Back to Journals » Psoriasis: Targets and Therapy » Volume 15
Real-World Experience of Guselkumab in the Elderly Population
Authors Fratton Z ![]() , Bighetti S
, Bighetti S ![]() , Bettolini L
, Bettolini L ![]() , Maione V, Rossi M, Venturini M
, Maione V, Rossi M, Venturini M ![]() , Mazzoletti V, Zelin E, Stinco G, Errichetti E
, Mazzoletti V, Zelin E, Stinco G, Errichetti E
Received 25 June 2025
Accepted for publication 23 December 2025
Published 26 December 2025 Volume 2025:15 Pages 581—601
DOI https://doi.org/10.2147/PTT.S549502
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Mio Nakamura
Zeno Fratton,1 Stefano Bighetti,2 Luca Bettolini,2 Vincenzo Maione,2 Mariateresa Rossi,2 Marina Venturini,2 Vanessa Mazzoletti,3 Enrico Zelin,3 Giuseppe Stinco,1 Enzo Errichetti1
1Institute of Dermatology, Department of Medicine, University of Udine, Udine, Italy; 2Dermatology Department, University of Brescia, ASST Spedali Civili Di Brescia, Brescia, Italy; 3Institute of Dermatology, Santa Maria Della Misericordia University Hospital, Udine, Italy
Correspondence: Zeno Fratton, Institute of Dermatology, Department of Medicine, University of Udine, Piazzale Santa Maria della Misericordia, 15, Udine, 33100, Italy, Tel +39 0432559820, Email [email protected]
Introduction: Psoriasis is a chronic inflammatory disease whose burden peaks in older age groups. Despite the increasing prevalence of elderly patients with moderate-to-severe psoriasis, real-world data on biologics in this population remain limited, particularly for anti-IL-23 agents like guselkumab. This study evaluates the long-term effectiveness and safety of guselkumab in patients aged ≥ 65 years.
Methods: This retrospective study included 66 patients aged ≥ 65 years with plaque psoriasis treated with guselkumab 100 mg between June 2019 and June 2024. PASI scores were recorded at baseline and during follow-up visits at weeks 4, 16, 24, 36, 52, 76, and 104. Effectiveness was assessed using PASI75/90/100 and PASI ≤ 2 responses. Multivariable logistic regression with Firth correction identified baseline predictors of PASI90 and PASI100 at weeks 16 and 52. Safety outcomes included treatment-emergent adverse events (TEAEs).
Results: Mean PASI improved from 13.3 at baseline to 1.0 at week 24 and remained stable through week 104. PASI90 and PASI100 were achieved by 83.9% and 71.0% at week 36 and maintained in 69.2% and 61.5% at week 104. Higher baseline PASI independently predicted PASI90 and PASI100 at week 16, while lower eosinophil-to-lymphocyte ratio (ELR) independently predicted PASI100. At week 52, chronic beta-blocker intake and PASI90 at week 16 predicted PASI90 response, while PASI100 was independently associated with low-dose aspirin use and positive family history of psoriasis. TEAEs occurred in 16.7% of patients, with treatment discontinued in 9.1%. Eczematous or urticarial AEs were associated with elevated baseline eosinophils and ELR.
Conclusion: Guselkumab is effective and well tolerated in older adults with psoriasis. Baseline ELR, early PASI response, and chronic use of beta-blockers or aspirin may influence long-term treatment outcomes. While limited by the small sample size (66 patients), our findings represent the longest real-world follow-up to date among older psoriatic patients treated with guselkumab and support its use as a valuable therapeutic option in this population.
Keywords: guselkumab, efficacy, safety, elderly, over 65 year
Introduction
Psoriasis, a chronic inflammatory skin condition affecting 2–3% of the world population,1 impacts quality of life and has the highest burden in the age groups of 60–64 and 65–69 years.2 A few studies have tried to estimate the exact prevalence of psoriasis in older adults,3,4 finding that between 3.9% and 5.3% are affected by the disease. Given that individuals with psoriasis have a life expectancy comparable to the general population and, considering the projected growth of the elderly demographic worldwide,5 the prevalence of psoriasis among older adults is expected to rise in the coming decades.
Biologics have emerged as the treatment of choice in patients with moderate-to-severe psoriasis, especially in cases where conventional therapies, like cyclosporine or methotrexate, are contraindicated due to comorbidities. On the other hand, while the elderly have a higher multimorbidity than the general population,6 this age group is often excluded from clinical trials on biologic therapies. As a consequence, data regarding the effectiveness and safety of these therapies in this specific age group is currently derived from real world experiences.
Older adults tend to show slower responses to biologic therapies compared to younger patients,7 mainly due to age-related changes in pharmacokinetics (eg lower peripheral tissue perfusion), comorbidities and immunesenescence. Among comorbidities, insulin resistance and the resulting hyperinsulinemia are more common in the aging population,8 which may contribute to reduced biologic responsiveness by promoting interleukin-23 (IL-23) production from adipocytes.9 Treatment responses may also be affected by an age-related decline in the number and function of regulatory T lymphocytes, whose activity, however, may be partially restored by anti–IL-23 therapies.10
While the effectiveness and safety of anti-IL-17 agents in the elderly have been extensively studied,11–14 little evidence has been published on tildrakizumab15 and other anti-IL-23 agents,16 mainly in studies with small sample sizes and short follow-up periods, thus limiting the currently available knowledge of this biologic class in this age group.
This retrospective study aims to bridge this gap by providing long-term real-world data on the effectiveness and safety of guselkumab, an anti-IL-23p19 agent, in patients aged 65 years or older.
Patients and Methods
Methods and Data Extraction from Patient Database
Eligible patients were elderly subjects (≥65 years old) with chronic plaque psoriasis under treatment with guselkumab 100 mg in accordance with the Italian guidelines [psoriasis area and severity index (PASI) ≥10 or a PASI < 10 with involvement of sensitive areas (including face, nails, palms/soles or genitals)]17 during the period June 2019-June 2024. Patients who had used concomitant systemic anti-psoriatic therapies and those with less than 24 weeks of follow-up after commencing guselkumab 100 mg were excluded from the analysis. To avoid underestimating the incidence of adverse events, patients who discontinued guselkumab due to treatment-related adverse events but attended follow-up visits for at least 24 weeks after the first guselkumab dose were included.
The characteristics of all patients, including age, comorbidities, chronic pharmacotherapy, baseline blood biomarkers, disease duration, previous treatments and PASI scores at each visit, were obtained from electronic medical records. At weeks 4, 16, 24, 36, 52, 76 and 104, the proportions of patients reaching a reduction of 75%, 90%, and 100% in PASI compared with baseline (PASI75, PASI90 and PASI100, respectively) were recorded. We also analyzed the percentages of patients who achieved an absolute PASI of 2 or less at each visit. During each dermatological examination, patients were asked about the onset of any adverse event (AE), including AEs leading to the discontinuation of guselkumab.
Given the retrospective design of our study, not all visits were completed by all patients. Therefore, all data for follow-up visits they had not attended were deemed missing. When a value for an intermediate visit was missed, it was imputed using the last observation carried forward (LOCF) method.
The study was conducted in accordance with the ethical standards established by the 1964 Declaration of Helsinki. Ethical approval was obtained from local Ethics Committee (Comitato Etico Territoriale Lombardia 6, protocol 4710). Written informed consent was obtained from all individual participants included in the study. All the participants gave their consent to the use of medical records for research purposes.
Outcome Measures
Effectiveness was measured by assessing the rate of patients reaching either improvement of 75%, 90%, and 100% in PASI compared with baseline score or an absolute PASI < 2. Safety was measured assessing clinically significant Treatment Emergent Adverse Events (TEAEs) defined as those that led to drug discontinuation, required hospitalization, or prompted the initiation of specific medical treatment. We collected information regarding TEAEs type, week of onset and whether they led to therapy discontinuation.
Statistical Analysis
Continuous variables were reported using mean and standard deviation (SD), while categorical variables were presented as absolute numbers and frequencies. The effectiveness of guselkumab in terms of achievement of PASI90 and PASI100 at weeks 16 and 52 was evaluated according to different baseline characteristics, including gender, age, involvement of difficult to treat areas (scalp, palms/soles, genitals, nails), body mass index (BMI), psoriasis duration, comorbidity burden and type, number of daily pharmacotherapies, and baseline blood biomarkers. Categorical variables were compared using Chi-square or Fisher’s exact test, as appropriate. For continuous variables, either Student’s t-test or Mann–Whitney U-test was applied based on data distribution, which was assessed using the Shapiro–Wilk test. Paired t-test was used to assess significant differences in PASI values between visits. To identify baseline factors independently associated with the achievement of PASI90 and PASI100 responses at weeks 16 and 52, multivariable logistic regression using Firth’s penalized likelihood method was employed. All variables with p < 0.1 in univariate analysis and those considered clinically relevant (age, baseline PASI, bio-naïve status, and BMI) were included in the initial models. Multicollinearity among predictors was assessed by calculating variance inflation factors (VIF), and variables with VIF > 5 were excluded to improve model stability.
Results of the multivariate analysis were reported as odds ratios (ORs) with corresponding 95% confidence intervals (CIs). Model performance was evaluated using the residual deviance, Wald test, and Likelihood Ratio Test (LRT).
Microsoft Excel was used for data collection, while GraphPad Prism version 10.0.0 for Mac OS (GraphPad Software, Boston, Massachusetts, USA) was used to generate graphs. All analyses were performed using R Statistical Software (v4.1.2; R Core Team 2021).
Results
Clinical and Demographic Characteristics of the General Population
Sixty-six patients were included in this study. Of these, 64 patients completed 24 weeks of treatment, while 62, 55, 35 and 26 of them respectively reached 36, 52, 76 and 104 weeks of follow up. Forty-three patients were male (65.2%), the mean age was 70.7 years, with a standard deviation (SD) of 6.3. Mean psoriasis duration was 24.9 years (SD 14.8). Mean BMI was 27.7 (SD 5.0) and 25.8% of our patients were obese (BMI ≥ 30). A concomitant diagnosis of Psoriatic Arthritis (PsA) was observed in 25.8% of patients, and 95.5% of all the patients were affected by at least one comorbidity, with 39.4% of patients being affected by four or more comorbidities. The most represented comorbidity was hypertension (74.2%), followed by cardiac comorbidities (28.8%), obesity (25.8%) and chronic kidney disease (CKD; 25.8%). Twenty-one patients (31.8%) were chronically taking more than 3 concomitant medications for their comorbidities, and participants were taking on average 3.10 (SD 2.6) daily medications. The most prescribed daily medications were beta-blockers (34.8%) followed low-dose aspirin (28.8%) and statins (27.3%).
More than one third of patients had never received a biologic therapy before starting guselkumab (39.4%), while the most prescribed biologics in bio-experienced patients were adalimumab (48.5%) followed by secukinumab (18.2%), etanercept (9.1%) and ixekizumab (6.1%). Twenty-five patients (37.9%) had failed one biologic, while six (9.1%) had failed three or more biologics, with an average of 1.0 (SD 1.0) failures per patient. Thirty-six patients (54.5%) had involvement of one or more sensitive areas (scalp, genitals, palms and soles), while 17 (25.8%) suffered from nail psoriasis. Additional data regarding the characteristics of our populations are summarized in Table 1.
 |
Table 1 Summary of Demographic and Clinical Characteristics of Included Patients |
Effectiveness of Guselkumab
At baseline, the mean PASI was 13.3 (SD 7.1). During the treatment with guselkumab, it significantly decreased to 5.8 (SD 3.7) at week 4, 2.0 (SD 1.9) at week 16 and 1.0 (SD 1.4) after 24 weeks of treatment. Mean PASI further improved after 36 weeks (0.6 ± 1.3), while it remained stable at weeks 52, 76 and 104 with no statistically significant fluctuations, being 1.0 (SD 2.0), 1.1 (SD 2.2) and 1.2 (SD 2.3), respectively. At week 4, 15.6% of the patients reached PASI75, 3.1% PASI90, 1.6% PASI100 and 3.1% PASI ≤ 2. The effectiveness of guselkumab progressively improved during the first 36 weeks of treatment, with 39.1%, 64.1% and 83.9% of patients reaching PASI90 after 16, 24, 36 weeks of treatment, respectively. In the same time intervals 25.0%, 50.0% and 71.0% of patients achieved PASI100. The effectiveness of guselkumab was maintained throughout the study period, with 76.4%, 74.3% and 69.2% of patients maintaining PASI90 and 65.5%, 65.7% and 61.5% of patients maintaining PASI100 at weeks 52, 76 and 104, respectively.
Additional data on the effectiveness of guselkumab at each time point in terms of mean PASI, PASI75/90/100 and PASI ≤ 2 are shown in Figures 1 and 2.
 |
Figure 1 Share of patients achieving PASI75, -90, -100 and < 2 responses over time. |
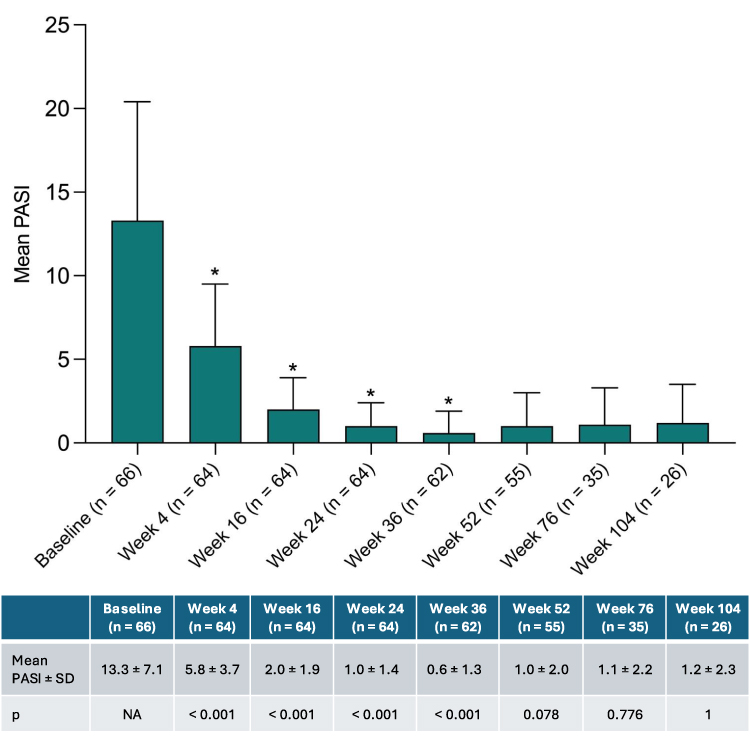 |
Figure 2 Mean ± SD PASI scores at several time-points over the follow up period. Symbol “*” indicates a statistically significant (p < 0.05) change in PASI. |
Predictors of PASI90 and -100 Responses at Week 16
Table 2 reports baseline demographic and clinical characteristics of the psoriasis cohort stratified by treatment response to guselkumab at week 16. Patients who achieved a PASI90 response at week 16 were older (73.6 ± 8.2 vs 68.9 ± 4.1; p = 0.045) had a significantly lower baseline BMI (25.8 ± 4.2 vs 28.3 ± 4.1; p = 0.016), a higher baseline PASI (16.4 ± 8.9 vs 11.2 ± 4.8; p = 0.020), a higher proportion of individuals aged ≥75 years (52.0% vs 23.1%; p = 0.035), lower lymphocyte (1.67 ± 0.76 vs 2.01 ± 0.65; p = 0.015) and eosinophil (0.16 ± 0.15 vs 0.45 ± 0.68; p = 0.009) counts, as well as a reduced eosinophil-to-lymphocyte (ELR; 0.09 ± 0.08 vs 0.22 ± 0.34; p = 0.017) and higher platelet-to-lymphocyte ratio (PLR; 170.89 ± 88.74 vs 126.88 ± 49.42; p 0.031).
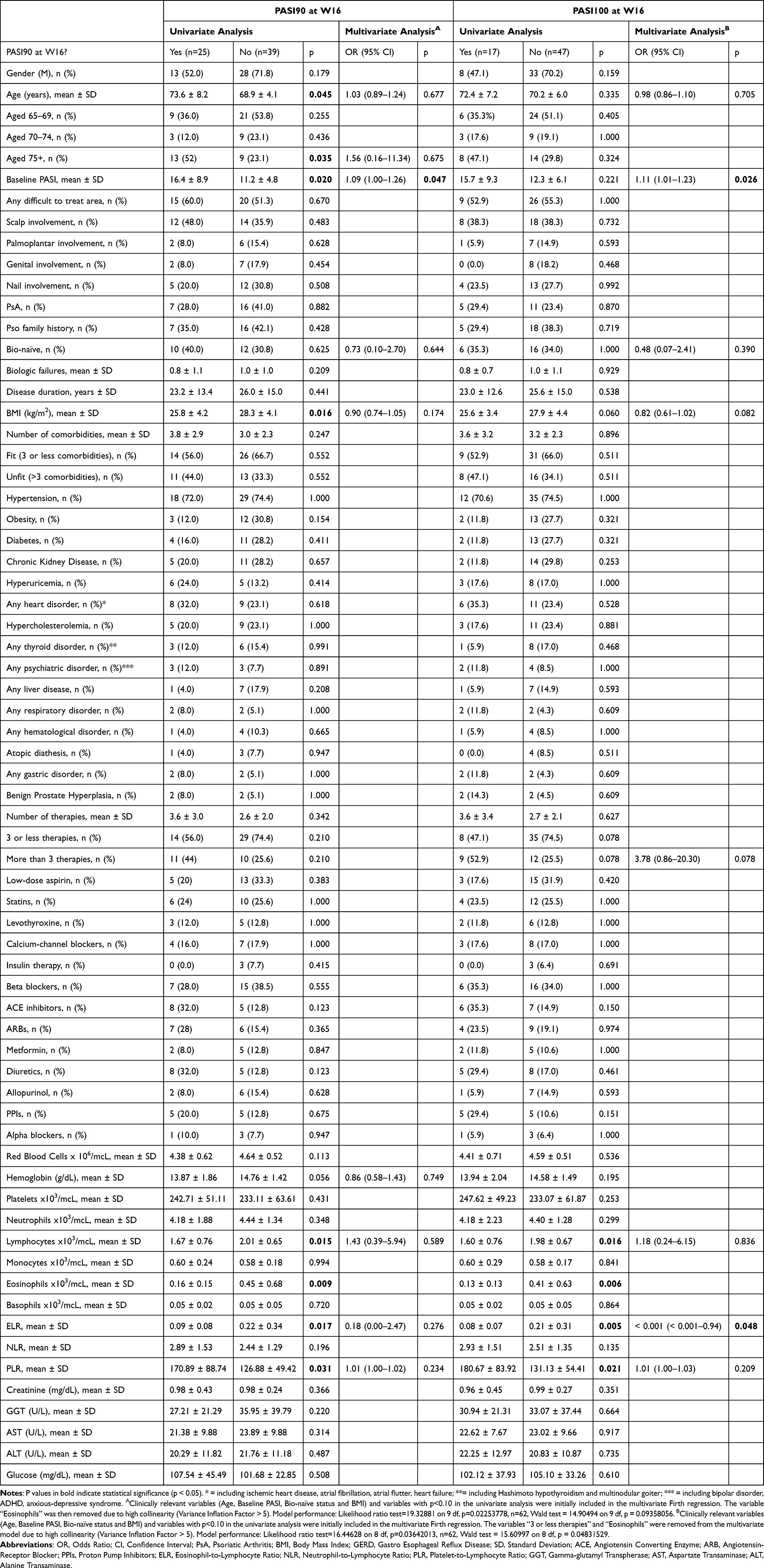 |
Table 2 Variables Associated with the Achievement of PASI90 and PASI100 at W16 |
Higher baseline PASI emerged as the only independent predictor of achieving PASI-90 response at week 16 in the multivariate model (OR 1.09, 95% CI 1.00–1.26, p = 0.047).
Regarding the achievement of PASI100 at week 16, no baseline clinical variable showed any significant association, although this outcome correlated with lower lymphocyte counts (1.60 ± 0.76 vs 1.98 ± 0.67; p = 0.016), eosinophils (0.13 ± 0.15 vs 0.41 ± 0.63; p = 0.006), ELR (0.08 ± 0.07 vs 0.21 ± 0.31; p = 0.005), and higher platelet-to-lymphocyte ratio (PLR; 180.67 ± 83.92 vs 131.13 ± 54.41; p = 0.021). Patients who reached PASI100 at week 16 had on average a lower BMI (25.6 ± 3.4 vs 27.9 ± 4.4), although not significantly (p = 0.06).
Higher baseline PASI (OR 1.11, 95% CI 1.01–1.23 p = 0.026) and lower baseline ELR (OR < 0.001, 95% CI < 0.001–0.94; p = 0.048) emerged as the only independent predictors of achieving PASI100 response at week 16 in the multivariate model.
Predictors of PASI90 and -100 Responses at Week 52
Table 3 reports baseline demographic and clinical characteristics of the psoriasis cohort, stratified according to treatment response to guselkumab at week 52. Patients who achieved PASI90 at week 52 had a lower prevalence of obesity (17.1% vs 50.0%; p = 0.037), and more frequently achieved a PASI90 (51.2% vs 0.00%; p = 0.002) or PASI-100 (34.1% vs 0.00%; p 0.029) response at week 16. Furthermore, patients achieving PASI90 at week 52 were more frequently taking beta-blockers (46.3% vs 14.3%) and low-dose aspirin (36.6% vs 7.1%), although not significantly (respectively p = 0.07 and p = 0.08).
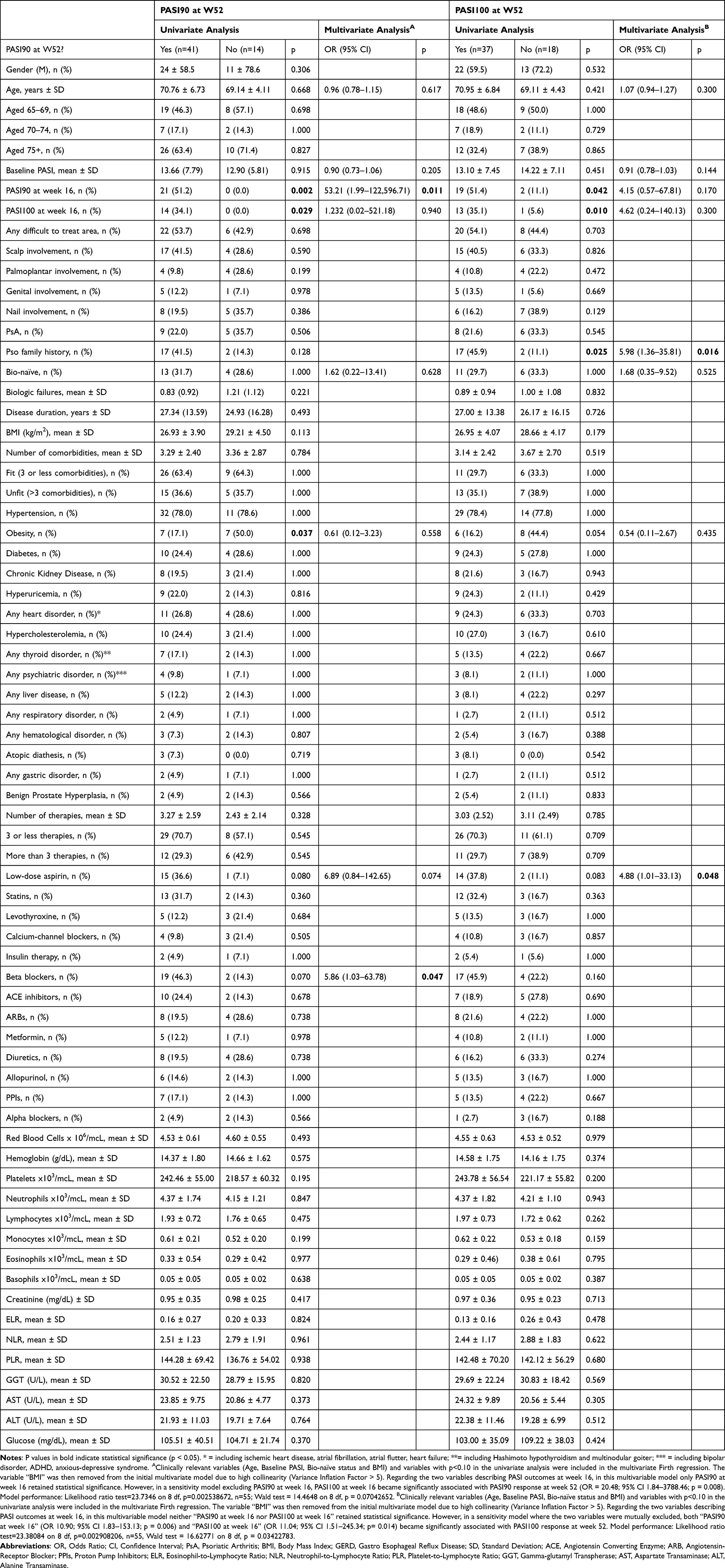 |
Table 3 Variables Associated with the Achievement of PASI90 and PASI100 at Week 52 |
In the multivariate model, the chronic intake of beta-blockers emerged as an independent predictor of PASI90 achievement at week 52 (OR 5.86, 95% CI 1.03–63.78; p = 0.047). Achieving PASI90 at week 16 independently predicted the maintenance of PASI90 response at week 52 (OR 53.21, 95% CI 1.99–122,596.71). Conversely, achieving PASI100 at week 16 did not retain independent significance in the main model, but became statistically significant when PASI90 at week 16 was excluded from the sensitivity analysis (OR 20.48, 95% CI 1.84–3788.46; p = 0.008).
Patients who achieved PASI100 at week 52 had more frequently reached PASI90 (51.4% vs 11.1%; p = 0.042) and PASI100 (35.1% vs 5.6%; p = 0.010) responses at week 16, and more often had a positive family history of psoriasis (45.9% vs 11.1%; p = 0.025). They were less frequently obese (16.2% vs 44.4%; p = 0.054) and more frequently on chronic low-dose aspirin therapy (37.8% vs 11.1%; p = 0.083), although these associations did not reach statistical significance.
In the multivariate model, a positive family history of psoriasis (OR 5.98, 95% CI 1.36–35.81; p = 0.016) and chronic low-dose aspirin intake (OR 4.88, 95% CI 1.01–33.13; p = 0.048) emerged as independent predictors of achieving PASI100 at week 52. Neither PASI90 nor PASI100 achievement at week 16 retained independent significance in the main model; however, when the two variables were alternately excluded from a sensitivity analysis, both became significantly associated with the outcome (PASI90 at week 16: OR 10.90, 95% CI 1.83–153.13, p = 0.006; PASI100 at week 16: OR 11.04, 95% CI 1.51–245.34, p = 0.014) (see Table 3).
Safety of Guselkumab and Causes of Treatment Discontinuation
A total of 11 patients (16.7%) experienced a clinically significant treatment-emergent adverse event (TEAE) during the 104-week follow-up for a total TEAE rate of 11.9 TEAEs/100 patient-years (see Table 4). The most frequently reported AE was the diagnosis of a previously undiagnosed malignancy (3 patients, 4.5%), followed by eczematous eruptions (2 patients, 3.1%), submammary and axillary candidiasis (2 patients, 3.1%), bullous pemphigoid (1 patient, 1.5%), pemphigus vulgaris (1 patient, 1.5%), urticaria (1 patient, 1.5%), and infectious endocarditis (1 patient, 1.5%).
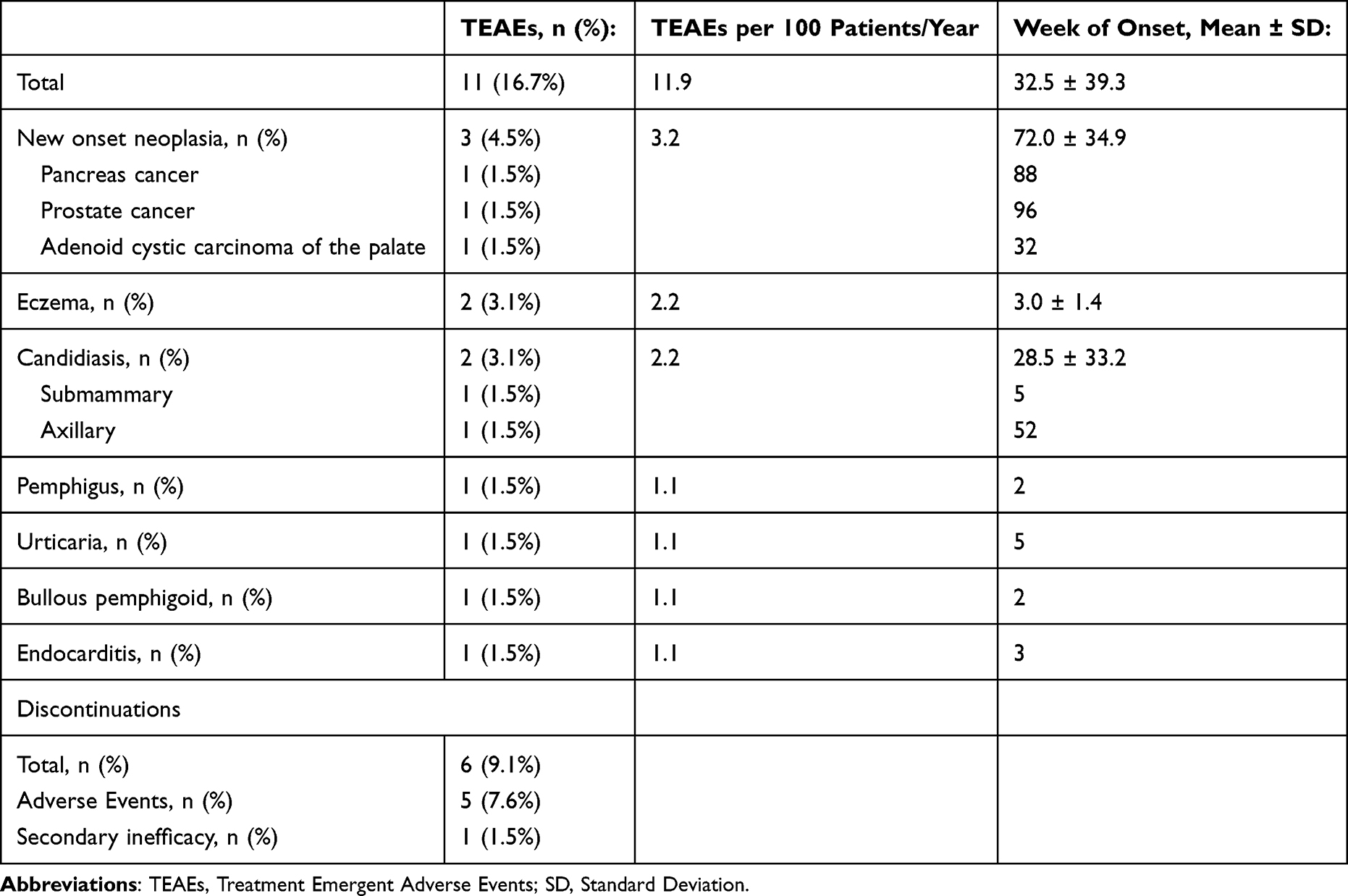 |
Table 4 Clinically Significant Treatment Emergent Adverse Events Observed During the Treatment Period and Causes of Discontinuation |
TEAEs occurred on average at week 32.5 of treatment (see Table 2), with neoplasms diagnosed at weeks 32, 88, and 96, respectively.
Treatment discontinuation was recorded in 6 patients (9.1%). One patient discontinued guselkumab due to secondary loss of efficacy on both skin and joint domains. The remaining five discontinued treatment following the onset of adverse events, including neoplasia (n=3), bullous pemphigoid (n=1), and pemphigus vulgaris (n=1).
To explore potential associations between baseline clinical characteristics and the development of specific categories of AEs, a univariate analysis was performed (see Table S1).
Among the findings, a significantly higher baseline eosinophil count (2.15 ± 0.72 vs 0.25 ± 0.37; p = 0.004), lymphocyte count (2.97 ± 0.39 vs 1.81 ± 0.66; p = 0.014) and ELR (0.71 ± 0.17 vs 0.15 ± 0.25; p = 0.007) were observed in patients who developed eczematous or urticarial reactions. Daily ARBs intake showed a statistically significant association (100.0% vs 17.5%, p = 0.007) with the development of malignancies. Due to the low number of positive events, a multivariate analysis was not undertaken.
Discussion
Effectiveness and Safety Comparison with Other Real-Life Studies
Several real-life studies have been reported on the effectiveness and safety of anti-IL-23 agents in the elderly,15,16,18,19 yet few of them specifically focused on guselkumab. Ruggiero et al16 investigated the efficacy of guselkumab in 20 elderly subjects followed up for 40–44 weeks, reporting better responses compared to our observations in the short term (at week 4: 65.0% vs 3.1% patients achieving PASI90; 30.0% vs 1.5% patients achieving PASI100) but inferior responses in the medium to long term (75.0% and 55.0% patients respectively reaching PASI90 and PASI100 at week 40–44 vs and 83.9% and 71.0% patients respectively reaching PASI90 and PASI100 at week 36 in our study). The differences in baseline PASI (17.1 ± 5.1 vs 12.9 ± 7.1) and rate of bio-naïve patients (10.0% vs 33.3%) might partially explain the observed differences in treatment outcomes, especially in the medium to long term. In the same study a higher rate of patients experienced an adverse event (25.0% in 44 weeks vs 16.7% in 104 weeks), although no serious AEs were reported.
The effectiveness and safety of tildrakizumab in the elderly was investigated in the ESTER study,15 involving 49 patients with a mean age of 73.1 ± 6.0 followed up for 28 weeks. During the study, better responses were observed in the short term compared to our observations (at week 4: PASI100 observed in 6.4% vs 1.5%) while results were comparable in the medium term (PASI100 observed in 47.5% at week 28 vs 50.0% at week 24). No severe AE was reported by the authors, however no comparison with our observations can be made due to the significantly different study durations (28 vs 104 weeks). Fiorillo et al19 conducted a retrospective study on 205 elderly patients receiving IL-17 and IL-23 inhibitors, of which 35 were treated with guselkumab, 87 with risankizumab and 9 with tildrakizumab. While no sub-analysis on different biologics or biologic classes was reported, no severe AE was observed during the 104 weeks follow up, confirming the safety of these drugs in older patients. The reported efficacy outcomes were comparable, with 34.6%, 59.5% and 57.3% (vs 25.0%, 65.5% and 61.5% in our study) achieving PASI100 at weeks 16, 52 and 104, respectively.
Beyond IL-23 inhibitors, several studies have assessed the effectiveness and safety of IL-17 inhibitors in elderly patients with psoriasis. Phan et al20 conducted a retrospective multicenter study on 114 patients aged 65 years and older, treated with secukinumab, ixekizumab, or brodalumab, reporting that 70% of the total participants achieved Physician Global Assessment (PGA) score of 0/1 between 3 and 6 months after initiation of treatment, while 28.9% of patients discontinued the anti-IL-17 therapy either due to psoriasis relapses (41.2%), primary failures (32.4%) and AEs (20.6%), showing higher discontinuation and AEs rates than what we observed with guselkumab in the same subpopulation.
The efficacy and safety of secukinumab alone in the elderly were investigated in a post-hoc analysis of the SUPREME Study,11 involving 36 patients aged 65 years or above. Of these, 69.4% and 44.4% respectively reached PASI90 and PASI100 at week 16 (compared to 39.1% and 25.0% observed in our study in the same time point), confirming the well-known faster short-term action of anti-IL-17 agents,21 while 66.7% reached PASI90 at week 24 (similarly to what we observed in the same point, with 64.1% reaching the same outcome). Regarding safety, 47.2% of patients in the aforementioned study developed a TEAE, however only 8.33% discontinued treatment for this reason.
Regarding bimekizumab, a multicenter Italian real-world study by Orsini et al13 analyzed its performance in elderly patients. In their cohort of 98 patients, PASI90 and PASI100 were respectively achieved by 72.4% and 53.1% at week 16, and mean improvement scores were maintained at week 36. AEs were reported by 5.1% of patients, but none lead to discontinuation.
A retrospective multicenter real-world study on a cohort of 69 patients treated with brodalumab14 found improvements comparable to the other studies investigating the efficacy of IL-17-inhibitors in the elderly, with 69.1% and 55.9% respectively reaching PASI90 and PASI100 at week 16 with further improvements to 86.4% and 75.8% at week 52. It must be noted however that the cohort in the aforementioned study had a lower BMI than those in our experience (26.9 ± 4.4 vs 28.0 ± 5.1), a lower prevalence of obesity (15.9% vs 28.3%) and a higher rate of bio-naïve patients (40.6% vs 33.3%), clinical features with proven impact on treatment outcomes.22 Treatment was discontinued in 8.7% of patients, mainly due to adverse events.
Finally, Sobotkova et al23 compared the overall effectiveness and safety of different biologic classes in elderly versus younger patients, finding no significant difference in PASI90 and PASI100 outcomes over 52 weeks, and similar safety outcomes in the two groups. However, no comparison between biologic classes was performed, limiting the possibility to assess any efficacy and safety difference between elderly and younger patients among anti-IL-17 and anti-IL-23 agents.
Features Influencing Treatment Response
We explored whether baseline demographic, clinical and laboratory characteristics could influence the probability of achieving PASI90 and PASI100 responses at weeks 16 and 52 during guselkumab treatment. In the short term, univariate analyses identified age over 75 years, lower BMI, higher baseline PASI, reduced baseline lymphocyte and eosinophil counts, lower ELR and higher PLR as significantly associated with PASI90 response. PASI100 response was similarly linked to lower lymphocytes, eosinophils, ELR, and higher PLR. Multivariate Firth regression confirmed higher baseline PASI, as the only independent predictor of both outcomes, while lower ELR emerged as an independent predictor of PASI100.
In the long term, patients who reached PASI90 or PASI100 at week 52 were more likely to have a positive family history of psoriasis, be non-obese, and to have already achieved PASI90 or PASI100 at week 16. Interestingly, they were also more frequently treated with beta-blockers, although not significantly. In multivariate analysis, the chronic intake of beta-blockers and having reached PASI90 at week 16 emerged as independent predictors of PASI90 long term response, while a positive psoriasis family history and the daily intake of low-dose aspirin emerged as independent predictors of PASI100 long term response. The latter also showed a tendency towards association with PASI90 response, although not reaching statistical significance.
The association between baseline PASI score and treatment response has been explored in multiple studies. While some have reported that achieving PASI100 (complete clearance) is more likely in patients with lower baseline PASI scores,22 others have found that higher baseline PASI values are associated with increased rates of PASI75 and PASI90 responses.24,25 These contrasting findings highlight the limitations of relative PASI reduction as an efficacy metric—particularly in patients with low baseline disease severity—since a substantial relative improvement may not correspond to complete skin clearance.26 Our results should therefore be interpreted with caution, especially in light of this methodological consideration.
Weissman et al27 investigated the association of hematological ratios with psoriasis in a nationwide cohort study. Among the reported findings, patients with severe psoriasis presented with higher eosinophils, lower lymphocytes and consequently higher ELR, however its relationship with treatment responses was not the object of the study. Some works have suggested that eosinophils are capable of producing IL-23, IL-17 and other inflammatory factors that activate and recruit neutrophils, thus contributing to the pathogenesis of psoriasis.28,29 Other works have shown a correlation between severe psoriasis and lower peripheral blood lymphocytes counts,30 further contributing to increase ELR in patients with more severe psoriasis, thus strengthening the hypothesis of ELR as a possible marker of psoriasis severity. The association of a higher ELR with worse treatment responses in the short- but not in the long-term further consolidates this hypothesis, as patients with more severe psoriasis might require more time to experience a marked reduction in systemic inflammation.
PLR has been investigated as a possible marker of systemic inflammation in plentiful studies.31 While the association with psoriasis emerged clearly, its correlation with psoriasis severity is still debated, and it has been demonstrated only in a few studies.27 Its potential role as a predictor of treatment response, however, has been rarely explored, and no significant correlation was found in the study by Kearney et al.32 Furthermore, the association we found in the univariate analysis was not confirmed after adjusting for the variables considered in the multivariate analysis.
Age emerged as a negative predictor of PASI100 response at week 28 in the GUIDE study33 and at week 20 in a large Italian multicenter retrospective study.22 While these findings contrast with our results, it is worth noting that in the GUIDE study, the difference in the prevalence of super responders versus non–super responders among patients aged over 65 years was more pronounced in the subgroup with psoriasis duration ≤2 years (2.6% vs 10.0%) than in those with longer disease duration (4.8% vs 7.7%). This observation suggests that age may have a greater impact in patients with shorter disease duration and a less considerable influence in those with longer disease duration (as the patients in our study). Notably, in both the Italian multicenter study and in our analysis, age was not retained as an independent predictor of PASI100 response in the multivariate model. Therefore, the true influence of age on the likelihood of achieving complete clearance either in the short or in the long term remains uncertain and should be interpreted with caution.
Obesity and higher BMI have consistently emerged as predictors of reduced treatment response across multiple studies.22,33–36 From an immunological standpoint, this association may be explained by the observation that obese individuals exhibit elevated levels of IL-23,37,38 largely due to increased production by subcutaneous adipocytes in response to insulin stimulation.9 Insulin levels tend to be higher in obese patients, particularly those with metabolic syndrome or insulin resistance.39
Regarding the association between a family history (FH) of psoriasis and PASI90 and PASI100 responses, our findings are consistent with existing literature. FH has been associated with better short-term treatment outcomes,40 fewer biologic switches,41 and longer drug survival.42 These observations may reflect underlying differences in the inflammatory burden between patients with and without a family history of psoriasis.
Explaining the association between short-term PASI90 responses and chronic beta-blocker use is more challenging. Several studies have reported a link between beta-blockers and both de novo psoriasis and psoriasis flares,43 and a recent meta-analysis confirmed an increased incidence of psoriasis among beta-blocker users.44 While the underlying mechanisms remain incompletely understood, one study demonstrated that propranolol can enhance IL-23 secretion by monocyte-derived Langerhans cells and promote Th17 differentiation from naïve CD4⁺ T cells.45
We speculate that psoriasis in beta-blocker users may be more dependent on IL-23–driven pathways. Consequently, targeting IL-23 in this subgroup might result in a more pronounced therapeutic response compared to patients with less IL-23-centric inflammation.
The relationship between Non-Steroidal Anti-Inflammatory Drugs (NSAIDs) and psoriasis has been investigated in several studies.46 Among these, Wu et al found no association between regular aspirin use and the risk of developing psoriasis in a large cohort.47 Interestingly, psoriasis patients appear to exhibit increased platelet COX-1 mRNA expression, which correlates with both PASI scores and circulating IL-17A levels.48 These findings suggest that platelets may contribute to psoriatic inflammation, and that aspirin could exert anti-inflammatory effects by directly targeting this component of the inflammatory cascade.
Features Influencing Safety
The association between the onset of paradoxical eczemas and acute urticaria with elevated peripheral eosinophil counts and higher ELR is not unexpected, as both markers are correlated with atopic dermatitis,49 a known risk factor for paradoxical eczema during biologic therapy.50 Moreover, both conditions share a predominant Th2 immune signature.51
The only variable associated with the new diagnosis of a previously undetected neoplasm in our cohort was the chronic use of angiotensin receptor blockers (ARBs). While a large population-based study found no significant association between ARB use and cancer incidence,52 a separate multicenter retrospective study suggested a potential protective effect of this antihypertensive class.53 Given these conflicting findings, our results should be interpreted with caution, particularly in light of the low number of events, which precluded multivariate analysis.
Furthermore, although the frequency of new cancer diagnoses in our study population might initially appear alarming, our results do not markedly differ from the reported incidence of malignancies in older adults,54,55 particularly considering that patients with moderate-to-severe psoriasis have an increased relative risk of developing cancer.56
Clinical Implications for the Practicing Physician
As elderly and frail patients are rarely included in clinical trials, information about the safety of psoriasis biological treatments in this special population mainly derives from real world experiences. In our study, guselkumab demonstrated a good safety profile and effectiveness, supporting its use as a valid therapeutic option in older adults.
Because elderly patients are often affected by multimorbidity and chronic polypharmacy, a thorough assessment of concomitant medications is essential before initiating biologic therapy. In our study, chronic use of beta-blockers and low-dose aspirin emerged as independent predictors of long-term effectiveness at week 52. Clinicians should be aware that patients taking these drugs might achieve better sustained responses and be more likely to reach complete or near-complete psoriasis clearance under guselkumab treatment.
Conversely, obese patients may show a less pronounced clinical response to guselkumab, and other biologics classes (eg IL-17-inhibitors) might represent effective options in this subgroup. However, due to its favorable safety profile, guselkumab might be preferred in clinically complex patients regardless of their BMI. In this last case, weight loss might be further encouraged in obese patients as an intervention favoring treatment effectiveness and thus improving quality of life, especially in patients with a high baseline Dermatology Life Quality Index (DLQI).
Finally, a positive family history of psoriasis should be noted during clinical assessment, as these patients may experience greater benefits from guselkumab therapy.
These practical considerations may help dermatologists tailor therapeutic decisions for elderly patients with psoriasis, although the findings should be interpreted with caution given the retrospective design and limited sample size of the study.
Limitations
The main limitations of the present study are inherent to its retrospective nature and the relatively small sample size, which may have limited the statistical power to detect additional predictors of treatment response. Moreover, the presence of some missing data could have affected the completeness of the longitudinal analyses. Furthermore, while the majority of the included patients were of Caucasian background, no information on racial or ethnic background was collected or considered in our analysis, thereby limiting the generalizability of our results. Finally, no statistical analysis was conducted regarding longer-term outcomes (ie, predictors of response maintenance at week 104) due to the low number of patients with adequate follow-up.
Conclusions
Our study confirms the effectiveness and safety profile of guselkumab in older adults with psoriasis in a real-world setting. Short term achievement of PASI90 and PASI100 was positively influenced by higher baseline PASI scores and higher ELR, while long-term PASI90 and PASI100 responses were positively associated with the daily intake of beta-blockers and low-dose aspirin, a positive family history of psoriasis and having achieved PASI100 at week 16.
Collectively, this real-world study confirms that guselkumab, is highly effective and safe in elderly patients with psoriasis, supporting the use of this biologic agent in this population. Future prospective studies on larger cohorts are warranted to confirm and further elucidate these findings.
Data Sharing Statement
All the data are contained in the manuscript.
Consent Statement
Consent to Publication form has been signed by the patients included in this study.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Parisi R, Iskandar IYK, Kontopantelis E, Augustin M, Griffiths CEM, Ashcroft DM. National, regional, and worldwide epidemiology of psoriasis: systematic analysis and modelling study. BMJ. 2020;369:m1590. doi:10.1136/bmj.m1590
2. Damiani G, Bragazzi NL, Karimkhani Aksut C, et al. The global, regional, and national burden of psoriasis: results and insights from the global burden of disease 2019 study. Front Med. 2021;8:743180. doi:10.3389/fmed.2021.743180
3. Drewitz KP, Stark KJ, Zimmermann ME, Heid IM, Apfelbacher CJ. Frequency of atopic dermatitis and psoriasis in the elderly: cross-sectional findings from the German AugUR study. Dermatology. 2025;241(1):1–9. doi:10.1159/000541590
4. Armstrong AW, Mehta MD, Schupp CW, et al. Psoriasis prevalence in adults in the United States. JAMA Dermatol. 2021;157(8):940–946. doi:10.1001/jamadermatol.2021.2007
5. Statista Research Department. Projected world population distribution, by age group 2100. Statista. 2025. Available from: https://www.statista.com/statistics/672546/projected-world-population-distribution-by-age-group/.
6. Chowdhury SR, Chandra Das D, Sunna TC, Beyene J, Hossain A. Global and regional prevalence of multimorbidity in the adult population in community settings: a systematic review and meta-analysis. EClinicalMedicine. 2023;57:101860. doi:10.1016/j.eclinm.2023.101860
7. Hacınecipoğlu F, Çelik G, Kartal SP. Efficacy and safety of IL-17 and IL-23 inhibitors in elderly patients with plaque psoriasis: a real-world study. J Dermatol. 2025;52(7):1166–1174. doi:10.1111/1346-8138.17755
8. Kurauti MA, Soares GM, Marmentini C, Bronczek GA, Branco RCS, Boschero AC. Insulin and aging. Vitam Horm. 2021;115:185–219.
9. Di Vincenzo A, Granzotto M, Crescenzi M, et al. Insulin stimulates IL-23 expression in human adipocytes: a possible explanation for the higher prevalence of psoriasis in obesity. Diabetes Metab Syndr Obes. 2023;16:1885–1893. doi:10.2147/DMSO.S405374
10. Fukasawa T, Yamashita T, Enomoto A, et al. The optimal use of tildrakizumab in the elderly via improvement of Treg function and its preventive effect of psoriatic arthritis. Front Immunol. 2023;14:1286251. doi:10.3389/fimmu.2023.1286251
11. Talamonti M, Russo F, Malara G, et al. Efficacy and safety of secukinumab in elderly patients with moderate to severe plaque-type psoriasis: post-hoc analysis of the SUPREME study. Clin Cosmet Investig Dermatol. 2023;16:847–852. doi:10.2147/CCID.S400520
12. Fratton Z, Maione V, Bighetti S, et al. Real-world Experience of bimekizumab in an elderly patients cohort with plaque-type psoriasis: a 24-week retrospective study. Clin Cosmet Investig Dermatol. 2024;17:2177–2181. doi:10.2147/CCID.S487869
13. Orsini D, Megna M, Assorgi C, et al. Efficacy and Safety of bimekizumab in elderly patients: real-world multicenter retrospective study - IL PSO (Italian landscape psoriasis). J Dermatolog Treat. 2024;35(1):2393376. doi:10.1080/09546634.2024.2393376
14. Orsini D, Graceffa D, Burlando M, et al. Effectiveness, speed of action and safety of brodalumab in elderly psoriasis patients: a multicenter real-world study - IL PSO (Italian landscape psoriasis). J Dermatolog Treat. 2025;36(1):2452948. doi:10.1080/09546634.2025.2452948
15. Orsini D, Caldarola G, Dattola A, et al. Efficacy and safety of tildrakizumab in elderly patients: real-world multicenter study (ESTER - study). J Dermatolog Treat. 2024;35(1):2319304. doi:10.1080/09546634.2024.2319304
16. Ruggiero A, Fabbrocini G, Cinelli E, et al. Anti-interleukin-23 for psoriasis in elderly patients: guselkumab, risankizumab and tildrakizumab in real-world practice. Clin Exp Dermatol. 2022;47(3):561–567. doi:10.1111/ced.14979
17. Gisondi P, Fargnoli MC, Amerio P, et al. Italian adaptation of EuroGuiDerm guideline on the systemic treatment of chronic plaque psoriasis. Ital J Dermatol Venerol. 2022;157(Suppl. 1 to No. 1):1–78. doi:10.23736/S2784-8671.21.07132-2
18. Ter Haar ELM, den Reek JMPA V, Gaarn Du Jardin K, et al. Efficacy and safety of tildrakizumab in older patients: pooled analyses of two randomized phase iii clinical trials (reSURFACE 1 and reSURFACE 2) through 244 weeks. Acta Derm Venereol. 2023;103:17752. doi:10.2340/actadv.v103.17752
19. Fiorillo G, Ibba L, Gargiulo L, et al. Effectiveness and safety of anti-IL-23 and anti-IL-17 biological therapies for psoriasis in elderly patients: real-world experience from two Italian hospitals. J Eur Acad Dermatol Venereol. 2023;37(12):e1444–e1446. doi:10.1111/jdv.19355
20. Phan C, Beneton N, Delaunay J, et al. Effectiveness and safety of anti-interleukin-17 therapies in elderly patients with psoriasis. Acta Derm Venereol. 2020;100(18):adv00316. doi:10.2340/00015555-3678
21. Sbidian E, Chaimani A, Garcia-Doval I, et al. Systemic pharmacological treatments for chronic plaque psoriasis: a network meta-analysis. Cochrane Database Syst Rev. 2022;5(5):CD011535. doi:10.1002/14651858.CD011535.pub5
22. Mortato E, Talamonti M, Marcelli L, et al. Predictive factors for super responder status and long-term effectiveness of guselkumab in psoriasis: a multicenter retrospective study. Dermatol Ther. 2025;15(5):1239–1250. doi:10.1007/s13555-025-01394-2
23. Sobotkova T, Hugo J, Salavec M, et al. Efficacy, safety, and drug survival during the first year of biologic therapy for psoriasis in elderly versus younger patients. Int J Dermatol. 2025;64(8):1401–1408. doi:10.1111/ijd.17814
24. Norlin JM, Nilsson K, Persson U, Schmitt-Egenolf M. Complete skin clearance and psoriasis area and severity index response rates in clinical practice: predictors, health-related quality of life improvements and implications for treatment goals. Br J Dermatol. 2020;182(4):965–973. doi:10.1111/bjd.18361
25. Tada Y, Sugiura Y, Kamishima M, et al. Real-world safety and effectiveness of guselkumab in patients with psoriasis: a post-marketing surveillance study through up to week 52 in Japan. J Dermatol. 2025;52(6):967–982. doi:10.1111/1346-8138.17710
26. Seidl U, Pinter A, Wilsmann-Theis D, et al. Absolute psoriasis area and severity index as a valuable marker to determine initial treatment response in psoriasis patients treated with guselkumab in routine clinical care. Dermatol Ther. 2022;35(1):e15193. doi:10.1111/dth.15193
27. Weissmann S, Babyev AS, Gordon M, et al. Association of hematological ratios with psoriasis: a nationwide retrospective cohort study. Int J Dermatol. 2024;63(10):1369–1374. doi:10.1111/ijd.17133
28. Guerra ES, Lee CK, Specht CA, et al. Central role of IL-23 and IL-17 producing eosinophils as immunomodulatory effector cells in acute pulmonary aspergillosis and allergic asthma. PLoS Pathog. 2017;13(1):e1006175. doi:10.1371/journal.ppat.1006175
29. Kim HJ, Roh JY, Jung Y. Eosinophils accelerate pathogenesis of psoriasis by supporting an inflammatory milieu that promotes neutrophil infiltration. J Invest Dermatol. 2018;138(10):2185–2194. doi:10.1016/j.jid.2018.03.1509
30. Langewouters AM, van Erp PE, de Jong EM, et al. Lymphocyte subsets in peripheral blood of patients with moderate-to-severe versus mild plaque psoriasis. Arch Dermatol Res. 2008;300(3):107–113. doi:10.1007/s00403-007-0819-9
31. Ye JH, Zhang Y, Naidoo K, et al. Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio in psoriasis: a systematic review and meta-analysis. Arch Dermatol Res. 2024;316(3):85. doi:10.1007/s00403-024-02823-6
32. Kearney N, Gorecki P, Acciarri L, et al. Treatment of plaque psoriasis with guselkumab reduces systemic inflammatory burden as measured by neutrophil/lymphocyte ratio, platelet/lymphocyte ratio, and monocyte/lymphocyte ratio: a post hoc analysis of three randomised clinical trials. Dermatology. 2025;241(3):272–286. doi:10.1159/000545148
33. Schäkel K, Reich K, Asadullah K, et al. Early disease intervention with guselkumab in psoriasis leads to a higher rate of stable complete skin clearance (‘clinical super response’): week 28 results from the ongoing phase IIIb randomized, double-blind, parallel-group. GUIDE Study. J Eur Acad Dermatol Venereol. 2023;37(10):2016–2027. doi:10.1111/jdv.19236
34. Reich K, Gordon KB, Strober B, et al. Super-response to guselkumab treatment in patients with moderate-to-severe psoriasis: age, body weight, baseline psoriasis area and severity index, and baseline investigator’s global assessment scores predict complete skin clearance. J Eur Acad Dermatol Venereol. 2022;36(12):2393–2400. doi:10.1111/jdv.18474
35. Gargiulo L, Ibba L, Malagoli P, et al. Real-life effectiveness and safety of guselkumab in patients with psoriasis who have an inadequate response to ustekinumab: a 104-week multicenter retrospective study - IL PSO (Italian LANDSCAPE PSORIASIS). J Eur Acad Dermatol Venereol. 2023;37(5):1017–1027. doi:10.1111/jdv.18913
36. Del Alcázar E, López-Ferrer A, Martínez-Doménech Á, et al. Effectiveness and safety of guselkumab for the treatment of psoriasis in real-world settings at 24 weeks: a retrospective, observational, multicentre study by the Spanish Psoriasis Group. Dermatol Ther. 2022;35(2):e15231. doi:10.1111/dth.15231
37. Sumarac-Dumanovic M, Stevanovic D, Ljubic A, et al. Increased activity of interleukin-23/interleukin-17 proinflammatory axis in obese women. Int J Obes (Lond). 2009;33(1):151–156. doi:10.1038/ijo.2008.216
38. Pirowska M, Obtułowicz A, Lipko-Godlewska S, et al. The level of proinflammatory cytokines: interleukins 12, 23, 17 and tumor necrosis factor α in patients with metabolic syndrome accompanying severe psoriasis and psoriatic arthritis. Postepy Dermatol Alergol. 2018;35(4):360–366. doi:10.5114/ada.2018.77665
39. Guilherme A, Virbasius JV, Puri V, et al. Adipocyte dysfunctions linking obesity to insulin resistance and type 2 diabetes. Nat Rev Mol Cell Biol. 2008;9(5):367–377. doi:10.1038/nrm2391
40. Jiang Y, Liu X, Ma R, et al. The impact of family history on clinical presentation and biologic treatment response in patients with psoriasis: a multicenter prospective cohort study. Am J Clin Dermatol. 2025;26(2):291–300. doi:10.1007/s40257-025-00918-y
41. Manzo Margiotta F, Michelucci A, Panduri S, et al. Family history of psoriasis: a novel protective factor for therapy switch in patients treated with secukinumab or ixekizumab. J Eur Acad Dermatol Venereol. 2022;36(6):e454–e456. doi:10.1111/jdv.17944
42. Torres T, Puig L, Vender R, et al. Drug survival of interleukin (IL)-17 and IL-23 inhibitors for the treatment of psoriasis: a retrospective multi-country, multicentric cohort study. Am J Clin Dermatol. 2022;23(6):891–904. doi:10.1007/s40257-022-00722-y
43. Kim YE, Cho Y, Jo SJ. Risk of de novo psoriasis in hypertension patients initially treated with beta-blockers: nationwide population-based cohort study in Korea. J Eur Acad Dermatol Venereol. 2022;36(3):e202–e205. doi:10.1111/jdv.17733
44. Song G, Yoon HY, Yee J, et al. Antihypertensive drug use and psoriasis: a systematic review, meta- and network meta-analysis. Br J Clin Pharmacol. 2022;88(3):933–941. doi:10.1111/bcp.15060
45. Müller G, Lübow C, Weindl G. Lysosomotropic beta blockers induce oxidative stress and IL23A production in Langerhans cells. Autophagy. 2020;16(8):1380–1395. doi:10.1080/15548627.2019.1686728
46. Balak DMW, Hajdarbegovic E. Do NSAIDs trigger or exacerbate psoriasis?. Psoriasis. 2024;14:121–122. doi:10.2147/PTT.S496118
47. Wu S, Han J, Qureshi AA. Use of aspirin, non-steroidal anti-inflammatory drugs, and acetaminophen (paracetamol), and risk of psoriasis and psoriatic arthritis: a cohort study. Acta Derm Venereol. 2015;95(2):217–223. doi:10.2340/00015555-1855
48. Garshick MS, Tawil M, Barrett TJ, et al. Activated platelets induce endothelial cell inflammatory response in psoriasis via COX-1. Arterioscler Thromb Vasc Biol. 2020;40(5):1340–1351. doi:10.1161/ATVBAHA.119.314008
49. Zeng-Yun-Ou Z, Zhong-Yu J, Wei L. Bidirectional associations between eosinophils, basophils, and lymphocytes with atopic dermatitis: a multivariable Mendelian randomization study. Front Immunol. 2022;13:1001911. doi:10.3389/fimmu.2022.1001911
50. Al-Janabi A, Alabas OA, Yiu ZZN, et al. Risk of Paradoxical eczema in patients receiving biologics for psoriasis. JAMA Dermatol. 2024;160(1):71–79. doi:10.1001/jamadermatol.2023.4846
51. Chen Q, Zhong H, Chen WC, et al. Different expression patterns of plasma Th1-, Th2-, Th17- and Th22-related cytokines correlate with serum autoreactivity and allergen sensitivity in chronic spontaneous urticaria. J Eur Acad Dermatol Venereol. 2018;32(3):441–448. doi:10.1111/jdv.14541
52. Franchi M, Torrigiani G, Kjeldsen SE, et al. Long-term exposure to antihypertensive drugs and the risk of cancer occurrence: evidence from a large population-based study. J Hypertens. 2024;42(12):2107–2114. doi:10.1097/HJH.0000000000003841
53. Dagher YG, El Helou S, Haifa KG, et al. The association between angiotensin receptor blockers and lung, bladder, and colon cancer development: a 10-year multicentric retrospective Lebanese study. Medicine (Baltimore). 2023;102(36):e34901. doi:10.1097/MD.0000000000034901
54. Xiang D, Hu S, Mai T, et al. Worldwide cancer statistics of adults over 75 years old in 2019: a systematic analysis of the global burden of disease study 2019. BMC Public Health. 2022;22(1):1979. doi:10.1186/s12889-022-14412-1
55. Xu J, Liao J, Yan Q, et al. Trends analysis of cancer incidence, mortality, and survival for the elderly in the United States, 1975-2020. Cancer Med. 2024;13(15):e70062. doi:10.1002/cam4.70062
56. Trafford AM, Parisi R, Kontopantelis E, Griffiths CEM, Ashcroft DM. Association of psoriasis with the risk of developing or dying of cancer: a systematic review and meta-analysis. JAMA Dermatol. 2019;155(12):1390–1403. doi:10.1001/jamadermatol.2019.3056
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Relative Safety and Efficacy of Two Doses of Tandospirone Citrate for Generalized Anxiety Disorder: A Multicenter Randomized Controlled Trial
Li Q, Zhang H, Lin G, Shi S, Zhang Y, Ji J, Yang L, Yao J, Wu W
Neuropsychiatric Disease and Treatment 2022, 18:1653-1664
Published Date: 8 August 2022
Biosimilars: Science, Implications, and Potential Outlooks in the Middle East and Africa
Batran RA, Elmoshneb M, Hussein AS, Hussien OM, Adel F, Elgarhy R, Morsi MI
Biologics: Targets and Therapy 2022, 16:161-171
Published Date: 6 October 2022
Efficacy and Safety of TKI Plus PD-1 Inhibitors in Elderly uHCC Patients: A Retrospective Study
Chen B, Lei J, Zhao H, Dong J, Zeng Z, Li Y, Yu L, Zhou L, Jia A, Lu Y, Cheng J
Journal of Hepatocellular Carcinoma 2022, 9:1171-1185
Published Date: 8 November 2022
Current Insights into the Risks of Using Melatonin as a Treatment for Sleep Disorders in Older Adults
Tuft C, Matar E, Menczel Schrire Z, Grunstein RR, Yee BJ, Hoyos CM
Clinical Interventions in Aging 2023, 18:49-59
Published Date: 12 January 2023
Clinical Evaluation of Risankizumab in the Treatment of Adults with Moderately to Severely Active Crohn’s Disease: Patient Selection and Reported Outcomes
Horst S, Cross RK
Drug Design, Development and Therapy 2023, 17:273-282
Published Date: 31 January 2023