Back to Journals » OncoTargets and Therapy » Volume 16
Targeting B Cell Maturation Antigen in Patients with Multiple Myeloma: Current Perspectives
Authors Shrivastava T ![]() , Van Rhee F, Al Hadidi S
, Van Rhee F, Al Hadidi S
Received 16 April 2023
Accepted for publication 15 June 2023
Published 20 June 2023 Volume 2023:16 Pages 441—464
DOI https://doi.org/10.2147/OTT.S370880
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Tohru Yamada
Trilok Shrivastava, Frits Van Rhee, Samer Al Hadidi
Myeloma Center, Winthrop P. Rockefeller Cancer Institute, University of Arkansas for Medical Sciences, Little Rock, AR, USA
Correspondence: Samer Al Hadidi, Myeloma Center, Winthrop P. Rockefeller Cancer Institute, University of Arkansas for Medical Sciences, Little Rock, AR, USA, Email [email protected]
Abstract: Relapsed/refractory multiple myeloma remains a challenging disease necessitating the development of more effective treatment options. In the past decade, myeloma therapies have made significant advancements with the introduction of new treatment modalities. One of the new major targets for these novel therapeutics has been B-cell maturation antigen (BCMA), which is expressed on mature B-lymphocytes and plasma cells. There are three main categories of BCMA-targeted therapies currently available, including bispecific antibodies (BsAbs), antibody drug conjugates (ADCs), and chimeric antigen receptor (CAR) T-cell therapies. In this review, we discuss the existing BCMA-targeted therapies and provide insights into currently available treatment and future developments, with a particular focus on clinical efficacy and common drug-related adverse events.
Keywords: BCMA, multiple myeloma, bispecific antibody, BiTE, CAR T cells, B-cell maturation antigen
Introduction
Multiple myeloma (MM) is a clonal proliferation of plasma cells, which arises from B lymphocytes.1,2 MM accounts for nearly 2% of all cancers and cancer-related deaths with the 5-year relative survival rate of 58%.3 Although clinical outcomes have improved over the last decade, the prognosis for patients with high-risk disease or relapsed/refractory (R/R) disease remains poor, highlighting the need for newer treatment approaches.4–6 Many potential targets in MM have been identified which includes CD24, CD38, CD56, CD138, signaling lymphocytic activation molecule family member 7 (SLAMF7), programmed cell death-ligand 1 (PD-L1).7–10 However, many normal cells also express these receptors on their surface raising the possibility for systemic adverse reactions, while others have failed to show response in clinical trials.11–13 There are other novel targets such as G protein-coupled receptor class C, group 5, member D (GPRC5D) and integrin β7 with targeted agents under investigation.14–17 One promising target in the treatment of MM is B-cell maturation antigen (BCMA), which is specifically expressed on mature B-lymphocytes and plasma cells, but not in other normal cells.18–20 In this review, we discuss the rationale behind targeting BCMA and the available BCMA-targeted therapies.
Rationale of BCMA
BCMA, also known as TNFRSF17 or CD269, is a transmembrane glycoprotein and a member of the tumor necrosis factor (TNF) receptor family. It is expressed on mature B-lymphocytes and is overexpressed on malignant plasma cells. Activation of BCMA leads to the survival of plasma cells, and it serves as a binding site for a proliferation-inducing ligand (APRIL) and B cell activating factor of the TNF family (BAFF), which are crucial for normal B-cell and plasma cell development (Figure 1).21–23
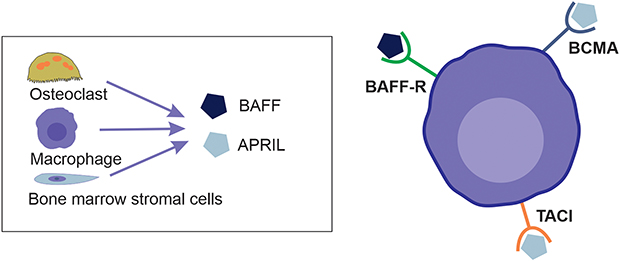 |
Figure 1 Myeloma cell with its receptors and substrates – BAFF and April which are mainly produced by osteoclast, macrophages and bone marrow stromal cells. |
APRIL has a higher affinity for BCMA compared to BAFF, and binding of APRIL or BAFF to BCMA triggers downstream gene expressions that play a significant role in the pathogenesis of MM23,24 Soluble BCMA (sBCMA) levels have been shown to be elevated in patients with MM and correlate with the proportion of plasma cells in bone marrow biopsies in MM patients. Elevated sBCMA also carries prognostic implications in monoclonal gammopathy of undetermined significance (MGUS) and smoldering multiple myeloma.25,26 In patients with MM, increased sBCMA levels prevent circulating BAFF from performing its normal signaling and impairs B-cell development, resulting in lower polyclonal antibody levels.27
Currently, there are three main categories of targeted therapies for BCMA, including bispecific antibodies (BsAbs), antibody-drug conjugates (ADCs), and chimeric antigen receptor modified T-cell (CAR-T) therapy.
Antibody-Drug Conjugates (ADCs)
Antibody-drug conjugates (ADCs) consist of a monoclonal antibody that is directed towards a specific antigen on tumor cells and a cytotoxic payload that is connected to the antibody by a chemical linker. (Figure 2) ADCs are associated with reduced systemic toxicity compared to other classes of drugs due to their tumor cell-specific targeting.28
 |
Figure 2 ADC binds to BCMA receptor in myeloma cell and gets internalized forming an endosome (yellow dotted circle) releasing toxic payload that leads to myeloma cell death. |
Belantamab mafodotin is a humanized IgG1 monoclonal antibody targeting BCMA, which is conjugated to a tubulin polymerization inhibitor known as monomethyl auristatin-F (MMAF or mafodotin) via a maleimidocaproyl (MC) linker that is resistant to proteolysis. Once the ADC attaches to the cell surface, it is internalized, and the active components are released, leading to antibody-mediated cytotoxicity and subsequent cell death.29 Belantamab mafodotin was granted accelerated FDA approval in 2020 based on the DREAMM-2 study (NCT03525678) for the treatment of patients with R/R MM who had received at least three prior myeloma-directed therapies. However, it was withdrawn from the market in November 2022 due to results from the Phase III confirmatory trial, DREAMM-3 (NCT04162210), which showed that Belantamab mafodotin did not demonstrate superiority in progression-free survival (PFS) compared to pomalidomide and low-dose dexamethasone.30–32 Additionally, high-grade keratopathy was a common adverse event (AE), with grade 3 keratopathy occurring in 54% of patients, which can be a limiting factor in delivering therapy.33 It is currently only available through an expanded access protocol.34
Bispecific Antibodies
Bispecific antibodies (BsAbs) are unique molecules that can bind to two separate epitopes or antigens simultaneously. In the context of MM, commonly selected target-binding epitopes for BsAbs are BCMA on myeloma cells and CD3 receptor on T cells. (Figure 3) When the target is the CD3 receptor on T cells, these BsAbs are commonly referred to as bispecific T-cell engagers (BiTE).35,36 (Figure 2) However, there are many other potential target sites, including GPRC5D, Fc receptor-homolog 5 (FcRH5), CD138, CD38, SLAMF7 on myeloma cells, as well as natural killer group 2 D (NKG2D), CD16A, and natural cytotoxicity receptor 3 (NKp30) on natural killer (NK) cells and T cells.14,37–44 BsAbs form a cross-linkage between myeloma cells and T cells upon binding to their respective receptors. This interaction activates CD4+/CD8+ T cells which releases perforin, granzyme, and interferon-γ, resulting in lysis of myeloma cells.45
 |
Figure 3 Bispecific antibody forms cross linkage with CD3 in T cell and BCMA receptor in myeloma cell that leads to activation of CD4+/CD8+ T-cell and release of cytotoxic cytokines ultimately causing myeloma cell death. |
Teclistamab
Teclistamab is a humanized IgG4 BsAb that specifically targets BCMA on myeloma cells and CD3 receptor on T cells.30 It is the only FDA approved BsAb for relapsed/refractory (R/R) MM, based on the results of the MajesTEC-1 study (NCT04557098).46,47 This multicohort phase I/II trial enrolled 165 patients, including more than two-thirds of patients with triple-class refractory disease, who received weekly subcutaneous teclistamab. At a median follow-up of approximately 14 months, the overall response rate (ORR) was 63%, with 19.4% patients achieving very good partial response (VGPR), 32.7% stringent complete response (sCR), 6.7% complete response (CR). About one-fourth (44/165) of patients had negative minimal residual disease (MRD) assessed by next-generation sequencing with a threshold of 10−5 cells. Median duration of response (DOR) was about 18 months and median duration of progression-free survival (PFS) was 11.3 months.47
Cytokine release syndrome (CRS) occurred in 72.1% of patients, with grade 1 CRS in 50.3% of patients, grade 2 in 21.2%, and grade 3 or higher in 0.6% of patients. Neurotoxicity occurred in 24% of patients, with only 1% experiencing grade 3 or higher neurotoxicity.
Teclistamab and other BCMA targeting agents also target normal plasma cells, which can result in profound hypogammaglobulinemia increasing the risk of infections.48–50 In the MajesTEC-1 study, infections were reported in 76.4% of patients, with COVID-19 occurring in 17.6% of patients, pneumonia in 18.2%, bronchitis in 13.3%, cellulitis in 2.4%, and pneumocystis jirovecii (PJP) pneumonia in 3.6% of patients. There were also 41.2% reported deaths, with 24.8% attributed to progressive disease and 11.5% due to infections.
Cytopenias were also commonly observed, with neutropenia being the most frequent (all grade neutropenia in 70.9% of patients, with grade 3 neutropenia in 64.2%), anemia occurring in 52.1% of patients, and thrombocytopenia in 40% of patients.47
Based on these results, teclistamab appears to be a promising agent awaiting long-term outcomes and the results of future randomized clinical trials.
Elranatamab
Elranatamab (PF-06863135) is a BsAb that has received “breakthrough therapy” designation from the United States Food and Drug Administration (FDA), based on the results of the Phase II MagnetisMM-3 study (NCT04649359).51–53 In this open-label, multicenter, single-arm trial, 123 patients received subcutaneous elranatamab weekly with a 2-step-up priming dose regimen. At a median follow-up of 6.8 months, patients achieved an ORR of 61%, with more than half achieving CR or better. Median time to response was noted to be 36 days.
Incidences of grade 1 and 2 CRS were reported in 71% of patients, with no events of grade 3 or higher CRS reported. Neurotoxicity was observed in 3.4%, all of which were either grade 1 or grade 2. Infections were reported in about 62% of patients, with upper respiratory tract infections occurring in 14.6% and pneumonia in 10.6%.
Peripheral neuropathy was reported in 17.1% of patients, with peripheral sensory neuropathy (4.9%), paresthesia (4.1%), and gait disturbance (2.4%) being the most common manifestations.54
Considering the risks and responses observed in the trial, elranatamab shows promise as a potential addition to the armamentarium of BsAbs, pending complete data from the phase II trial.
Linvoseltamab (REGN5458)
Linvoseltamab, a BCMAxCD3 BsAb, is currently in development and being studied in the LINKER-MM2 trial (NCT05137054). Phase 1/2 data from this trial involving 167 recruited patients showed that linvoseltamab achieved an ORR of 75% at doses greater than or equal to 200mg, with 37.5% of patients achieving CR or better. The most common AEs were CRS with an overall incidence of 47.9% (grade 1: 36.5%, grade 2: 10.8%, and grade 3: 0.6%), anemia (36.5%), fatigue (34.1%), neutropenia (28.7%), and thrombocytopenia (16.2%).55–57 The trial is currently ongoing and is also being explored for potential benefits in combination with other anti-myeloma therapies.58
Pavurutamab (AMG701)
Pavurutamab is currently being evaluated in the phase 1/2 ParadigMM-1B trial (NCT03287908) to assess its efficacy as monotherapy or in combination with pomalidomide in patients with R/R MM.59 According to preliminary results from the first in-human study, out of 75 patients treated for a median duration of approximately 6 weeks, the ORR was 36%. However, in 6 patients who received earlier dose escalation, the ORR was as high as 83%, among which 33.3% were VGPR and 50% were partial response (PR). The most common non-hematological AEs included CRS in 61% of patients, mostly grade 1 and grade 2 (53%), with grade 3 CRS occurring in 7% of patients. Hematological AEs included anemia (43%), neutropenia (23%), and thrombocytopenia (20%). Infections were reported in 13% of patients.60
Alnuctamab (CC-93269)
Alnuctamab (ALNUC; BMS-986349; CC-93269) is a humanized IgG antibody with bivalent affinity for BCMA and monovalent affinity for CD3.61 In the first in-human study involving 70 patients (NCT03486067) treated with alnuctamab in a dose-escalation fashion, the ORR was 39%. Among the 10 patients who received a targeted escalated dose of ≥30mg, the ORR was 77%, that included 23% sCR/CR, 8% VGPR, and 46% PR. The median time to response was 4.3 weeks. Common AEs included CRS in 53% of patients, all limited to grade 1 or grade 2. Grade 1 neurotoxicity was observed in only one patient. Neutropenia was reported in 34% patients and anemia in 34%.61,62 Alnuctamab continues to be evaluated in a Phase I trial, which is expected to be completed in 2027.63
ABBV-383
ABBV-383, previously known as TNB-383SB, is a BCMA x CD3 T-cell engaging BsAb currently in development (NCT03933735) with promising early results.64 In a phase I study, 124 patients, who received ABBV-383 every 3 weeks, the ORR was 57%, out of which 43% was VGPR or better. However, when stratified to the dose escalation group, with patients receiving the drug at 40mg, the ORR increased to 83% with 67% achieving CR or better and 83% achieving VGPR or better. Among 58 patients in 60 mg dose escalation and expansion group, ORR was 60% with 29% CR or better and 43% VGPR or better.
CRS occurred in 83% of patients in the 40 mg group (with 0% classified as grade 2 or above), and in 72% of patients in the 60 mg group (with 2% classified as grade 2 or above). Infections were reported in 50% of patients in the 40mg cohort and 43% in the 60 mg cohort. Neutropenia (67%) and anemia (33%) were other common AEs reported.65,66
BsAbs have emerged as an important treatment modality for patients with R/R MM, showing promising responses. Teclistamab is currently the only commercially available BsAb for MM treatment, while others are still in early development. Additionally, there are ongoing studies exploring the use of BsAbs in combination with other anti-myeloma agents, although this approach may be associated with an increased risk of infections.49,58,67,68 Table 1 provides a summary of BsAbs.
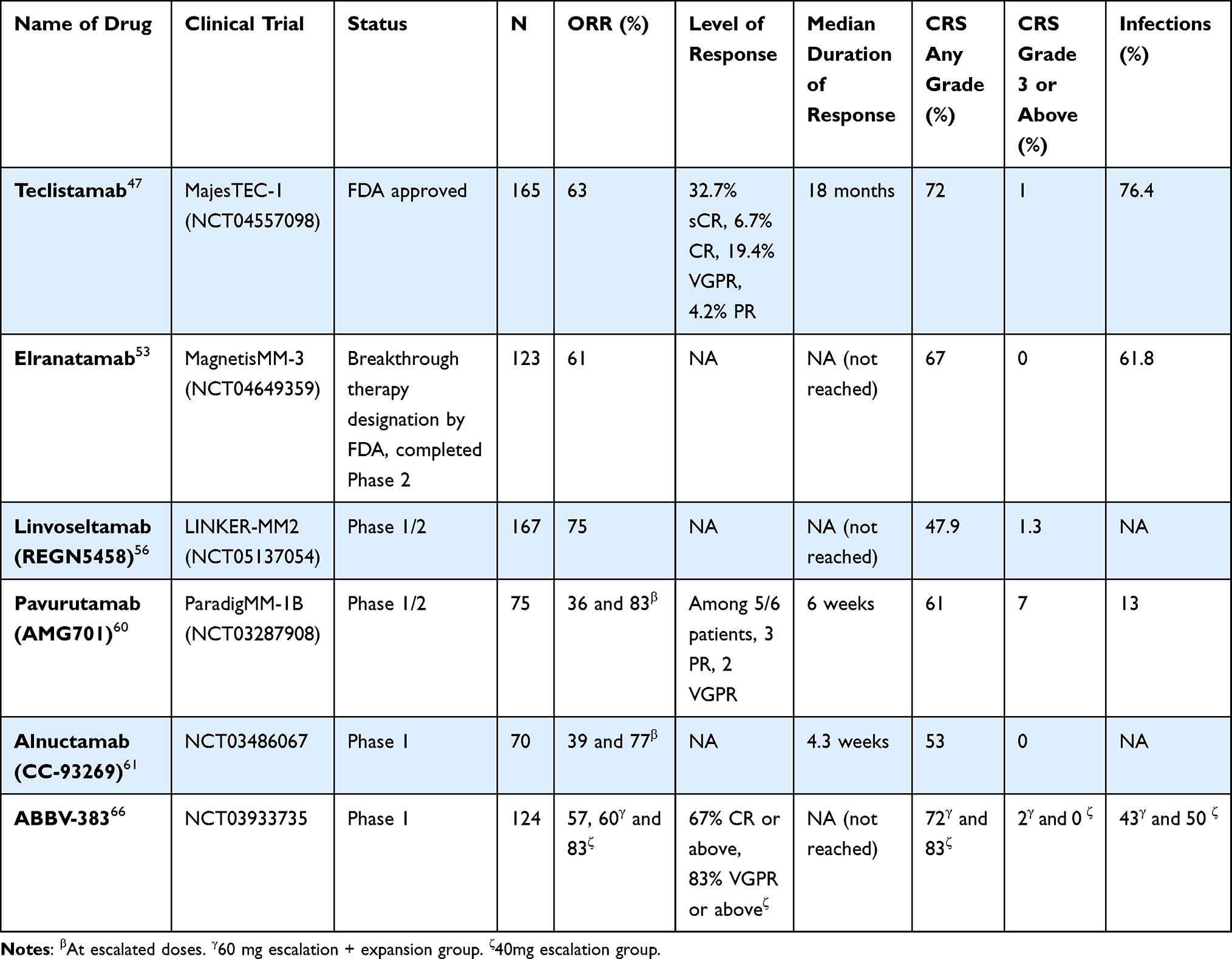 |
Table 1 Summary of Bispecific Antibodies in Clinical Trials |
CAR-T Therapy
CAR-T cells are engineered to recognize and bind tumor antigens without the need for major histocompatibility complex (MHC)-mediated antigen presentation, leading to cytokine release, cytotoxicity, and tumor lysis. This process is illustrated in Figure 4.69
 |
Figure 4 Signaling domain on CAR T cell binds to BCMA receptor on myeloma cell surface which leads to activation of CAR T cells and release of cytotoxic cytokines leading to myeloma cell lysis and death. Abbreviations: BAFF, B cell-activating factor of the TNF family; BAFF-R, BAFF Receptor; BCMA, B cell maturation receptor; TACI, Transmembrane activator; APRIL, A proliferation-inducting ligand. |
The first-in-human clinical trial that studied BCMA-targeting CAR-T cells took place in 2018, using γ-retrovirus as a vector to encode CAR-BCMA for transduction into T cells.70 The manufacturing process of CAR T cells begins with autologous leukapheresis to obtain peripheral blood mononuclear cells, which are then sorted using magnetic cell sorting kits to enrich for CD3+ T lymphocytes. These T cells are then genetically modified using an inactivated lentivirus/retrovirus or a non-viral DNA modification system to introduce the CARs, followed by immunophenotyping, in-vitro expansion, formulation, and cryopreservation before infusion.71–73
Currently, there are several BCMA CAR-T therapies in development, but only idecabtagene vicleucel (ide-cel) and ciltacabtagene autoleucel (cilta-cel) have received FDA approval for the treatment of R/R MM (Table 2).74,75
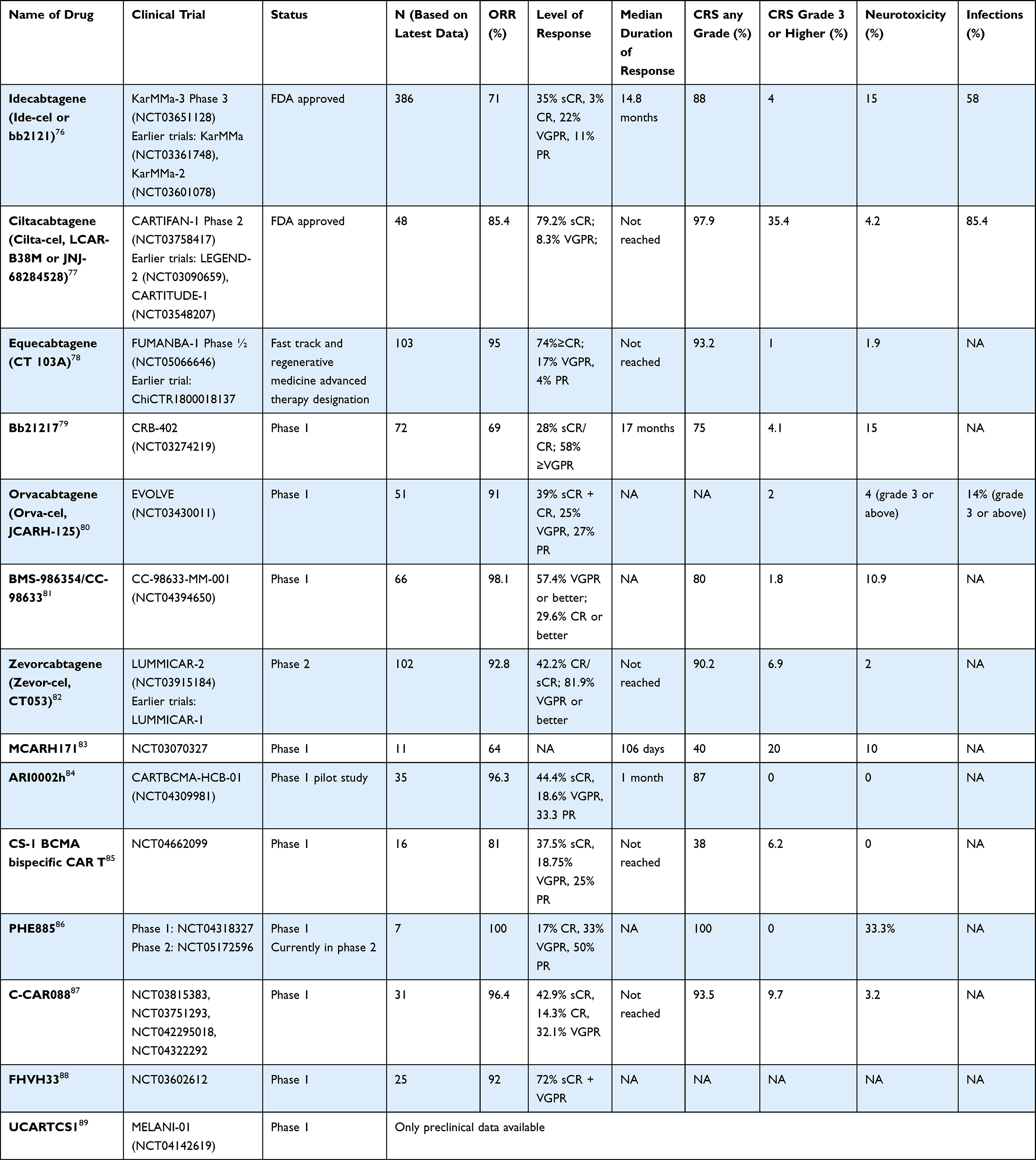 |
Table 2 Summary of CAR-T Cell Therapies in Clinical Trials |
Idecabtagene Vicleucel
Idecabtagene vicleucel, also known as ide-cel or bb2121, demonstrated promising interim results in its phase 1 study (NCT02658929) with an ORR of 85% in 33 patients and a median DOR of 10.9 months. In the phase 2 KarMMA study (NCT03601078), which reported results on 128 out of 140 enrolled patients, ide-cel showed an ORR of 73%. The median PFS was 8.8 months with median DOR of 10.7 months.90,91
Recently published results from KarMMA-3 (NCT03651128), involving 386 patients from 12 countries, compared ide-cel to variable regimens in patients with triple-class-refractory (66%) or daratumumab-refractory (95%) MM. Both groups had similar distribution of Eastern Cooperative Oncology Group (ECOG) score, tumor burden, extramedullary disease, high-risk cytogenetics, and previous class exposures. Median follow-up duration was 18.6 months. In the ide-cel group, 71% of patients achieved an OR, with 35% sCR, 3% CR, 22% VGPR and 11% PR. MRD negativity was 20% (51/254) in the ide-cel group within 3 months, compared to 1/132 in the standard regimen group. Median DOR was 14.8 months, and PFS was 13.3 months in the ide-cel group, compared to 4.4 months in the standard regimen group. Common non-hematological AEs included CRS in 88% of patients, with 4% experiencing grade 3 or higher CRS, and neurotoxicity in 15% of patients, with 3% experiencing grade 3 or higher neurotoxicity. The most common hematological AEs were neutropenia (90%), anemia (66%), and thrombocytopenia (54%). Infections occurred in 58% of patients, with upper respiratory tract infection being the most common (12%) and pneumonia following thereafter (10%).76 It is important to note that higher percentage of grade V all cause event occurred in the ide-cel group (14% vs 6%). Moreover grade III/IV neutropenia in patients treated with ide-cel was high at 76% with a median time to recover of 1.7 months.
Health-related quality of life was assessed using standardized questionnaires in patients enrolled in the KarMMA trial, and those who received ide-cel showed improvement in pain, physical functioning, fatigue, and overall quality of life lasting for 15–18 months.92
Ciltacabtagene Autoleucel
Ciltacabtagene autoleucel or cilta-cel (previously known as LCAR-B38M or JNJ-68284528) was first evaluated in the LEGEND-2 multicenter study in China (NCT03090659) in 57 patients. ORR was 88% with 68% achieving CR, 5% VGPR and 14% PR. MRD negativity was achieved in 63% patients. Median PFS was 15 months. Ninety percent patients experienced CRS with 7% having grade 3 or higher CRS. Others common AEs were leukopenia (30%), thrombocytopenia (23%).93–95 A four-year follow-up data to this study was published in 2022 with 74 patients which showed a median PFS to 18 months with median duration of response of 23.3 months.96 After promising results from the LEGEND-2 study, cilta-cel was further studied in CARTITUDE-1 phase 1b/2 study (NCT03548207) done in 113 patients from 16 USA centers. Patients received a single cilta-cel infusion at a target dose of 0.75×106 CAR T cells/kg and followed up at a median duration of 12.5 months. ORR was at a striking 97% among which 67% had achieved sCR with time-to-first response being 1 month. Twelve-month PFS was 77% and overall survival rate was 89%. CRS occurred in 95% patients with 4% being grade 3 or higher. The median time to onset of CRS was 7 days. ICANS occurred in 21% patients where 9% were grade 3 or higher. BCMA agents have also shown to cause delayed movement disorders and parkinsonian features.97,98 In the CARTITUDE-1 trial, late neurotoxicity was reported in 12% and parkinsonism in 4% patients. There were 14 mortalities, 6 of which was attributed to treatment-related AEs. In terms of hematological AEs, neutropenia was the most common (95%), followed by anemia (68%), leukopenia (60%) and thrombocytopenia (60%). Infections occurred in 58% patients.99 A follow-up study was conducted to above study which showed slightly better ORR at 97.9% with 82.5% achieving sCR. PFS at 27-month was 54.9% and OS was 70.4%.100
A phase-2 study is ongoing in China, called CARTIFAN-1 (NCT03758417) and data from 48 patients were published at a median follow-up of 26.4 months, that shows an ORR of 85.4%. 79.2% patients achieved sCR and MRD negativity of 40%. PFS & OS rates were 52.6% and 74.2% in 24-months respectively. Again, CRS occurred in most patients (97.9%) out of which 35.4% were grade 3 or higher. Neurotoxicity occurred in 4.2%, infections occurred in 85.4% patients, 37.5% were grade 3 or higher. There were 12 reported deaths, out of which 8 were attributed as treatment related.77,101,102
CAR-T cell therapies show promising outcomes, but comes at a cost of increased CRS, neurotoxicity and prolonged cytopenias, which may require stem cell boost. Besides, availability of treatment is limited, and there is also a component of disparity in access to treatment.103 Therefore, patients can clinically decline awaiting treatment given the length of wait time.104
Mechanisms of BCMA Resistance
Both antigen and T-cell related mechanisms are responsible for resistance to BCMA treatment. T-cell mediated processes leading to BCMA-treatment resistance are T-cell senescence/exhaustion and development of immunosuppressive bone marrow microenvironment.105 T-cell exhaustion and senescence are the primary mechanisms for BCMA resistance and refer to loss of cytokine producing and proliferating abilities respectively, which would otherwise play key roles in tumor lysis.105
One of the antigen-related mechanisms is antigen escape, that occurs because of dysregulated expression of MHC or changes in tumor-associated antigen epitopes.106 Dual-targeting BCMA with another antigen has shown to prevent antigen escape-related relapse.107,108 BCMA shedding from plasma cells driven by γ-secretase results in circulation of sBCMA, that can potentially lead to masking of antigen.109 The third antigen-dependent process is the development of anti-scFv antibodies, which was more common with non-human scFv.110 Use of humanized scFv has been shown to reduce production of anti-scFv antibodies, decreasing the risk for resistance.109
Future Directions
Allogeneic BCMA-targeted CAR T cells are being studied to address the logistical challenges with autologous CAR-T, that largely limits its access. UNIVERSAL is a phase 1, first-in-human trial of ALLO-715 (NCT04093596) used in escalating doses with an anti-CD52 antibody ALLO-647. ALLO-715 is an allogeneic CAR-T therapy comprising a second-generation anti-BCMA CAR containing humanized scFv and intracellular domains of 4–1BB and CD3ζ. T cell receptor alpha constant (TRAC) is knocked out of in this that reduces the risk of graft-versus-host disease (GVHD). Based on interim results of 48 patients with relapsed/refractory MM, 70.8% patients had a response with 45.8% VGPR or better and 25% with CR or sCR. Median duration of response was 8.4 months. CRS occurred in 55.8% patients with grade 3 or move in 2.3%, neurotoxicity was observed in 14% patients with no grade 3 or more events. Infections occurred in 53.5% patients with 23.3% above grade 3. No cases of GVHD were reported.111
Bispecific CAR-T has been studied using BCMA & CD24 CARs which showed both in-vitro and in-vivo cytotoxic activity against myeloma warranting further studies.10 Similarly, anti-BCMA CAR-NK cells are being studied in pre-clinical phase in different models, with good results and may possess a place in the BCMA therapeutics shelf in the future.112,113
Currently, BCMA directed therapies are only available for R/R MM patients, but many trials are underway to explore their role at earlier stages and in combination with other myeloma therapies and in patients with high-risk disease (Table 3).
 |
Table 3 Ongoing Trials in BCMA |
Conclusion
BCMA targeted therapy remains the core of treatment for R/R MM with new available agents and many in development that have shown encouraging results. Teclistamab, ide-cel and cilta-cel are the currently FDA approved agents with some in queue for approval. Overall, these add significantly to the treatment arsenal for patients with R/R MM. Other non-BCMA targeted therapies, particularly GPRC5D has shown good results in early clinical trials, but data to compare them with anti-BCMA agents is lacking.
Disclosure
The authors report no competing interests in this work.
References
1. Mahindra A, Hideshima T, Anderson KC. Multiple myeloma: biology of the disease. Blood Rev. 2010;24:S5–S11. doi:10.1016/S0268-960X(10)70003-5
2. Palumbo A, Anderson K. Multiple myeloma. N Engl J Med. 2011;364(11):1046–1060. doi:10.1056/NEJMra1011442
3. Seer.cancer.gov. Cancer stat facts: myeloma; 2022. Available from: https://seer.cancer.gov/statfacts/html/mulmy.html.
4. Barlogie B, Mitchell A, van Rhee F, Epstein J, Morgan GJ, Crowley J. Curing myeloma at last: defining criteria and providing the evidence. Blood. 2014;124(20):3043–3051. doi:10.1182/blood-2014-07-552059
5. Nishimura KK, Barlogie B, van Rhee F, et al. Long-term outcomes after autologous stem cell transplantation for multiple myeloma. Blood Adv. 2020;4(2):422–431. doi:10.1182/bloodadvances.2019000524
6. Rasche L, Weinhold N, Morgan GJ, van Rhee F, Davies FE. Immunologic approaches for the treatment of multiple myeloma. Cancer Treat Rev. 2017;55:190–199. doi:10.1016/j.ctrv.2017.03.010
7. Tai Y-T, Dillon M, Song W, et al. Anti-CS1 humanized monoclonal antibody HuLuc63 inhibits myeloma cell adhesion and induces antibody-dependent cellular cytotoxicity in the bone marrow milieu. Blood. 2008;112(4):1329–1337. doi:10.1182/blood-2007-08-107292
8. Görgün G, Samur MK, Cowens KB, et al. Lenalidomide enhances immune checkpoint blockade-induced immune response in multiple myeloma. Clin Cancer Res. 2015;21(20):4607–4618. doi:10.1158/1078-0432.CCR-15-0200
9. Nijhof IS, Groen RWJ, Lokhorst HM, et al. Upregulation of CD38 expression on multiple myeloma cells by all-trans retinoic acid improves the efficacy of daratumumab. Leukemia. 2015;29(10):2039–2049. doi:10.1038/leu.2015.123
10. Sun F, Cheng Y, Peng B, et al. Bispecific CAR-T cells targeting both BCMA and CD24: a potentially treatment approach for multiple myeloma. Blood. 2021;138(Supplement 1):2802. doi:10.1182/blood-2021-148543
11. Lesokhin AM, Ansell SM, Armand P, et al. Nivolumab in patients with relapsed or refractory hematologic malignancy: preliminary results of a phase Ib study. J Clin Oncol. 2016;34(23):2698–2704. doi:10.1200/JCO.2015.65.9789
12. Drent E, Groen RWJ, Noort WA, et al. Pre-clinical evaluation of CD38 chimeric antigen receptor engineered T cells for the treatment of multiple myeloma. Haematologica. 2016;101(5):616–625. doi:10.3324/haematol.2015.137620
13. Gogishvili T, Danhof S, Prommersberger S, et al. SLAMF7-CAR T cells eliminate myeloma and confer selective fratricide of SLAMF7+ normal lymphocytes. Blood. 2017;130(26):2838–2847. doi:10.1182/blood-2017-04-778423
14. Smith EL, Harrington K, Staehr M, et al. GPRC5D is a target for the immunotherapy of multiple myeloma with rationally designed CAR T cells. Sci Transl Med. 2019;11(485):eaau7746. doi:10.1126/scitranslmed.aau7746
15. Mailankody S, Devlin SM, Landa J, et al. GPRC5D-targeted CAR T cells for myeloma. N Engl J Med. 2022;387(13):1196–1206. doi:10.1056/NEJMoa2209900
16. Roy Choudhury S, Byrum SD, Alkam D, et al. Expression of integrin β-7 is epigenetically enhanced in multiple myeloma subgroups with high-risk cytogenetics. Clin Epigenetics. 2023;15(1):18. doi:10.1186/s13148-023-01433-9
17. Hosen N, Matsunaga Y, Hasegawa K, et al. The activated conformation of integrin β7 is a novel multiple myeloma–specific target for CAR T cell therapy. Nat Med. 2017;23(12):1436–1443. doi:10.1038/nm.4431
18. Tai Y-T, Mayes PA, Acharya C, et al. Novel anti–B-cell maturation antigen antibody-drug conjugate (GSK2857916) selectively induces killing of multiple myeloma. Blood. 2014;123(20):3128–3138. doi:10.1182/blood-2013-10-535088
19. Carpenter RO, Evbuomwan MO, Pittaluga S, et al. B-cell maturation antigen is a promising target for adoptive T-cell therapy of multiple myeloma. Clin Cancer Res. 2013;19(8):2048–2060. doi:10.1158/1078-0432.CCR-12-2422
20. Tai Y-T, Acharya C, An G, et al. April and BCMA promote human multiple myeloma growth and immunosuppression in the bone marrow microenvironment. Blood. 2016;127(25):3225–3236. doi:10.1182/blood-2016-01-691162
21. O’Connor BP, Raman VS, Erickson LD, et al. BCMA is essential for the survival of long-lived bone marrow plasma cells. J Exp Med. 2004;199(1):91–98. doi:10.1084/jem.20031330
22. Bossen C, Schneider P. BAFF, April and their receptors: structure, function and signaling. Semin Immunol. 2006;18(5):263–275. doi:10.1016/j.smim.2006.04.006
23. Tai Y-T, Anderson KC. B cell maturation antigen (BCMA)-based immunotherapy for multiple myeloma. Expert Opin Biol Ther. 2019;19(11):1143–1156. doi:10.1080/14712598.2019.1641196
24. Day ES, Cachero TG, Qian F, et al. Selectivity of BAFF/BLyS and April for binding to the TNF family receptors BAFFR/BR3 and BCMA. Biochemistry. 2005;44(6):1919–1931. doi:10.1021/bi048227k
25. Ghermezi M, Li M, Vardanyan S, et al. Serum B-cell maturation antigen: a novel biomarker to predict outcomes for multiple myeloma patients. Haematologica. 2017;102(4):785–795. doi:10.3324/haematol.2016.150896
26. Dispenzieri A, Soof CM, Rajkumar SV, et al. Serum BCMA levels to predict outcomes for patients with MGUS and smoldering multiple myeloma (SMM). Clin Lymphoma Myeloma Leuk. 2019;37(15_suppl):8020.
27. Sanchez E, Gillespie A, Tang G, et al. Soluble B-cell maturation antigen mediates tumor-induced immune deficiency in multiple myeloma. Clin Cancer Res. 2016;22(13):3383–3397. doi:10.1158/1078-0432.CCR-15-2224
28. Khongorzul P, Ling CJ, Khan FU, Ihsan AU, Zhang J. Antibody–drug conjugates: a comprehensive review. Mol Cancer Res. 2020;18(1):3–19. doi:10.1158/1541-7786.MCR-19-0582
29. Trudel S, Lendvai N, Popat R, et al. Targeting B-cell maturation antigen with GSK2857916 antibody–drug conjugate in relapsed or refractory multiple myeloma (BMA117159): a dose escalation and expansion phase 1 trial. Lancet Oncol. 2018;19(12):1641–1653. doi:10.1016/S1470-2045(18)30576-X
30. GSK. GSK provides update on DREAMM-3 phase III trial for blenrep in relapsed/refractory multiple myeloma; 2022. Available from: https://www.gsk.com/en-gb/media/press-releases/gsk-provides-update-on-dreamm-3-phase-iii-trial-for-blenrep/.
31. Administration USFD. FDA granted accelerated approval to belantamab mafodotin-blmf for multiple myeloma; 2020. Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-granted-accelerated-approval-belantamab-mafodotin-blmf-multiple-myeloma.
32. Lonial S, Lee HC, Badros A, et al. Belantamab mafodotin for relapsed or refractory multiple myeloma (DREAMM-2): a two-arm, randomised, open-label, phase 2 study. Lancet Oncol. 2020;21(2):207–221. doi:10.1016/S1470-2045(19)30788-0
33. Mohan M, Rein LE, Thalambedu N, et al. Corneal toxicity with belantamab mafodotin: multi-institutional real-life experience. Am J Hematol. 2022;97(12):E451–E453. doi:10.1002/ajh.26728
34. Compassionate use individual request program for belantamab mafodotin in multiple myeloma 213304: expanded access program for belantamab mafodotin in patients with relapsed/refractory multiple myeloma who are refractory to a proteasome inhibitor, and an immunomodulatory agent, and an anti-CD38 antibody. Available from: https://navigator.reaganudall.org/expanded-access/expanded-access-request-program-belantamab-mafodotin-gsk2857916-multiple-myeloma.
35. Labrijn AF, Janmaat ML, Reichert JM, Parren PWHI. Bispecific antibodies: a mechanistic review of the pipeline. Nat Rev Drug Discov. 2019;18(8):585–608. doi:10.1038/s41573-019-0028-1
36. Lancman G, Sastow DL, Cho HJ, et al. Bispecific antibodies in multiple myeloma: present and future. Blood Cancer Discovery. 2021;2(5):423–433. doi:10.1158/2643-3230.BCD-21-0028
37. Elkins K, Zheng B, Go M, et al. FcRL5 as a target of antibody-drug conjugates for the treatment of multiple myeloma. Mol Cancer Ther. 2012;11(10):2222–2232. doi:10.1158/1535-7163.MCT-12-0087
38. Lokhorst HM, Plesner T, Laubach JP, et al. Targeting CD38 with daratumumab monotherapy in multiple myeloma. N Engl J Med. 2015;373(13):1207–1219. doi:10.1056/NEJMoa1506348
39. Watkins-Yoon J, Guzman W, Oliphant A, et al. CTX-8573, an innate-cell engager targeting BCMA, is a highly potent multispecific antibody for the treatment of multiple myeloma. Blood. 2019;134(Supplement_1):3182. doi:10.1182/blood-2019-128749
40. Wu L, Seung E, Xu L, et al. Trispecific antibodies enhance the therapeutic efficacy of tumor-directed T cells through T cell receptor co-stimulation. Nat Cancer. 2019;1(1):86–98. doi:10.1038/s43018-019-0004-z
41. Gantke T, Reusch U, Kellner C, et al. AFM26 is a novel, highly potent BCMA/CD16A-directed bispecific antibody for high affinity NK-cell engagement in multiple myeloma. J Clin Oncol. 2017;35(15_suppl):8045.
42. Chen D, Zou J, Zong Y, Meng H, An G, Yang L. Anti-human CD138 monoclonal antibodies and their bispecific formats: generation and characterization. Immunopharmacol Immunotoxicol. 2016;38(3):175–183. doi:10.3109/08923973.2016.1153110
43. Kodama T, Kochi Y, Nakai W, et al. Anti-GPRC5D/CD3 bispecific T-cell–redirecting antibody for the treatment of multiple myeloma. Mol Cancer Ther. 2019;18(9):1555–1564. doi:10.1158/1535-7163.MCT-18-1216
44. Chari A, Minnema MC, Berdeja JG, et al. Talquetamab, a T-cell–redirecting GPRC5D bispecific antibody for multiple myeloma. N Engl J Med. 2022;387(24):2232–2244. doi:10.1056/NEJMoa2204591
45. Suurs FV, Lub-de Hooge MN, de Vries EGE, de Groot DJA. A review of bispecific antibodies and antibody constructs in oncology and clinical challenges. Pharmacol Ther. 2019;201:103–119. doi:10.1016/j.pharmthera.2019.04.006
46. FDA approves teclistamab-cqyv for relapsed or refractory multiple myeloma. Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-teclistamab-cqyv-relapsed-or-refractory-multiple-myeloma.
47. Moreau P, Garfall AL, van de Donk NWCJ, et al. Teclistamab in relapsed or refractory multiple myeloma. N Engl J Med. 2022;387(6):495–505. doi:10.1056/NEJMoa2203478
48. Morelli T, Fujita K, Redelman-Sidi G, Elkington PT. Infections due to dysregulated immunity: an emerging complication of cancer immunotherapy. Thorax. 2022;77(3):304–311. doi:10.1136/thoraxjnl-2021-217260
49. Mazahreh F, Mazahreh L, Schinke C, et al. Risk of infections associated with the use of bispecific antibodies in multiple myeloma: a pooled analysis. Blood Adv. 2023. doi:10.1182/bloodadvances.2022009435
50. Guido Lancman KP, Rodriguez C, Richter J, et al. Infections and severe hypogammaglobulinemia in multiple myeloma patients treated with anti-BCMA bispecific antibodies; 2022. Available from: https://ash.confex.com/ash/2022/webprogram/Paper163733.html.
51. MagnetisMM-3: study of elranatamab (PF-06863135) monotherapy in participants with multiple myeloma who are refractory to at least one PI, One IMiD and one anti-CD38 mAb. Available from: https://clinicaltrials.gov/ct2/show/NCT04649359.
52. Pfizer’s elranatamab granted FDA breakthrough therapy designation for relapsed or refractory multiple myeloma. Available from: https://www.pfizer.com/news/press-release/press-release-detail/pfizers-elranatamab-granted-fda-breakthrough-therapy.
53. Raje N, Bahlis NJ, Costello C, et al. Elranatamab, a BCMA targeted T-cell engaging bispecific antibody, induces durable clinical and molecular responses for patients with relapsed or refractory multiple myeloma. Blood. 2022;140(Supplement 1):388–390. doi:10.1182/blood-2022-166494
54. 159 efficacy and safety of elranatamab in patients with relapsed/refractory multiple myeloma naïve to B-Cell Maturation Antigen (BCMA)-directed therapies: results from cohort a of the magnetismm-3 study; 2022. Available from: https://ash.confex.com/ash/2022/webprogram/Paper162440.html.
55. Cooper D, Madduri D, Lentzsch S, et al. Safety and preliminary clinical activity of REGN5458, an anti-Bcma x anti-CD3 bispecific antibody, in patients with relapsed/refractory multiple myeloma. Blood. 2019;134(Supplement_1):3176. doi:10.1182/blood-2019-126818
56. Naresh Bumma JR, Brayer J, Zonder JA, et al. 4555 updated safety and efficacy of REGN5458, a BCMAxCD3 bispecific antibody, treatment for relapsed/refractory multiple myeloma: a phase 1/2 first-in-human study; 2022. Available from: https://ash.confex.com/ash/2022/webprogram/Paper159969.html.
57. Regeneron. Linvoseltamab (BCMAXCD3) initial pivotal phase 2 data show clinically meaningful responses in patients with heavily pre-treated multiple myeloma; 2022. Available from: https://investor.regeneron.com/node/27321.
58. Naresh Bumma JR, Brayer J, Zonder JA, et al. Updated safety and efficacy of REGN5458, a BCMAxCD3 bispecific antibody, treatment for relapsed/refractory multiple myeloma: a phase 1/2 first-in-human study; 2022. Available from: https://ash.confex.com/ash/2022/webprogram/Paper159969.html.
59. ClinicalTrials.gov. A study to assess AMG 701 montherapy, or in combination with pomalidomide, with or without, dexamethasone in subjects with relapsed or refractory multiple myeloma; 2017. Available from: https://clinicaltrials.gov/ct2/show/NCT03287908.
60. Harrison SJ, Minnema MC, Lee HC, et al. A Phase 1 First in Human (FIH) study of AMG 701, an Anti-B-Cell Maturation Antigen (BCMA) Half-Life Extended (HLE) BiTE® (bispecific T-cell engager) molecule, in Relapsed/Refractory (RR) Multiple Myeloma (MM). Blood. 2020;136(Supplement 1):28–29. doi:10.1182/blood-2020-134063
61. Wong NB SW, Paris L, Hofmeister CC, et al. Alnuctamab (ALNUC; BMS-986349; CC-93269), a B-Cell Maturation Antigen (BCMA) x CD3 T-Cell Engager (TCE), in Patients (pts) with Relapsed/Refractory Multiple Myeloma (RRMM): results from a phase 1 first-in-human clinical study; 2022.
62. Costa LJ, Wong SW, Bermúdez A, et al. First clinical study of the B-Cell Maturation Antigen (BCMA) 2+1 T Cell Engager (TCE) CC-93269 in Patients (Pts) with Relapsed/Refractory Multiple Myeloma (RRMM): interim results of a phase 1 multicenter trial. Blood. 2019;134(Supplement_1):143. doi:10.1182/blood-2019-122895
63. ClinicalTrials.gov. Study of CC-93269, a BCMA x CD3 T cell engaging antibody, in participants with relapsed and refractory multiple myeloma; 2018. Available from: https://clinicaltrials.gov/ct2/show/NCT03486067.
64. ClinicalTrials.gov. A study of TNB-383B in participants with relapsed or refractory multiple myeloma; 2019.
65. Voorhees PM, D’Souza A, Weisel K, et al. A phase 1 first-in-human study of Abbv-383, a BCMA × CD3 bispecific T-cell-redirecting antibody, as monotherapy in patients with relapsed/refractory multiple myeloma. Blood. 2022;140(Supplement 1):4401–4404. doi:10.1182/blood-2022-167008
66. D’Souza A, Shah N, Rodriguez C, et al. A phase I first-in-human study of ABBV-383, a B-cell maturation antigen × CD3 bispecific T-cell redirecting antibody, in patients with relapsed/refractory multiple myeloma. J Clin Oncol. 2022;40(31):3576–3586. doi:10.1200/JCO.22.01504
67. Emma Searle HQ, Wong SW, Megala Costa LJ, et al. Teclistamab in combination with subcutaneous daratumumab and lenalidomide in patients with multiple myeloma: results from one cohort of majesTEC-2, a phase1b, multicohort study; 2022. Available from: https://ash.confex.com/ash/2022/webprogram/Paper159711.html.
68. Lindsay H, Szabo A, Bhatlapenumarthi V, et al. Changing spectrum of infection with BCMA and GPRC5D targeting bispecific antibody therapy in patients with relapsed refractory multiple myeloma (RRMM). J Clin Oncol. 2023;41(16_suppl):8019.
69. June CH, Sadelain M. Chimeric antigen receptor therapy. N Engl J Med. 2018;379(1):64–73. doi:10.1056/NEJMra1706169
70. Brudno JN, Maric I, Hartman SD, et al. T cells genetically modified to express an anti–B-cell maturation antigen chimeric antigen receptor cause remissions of poor-prognosis relapsed multiple myeloma. J Clin Oncol. 2018;36(22):2267–2280. doi:10.1200/JCO.2018.77.8084
71. Wang X, Rivière I. Clinical manufacturing of CAR T cells: foundation of a promising therapy. Mol Ther Oncolytics. 2016;3:16015. doi:10.1038/mto.2016.15
72. Noaks E, Peticone C, Kotsopoulou E, Bracewell DG. Enriching leukapheresis improves T cell activation and transduction efficiency during CAR T processing. Mol Ther Methods Clin Dev. 2021;20:675–687. doi:10.1016/j.omtm.2021.02.002
73. Lukjanov V, Koutná I, Šimara P, Ponce-Soto LA. CAR T-cell production using nonviral approaches. J Immunol Res. 2021;2021:6644685. doi:10.1155/2021/6644685
74. FDA approves ciltacabtagene autoleucel for relapsed or refractory multiple myeloma; 2022. Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-approves-ciltacabtagene-autoleucel-relapsed-or-refractory-multiple-myeloma.
75. FDA approves first cell-based gene therapy for adult patients with multiple myeloma; 2021. Available from: https://www.fda.gov/news-events/press-announcements/fda-approves-first-cell-based-gene-therapy-adult-patients-multiple-myeloma.
76. Rodriguez-Otero P, Ailawadhi S, Arnulf B, et al. Ide-cel or standard regimens in relapsed and refractory multiple myeloma. N Engl J Med. 2023;388(11):1002–1014. doi:10.1056/NEJMoa2213614
77. Mi J-Q, Zhao W, Jing H, et al. Phase 2, open-label study of ciltacabtagene autoleucel, an anti-BCMA CAR-T cell therapy, in Chinese patients with relapsed/refractory multiple myeloma (CARTIFAN-1): 26-month median follow-up. Blood. 2022;140(Supplement 1):7542–7544. doi:10.1182/blood-2022-159185
78. Chunrui LM, Di Wang MD, Baijun Fang MD, et al. 3311 updated results of fumanba-1: a phase 1b/2 study of a novel fully human B-cell maturation antigen-specific CAR T cells (CT103A) in patients with relapsed and/or refractory multiple myeloma; 2022. Available from: https://ash.confex.com/ash/2022/webprogram/Paper166465.html.
79. Raje NS, Shah N, Jagannath S, et al. Updated clinical and correlative results from the phase I CRB-402 study of the BCMA-targeted CAR T cell therapy bb21217 in patients with relapsed and refractory multiple myeloma. Blood. 2021;138(Supplement 1):548. doi:10.1182/blood-2021-146518
80. Mailankody S, Jakubowiak AJ, Htut M, et al. Orvacabtagene autoleucel (orva-cel), a B-cell maturation antigen (BCMA)-directed CAR T cell therapy for patients (pts) with relapsed/refractory multiple myeloma (RRMM): update of the phase 1/2 EVOLVE study (NCT03430011). J Clin Oncol. 2020;38(15_suppl):8504.
81. Costa LJ, Kumar SK, Atrash S, et al. Results from the first phase 1 clinical study of the B-Cell Maturation Antigen (BCMA) Nex T Chimeric Antigen Receptor (CAR) T cell therapy CC-98633/BMS-986354 in Patients (pts) with Relapsed/Refractory Multiple Myeloma (RRMM). Blood. 2022;140(Supplement 1):1360–1362. doi:10.1182/blood-2022-160038
82. Chen W, Fu C, Fang B, et al. Phase II study of fully human BCMA-targeting CAR-T cells (zevorcabtagene autoleucel) in patients with relapsed/refractory multiple myeloma. Blood. 2022;140(Supplement 1):4564–4565. doi:10.1182/blood-2022-168610
83. Mailankody S, Ghosh A, Staehr M, et al. Clinical responses and pharmacokinetics of MCARH171, a human-derived bcma targeted CAR T cell therapy in relapsed/refractory multiple myeloma: final results of a phase I clinical trial. Blood. 2018;132(Supplement 1):959. doi:10.1182/blood-2018-99-119717
84. Fernandez de Larrea C, Gonzalez-Calle V, Cabañas V, et al. Results from a pilot study of ARI0002h, an academic BCMA-directed CAR-T cell therapy with fractionated initial infusion and booster dose in patients with relapsed and/or refractory multiple myeloma. Blood. 2021;138(Supplement 1):2837. doi:10.1182/blood-2021-147188
85. Li C, Wang X, Wu Z, et al. Bispecific CS1-BCMA CAR-T cells are clinically active in relapsed or refractory multiple myeloma: an updated clinical study. Blood. 2022;140(Supplement 1):4573–4574. doi:10.1182/blood-2022-170686
86. Sperling AS, Nikiforow S, Nadeem O, et al. Phase I study of PHE885, a fully human BCMA-directed CAR-T cell therapy for relapsed/refractory multiple myeloma manufactured in <2 days using the T-charge TM platform. Blood. 2021;138(Supplement 1):3864.
87. Qu X, An G, Sui W, et al. Updated phase 1 results of C-CAR088, an anti-BCMA CAR T-cell therapy in relapsed or refractory multiple myeloma. Blood. 2021;138(Supplement 1):1830. doi:10.1182/blood-2021-150037
88. T cells expressing a fully-human anti-BCMA chimeric antigen receptor with a heavy-chain-only antigen-recognition domain exhibit rapid and durable activity against multiple MyelomaClinically relevant abstract; 2022. Available from: https://ash.confex.com/ash/2022/webprogram/Paper159156.html.
89. Korst CLBM, Bruins WSC, Cosovic M, et al. Preclinical activity of allogeneic CS1-specific CAR T-cells (UCARTCS1) in multiple myeloma. Blood. 2022;140(Supplement 1):4215–4216. doi:10.1182/blood-2022-157950
90. ClinicalTrials.gov. Study of bb2121 in multiple myeloma; 2016. Available from: https://clinicaltrials.gov/ct2/show/NCT02658929.
91. Munshi NC, Anderson LD, Shah N, et al. Idecabtagene vicleucel in relapsed and refractory multiple myeloma. N Engl J Med. 2021;384(8):705–716. doi:10.1056/NEJMoa2024850
92. Delforge M, Shah N, Miguel JSF, et al. Health-related quality of life with idecabtagene vicleucel in relapsed and refractory multiple myeloma. Blood Adv. 2022;6(4):1309–1318. doi:10.1182/bloodadvances.2021005913
93. Zhao W-H, Liu J, Wang B-Y, et al. A phase 1, open-label study of LCAR-B38M, a chimeric antigen receptor T cell therapy directed against B cell maturation antigen, in patients with relapsed or refractory multiple myeloma. J Hematol Oncol. 2018;11(1):141. doi:10.1186/s13045-018-0681-6
94. ClinicalTrials.gov. LCAR-B38M cells in treating Relapsed/Refractory (R/R) Multiple Myeloma (LEGEND-2); 2017. Available from: https://clinicaltrials.gov/ct2/show/NCT03090659.
95. Summary basis for regulatory action – carvykti; 2022. Available from: https://www.fda.gov/media/156999/download.
96. Zhao W-H, Wang B-Y, Chen L-J, et al. Four-year follow-up of LCAR-B38M in relapsed or refractory multiple myeloma: a Phase 1, single-arm, open-label, multicenter study in China (LEGEND-2). J Hematol Oncol. 2022;15(1):86. doi:10.1186/s13045-022-01301-8
97. Cohen AD, Parekh S, Santomasso BD, et al. Incidence and management of CAR-T neurotoxicity in patients with multiple myeloma treated with ciltacabtagene autoleucel in CARTITUDE studies. Blood Cancer J. 2022;12(2):32. doi:10.1038/s41408-022-00629-1
98. Van Oekelen O, Aleman A, Upadhyaya B, et al. Neurocognitive and hypokinetic movement disorder with features of parkinsonism after BCMA-targeting CAR-T cell therapy. Nat Med. 2021;27(12):2099–2103. doi:10.1038/s41591-021-01564-7
99. Berdeja JG, Madduri D, Usmani SZ, et al. Ciltacabtagene autoleucel, a B-cell maturation antigen-directed chimeric antigen receptor T-cell therapy in patients with relapsed or refractory multiple myeloma (CARTITUDE-1): a phase 1b/2 open-label study. Lancet. 2021;398(10297):314–324. doi:10.1016/S0140-6736(21)00933-8
100. Martin T, Usmani SZ, Berdeja JG, et al. Ciltacabtagene autoleucel, an anti–B-cell maturation antigen chimeric antigen receptor T-cell therapy, for relapsed/refractory multiple myeloma: CARTITUDE-1 2-year follow-up. J Clin Oncol. 2023;41(6):1265–1274. doi:10.1200/JCO.22.00842
101. Mi JQ, Zhao W, Jing H, et al. Phase II, open-label study of ciltacabtagene autoleucel, an anti-B-cell maturation antigen chimeric antigen receptor-T-cell therapy, in Chinese patients with relapsed/refractory multiple myeloma (CARTIFAN-1). J Clin Oncol. 2023;41(6):1275–1284. doi: 10.1200/JCO.22.00690
102. ClinicalTrials.gov. A study of LCAR-B38M CAR-T cells, a Chimeric Antigen Receptor T-cell (CAR-T) therapy directed against B-cell Maturation Antigen (BCMA) in Chinese Participants With Relapsed or Refractory Multiple Myeloma (CARTIFAN-1); 2018. Available from: https://www.clinicaltrials.gov/ct2/show/NCT03758417.
103. Alqazaqi R, Schinke C, Thanendrarajan S, et al. Geographic and racial disparities in access to chimeric antigen receptor–T cells and bispecific antibodies trials for multiple myeloma. JAMA Netw Open. 2022;5(8):e2228877–e2228877. doi:10.1001/jamanetworkopen.2022.28877
104. Faris Jamal Abu Za’nouneh OA, Schinke C, Thanendrarajan S, et al. Variability of definition of high-risk multiple myeloma in phase III clinical trials; 2022. Available from: https://ash.confex.com/ash/2022/webprogram/Paper158188.html.
105. Leblay N, Maity R, Barakat E, et al. Cite-seq profiling of T cells in multiple myeloma patients undergoing BCMA targeting CAR-T or bites immunotherapy. Blood. 2020;136:11–12.
106. Swamydas M, Murphy EV, Ignatz-Hoover JJ, Malek E, Driscoll JJ. Deciphering mechanisms of immune escape to inform immunotherapeutic strategies in multiple myeloma. J Hematol Oncol. 2022;15(1):17. doi:10.1186/s13045-022-01234-2
107. Fernández de Larrea C, Staehr M, Lopez AV, et al. Defining an optimal dual-targeted CAR T-cell therapy approach simultaneously targeting BCMA and GPRC5D to prevent BCMA escape–driven relapse in multiple myeloma. Blood Cancer Discovery. 2020;1(2):146–154. doi:10.1158/2643-3230.BCD-20-0020
108. Reiser J, Mathavan K, Mahmood S, et al. Dual chimeric antigen receptor approach combining novel tumor targeting strategies circumvents antigen escape in multiple myeloma. Blood. 2021;138(Supplement 1):1718. doi:10.1182/blood-2021-154025
109. Gazeau N, Beauvais D, Yakoub-Agha I, et al. Effective anti-BCMA retreatment in multiple myeloma. Blood Adv. 2021;5(15):3016–3020. doi:10.1182/bloodadvances.2021004176
110. Xu J, Chen LJ, Yang SS, et al. Exploratory trial of a biepitopic CAR T-targeting B cell maturation antigen in relapsed/refractory multiple myeloma. Proc Natl Acad Sci U S A. 2019;116(19):9543–9551. doi:10.1073/pnas.1819745116
111. Mailankody S, Matous JV, Chhabra S, et al. Allogeneic BCMA-targeting CAR T cells in relapsed/refractory multiple myeloma: phase 1 UNIVERSAL trial interim results. Nat Med. 2023;29(2):422–429. doi:10.1038/s41591-022-02182-7
112. Cao Z, Yang C, Wang Y, et al. Allogeneic CAR-NK cell therapy targeting both BCMA and GPRC5D for the treatment of multiple myeloma. Blood. 2022;140(Supplement 1):7378. doi:10.1182/blood-2022-159289
113. Motais B, Charvátová S, Hrdinka M, Hájek R, Bago JR. Anti-BCMA-CAR NK cells expressing soluble TRAIL: promising therapeutic approach for multiple myeloma in combination with bortezomib and γ-secretase inhibitors. Blood. 2022;140(Supplement 1):12683–12684. doi:10.1182/blood-2022-166167
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
The Antibody Drug Conjugate, Belantamab-Mafodotin, in the Treatment of Multiple Myeloma: A Comprehensive Review
Almodovar Diaz AA, Alouch SS, Chawla Y, Gonsalves WI
Blood and Lymphatic Cancer: Targets and Therapy 2024, 14:71-87
Published Date: 6 December 2024
Teclistamab for Relapsed or Refractory Multiple Myeloma: A Review of Efficacy, Safety, Resistance Mechanisms and Future Directions
Piron B, Moreau P, Touzeau C
Biologics: Targets and Therapy 2026, 20:539066
Published Date: 13 January 2026
Real-World Treatment Patterns of Elranatamab in Patients with Multiple Myeloma in Japan: The EVEREST Study
Yoshihara S, Meche A, Hlavacek P, Johnson SM, Demers AS, Nador G, Ikoma S, Yadav CP, Assaf CA, DiBonaventura M, Chen Y
ClinicoEconomics and Outcomes Research 2026, 18:581258
Published Date: 11 March 2026
Integrin alpha8beta1 is Identified as a Potential CAR-T Target for BCMA-Resistant Relapsed Multiple Myeloma
Liu S, Wu J, Liu J, Wu K, Huang Y, Geng S, Wang Y, Weng J, Du X, Lai P
ImmunoTargets and Therapy 2026, 15:605729
Published Date: 28 May 2026