")
Back to Journals » Journal of Pain Research » Volume 16
A Systematic Review and Meta-Analysis of the Effects of Rehabilitation Using Digital Healthcare on Musculoskeletal Pain and Quality of Life
Authors Jang S , Lee B , Lee E, Kim J, Lee JI, Lim JY , Hwang JH, Jang S
Received 5 September 2022
Accepted for publication 5 May 2023
Published 31 May 2023 Volume 2023:16 Pages 1877—1894
DOI https://doi.org/10.2147/JPR.S388757
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Alaa Abd-Elsayed
Suhyun Jang,1,* Boram Lee,2,* Eunji Lee,1 Jungbin Kim,1 Jong In Lee,3 Jae-Young Lim,4,5 Ji Hye Hwang,6 Sunmee Jang1
1College of Pharmacy and Gachon Institute of Pharmaceutical Sciences, Gachon University, Incheon, Republic of Korea; 2Graduate School of Public Health, Seoul National University, Seoul, Republic of Korea; 3Department of Rehabilitation Medicine, Seoul St. Mary’s Hospital, College of Medicine, The Catholic University of Korea, Seoul, Republic of Korea; 4Department of Rehabilitation Medicine, Seoul National University Bundang Hospital, Seongnam-si, Republic of Korea; 5Department of Rehabilitation Medicine, Seoul National University College of Medicine, Seoul, Republic of Korea; 6Department of Physical and Rehabilitation Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Republic of Korea
*These authors contributed equally to this work
Correspondence: Sunmee Jang, College of Pharmacy and Gachon Institute of Pharmaceutical Sciences, Gachon University, 191 Hambakmoe‑Ro, Yeonsu‑Gu, Incheon, 21936, Republic of Korea, Tel +82 32 820 4941, Email [email protected] Ji Hye Hwang, Department of Physical and Rehabilitation Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, #81 Irwon-Ro, Gangnam-Gu, Seoul, 06351, Republic of Korea, Tel +82 10 9933 2816, Email [email protected]
Abstract: Rehabilitation using digital healthcare (DHC) has the potential to enhance the effectiveness of treatment for musculoskeletal disorders (MSDs) and associated pain by improving patient outcomes, while being cost-effective, safe, and measurable. This systematic review and meta-analysis aimed to evaluate the effectiveness of musculoskeletal rehabilitation using DHC. We searched PubMed, Ovid-Embase, Cochrane Library, and PEDro Physiotherapy Evidence Database from inception to October 28, 2022 for controlled clinical trials comparing DHC to conventional rehabilitation. We used a random-effects model for the meta-analysis, pooling the effects of DHC on pain and quality of life (QoL) by calculating standardized mean differences (SMDs) with 95% confidence intervals (CIs) between DHC rehabilitation and conventional rehabilitation (control). Fifty-four studies with 6240 participants met the inclusion criteria. The sample size ranged from 26 to 461, and the average age of the participants ranged from 21.9 to 71.8 years. The majority of the included studies focused on knee or hip joint MSD (n = 23), and the most frequently utilized DHC interventions were mobile applications (n = 26) and virtual or augmented reality (n = 16). Our meta-analysis of pain (n = 45) revealed that pain reduction was greater in DHC rehabilitation than in conventional rehabilitation (SMD: − 0.55, 95% CI: − 0.74, − 0.36), indicating that rehabilitation using DHC has the potential to ameliorate MSD pain. Furthermore, DHC significantly improved health-related QoL and disease-specific QoL (SMD: 0.66, 95% CI: 0.29, 1.03; SMD: − 0.44, 95% CI: − 0.87, − 0.01) compared to conventional rehabilitation. Our findings suggest that DHC offers a practical and flexible rehabilitation alternative for both patients with MSD and healthcare professionals. Nevertheless, further researches are needed to elucidate the underlying mechanisms by which DHC affects patient-reported outcomes, which may vary depending on the type and design of the DHC intervention.
Keywords: musculoskeletal disorder, rehabilitation, digital healthcare, pain, quality of life, patient-reported outcomes
Introduction
The World Health Organization (WHO) adopted the “Resolution on Digital Health” introduced during the 71st World Health Assembly in May 2018 and recognized the need for digital technology to achieve universal health coverage and sustainable development goals.1 As such, digital healthcare (DHC), in which digital technology is converging with healthcare, has become increasingly important. Along with the fourth industrial revolution, changes in demographic structure, such as population aging, and social changes, such as smart device popularization, have stimulated the demand for DHC.2 Above all, the coronavirus disease 2019 pandemic has led to dramatic changes in the healthcare sector. Enabling contactless healthcare services, DHC has spread faster than ever.
Musculoskeletal disorders (MSDs) are a broad spectrum of chronic diseases affecting bones, joints, and soft tissues.3 Musculoskeletal pain is a typical symptom caused by MSD, and especially, low back and neck pain is the leading causative factor of disability worldwide.4 Globally, 1.71 billion people suffer from MSDs, which are also the leading cause of disability.5 Approximately one-third of the UK population has MSDs, such as arthritis and back pain, making MSD the third–largest burden of the National Health System’s expenditure.6 According to a recent study in Korea, where national health insurance is available, one in three Koreans visits healthcare providers for musculoskeletal pain and functional decline; MSD prevalence is also increasing among older patients.7 Rehabilitation is essential for patients with MSDs. In 2017, when the WHO launched the “Rehabilitation 2030 initiative”, everyone should be able to rehabilitate at all life cycle stages, especially for musculoskeletal health.8 In addition, pain control is a major concern in MSD care and rehabilitation programs. In the MSD rehabilitation program, the specific needs of each patient are considered. An exercise program designed to increase muscle strength, flexibility and mobility is crucial, and through such rehabilitation, the patient can become independent and lead a regular life. Active participation of both patients and their families during this process is essential.9 Recently, Austria introduced a secondary preventive program for patients with MSD, aiming to prevent rehospitalization. As part of the appraisal for this program, a large observational study was conducted, and the results indicated that physical inactivity is the factor that is most associated with the need for healthcare services.10
Using DHC for health improvement is cost-effective, safe, and measurable.11 In particular, rehabilitation for MSD, which requires physical activity (PA), may have great potential when combined with DHC based on the Internet, smartphone applications, augmented reality (AR), and virtual reality (VR). Currently, most smartphones and smartwatches already include accelerometer-based PA trackers, allowing easy access even for older adults unfamiliar with innovative technology.12 The development of sensors and wearable devices not only enhances the convenience of systematic health management but also helps healthcare providers access and manage the rehabilitation of patients with MSD in daily life outside hospitals or facilities. In addition, by making the VR and AR content more interactive and engaging, patients can become interested in rehabilitation.
DHC can offer a practical and flexible rehabilitation alternative for both patients and healthcare professionals. However, the effectiveness of DHC remains inadequately assessed; in particular, studies suggesting a relationship between MSD management and DHC are difficult to find.13 Hence, this systematic review and meta-analysis aimed to evaluate the effectiveness of musculoskeletal rehabilitation using a DHC system.
Materials and Methods
Search Strategy and Study Selection
We evaluated the effectiveness of musculoskeletal rehabilitation using a DHC system compared with that of conventional rehabilitation. DHC refers to the digital and mobile technologies used to support health system needs by promoting healthy behaviors, improving outcomes, and providing remote access to adequate care.11,14 We defined DHC as a healthcare intervention that utilizes internet-based technologies, telephone-supported technologies, interactive voice response, AR or VR, video conferencing, or mobile phone applications, in line with previous studies.15
Our systematic review and meta-analysis was conducted using PRISMA guidelines.16 We conducted literature searches on July 20, 2020, and updated it on October 28, 2022, using the following databases: PubMed, Ovid-Embase, Cochrane Library, and PEDro Physiotherapy Evidence Database. We used search terms modified to the characteristics of each database according to the PubMed terms. Queries were input using MeSH terms, Boolean conjunctions, and truncation searches (Supplementary Table 1). In addition, references included in the searched studies were reviewed and added as per the inclusion and exclusion criteria. EndNote, a widely used reference management tool,17,18 was used to increase efficiency and save time. We imported all the database references into EndNote and deduplicated the datasets by using EndNote’s duplicate identification feature.
After removing duplicates from the searched studies, the authors (SJ1, BL, EL, and JK) independently selected relevant studies for further analysis. We first selected the studies to be included by reviewing the title and abstract. We further evaluated these studies by checking the full text of the articles. In case of disagreement, all authors were consulted to resolve it and made a consensus. Inclusion/exclusion decisions were made according to the designated criteria.
The inclusion criteria were as follows:
- MSDs that require rehabilitation (eg MSDs involving chronic pain).
- Rehabilitation using DHC as a target intervention.
- Conventional rehabilitation as the control intervention.
- Reported pain and quality of life (QoL).
- Randomized controlled or non-randomized controlled studies.
- Full-text articles published in English.
The exclusion criteria were as follows:
- Animal experiments or preclinical studies.
- Target population for immune disorders.
- Non-original article (letters, comments, and conference abstract).
- Inability to secure full-text.
Data Extraction
Four authors (SJ1, BL, EL and JK) extracted the data from the selected studies by using the previously set extraction format. The extracted information was as follows:
- General characteristics of the study (author, publication year, study design, target country, target disease, healthcare setting, and inclusion/exclusion criteria);
- Characteristics of the participants (sample size, each group size, average age, proportion of women);
- Intervention information (intervention type, intervention method, intervention period and follow-up period);
- Outcomes of interest (pain, health-related QoL [HRQoL], and Western Ontario and McMaster Universities Arthritis [WOMAC] index as a disease-specific QoL)19–21 and measurement tools for the outcomes.
Risk of Bias Assessment
The authors mentioned above also evaluated the risk of bias (RoB) according to Cochrane’s risk of bias.22 Disparity was solved through discussion with all reviewers.
Statistical Analysis
The effects of pain and QoL were pooled in a meta-analysis. To standardize the results measured by different tools, we calculated standardized mean differences (SMD) and 95% confidence intervals (CIs) for each study. SMD expresses a difference in the mean outcome between groups in units of the pooled standard deviation in each study.23 Several studies reported post-intervention measurements only, others reported changes from baseline only, and others reported both. In the meta-analysis of Da Costa et al, SMD derived from post-intervention estimates did not differ from that derived from change data. Regarding availability for both measurements, we used post-intervention measurements for meta-analysis. The Cochrane Review Manager software (RevMan 5.3, Cochrane Collaboration, Oxford, UK) was used for the inverse variance method, according to Deeks and Higgins.24 This method assigns more weight to studies with a precise estimate (i.e. low variance) than those with high variance.25 A random-effects model assumes the distribution of true effects and considers the within-study and between-study variances when estimating pooled effects.25,26 We conducted a random-effects meta-analysis accounting for different aspects of variation among studies. In the meta-analysis, a reduction in pain and WOMAC index indicated a better outcome; therefore, the left side of the forest plot favored DHC rehabilitation. The right side also favored DHC rehabilitation because an increase in the score indicates a better outcome for HRQoL. SMD results were interpreted as having no effect (< 0.2), small effect (0.2–0.5), moderate effect (0.5–0.8), or large effect (> 0.8) based on the interpretation of Cohen’s d.27
Heterogeneity was evaluated by comparing the results between studies using a forest plot and I2 statistics to measure the proportion of variation. We determined heterogeneity if I2 ≥ 50%.28 To ensure the robustness of the meta-analysis, we assessed the potential presence of publication bias through the funnel plots of each outcome.
Results
A total of 1366, 762, 76, and 111 articles were assessed from PubMed, EMBASE, Cochrane and PEDro, respectively. Following a search update, additional 597, 484, 403, and 62 articles were assessed for each database, respectively. After deduplication, the titles and abstracts of 2112 articles and 1258 updated articles were checked, and based on the inclusion and exclusion criteria, 94 and 112 were selected, respectively. After reviewing their full text, we finally included 54 (23 records and 31 updated records) studies (Supplementary Figures 1–2).
General Characteristics
Table 1 presents the main characteristics of the 54 included studies, which had a total of 6240 participants.29–82 The sample size ranged from 26 to 461 participants with an average age range of 21.9–71.8 years, and female representation ranging from 33.3 to 100%. The measurement outcomes, such as pain, physical function, joint range of motion, self-efficacy, and QoL, and the measurement tools varied among studies. Physical function and pain were suggested as the primary outcomes (Supplementary Table 2). We found 1 study using video-based intervention,74, 1 using artificial intelligence-assisted program,48 and 2 using telerehabilitation,35,43 8 using web-based interventions,29,30,32,36,56,59,60,66 16 evaluating interventions used VR or AR,37,40–42,45,52,57,58,62,65,67,68,70,71,77,82 and 26 using a mobile application.31,33,34,38,39,44,46,47,49–51,53–55,61,63,64,69,72,73,75,76,78–81
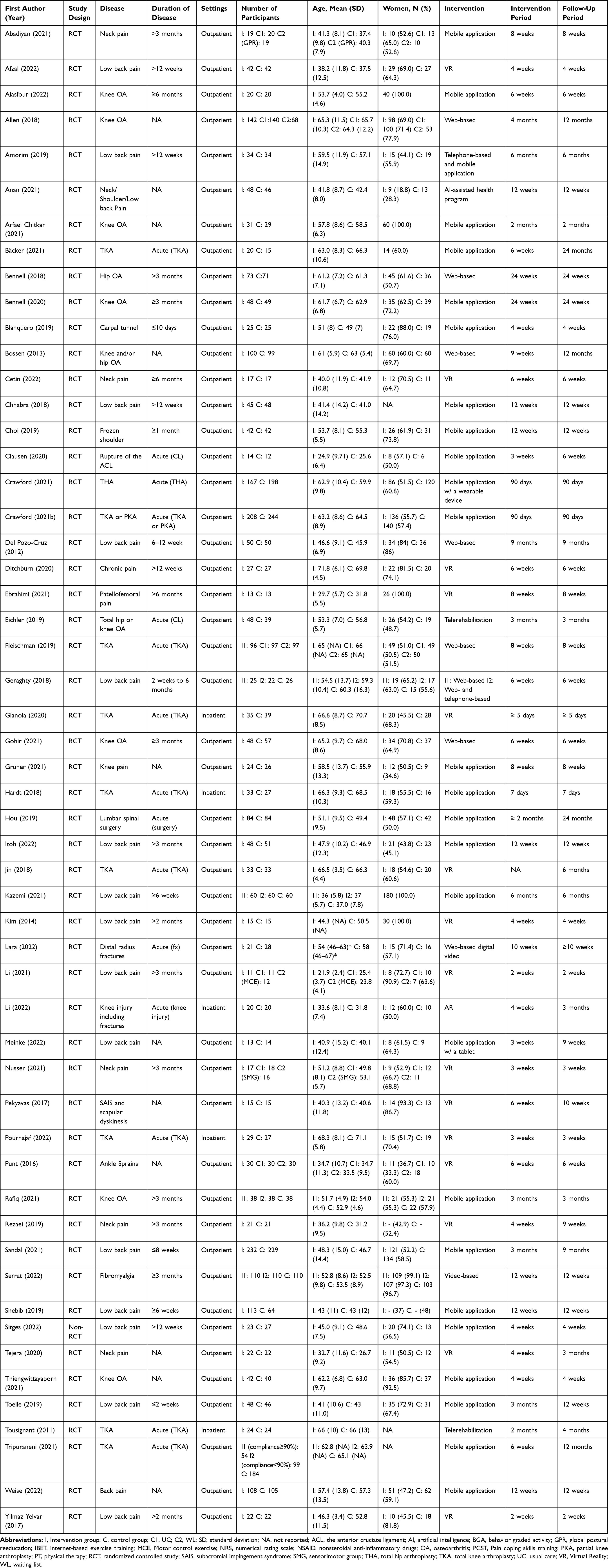 |
Table 1 Characteristics of the Included Studies |
Most of the included MSD studies (n = 22) were conducted on patients with affected knee or hip joints.29,30,32,34–38,40,43,46,49–51,54,55,60,67,71,72,78,80 Among these studies, 1 was conducted on patients undergoing hip arthroplasty,55 and 9 on patients undergoing knee arthroplasty.35–38,40,43,54,71,80 In addition to studies on carpal tunnel release31 and shoulder MSD,33,41 studies on patients with ankle sprains,42 fibromyalgia,74 distal radius fractures,66 and lumbar discs39 were included. All other studies were for patients with musculoskeletal pain (n = 25).53,56–59,61–65,68–70,73,75–77,79,81,82
In five studies evaluating the effectiveness of rehabilitation from hospitalization,37,38,43,67,71 the follow-up period ranges from less than 1 week to 4 months. In the other studies, it ranged from 2 weeks to 24 months to evaluate the effect of DHC intervention in an outpatient setting.29–36,39–42,44–66,68–70,72–82 Further detailed descriptions of the intervention included studies are shown in Table 1 and Supplementary Table 2.
Risk of Bias
For randomized controlled trials (RCTs) or non-RCTs, the RoB was evaluated using the Cochrane risk-of-bias tool (version 1) (Supplementary Figure 3).83 Except for one nonrandomized study,76 most studies generated random sequences by using computer-generated methods; therefore, in general, we evaluated the low risk of selection bias related to randomization. However, in one study, allocations were made in order of enrollment,79 thus, we rated it with a high selection bias risk. In studies with independent central randomization using web- or telephone-based methods, the RoB for allocation concealment was low.30–34,37–39,42–44,46,47,49–51,53–59,61,64,71,73,74,77,80,81 However, the included studies have a relatively tricky design for blinding of participants, because the rehabilitation method differs depending on the assigned group. Among the selected studies, only six were rated as having a low risk of performance bias.30,44,46,51,64,75 Six studies were marked as having a high risk of attrition bias,45,46,70,72,78,79 and the occurrence of this bias remained uncertain in some of the studies.41,44,62,65,67,68,82 Furthermore, some studies confirmed having unreported results; therefore, the risk of reporting bias was evaluated as high.34,43,52,69,76 The possibility of another bias was evaluated using limitations and the funding of each study, and eight studies were assessed as having a high RoB because the author was an intervention developer32 or received benefits related directly or indirectly to work.32,51,54,61–63,68,75,80,81 The results of the evaluation for the RoB were represented in the Supplementary Figure 3.
Effectiveness of DHC
Pain
We pooled the results of 45 studies evaluating pain (Figure 1).29–33,37–42,44–48,50–53,56,57,59–79,81,82 A visual analog scale31,33,34,37,39–42,44,45,52,58,62,64–68,71,73–77,82 was used in 25 studies, and a numerical rating scale in 16.32,34,38,46–48,51,53,59,60,63,69,70,73,79,81 Pooled results with substantial heterogeneity showed that rehabilitation using DHC significantly improved pain compared to the control (SMD: −0.55, 95% CI: −0.74, −0.36; I2 = 88%). We divided the studies into subgroups based on the duration of disease. Acute was defined as less than 1 month, and chronic was defined as 3 months or longer.84,85 In individuals with acute or subacute musculoskeletal pain, DHC rehabilitation resulted in more favorable outcomes compared to the control group (SMD: −0.44, 95% CI −0.69, −0.16 for acute pain; SMD: −0.93, 95% CI −1.40, −0.46 for subacute pain), whereas in individuals with chronic pain, the difference was marginally significant (SMD −0.42, 95% CI −0.83, −0.00). (Figure 1). Subgroup analysis was conducted based on follow-up duration, revealing that DHC intervention significantly reduced pain compared to conventional rehabilitation regardless of follow-up duration (Figure 2). The greatest reduction in pain was observed with a follow-up duration of less than one month (SMD: −0.75, 95% CI −1.32, −0.18). The effect of DHC on pain reduction decreased as follow-up duration increased. In addition, the funnel plot appears symmetrical, suggesting a low potential for publication bias (Supplementary Figure 4).
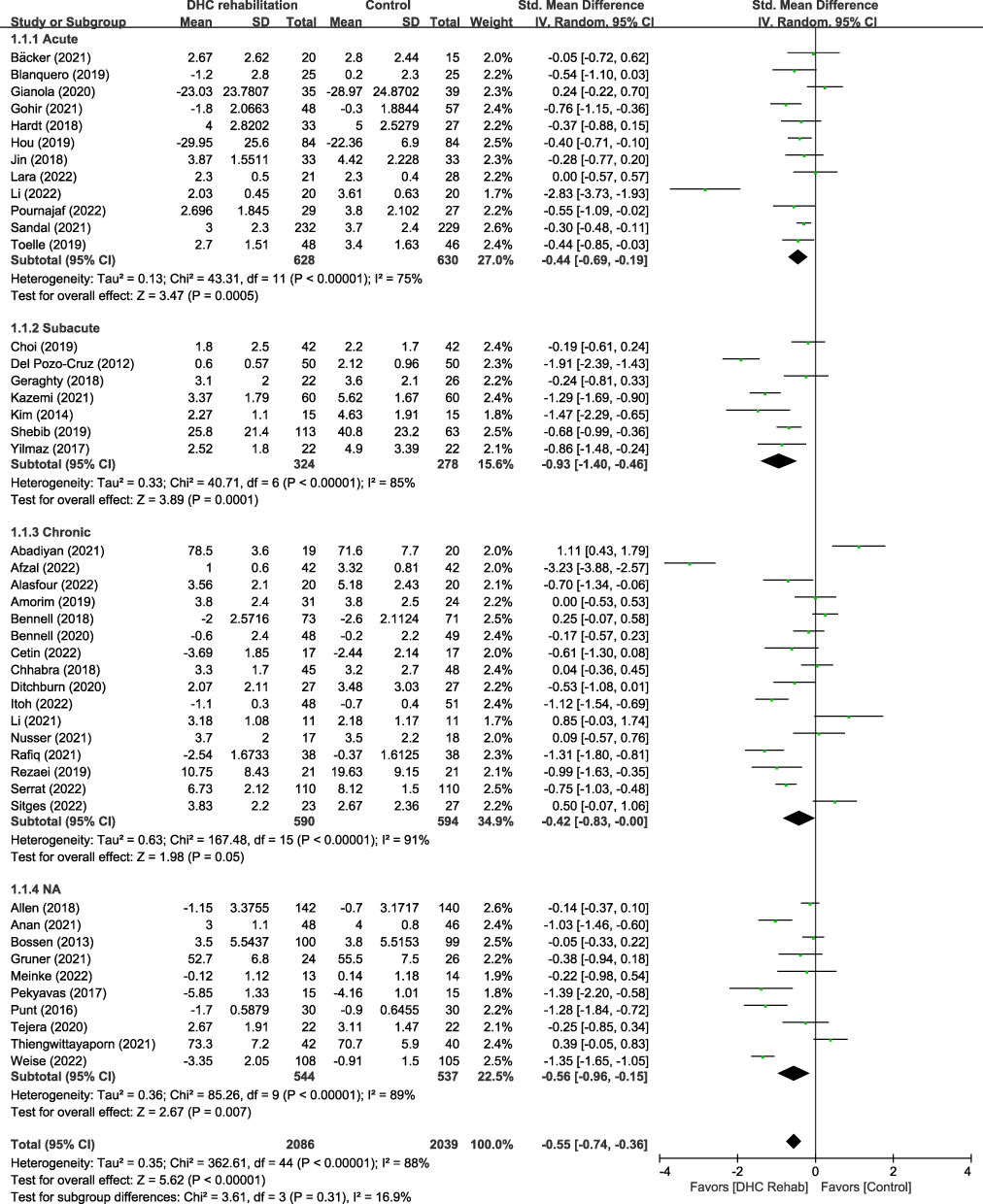 |
Figure 1 Forest plot of the standardized mean difference between DHC rehabilitation and control in pain. Abbreviations: IV, inverse variance; 95% CI, 95% confidence interval; Rehab, Rehabilitation. Note: Acute is defined as less than 1 month, and chronic is defined as 3 months or longer. |
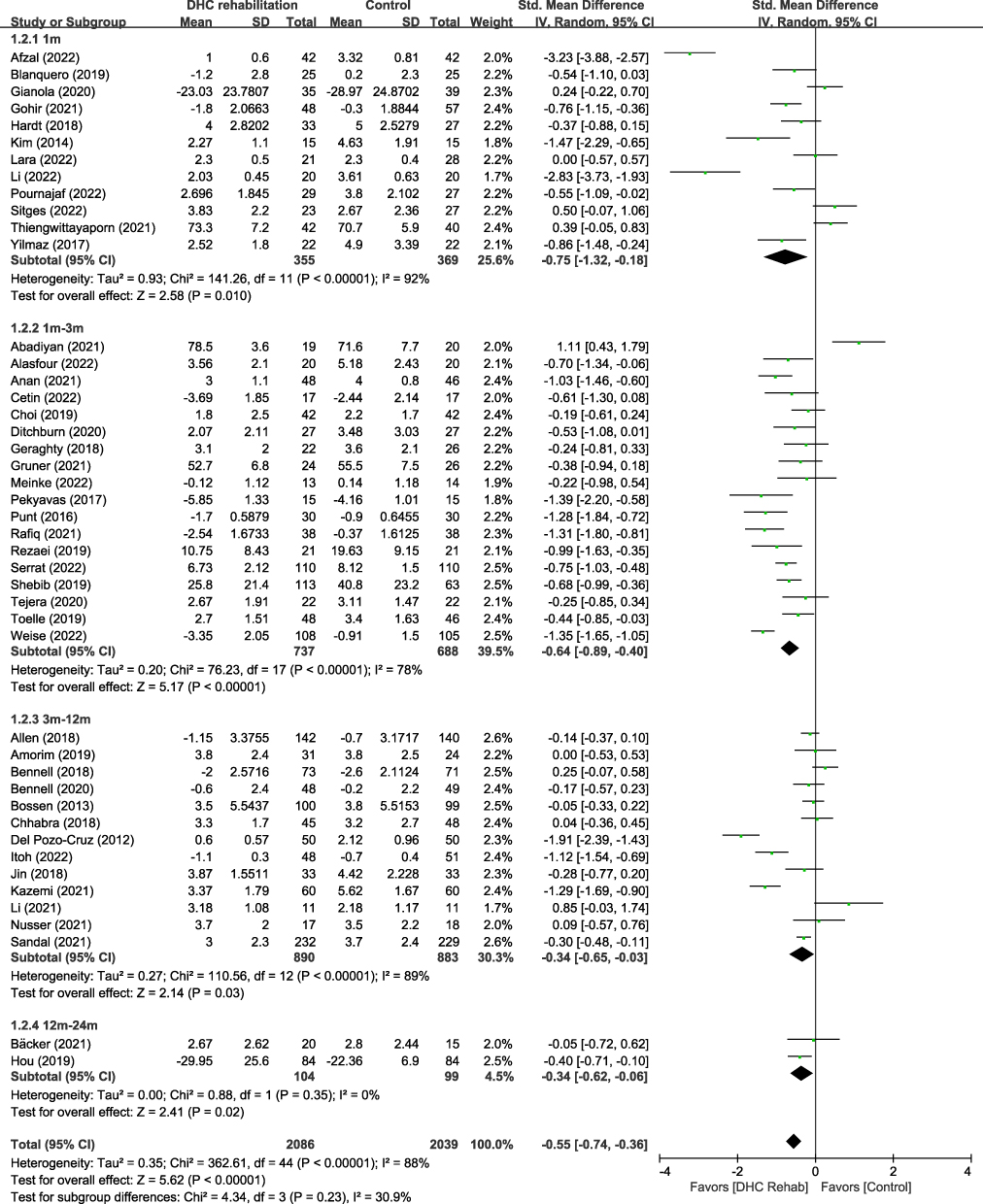 |
Figure 2 Forest plot of the standardized mean difference between DHC rehabilitation and control in pain according to the follow-up duration. Abbreviations: IV, inverse variance; 95% CI, 95% confidence interval; Rehab, Rehabilitation. |
QoL
We pooled the results of 18 studies assessing HRQoL30,32,35,37,39,44,50,51,54–56,63,69,73,78–80,82 (Figure 3). In each study, HRQoL was measured using various measurement tools, such as the Assessment of QoL instrument,30 subscales of Knee Injury and Osteoarthritis Outcome Score,50,51,78 Hip Injury OA Outcome Score,32 36-item Short-Form Health Survey,35,39,44 World Health Organization QoL,69 Veterans RAND 12-Item Health Survey,79 Nottingham Health Profile,82 and EuroQol 5-Dimension health questionnaire.37,39,54–56,63,73,80 In the meta-analysis, rehabilitation using DHC was found to significantly improve HRQoL compared to the control group (SMD: 0.66, 95% CI: 0.29, 1.03; I2 = 95%) (Figure 2 and Figure 3). The improvement in HRQoL was not significant in each group based on the duration of pain (SMD: 0.45, 95% CI −0.05, 0.94 for acute pain; SMD: 1.24, 95% CI −0.23, 2.72 for subacute pain; and SMD: 0.82, 95% CI −0.33, 1.98 for chronic pain, respectively). However, there was a significant improvement in HRQoL in studies where the duration of the pain could not be confirmed (SMD: 0.76, 95% CI 0.53, 1.00).
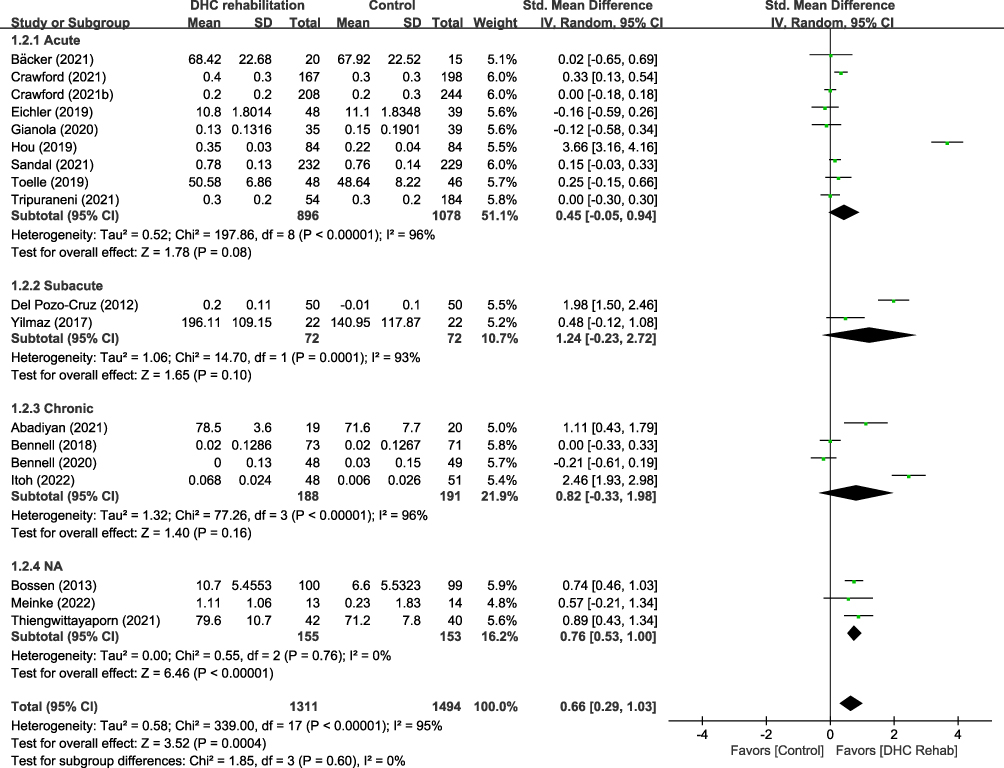 |
Figure 3 Forest plot of the standardized mean difference between DHC rehabilitation and control in the quality of life. Abbreviations: IV, inverse variance; 95% CI, 95% confidence interval; Rehab, Rehabilitation. |
We also estimated the pooled results for disease-specific QoL using the WOMAC global index (Figure 4).29,30,35,37,40,49,60 The meta-analysis included five out of seven studies that mentioned the WOMAC index as a measuring outcome.29,35,37,40,49 Two studies were excluded due to the lack of reported total WOMAC index results.30,60 The pooled results indicated that DHC rehabilitation had a marginally favorable effect on disease-specific QoL (SMD: −0.44, 95% CI: −0.87, −0.01; I2 = 81%). In addition, a subgroup meta-analysis of three studies focusing on WOMAC showed a significant improvement (SMD: −0.27; 95% CI −0.53, −0.01). The funnel plots appear asymmetrical, and studies with favorable control groups are relatively scarce; therefore, the risk of publication bias is high (Supplementary Figure 4).
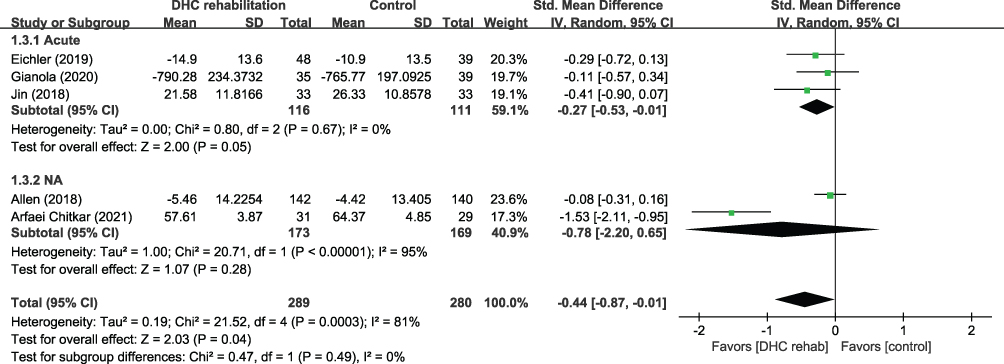 |
Figure 4 Forest plot of the standardized mean difference between DHC rehabilitation and control in the disease-specific quality of life (WOMAC index). Abbreviations: IV, inverse variance; 95% CI, 95% confidence interval; Rehab, Rehabilitation. |
Discussion
DHC has introduced new alternatives for the rehabilitation of patients with MSDs. In this systematic review and meta-analysis, we assessed the effects of rehabilitation based on digital technologies in patients with MSD. The meta-analyses of the studies were divided into 45, 16 and 5 studies evaluating pain, general HRQoL, and disease-specific QoL (measured with WOMAC), respectively. Our meta-analysis demonstrated that DHC rehabilitation was significantly more effective in reducing pain than conventional rehabilitation, with a moderated effect size (SMD: −0.55, 95% CI: −0.74, −0.36). This suggests that DHC-based interventions have potential for ameliorating MSD pain. The effectiveness of DHC rehabilitation in reducing pain remained significant in subgroups with acute or chronic pain (SMD: −0.44, 95% CI: −0.69, −0.19 for acute; SMD: −0.42, 95% CI: −0.83, −0.00 for chronic), indicating the potential use of DHC rehabilitation for pain management in individuals with MSDs in both short- and long-term pain conditions. Furthermore, although the effect size decreased somewhat with more extended follow-up periods, a significant effect was observed over the long term. In our meta-analysis of general HRQoL, significant improvement was more noted in the DHC group than in the control group (SMD: 0.66, 95% CI: 0.29, 1.03). However, subgroup analysis based on the duration of pain, did not reveal a significant improvement in HRQoL for the DHC group. This lack of significance may be attributed to the heterogeneity of studies included in the synthesis. As for the meta-analysis of disease-specific QoL measured using the WOMAC index, the improvement showed a marginal difference (SMD: −0.44, 95% CI: −0.87, −0.01).
The potential impact of DHC has already been widely studied. However, if limited to the rehabilitation of patients with MSD or pain via DHC, attempts to comprehend previous studies by adopting systematic reviews and meta-analyses have been relatively few. Nicholl et al86 systematically reviewed the effects of digital support interventions in the self-management of lower back pain but owing to high heterogeneity, they were unable to identify how DHC could be optimally used. Conversely, Cottrell et al13 succeeded in proving the possibility of real-time telerehabilitation in patients with MSD. They concluded that the target intervention group exhibited significantly better performance in terms of physical function and disability than the control group receiving usual care. Furthermore, Gumaa et al87 systematically reviewed controlled clinical trials for orthopedic rehabilitation through VR and performed a meta-analysis. They reported their findings regarding general MSD and region-specific MSD separately and confirmed that VR can effectively ameliorate chronic neck pain and shoulder impingement syndrome. Hewitt et al3 also conducted a systematic review of digital health interventions in patients with MSDs, demonstrating the clinical benefits of digital health interventions in reducing pain and alleviating dysfunction.
Most of the included studies reported pain as their outcome, and our pooled results found that rehabilitation using DHC is more likely to reduce pain than the usual rehabilitation. Pain is an easily perceived symptom in patients with MSD and the main reason why patients visit healthcare providers.88 Therefore, daily pain management is important as part of the care and rehabilitation programs for patient with MSD. Conventional rehabilitation services may have few hurdles because of physical constraints, such as the travel distance to medical institutions, shortage of healthcare providers, and a long waiting time. DHC has been demonstrated as a powerful and promising alternative to conventional rehabilitation. Using innovative technology, DHC can help reduce inequality in access to healthcare.
We specified QoL in the inclusion criteria because chronic pain can easily deteriorate the QoL of patients with MSD. The included studies used various instruments and scales to measure QoL. The synthesized result across the whole HRQoL outcomes showed statistical significance. In addition, in the subgroup analysis using the WOMAC index, DHC rehabilitation obtained favorable results. Considering the multidimensional and subjective aspects of QoL, positive possibilities are still noted in rehabilitation using DHC.
While previous systematic reviews reported only qualitative and comprehensive results. However, this study attempted to quantitatively analyze the evidence collected through a systematic review. In patients with MSD, as in other diseases, reduction in pain and promotion of QoL are important health outcomes. Clinical deterioration affects patients’ ability to work and perform daily activities. Pain affects the QoL, daily life, and social relationships of patients with MSD.89–91 The pain and HRQoL assessed in the present study are representative of patient-reported outcomes (PROs). As one of the key components of patient-centered medicine, the PROs should be identified by healthcare providers for continuous patient care. Carefully assessing patients’ experiences helps evaluate the effectiveness of treatment or disease progression.92,93 In many clinical trials, PROs were used not only as primary or secondary endpoints94–96 but also for measuring health outcomes for economic evaluation.97,98
This study has several limitations. First, only studies published in English were included. Second, presenting more consistent results was challenging because of the heterogeneity between studies. Although the effects of DHC rehabilitation on MSD and associated pain could be evaluated extensively, the characteristics of the disease itself may vary and may have contributed to significant heterogeneity. Third, further consideration is needed for different types and designs of DHC. Nevertheless, we made efforts to integrate the results of various studies by clearly defining the types of DHC included in the study. Despite our evaluation of the impact of DHC on PROs, further research is needed to comprehensively ascertain the potential benefits of DHC-based interventions for pain management and improvement in physical function.
Conclusion
DHC-based interventions may serve as a valuable alternative for rehabilitating patients with MSD and associated pain. This present study found significant pain reduction and improvement in QoL in response to DHC intervention. Nevertheless, further research is needed to elucidate the underlying mechanism by which DHC affects PROs, as this may vary depending on the type and design of the DHC intervention.
Abbreviations
AR, augmented reality; CI, confidence intervals; DHC, digital healthcare; HRQoL health-related quality of life; MSDs, musculoskeletal disorders; PA, physical activity; PROs, patient-reported outcomes; QoL, quality of life; RCTs, randomized controlled studies; RoB, risk of bias; SMD, standardized mean differences; VR, virtual reality; WHO, World Health Organization.
Data Sharing Statement
The datasets used in this study can be obtained from the corresponding authors upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was supported by the Korea Health Technology R&D Project through the Korea Health Industry Development Institute, funded by the Ministry of Health & Welfare, Republic of Korea (grant number: HI19C0781).
Disclosure
The authors have no conflicts of interest to declare.
References
1. World Health Organization. Digital Health. Geneva: World Health Organization; 2018.
2. Kim KI, Gollamudi SS, Steinhubl S. Digital technology to enable aging in place. Exp Gerontol. 2017;88:25–31. doi:10.1016/j.exger.2016.11.013
3. Hewitt S, Sephton R, Yeowell G. The effectiveness of digital health interventions in the management of musculoskeletal conditions: systematic literature review. J Med Internet Res. 2020;22(6):e15617. doi:10.2196/15617
4. Vos T, Abajobir AA, Abate KH, et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: a systematic analysis for the Global Burden of Disease Study 2016. Lancet. 2017;390(10100):1211–1259.
5. World Health Organization. Musculoskeletal conditions World Health Organization; 2022. Available from: https://www.who.int/news-room/fact-sheets/detail/musculoskeletal-conditions.
6. Versus Arthritis. Arthritis and other musculoskeletal conditions in numbers. The State of Musculoskeletal Health 2021; 2021. Available from: https://www.versusarthritis.org/media/24653/state-of-msk-health2-2021.pdf.
7. Health Insurance Review and Assessment Service. One out of three Korean people are treated for musculoskeletal disorders; 2020. Available from: http://www.hira.or.kr/bbsDummy.do;INTERSESSIONID=KbmMZMUEzDPsVceyHOThoVmeT5yb6eRf1QYBXtOxPkiSYfwgTdRH!1461541086!69048830?pgmid=HIRAA020041000100&brdScnBltNo=4&brdBltNo=10167#none.
8. World Health Orginization. Rehabilitation 2030 Initiative. World Health Organization; 2022. Available from: https://www.who.int/initiatives/rehabilitation-2030.
9. Department of Rehabilitation and Regenerative Medicine CU. Musculoskeletal rehabilitation. Columbia University Irving Medical Center; 2022. Available from: https://www.cuimc.columbia.edu/rehab/staywell/musculoskeletal-rehabilitation.
10. Grote V, Bottcher E, Unger A, Hofmann P, Moser M, Fischer MJ. Observational study of an inpatient program for musculoskeletal disorders: the effects of gender and physical activity. Medicine. 2021;100(43):e27594. doi:10.1097/MD.0000000000027594
11. Murray E, Hekler EB, Andersson G, et al. Evaluating digital health interventions: key questions and approaches. Am J Prev Med. 2016;51(5):843–851. doi:10.1016/j.amepre.2016.06.008
12. Negrini F, de Sire A, Lazzarini SG, et al. Reliability of activity monitors for physical activity assessment in patients with musculoskeletal disorders: a systematic review. J Back Musculoskelet Rehabil. 2021;34(6):915–923. doi:10.3233/BMR-200348
13. Cottrell MA, Galea OA, O’Leary SP, Hill AJ, Russell TG. Real-time telerehabilitation for the treatment of musculoskeletal conditions is effective and comparable to standard practice: a systematic review and meta-analysis. Clin Rehabil. 2017;31(5):625–638. doi:10.1177/0269215516645148
14. World Health Organization. Classification of digital health interventions v1.0: a shared language to describe the uses of digital technology for health; 2018. Available from: https://apps.who.int/iris/handle/10665/260480.
15. Slattery BW, Haugh S, O’Connor L, et al. An evaluation of the effectiveness of the modalities used to deliver electronic health interventions for chronic pain: systematic review with network meta-analysis. J Med Internet Res. 2019;21(7):e11086. doi:10.2196/11086
16. Moher D, Liberati A, Tetzlaff J, Altman DG; PRISMA Group* t. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. Ann Intern Med. 2009;151(4):264–269. doi:10.7326/0003-4819-151-4-200908180-00135
17. Emanuel J. Users and citation management tools: use and support. Ref Serv Rev. 2013;41(4):639–659. doi:10.1108/RSR-02-2013-0007
18. The EndNote Team. EndNote 20. Clarivate; 2013.
19. Rampazo-Lacativa MK, Santos AA, Coimbra AM, D’Elboux MJ. WOMAC and SF-36: instruments for evaluating the health-related quality of life of elderly people with total Hip arthroplasty. A descriptive study. Sao Paulo Med J. 2015;133(4):290–297. doi:10.1590/1516-3180.2014.8381508
20. Tangtrakulwanich B, Wiwatwongwana S, Chongsuvivatwong V, Geater AF. Comparison of validity, and responsiveness between general and disease-specific quality of life instruments (Thai version) in knee osteoarthritis. J Med Assoc Thai. 2006;89(9):1454–1459.
21. Fang WH, Huang GS, Chang HF, et al. Gender differences between WOMAC index scores, health-related quality of life and physical performance in an elderly Taiwanese population with knee osteoarthritis. BMJ Open. 2015;5(9):e008542. doi:10.1136/bmjopen-2015-008542
22. Higgins JP, Altman DG, Gotzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi:10.1136/bmj.d5928
23. Higgins JPTTJ, Chandler J, Cumpston M, Li T, Page MJ, Welch VA. Chapter 6: choosing effect measures and computing estimates of effect. In: Higgins JPTLT, Deeks JJ, editors. Cochrane Handbook for Systematic Reviews of Interventions Version 63 (Updated February 2022). Cochrane; 2022.
24. Deeks JJ, Higgins JP. Statistical algorithms in review manager 5. Statistical Methods Group of the Cochrane Collaboration. Cochrane Collab. 2010;1(11):1–11.
25. Borenstein M, Hedges LV, Higgins JP, Rothstein HR. A basic introduction to fixed‐effect and random‐effects models for meta‐analysis. Res Synth Methods. 2010;1(2):97–111. doi:10.1002/jrsm.12
26. Crocetti E. Systematic reviews with meta-analysis: why, when, and how? Emerging Adulthood. 2016;4(1):3–18. doi:10.1177/2167696815617076
27. Cohen J. Statistical Power Analysis for the Behavioral Sciences. Routledge; 2013.
28. Higgins JP, Thomas J, Chandler J, et al. Cochrane Handbook for Systematic Reviews of Interventions. John Wiley & Sons; 2019.
29. Allen KD, Arbeeva L, Callahan LF, et al. Physical therapy vs internet-based exercise training for patients with knee osteoarthritis: results of a randomized controlled trial. Osteoarthritis Cartilage. 2018;26(3):383–396. doi:10.1016/j.joca.2017.12.008
30. Bennell KL, Nelligan RK, Rini C, et al. Effects of internet-based pain coping skills training before home exercise for individuals with Hip osteoarthritis (HOPE trial): a randomised controlled trial. Pain. 2018;159(9):1833–1842. doi:10.1097/j.pain.0000000000001281
31. Blanquero J, Cortes-Vega MD, Garcia-Frasquet MA, Sanchez-Laulhe PR, Nieto Diaz de Los Bernardos MI, Suero-Pineda A. Exercises using a touchscreen tablet application improved functional ability more than an exercise program prescribed on paper in people after surgical carpal tunnel release: a randomised trial. J Physiother. 2019;65(2):81–87. doi:10.1016/j.jphys.2019.02.008
32. Bossen D, Veenhof C, Van Beek KE, Spreeuwenberg PM, Dekker J, De Bakker DH. Effectiveness of a web-based physical activity intervention in patients with knee and/or Hip osteoarthritis: randomized controlled trial. J Med Internet Res. 2013;15(11):e257. doi:10.2196/jmir.2662
33. Choi Y, Nam J, Yang D, Jung W, Lee H-R, Kim SH. Effect of smartphone application-supported self-rehabilitation for frozen shoulder: a prospective randomized control study. Clin Rehabil. 2018;33(4):653–660. doi:10.1177/0269215518818866
34. Clausen JD, Nahen N, Horstmann H, et al. Improving maximal strength in the initial postoperative phase after anterior cruciate ligament reconstruction surgery: randomized controlled trial of an app-based serious gaming approach. JMIR Serious Games. 2020;8(1):e14282. doi:10.2196/14282
35. Eichler S, Salzwedel A, Rabe S, et al. The effectiveness of telerehabilitation as a supplement to rehabilitation in patients after total knee or hip replacement: randomized controlled trial. JMIR Rehabil Assist Technol. 2019;6(2):e14236. doi:10.2196/14236
36. Fleischman AN, Crizer MP, Tarabichi M, et al. 2018 John N. Insall Award: recovery of knee flexion with unsupervised home exercise is not inferior to outpatient physical therapy after TKA: a randomized trial. Clin Orthop Relat Res. 2019;477(1):60–69. doi:10.1097/CORR.0000000000000561
37. Gianola S, Stucovitz E, Castellini G, et al. Effects of early virtual reality-based rehabilitation in patients with total knee arthroplasty: a randomized controlled trial. Medicine. 2020;99(7):e19136. doi:10.1097/MD.0000000000019136
38. Hardt S, Schulz MRG, Pfitzner T, et al. Improved early outcome after TKA through an app-based active muscle training programme-a randomized-controlled trial. Knee Surg Sports Traumatol Arthrosc. 2018;26(11):3429–3437. doi:10.1007/s00167-018-4918-2
39. Hou J, Yang R, Yang Y, et al. The effectiveness and safety of utilizing mobile phone-based programs for rehabilitation after lumbar spinal surgery: multicenter, prospective randomized controlled trial. JMIR Mhealth Uhealth. 2019;7(2):e10201. doi:10.2196/10201
40. Jin C, Feng Y, Ni Y, Shan Z. Virtual reality intervention in postoperative rehabilitation after total knee arthroplasty: a prospective and randomized controlled clinical trial. Int J Clin Exp Med. 2018;11(6):6119–6124.
41. Pekyavas NO, Ergun N. Comparison of virtual reality exergaming and home exercise programs in patients with subacromial impingement syndrome and scapular dyskinesis: short term effect. Acta Orthop Traumatol Turc. 2017;51(3):238–242. doi:10.1016/j.aott.2017.03.008
42. Punt IM, Ziltener JL, Monnin D, Allet L. Wii Fit exercise therapy for the rehabilitation of ankle sprains: its effect compared with physical therapy or no functional exercises at all. Scand J Med Sci Sports. 2016;26(7):816–823. doi:10.1111/sms.12509
43. Tousignant M, Moffet H, Boissy P, Corriveau H, Cabana F, Marquis F. A randomized controlled trial of home telerehabilitation for post-knee arthroplasty. J Telemed Telecare. 2011;17(4):195–198. doi:10.1258/jtt.2010.100602
44. Abadiyan F, Hadadnezhad M, Khosrokiani Z, Letafatkar A, Akhshik H. Adding a smartphone app to global postural re-education to improve neck pain, posture, quality of life, and endurance in people with nonspecific neck pain: a randomized controlled trial. Trials. 2021;22(1):274. doi:10.1186/s13063-021-05214-8
45. Afzal MW, Ahmad A, Mohseni Bandpei MA, Gilani SA, Hanif A, Waqas MS. Effects of virtual reality exercises and routine physical therapy on pain intensity and functional disability in patients with chronic low back pain. J Pak Med Assoc. 2022;72(3):413–417. doi:10.47391/JPMA.3424
46. Alasfour M, Almarwani M. The effect of innovative smartphone application on adherence to a home-based exercise programs for female older adults with knee osteoarthritis in Saudi Arabia: a randomized controlled trial. Disabil Rehabil. 2022;44(11):2420–2427. doi:10.1080/09638288.2020.1836268
47. Amorim AB, Pappas E, Simic M, et al. Integrating Mobile-health, health coaching, and physical activity to reduce the burden of chronic low back pain trial (IMPACT): a pilot randomised controlled trial. BMC Musculoskelet Disord. 2019;20(1):71. doi:10.1186/s12891-019-2454-y
48. Anan T, Kajiki S, Oka H, et al. Effects of an artificial intelligence-assisted health program on workers with neck/shoulder pain/stiffness and low back pain: randomized controlled trial. JMIR Mhealth Uhealth. 2021;9(9):e27535. doi:10.2196/27535
49. Arfaei Chitkar SS, Mohaddes Hakkak HR, Saadati H, Hosseini SH, Jafari Y, Ganji R. The effect of mobile-app-based instruction on the physical function of female patients with knee osteoarthritis: a parallel randomized controlled trial. BMC Womens Health. 2021;21(1):333. doi:10.1186/s12905-021-01451-w
50. Backer HC, Wu CH, Schulz MRG, Weber-Spickschen TS, Perka C, Hardt S. App-based rehabilitation program after total knee arthroplasty: a randomized controlled trial. Arch Orthop Trauma Surg. 2021;141(9):1575–1582. doi:10.1007/s00402-021-03789-0
51. Bennell K, Nelligan RK, Schwartz S, et al. Behavior change text messages for home exercise adherence in knee osteoarthritis: randomized trial. J Med Internet Res. 2020;22(9):e21749. doi:10.2196/21749
52. Cetin H, Kose N, Oge HK. Virtual reality and motor control exercises to treat chronic neck pain: a randomized controlled trial. Musculoskelet Sci Pract. 2022;62:102636. doi:10.1016/j.msksp.2022.102636
53. Chhabra HS, Sharma S, Verma S. Smartphone app in self-management of chronic low back pain: a randomized controlled trial. Eur Spine J. 2018;27(11):2862–2874. doi:10.1007/s00586-018-5788-5
54. Crawford DA, Duwelius PJ, Sneller MA, et al. 2021 Mark Coventry Award: use of a smartphone-based care platform after primary partial and total knee arthroplasty: a prospective randomized controlled trial. Bone Joint J. 2021;103-B(6 Supple A):3–12. doi:10.1302/0301-620X.103B6.BJJ-2020-2352.R1
55. Crawford DA, Lombardi AV, Berend KR, et al. Early outcomes of primary total Hip arthroplasty with use of a smartphone-based care platform: a prospective randomized controlled trial. Bone Joint J. 2021;103-B(7 Supple B):91–97. doi:10.1302/0301-620X.103B7.BJJ-2020-2402.R1
56. Del Pozo-Cruz B, Adsuar JC, Parraca J, Del Pozo-Cruz J, Moreno A, Gusi N. A web-based intervention to improve and prevent low back pain among office workers: a randomized controlled trial. J Orthop Sports Phys Ther. 2012;42(10):831–841. doi:10.2519/jospt.2012.3980
57. Ditchburn JL, van Schaik P, Dixon J, MacSween A, Martin D. The effects of exergaming on pain, postural control, technology acceptance and flow experience in older people with chronic musculoskeletal pain: a randomised controlled trial. BMC Sports Sci Med Rehabil. 2020;12:63. doi:10.1186/s13102-020-00211-x
58. Ebrahimi N, Rojhani-Shirazi Z, Yoosefinejad AK, Nami M. The effects of virtual reality training on clinical indices and brain mapping of women with patellofemoral pain: a randomized clinical trial. BMC Musculoskelet Disord. 2021;22(1):900. doi:10.1186/s12891-021-04785-6
59. Geraghty AWA, Stanford R, Stuart B, et al. Using an internet intervention to support self-management of low back pain in primary care: findings from a randomised controlled feasibility trial (SupportBack). BMJ Open. 2018;8(3):e016768. doi:10.1136/bmjopen-2017-016768
60. Gohir SA, Eek F, Kelly A, Abhishek A, Valdes AM. Effectiveness of Internet-Based Exercises Aimed at Treating Knee Osteoarthritis: the iBEAT-OA Randomized Clinical Trial. JAMA Netw Open. 2021;4(2):e210012. doi:10.1001/jamanetworkopen.2021.0012
61. Gruner MP, Hogaboom N, Hasley I, et al. Prospective, single-blind, randomized controlled trial to evaluate the effectiveness of a digital exercise therapy application compared with conventional physical therapy for the treatment of nonoperative knee conditions. Arch Rehabil Res Clin Transl. 2021;3(4):100151. doi:10.1016/j.arrct.2021.100151
62. Rezaei I, Razeghi M, Ebrahimi S, Kayedi S, Novel Virtual A. Reality technique (Cervigame(R)) compared to conventional proprioceptive training to treat neck pain: a randomized controlled trial. J Biomed Phys Eng. 2019;9(3):355–366. doi:10.31661/jbpe.v0i0.556
63. Itoh N, Mishima H, Yoshida Y, Yoshida M, Oka H, Matsudaira K. Evaluation of the effect of patient education and strengthening exercise therapy using a mobile messaging app on work productivity in Japanese patients with chronic low back pain: open-label, randomized, parallel-group trial. JMIR Mhealth Uhealth. 2022;10(5):e35867. doi:10.2196/35867
64. Kazemi SS, Tavafian SS, Hiller CE, Hidarnia A, Montazeri A. The effectiveness of social media and in-person interventions for low back pain conditions in nursing personnel (SMILE). Nurs Open. 2021;8(3):1220–1231. doi:10.1002/nop2.738
65. Kim SS, Min WK, Kim JH, Lee BH. The effects of VR-based wii fit yoga on physical function in middle-aged female LBP patients. J Phys Ther Sci. 2014;26(4):549–552. doi:10.1589/jpts.26.549
66. Lara TR, Kagan RP, Hiratzka SL, Thompson AR, Nazir OF, Mirarchi AJ. Traditional versus digital media-based hand therapy after distal radius fracture. J Hand Surg Am. 2022;47(3):291e1–291 e8. doi:10.1016/j.jhsa.2021.06.018
67. Li L. Effect of remote control augmented reality multimedia technology for postoperative rehabilitation of knee joint injury. Comput Math Methods Med. 2022;2022:9320063. doi:10.1155/2022/9320063
68. Li Z, Yu Q, Luo H, et al. The effect of virtual reality training on anticipatory postural adjustments in patients with chronic nonspecific low back pain: a preliminary study. Neural Plast. 2021;2021:9975862. doi:10.1155/2021/9975862
69. Meinke A, Peters R, Knols RH, Swanenburg J, Karlen W. Feedback on trunk movements from an electronic game to improve postural balance in people with nonspecific low back pain: pilot randomized controlled trial. JMIR Serious Games. 2022;10(2):e31685. doi:10.2196/31685
70. Nusser M, Knapp S, Kramer M, Krischak G. Effects of virtual reality-based neck-specific sensorimotor training in patients with chronic neck pain: a randomized controlled pilot trial. J Rehabil Med. 2021;53(2):jrm00151. doi:10.2340/16501977-2786
71. Pournajaf S, Goffredo M, Pellicciari L, et al. Effect of balance training using virtual reality-based serious games in individuals with total knee replacement: a randomized controlled trial. Ann Phys Rehabil Med. 2022;65(6):101609. doi:10.1016/j.rehab.2021.101609
72. Rafiq MT, Abdul Hamid MS, Hafiz E. The effect of rehabilitation protocol using mobile health in overweight and obese patients with knee osteoarthritis: a clinical trial. Adv Rheumatol. 2021;61(1):63. doi:10.1186/s42358-021-00221-4
73. Sandal LF, Bach K, Overas CK, et al. Effectiveness of app-delivered, tailored self-management support for adults with lower back pain-related disability: a selfBACK randomized clinical trial. JAMA Intern Med. 2021;181(10):1288–1296. doi:10.1001/jamainternmed.2021.4097
74. Serrat M, Albajes K, Navarrete J, et al. Effectiveness of two video-based multicomponent treatments for fibromyalgia: the added value of cognitive restructuring and mindfulness in a three-arm randomised controlled trial. Behav Res Ther. 2022;158:104188. doi:10.1016/j.brat.2022.104188
75. Shebib R, Bailey JF, Smittenaar P, Perez DA, Mecklenburg G, Hunter S. Randomized controlled trial of a 12-week digital care program in improving low back pain. NPJ Digit Med. 2019;2:1. doi:10.1038/s41746-018-0076-7
76. Sitges C, Terrasa JL, Garcia-Dopico N, et al. An educational and exercise mobile phone-based intervention to elicit electrophysiological changes and to improve psychological functioning in adults with nonspecific chronic low back pain (BackFit App): nonrandomized clinical trial. JMIR Mhealth Uhealth. 2022;10(3):e29171. doi:10.2196/29171
77. Tejera DM, Beltran-Alacreu H, Cano-de-la-Cuerda R, et al. Effects of virtual reality versus exercise on pain, functional, somatosensory and psychosocial outcomes in patients with non-specific chronic neck pain: a randomized clinical trial. Int J Environ Res Public Health. 2020;17(16):5950. doi:10.3390/ijerph17165950
78. Thiengwittayaporn S, Wattanapreechanon P, Sakon P, et al. Development of a mobile application to improve exercise accuracy and quality of life in knee osteoarthritis patients: a randomized controlled trial. Arch Orthop Trauma Surg. 2023;143(2):729–738. doi:10.1007/s00402-021-04149-8
79. Toelle TR, Utpadel-Fischler DA, Haas KK, Priebe JA. App-based multidisciplinary back pain treatment versus combined physiotherapy plus online education: a randomized controlled trial. NPJ Digit Med. 2019;2:34. doi:10.1038/s41746-019-0109-x
80. Tripuraneni KR, Foran JRH, Munson NR, Racca NE, Carothers JT, Smartwatch Paired A. With a mobile application provides postoperative self-directed rehabilitation without compromising total knee arthroplasty outcomes: a randomized controlled trial. J Arthroplasty. 2021;36(12):3888–3893. doi:10.1016/j.arth.2021.08.007
81. Weise H, Zenner B, Schmiedchen B, et al. The effect of an app-based home exercise program on self-reported pain intensity in unspecific and degenerative back pain: pragmatic open-label randomized controlled trial. J Med Internet Res. 2022;24(10):e41899. doi:10.2196/41899
82. Yilmaz Yelvar GD, Cirak Y, Dalkilinc M, Parlak Demir Y, Guner Z, Boydak A. Is physiotherapy integrated virtual walking effective on pain, function, and kinesiophobia in patients with non-specific low-back pain? Randomised controlled trial. Eur Spine J. 2017;26(2):538–545. doi:10.1007/s00586-016-4892-7
83. Higgins JPTTJ, Chandler J, Cumpston M, et al. Cochrane Handbook for Systematic Reviews of Interventions Version 6.2 (Updated February 2021). Cochrane; 2021.
84. Meucci RD, Fassa AG, Faria NMX. Prevalence of chronic low back pain: systematic review. Rev Saude Publica. 2015;49. doi:10.1590/S0034-8910.2015049005874
85. Qaseem A, Wilt TJ, McLean RM, Forciea MA; Physicians* CGCotACo. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2017;166(7):514–530. doi:10.7326/M16-2367
86. Nicholl BI, Sandal LF, Stochkendahl MJ, et al. Digital support interventions for the self-management of low back pain: a systematic review. J Med Internet Res. 2017;19(5):e179. doi:10.2196/jmir.7290
87. Gumaa M, Rehan Youssef A. Is virtual reality effective in orthopedic rehabilitation? A systematic review and meta-analysis. Phys Ther. 2019;99(10):1304–1325. doi:10.1093/ptj/pzz093
88. Varsi C, Ledel Solem IK, Eide H, et al. Health care providers’ experiences of pain management and attitudes towards digitally supported self-management interventions for chronic pain: a qualitative study. BMC Health Serv Res. 2021;21(1):275. doi:10.1186/s12913-021-06278-7
89. Tuzun EH. Quality of life in chronic musculoskeletal pain. Best Pract Res Clin Rheumatol. 2007;21(3):567–579. doi:10.1016/j.berh.2007.03.001
90. de Carvalho MP, Schmidt LG, Soares MC. Musculoskeletal disorders and their influence on the quality of life of the dockworker: a cross-sectional study. Work. 2016;53(4):805–812. doi:10.3233/WOR-162249
91. Manos Savvakis NK. Quality of life and chronic pain: coping practises and experiences of patients with musculoskeletal diseases. Int J Caring Sci. 2019;12(3):1423–1429.
92. Fung CH, Hays RD. Prospects and challenges in using patient-reported outcomes in clinical practice. Qual Life Res. 2008;17(10):1297–1302. doi:10.1007/s11136-008-9379-5
93. Doward LC, McKenna SP. Defining patient-reported outcomes. Value Health. 2004;7(Suppl 1):S4–S8. doi:10.1111/j.1524-4733.2004.7s102.x
94. Mercieca-Bebber R, King MT, Calvert MJ, Stockler MR, Friedlander M. The importance of patient-reported outcomes in clinical trials and strategies for future optimization. Patient Relat Outcome Meas. 2018;9:353–367. doi:10.2147/PROM.S156279
95. Anker SD, Agewall S, Borggrefe M, et al. The importance of patient-reported outcomes: a call for their comprehensive integration in cardiovascular clinical trials. Eur Heart J. 2014;35(30):2001–2009. doi:10.1093/eurheartj/ehu205
96. Leidy NK, Vernon M. Perspectives on Patient-Reported Outcomes. Pharmaco Econom. 2008;26(5):363–370. doi:10.2165/00019053-200826050-00002
97. Schilling C, Dowsey MM, Clarke PM, Choong PF. Using patient-reported outcomes for economic evaluation: getting the timing right. Value Health. 2016;19(8):945–950. doi:10.1016/j.jval.2016.05.014
98. Gater A, Kitchen H, Heron L, et al. Development of a conceptual model evaluating the humanistic and economic burden of Crohn’s disease: implications for patient-reported outcomes measurement and economic evaluation. Expert Rev Pharmacoecon Outcomes Res. 2015;15(4):643–656. doi:10.1586/14737167.2015.1045883
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.