metastatic, or terminal cancer experienced moderate to severe cancer pain.
Cancer pain can result from a number of causes, but bone metastases are the most common cause in advanced disease.15 Bone metastases are relatively uncommon at initial cancer diagnosis but become increasingly common as the cancer metastasizes (Table 1). For most solid tumors, the incidence rate of bone metastases at initial diagnosis is in the single digits; however, 4.1–23.0% of patients in the United States (US) and up to 20.0% of patients in Japan present with bone metastases at their initial diagnosis with lung cancer.16–18 Still, at the initial diagnosis of metastatic cancer, nearly 40% of patients with kidney and renal pelvis cancer, 65% of patients with breast cancer, and 89% of patients with prostate cancer present with bone metastases.16,17,19 Overall, nearly 70% of patients with metastatic prostate cancer or breast cancer experience bone metastases.20–22 Additionally, most patients who do develop bone metastases experience pain. Across all cancer subtypes, approximately 80% of patients with bone metastases report moderate to severe bone pain.23 Routine assessment of the patient’s pain intensity is critical for effective pain management. Pain intensity is categorized as mild, moderate, or severe and treated accordingly, as described below.
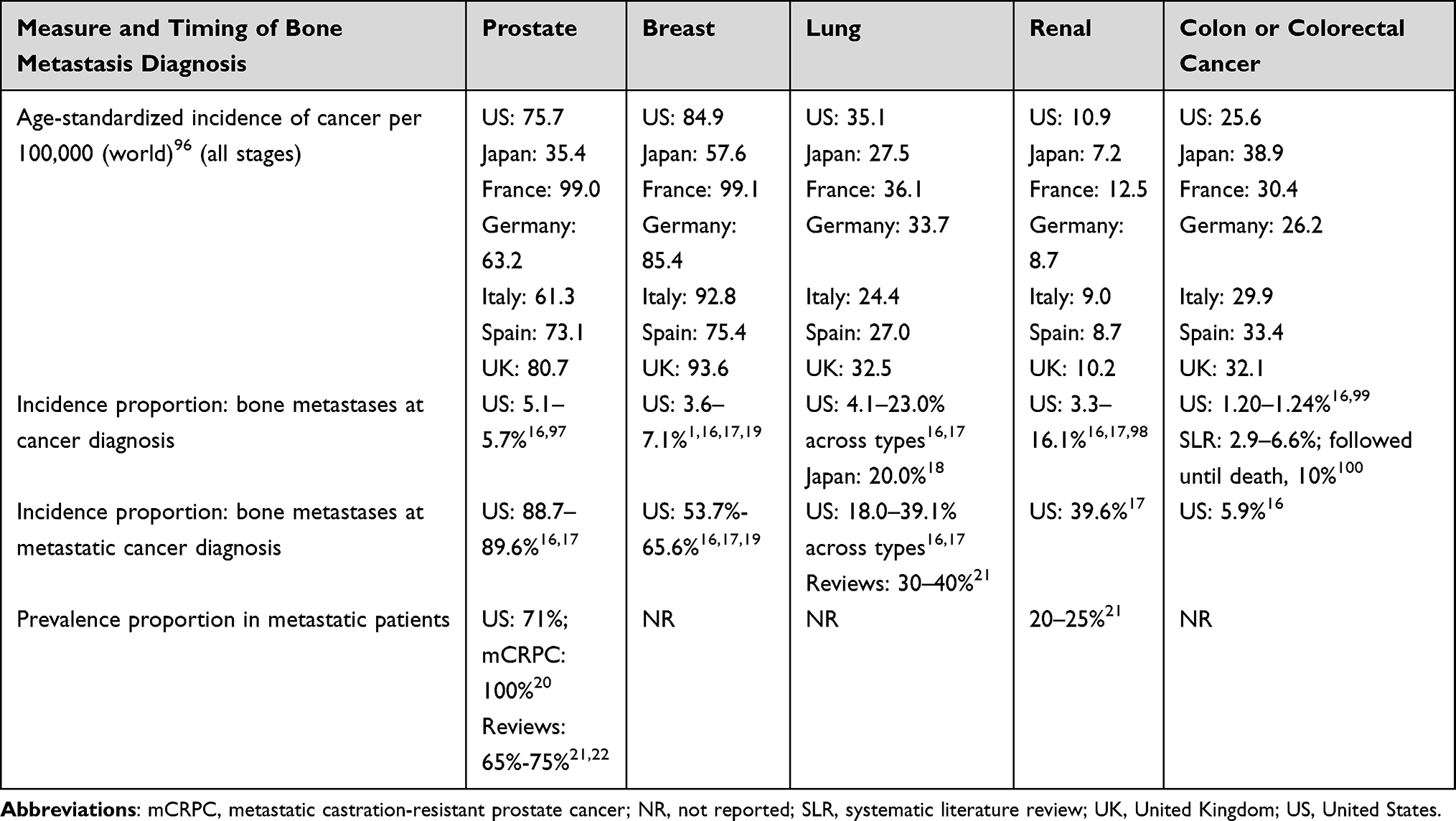 |
Table 1 Incidence Rates of Cancers by Country and Proportion with Bone Metastases |
Impact of Cancer Pain Due to Bone Metastases on HRQOL
The reduced quality of life experienced by cancer patients at an advanced disease state, who are often also experiencing treatment side effects, are compounded by mCIBP (Table 2). Cross-sectional studies of bone metastases arising from any primary cancer found that pain from bone metastases is associated with poorer HRQOL and worse physical function.24,25 Among the 174 patients with bone metastases in Japan surveyed by Shinoda, et al,24 the mean EQ-5D quality of life (QOL) score was found to be 0.58, lower than the population average of 0.85. Additionally, although physical function tends to worsen as patients’ pain intensity increases, the correlation between these two outcomes was reported as moderate in a study of 211 patients with cancer pain due to bone metastases.25 The authors could not definitively state that there was a causative relationship between pain intensity and physical function because of the presence of confounding variables (eg, tumor histology, disabling conditions). Higher bone pain severity was associated with significantly lower scores on the European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire–Core (EORTC QLQ-C30) generic cancer (Table 2). Patients with severe pain had a 21-point reduction in Global Health Status (GHS) score/QOL (as measured using EORTC QLQ-C30; total possible score = 100) compared with those who had no bone pain or only mild/moderate bone pain (P < 0.05) and an 18-point reduction in their physical functioning score compared with those with mild or no bone pain (P < 0.05).
 |
Table 2 Effect of Cancer Pain Due to Bone Metastasis on HRQOL |
Treatment Strategies and Outcomes
Several organizations have issued treatment guidelines for cancer pain, some of which are specifically for mCIBP.26–28 Other guidelines for cancer pain have sections on the treatment of bone metastases and related pain.8,29 In a European Society for Medical Oncology (ESMO) guideline subsection specifically on bone pain, Fallon et al8 state that external beam radiation therapy (EBRT) is the first line of treatment for cancer pain due to bone metastases, preceding or concurrent with analgesics if pain from uncomplicated bone metastases continues.8 Guidelines issued by the World Health Organization, ESMO, and the Spanish Society for Medical Oncology for the treatment of CIBP or mCIBP advocate a stepwise approach for pharmacological and minimally invasive therapies, using the mildest agents first (nonsteroidal anti-inflammatory drugs [NSAIDs] ± adjuvants), and if pain relief is inadequate, adding opioids, then minimally invasive procedures.8,30,31 Pain control should be evaluated to maintain medication at the lowest required doses.31,32
Radiation Therapy
Pain relief is obtained in 60% to 80% of patients with mCIBP treated with EBRT, including complete pain relief for 30%.8 Stereotactic body radiotherapy administers very high ablative doses of concentrated radiation but avoids radiation damage to critical normal tissues.8 Several representative studies have shown that patients who respond to palliative radiation therapy (RT) for painful bone metastases also experience improvements in functional outcomes and HRQOL (Table 3).33–38 These effects appear to be independent of the treatment regimen, which varies from a single dose of 8 grays (Gy) to longer treatment regimens (30 Gy in 10 fractions).34,35,39,40 Although a single 8-Gy fraction is equally effective for pain relief and is more cost-effective than higher fractionated doses of RT,41,42 it is associated with a higher incidence of retreatment.41
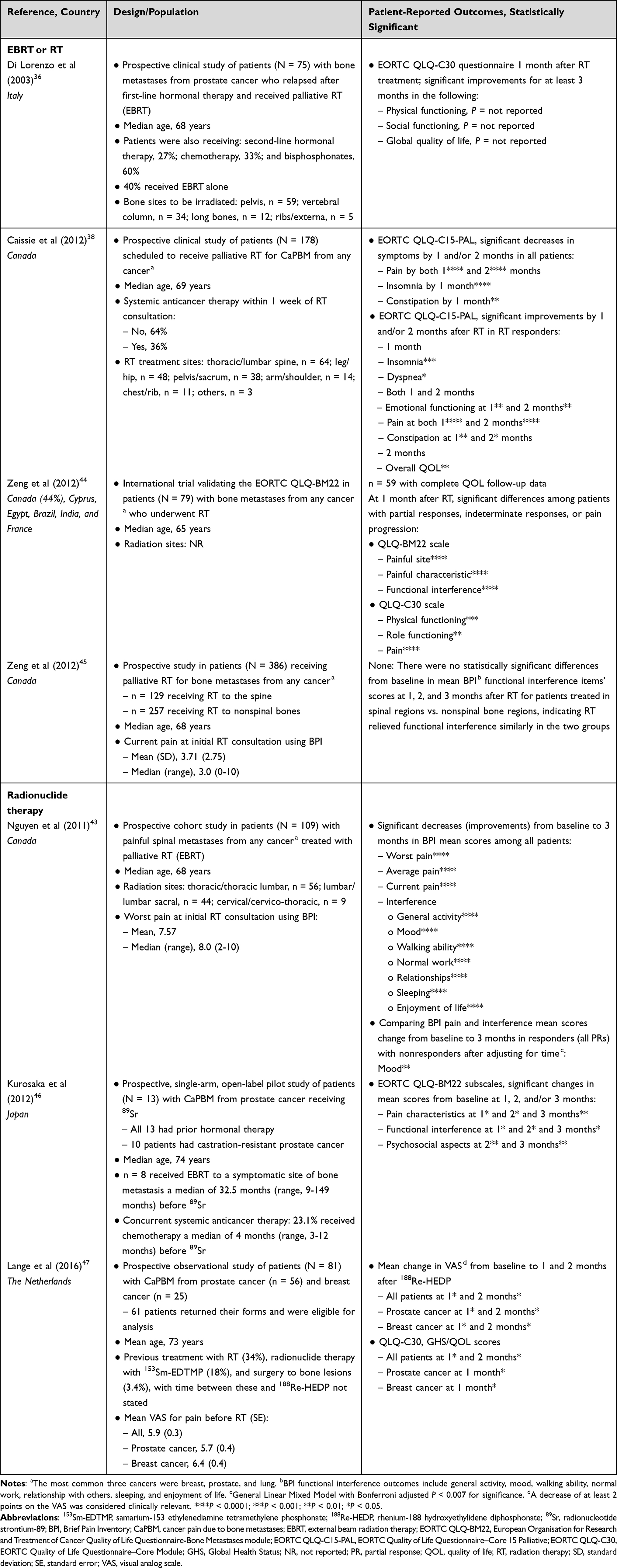 |
Table 3 Effect of Radiation Therapy on Cancer Pain Due to Bone Metastases |
In a prospective study involving 75 patients with painful bone metastases from prostate cancer treated with palliative RT, 81% experienced at least some form of pain relief, with 23% of patients experiencing complete relief following treatment.36 Significant improvements in physical functioning, social functioning, and global QOL scales of the EORTC QLQ-C30 persisted for at least 3 months, disappearing at 6 months’ posttreatment. Reduction in pain, fatigue, dyspnea, and sleep disturbance was also seen at 1 month and at 3 months but reoccurred at 6 months.
Similar results were observed in a separate study in which HRQOL was assessed using the EORTC Quality of Life Questionnaire Core-15 Palliative (EORTC QLQ-C15-PAL).38 Patients (n = 178) scheduled to receive palliative RT for painful bone metastases were assessed at Week 1, Week 2, Month 1, and Month 2 after receiving RT. Response to RT was defined according to the International Bone Metastases Consensus criteria43 as complete response (CR), partial response (PR), stable pain, or pain progression. Among those patients, 45% experienced either CR or PR at Week 1, which increased to 62% of patients at Week 2 and 65% at Month 2. Significant reductions in pain, insomnia, and constipation were seen by Month 1, and overall QOL improved significantly by Month 2 for patients who responded to RT. The proportion of nonresponders (patients with stable pain or pain progression) decreased over time from 54% at Week 1 to 38% at Week 2 and 35% at Month 2. Nonresponders had no improvement in median scores for overall QOL or functioning scales.
The EORTC QLQ-Bone Metastases module (EORTC QLQ-BM22) was used to assess bone metastasis–specific HRQOL in a multinational study involving 59 patients undergoing palliative RT.44 One month after RT, patients who responded to RT significantly improved in three of four QLQ-BM22 domains (painful site, painful characteristic, and functional interference) and three QLQ-C30 domains (physical functioning, role functioning, and pain). Patients with pain progression had significantly worse functional interference and pain compared with those who had a PR.
Studies specifically examining the benefits of palliative RT on spinal metastases showed pain scores decreased significantly after RT. A comparison between the outcomes for patients with spinal metastases versus nonspinal metastases showed that there was no statistical difference in the pain improvement or functional difference between the two groups, indicating that RT improved functional interference scores similarly for patients with spinal and nonspinal bone metastases.45 A separate study of palliative RT using radionucleotide strontium-89 (89Sr) to manage pain from spinal bone metastases found that 64% of patients experienced a PR after 3 months. Both psychosocial aspects and functional interference subscales improved by 2 months and remained improved by 3 months.46
89Sr was also able to reduce bone pain and improve HRQOL among 13 patients with prostate cancer and bone metastases for at least 3 months.46 Although this study had a small sample size, it showed that radionuclide therapy not only reduced pain but improved QOL in patients with prostate cancer with painful bone metastases. Similar improvements in pain and HRQOL were reported in a separate study using palliative radionucleotide therapy (188Rhenium-hydroxyethylidene diphosphonate [188Re-HEDP]) in routine clinical practice in patients with prostate or breast cancer and painful bone metastases.47 In this study, pain palliation was assessed using a visual analog scale, and QOL was assessed using the EORTC QLQ-C30 GHS/QOL scale. Overall, 69% of patients experienced reduction in pain following treatment with 188Re-HEDP while not increasing their opioid intake. The mean visual analog scale scores decreased across both subgroups at Weeks 4 and 8, while the mean GHS scores increased over the same period, indicating a reduction in bone pain and an increase in QOL, respectively.
One additional radiotherapy option for the management of mCIBP is brachytherapy with iodine-125 (125I brachytherapy), an internal RT. Surgical implantation of brachytherapy seeds near metastatic lesions is guided by computed tomography. In several studies, the use of 125I brachytherapy, which was occasionally performed in combination with other interventions like vertebroplasty, was able to reduce pain for patients with mCIBP for at least 24 weeks.48–50 One retrospective study that directly compared the outcomes for patients treated with EBRT or 125I brachytherapy found that 125I brachytherapy reduced pain scores on the Brief Pain Inventory and that it improved HRQOL.48 Clinical studies conducted by Wang et al and Yang et al also found that 125I brachytherapy reduced pain and improved HRQOL; Yang et al found that 98.0% of patients reported pain relief following 125I brachytherapy.49,50
Opioids
As previously mentioned, 60% to 80% of patients experience at least some pain relief after palliative RT, but only 30% experience complete pain relief following palliative RT.8 This leaves 20% to 40% of patients with no pain improvement from EBRT and another 30% to 50% with inadequate pain improvement. Analgesic options for cancer pain, including pain related to bone metastases, are based on the intensity of the pain. The drug classes considered for analgesia are NSAIDs, weak opioids, and strong opioids.31 Adjuvant therapies (eg, antidepressants, anticonvulsants, topical therapies) enhance the analgesic effects of other drugs and potentially allow for the reduction of analgesic doses.32,51 Relatively strong opioids (morphine, methadone, fentanyl, oxycodone, buprenorphine, tapentadol, hydromorphone, oxymorphone) with or without nonopioid analgesics or adjuvants are used for severe and persistent pain.32 Strong opioids are recommended for patients with moderate to severe cancer pain, including cancer pain due to bone metastases.8,29,31 Breakthrough cancer pain may be treated with rapid-onset opioids like fentanyl formulations, although the prevalence of breakthrough cancer pain is still 59% even after these drugs are introduced.14,52,53 Methadone is effective against both nociceptive and neuropathic pain and has been formulated for multiple delivery routes, making it an attractive candidate for treating cancer pain due to bone metastases.54 However, specific studies on methadone use on cancer pain due to bone metastases are lacking.
None of the studies identified in this targeted review assessed the impact of opioids on HRQOL in patients with cancer pain due to bone metastases. However, Table 4 summarizes the studies from this literature review that assessed whether patients with bone metastases were being treated appropriately for their pain level or cancer pain due to bone metastases. There is evidence for international underuse of opioids for cancer pain due to bone metastases. Two separate Canadian studies found that 25.8% to 48% of cancer patients with bone metastases were not prescribed adequately strong analgesics for their pain,55,56 and one of the studies found an increase in the proportion of patients undertreated over the study period (1999–2006).55 A Portuguese study found even greater undertreatment of adults with self-reported metastatic bone pain, with 84% of patients with moderate to severe pain not treated with a strong opioid.57 A multicountry study of analgesic and bone-targeting agent use in Europe found that 15% of patients with prostate cancer and moderate to severe pain from bone metastases were receiving only nonopioid analgesics, and another 33% were not receiving strong opioids.58 However, in a French study, analgesic use (89.9%) and, in particular, opioid use (77.7%) were common in patients with lung cancer and bone metastases.59
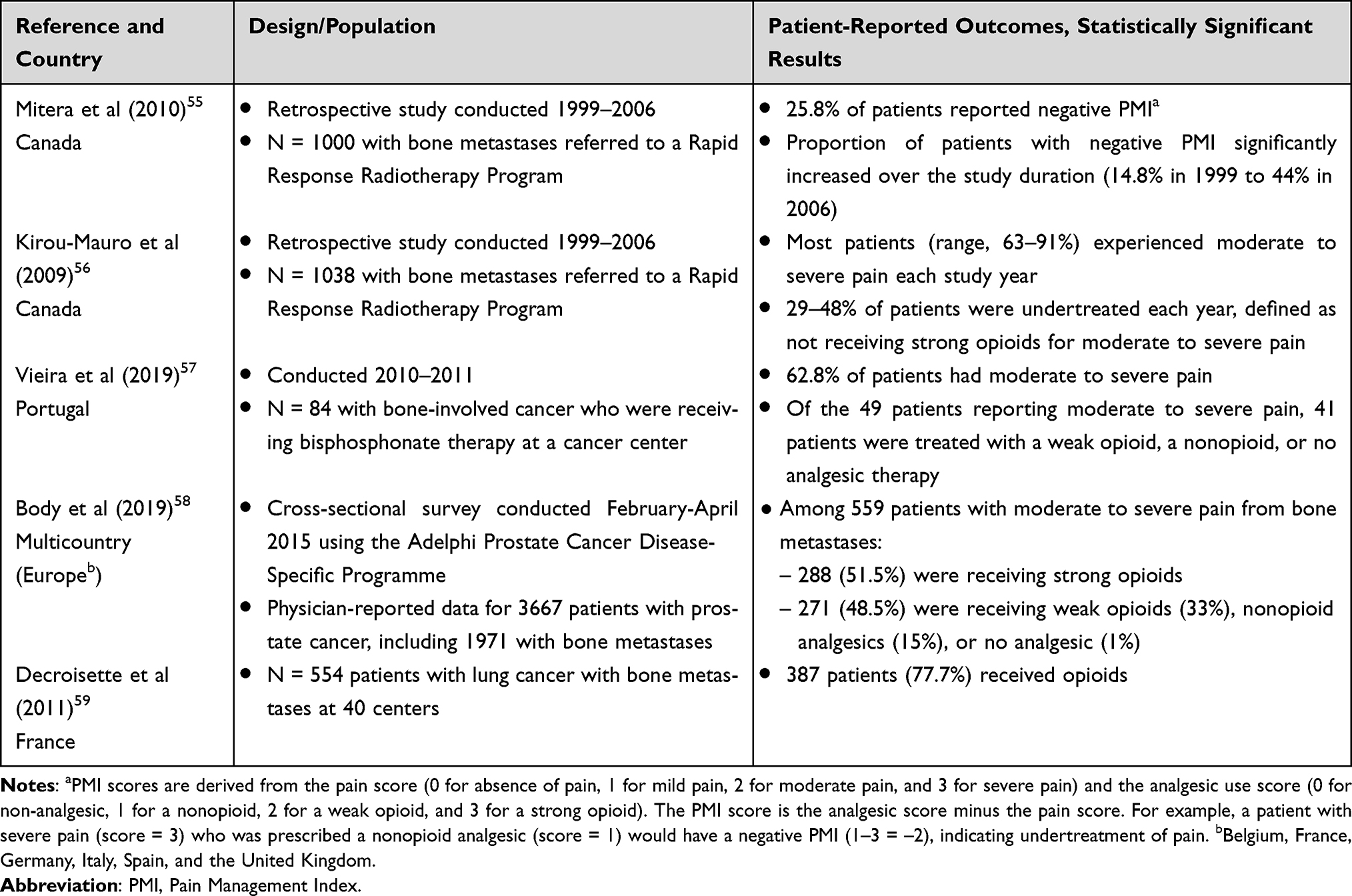 |
Table 4 Opioid Treatment Patterns |
Studies suggest that pain from bone metastases is more likely to be addressed when physicians are aware of the pain, such as following a skeletal-related event (SRE) or when cancer progresses after each successive line of therapy. A study with an international population of clinical trial participants with solid tumors found that the proportion of patients using strong opioids for moderate to severe pain remained relatively stable in patients who did not experience an SRE, whereas the proportion of patients using strong opioids increased in the 6 months preceding an SRE.60
Other Pharmacological Interventions
Radiation therapy and opioids are the most commonly used and effective forms of pain control for cancer patients with bone metastases, but many patients receive other pharmacological interventions, including NSAIDs and bisphosphonates. By blocking osteoclast activity, bisphosphonates can prevent fractures and other SREs.31 A chart review study in Japan found that both bisphosphonate and pain medication use increased as their other treatments progressed from first-line therapy to fourth-line therapy, with significantly higher use of bisphosphonates, NSAIDs, and opioids in patients with symptomatic skeletal events compared with patients without symptomatic skeletal events.61 However, the evidence for an analgesic effect of bisphosphonates on bone pain is weak.8 The analgesic effects of bisphosphonates are modest, so other medications are needed as the primary agent for pain relief.29 Similarly, evidence indicates denosumab delays the onset of pain but does not provide relief for established pain.8,62 Data from a systematic review by Hendriks et al63 highlight the lack of high-level evidence showing that bisphosphonates or denosumab reduce pain or improve QOL in patients with non–small-cell lung cancer with bone pain. Of 13 studies of bisphosphonates or denosumab identified in the Hendriks et al63 review, only five studies (in 6 reports) assessed QOL.64–69 Measures of QOL included the Functional Assessment of Cancer Therapy–General (FACT-G), EORTC QLQ-C30, and Lung Cancer Symptom Scale. Only two of the five studies reported a significant improvement in QOL.66,69 Hendriks et al63 concluded that the evidence that bisphosphonates or denosumab has an influence on QOL in patients with non–small-cell lung cancer and bone metastases is “very weak.”
Minimally Invasive and Surgical Interventions
A substantial proportion of the population with mCIBP has undertreated pain. Minimally invasive therapies (eg, epidural or intrathecal anesthesia, nerve blocks, ablative procedures, kyphoplasty, cementoplasty, and vertebroplasty) are an option when oral or injectable pharmacological therapies are not effective for persistent pain relief. Pain specialists may choose to use these minimally invasive, interventional treatments early in the pain treatment process or as complementary treatments alongside a standard pain management plan.9 However, minimally invasive, interventional therapies are currently underutilized.9 Minimally invasive procedures to strengthen bones weakened or fractured by the presence of metastases, including kyphoplasty and vertebroplasty, are recommended by several medical governing bodies to potentially improve QOL for patients with bone metastases.30,41,70,71 However, recent data on the impact of kyphoplasty or vertebroplasty on HRQOL are limited, and vertebroplasty is controversial, as studies on its efficacy in reducing mCIBP are mixed.72–75 A 2021 publication reported that, in patients with cancer pain due to bone metastases, pain was significantly reduced and HRQOL was significantly improved up to 6 months after either radiofrequency ablation alone or radiofrequency ablation with vertebroplasty.76
Surgery is an option for serious complications of bone metastases, including restoration of function because of spinal instability or impending spinal instability and pain that is intractable or was not relieved by nonsurgical therapy.77 Additionally, although surgical management of painful bone metastases improves patients’ functional outcome and pain as early as 2 weeks postoperatively, it does not appear to have any impact on HRQOL.78 However, HRQOL is affected by several factors, including bone metastases, the operation procedures endured by the patients, other comorbidities, and adjunctive treatments; these may have limited the ability to detect differences in HRQOL resulting from surgery.78
Discussion and Further Research
Although patients with bone metastases have limited longevity,79 for many patients, cancer pain due to bone metastases impacts their QOL for months or even years. For some cancers, such as breast and prostate cancer, the median survival of patients with bone metastases is approximately 2 years.80,81 There is a great need for therapeutic options that can provide pain relief and improve emotional, social, and physical functioning and overall HRQOL.
As described in this review, pain relief and improvements in HRQOL have been demonstrated for substantial proportions of patients treated with RT, although the improvements may take time to manifest and then wane over subsequent months. For patients continuing to experience moderate to severe cancer pain after RT for bone metastases, the current nonsurgical strategy is to treat the patient with strong opioids. However, evidence on opioid treatment patterns by pain severity suggests that opioids are underutilized in this patient population. The studies of undertreatment for cancer pain due to bone metastases were not designed to determine why patients were undertreated. A thorough, systematic investigation of opioid treatment patterns in patients with mCIBP is warranted.
Likely explanations for underuse are stigma around opioid addiction, prescribing limitations, and opioid side effects. Side effects include severe drowsiness, dry mouth, dizziness, breathing difficulties, and constipation, with the constipation persisting throughout treatment.82–84 Although persistent constipation can now be medically managed,8,85 in the US, patients with legitimate need for opioids now face stigma, fear, and guilt for using opioids.86 US patients also face access issues relating to pharmacy obstacles to filling prescriptions, insurance companies’ rules about types or amounts of medication allowed, and decreased manufacturing of opioids as a measure to limit inappropriate access.86,87 Outside the US in countries that did not experience an opioid crisis,88–90 physician and patient awareness and attitudes about pain and analgesics to control pain may still be contributing to the rise in undertreatment over time.55 Additionally, the lack of opioid availability and socioeconomic factors in some countries may negatively impact access to health care and pain management.
Palliative care is known to improve the QOL of patients with advanced cancer, and opioids remain a backbone of cancer palliative care. Patients with prolonged access (greater than 4 weeks prior to death) to strong opioids as part of their end-of-life care were less likely to require emergency hospitalization and chemotherapy near the end of life.91 While opioid use poses a number of challenges, leading to a large push to find opioid alternatives, access to opioids is essential for adequate cancer pain treatment. Ensuring patients have access to sufficient care, whether that takes the form of radiation or pharmacological interventions, is critical to ensuring the most positive outcomes possible.
This literature review indicates that there is a significant gap in research on the impact of cancer pain due to bone metastases on patients’ QOL. In particular, most studies of cancer pain due to bone metastases do not investigate the barriers to adequate pain management that can prolong patients’ QOL. Additionally, our findings suggest that additional treatment strategies are needed to sufficiently manage cancer pain due to bone metastases.
Limitations of This Review
This literature review was focused specifically on pain related to bone metastases. Other recent reviews have described management of cancer pain, and these articles provide discussions of opioids and other pharmacological and nonpharmacological interventions regardless of the source of cancer pain.54,92–95 Because of the narrow focus of our review, studies of the effect of opioids on HRQOL were not identified, nor were studies of economic burden associated with cancer pain due to bone metastases. Few of the identified studies provided real-world treatment patterns for patients with mCIBP. Only a few treatment pattern studies addressed whether moderate to severe cancer pain due to bone metastases was being treated per guidelines. Our intent was not to compare opioid use across countries that may have different restrictions on opioid use.
The proportion of patients seen at radiation centers may be an overestimation of the undertreatment problem because patients with adequately controlled cancer pain due to bone metastases are not typically referred to these centers.55,56 However, studies of patients with bone metastases seen at oncology or medical centers do not have this selection bias, and this review identified non‒radiation-center studies that also report undertreatment.57,58 None of the studies in this review were designed to determine the reason for undertreatment of their study populations.
Conclusions
Patients with mCIBP have lower HRQOL because of the impact of bone pain, in addition to other cancer symptoms, and our review found that these patients are globally undertreated for their pain. Radiation therapy for cancer pain due to bone metastases provides relief for many and improves HRQOL. However, a substantial proportion of patients obtain no relief from RT, and most others have incomplete relief. Strong opioids are recommended for those with moderate to severe cancer pain due to bone metastases. For many patients, RT fails to bring adequate relief and the use of opioids is often limited by side effects. This has created an ongoing unmet need for many patients with metastatic cancer–induced bone pain. Additional research is needed to determine patient preferences and physician attitudes regarding choice of analgesic for moderate to severe cancer pain due to bone metastases.
Abbreviations
125I, iodine-125; 153Sm, samarium-153; 188Re-HEDP, rhenium-188 hydroxyethylidene diphosphonate; 223R, radium; 89Sr, strontium-89; BPI, brief pain inventory; CI, confidence interval; CR, complete response; EBRT, external beam radiation therapy; EDTMP, ethylenediamine tetramethylene phosphonate; EORTC, European Organisation for Research and Treatment of Cancer; EORTC QLQ-BM22, EORTC-Bone Metastases module; EORTC QLQ-C15-PAL, EORTC Quality of Life Questionnaire Core-15 Palliative; EORTC QLQ-C30, European Organisation for Research and Treatment of Cancer Quality of Life Questionnaire–Core Module; EORTC QLQ-MY20, EORTC Quality of Life Questionnaire Multiple Myeloma module; ESMO, European Society for Medical Oncology; FACT-G, Functional Assessment of Cancer Therapy–General; GHS, Global Health Status; HEDP, hydroxyethylidene diphosphonate; HRQOL, health-related quality of life; K6 distress scale = Kessler Psychological Distress Scale 6; mCIBP, metastatic cancer–induced bone pain; mCRPC, metastatic castration-resistant prostate cancer; NR, not reported; NSAID, nonsteroidal anti-inflammatory drug; PMI, Pain Management Index; PR, partial response; PROMIS, Patient-Reported Outcomes Measurement Information System; QOL, quality of life; RT, radiation therapy; SD, standard deviation; SE, standard error; SLR, systematic literature review; SRE, skeletal-related event; UK, United Kingdom; US, United States; VAS, visual analog scale.
Acknowledgments
Medical writing support was provided by Sara Musetti Jenkins, PhD, RTI Health Solutions and was funded by Pfizer and Eli Lilly and Company. Editorial support was provided by Paul Hobson and Denise Lingenfelser of RTI Health Solutions, in the form of editorial and graphic services, and was funded by Pfizer and Eli Lilly and Company.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was sponsored by Pfizer and Eli Lilly and Company.
Disclosure
SR is an employee of the University of Southern California Medical Center. ZB, RR, and KMS are employees and stockholders of Eli Lilly. ED and ST are employees of Pfizer with stock and/or stock options. AC and AN are employees of RTI Health Solutions, an independent nonprofit research organization, which received funding from Pfizer and Eli Lilly and Pfizer to conduct this study and develop the manuscript. The authors report no other conflicts of interest in this work.
References
1. Body JJ, Quinn G, Talbot S, et al. Systematic review and meta-analysis on the proportion of patients with breast cancer who develop bone metastases. Crit Rev Oncol Hematol. 2017;115:67–80. doi:10.1016/j.critrevonc.2017.04.008
2. Hernandez RK, Adhia A, Wade SW, et al. Prevalence of bone metastases and bone-targeting agent use among solid tumor patients in the United States. Clin Epidemiol. 2015;7:335–345. doi:10.2147/CLEP.S85496
3. Ziu E, Viswanathan VK, Mesfin FB. Spinal Metastases. Treasure Island, FL: StatPearls Publishing; 2020.
4. American Cancer Society. Managing symptoms of bone metastases. American Cancer Society; 2016. Available from: https://www.cancer.org/treatment/understanding-your-diagnosis/advanced-cancer/bone-metastases.html.
5. Mantyh PW. Bone cancer pain: from mechanism to therapy. Curr Opin Support Palliat Care. 2014;8(2):83–90. doi:10.1097/SPC.0000000000000048
6. Cleeland C, von Moos R, Walker MS, et al. Burden of symptoms associated with development of metastatic bone disease in patients with breast cancer. Support Care Cancer. 2016;24(8):3557–3565. doi:10.1007/s00520-016-3154-x
7. Laird BJ, Walley J, Murray GD, et al. Characterization of cancer-induced bone pain: an exploratory study. Support Care Cancer. 2011;19(9):1393–1401. doi:10.1007/s00520-010-0961-3
8. Fallon M, Giusti R, Aielli F, et al. Management of cancer pain in adult patients: ESMO clinical practice guidelines. Ann Oncol. 2018;29(Suppl 4):191. doi:10.1093/annonc/mdy152
9. Sindhi V, Erdek M. Interventional treatments for metastatic bone cancer pain. Pain Manag. 2019;9(3):307–315. doi:10.2217/pmt-2018-0073
10. Falk S, Dickenson AH. Pain and nociception: mechanisms of cancer-induced bone pain. J Clin Oncol. 2014;32(16):1647–1654. doi:10.1200/JCO.2013.51.7219
11. Mercadante S, Villari P, Ferrera P, et al. Optimization of opioid therapy for preventing incident pain associated with bone metastases. J Pain Symptom Manage. 2004;28(5):505–510. doi:10.1016/j.jpainsymman.2004.02.024
12. Gater A, Abetz-Webb L, Battersby C, et al. Pain in castration-resistant prostate cancer with bone metastases: a qualitative study. Health Qual Life Outcomes. 2011;12(9):88. doi:10.1186/1477-7525-9-88
13. Habberstad R, Frøseth TCS, Aass N, et al. The Palliative Radiotherapy and Inflammation Study (PRAIS) - protocol for a longitudinal observational multicenter study on patients with cancer induced bone pain. BMC Palliat Care. 2018;17(1):110. doi:10.1186/s12904-018-0362-9
14. Smith H. A comprehensive review of rapid-onset opioids for breakthrough pain. CNS Drugs. 2012;26(6):509–535. doi:10.2165/11630580-000000000-00000
15. Dómine Gómez M, Díaz Fernández N, Cantos Sánchez de Ibargüen B, et al. Association of performance status and pain in metastatic bone pain management in the Spanish clinical setting. Adv Ther. 2017;34(1):136–147. doi:10.1007/s12325-016-0435-1
16. Huang JF, Shen J, Li X, et al. Incidence of patients with bone metastases at diagnosis of solid tumors in adults: a large population-based study. Ann Transl Med. 2020;8(7):482. doi:10.21037/atm.2020.03.55
17. Jiang W, Rixiati Y, Zhao B, et al. Incidence, prevalence, and outcomes of systemic malignancy with bone metastases. J Orthop Surg. 2020;28(2):2309499020915989. doi:10.1177/2309499020915989
18. Tsuya A, Kurata T, Tamura K, et al. Skeletal metastases in non-small cell lung cancer: a retrospective study. Lung Cancer. 2007;57(2):229–232. doi:10.1016/j.lungcan.2007.03.013
19. Gong Y, Zhang J, Ji P, et al. Incidence proportions and prognosis of breast cancer patients with bone metastases at initial diagnosis. Cancer Med. 2018;7(8):4156–4169. doi:10.1002/cam4.1668
20. Autio KA, Bennett AV, Jia X, et al. Prevalence of pain and analgesic use in men with metastatic prostate cancer using a patient-reported outcome measure. J Oncol Pract. 2013;9(5):223–229. doi:10.1200/JOP.2013.000876
21. Coleman RE. Metastatic bone disease: clinical features, pathophysiology and treatment strategies. Cancer Treat Rev. 2001;27(3):165–176. doi:10.1053/ctrv.2000.0210
22. Guerra Liberal FDC, Tavares AAS, Tavares J. Palliative treatment of metastatic bone pain with radiopharmaceuticals: a perspective beyond Strontium-89 and Samarium-153. Appl Radiat Isot. 2016;110:87–99. doi:10.1016/j.apradiso.2016.01.003
23. Janjan NA, Payne R, Gillis T, et al. Presenting symptoms in patients referred to a multidisciplinary clinic for bone metastases. J Pain Symptom Manage. 1998;16(3):171–178. doi:10.1016/S0885-3924(98)00069-4
24. Shinoda Y, Sawada R, Yoshikawa F, et al. Factors related to the quality of life in patients with bone metastases. Clin Exp Metastasis. 2019;36(5):441–448. doi:10.1007/s10585-019-09983-0
25. Janssen SJ, Pereira NRP, Thio Q, et al. Physical function and pain intensity in patients with metastatic bone disease. J Surg Oncol. 2019;120(3):376–381. doi:10.1002/jso.25510
26. Japan Society of Clinical Oncology. Bone metastasis clinical practice guidelines [article in Japanese]; 2015. Available from: https://minds.jcqhc.or.jp/n/med/4/med0203/G0000748/0001.
27. Lutz S, Chow E. A review of recently published radiotherapy treatment guidelines for bone metastases: contrasts or convergence? J Bone Oncol. 2012;1(1):18–23. doi:10.1016/j.jbo.2012.04.002
28. Van Poznak CH, Temin S, Yee GC, et al. American society of clinical oncology executive summary of the clinical practice guideline update on the role of bone-modifying agents in metastatic breast cancer. J Clin Oncol. 2011;29(9):1221–1227. doi:10.1200/JCO.2010.32.5209
29. NCCN, National Comprehensive Cancer Network. NCCN Clinical Practice Guidelines In Oncology (NCCN Guidelines®) for Adult Cancer Pain. V.1.2020.
30. Jara C, Del Barco S, Grávalos C, et al. SEOM clinical guideline for treatment of cancer pain (2017). Clin Transl Oncol. 2018;20(1):97–107. doi:10.1007/s12094-017-1791-2
31. World Health Organization. World Health Organization guidelines for the pharmacological and radiotherapeutic management of cancer pain in adults and adolescents. World Health Organization; 2019. Available from: https://www.who.int/publications/i/item/who-guidelines-for-the-pharmacological-and-radiotherapeutic-management-of-cancer-pain-in-adults-and-adolescents.
32. Anekar AA, Cascella M. World Health Organization analgesic ladder. In: StatPearls. Treasure Island (FL): StatPearls Publishing. Copyright © 2020, StatPearls Publishing LLC; 2020.
33. Koufopoulou C, Mosa E, Charalampakis N, et al. Evaluation of quality of life outcomes following palliative radiotherapy in bone metastases: a literature review. J BUON. 2019;24(5):1747–1760.
34. Faris A, Expósito J, Martínez-única A, et al. The efficacy of three-dimensional conformal radiation therapy on pain and quality of life in patients with painful bone metastases: a prospective study. Croat Med J. 2020;61(3):215–222. doi:10.3325/cmj.2020.61.215
35. Arias F, Arrarás JI, Asín G, et al. To what extent does radiotherapy improve the quality of life of patients with bone metastasis? A prospective, single-institutional study. Am J Clin Oncol. 2018;41(2):163–166. doi:10.1097/COC.0000000000000249
36. Di Lorenzo G, Autorino R, Ciardiello F, et al. External beam radiotherapy in bone metastatic prostate cancer: impact on patients’ pain relief and quality of life. Oncol Rep. 2003;10(2):399–404.
37. McDonald R, Chow E, Rowbottom L, et al. Quality of life after palliative radiotherapy in bone metastases: a literature review. J Bone Oncol. 2015;4(1):24–31. doi:10.1016/j.jbo.2014.11.001
38. Caissie A, Zeng L, Nguyen J, et al. Assessment of health-related quality of life with the European Organization for Research and Treatment of Cancer QLQ-C15-PAL after palliative radiotherapy of bone metastases. Clin Oncol. 2012;24(2):125–133. doi:10.1016/j.clon.2011.08.008
39. Conway JL, Yurkowski E, Glazier J, et al. Comparison of patient-reported outcomes with single versus multiple fraction palliative radiotherapy for bone metastasis in a population-based cohort. Radiother Oncol. 2016;119(2):202–207. doi:10.1016/j.radonc.2016.03.025
40. Westhoff PG, Verdam MGE, Oort FJ, et al. Course of quality of life after radiation therapy for painful bone metastases: a detailed analysis from the Dutch bone metastasis study. Int J Radiat Oncol Biol Phys. 2016;95(5):1391–1398. doi:10.1016/j.ijrobp.2016.03.032
41. Lutz S, Balboni T, Jones J, et al. Palliative radiation therapy for bone metastases: update of an ASTRO evidence-based guideline. Pract Radiat Oncol. 2017;7(1):4–12. doi:10.1016/j.prro.2016.08.001
42. Simoff MJ, Lally B, Slade MG, et al. Symptom management in patients with lung cancer: diagnosis and management of lung cancer, 3rd ed: American College of Chest Physicians evidence-based clinical practice guidelines. Chest. 2013;143(5 SUPPL):e455S–e497S. doi:10.1378/chest.12-2366
43. Nguyen J, Chow E, Zeng L, et al. Palliative response and functional interference outcomes using the brief pain inventory for spinal bony metastases treated with conventional radiotherapy. Clin Oncol. 2011;23(7):485–491. doi:10.1016/j.clon.2011.01.507
44. Zeng L, Chow E, Bedard G, et al. Quality of life after palliative radiation therapy for patients with painful bone metastases: results of an international study validating the EORTC QLQ-BM22. Int J Radiat Oncol Biol Phys. 2012;84(3):e337–342. doi:10.1016/j.ijrobp.2012.05.028
45. Zeng L, Chow E, Zhang L, et al. Comparison of pain response and functional interference outcomes between spinal and non-spinal bone metastases treated with palliative radiotherapy. Support Care Cancer. 2012;20(3):633–639. doi:10.1007/s00520-011-1144-6
46. Kurosaka S, Satoh T, Chow E, et al. EORTC QLQ-BM22 and QLQ-C30 quality of life scores in patients with painful bone metastases of prostate cancer treated with strontium-89 radionuclide therapy. Ann Nucl Med. 2012;26(6):485–491. doi:10.1007/s12149-012-0598-z
47. Lange R, Overbeek F, de Klerk JM, et al. Treatment of painful bone metastases in prostate and breast cancer patients with the therapeutic radiopharmaceutical rhenium-188-HEDP. Clinical benefit in a real-world study. Nuklearmedizin. 2016;55(5):188–195. doi:10.3413/Nukmed-0828-16-05
48. Xiang Z, Wang L, Yan H, et al. (125) I seed brachytherapy versus external beam radiation therapy for the palliation of painful bone metastases of lung cancer after one cycle of chemotherapy progression. Onco Targets Ther. 2018;11:5183–5193. doi:10.2147/OTT.S154973
49. Yang Z, Tan J, Zhao R, et al. Clinical investigations on the spinal osteoblastic metastasis treated by combination of percutaneous vertebroplasty and (125)I seeds implantation versus radiotherapy. Cancer Biother Radiopharm. 2013;28(1):58–64. doi:10.1089/cbr.2012.1204
50. Wang W, Liu Z, Zhu J, et al. Brachytherapy with iodine 125 seeds for bone metastases. J Cancer Res Ther. 2017;13(5):742–747. doi:10.4103/jcrt.JCRT_399_17
51. Swarm RA, Paice JA, Anghelescu DL, et al. Adult cancer pain, version 3.2019. J Natl Compr Canc Netw. 2019;17(8):977–1007.
52. Deandrea S, Corli O, Consonni D, et al. Prevalence of breakthrough cancer pain: a systematic review and a pooled analysis of published literature. J Pain Symptom Manage. 2014;47(1):57–76. doi:10.1016/j.jpainsymman.2013.02.015
53. van den Beuken-van Everdingen M.H., Hochstenbach, L. M., Joosten, E. A., Tjan-Heijnen, V.C., Janssen, D. J. Update on prevalence of pain in patients with cancer: systematic review and meta-analysis. J Pain Symptom Manage. 2016;51(6):1070–1090.e9. doi:10.1016/j.jpainsymman.2015.12.340
54. Edmonds KP, Saunders IM, Willeford A, et al. Emerging challenges to the safe and effective use of methadone for cancer-related pain in paediatric and adult patient populations. Drugs. 2020;80(2):115–130. doi:10.1007/s40265-019-01234-6
55. Mitera G, Zeiadin N, Kirou-Mauro A, et al. Retrospective assessment of cancer pain management in an outpatient palliative radiotherapy clinic using the pain management index. J Pain Symptom Manage. 2010;39(2):259–267. doi:10.1016/j.jpainsymman.2009.07.005
56. Kirou-Mauro AM, Hird A, Wong J, et al. Has pain management in cancer patients with bone metastases improved? A seven-year review at an outpatient palliative radiotherapy clinic. J Pain Symptom Manage. 2009;37(1):77–84. doi:10.1016/j.jpainsymman.2007.12.014
57. Vieira C, Fragoso M, Pereira D, et al. Pain prevalence and treatment in patients with metastatic bone disease. Oncol Lett. 2019;17(3):3362–3370.
58. Body JJ, von Moos R, Rider A, et al. A real-world study assessing the use of bone-targeted agents and their impact on bone metastases in patients with prostate cancer treated in clinical practice in Europe. J Bone Oncol. 2019;14:100212. doi:10.1016/j.jbo.2018.100212
59. Decroisette C, Monnet I, Berard H, et al. Epidemiology and treatment costs of bone metastases from lung cancer: a French prospective, observational, multicenter study (GFPC 0601). J Thorac Oncol. 2011;6(3):576–582. doi:10.1097/JTO.0b013e318206a1e3
60. von Moos R, Body -J-J, Egerdie B, et al. Pain and analgesic use associated with skeletal-related events in patients with advanced cancer and bone metastases. Support Care Cancer. 2016;24(3):1327–1337. doi:10.1007/s00520-015-2908-1
61. Uemura H, DiBonaventura M, Wang E, et al. The treatment patterns of castration-resistant prostate cancer in Japan, including symptomatic skeletal events and associated treatment and healthcare resource use. Expert Rev Pharmacoecon Outcomes Res. 2017;17(5):511–517. doi:10.1080/14737167.2017.1300530
62. Porta-Sales J, Garzón-Rodríguez C, Llorens-Torromé S, et al. Evidence on the analgesic role of bisphosphonates and denosumab in the treatment of pain due to bone metastases: a systematic review within the European Association for Palliative Care guidelines project. Palliat Med. 2017;31(1):5–25. doi:10.1177/0269216316639793
63. Hendriks LE, Hermans BC, van den Beuken-van Everdingen MH, et al. Effect of bisphosphonates, denosumab, and radioisotopes on bone pain and quality of life in patients with non-small cell lung cancer and bone metastases: a systematic review. J Thorac Oncol. 2016;11(2):155–173. doi:10.1016/j.jtho.2015.10.001
64. Rosen LS, Gordon D, Tchekmedyian NS, et al. Long-term efficacy and safety of zoledronic acid in the treatment of skeletal metastases in patients with nonsmall cell lung carcinoma and other solid tumors: a randomized, phase III, double-blind, placebo-controlled trial. Cancer. 2004;100(12):2613–2621. doi:10.1002/cncr.20308
65. Rosen LS, Gordon D, Tchekmedyian S, et al. Zoledronic acid versus placebo in the treatment of skeletal metastases in patients with lung cancer and other solid tumors: a phase III, double-blind, randomized trial--the zoledronic acid lung cancer and other solid tumors study group. J Clin Oncol. 2003;21(16):3150–3157. doi:10.1200/JCO.2003.04.105
66. Facchini G, Caraglia M, Santini D, et al. The clinical response on bone metastasis from breast and lung cancer during treatment with zoledronic acid is inversely correlated to skeletal related events (SRE). J Exp Clin Cancer Res. 2007;26(3):307–312.
67. Ishiwata T, Hirose T, Hirama M, et al. A feasibility study of zoledronic acid combined with carboplatin/nedaplatin plus paclitaxel in patients with non-small cell lung cancer with bone metastases. Tumori. 2011;97(5):568–572. doi:10.1177/030089161109700505
68. Longo F, Del Signore E, De Sanctis R, et al. Zoledronic acid and treatment of bone metastasis in patients with advanced lung cancer (NSCLC and SCLC). Ann Oncol. 2008;19(S8):viii258.
69. Del Signore E, De Marinis F. Zoledronic acid role in SREs prevention: an advantage for all patients with advanced NSCLC and bone metastases? J Thorac Oncol. 2012;7(6):S78.
70. Terpos E, Morgan G, Dimopoulos MA, et al. International Myeloma Working Group recommendations for the treatment of multiple myeloma-related bone disease. J Clin Oncol. 2013;31(18):2347–2357. doi:10.1200/JCO.2012.47.7901
71. Lutz S, Berk L, Chang E, et al. Palliative radiotherapy for bone metastases: an ASTRO evidence-based guideline. Int J Radiat Oncol Biol Phys. 2011;79(4):965–976. doi:10.1016/j.ijrobp.2010.11.026
72. Hackbarth CB, Vogl TJ, Naguib N, et al. Long-term evaluation of pain reduction after vertebroplasty and kyphoplasty. Acta Radiol Open. 2021;10(7):20584601211028994. doi:10.1177/20584601211028994
73. Sadeghi-Naini M, Aarabi S, Shokraneh F, et al. Vertebroplasty and kyphoplasty for metastatic spinal lesions: a systematic review. Clin Spine Surg. 2018;31(5):203–210. doi:10.1097/BSD.0000000000000601
74. Bao L, Jia P, Li J, et al. Percutaneous vertebroplasty relieves pain in cervical spine metastases. Pain Res Manag. 2017;2017:3926318. doi:10.1155/2017/3926318
75. Mezrich JL, Resnik CS. Panacea or sham? Legal issues of vertebroplasty. J Am Coll Radiol. 2016;13(6):663–665. doi:10.1016/j.jacr.2016.02.006
76. Yildizhan S, Boyaci MG, Rakip U, et al. Role of radiofrequency ablation and cement injection for pain control in patients with spinal metastasis. BMC Musculoskelet Disord. 2021;22(1):912. doi:10.1186/s12891-021-04799-0
77. Biermann JS, Holt GE, Lewis VO, et al. Metastatic bone disease: diagnosis, evaluation, and treatment. J Bone Joint Surg Am. 2009;91(6):1518–1530.
78. Nooh A, Goulding K, Isler MH, et al. Early improvement in pain and functional outcome but not quality of life after surgery for metastatic long bone disease. Clin Orthop Relat Res. 2018;476(3):535–545. doi:10.1007/s11999.0000000000000065
79. Sugiura H, Yamada K, Sugiura T, et al. Predictors of survival in patients with bone metastasis of lung cancer. Clin Orthop Relat Res. 2008;466(3):729–736. doi:10.1007/s11999-007-0051-0
80. McCloskey EV, Guest JF, Kanis JA. The clinical and cost considerations of bisphosphonates in preventing bone complications in patients with metastatic breast cancer or multiple myeloma. Drugs. 2001;61(9):1253–1274. doi:10.2165/00003495-200161090-00003
81. Halabi S, Kelly WK, Ma H, et al. Meta-analysis evaluating the impact of site of metastasis on overall survival in men with castration-resistant prostate cancer. J Clin Oncol. 2016;34(14):1652–1659. doi:10.1200/JCO.2015.65.7270
82. ALMouaalamy N. Opioid-induced constipation in advanced cancer patients. Cureus. 2021;13(4):e14386. doi:10.7759/cureus.14386
83. Khan F, Mehan A. Addressing opioid tolerance and opioid-induced hypersensitivity: recent developments and future therapeutic strategies. Pharmacol Res Perspect. 2021;9(3):e00789. doi:10.1002/prp2.789
84. Wiffen PJ, Derry S, Moore RA. Impact of morphine, fentanyl, oxycodone or codeine on patient consciousness, appetite and thirst when used to treat cancer pain. Cochrane Database Syst Rev. 2014;2014(5):Cd011056.
85. Streicher JM, Bilsky EJ. Peripherally acting mu-opioid receptor antagonists for the treatment of opioid-related side effects: mechanism of action and clinical implications. J Pharm Pract. 2018;31(6):658–669. doi:10.1177/0897190017732263
86. Azizoddin DR, Knoerl R, Adam R, et al. Cancer pain self-management in the context of a national opioid epidemic: experiences of patients with advanced cancer using opioids. Cancer. 2021;127:3239–3245. doi:10.1002/cncr.33532
87. Rodrigue D, Winkelmann J, Price M, et al. Opioid misuse: an organizational response while managing cancer-related pain. Clin J Oncol Nurs. 2020;24(2):170–176. doi:10.1188/20.CJON.170-176
88. Rosner B, Neicun J, Yang JC, et al. Opioid prescription patterns in Germany and the global opioid epidemic: systematic review of available evidence. PLoS One. 2019;14(8):e0221153. doi:10.1371/journal.pone.0221153
89. Fischer B, Daldegan-Bueno COK-M, Daldegan-Bueno D, et al. Why comparative epidemiological indicators suggest that New Zealand is unlikely to experience a severe opioid epidemic. Int J Drug Policy. 2021;93:103166. doi:10.1016/j.drugpo.2021.103166
90. Singh B, Rao R. PerspectivesIs there an opioid epidemic in India? J Public Health. 2021;43((Suppl 2)):ii43–ii50. doi:10.1093/pubmed/fdab322
91. Ziegler LE, Craigs CL, West RM, et al. Is palliative care support associated with better quality end-of-life care indicators for patients with advanced cancer? A retrospective cohort study. BMJ Open. 2018;8(1):e018284. doi:10.1136/bmjopen-2017-018284
92. Chapman EJ, Edwards Z, Boland JW, et al. Practice review: evidence-based and effective management of pain in patients with advanced cancer. Palliat Med. 2020;34(4):444–453. doi:10.1177/0269216319896955
93. Hao D, Sidharthan S, Cotte J, et al. Interventional therapies for pain in cancer patients: a narrative review. Curr Pain Headache Rep. 2021;25(7):44. doi:10.1007/s11916-021-00963-2
94. Gress KL, Charipova K, Kaye AD, et al. An overview of current recommendations and options for the management of cancer pain: a comprehensive review. Oncol Ther. 2020;8(2):251–259. doi:10.1007/s40487-020-00128-y
95. Degnan M, Mousa SA. A narrative review of buprenorphine in adult cancer pain. Expert Rev Clin Pharmacol. 2020;13(10):1159–1167. doi:10.1080/17512433.2020.1822163
96. IARC. Global cancer observatory: GLOBOCAN 2018. International Agency for Research on Cancer. 2018. Available from: https://gco.iarc.fr/.
97. Guo X, Zhang C, Guo Q, et al. The homogeneous and heterogeneous risk factors for the morbidity and prognosis of bone metastasis in patients with prostate cancer. Cancer Manag Res. 2018;10:1639–1646. doi:10.2147/CMAR.S168579
98. Guo Q, Zhang C, Guo X, et al. Incidence of bone metastasis and factors contributing to its development and prognosis in newly diagnosed renal cell carcinoma: a population-based study. Cancer Manag Res. 2018;10:2935–2944. doi:10.2147/CMAR.S170083
99. Guo X, Zhang C, Ma W, et al. Patterns of bone metastases in newly diagnosed colorectal cancer: a real-world analysis in the SEER database. Int J Colorectal Dis. 2019;34(3):533–543. doi:10.1007/s00384-018-3213-5
100. Christensen TD, Jensen SG, Larsen FO, et al. Systematic review: incidence, risk factors, survival and treatment of bone metastases from colorectal cancer. J Bone Oncol. 2018;13:97–105. doi:10.1016/j.jbo.2018.09.009
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.