Back to Journals » Clinical Interventions in Aging » Volume 18
Current Insights into the Risks of Using Melatonin as a Treatment for Sleep Disorders in Older Adults
Authors Tuft C, Matar E, Menczel Schrire Z, Grunstein RR, Yee BJ, Hoyos CM ![]()
Received 10 August 2022
Accepted for publication 19 December 2022
Published 12 January 2023 Volume 2023:18 Pages 49—59
DOI https://doi.org/10.2147/CIA.S361519
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Colin Tuft,1 Elie Matar,2 Zoe Menczel Schrire,2 Ronald R Grunstein,2,3 Brendon J Yee,1– 3 Camilla M Hoyos2,4
1Department of Respiratory and Sleep Medicine, Royal Prince Alfred Hospital, Sydney, NSW, Australia; 2Centre for Sleep and Chronobiology, Woolcock Institute of Medical Research, Sydney Medical School, Sydney, NSW, Australia; 3Central Clinical School, Faculty of Medicine and Health, University of Sydney, Sydney, NSW, Australia; 4School of Psychology, Faculty of Science, The University of Sydney, Sydney, NSW, Australia
Correspondence: Camilla M Hoyos, Centre for Sleep and Chronobiology, Woolcock Institute of Medical Research, Sydney Medical School, Sydney, NSW, Australia, Tel +61 2 9114 0409, Email [email protected]
Abstract: Exogenous melatonin is commonly used for sleep disorders in older adults, and its use is increasing over time. It appears to have modest efficacy in treating insomnia and circadian rhythm sleep-wake disorders. Melatonin is commonly perceived to be a safe alternative to other hypnotics and is available without prescription in some jurisdictions. New evidence suggests that endogenous melatonin has pleomorphic effects on multiple organ systems, many of which are poorly understood. This narrative review summarizes the current evidence regarding the safety of melatonin in older adults (defined by age over 65 years). Melatonin appears to have a favorable safety profile in this population, however there is a dearth of evidence regarding the safety of prolonged use. There are several factors which increase the risk of adverse effects of melatonin in older adults, and these should be taken into consideration when prescribing to this population.
Keywords: adverse effect, safety, insomnia, elderly, sleep wake phase disorder
Introduction
Melatonin is one of the most widely used medications for sleep disorders that can be obtained without prescription in many countries.1,2 It is a synthetic version of the naturally occurring hormone which is primarily synthesized in the pineal gland from the precursor amino acid L-tryptophan and released into the third ventricle, subsequently reaching the systemic circulation. Melatonin synthesis and release is under the inhibitory control of the suprachiasmatic nucleus (SCN), which receives light input from retinal ganglion cells. Bright light suppresses melatonin secretion, which rises during the early evening, is maximal in the early hours of the night and falls to virtually undetectable levels in the early morning and during daylight hours.3 Melatonin is also produced in numerous other tissues apart from the pineal gland, including the thymus, gastrointestinal tract, as well as in innate and adaptive immune cells in the bone marrow and systemic circulation.4 Overall, the daily endogenous production of melatonin is relatively small (less than 100 µg) compared to the doses commonly administered exogenously.5
Melatonin’s primary function is regulation of the sleep-wake cycle. Highly sensitive melatonin receptors (MT1 and MT2) in the SCN and other areas of hypothalamus are primarily responsible for the effect of melatonin on sleep-wake rhythms. Melatonin receptors are also found throughout the brain and likely have other neurological effects beyond promoting sleep initiation. Recent research has suggested a role in regulating the stages of sleep, as well as affecting the duration and proportion of rapid-eye movement (REM) and non- rapid-eye movement (NREM) sleep.6 Furthermore, melatonin receptors have been found in numerous other tissues including adipose tissue, coronary arteries, alpha and beta pancreatic cells, myometrium and testis. Thus, exogenous melatonin could be expected to affect numerous other physiological processes in addition to regulation of sleep. Melatonin has also been shown to be a potent immunomodulatory hormone and antioxidant4 as well as reduce blood pressure,7 upregulate bone cell proliferation and inhibit bone resorption.8 Therapeutic strategies taking advantage of the diverse effects of melatonin remain an active area of academic inquiry.9
Several changes in sleep behavior and physiology occur with aging, though these can be difficult to decouple from concomitant pathology and medication effects. Ageing is associated with a reduction of total sleep time and an advancement in sleep phase, with peak sleepiness and wake times occurring earlier.10 Also, the proportion of slow wave or deep (N3) sleep is reduced, and arousals occur more frequently.11 Although initially contested, there is now growing evidence supporting a natural decline in peak melatonin secretion with age, which has been implicated as a mechanism for these observed changes12,13 Furthermore, sleep disorders are more common in older adults, with rates of insomnia rising dramatically with age. Insomnia symptoms have been reported in up to 50% of individuals over the age of 60, with rates of diagnosed insomnia disorder between 12% and 20%.14 Circadian rhythm sleep-wake phase disorders, especially advanced-sleep phase disorder, also occur more frequently in older persons.15 It is also well established that sleep-wake disturbance is a key feature of most neurodegenerative diseases including dementia, being present in up to 70% of patients with early dementia and 86% of patients with Parkinson’s disease.16,17
Exogenous melatonin has been well studied as pharmacotherapy for insomnia and circadian rhythm disorders in adults. It is taken orally and has oral bioavailability of 15% due to extensive first-pass metabolism, though this is highly variable. When prescribed as a hypnotic, it is usually taken 30 minutes before bedtime and is available as immediate, slow-release or a combined formulation.
In Europe and Australia, prolonged-release melatonin is available as an over-the-counter monotherapy for the short-term treatment of primary insomnia in patients aged 55 or over. Trials in adults have shown exogenous melatonin to have modest efficacy in primary insomnia, with an increase in total sleep time of 12.8 minutes, and a reduction in sleep latency of 4 minutes.18 A more pronounced effect has been observed in young adults with delayed sleep-wake phase disorder, with a dose of 0.5mg of melatonin advancing sleep by 34 minutes in a recent randomized controlled trial.19 Several smaller trials in adults over 55 years of age have shown modest improvements in sleep latency and subjective measures of sleep quality with doses of melatonin between 0.3 and 1mg.20–24 Some studies have claimed efficacy of melatonin in reducing the symptoms of REM sleep behavior disorder, however recent randomized control trials have not shown benefit.25,26 Melatonin is also prescribed to assist in withdrawing from hypnotic medications, although a systematic review revealed minimal efficacy.27 There is currently much interest in the use of melatonin for treating the sleep-related symptoms of neurodegenerative diseases and even potentially to prevent their development, though there is limited evidence for this at present.28
For these reasons, melatonin is one of the most commonly used medications for sleep disorders in older adults. The pattern of use of melatonin and regulations dictating its availability vary globally. Clinicians should consult local guidelines when considering prescribing melatonin. In the United States, melatonin is considered a dietary supplement and has been available without prescription since 1994. Substances classed as dietary supplements by the United States Food and Drug Administration are not assessed for safety or efficacy and are not subject to the same quality control requirements as those classed as medications. In most European countries and Australia, doses below a certain threshold are available without prescription but are regulated as medications by the relevant authorities. Regulations vary within Europe, but several countries classify products containing up to a certain dose of melatonin (usually 1mg) as a dietary supplement, with higher doses available over-the-counter or with a prescription. In the United Kingdom, it is available with prescription only, and, in Japan, it is not approved as a pharmaceutical. The use of melatonin is rising, with an increase in prevalence of use in the US in those 65 or older from 0.6% to 2.1% in the years from 1999 to 2018, and a similar trend in the UK.2,29
This review aims to summarize the current evidence for the safety of melatonin use for sleep disorders in older adults.
Search Methodology
This narrative review on the subject of “the risk of using melatonin as a treatment for sleep disorders in older adults” examined both primary and secondary sources of literature on the topic. PubMed, Web of Science and Google Scholar served as search engines and were used to access relevant literature. Key phrases used to conduct the literature search included “melatonin”, “elderly”, “older adults”, “sleep disorder”, “sleep-wake disorder”, “insomnia”, “dementia”, “adverse effects”, “adverse events” and “safety”.
Articles available on human studies in the English language, published within the last four decades, and articles focusing on melatonin, adverse effects, safety, insomnia and circadian rhythm disorders were included. We defined older adults as those over 65 years of age.
Results
General Safety Data
Our literature search found two recent systematic reviews on the safety of melatonin in the general population.30,31 In the analysis of safety data from randomized, placebo-controlled trials, minimal adverse effects were reported with both melatonin and placebo. A systematic review by Besag et al of randomized controlled trials including 2130 patients reported that the most common adverse effects (compared to placebo) were daytime sleepiness in 1.66%, headache in 0.74% and dizziness in 0.74%.31 The rates of adverse effects were more common with melatonin than placebo but were considered of minor clinical significance given the mild nature of reported symptoms. The mean age of participants was not able to be precisely determined but was in the 5th decade of life, with the doses of melatonin used between 0.15mg/day to 15mg/day. The majority of the included trials were of a short duration (<12 weeks) and thus give no evidence for long-term safety.
Trials performed without a placebo arm have naturally reported greater rates of adverse effects. However, a systematic review of such trials concluded that the rate of adverse events is similar to data from placebo-controlled studies, with the most commonly attributed adverse effects being headache and dizziness. The age of participants was between 20 and 80 years, and the doses of melatonin used varied from 0.13mg/day to 15mg/day. A systematic review by Foley et al including those with and without placebo arms reported at least one adverse effect potentially attributable to melatonin in 24 of the 50 trials studied.30 Such effects were generally mild and related to sleepiness or daytime performance and were considered related to daytime dosing of melatonin. The trials included in these reviews were of a longer duration (between 2 months and 12 years) and included patients between the ages of 1 and 80 years but with the majority in adults less than 65 years old. Doses of melatonin were mostly between 2 mg and 10 mg daily; however, exceptions to this ranged from 0.3mg to 1600mg daily. The authors concluded that there was no increased risk of adverse effects in the melatonin arms compared to placebo in the trials included in the analysis.
Post-marketing surveillance data provide longer-term evidence regarding melatonin safety in the general population. A report from Germany reported adverse effects in less than 10% of the 597 surveyed patients taking long-term controlled-release melatonin at a dose of 2mg. The most common adverse effects were nausea and dizziness, with less than 2% discontinuing treatment due to adverse effects.32 A much larger post-marketing study of almost 1 million adults reported a much lower rate of adverse effects of 0.008%, with headaches and dizziness being the most commonly reported.33
Melatonin appears to have a very low risk of dependence or withdrawal effects. However, there has been a case of an emergent movement disorder and agitation following melatonin withdrawal has been reported in a 22-year-old woman with severe deficits from cerebral palsy.34 There may be an increased risk of adverse neurological effects in those with significant organic brain injury, though to the authors’ knowledge no cases have been reported in studies of older adults with dementia.
There is a great variability in the doses of melatonin used in trials. A randomized controlled trial in children reported a greater rate of adverse effects with higher doses.35 However, a systematic review found no association between adverse effects and melatonin dose.31 A more recent systematic review into the safety of melatonin at doses in excess of 10mg/day found an increase in the rate of minor adverse effects such as drowsiness, headache and dizziness, but no increase in the rate of serious adverse effects in the four trials included in the meta-analysis.36 In the United States, the usage of melatonin at doses of 5mg/day or higher is increasing.2 Furthermore, there is much interest in higher doses of melatonin as therapy or prevention of neurodegenerative diseases, with some mouse models using doses equivalent to 600mg/day in humans.37 Given the evidence for higher rates and severity of adverse effects at doses in excess of 10mg/day, appropriate scrutiny should be employed in trials using higher doses in older adults.
There are fewer randomized, placebo-controlled trials of melatonin specifically in older adults. The indications for melatonin in these studies are more varied and include patients without sleep disorders. Data from these trials generally report similar frequencies and types of adverse events to data from the general population. A large, 26-week randomized controlled trial of 791 patients with primary insomnia noted no increased rate of adverse effects compared to placebo.39 A 6-month study of patients with Alzheimer’s disease reported an increased rate of diarrhea (4.4%) and respiratory tract infection (3.7%) in those taking melatonin, though these were not considered to be related to treatment.40 An 8-week trial of melatonin for REM-behavior disorder in 30 patients with Parkinson’s Disease with a mean age of 65 noted adverse events including headaches, fatigue, lightheadedness, and morning sleepiness, but with similar rates to placebo.41 No statistically significant differences in the number of adverse effects reported between the melatonin and placebo groups were observed in a 3-month trial of 25mg melatonin to prevent depression following acute coronary syndrome involving 252 patients over 60 years of age.
A Cochrane review of the efficacy and safety of pharmacotherapies in dementia provides the most detailed analysis of safety data in older adults,38 This review included two trials of 164 patients over the age of 52 with detailed safety data. It concluded with low certainty that there was no difference in rates of adverse events between the melatonin and placebo arms (mean difference 0.2 events/person).
Three other systematic reviews of melatonin in older adults were found in our literature review, though none specifically investigated for adverse effects. The review by Vural et al examined 16 studies of patients over 55 years of age and concluded that the effects of melatonin were mainly positive, though no specific analysis of adverse events was performed.42 A review of four randomized controlled trials in 243 patients over 77 years of age with dementia noted no adverse effects.43 A third by Almond et al found one case of increased sedation with melatonin and two self-limiting cases of pruritus in their analysis of three randomized controlled trials, but minimal other adverse effects.44 No systematic reviews specifically on the topic of adverse effects of melatonin in older adults were found.
Evidence from randomized control trials suggests that melatonin may have a mildly increased rate of minor adverse effects, but there is a dearth of long-term safety data in older adults. A summary of the most important systematic reviews is provided in Table 1.
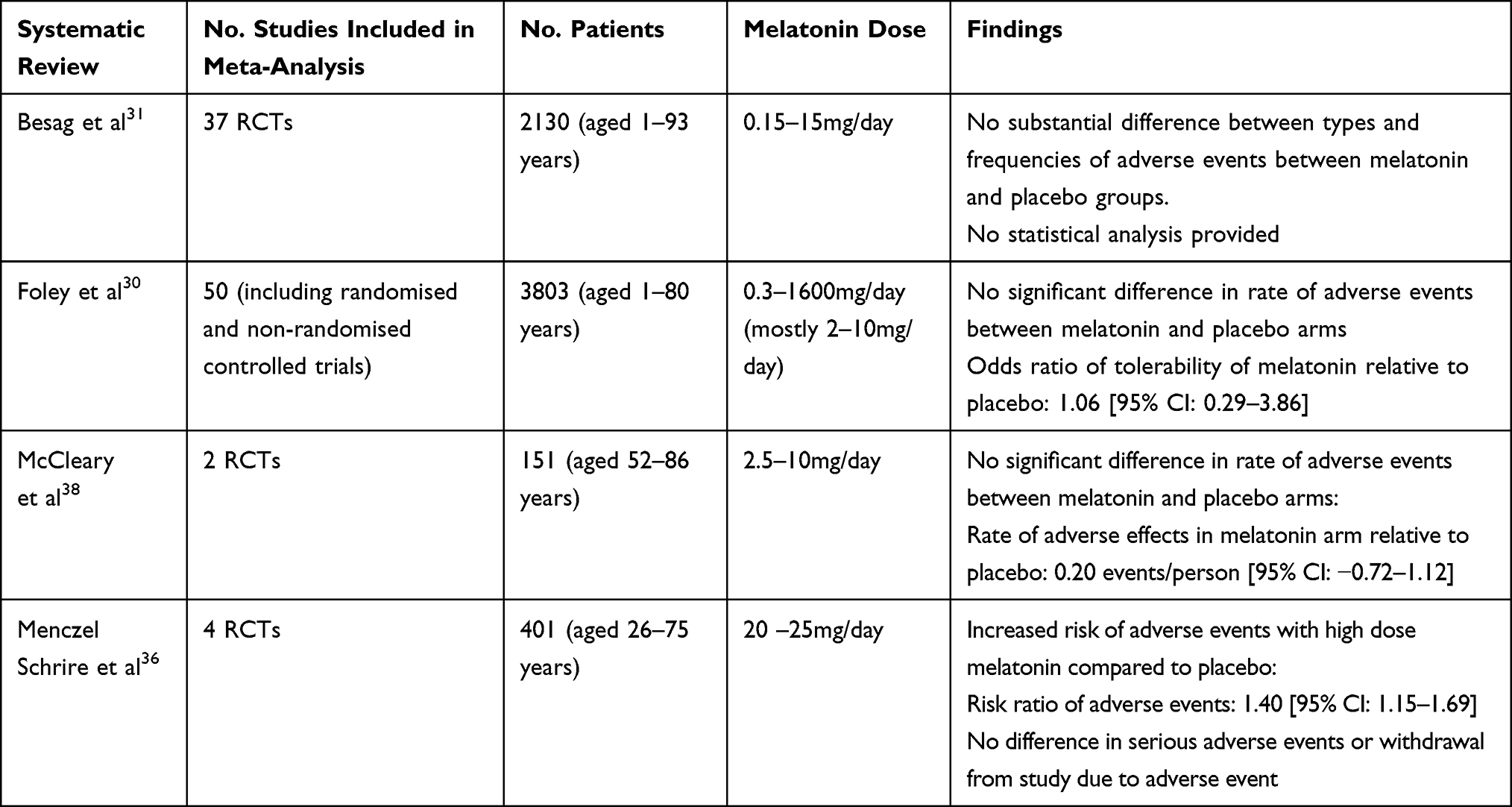 |
Table 1 Summary of Meta-Analysis Findings Regarding the Safety of Melatonin |
Regulation of Melatonin
In countries where melatonin is available as a dietary supplement, there is a risk of inappropriate use and a lack of medical supervision for potential adverse effects. The majority of melatonin consumption in the US and a substantial proportion in Europe is in the form of a dietary supplement.2
Pharmacological agents categorized as dietary supplements are not subject to the same quality control and regulatory scrutiny as medicines, whether prescribed or over the counter. There is a risk of poor quality-control resulting in inaccurate dosing and formulation of the active ingredients, as well as the presence of active contaminants. A study of 31 supplements containing melatonin in Canada found a measured content of −83% to +478% of the labeled melatonin dose. There was variability in content within the same product of up to 465%.45 In addition, a pharmacologically active contaminant, serotonin, was found in eight of the supplements.
There is no post-marketing surveillance performed by regulatory bodies for adverse effects of dietary supplements. Adverse events from particular formulations and products are thus less likely to be reported. The safety data presented in this paper relate to products containing melatonin, which has been regulated as a medicine, not a dietary supplement (with the exception of the telephone survey by Brodner et al). Physicians should caution patients to purchase melatonin in a form that is regulated as a medicine to avoid under- or over-dosing and potential exposure to contaminants.
Pharmacokinetics and Pharmacodynamics
Several melatonin formulations are available, including extended-release, immediate-release and combined immediate and extended-release. Melatonin has demonstrated substantial variability in bioavailability, primarily due to first-pass metabolism and poor absorption. Absorption is also affected by food. Studies in healthy adults have reported bioavailability ranging from 1% to 37%.46–48 Food delays the absorption of melatonin, with the time of peak concentration increasing from 0.75 hours in a fasted state to 3 hours when taken with food. Peak concentrations after oral administration have been reported as substantially higher in older adults, up to 240% greater than in adults under the age of 45 years.42,49 Other studies have found lower peak serum concentrations but approximately 50% higher mean concentrations with a greater variability in those aged 50 years and above.50 It is reasonable to expect that the same dose administered to an older individual would have more pronounced effects. Combined with the variation in bioavailability, there is a compounded risk of unpredictable serum concentration. This may result in an increased variability and risk of other adverse effects in older adults.
Melatonin is metabolized by the liver via the cytochrome-P450 enzymes CYP1A1, CYP1A2 and CYP2C19 enzymes to form 6-hydroxymelatonin and is finally excreted as 6-glucuronylmelatonin and 6-hydroxymelatonin via the kidneys. Clearance of melatonin is reduced in the presence of liver disease, although most research has been in cirrhotic patients.51,52 There is little evidence of the effects of chronic liver disease on melatonin metabolism in older adults.
Drug Interactions
Melatonin is metabolized by the same enzymes as many drugs commonly prescribed in older adults. The magnitude of interactions appears to be quite variable, and only a small fraction of potential interactions have been studied.
Several selective serotonin reuptake inhibitors have been shown to substantially increase serum melatonin concentrations including fluvoxamine and citalopram. These medications are commonly prescribed in older adults and have been found to be used by 20% of older patients in nursing homes.53 Fluvoxamine has been shown to result to increase maximum serum concentrations by a factor of 2.8 to 12.54,55 Citalopram on its own does not appear to increase melatonin concentration. However, citalopram when given with a proton-pump inhibitor (both CYP2C19 substrates) has been shown to double the concentration of melatonin metabolites in the urine.56 Nortriptyline is an even more potent inhibitor of CYP2C19 and is expected to have a significant interaction with melatonin, though no in vitro studies have been performed. A case of severe sedation after commencing melatonin in a patient taking oxycodone, citalopram and nortriptyline has been reported.57 There appears to be a significant risk of adverse effects with concomitant use of melatonin and antidepressants. The high prevalence of use of these medications and the high incidence of polypharmacy in older adults increases this risk further. Careful interaction checking, low initial doses of melatonin and close monitoring for adverse effects after initiation should be performed in this population.
Melatonin has been shown to reduce the efficacy of the calcium channel blocker nifedipine. A dose of 5mg of melatonin for four weeks in those taking nifedipine resulted in an increase in systolic and diastolic blood pressure of 6.5 and 4.5 mmHg, respectively.58 Interactions with other antihypertensives have not been reported. Given the blood-pressure lowering effect of melatonin, there is a potential for unpredictable changes in blood pressure with the addition of melatonin to older adult patients taking antihypertensive medications. Monitoring for changes in blood pressure should be performed after commencing melatonin in such a population, in order to avoid increasing cardiovascular risk or the possibility of presyncope and falls.
Another potentially significant interaction is between melatonin and warfarin. There is some evidence that concomitant administration of melatonin and warfarin increases the prothrombin time and international normalized ratio, particularly in older adults. There are case reports of increased bleeding in patients taking both melatonin and warfarin, though no life-threatening bleeding has been reported.59 Clinicians should consider increased frequency of monitoring of coagulation for patients taking this combination.
There is a risk of compound effects with co-administration of melatonin with other sedatives. A study in middle-older aged adults found that melatonin potentiated the effect of zolpidem in impairing psychomotor function and driving skills.60 Concomitant administration of caffeine with melatonin in younger adults has been shown to increase maximum concentrations of melatonin by 42%, presumably due to the effect of inhibition of the CYP1A2 enzyme on first-pass metabolism.61
Sedation, Cognition and Psychiatric Risks
As melatonin is used primarily as a hypnotic agent, there is a concern that it may be associated with sedation and impaired functional and cognitive performance. Other hypnotic agents can cause sedation the following morning: the so-called “next-day hangover” effect. Numerous trials have evaluated for this as an expected adverse effect of melatonin. There are occasional reports of impaired daytime performance, though these mostly occur with daytime administration and resolve with a change in the timing of dosing.31,62
Three randomized controlled trials reported increased subjective sleepiness with melatonin compared to placebo at doses between 2mg and 100mg, without impairment of psychomotor performance.63 Numerous small trials have reported sedation as an adverse effect, though the prevalence varies greatly. Systematic reviews of studies primarily involving younger individuals reported rates of increased sedation in 1.66% of patients compared to placebo, though this was not considered significant.30,31 It is not clear if this was related to early administration of melatonin. Short- and long-term studies (duration of 3 weeks or less) in older adult patients with delirium and insomnia have not reported significant sedation in the treatment arms.21,22,40,43,64–67
Worsening of insomnia symptoms after sudden withdrawal of sleep-promoting agents (so-called rebound insomnia) has been reported with benzodiazepines and “Z-drugs” such as zolpidem.68 This phenomenon has not been reported in large randomized trials of melatonin. A three-week trial in 170 patients aged over 55, specifically evaluating for rebound insomnia with a withdrawal phase, found no evidence of increased sleep disturbance after cessation of therapy.21
Melatonin has been studied as a treatment for depression in conjunction with traditional pharmacotherapy. Systematic reviews in patients aged between 18 and 90 years have found no significant therapeutic or adverse effect of melatonin in depression.69 No other psychiatric adverse effects have been associated with melatonin in systematic reviews.31
Cardiovascular Risks
There is increasing interest into the potential cardioprotective effects of melatonin. Slow-release melatonin has been shown to have an antihypertensive effect, with a meta-analysis reporting fall in blood pressure of 6.1mmHg.70 Melatonin has been shown to have an unpredictable effect on the diurnal variation of blood pressure.71 While further research may find a therapeutic use for this effect, it may be prudent to monitor blood pressure after commencement of melatonin to avoid hypotension. Palpitations were reported by a 68-year-old participant in a study of prolonged-release melatonin and were considered possibly drug-related.64
Systematic reviews have not found a significant increase in major cardiovascular events with melatonin use.30,31,36 However, older adult populations are rarely included in randomized controlled trials of melatonin, and the risk in this population is not well known.
Endocrine Risks
Melatonin has been demonstrated to have pleomorphic effects on the endocrine system.72–74 The minor effect of melatonin on levels of luteinizing hormone, follicle stimulating hormone, prolactin and growth hormone that have been demonstrated in younger adults are likely to be not clinically significant in older adults.
Exogenous melatonin at doses of 1–10mg has been shown to worsen glucose tolerance and insulin sensitivity compared to placebo in men as well as in pre- and post-menopausal women after a single dose and persisting after up to 3 months of treatment.75–77 However, as melatonin is usually not administered during the waking hours when food is consumed, the risk of clinically significant effects on glucose tolerance is likely to be minimal.
Furthermore, a 3-week double-blind placebo-controlled trial of 2mg of prolonged-release melatonin in patients with a mean age of 63 years with established type 2 diabetes and insomnia showed no effects on glucose markers, but sleep was improved. An uncontrolled, open-label follow-up period for 5 months was associated with a mild improvement in HbA1c of 0.66% ± 1.15%.78 There are few trials that had follow-up of sufficient duration to find an association between melatonin use and the development of type 2 diabetes mellitus in older adults.
Endogenous melatonin is thought to have a role in bone health, primarily by influencing the circadian rhythm of osteoblastic and osteoclastic hormones.79 There are mixed results of randomized controlled trials of melatonin in perimenopausal women, but a modest improvement in bone mineral density was seen in women with osteopenia after 12 months of 3mg of melatonin.80,81 Randomized controlled trials have reported infrequent fractures in those taking melatonin but were assessed as not associated with treatment.67 One 12-month trial of 2mg of prolonged-release melatonin reported three falls resulting in fracture. Musculoskeletal adverse events were not associated with older age.30
There are few and conflicting studies concerning the role of exogenous melatonin on body weight. Melatonin at a dose of 10mg in addition to caloric restriction has been shown to produce significant weight loss in young, obese adults (7% versus 4% of body weight in caloric restriction only).82 Whilst a recent meta-analysis and systematic review of trials including patients between the ages of 31 and 68 years found a mean reduction in weight of only 0.48kg.83 A study of melatonin supplementation in postmenopausal women with normal BMI and a mean age of 56 years demonstrated no significant weight loss.84 The effect of melatonin on weight loss in older age groups is unknown, but melatonin is unlikely to cause harmful weight loss in older adult patients.
The effects of endogenous melatonin on thermoregulation are well described. Studies of melatonin administration in older adult patients have demonstrated only modest falls in body temperature (0.05 degrees).85 There appears to be minimal risk of causing deleterious hypothermia with melatonin administration in older adults.
Conclusion
Overall, melatonin appears to be a safe medication in older adults relative to other commonly prescribed medications in this age group such as benzodiazepines, antidepressants, antiplatelets and antipsychotics.86 The vast majority of safety data is from younger populations, as is the case for most medications, and thus the risk in older adults therefore cannot be as precisely quantified. However, the small number of trials for dementia and insomnia in older adults are reassuring in their safety profile.
A general principle in the investigation of potential adverse effects in pharmaceutical development is the number of patients required to detect rare events.87 Small trials can detect frequent adverse effects associated with treatment, whilst large trials are required to detect infrequent effects. Infrequent adverse effects can have a significant impact in medications taken by tens of millions of people (as melatonin is in the US). A serious adverse effect from melatonin occurring at a rate of 0.1% would not be detected in trials involving less than 10,000 participants but would affect tens of thousands of patients in the US. Recent post-marketing surveillance data is reassuring in this regard, but the potential for serious adverse effects in older adults is significant given melatonin’s very widespread use.
There is still a risk of idiosyncratic adverse effects as detailed above, and these are likely to have a higher chance of adverse outcomes given the increased frailty and organ dysfunction in older adults. In countries where melatonin is available as a dietary supplement, there is robust evidence that melatonin content can vary wildly. Combined with the higher variation in absorption in older adults in addition to known and unknown drug interactions, there is considerable uncertainty in the plasma concentrations that will occur with administration. Appropriate timing of administration, 30–60 minutes before bedtime, is important to avoid sedation.
Furthermore, given the diverse systemic actions of melatonin, due diligence should be exercised during prescribing with regard to related comorbidities, such as in those with liver disease and at risk of labile blood pressure or falls. Clinicians are advised to monitor patients for potential adverse effects after commencing therapy.
In view of the above, melatonin should thus be considered a medication, albeit a relatively safe one, rather than a harmless dietary supplement. In relevant jurisdictions, clinicians should advise patients to consume melatonin in a form that is regulated as a medicine rather than a dietary supplement. The judicious use of melatonin is also advised, noting that the most recent guidelines from the American Academy of Sleep Medicine provide only a weak recommendation for its use in delayed sleep-wake phase disorder in adults, and recommend against the use of melatonin for sleep onset or sleep maintenance insomnia in adults.1,88 The lowest effective dose should be administered, with recommendations from the European Food Safety Authority and the American Academy of Sleep Medicine recommending maximum doses of 1mg and 2mg, respectively.1,89
Further research into the long-term safety of melatonin in older adults is warranted given its widespread use. The recent interest in its use in dementia and delirium will hopefully provide more evidence for its safe use in this population. Several trials in older adults have not reported safety data, and future trials should screen thoroughly for adverse events.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sateia MJ, Buysse DJ, Krystal AD, Neubauer DN, Heald JL. Clinical practice guideline for the pharmacologic treatment of chronic insomnia in adults: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2017;13(2):307–349. doi:10.5664/jcsm.6470
2. Li J, Somers VK, Xu H, Lopez-Jimenez F, Covassin N. Trends in use of melatonin supplements among US adults, 1999–2018. JAMA. 2022;327(5):483–485. doi:10.1001/jama.2021.23652
3. Zisapel N. New perspectives on the role of melatonin in human sleep, circadian rhythms and their regulation. Br J Pharmacol. 2018;175(16):3190–3199. doi:10.1111/bph.14116
4. Kvetnoy I, Ivanov D, Mironova E, et al. Melatonin as the cornerstone of neuroimmunoendocrinology. Int J Mol Sci. 2022;23(3):1835. doi:10.3390/ijms23031835
5. Peuhkuri K, Sihvola N, Korpela R. Dietary factors and fluctuating levels of melatonin. Food Nutr Res. 2012;56:17252. doi:10.3402/fnr.v56i0.17252
6. Gobbi G, Comai S. Differential function of melatonin MT(1) and MT(2) receptors in REM and NREM sleep. Front Endocrinol. 2019;10:87. doi:10.3389/fendo.2019.00087
7. Arangino S, Cagnacci A, Angiolucci M, et al. Effects of melatonin on vascular reactivity, catecholamine levels, and blood pressure in healthy men. Am J Cardiol. 1999;83(9):1417–1419. doi:10.1016/S0002-9149(99)00112-5
8. Koyama H, Nakade O, Takada Y, Kaku T, Lau KHW. Melatonin at pharmacologic doses increases bone mass by suppressing resorption through down‐regulation of the RANKL‐mediated osteoclast formation and activation. J Bone Mineral Res. 2002;17(7):1219–1229. doi:10.1359/jbmr.2002.17.7.1219
9. Tordjman S, Chokron S, Delorme R, et al. Melatonin: pharmacology, functions and therapeutic benefits. Curr Neuropharmacol. 2017;15(3):434–443. doi:10.2174/1570159X14666161228122115
10. Cooke JR, Ancoli-Israel S. Normal and abnormal sleep in the elderly. Handb Clin Neurol. 2011;98:653–665. doi:10.1016/b978-0-444-52006-7.00041-1
11. Gulia KK, Kumar VM. Sleep disorders in the elderly: a growing challenge. Psychogeriatrics. 2018;18(3):155–165. doi:10.1111/psyg.12319
12. Mahlberg R, Tilmann A, Salewski L, Kunz D. Normative data on the daily profile of urinary 6-sulfatoxymelatonin in healthy subjects between the ages of 20 and 84. Psychoneuroendocrinology. 2006;31(5):634–641. doi:10.1016/j.psyneuen.2006.01.009
13. Scholtens RM, van Munster BC, van Kempen MF, de Rooij SE. Physiological melatonin levels in healthy older people: a systematic review. J Psychosom Res. 2016;86:20–27. doi:10.1016/j.jpsychores.2016.05.005
14. Patel D, Steinberg J, Patel P. Insomnia in the elderly: a review. J Clin Sleep Med. 2018;14(6):1017–1024. doi:10.5664/jcsm.7172
15. Sack RL, Auckley D, Auger RR, et al. Circadian rhythm sleep disorders: part II, advanced sleep phase disorder, delayed sleep phase disorder, free-running disorder, and irregular sleep-wake rhythm. An American Academy of Sleep Medicine review. Sleep. 2007;30(11):1484–1501. doi:10.1093/sleep/30.11.1484
16. Rongve A, Boeve BF, Aarsland D. Frequency and correlates of caregiver‐reported sleep disturbances in a sample of persons with early dementia. J Am Geriatr Soc. 2010;58(3):480–486. doi:10.1111/j.1532-5415.2010.02733.x
17. Rodriguez‐Blazquez C, Schrag A, Rizos A, Chaudhuri KR, Martinez‐Martin P, Weintraub D. Prevalence of non‐motor symptoms and non‐motor fluctuations in Parkinson’s disease using the MDS‐NMS. Movement Disord Clin Pract. 2021;8(2):231–239. doi:10.1002/mdc3.13122
18. Brzezinski A, Vangel MG, Wurtman RJ, et al. Effects of exogenous melatonin on sleep: a meta-analysis. Sleep Med Rev. 2005;9(1):41–50. doi:10.1016/j.smrv.2004.06.004
19. Sletten TL, Magee M, Murray JM, et al. Efficacy of melatonin with behavioural sleep-wake scheduling for delayed sleep-wake phase disorder: a double-blind, randomised clinical trial. PLoS Med. 2018;15(6):e1002587. doi:10.1371/journal.pmed.1002587
20. Zhdanova IV, Wurtman RJ, Regan MM, Taylor JA, Shi JP, Leclair OU. Melatonin treatment for age-related insomnia. J Clin Endocrinol Metab. 2001;86(10):4727–4730. doi:10.1210/jcem.86.10.7901
21. Lemoine P, Nir T, Laudon M, Zisapel N. Prolonged-release melatonin improves sleep quality and morning alertness in insomnia patients aged 55 years and older and has no withdrawal effects. J Sleep Res. 2007;16(4):372–380. doi:10.1111/j.1365-2869.2007.00613.x
22. Luthringer R, Muzet M, Zisapel N, Staner L. The effect of prolonged-release melatonin on sleep measures and psychomotor performance in elderly patients with insomnia. Int Clin Psychopharmacol. 2009;24(5):239–249. doi:10.1097/YIC.0b013e32832e9b08
23. Garfinkel D, Laudon M, Nof D, Zisapel N. Improvement of sleep quality in elderly people by controlled-release melatonin. Lancet. 1995;346(8974):541–544. doi:10.1016/s0140-6736(95)91382-3
24. Wade AG, Ford I, Crawford G, et al. Efficacy of prolonged release melatonin in insomnia patients aged 55–80 years: quality of sleep and next-day alertness outcomes. Curr Med Res Opin. 2007;23(10):2597–2605. doi:10.1185/030079907x233098
25. Matar E, McCarter S, St Louis E, Lewis S. Current concepts and controversies in the management of REM sleep behavior disorder. Neurotherapeutics. 2021;18(1):107–123. doi:10.1007/s13311-020-00983-7
26. Zhang W, Chen XY, Su SW, et al. Exogenous melatonin for sleep disorders in neurodegenerative diseases: a meta-analysis of randomized clinical trials. Neurol Sci. 2016;37(1):57–65. doi:10.1007/s10072-015-2357-0
27. Wright A, Diebold J, Otal J, et al. The effect of melatonin on benzodiazepine discontinuation and sleep quality in adults attempting to discontinue benzodiazepines: a systematic review and meta-analysis. Drugs Aging. 2015;32(12):1009–1018. doi:10.1007/s40266-015-0322-5
28. Lin L, Huang Q-X, Yang -S-S, Chu J, Wang J-Z, Tian Q. Melatonin in Alzheimer’s disease. Int J Mol Sci. 2013;14(7):14575–14593. doi:10.3390/ijms140714575
29. Wan M, Begum R, Rashed AN. Trends, geographical variation and factors associated with melatonin prescribing in general practices in England: a practice-level analysis. Br J Clin Pharmacol. 2022;88(5):2430–2436. doi:10.1111/bcp.15136
30. Foley HM, Steel AE. Adverse events associated with oral administration of melatonin: a critical systematic review of clinical evidence. Complement Ther Med. 2019;42:65–81. doi:10.1016/j.ctim.2018.11.003
31. Besag FMC, Vasey MJ, Lao KSJ, Wong ICK. Adverse events associated with melatonin for the treatment of primary or secondary sleep disorders: a systematic review. CNS Drugs. 2019;33(12):1167–1186. doi:10.1007/s40263-019-00680-w
32. Hajak G, Lemme K, Zisapel N. Lasting treatment effects in a postmarketing surveillance study of prolonged-release melatonin. Int Clin Psychopharmacol. 2015;30(1):36–42. doi:10.1097/yic.0000000000000046
33. Brodner D, Corsino P. 0471 24-month post marketing safety surveillance data of a novel continuous release and absorption melatonin (CRA-melatonin) delivery system, confirms favorable safety profile. Sleep. 2020;43(Supplement_1):A180–A181. doi:10.1093/sleep/zsaa056.468
34. Giladi N, Shabtai H. Melatonin-induced withdrawal emergent dyskinesia and akathisia. Mov Disord. 1999;14(2):381–382. doi:10.1002/1531-8257(199903)14:2<381::aid-mds1036>3.0.co;2-k
35. van Geijlswijk IM, van der Heijden KB, Egberts AC, Korzilius HP, Smits MG. Dose finding of melatonin for chronic idiopathic childhood sleep onset insomnia: an RCT. Psychopharmacology. 2010;212(3):379–391. doi:10.1007/s00213-010-1962-0
36. Menczel Schrire Z, Phillips CL, Chapman JL, et al. Safety of higher doses of melatonin in adults: a systematic review and meta-analysis. J Pineal Res. 2022;72(2):e12782. doi:10.1111/jpi.12782
37. Cardinali DP. Melatonin: clinical perspectives in neurodegeneration. Front Endocrinol. 2019;10:480. doi:10.3389/fendo.2019.00480
38. McCleery J, Cohen DA, Sharpley AL. Pharmacotherapies for sleep disturbances in dementia. Cochrane Database Syst Rev. 2016;11(11):Cd009178. doi:10.1002/14651858.CD009178.pub3
39. Wade AG, Ford I, Crawford G, et al. Nightly treatment of primary insomnia with prolonged release melatonin for 6 months: a randomized placebo controlled trial on age and endogenous melatonin as predictors of efficacy and safety. BMC Med. 2010;8(1):51. doi:10.1186/1741-7015-8-51
40. Wade AG, Farmer M, Harari G, et al. Add-on prolonged-release melatonin for cognitive function and sleep in mild to moderate Alzheimer’s disease: a 6-month, randomized, placebo-controlled, multicenter trial. Clin Interv Aging. 2014;9:947–961. doi:10.2147/cia.S65625
41. Gilat M, Coeytaux jackson A, Marshall NS, et al. Melatonin for rapid eye movement sleep behavior disorder in Parkinson’s disease: a randomised controlled trial. Mov Disord. 2020;35(2):344–349. doi:10.1002/mds.27886
42. Vural EM, van Munster BC, de Rooij SE. Optimal dosages for melatonin supplementation therapy in older adults: a systematic review of current literature. Drugs Aging. 2014;31(6):441–451. doi:10.1007/s40266-014-0178-0
43. de Jonghe A, Korevaar JC, van Munster BC, de Rooij SE. Effectiveness of melatonin treatment on circadian rhythm disturbances in dementia. Are there implications for delirium? A systematic review. Int J Geriatr Psychiatry. 2010;25(12):1201–1208. doi:10.1002/gps.2454
44. Almond SM, Warren MJ, Shealy KM, Threatt TB, Ward ED. A systematic review of the efficacy and safety of over-the-counter medications used in older people for the treatment of primary insomnia. Sr Care Pharm. 2021;36(2):83–92. doi:10.4140/TCP.n.2021.83
45. Erland LA, Saxena PK. Melatonin natural health products and supplements: presence of serotonin and significant variability of melatonin content. J Clin Sleep Med. 2017;13(2):275–281. doi:10.5664/jcsm.6462
46. DeMuro RL, Nafziger AN, Blask DE, Menhinick AM, Bertino JS. The absolute bioavailability of oral melatonin. J Clin Pharmacol. 2000;40(7):781–784. doi:10.1177/00912700022009422
47. Fourtillan JB, Brisson AM, Gobin P, Ingrand I, Decourt JP, Girault J. Bioavailability of melatonin in humans after day-time administration of D(7) melatonin. Biopharm Drug Dispos. 2000;21(1):15–22. doi:10.1002/1099-081x(200001)21:1<15::aid-bdd215>3.0.co;2-h
48. Andersen LP, Werner MU, Rosenkilde MM, et al Pharmacokinetics of oral and intravenous melatonin in healthy volunteers. BMC Pharmacol Toxicol. 2016;17:8. doi:10.1186/s40360-016-0052-2
49. Aspen Pharmacare, Circadin (melatonin prolonged release) [Consumer Medicine Information]. 2020. Available from: https://www.ebs.tga.gov.au/ebs/picmi/picmirepository.nsf/PICMI?OpenForm&t=pi&q=Circadin.
50. Zhdanova IV, Wurtman RJ, Balcioglu A, Kartashov AI, Lynch HJ. Endogenous melatonin levels and the fate of exogenous melatonin: age effects. J Gerontol a Biol Sci Med Sci. 1998;53(4):B293–8. doi:10.1093/gerona/53a.4.b293
51. Chojnacki C, Wachowska-Kelly P, Błasiak J, Reiter RJ, Chojnacki J. Melatonin secretion and metabolism in patients with hepatic encephalopathy. J Gastroenterol Hepatol. 2013;28(2):342–347. doi:10.1111/jgh.12055
52. Iguchi H, Kato KI, Ibayashi H. Melatonin serum levels and metabolic clearance rate in patients with liver cirrhosis. J Clin Endocrinol Metab. 1982;54(5):1025–1027. doi:10.1210/jcem-54-5-1025
53. Giovannini S, Onder G, van der Roest HG, et al. Use of antidepressant medications among older adults in European long-term care facilities: a cross-sectional analysis from the SHELTER study. BMC Geriatr. 2020;20(1):310. doi:10.1186/s12877-020-01730-5
54. von Bahr C, Ursing C, Yasui N, Tybring G, Bertilsson L, Röjdmark S. Fluvoxamine but not citalopram increases serum melatonin in healthy subjects-- an indication that cytochrome P450 CYP1A2 and CYP2C19 hydroxylate melatonin. Eur J Clin Pharmacol. 2000;56(2):123–127. doi:10.1007/s002280050729
55. Härtter S, Grözinger M, Weigmann H, Röschke J, Hiemke C. Increased bioavailability of oral melatonin after fluvoxamine coadministration. Clin Pharmacol Ther. 2000;67(1):1–6. doi:10.1067/mcp.2000.104071
56. Huuhka K, Riutta A, Haataja R, Ylitalo P, Leinonen E. The effect of CYP2C19 substrate on the metabolism of melatonin in the elderly: a randomized, double-blind, placebo-controlled study. Methods Find Exp Clin Pharmacol. 2006;28(7):447–450. doi:10.1358/mf.2006.28.7.1003545
57. Foster BC, Cvijovic K, Boon HS, et al. Melatonin interaction resulting in severe sedation. J Pharm Pharm Sci. 2015;18(2):124–131. doi:10.18433/j3ss35
58. Lusardi P, Piazza E, Fogari R. Cardiovascular effects of melatonin in hypertensive patients well controlled by nifedipine: a 24-hour study. Br J Clin Pharmacol. 2000;49(5):423–427. doi:10.1046/j.1365-2125.2000.00195.x
59. Ashy N, Shroff K, Ashy N. Evaluation of the potential drug interaction of melatonin and warfarin: a case series. Life Sci J. 2016;13(6):124.
60. Otmani S, Demazières A, Staner C, et al. Effects of prolonged-release melatonin, zolpidem, and their combination on psychomotor functions, memory recall, and driving skills in healthy middle aged and elderly volunteers. Hum Psychopharmacol. 2008;23(8):693–705. doi:10.1002/hup.980
61. Härtter S, Nordmark A, Rose DM, Bertilsson L, Tybring G, Laine K. Effects of caffeine intake on the pharmacokinetics of melatonin, a probe drug for CYP1A2 activity. Br J Clin Pharmacol. 2003;56(6):679–682. doi:10.1046/j.1365-2125.2003.01933.x
62. Dolberg OT, Hirschmann S, Grunhaus L. Melatonin for the treatment of sleep disturbances in major depressive disorder. Am J Psychiatry. 1998;155(8):1119–1121. doi:10.1176/ajp.155.8.1119
63. Andersen LP, Gögenur I, Rosenberg J, Reiter RJ. The safety of melatonin in humans. Clin Drug Investig. 2016;36(3):169–175. doi:10.1007/s40261-015-0368-5
64. Wade AG, Crawford G, Ford I, et al. Prolonged release melatonin in the treatment of primary insomnia: evaluation of the age cut-off for short- and long-term response. Curr Med Res Opin. 2011;27(1):87–98. doi:10.1185/03007995.2010.537317
65. Chakraborti D, Tampi DJ, Tampi RR. Melatonin and melatonin agonist for delirium in the elderly patients. Am J Alzheimers Dis Other Demen. 2015;30(2):119–129. doi:10.1177/1533317514539379
66. Shi Y. Effects of melatonin on postoperative delirium after PCI in elderly patients: a randomized, single-center, double-blind, placebo-controlled trial. Heart Surg Forum. 2021;24(5):E893–e897. doi:10.1532/hsf.4049
67. Lemoine P, Garfinkel D, Laudon M, Nir T, Zisapel N. Prolonged-release melatonin for insomnia - an open-label long-term study of efficacy, safety, and withdrawal. Ther Clin Risk Manag. 2011;7:301–311. doi:10.2147/tcrm.S23036
68. Soldatos CR, Dikeos DG, Whitehead A. Tolerance and rebound insomnia with rapidly eliminated hypnotics: a meta-analysis of sleep laboratory studies. Int Clin Psychopharmacol. 1999;14(5):287–303. doi:10.1097/00004850-199909000-00004
69. Hansen MV, Danielsen AK, Hageman I, Rosenberg J, Gögenur I. The therapeutic or prophylactic effect of exogenous melatonin against depression and depressive symptoms: a systematic review and meta-analysis. Eur Neuropsychopharmacol. 2014;24(11):1719–1728. doi:10.1016/j.euroneuro.2014.08.008
70. Grossman E, Laudon M, Zisapel N. Effect of melatonin on nocturnal blood pressure: meta-analysis of randomized controlled trials. Vasc Health Risk Manag. 2011;7:577–584. doi:10.2147/vhrm.S24603
71. Rechciński T, Trzos E, Wierzbowska-Drabik K, Krzemińska-Pakuła M, Kurpesa M. Melatonin for nondippers with coronary artery disease: assessment of blood pressure profile and heart rate variability. Hypertens Res. 2010;33(1):56–61. doi:10.1038/hr.2009.174
72. Kostoglou-Athanassiou I, Treacher DF, Wheeler MJ, Forsling ML. Melatonin administration and pituitary hormone secretion. Clin Endocrinol. 1998;48(1):31–37. doi:10.1046/j.1365-2265.1998.00341.x
73. Webley GE, Böhle A, Leidenberger FA. Positive relationship between the nocturnal concentrations of melatonin and prolactin, and a stimulation of prolactin after melatonin administration in young men. J Pineal Res. 1988;5(1):19–33. doi:10.1111/j.1600-079x.1988.tb00765.x
74. Forsling ML, Wheeler MJ, Williams AJ. The effect of melatonin administration on pituitary hormone secretion in man. Clin Endocrinol. 1999;51(5):637–642. doi:10.1046/j.1365-2265.1999.00820.x
75. Lauritzen ES, Kampmann U, Pedersen MGB, et al. Three months of melatonin treatment reduces insulin sensitivity in patients with type 2 diabetes—A randomized placebo-controlled crossover trial. J Pineal Res. 2022;73:e12809. doi:10.1111/jpi.12809
76. Cagnacci A, Arangino S, Renzi A, et al. Influence of melatonin administration on glucose tolerance and insulin sensitivity of postmenopausal women. Clin Endocrinol. 2001;54(3):339–346. doi:10.1046/j.1365-2265.2001.01232.x
77. Rubio-Sastre P, Scheer FA, Gómez-Abellán P, Madrid JA, Garaulet M. Acute melatonin administration in humans impairs glucose tolerance in both the morning and evening. Sleep. 2014;37(10):1715–1719. doi:10.5665/sleep.4088
78. Garfinkel D, Zorin M, Wainstein J, Matas Z, Laudon M, Zisapel N. Efficacy and safety of prolonged-release melatonin in insomnia patients with diabetes: a randomized, double-blind, crossover study. Diabetes Metab Syndr Obes. 2011;4:307–313. doi:10.2147/dmso.S23904
79. Munmun F, Witt-Enderby PA. Melatonin effects on bone: implications for use as a therapy for managing bone loss. J Pineal Res. 2021;71(1):e12749. doi:10.1111/jpi.12749
80. Amstrup AK, Sikjaer T, Heickendorff L, Mosekilde L, Rejnmark L. Melatonin improves bone mineral density at the femoral neck in postmenopausal women with osteopenia: a randomized controlled trial. J Pineal Res. 2015;59(2):221–229. doi:10.1111/jpi.12252
81. Kotlarczyk MP, Lassila HC, O’Neil CK, et al. Melatonin osteoporosis prevention study (MOPS): a randomized, double-blind, placebo-controlled study examining the effects of melatonin on bone health and quality of life in perimenopausal women. J Pineal Res. 2012;52(4):414–426. doi:10.1111/j.1600-079X.2011.00956.x
82. Szewczyk-Golec K, Rajewski P, Gackowski M, et al. Melatonin supplementation lowers oxidative stress and regulates adipokines in obese patients on a calorie-restricted diet. Oxid Med Cell Longev. 2017;2017:8494107. doi:10.1155/2017/8494107
83. Delpino FM, Figueiredo LM. Melatonin supplementation and anthropometric indicators of obesity: a systematic review and meta-analysis. Nutrition. 2021;91–92:111399. doi:10.1016/j.nut.2021.111399
84. Walecka-Kapica E, Klupińska G, Chojnacki J, Tomaszewska-Warda K, Błońska A, Chojnacki C. The effect of melatonin supplementation on the quality of sleep and weight status in postmenopausal women. Prz Menopauzalny. 2014;13(6):334–338. doi:10.5114/pm.2014.47986
85. Lushington K, Pollard K, Lack L, Kennaway DJ, Dawson D. Daytime melatonin administration in elderly good and poor sleepers: effects on core body temperature and sleep latency. Sleep. 1997;20(12):1135–1144. doi:10.1093/sleep/20.12.1135
86. American Geriatrics Society. 2019 updated AGS beers criteria® for potentially inappropriate medication use in older adults. J Am Geriatr Soc. 2019;67(4):674–694. doi:10.1111/jgs.15767
87. Berlin JA, Glasser SC, Ellenberg SS. Adverse event detection in drug development: recommendations and obligations beyond Phase 3. Am J Public Health. 2008;98(8):1366–1371. doi:10.2105/ajph.2007.124537
88. Auger RR, Burgess HJ, Emens JS, Deriy LV, Thomas SM, Sharkey KM. Clinical practice guideline for the treatment of intrinsic circadian rhythm sleep-wake disorders: Advanced Sleep-Wake Phase Disorder (ASWPD), Delayed Sleep-Wake Phase Disorder (DSWPD), Non-24-Hour Sleep-Wake Rhythm Disorder (N24SWD), and Irregular Sleep-Wake Rhythm Disorder (ISWRD). An update for 2015: an American Academy of Sleep Medicine clinical practice guideline. J Clin Sleep Med. 2015;11(10):1199–1236. doi:10.5664/jcsm.5100
89. EFSA Panel on Dietetic Products, Nutrition and Allergies (NDA). Scientific opinion on the substantiation of a health claim related to melatonin and reduction of sleep onset latency (ID 1698, 1780, 4080) pursuant to Article 13 (1)of Regulation (EC) No 1924/2006. EFSA J. 2011;9(6):2241. doi:10.2903/j.efsa.2011.2241
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Safety of TKI Plus PD-1 Inhibitors in Elderly uHCC Patients: A Retrospective Study
Chen B, Lei J, Zhao H, Dong J, Zeng Z, Li Y, Yu L, Zhou L, Jia A, Lu Y, Cheng J
Journal of Hepatocellular Carcinoma 2022, 9:1171-1185
Published Date: 8 November 2022
Benzodiazepine Usage, Healthcare Resource Utilization, and Costs Among Older Adults Treated with Common Insomnia Medications: A Retrospective Cohort Study
Wickwire EM, Juday TR, Gor D, Amari DT, Frech FH
ClinicoEconomics and Outcomes Research 2023, 15:413-424
Published Date: 2 June 2023
Idiopathic Epiretinal Membrane Surgery in Patients Aged Over 80 Years: Efficacy and Safety
Li Q, Yang K, Ji Q, Jiang J, Zong R, Zhang Y, Qian Y, Che X, Suo J, Wang Z
Clinical Ophthalmology 2023, 17:3365-3372
Published Date: 3 November 2023
Safety and Performance of OptiVantage, a CT Contrast Media Injector, in Multi-Patient Mode
Tirri A, Iannelli FN, Sequeira A, Hebert F
Medical Devices: Evidence and Research 2025, 18:233-240
Published Date: 12 April 2025
Real-World Experience of Guselkumab in the Elderly Population
Fratton Z, Bighetti S, Bettolini L, Maione V, Rossi M, Venturini M, Mazzoletti V, Zelin E, Stinco G, Errichetti E
Psoriasis: Targets and Therapy 2025, 15:581-601
Published Date: 26 December 2025