Back to Journals » Journal of Pain Research » Volume 16
The Effect of Virtual Reality Glasses Applied During the Episiotomy On Pain and Satisfaction: A Single Blind Randomized Controlled Study
Received 11 April 2023
Accepted for publication 17 June 2023
Published 29 June 2023 Volume 2023:16 Pages 2227—2239
DOI https://doi.org/10.2147/JPR.S412883
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Ellen Soffin
Merva Orhan,1 Aysel Bülez2
1Kahramanmaras Necip Fazil City Hospital, Obstetric Clinic, Kahramanmaraş, Turkey; 2Kahramanmaras Sütcü Imam University, Faculty of Health Sciences, Midwifery Department, Kahramanmaraş, Turkey
Correspondence: Aysel Bülez, Midwifery Department, Kahramanmaras Sütcü Imam University, Faculty of Health Sciences, Bahcelievler Campus, Emniyet Street, Kahramanmaras, 46100, Turkey, Tel +90 344 300 26 01/ 4737, Email [email protected]
Objective: The research was conducted as a randomized controlled study to determine the effect of virtual reality glasses on the mother’s pain and satisfaction during episiotomy.
Methods: The sample consisted of 50 pregnant women determined by randomization among primiparous pregnant women. Data were collected with the Mother Information Form and Visual Analog Scales Pain and Satisfaction Evaluation forms. 5 mL of lidocaine was administered to mothers in the intervention and control groups during episiotomy repair. Only the mothers in the intervention group watched a video with virtual reality glasses for an average of 10 minutes during the episiotomy procedure. SPSS 22.0 was used in the analysis.
Results: In the comparison between the groups, it was found that the mean pain score measured during episiotomy inner and episiotomy skin suturing was statistically significantly lower in the intervention group than in the control group; there was no significant difference between the intervention and control groups in the mean pain scores measured before and after episiotomy repair. It was determined that the mean satisfaction score of the intervention group was higher than that of the control group.
Conclusion: Virtual reality glasses reduced pain during episiotomy and increased satisfaction. According to the results, it is recommended to be used by midwives because it is an easily applicable non-pharmacological method and increases the mother’s birth satisfaction.
Keywords: birth satisfaction, episiotomy, labor pain, obstetrics, virtual reality
Introduction
Birth is more than a mechanical process in which the fetus is transferred from the womb to the outside world. Listening to women’s birth experiences, understanding what constitutes a psychologically safe birth environment for them and learning their expectations from them is very important for a positive birth experience.1
During vaginal delivery, usually when the baby’s head is born, it can cause trauma to the perineum and surrounding tissues, and sometimes lacerations can reach the size of the breech. Lacerations are surgically repaired, but take time to heal. Health professionals have recommended a surgical incision in the perineum with scissors or a scalpel to prevent these uncontrolled serious lacerations and facilitate delivery. Known as an episiotomy, this intervention has been used as a policy of routine care during deliveries in some countries.2–8 Lacerations and episiotomy are serious procedures that require surgical sutures.2–4 While episiotomy affects the body image and sexual life of the woman, it also affects the comfort of the mother with perineal pain in the postpartum period.5 Episiotomy is a very critical and life-saving practice in cases where there are necessary indications, but since it is a surgical intervention, it is recommended not to be applied routinely and to give priority to natural birth methods. It is very difficult to provide comfort and satisfaction, which is a basic need at birth, and there are not enough studies on this subject. It is very difficult to provide comfort and satisfaction, which is a basic need at birth, and there are not enough studies on this subject.6 Midwives accompanying pregnant women at all stages of labor use non-pharmacological methods and various techniques to help reduce genital tract trauma rates after vaginal delivery.7,8
The factor that increases the satisfaction in the labor process is related to the comfort provided to the pregnant woman.9 According to the studies, it was stated that less analgesia can be used when the effectiveness of relaxing applications is applied to the woman during the birth process.10 Studies conducted on this have revealed that non-pharmacological methods are widely used in pain management today.11 Carolli and Magnini stated in their study that restrictive episiotomy creates milder perineal trauma, less suturing and less postpartum episiotomy complications compared to routine episiotomy.3 The routine application of episiotomy, which is one of the most negative traumas for pregnant women during labor, should be considered as an obstetric violence against women.12 He et al stated in his studies that women have a fear of episiotomy in vaginal delivery due to the presence of episiotomy pain and aesthetic concerns during childbirth.13
Applied cognitive behavioral techniques widely include non-pharmacological methods; they include techniques of imagination, relaxation, meditation, music, and distraction.11,14 These techniques reduce pain by affecting all dimensions of pain (perceptual, behavioral and emotional), increase birth satisfaction and do not have any side effects like pharmacological methods.11 Techniques by increasing the release of endorphins; it helps to relax the muscles, relieve pain, relax and activate the feelings of self-control.15 In Turkey, episiotomy is applied in more than 65% of all deliveries in the hospital and more than 90% of primiparous deliveries.16,17
The aim of this study was to examine the effect of virtual reality glasses applied during episiotomy repair in primiparous pregnant women on the level of pain and satisfaction of the mother.18 Morever, our study on the episiotomy application, which is widely used in both literature and Turkey, will both present a non-pharmacological alternative method for episiotomy pain and contribute to the national and international literature.
Materials and Methods
Study Design and Procedure
The research was carried out in the maternity ward of a city hospital between 15.06.2021 and 15.12.2021. In the delivery room team consisting of 5 midwives, 1 specialist, 1 secretary and 2 cleaning personnel; births are actively managed by midwives.
Sample
Sampling was calculated based on the study in the literature.17 The minimum number of patients required for the VAS change of 22.6±19.5 units between the two groups to be statistically significant at 90% power level during the episiotomy repair procedure was determined as 18 (α=0.05, 1-β=0.90). Analysis was done in Gpower3.1 version.
The research was carried out with a total of 50 primiparous pregnants, 25 of which were in the intervention group and 25 in the control group, considering the possible losses. The flow chart for this study is shown in Figure 1.
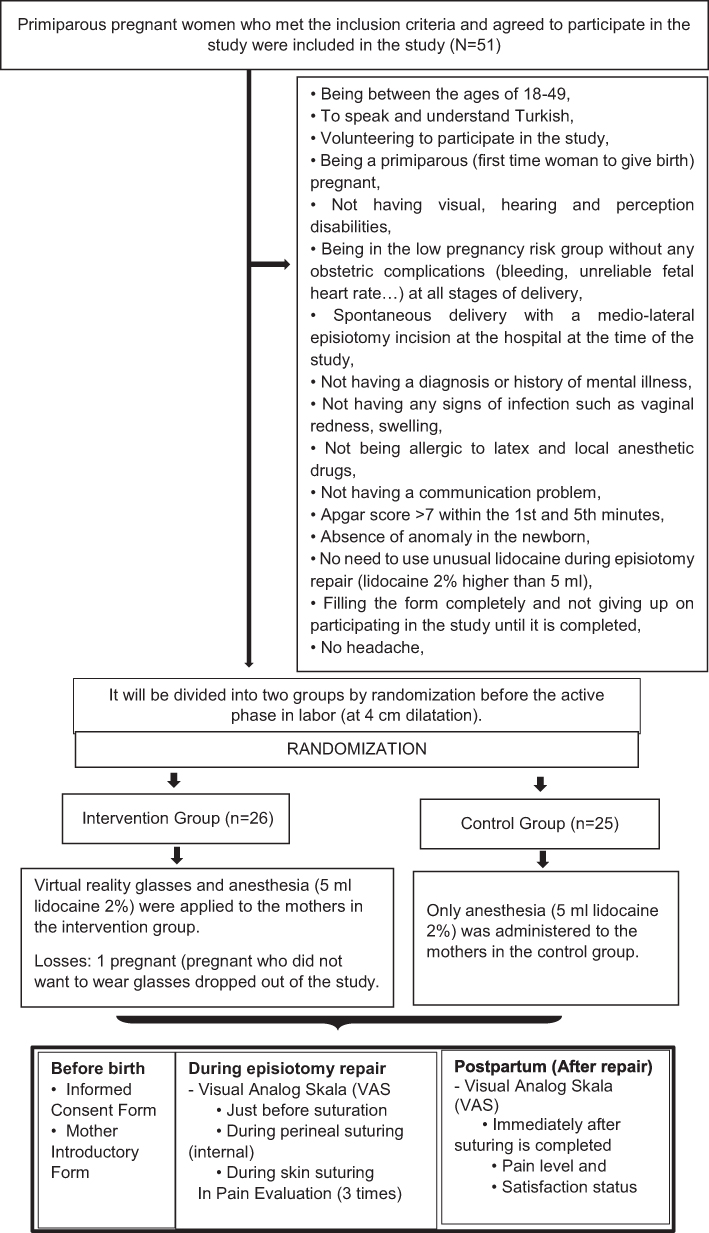 |
Figure 1 Study flow chart. |
Sampling Strategy
In the sample of the study, primiparous patients who were admitted to the delivery room at the time of the study and met the inclusion criteria were randomly assigned to the study and control groups (Figure 1). In the randomization, the simple random sampling method, which is one of the probabilistic sampling methods, the flipping a coin method was used and the pregnant women who volunteered to participate in the research meeting the criteria were assigned to the study and control groups according to their coin flip preferences.
The first pregnant woman in the study was included in the intervention group and her preference was asked to flipping a coin. Then, all pregnant women were included in the groups according to this preference category (text: control group, heads: intervention group).
Inclusion Criteria
Being between the ages of 18–49, to speak and understand Turkish, volunteering to participate in the study, being a primiparous (first time woman to give birth) pregnant, not having visual, hearing and perception disabilities, being in the low pregnancy risk group without any obstetric complications (bleeding, unreliable fetal heart rate…) at all stages of delivery, spontaneous delivery with a medio-lateral episiotomy incision at the hospital at the time of the study, not having a diagnosis or history of mental illness, not having any signs of infection such as vaginal redness, swelling, not being allergic to latex and local anesthetic drugs, not having a communication problem, apgar score >7 within the 1st and 5th minutes, absence of anomaly in the newborn, no need to use unusual lidocaine during episiotomy repair (lidocaine 2% higher than 5 mL), filling the form completely and not giving up on participating in the study until it is completed, no headache.
Research Hypotheses
Ho hypothesis: Virtual reality glasses applied during the episiotomy repair procedure have no effect on pain and patient satisfaction. H1 hypothesis: Virtual reality glasses applied during the episiotomy repair process have an effect on pain. H2 hypothesis: Virtual reality glasses applied during the episiotomy repair process have an effect on patient satisfaction.
Variables of the Study
Dependent variables of the study: Pain during episiotomy suturing procedure, patient satisfaction. Independent variables of the study: Socio-demographic characteristics of the patient, clinical characteristics, virtual reality glasses.
Data Collection Tools
In data collection, it was aimed to determine the personal and obstetric characteristics of the virtual reality glasses applied before episiotomy repair that may affect the pain and satisfaction of the mother; The “Mother introduction form” created by the researcher and the ‘Visual Analog Scales/VAS’ were used to determine the level of pain during episiotomy repair and satisfaction after repair.
Mother identification form: This form, which was developed by the researcher by examining the literature, will be filled before birth for the purpose of evaluating the mother.9,16 The form includes 13 questions in which some sociodemographic characteristics, gestational week, disease diagnoses and history, newborn apgar score and weight, episiotomy characteristics and repair time are questioned.
Visual analog scales (VAS): It is a scale used to measure subjective experiences. Visual Equivalence Scale is a scale developed by Price et al, and it is a pain measurement method that is extremely simple, easy to apply and requires minimal tools.19–22 It is a scale that is evaluated by individuals by making markings on a horizontal or vertical line of 10 cm or 100 mm, one end of which indicates that the person is very good and the other end is very bad. Pain assessment with VAS has long been an accepted method in the world literature.
Virtual reality glasses and video content: To be applied to the intervention group, virtual reality glasses and video images with music were used by the researcher to focus on the mothers during episiotomy repair. Four different video images with relaxing music were prepared, determined by the search method from interactive platforms, based on expert opinion. Schulzz Vrg Pro 5–7 inch smartphone 3D Vr virtual reality glasses as glasses were provided by the researcher and applied to the mothers in the collection of research data. Video images are shown in Figure 2.
 |
Figure 2 Video images. |
Data Collection
After explaining the purpose, importance and objectives of the research to the participants who volunteered to participate, verbal and written consent was obtained. Then, the pregnant women who met the inclusion criteria in the study were divided into two groups by randomization before the active phase (at 4–5 cm dilatation) and the data collection stages were followed up with the application. The first pregnant woman who was suitable for the study and agreed to participate was included in the intervention group and she was asked to choose flipping a coin method. The option preferred by the pregnant was accepted as the reference choice for the intervention group; pregnant women after that were included in the application groups according to their coin/toss preferences. The procedures were repeated until the targeted sample number (n: 50) was completed (Text: control group, Head: intervention group).
Episiotomy repair was performed by the investigator in the lithotomy position for all deliveries; before starting the procedure, the episiotomy depth and episiotomy length were determined with the help of a pipette (soft tissue (flexible during perineum measurement), sterile, disposable packaged features) and measured with a tape measure (0–100 cm interval measurement) and recorded in the mother information form. Afterwards, all stages were applied by the researcher.
Research data were collected in three stages; Phase I: Informed Consent Form, Mother Identification Form and the Mother Identification Form were applied by the researcher to the mothers in the experimental-control group determined by the randomization method, who met the research criteria and agreed to participate in the study.
Phase II: Anesthesia (5 mL lidocaine 2%) was administered by the researcher in the 3rd stage of labor of the pregnant women and at the stage of starting episiotomy repair in the lithotomy position; The intervention group was put on virtual reality glasses and watched one of the musical-videos determined in line with the mother’s preference (underwater videos (3 options), nature landscape videos (2 options)); no other application was made to the control group; Visual Analog Scale (VAS) was applied to determine the level of pain just before suturing, during (internal) perineal suturing, during skin suturing, and immediately after suturing was completed. Newborn apgar score and weight, episiotomy characteristics, and repair time were recorded in the Mother Identification Form.
Phase III: It was carried out in the postpartum room (intervention/control group). In order to determine the satisfaction level, the Visual Analog Scale (VAS) was applied by the researcher with face-to-face interview method and observation method.
Data Analysis
SPSS 22.0 (Scientific Packages for Social Sciences) Windows version package program was used for statistical analysis of the data. Compliance of numerical variables with normal distribution was tested with the Shapiro Wilk test. Student’s t-test was used to compare normally distributed variables in two groups, and Mann Whitney U-test was used to compare non-normally distributed variables in two groups. Repeated measure analysis of variance was applied in testing the variables in different groups and times. Relationships between categorical variables by CI-square test, Relationships between non-normally distributed numerical variables were tested with the Spearman rank correlation coefficient. P < 0.05 was considered significant.
Ethical Statement
Ethics committee approval was received from a Kahramanmaras Sutcu Imam University Faculty of Medicine Non-Interventional Clinical Research Ethics Committee (GAEK) dated 15.06.2021, session number: 2021/21 and decision number: 02 in order to conduct the research.
The trial is registered under the Clinical Trial reference number: NCT05578989. After the purpose, importance and objectives of the study were explained to the participants who volunteered to participate in the study, an informed consent form was signed.
It was explained that participation in the research is voluntary and all participants were asked to voluntarily sign a consent form. If interviewees felt disturbed responding to any questions at any point of time, they were free to stop the interview. Individual identification was kept anonymous.
The ethics review followed the principles outlined in the Declaration of Helsinki.
Results
The distribution and comparison of the patients in the intervention and control groups included in the study according to their socio-demographic and obstetric characteristics are shown in Table 1 and Table 2.
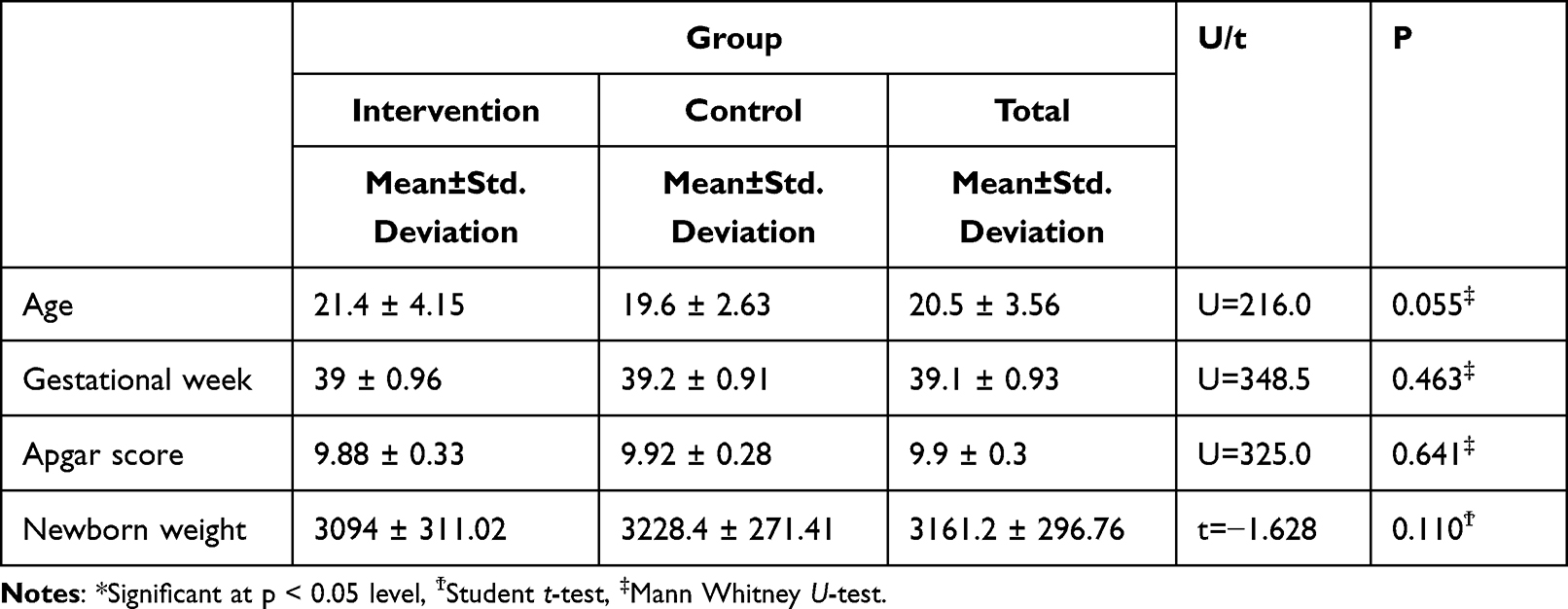 |
Table 1 Comparison of the Mean of some Sociodemographic and Obstetric Characteristics of Pregnant Women |
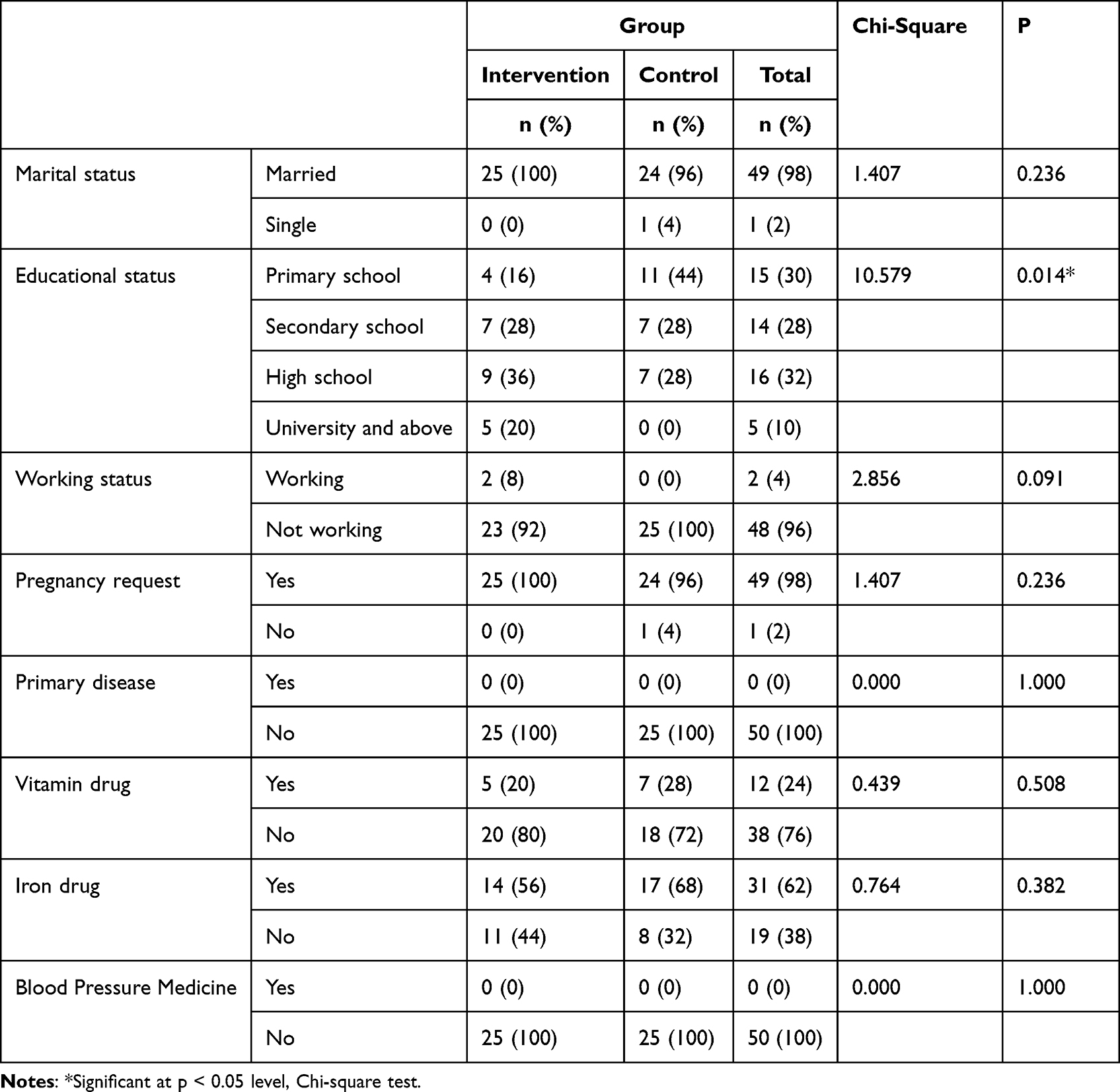 |
Table 2 General Distribution of Socio-Demographic and Obstetric Characteristics of Pregnant Women |
There was no statistically significant difference between the pregnant women in the intervention and control groups in terms of age, marital status, gestational week, newborn weight, newborn apgar score, occupational status, primary disease, pregnancy desire (whether or not the pregnancy was voluntary or not), and drugs used during pregnancy (p > 0.05), a statistically significant difference was found between the groups in terms of educational status (p = 0.014, p < 0.05) (Table 1).
It was observed that the mean age of the pregnant women participating in the study was 20.5 ± 3.56, the mean week of gestation was 39.1 ± 0.93 weeks, the mean newborn apgar score was 9.9 ± 0.3 points, and the mean newborn weight was 3161.2 ± 296.76 grams. It was determined that 98% of the pregnant women were married, 96% did not work in any job, 98% became pregnant voluntarily, none of them had a known primary disease, 24% did not use vitamins, and 62% did not use any medication other than iron supplements (Table 2).
In terms of education, it was observed that 16% of the intervention group was at primary school, 28% at secondary school, 36% at high school, and 20% at university and above, and the mothers in the intervention group had a higher education level than the mothers in the control group (p < 0.05) (Table 2).
The total average of the episiotomy length of the mothers included in the study, respectively; The total mean depth of episiotomy was 4.76 ± 0.89 cm in mothers in the intervention group, 4.92 ± 0.9% in mothers in the control group. It was determined that it was 75 cm, and the total average of the episiotomy repair time was 8.6 ± 2.89 minutes in the mothers in the intervention group and 10.04 ± 3.19 minutes in the mothers in the control group. There was no statistically significant difference between the control and intervention groups in terms of episiotomy length, depth and repair time (p > 0.05). Both groups are similar in terms of episiotomy features (Table 2).
The variation of pain score averages according to stages and groups are shown in Table 3. It was determined that the pain score averages showed statistically significant differences according to the stages and groups.
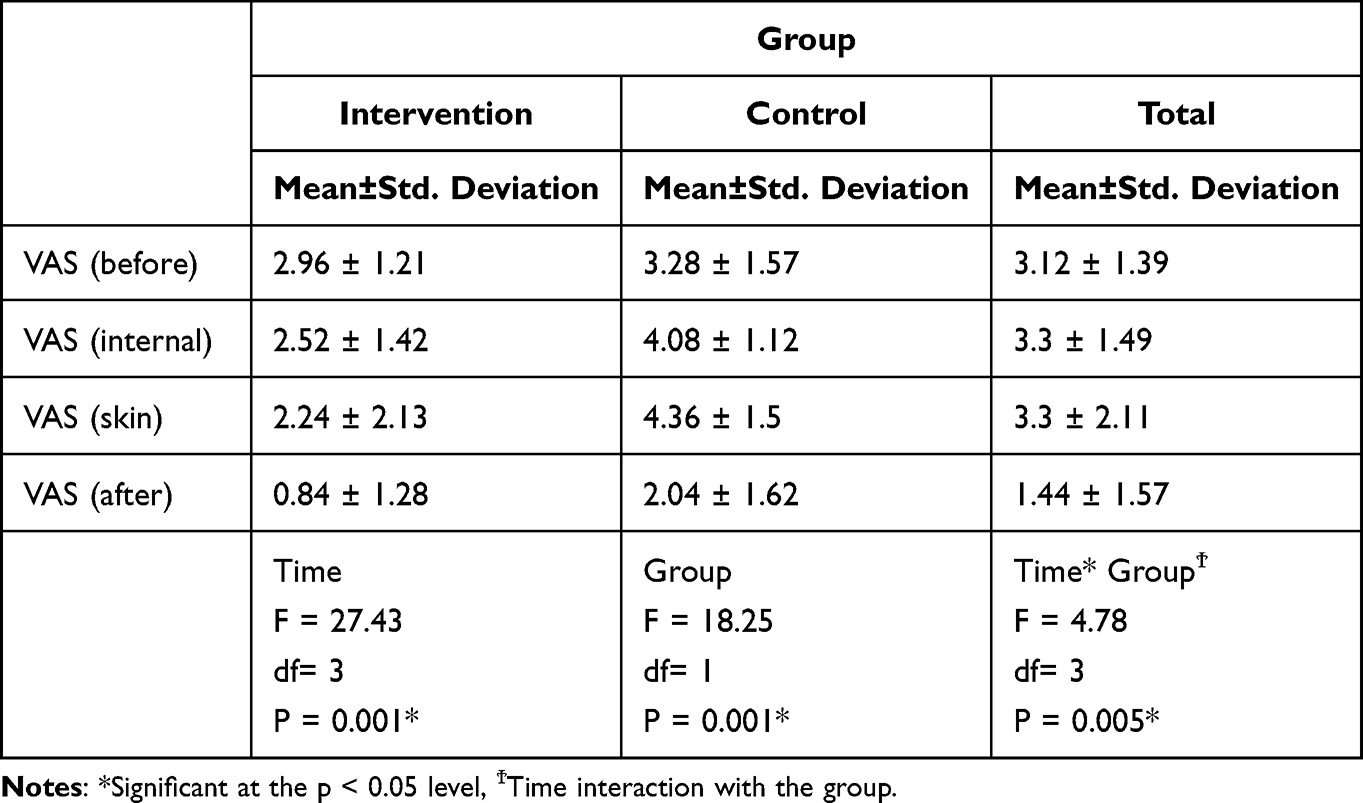 |
Table 3 Variation of Pain Score Averages According to Stages and Groups |
There was no significant difference between the two groups (control and intervention) in terms of VAS pain score averages evaluated before episiotomy repair (p: 0.601, p > 0.05) (Table 3).
There was a significant difference in VAS pain score averages evaluated during episiotomy internal suturing (p: 0.014, p < 0.05). It was observed that the mean pain score of the mothers in the control group was higher than that of the intervention group (Table 3).
There was a significant difference in VAS pain score averages evaluated during episiotomy skin suturing (p: 0.001, p < 0.05). It was observed that the mean pain score of the mothers in the control group was higher than that of the intervention group (Table 3).
There was no significant difference between the two groups in terms of VAS pain score averages evaluated immediately after episiotomy repair (p: 0.054, p > 0.05) (Table 3).
The distribution of pain scores at different stages of episiotomy in the two groups according to episiotomy characteristics is analyzed in Table 4.
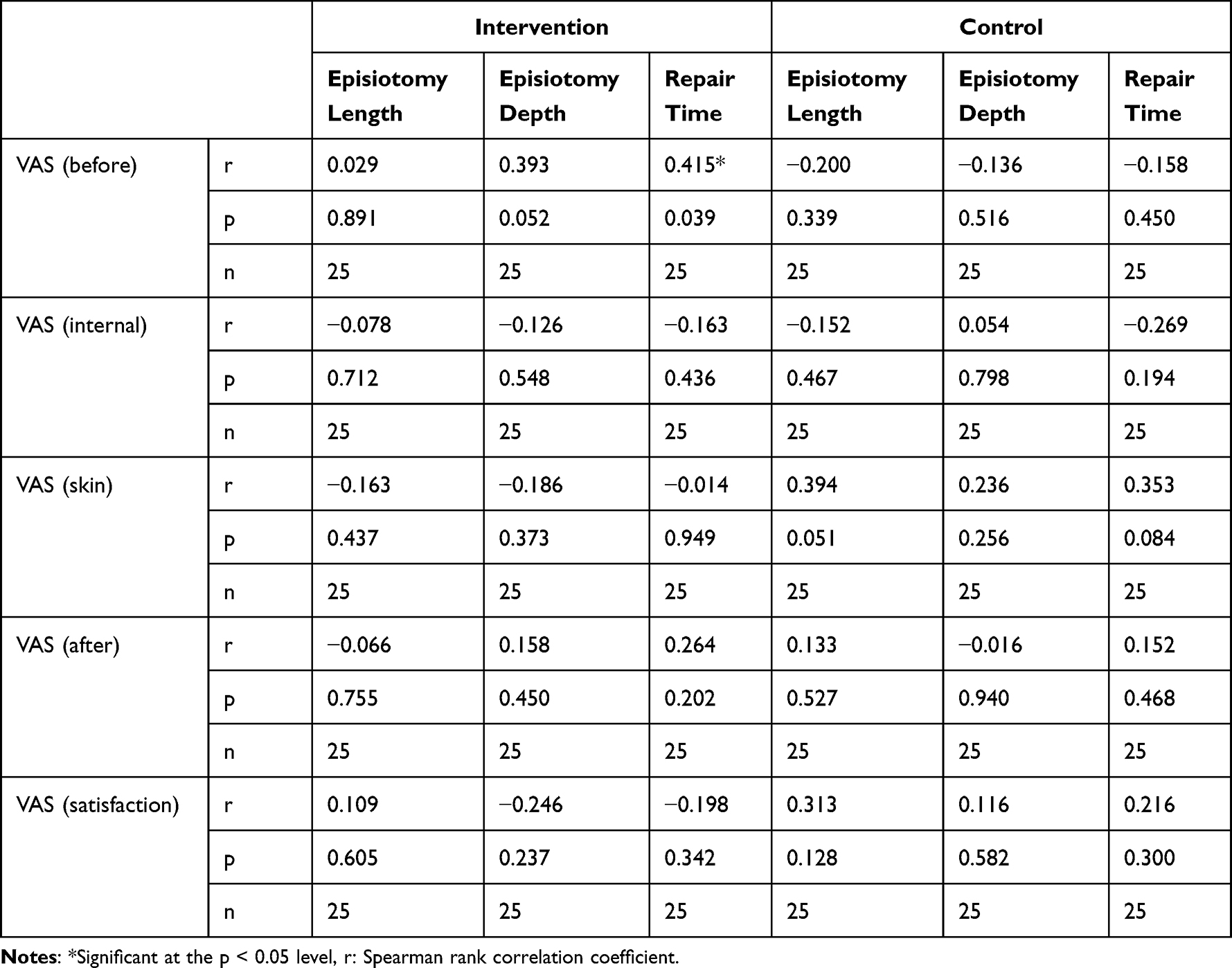 |
Table 4 Distribution of Pain Scores at Different Stages of Episiotomy in Two Groups According to Episiotomy Characteristics |
When the relationship between the change in pain scores of women in the control group at different stages of episiotomy and the variables of depth, length and repair time in their episiotomy was evaluated, no statistically significant correlation was found. While no statistically significant correlation was found between the pain scores of the women in the intervention group at different stages and the depth and length of the episiotomy, a positive correlation was found between the mean VAS pain scores before the episiotomy repair and the duration of the repair (p: 0.039, p < 0.05). As the VAS pain scores of the women in the intervention group, evaluated before episiotomy repair, increased, the duration of episiotomy repair also increased (Table 4).
At different stages of episiotomy, pain scores were classified according to pain scores in two groups, and the averages and percentages of pain scores are given in Table 5.
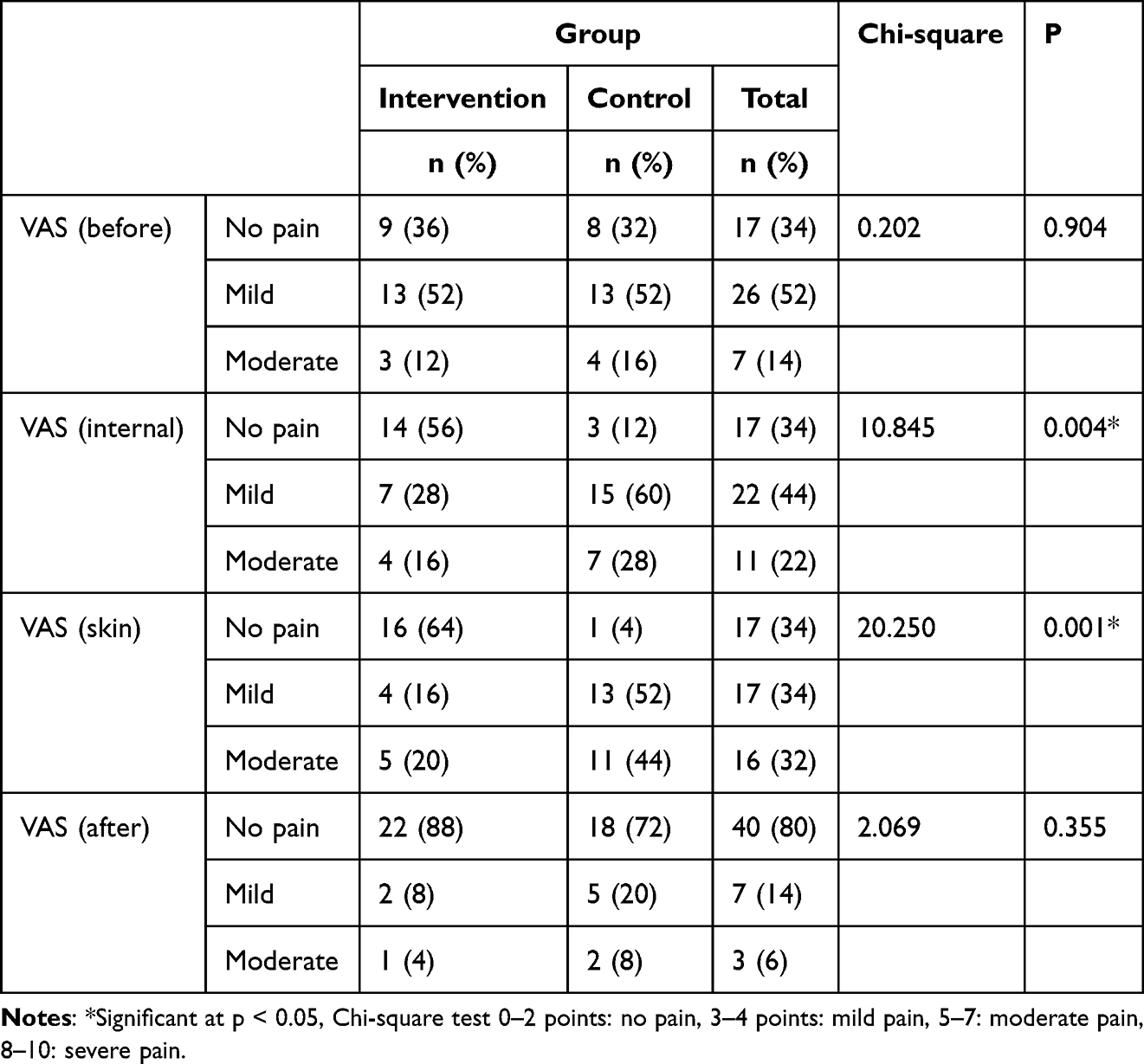 |
Table 5 Pain Score in Two Groups at Different Stages of Episiotomy |
In the control group, 12% of the mothers reported no pain during episiotomy internal suturing, 60% had mild pain and 28% reported moderate pain; it was determined that 56% of the mothers in the intervention group reported no pain, 28% reported mild pain and 16% reported moderate pain. Again, during the skin suturing of the episiotomy, 4% of the mothers in the control group reported no pain, 52% reported mild pain, and 44% reported moderate pain; it was determined that 64% of the mothers in the intervention group stated their pain as no pain, 16% as mild pain and 20% as moderate pain (Table 5).
It was observed that the mothers in the intervention group, who were applied virtual glasses, felt less pain in the perineal internal suturing and skin suturing stages of episiotomy repair compared to the mothers in the control group (Table 6).
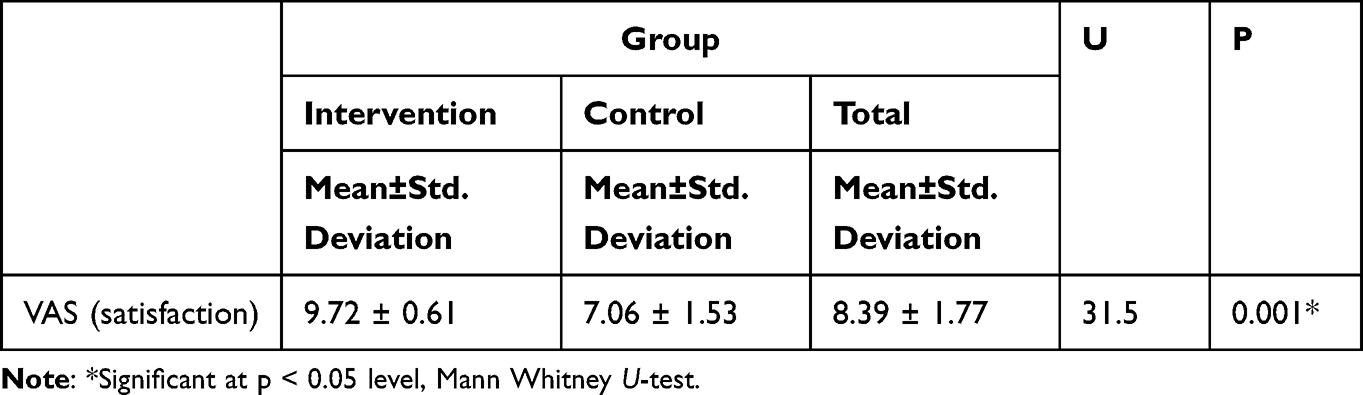 |
Table 6 Comparison of Satisfaction Scores in Both Groups |
When the two groups are examined according to their satisfaction score averages, statistically significant differences were found between control and intervention groups (p: 0.001, p < 0.05) (Table 6).
It was observed that the mothers in the intervention group, who were applied virtual glasses, had higher satisfaction levels, which were evaluated within the first hour after episiotomy repair, compared to the mothers in the control group (Table 6).
Discussion
When the educational status is examined, 30% of the pregnant women in our study have primary school, 28% have secondary school, 32% have high school and 10% have university or higher education level. While there was a difference in educational status between the control and intervention groups, the educational status statistics of our study are similar to the studies in the literature and Turkey Demographic and Health Survey (TDHS) 2018 data.11,21,23–25
In our study, it was determined that 98% of the pregnant women had a planned pregnancy. In the studies of Gür and E. Apay, it was found that pregnant women became pregnant voluntarily at a high rate, Shoorab et al. In their studies, it was determined that all pregnant women were satisfied with their newborn gender and sexual life.9,16 In addition, in the TDHS 2018 report, the rate of planned pregnancies was 75% and the rate of unwanted pregnancies was 15% in Turkey.
Unplanned pregnancies draw a parameter directly proportional to the mother’s age and birth order. While the rate of unplanned pregnancy is 5% in women younger than 20 years of age, it increases to 53% over the age of 40; While the rate of unplanned pregnancy is 2% in primiparas, it increases to 42% in multiparas with fourth and subsequent births. The mean age of the pregnant women in our study was 20.5 ± 3.56 years old and primiparous; explains the high rate of planned pregnancies.23
In the study, no statistically significant difference was found in terms of episiotomy length, depth and repair time of mothers in the intervention and control groups (p > 0.05). There was no statistically significant difference in terms of episiotomy length, depth and repair time of mothers included in the literature study to reduce the level of pain during episiotomy repair with virtual reality glasses.18
When the pain intensity VAS score average of the mothers included in the study was compared between the groups, the mean pain severity score measured during episiotomy internal suturing and episiotomy skin suturing was statistically significantly lower in the intervention group than the control group (p < 0.05), and the mean pain severity score measured before and immediately after episiotomy repair was between the intervention group and the control group. No significant difference was found (p > 0.05). This conclusion of the research is “H1: Virtual reality glasses applied during episiotomy repair process have an effect on pain” confirms the hypothesis.
As a result of these findings, it was determined that virtual reality glasses were effective in reducing the severity of pain during episiotomy repair. There is only one study in the literature that examines the effect of virtual reality glasses on pain severity during episiotomy repair procedure, which we refer to our research.18 In this clinical study conducted by Jahani Shoorab et al with 30 pregnant women to observe the effect of virtual reality glasses applied on anxiety and pain during episiotomy repair, clinical treatment with virtual reality glasses (video glasses and local infiltration 5 mL lidocaine solution 2%) in the intervention group during episiotomy repair. Anxiety and pain levels were measured by giving only local infiltration (5 mL of lidocaine solution 2%) to the control group. In conclusion, it was stated that virtual reality is an effective, complementary, non-pharmacological method to reduce pain during episiotomy repair. However, in the studies conducted with patients with different groups and diagnoses in the literature, there are results emphasizing that virtual reality glasses are effective on pain.26–29 In the study of Frey et al, it was determined that the use of virtual reality (VR) glasses in pregnant women during labor is an effective technique to reduce pain and anxiety during labor.28 Pratiw et al examined the effect of Virtual Reality on the reduction of pain during labor in primiparous women, and it was reported that virtual reality is an effective complementary non-pharmacological method to reduce pain during labor.29
The average of the satisfaction VAS score of the mothers included in the study, measured in the first hour; was found to be statistically significantly higher in the intervention group than in the control group (p: 0.001, p < 0.05). In the study, no statistically significant difference was found between the groups in terms of episiotomy length, depth and repair time, and satisfaction VAS score averages of mothers in the intervention and control groups (p > 0.05). This result of the research is “H2: Virtual reality glasses applied during the episiotomy repair process have an effect on patient satisfaction” confirms the hypothesis.
As a result of these findings, it was determined that virtual reality glasses increased the level of satisfaction during episiotomy repair. There is no study in the literature examining the effect of virtual reality glasses on satisfaction level during the episiotomy repair procedure. In this clinical study conducted by Jahani Shoorab et al with 30 pregnant women to observe the effect of virtual reality glasses applied during episiotomy repair on anxiety and pain; it was determined that the anxiety level during episiotomy repair and in the first hour after birth in the intervention group was lower than the anxiety level of primiparous women in the control group.30 However, in the studies conducted with different groups and patients with diagnoses in the literature, there are results examining the effect of virtual reality glasses on satisfaction; In Şen’s study examining the effect of virtual reality glasses applied during arteriovenous fistula (AVF) cannulation procedure in the hemodialysis unit on pain and patient satisfaction; It has been determined that virtual reality glasses increase patient satisfaction during the AVF cannulation procedure.21 Ebrahimian and Bilandi’s study with 93 pregnant women; It was determined that chewing gum and watching virtual reality videos increased birth satisfaction.31 In the meta-analysis conducted by Riva et al to systematically evaluate the studies published on virtual reality in the last twenty-two months; this technology has been found to have long-term positive effects in both the diagnosis and treatment of mental health disorders, anxiety disorders, eating and weight disorders, and pain management, along with existing treatments.32 In the bibliometric analysis of Yeung et al, in which virtual and augmented reality applications in medicine analyzed the scientific literature and scanned more than 8000 studies, it was found that it can be effective in many subjects such as anxiety disorders, pain, depression, paralysis, and that this technology should be developed further and made accessible to patients, required was determined.29 Also, a meta analysis shows that virtual reality is an effective technique for reducing anxiety, increasing satisfaction, and improving pain management during normal labor.33
Strengths and Limitations
The research was conducted in the delivery room of a single-center hospital. Since it is single-centered, it can only be generalized to primiparous pregnant women in this region.
Another limitation, we were not able to do a double-blind study first. Since the research was carried out within the scope of a master's thesis, the interventions were made by the first researcher and the data were collected by the same researcher.
While the study only involves a small number of women in one region/country, the strength is that the experiences of these women may be shared by women in other countries and the information may be relevant globally for midwives and other health-care professionals working with childbearing women.
Recommendations and Suggestions
In line with the research results, application of virtual reality glasses to mothers as a method of coping with pain during episiotomy repair process. It is applied in obstetrics clinics because it is an easy-to-apply, safe and effective method with no side effects. It is applied by midwives as it provides the mother’s harmony during episiotomy repair in labor, improves self-control mechanism, increases relaxation and satisfaction.
The inclusion of virtual reality glasses in midwifery care and practices. Since there is no scale to determine the level of satisfaction with the episiotomy repair process, developing a satisfaction scale for interventional applications at birth, which can be a specific scale for the satisfaction level we evaluate with VAS.
Making researches such as differentiating the video content watched with virtual reality glasses or determining which of the video content increases the pain and satisfaction more during episiotomy repair and increasing the researches on the subject since there is only one research in the literature. It is recommended to contribute more to the literature on non-pharmacological applications in reducing pain during episiotomy repair.
Conclusion
The results obtained in a randomized controlled clinical study to determine the effect of virtual reality glasses applied during the episiotomy repair procedure on pain and patient satisfaction are summarized below.
When the pain intensity VAS score average was compared within the group in the study, the mean pain severity score of the mothers in the intervention group, which was measured during episiotomy internal suturing, during episiotomy skin suturing, and immediately after episiotomy repair, decreased significantly compared to the mean pain severity score measured before episiotomy repair (p < 0.05), in the control group, it was determined that the mean pain severity score measured during episiotomy internal suturing and episiotomy skin suturing increased significantly compared to the mean pain severity score measured before and after episiotomy repair (p < 0.05).
The mean VAS pain score during episiotomy repair was found to decreased significantly after the application of virtual reality glasses in the mothers in the intervention group and increase significantly in the mothers in the control group (p < 0.05). The average of the VAS satisfaction score evaluated within the first hour after episiotomy repair. It was found that it was statistically significantly higher in mothers in the intervention group than in the mothers in the control group (p < 0.05).
Data Sharing Statement
The clinical trial data of this article will not be shared.
Acknowledgments
We are thankful to the kind support of the staffs at Kahramanmaras Necip Fazıl City Hospital maternity clinic and participant pregnant women.
This study was produced from the master's thesis of Kahramanmaraş Sütçü İmam University Health Sciences Institute, Department of Midwifery.
Funding
The authors received no financial support for the research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Olza I, Uvnas-Moberg K, Ekström-Bergström A, et al. Birth as a neuro-psycho-social event: an integrative model of maternal experiences and their relation to neurohormonal events during childbirth. PLoS One. 2020;15(7 July):1–15. doi:10.1371/journal.pone.0230992
2. Jiang H, Qian X, Carroli G, Garner P. Selective versus routine use of episiotomy for vaginal birth. Cochrane Database Syst Rev. 2017;2017:2.
3. Carroli G, Mignini L. Episiotomy for vaginal birth. Cochrane Database Syst Rev. 2009;1:1–53.
4. Khresheh R, Barclay L. Knowledge, attitude and experience of episiotomy practice among obstetricians and midwives in Jordan. Women Birth. 2020;33(2):e176–81. doi:10.1016/j.wombi.2019.03.007
5. Çelik YI, Bal DM. Effects of perineal massage with vaseline on labor process. Marmara University Health Sciences Institute, Ulusal Tez Merkezi. yok.gov.tr; 2020.
6. Yaşar H, Derya AY. The effect of perineal massage performed during the labour on the childbirth comfort, perineal pain and trauma in nulliparous women İnönü University Health Sciences Institute; 2019. Available from: https://tez.yok.gov.tr/UlusalTezMerkezi/tezSorguSonucYeni.jsp.
7. Albers LL, Sedler KD, Bedrick EJ, Teaf D, Peralta P. Midwifery care measures in the second stage of labor and reduction of genital tract trauma at birth: a randomized trial. J Midwifery Women’s Heal. 2005;50(5):365–372. doi:10.1016/j.jmwh.2005.05.012
8. Gould J, Webb SS, Byrne C, et al. Red flags for episiotomy in a midwife-led birth: using co-production with midwives to capture clinical experience. Women Birth. 2022;36:217–223. doi:10.1016/j.wombi.2022.06.009
9. Potur DC, Merih YD, Külek H, Gürkan ÖC. The validity and reliability of the Turkish version of the childbirth comfort questionnaire. J Nurs. 2015;18(4):252–258.
10. Schuiling KD, Sampselle C, Kolcaba K. Exploring the presence of comfort within the context of childbirth. Theory Midwif Pract. 2011;2011:197–214.
11. Gür EY, Apay SE. The effect of cognitive behavioral techniques using virtual reality on birth pain: a randomized controlled trial. Midwifery. 2020;91:102856. doi:10.1016/j.midw.2020.102856
12. Kilci Ş, Demirel Bozkurt Ö, Saruhan A. A violation of women’s rights: obstetric violence. Arch Med Rev J. 2020;29(2):122–128.
13. He S, Jiang H, Qian X, Garner P. Women’s experience of episiotomy: a qualitative study from China. BMJ Open. 2020;10(7):e033354. doi:10.1136/bmjopen-2019-033354
14. Yanık Tok N, Ertem G. The systematic analyze them in terms the nonpharmacological methods used in the treatment of perineal pain after episiotomy. GUJHS. 2020;9(2):195–208.
15. Manesh MJ, Kalati M, Hosseini F. Snoezelen room and childbirth outcome: a randomized clinical trial. Iran Red Crescent Med J. 2015;17:5.
16. Fernando RJ. Risk factors and management of obstetric perineal injury. Curr Obstet Gynaecol. 2007;17(5):238–243.
17. Karaçam Z, Eroğlu K. Effects of episiotomy on bonding and mothers’ health. J Adv Nurs. 2003;43(4):384–394. doi:10.1046/j.1365-2648.2003.02727.x
18. Jahani Shoorab N, Zagami SE, Nahvi A, et al. The effect of virtual reality on pain in primiparity women during episiotomy repair: a randomize clinical trial. Iran J Med Sci. 2015;40(3):219–224.
19. Price DD, McGrath PA, Rafii A, Buckingham B. The validation of visual analogue scales as ratio scale measures for chronic and experimental pain. Pain. 1983;17(1):45–56. doi:10.1016/0304-3959(83)90126-4
20. Hasson D, Arnetz BB. Validation and findings comparing VAS vs. Likert scales for psychosocial measurements. Int Electron J Health Educ. 2005;8(8):178–192.
21. Sarman A, Sarman E, Tuncay S. Investigation of the quantity and content of postgraduate theses conducted using virtual reality in nursing and published in YOK Thesis in Turkey. Bingöl Univer Health J. 2021;2(2):71–82.
22. Akbay A. Evaluation of Visual analog scale (VAS). Turkish Neurosurgery Association. Available from: https://www.spinetr.com/uploads/files/skor/vizuelanalogskala.pdf.
23. Turkey Demographic and Health Survey (TDHS). Hacettepe university of population studies; 2018:148–149. Available from: http://www.hips.hacettepe.edu.tr/tnsa2018/rapor/TNSA2018_ana_Rapor.pdf.
24. Toker S, Çitak G. Investigation of health indicators of women in reproductive age in turkey according to turkey demographic and health surveys. J TOGU Health Sci. 2021;1(2):72–84.
25. Yılmaz AN. The effect of haptonomy and virtual reality on anxiety, prenatal attachment and acceptance of pregnancy in the unplanned pregnant women: imagining the baby. İnönü University Health Sciences Institute, Ulusal Tez Merkezi. yok.gov.tr; 2021.
26. Kaplan B The effect of virtual reality glasses on reducing pain during intravenous cannulation in children Erciyes. University Health Sciences Institute; 2020. Available from: https://tez.yok.gov.tr/UlusalTezMerkezi/tezSorguSonucYeni.jsp.
27. Goksu F The Effect of Virtual Reality Headset that is used during blood drawal on the pain felt by the children. Bülent Ecevit University Health Sciences Institute; 2017. Available from: https://tez.yok.gov.tr/UlusalTezMerkezi/tezSorguSonucYeni.jsp.
28. Frey DP, Bauer ME, Bell CL, et al. Virtual reality analgesia in labor: the VRAIL Pilot Study - a preliminary randomized controlled trial suggesting benefit of immersive virtual reality analgesia in unmedicated laboring women. Anesth Analg. 2019;128(6):E93–6. doi:10.1213/ANE.0000000000003649
29. Pratiw IG, Husin F, Ganiem AR, Susiarno H, Arifin A, Wirahkusuma F. The effect of virtual reality on pain in primiparity women. Int J Nurs Heal Sci. 2017;4(4):46–50.
30. Jahani Shourab N, Zagami SE, Golmakhani N, et al. Virtual reality and anxiety in primiparous women during episiotomy repair. Iran J Nurs Midwifery Res. 2016;21(5):521–526. doi:10.4103/1735-9066.193417
31. Ebrahimian A, Rahmani Bilandi R. Comparisons of the effects of watching virtual reality videos and chewing gum on the length of delivery stages and maternal childbirth satisfaction: a randomized controlled trial. Iran J Med Sci. 2021;46(1):15–22. doi:10.30476/ijms.2019.82782.1119
32. Riva G, Wiederhold BK, Mantovani F. Neuroscience of virtual reality: from virtual exposure to embodied medicine. Cyberpsychol Behav Soc Netw. 2019;22(1):82–96. doi:10.1089/cyber.2017.29099.gri
33. Baradwan S, Khadawardi K, Badghish E, et al. The impact of virtual reality on pain management during normal labor: a systematic review and meta-analysis of randomized controlled trials. Sex Reprod Healthc off J Swed Assoc Midwives. 2022;32(4):100720. doi:10.1016/j.srhc.2022.100720
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Efficacy of a Preoperative Occupational Therapy Educational Session for Saudi Patients Undergoing a Lower Extremity Joint Replacement
Al-Heizan MO, Shoman A, Tawffeq A, Banamah A, Balkhair F, Filimban S, Alsinan W, Batouk O, Turkistani T
Journal of Multidisciplinary Healthcare 2023, 16:31-38
Published Date: 10 January 2023
Investigating Factors Associated with the Development of Postnatal Depression After Cesarean Delivery: A Validation Cohort Study
Tan DJA, Sultana R, Chow SYX, Tan CW, Tan HS, Chen HY, Chua TE, Sng BL
Neuropsychiatric Disease and Treatment 2024, 20:439-447
Published Date: 29 February 2024