Back to Journals » ClinicoEconomics and Outcomes Research » Volume 18
Real-World Treatment Patterns of Elranatamab in Patients with Multiple Myeloma in Japan: The EVEREST Study
Authors Yoshihara S ![]() , Meche A, Hlavacek P, Johnson SM, Demers AS, Nador G, Ikoma S, Yadav CP, Assaf CA, DiBonaventura M
, Meche A, Hlavacek P, Johnson SM, Demers AS, Nador G, Ikoma S, Yadav CP, Assaf CA, DiBonaventura M ![]() , Chen Y
, Chen Y
Received 18 November 2025
Accepted for publication 14 February 2026
Published 11 March 2026 Volume 2026:18 581258
DOI https://doi.org/10.2147/CEOR.S581258
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Giorgio Colombo
Satoshi Yoshihara,1 Aster Meche,2 Patrick Hlavacek,3 Sarasa MA Johnson,4 Ann-Sophie Demers,4 Guido Nador,5 Shohei Ikoma,6 Chandra Prakash Yadav,7 Carla AL Assaf,8 Marco DiBonaventura,3 Yong Chen9
1Department of Hematology, Hyogo Medical University, Nishinomiya, Japan; 2Real World Evidence - Oncology, Pfizer Inc, New York, NY, USA; 3Patient and Health Impact, Pfizer Inc, New York, NY, USA; 4Statlog Inc, Quebec, QC, Canada; 5Oncology Medical - Global Hematology, Pfizer Ltd, Surrey, UK; 6Oncology Medical Affairs, Pfizer Japan Inc, Tokyo, Japan; 7Biostatistics, Pfizer Ltd, Chennai, India; 8Global Medical Affairs, Pfizer SA, Brussels, Belgium; 9Medical Real World Evidence/Epidemiology- Hematology Oncology, Pfizer Inc, Collegeville, PA, USA
Correspondence: Patrick Hlavacek, Patient Health and Impact, Pfizer Inc., New York, NY, USA, Email [email protected]
Introduction: Elranatamab, a B-cell maturation antigen-CD3 bispecific antibody, was approved in Japan in March 2024 for the treatment of relapsed or refractory multiple myeloma (MM). However, real-world (RW) data on its use remain limited. This retrospective study evaluated patient characteristics and elranatamab treatment patterns in patients with MM in Japan using the Medical Data Vision (MDV) database.
Methods: This EVEREST study used de-identified claims data from the MDV database for adult patients with MM who initiated treatment with elranatamab between March 26, 2024, and March 31, 2025. Follow-up was divided, based on expected dosing schedules, into a step-up dosing (SUD) period, a weekly (QW) maintenance period (MP1), an every 2 weeks (Q2W) maintenance period (MP2), and an overall follow-up period. Treatment patterns were reported descriptively. Estimated annual vial usage was extrapolated.
Results: Patients (N=253) with a median age of 74 years (range 41– 93 years) and median treatment duration of 60.0 days (interquartile range [IQR], 26.0– 136.0) were included. The mean (median [IQR]) time between elranatamab administrations across dosing periods were SUD 4.0 days (4.0 [3– 4]), MP1 9.8 days (7.0 [7– 9]), and MP2 13.0 days (14.0 [7– 14]), indicating less frequent dosing than recommended in MP1, and comparable dosing in MP2. Nearly all administrations were in inpatient settings during SUD, and most were in outpatient settings during maintenance periods. Despite variable dosing during the maintenance periods, annual elranatamab usage was lower than the approved label recommendations for Japan (34.4 vs 39.0 vials per year).
Conclusion: Early RW data on elranatamab administration and vial usage in patients with MM in Japan suggest that dosing is generally aligned with label expectations, with variable dosing during QW and Q2W maintenance for some patients. Projected vial usage in this RW setting was lower than the expected usage per label.
Keywords: bispecific antibody, elranatamab, Japan, multiple myeloma, real-world data, treatment patterns, vial usage
Introduction
Multiple myeloma (MM) is a hematologic malignancy characterized by clonal proliferation of plasma cells in the bone marrow, leading to end-organ damage and significant morbidity.1 The burden of MM in Japan is notable, with an incidence rate of 6.2 per 100,000 people2 and a 5-year overall survival rate of 45.6% estimated between 2006 and 2020.3 Although the therapeutic landscape is evolving, MM eventually relapses or becomes refractory to treatment,4 complicating the choice of subsequent treatment regimens and making new treatment options essential to improving survival in Japan and worldwide for patients with relapsed or refractory MM (RRMM).
On March 26, 2024, elranatamab became the first B-cell maturation antigen (BCMA)-CD3 bispecific antibody approved by the Pharmaceuticals and Medical Devices Agency (PMDA) in Japan for the treatment of adults with RRMM.5 Approval was based on the Phase 2 registrational MagnetisMM-3 trial (NCT04649359), in which elranatamab demonstrated deep and durable responses and a manageable safety profile in patients with RRMM who have triple-class refractory disease and have not received any prior BCMA-directed therapy.6,7 In an analysis of Japanese patients in MagnetisMM-3 and MagnetisMM-2 (NCT04798586), the efficacy and safety of elranatamab were similar to those of the overall MagnetisMM-3 trial population.8
Elranatamab is packaged in single-dose vials containing 44 mg (1.1 mL) or 76 mg (1.9 mL).9–11 The recommended dosing schedule for elranatamab in Japan includes 2 step-up doses (12 and 32 mg) administered subcutaneously on Day (D)1 and D4, respectively, followed by the first fixed full treatment dose (76 mg) on D8. Treatment continues on a weekly (QW) basis through D168 (28 days/cycle x 6 cycles) when responders are eligible to switch to dosing every 2 weeks (Q2W). As of June 2025, dosing frequency can be further reduced to every 4 weeks (Q4W) in patients who have maintained the response following 24 weeks of Q2W dosing.11 In MagnetisMM-3, most patients maintained or improved their response ≥6 months after switching to less frequent dosing (Q2W then Q4W) and the incidence of some grade 3 or 4 treatment-emergent adverse events (TEAEs) decreased.6,12
Although the efficacy and safety of elranatamab have been established in clinical trials,6–8,12,13 data on real-world (RW) usage of elranatamab is limited. The Administration of Elranatamab in the Real-World: Treatment Patterns, Healthcare Resource Utilization, Costs, Effectiveness, and Safety (ALTITUDE-1; EUPAS1000000229) study assessed RW treatment and dosing patterns of elranatamab using data from Komodo Health’s Healthcare Map™ in the US.14 In practice, elranatamab may be administered less frequently than indicated in the US prescribing information (39 vials/year).9,14
The Evaluation of Elranatamab Utilization in Real World Settings (EVEREST) study was carried out to assess the patient demographics, disease characteristics, and treatment patterns of patients with MM treated with elranatamab in Japan.
Materials and Methods
Study Design and Patient Population
This retrospective cohort analysis used de-identified data from the Japan Medical Data Vision (MDV) database, a comprehensive resource containing administrative data from more than 540 hospitals in Japan. The MDV database captures approximately 30% of advanced treatment hospitals in Japan and includes health claims data from all insurance types (ie, Social, National, and Elderly Insurance). The study period was from April 2008 (start of data availability in MDV) to March 2025 (end of data availability in MDV).
The study population comprised patients diagnosed with MM (ICD-10 code: C90.0) who were 18 years of age or older, with a first health claim for the administration of elranatamab on or after March 26, 2024, the PMDA approval date for elranatamab (See Figure S1 in the electronic supplementary material for details). The data cutoff was March 31, 2025. Patients with evidence of the administration of elranatamab as part of a clinical trial were excluded.
The date of the first claim with elranatamab administration after March 26, 2024 was defined as the index date. The follow-up period, between the index date and the last observed elranatamab administration, was divided into five sub-periods to allow for reporting study endpoints across different phases, based on the expected dosing schedule of patients switching to Q2W at the earliest possible time (D169). The five sub-periods were: index date, step-up dosing (SUD, index date to D8), maintenance period 1 (MP1, D9 to D168 post-index date, corresponding to QW dosing), maintenance period 2 (MP2, D169 post-index date to the end of follow-up, corresponding to earliest possible switch to Q2W dosing), and overall follow-up (index date to the end of follow-up). Patients were censored on the date of their last observed elranatamab administration.
Outcome Measures
Elranatamab timing and dosing variables included reported vial size utilized, time between elranatamab administrations, frequency of administrations (by vial size), and observed duration of treatment. Estimated annual vial use was extrapolated from the reported mean time between administrations throughout the follow-up period.
Statistical Analysis
All analyses were descriptive in nature and no formal statistical comparisons were made. If applicable, the frequency and percentage of patients with missing data for each variable were described. All patients who met the eligibility criteria were included in the analysis. For analyses conducted at the claims level, in which all claims with elranatamab administration recorded during the specified time period were evaluated, means and medians were calculated across all intervals between treatment administrations during the time period. Dichotomous and categorical variables were summarized by the number and percentage of administrations in each category. Continuous variables were described using mean (SD), median (IQR), minimum, and maximum.
The number of vials administered on an annualized basis was calculated to inform future economic modeling assumptions. These calculations for the first year of treatment assumed that the number of vials used during the SUD period matched that of the Japan prescribing information (J-PI). The mean number of days between administrations during MP1 and MP2 were separately applied to estimate the total number of vials a patient would be expected to use if they remained on treatment for the entire first year. These annualized vial usage estimates were descriptively compared to the annual vial usage reported from the MagnetisMM-3 trial data and the J-PI expected usage. SAS version 9.4 was used for statistical analysis.
Ethics
Approval from an institutional review board/independent ethics committee was not required for this study as only de-identified secondary data sources were used.
Results
Patients
During the year following PMDA approval of elranatamab, 253 patients with MM in the MDV database initiated elranatamab treatment (Table 1). The median (range) age was 74.0 (41.0–93.0) years and 54.5% of patients were female. In the 6 months prior to treatment initiation, the mean (SD) Charlson Comorbidity Index score was 6.9 (2.9), with 147 (58.1%) patients having a score of >5. Most patients were triple-class exposed (82.2%) and 42.3% were penta-drug exposed. Three (1.2%) patients had received prior chimeric antigen receptor T cell therapy, and 38 (15.0%) had undergone a stem cell transplant.
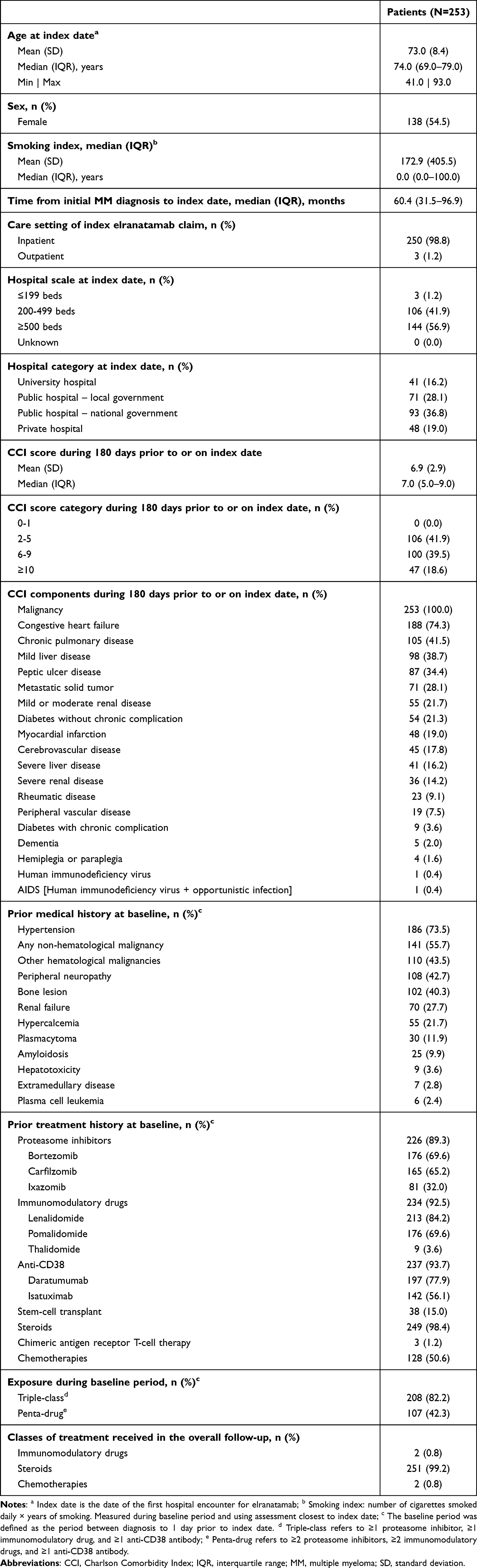 |
Table 1 Patient Demographics, Clinical Characteristics, and Treatment History of Patients Initiating Elranatamab |
Elranatamab Treatment Characteristics
The observation period (time from first to last claim for elranatamab administration) of the EVEREST study was 302 days. The median (IQR) duration of therapy between index date and the last recorded administration was 60.0 (26.0–136.0) days (Table 2). Of the 253 claims for elranatamab administration at the index date, 247 (97.6%) were from vial size 44 mg/1.1 mL, all on an inpatient basis. Six (2.4%) administrations were from 76 mg/1.9 mL vials, 3 (1.2%) were in an inpatient setting and 3 (1.2%) were in an outpatient setting.
 |
Table 2 Dosing and Administration Patterns of Patients Receiving Elranatamab |
In the SUD period, 606 claims for elranatamab administration were received for 253 patients, 474 (78.2%) administrations from 44 mg/1.1 mL vials (all inpatient), and 132 (21.8%) administrations from 76 mg/1.9 mL vials (126 [20.8%] inpatient and 6 [1.0%] outpatient). The mean time between administrations was 4.0 days (median [IQR], 4.0 [3.0–4.0]). During SUD, 230 (90.9%) patients received at least 2 administrations of elranatamab.
In MP1, 226 patients had sufficient follow-up to be observed and 97.6% of the 1833 claims for elranatamab administration were for 76 mg/1.9 mL vials, split between 445 (24.3%) inpatient and 1344 (73.3%) outpatient administrations. Forty-four administrations (2.4%) were from 44 mg/1.1 mL vials, with 35 (1.9%) on an inpatient basis. The mean time between administrations for MP1 was 9.8 days (median [IQR], 7.0 [7.0–9.0]), with 207 patients (81.8%) completing 2 or more administrations.
Forty patients had sufficient follow-up to be observed in MP2; submitting 140 claims for elranatamab administration for the period. Of these, 132 (94.3%) administrations were from 76 mg/1.9 mL vials, and 90.7% were administered outpatient. Twenty-seven patients received 2 or more administrations, and the mean time between administrations for MP2 was 13.0 days (median [IQR], 14.0 [7.0–14.0]).
Projected annualized vial usage in the first year of treatment, based on the expected vial usage during SUD (3 doses) and the mean days between administrations in MP1 (mean 9.8 days) and MP2 (mean 13.0 days), was 34.4 vials.
Discussion
The findings from this EVEREST study offer early insights into how elranatamab has been used in RW clinical practice in Japan since its approval by the PMDA in March 2024. This study provides a valuable complement to clinical trial data by reflecting how elranatamab is administered in routine clinical practice.
Our findings indicate that elranatamab is largely administered in accordance with the recommended dosing schedule during the SUD phase. During SUD, the mean number of days between administrations was 4.0 days compared with 5.7 days reported in the ALTITUDE-1 study using Komodo Health’s Healthcare Map™ databases in the US.14 In MP1 and MP2, the mean number of days between administrations using the MDV database was 9.8 and 13.0 days. Recommended dosing is every 7 days for MP1 and every 14 days for responders in MP2, with these data suggesting that, in Japan, elranatamab administration during the MPs varied slightly from the label recommendations, occurring at a reduced frequency in MP1 and a comparable frequency during MP2. Reduced dosing frequencies compared to the label recommendations were also shown in the ALTITUDE-1 study, where the mean number of days between administrations in MP1 and MP2 was 10.7 and 26.0 days, respectively.14 It was also noted that nearly one-quarter of administrations in MP1 occurred on a Q2W basis and one-quarter of administrations in MP2 occurred on a Q4W (every 28 days) cadence. Collectively, these RW data suggest that adherence to initial step-up and maintenance dosing of elranatamab is variable and that elranatamab is commonly administered less frequently than recommended by the J-PI and the US prescribing information. This reduced administration frequency may be due to treatment-related de-escalation, such as toxicity management, or factors unrelated to treatment, such as schedule constraints or patient preference. However, claims-based resources such as the MDV database do not capture clinician-reported reasons for administration frequency, so the drivers thereof cannot be ascertained.
The recommendation is to use a 44 mg/1.1 mL vial for each of the 2 step-up doses.9,10 However, it was reported that 6 patients (2.4%) received their initial dose on the index date using 76 mg/1.9 mL vials. Three of these patients received their initial dose as an outpatient, despite the protocol indicating that patients should be hospitalized for 48 hours after the first dose.11 However, as the patients’ full treatment histories may not have been captured in the MDV, it is possible that the first elranatamab administration reported may not have been the first administration for the patient. This may have impacted the reported deviations from the SUD protocols. During MP1 and MP2, the recommended dose is 76 mg, although 10.6% and 12.5% of patients, respectively, received at least 1 elranatamab administration from a 44 mg/1.1 mL vial. In MP1 and MP2, most patients were treated on an outpatient basis.
Annualized vial usage from this EVEREST study (34.4 vials) is lower than the usage recommended in the J-PI for the first year of treatment (39.0 vials), which includes two 44 mg/1.1 mL vials for SUD, twenty-three 76 mg/1.9 mL vials used during QW MP1 until scheduled transition at D168 to (Q2W) when a further fourteen 76 mg/1.9 mL vials should be used during MP2. Observed annualized vial usage from the MagnetisMM-3 trial data ranged from 20.0 vials for all patients (N=187) to 29.1 vials for patients who achieved a partial response or better (n=97), while RW data from ALTITUDE-1 also suggested less frequent dosing than recommended.14 Taken together, understanding RW annualized vial usage may help inform future cost-effectiveness and budget impact analyses by providing insight on RW dosing frequency and drug utilization that differ from label-based assumptions. Using these RW patterns in economic models may improve the accuracy of estimates of drug acquisition costs and support payer budgeting decisions within the Japanese healthcare system.
Use of the MDV database is limited by the completeness and accuracy of the underlying claims data, which does not include comprehensive medical and treatment histories of all patients. Not all hospitals are included in the MDV database, resulting in identification of a patient population that may not be representative of all patients with MM in Japan. There are also limited data on reasons for some of the deviations in maintenance dosing frequency. Interpretation of maintenance dosing patterns and annualized vial usage is limited by the short median treatment duration (60 days) and the small proportion of patients entering MP2 (15.8%), such that the reported annualized vial estimates reflect projections based on incomplete treatment courses rather than observed full-year utilization. This study was also limited to the evaluation of elranatamab dosing patterns and vial utilization; therefore, the effects of deviations from label-recommended dosing on efficacy or safety were unable to be evaluated.
Conclusion
Claims data provided RW information on elranatamab administration and vial usage in patients with MM in Japan. Early evidence indicates that elranatamab is administered largely according to initial dosing recommendations, with some deviations in maintenance period dosing frequency resulting in slightly lower projected annualized vial usage than recommended. Further research with longer follow-up is warranted to better understand treatment patterns and optimize dosing strategies in MM patients in Japan.
Abbreviations
BCMA, B-cell maturation antigen; D, day; IQR, interquartile range; J-PI, Japan prescribing information; MDV, Medical Data Vision; MM, multiple myeloma; MP, maintenance period; PMDA, Pharmaceuticals and Medical Devices Agency; QW, once weekly; Q2W, every 2 weeks; Q4W, every 4 weeks; RRMM, relapsed or refractory multiple myeloma; RW, real world; SUD, step-up dosing; TEAE, treatment-emergent adverse event.
Data Sharing Statement
Upon request, and subject to review, Pfizer will provide the data that support the findings of this study. Subject to certain criteria, conditions, and exceptions, Pfizer may also provide access to the related individual de-identified patient data. See https://www.pfizer.com/science/clinical-trials/trial-data-and-results for more information.
Ethics/Ethical Approval
Approval from an institutional review board/independent ethics committee was not required for this study as only de-identified secondary data sources were used.
Acknowledgment
The abstract of this paper was presented at the American Society of Hematology Annual Meeting as a poster presentation/conference talk with interim findings. The poster’s abstract was published in “Poster Abstracts” in Blood: https://www.sciencedirect.com/science/article/pii/S000649712505548X.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was sponsored by Pfizer. Medical writing support was provided by Robyn Roth, PhD, of Nucleus Global and was funded by Pfizer.
Disclosure
Satoshi Yoshihara: Consultancy (includes expert testimony): Bristol Myers Squibb, Gilead Sciences, Johnson and Johnson, Pfizer, Astellas Pharma, AbbVie, Genmab, Chugai-Pharma, Ono Pharma, GlaxoSmithKline, Kite Pharma, Sanofi. Aster Meche: Employment: Pfizer; Stock ownership: Pfizer. Patrick Hlavacek: Employment: Pfizer; Stock Ownership: Pfizer. Guido Nador: Employment: Pfizer; Stock Ownership: Pfizer. Shohei Ikoma: Employment: Pfizer; Stock ownership: Pfizer. Chandra Prakash Yadav: Employment: Pfizer; Stock ownership: Pfizer. Carla AL Assaf: Employment: Pfizer; Stock ownership: Pfizer. Marco DiBonaventura: Employment: Pfizer; Stockholder: Pfizer. Yong Chen: Employment: Pfizer; Stock ownership: Pfizer. Sarasa MA Johnson and Ann-Sophie Demers are employees of Statlog, a paid contractor to Pfizer in connection with the development of this manuscript and data collection and analysis. The authors report no other conflicts of interest in this work.
References
1. Cowan AJ, Allen C, Barac A, et al. Global burden of multiple myeloma: a systematic analysis for the Global Burden of Disease Study 2016. JAMA Oncol. 2018;4(9):1221–9. doi:10.1001/jamaoncol.2018.2128
2. National Cancer Center Cancer Information Service [homepage on the internet]. Multiple Myeloma. Available from: https://ganjoho.jp/aboutus/index.html.
3. Uno S, Midorikawa S, Inoue K, et al. Survival outcomes among patients with multiple myeloma in the era of novel agents: exploratory assessment using an electronic medical record database in Japan. PLoS One. 2023;18(5):e0285947. doi:10.1371/journal.pone.0285947
4. Rajkumar SV. Multiple myeloma: 2024 update on diagnosis, risk-stratification, and management. Am J Hematol. 2024;99(9):1802–1824. doi:10.1002/ajh.27422
5. Pharmaceuticals and Medical Devices Agency [homepage on the internet]. List of Approved Drugs. April 2004 to December 2024. Available from: https://www.pmda.go.jp/files/000274881.pdf.
6. Lesokhin AM, Tomasson MH, Arnulf B, et al. Elranatamab in relapsed or refractory multiple myeloma: phase 2 MagnetisMM-3 trial results. Nat Med. 2023;29(9):2259–2267. doi:10.1038/s41591-023-02528-9
7. Tomasson MH, Iida S, Niesvizky R, et al. Long-term survival and safety of elranatamab in patients with relapsed or refractory multiple myeloma: update from the MagnetisMM-3 study. Hemasphere. 2024;8(7):e136. doi:10.1002/hem3.136
8. Iida S, Ito S, Yokoyama H, et al. Elranatamab in Japanese patients with relapsed/refractory multiple myeloma: results from MagnetisMM-2 and MagnetisMM-3. Jpn J Clin Oncol. 2024;54(9):991–1000. doi:10.1093/jjco/hyae068
9. Elrexfio (elranatamab-bcmm) [package insert]. New York, NY: Pfizer; 2023.
10. Elrexfio (elranatamab) [summary of product characteristics]. European Medicines Agency; 2023.
11. Elrexfio (elranatamab) [package insert]. New York, NY: Pfizer; 2024.
12. Prince HM, Bahlis NJ, Rodriguez-Otero P, et al. MagnetisMM-3: long-term update and efficacy and safety of less frequent dosing of elranatamab in patients with relapsed or refractory multiple myeloma.
13. Bahlis NJ, Costello CL, Raje NS, et al. Elranatamab in relapsed or refractory multiple myeloma: the MagnetisMM-1 Phase 1 trial. Nat Med. 2023;29(10):2570–2576. doi:10.1038/s41591-023-02589-w
14. Banerjee R, Mohan M, Prince HM, et al. ALTITUDE-1: real-world treatment patterns associated with elranatamab among patients with multiple myeloma.
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Holistic View of Autografting Patients by Percentage of Total Body Surface Area Burned: Medical Record Abstraction Integrated with Administrative Claims
Hahn H, Yu TC, Teng CC, Tan H
ClinicoEconomics and Outcomes Research 2023, 15:251-267
Published Date: 8 April 2023
Targeting B Cell Maturation Antigen in Patients with Multiple Myeloma: Current Perspectives
Shrivastava T, Van Rhee F, Al Hadidi S
OncoTargets and Therapy 2023, 16:441-464
Published Date: 20 June 2023
Underdiagnosis of COPD: The Japan COPD Real-World Data Epidemiological (CORE) Study
Koga Y, Deguchi S, Matsuo T, Suzuki A, Terashima G, Tajima T, Shibata Y, Sagara H
International Journal of Chronic Obstructive Pulmonary Disease 2024, 19:1011-1019
Published Date: 7 May 2024
UK Stakeholder Perspectives on Surrogate Endpoints in Cancer, and the Potential for UK Real-World Datasets to Validate Their Use in Decision-Making
Baldwin D, Carmichael J, Cook G, Navani N, Peach J, Slater R, Wheatstone P, Wilkins J, Allen-Delingpole N, Kerr CEP, Siddiqui K
Cancer Management and Research 2024, 16:791-810
Published Date: 12 July 2024
Treatment Patterns, Adverse Events, and Clinical Outcomes with Steroidal Mineralocorticoid Receptor Antagonists: A Retrospective Analysis of Administrative Claims Data (RELICS)
Richard EL, Desai NR, Willey VJ, Gay A, Scott C, Folkerts K, Pessina E, Singh R, Teng CC, Oberprieler NG
Pragmatic and Observational Research 2025, 16:27-37
Published Date: 26 February 2025