Back to Journals » Journal of Pain Research » Volume 19
Proteomics and Metabolomics-Based Investigation of Local Microenvironmental Changes in Sensitized Acupoint Compared to Non-Sensitized Point Among Patients with Chronic Atrophic Gastritis: A Cross-Sectional Study Protocol
Authors Yang G ![]() , Liu CZ
, Liu CZ ![]() , Ren CH, Shi GX, Yang JW
, Ren CH, Shi GX, Yang JW ![]() , Wang YG
, Wang YG ![]() , Yang NN
, Yang NN
Received 10 November 2025
Accepted for publication 27 February 2026
Published 10 March 2026 Volume 2026:19 580054
DOI https://doi.org/10.2147/JPR.S580054
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Houman Danesh
Guang Yang,1,2 Cun-Zhi Liu,1,2 Chang-Hang Ren,1,2 Guang-Xia Shi,1,2 Jing-Wen Yang,1,2 Yan-Gang Wang,3 Na-Na Yang1,2
1International Acupuncture and Moxibustion Innovation Institute, Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 2School of Acupuncture-Moxibustion and Tuina, Beijing University of Chinese Medicine, Beijing, People’s Republic of China; 3Department of Gastroenterology, Beijing University of Chinese Medicine Third Affiliated Hospital, Beijing, People’s Republic of China
Correspondence: Na-Na Yang, International Acupuncture and Moxibustion Innovation Institute, Beijing University of Chinese Medicine, No. 11, Bei San Huan Dong Lu, Chaoyang District, Beijing, 100029, People’s Republic of China, Email [email protected] Yan-Gang Wang, Department of Gastroenterology, Beijing University of Chinese Medicine Third Affiliated Hospital, No. 51, An Wai Xiao Guan Street, Chaoyang District, Beijing, 100029, People’s Republic of China, Email [email protected]
Abstract: Acupoint sensitization is a key manifestation of disease response and plays a critical role in determining the effectiveness of acupuncture treatment. Chronic atrophic gastritis, characterized by persistent and pronounced acupoint sensitization, serves as an ideal model for studying this phenomenon. We aim to link local molecular alterations at sensitized acupoints with the pain-sensitization phenotype, thereby elucidating the comprehensive molecular mechanisms underlying acupoint sensitization and ultimately providing mechanistic guidance for how acupuncture exerts therapeutic effects in the clinical treatment of CAG. This study will recruit and sampling 30 patients with chronic atrophic gastritis who are aged between 40 and 65 years and whose CV12 and non-acupoint pain threshold are greater than 10N, aiming to explore the local metabolomics and proteomics changes in the acupoint in these patients. The non-acupoint located in the lateral abdomen, corresponding to the same spinal segment as the CV12 acupoint, will serve as the control group. We expect to find that, compared with the non-acupoint group, the content of pain-related metabolites and proteins in the tissue fluid of the CV12 acupoint will increase. These changes are anticipated to be correlated with the pain sensitization phenotype. The study will comply with the Declaration of Helsinki and has been approved by the Ethics Committee of Beijing University of Chinese Medicine (No. 2024BZYLL1006). All participants will undergo standardized training on the study protocol, and informed consent will be obtained from all patients.Trial registration: ITMCTR2025000156; International Traditional Medicine Clinical Trial Registry (https://itmctr.ccebtcm.org.cn/mgt/project/user/user-project-view/C96AC314-9A6A-44A4-ABD1-B602A84F5792).
Keywords: acupoint sensitization, chronic atrophic gastritis, protocol, pain, proteomics, metabolomics
Introduction
Acupoint sensitization refers to the changes in sensation in the acupoint, including the feelings of heat, itching, numbness, swelling, especially pain.1 It regularly observes in various chronic inflammatory diseases or disorders associated with dysfunction of internal organs, thereby facilitating the diagnosis of such diseases.2–4 Among these manifestations, pain sensitization, defined as a reduced pressure pain threshold (PPT), is the most widely studied and reproducible phenotype.5 Several clinical studies have consistently demonstrated decreased PPT values at specific acupoints in patients with chronic gastritis, knee osteoarthritis, and angina pectoris, supporting its validity as an operational definition of sensitization.4,6,7 In clinical acupuncture practice, selecting “Ah Shi” points, characterized by “Acupuncture at Pain Point” often yields significant therapeutic effects.8 Previous studies have showed that acupuncture stimulation targeting pain-sensitive acupoints achieves greater therapeutic efficacy compared to stimulation of conventional acupoints, particularly in alleviating pain.9 Therefore, it is essential to elucidate the changes in the local microenvironment of acupoint pain sensitization.
These pain-sensitive acupoints share similar characteristics with referred pain and trigger points, both of which are closely linked to the neural system and the pathological responses of local tissues.10,11 The mechanism of the phenomenon involves visceral nociceptive information that activates spinal dorsal horn cells via dorsal root ganglion neurons, transmitting retrogradely to the periphery through a dorsal root reflex, while visceral afferent impulses also retrogradely transmit via axonal reflexes at the dorsal root ganglion branches.12 These two types of transmission trigger the release of inflammatory mediators from peripheral terminals, which stimulate mast cell aggregation and degranulation. This process leads to the release of pain-inducing substances like histamine (HA) and serotonin (5-hydroxytryptamine, 5-HT), resulting in local skin hyperalgesia.13 A study using a gastric mucosal injury rat model found that mast cell aggregation occurred at the sensitized acupoint on the back, with SP (Substance P) levels significantly higher than those in the control group.14 Combined with metabolite analysis, the precursor of histamine, histidine, was found to be increased at the sensitized acupoint,15 accompanied by changes in the expression of related proteins5. This suggests that the phenomenon of acupoint sensitization is not caused by a single substance, but rather by the combined effects of multiple substances leading to local changes. However, Nociceptive alterations in acupoint is a complex phenomenon caused by subcutaneous changes in various substances and interactions, the substances that have been explored so far are insufficient to fully explain the occurrence of the phenomenon, and there is a lack of research on the local mechanism of human acupoints.
CAG is a chronic disease characterized by chronic inflammation of the gastric mucosa and glandular atrophy. Persistent inflammatory stimulation and immune imbalance can cause the visceral sensory input to remain in a state of high reactivity for a long time, and trigger peripheral and central sensitization.16 The segmental convergence of visceral and somatic sensory information in the dorsal horn of the spinal cord can translate visceral inflammation into body surface referred pain and local mechanical pain sensitivity.17 The rat experiments using acute gastritis as a model further proved that the axonal bifurcation of the same primary afferent neuron can convert the inflammatory input from the stomach into a neurogenic inflammatory response and pain sensitization on the body surface.18 As a chronic organic disease, the characteristics of CAG allow for the observation of significant and sustained acupoint pain sensitization in affected patients.19 The aim of this study was to analyze the proteomics and metabolomics of tissue fluids localized at sensitized acupoints and non-acupoints using High-Performance Liquid Chromatography-Mass Spectrometry (HPLC-MS/MS) in patients with CAG. We will analyze the material basis for the development of acupoint sensitization from the molecular material level, providing quantitative evidence for the material changes associated with sensitization and discussing the characteristics and molecular alterations of acupoint sensitization. By linking the acupoint sensitization phenotype to the local molecular profile, we aim to delineate key pathways and prioritize candidate mediators within the microenvironment of sensitized acupoints in CAG patients. This will generate testable molecular evidence for the mechanisms underlying acupuncture’s clinical effects and support response prediction, individualized acupoint selection, and biomarker development. Specifically, we will identify previously unrecognized molecular features at sensitized acupoints and quantify the contribution of putative algogenic mediators to sensitization, thereby nominating the most informative biomarker candidates.
Methods
Study Design
This single-center, cross-sectional study will recruit 30 CAG patients to assess PPT and microenvironmental variations between acupoints and non-acupoints. Participants will complete a one-week washout period at home to standardize lifestyle factors (diet, medication, smoking, alcohol consumption and physical activity20–23), with submitting daily reports to evaluate the quality of the washout period. Subsequent assessments will be conducted in the hospital using a Wagner FPX50 digital force gauge for PPT measurements and negative pressure suction for acupoints tissue fluid collection. All procedures were performed after a standardized 10-hour fasting period (08:30–09:00) to control for dietary confounders,24 with premenopausal women assessed during the luteal phase to mitigate hormonal variability.25 Metabolomics and proteomics differences between the two groups are analyzed to reveal the potential molecular mechanisms underlying acupoint sensitization. The study protocol follows the STROBE26 guidelines for reporting, and we have provided the STROBE checklist in the Supplementary 1. This single-center, cross-sectional study is conducted at Beijing University of Chinese Medicine Dongzhimen Hospital, China, from January 2025 to December 2025. All participants will undergo standardized training on the study protocol, and informed consent will be obtained from all patients. The SPIRIT schedule and technical roadmap of this study are respectively illustrated in Figures 1 and 2. We have also included the complete SPIRIT checklist, as well as the approved and complete original research protocol and informed consent form in the Supplementary 2–4.
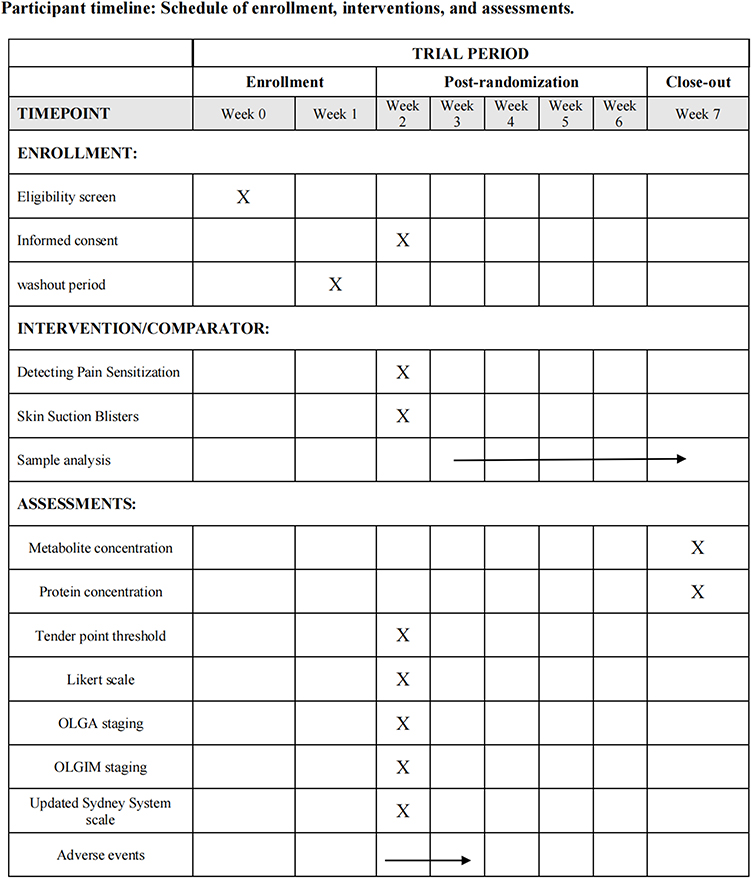 |
Figure 1 Shows the schedule for subject enrollment, intervention and assessment. The “X” and arrows in the figure respectively indicate the screening, intervention and assessment projects carried out during the corresponding time periods and their ongoing processes. |
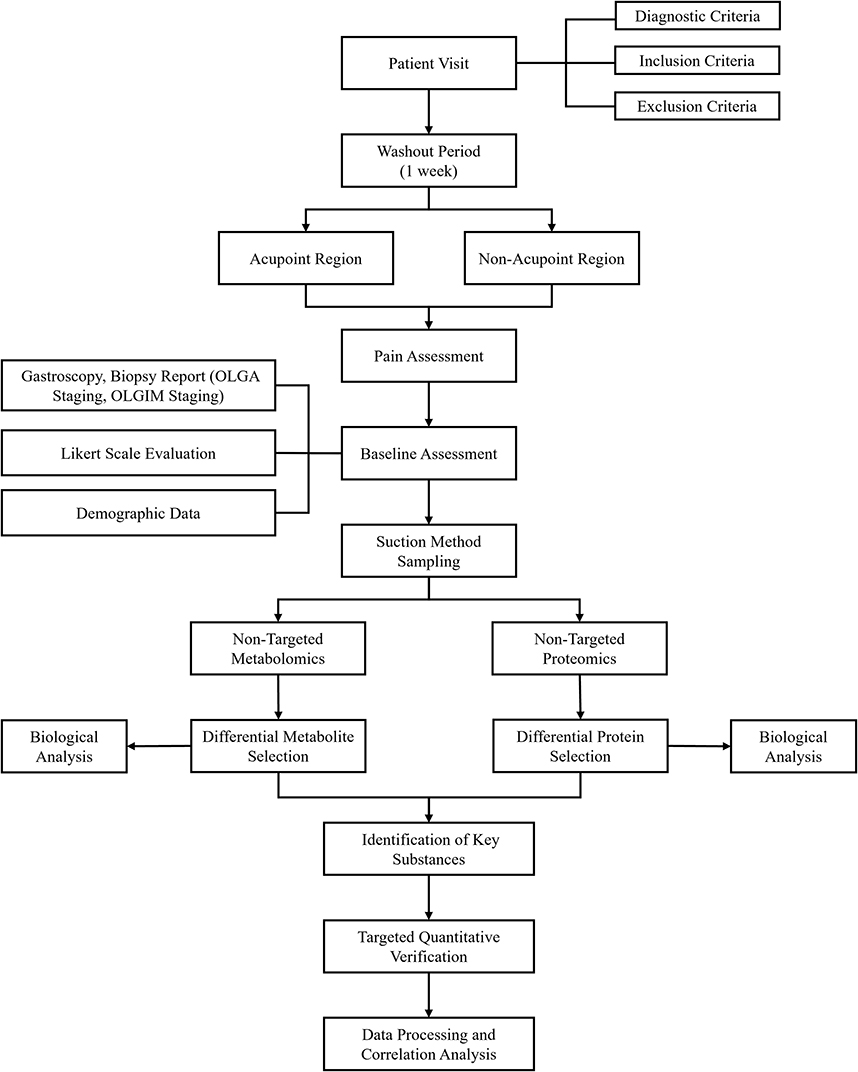 |
Figure 2 Illustrates the overall technical workflow of the study, encompassing participant screening and enrollment, cross-sectional intervention, baseline data collection, tissue fluid sample collection and processing, and subsequent metabolomic and proteomic analyses. |
Participants
This study will recruit 30 CAG patients aged 40–65 years with acupoint pain sensitization at the designated hospital. Recruitment procedures include poster campaigns, distribution of promotional materials, and referrals through specialized physicians.
Diagnostic Criteria
The diagnostic criteria will be established based on the 2021 Expert Consensus on Atrophic Gastritis by the American Gastroenterological Association27 and the “Chinese Guidelines for the Diagnosis and Treatment of Chronic Gastritis (2022, Shanghai)”.28
The endoscopic findings of CAG include mucosa displaying characteristic red and white coloration with white areas predominating, accompanied by flattened or absent folds, visible mucosal blood vessels, and mucosal granularity or nodular changes. The pathological diagnosis of CAG includes gastric mucosal atrophy or atrophy of the intrinsic glands, intestinal metaplasia of the gastric mucosa, and gastric mucosal dysplasia. The diagnosis of chronic atrophic gastritis involves both endoscopic diagnosis and pathological diagnosis. The severity of the condition is determined by the pathological diagnosis.
Inclusion Criteria
- Patients must have an endoscopic and pathological diagnosis report within the last six months meeting the diagnostic criteria for chronic atrophic gastritis, with OLGA staging of III–IV and OLGIM staging of 0-V.
- Age between 40–65 years, with no gender restriction.
- Difference in pressure pain threshold between the CV12 acupoint and a non-acupoint area greater than 10 N.
- Patients must demonstrate good compliance, voluntarily participate in the study, and sign an informed consent form.
Note: Only participants meeting all four criteria are eligible for inclusion in this study.
Exclusion Criteria
- Patients with coexisting autoimmune gastritis (Type A chronic atrophic gastritis), peptic ulcer, gastric ulcer, duodenal ulcer, special types of gastritis, or gastrointestinal bleeding.
- Patients with endoscopic or pathological biopsy results indicating cancer, or imaging findings suggesting cancer metastasis.
- Patients currently taking analgesics or hormone medications.
- Patients with impaired consciousness, inability to express subjective discomfort, or psychiatric disorders.
- Patients with severe life-threatening diseases, including serious cardiovascular, cerebrovascular, liver, kidney, hematopoietic disorders, or malignant tumors.
- Patients with a propensity for scarring or with scars, injuries, skin diseases, or peripheral nerve disorders at the acupoint sites.
- Patients with diseases causing abnormal basal body temperature, such as thyroid dysfunction or other metabolic disorders.
- Patients who have undergone gastric surgery or major surgeries resulting in significant organ damage or alteration.
- Pregnant or breastfeeding women.
- Patients who have received acupuncture or participated in other clinical trials within the past six months.
Note: Participants meeting any of the above criteria will be excluded from this study.
Sample Size
This study is exploratory research aimed at detecting differences in pain sensitizing substances in the local tissue fluid between the acupoint sensitization area and the control area. As this is an exploratory study, a formal sample size calculation was not required. A target of 30 pairs of valid samples was determined based on prior experience with similar biomarker studies. As this study does not involve follow-up, there is no dropout rate. Therefore, A total of 30 CAG patients will be recruited, with 60 tissue fluid samples collected in total.
Procedure
Acupoints and Position
Acupoints refer to the 2021 National Standard of the People’s Republic of China (GB/T 12346–2021)29 nomenclature and location of acupoints. (Table 1 and Figure 3).
 |
Table 1 Acupoint Position |
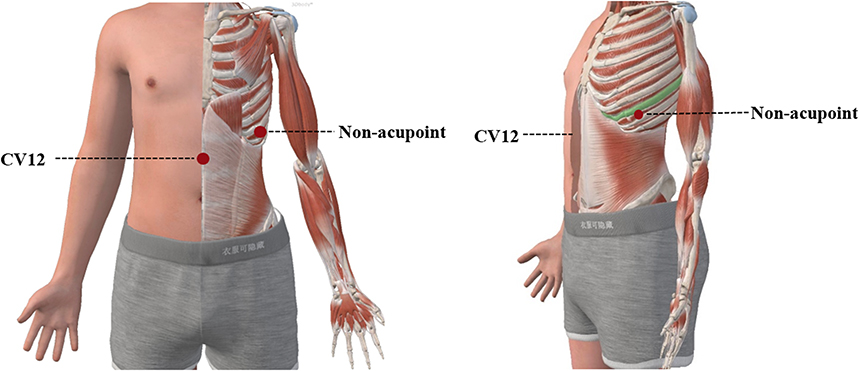 |
Figure 3 Shows anterior and lateral anatomical views of the upper human body, illustrating the specific locations of Zhongwan (CV12) and the non-acupoint. Red dots indicate the acupuncture/landmark points, and dashed lines are used for corresponding labels. |
Detecting Pain Sensitization
Participants will lie supine, and trained researchers will use a Wagner FPX50 digital force gauge to detect PPTs on the hand, ensuring they understand the sensation. Measurements will begin with the CV12 acupoint, followed by a non-acupoint area, with two readings taken at each site. If the difference between measurements exceeds 5 N, a third measurement will be performed. The average threshold will be calculated, and acupoint sensitization will be confirmed if the threshold difference exceeds 10 N. Participants meeting this criterion will proceed to blister suction sampling.
Skin Suction Blisters
After pain sensitization detection, the sampling area will be disinfected with 2.5% povidone-iodine, followed by de-iodination with 75% alcohol. A sterile three-hole skin suction plate will be applied to the CV12 acupoint or non-acupoint area to create a blister-prone skin area. Negative pressure (40–70 KPa) will be applied for 1–2 hours at 40–50°C using a BFY-IVC epidermal separator. Once blisters form, the negative pressure will be stopped, and fluid will be collected with a sterile syringe into a labeled centrifuge tube.30 The sampling site will be bandaged afterward. The samples will be collected into four 0.5 mL conical bottom centrifuge tubes, with each sample appropriately labeled and they will be stored at −80°C until further analysis. This storage method allows for direct metabolite extraction and other processing upon thawing, while avoiding repeated freeze-thaw cycles that could potentially affect the analysis results.31
Note: Throughout the entire procedure, closely monitor the participant’s mental state. If any adverse reactions occur, manage them according to the adverse event handling protocol outlined in the study plan.
Non-Targeted Metabolomics Analysis
Local tissue fluid samples from the CV12 acupoint and a non-acupoint area in CAG patients were collected using blister suction. A non-targeted metabolomics approach based on HPLC-MS/MS was employed to detect differential metabolites. After sample preparation and metabolite extraction, chromatography was performed using a reverse-phase column coupled to a high-resolution mass spectrometer. QC samples were injected at regular intervals throughout the run. Raw data were processed using metabolomics data analysis software and metabolite identification was conducted by matching spectra against publicly available databases.31
Non-Targeted Proteomics Analysis
Local tissue fluid samples were subjected to protein extraction, enzymatic digestion, and desalting. Peptide concentrations were quantified, and equal amounts were loaded for chromatographic separation using a C18 reverse-phase column coupled to a high-resolution mass spectrometer.32 MS/MS spectra were analyzed using proteomics data analysis software against the human-reviewed protein database.
Targeted Quantitative Validation of Key Substances
Tissue fluid collected from the CV12 acupoint and a non-acupoint area in CAG patients was analyzed for key metabolites such as 5-HT and Substance P (SP). Following sample preparation and derivatization, chromatography was conducted with a reverse-phase column, and quantification was performed based on a standard curve. Data processing was carried out using corresponding software.
Simple Western-Jess
Protein expression levels of pain-related markers such as SP and Calcitonin Gene-Related Peptide (CGRP) were analyzed using the automated Simple Western Jess system (Protein Simple, Bio-Techne). Protein concentrations were determined by BCA assay, and sample preparation and detection were performed according to the manufacturer’s instructions. Signals were acquired and quantified using Compass software, with the signal-to-noise ratio (N/S) set above 20 to ensure data quality. The system operated within its recommended linear detection range, and all samples were measured in technical duplicates to ensure reproducibility. Data were exported for further quantitative analysis.
Observation Indicators
Primary Indicators
This cross-sectional study primarily focuses on the differential metabolites and protein concentrations in acupoint interstitial fluid as the primary observation indicators. Non-targeted metabolomics and proteomics analysis of acupoint and non-acupoint local interstitial fluids from the subjects will be conducted using HPLC-MS/MS to compare the differences in the local microenvironment between the two groups. Furthermore, targeted analysis of key substances will be performed to identify the key metabolites and protein concentrations at the acupoints.
Secondary Indicators
Secondary indicators include the pain threshold values at acupoints measured after the washout period, as well as the proteomics and metabolomics of local tissue fluid samples. PPTs are measured using the Wagner FPX50 handheld pressure algometer, and the tissue fluid samples are analyzed using HPLC-MS/MS for non-targeted metabolomics and proteomics.
This study will use the CAG symptom assessment scale (Likert scale) to evaluate CAG symptoms. Pathological indicators include endoscopic reports, pathology reports, OLGA staging, OLGIM staging, and the Updated Sydney System scale. These data will serve as the baseline data for the patients.
Adverse Events
Any occurrences of infection or other adverse reactions during blister suction sampling should be documented. If an infection occurs after sampling, gently clean the wound with saline or a specialized wound-cleaning solution, monitor the wound regularly, and, in cases of severe infection, follow medical advice regarding the use of antibiotics and other relevant treatments. If bleeding occurs during or after sampling, stop the vacuum system and apply pressure with a cotton ball to control bleeding. Should localized skin pigmentation or scar hypertrophy develop post-sampling, follow medical recommendations for care. If the patient experiences electrolyte or acid-base imbalances during sampling, regularly monitor their electrolyte and acid-base levels and administer appropriate electrolyte supplementation or medication to correct any imbalances. One week after tissue fluid sampling, all patients will be contacted by phone to check on their condition and ensure their safety.
Statistical Analysis
Statistical analysis will be performed using SPSS 20.0 software. The data will first undergo tests for normality and homogeneity of variance. Normally distributed continuous variables will be described as mean ± standard deviations (M ± SD) and analyzed using independent t-test. Non-normally continuous variables will be represented as medians combined with interquartile ranges (IQR) and analyzed using the Wilcoxon rank-sum test. Categorical data will be analyzed using the chi-squared test and presented as frequencies, percentages, or constituent ratios. For the metabolomics and proteomics data, principal component analysis (PCA) and partial least squares discriminant analysis (PLS-DA) will be employed for pattern recognition and intergroup comparison. Differential metabolites will be identified based on the variable importance in projection (VIP) value, with VIP > 1.0. Additionally, bioinformatics analyses will be conducted, including clustering of differential metabolites and Kyoto Encyclopedia of Genes and Genomes (KEGG) pathway analysis. Correlation analysis will be conducted on the pain thresholds of key substances and the acupoint areas or non-acupoint areas. The specific method will be Pearson correlation or Spearman correlation depending on the situation, and the operation will be carried out using SPSS. A p-value of less than 0.05 will be considered statistically significant. The data analyst was blinded.
Data Availability and Management Statement
All personnel responsible for data entry and statistical analysis will undergo standardized training in data management procedures. Participant information will be documented in the original case report forms (CRFs) in accordance with Good Clinical Practice requirements. Data will be double-entered independently by two trained staff members into pre-designed Excel spreadsheets, followed by cross-validation to ensure accuracy. Any discrepancies identified will be resolved and, if necessary, corrected by the designated data manager, with a complete audit trail maintained. Access to the de-identified original dataset may be provided upon reasonable request to the corresponding author, subject to approval by the principal investigator and relevant ethics committee. The confidentiality of all participants’ personal information will be strictly protected at all times. Study records will be securely stored—paper in locked archives, electronic on password-protected, access-restricted systems—and retained for at least five years after publication per regulatory requirements.
Quality Control
Subjects were enrolled according to predefined diagnostic, inclusion, and exclusion criteria. All assessors underwent standardized training to ensure consistency in pressure pain threshold measurement and scale application. CRFs were uniformly prepared, coded, and completed in strict compliance with the protocol. Blinding was implemented by maintaining separation between operators and statisticians, with data analysts kept blinded. Participants provided written informed consent, and their contact information was recorded to facilitate follow-up during the washout period; all sampling and examinations were provided free of charge under study funding. Independent monitors conducted random inspections at 10% and 90% of enrollment to verify data quality and protocol adherence, with corrective actions taken as required.
Patient and Public Involvement
Neither the patients nor the public were involved in the design, or conduct, or reporting, or dissemination plans of the research. The study results will be disseminated to all patients at the end of the trial.
Discussion
This study analyzes the mechanism of acupoint sensitization from the perspective of a non-targeted to targeted combination. Based on metabolomics and proteomics, it conducts a more comprehensive and objective exploration of the local microenvironment of reduction in acupoint pain threshold. The study directly enrolls clinical patients for detection and sampling. Compared to animal experimental models, this approach more accurately reflects the characteristics of human acupoint sensitization by minimizing biases arising from interspecies differences, thereby offering direct evidence to elucidate clinically relevant mechanisms. Compared with clinical research that examines the acupoint sensitization in healthy individuals and patients,6 the study’s design employs a cross-sectional model, with comparisons made between sensitized and non-sensitized acupoints in the same patient. This design avoids inter-subject variability and ensures that the observed differences in the local microenvironment are primarily attributable to sensitization rather than other confounding factors.
The reduction of pain threshold is a common type of sensory abnormality at acupoints, exhibits marked interindividual variability in its phenotypic expression. Current clinical evidence indicates that the prevalence of acupoint sensitization in the general population is approximately 70%,33 and there is a lack of specific definition for the pain sensitization threshold of CV12. Consequently, we do not use a fixed threshold value to define the occurrence of acupoint sensitization, but instead assess it by comparing the differences between the acupoint and non-acupoint. Based on previous studies on acupoint pain sensitization and our preliminary experimental results,6 a 10 N difference is established as the threshold for the occurrence of acupoint sensitization. This threshold-based approach avoids reliance on subjective “open/close” states and instead emphasizes measurable, reproducible phenomena that can be correlated with molecular data.34 By doing so, we strengthen the clinical validity of sensitization categories.
In this study, tissue fluid samples are collected using the suction blister technique. This technique is widely applied in disease mechanism research, and its operational standardization and ethical compliance are rigorously verified.35 The suction blister technique offers the advantages of being easy to operate, non-invasive, and suitable for in vivo use.36 Previous research indicates that bubble fluid holds potential applicability in the study of disease mechanisms and biomarker identification.37 This technique involves using negative pressure to draw the tissue fluid located deep beneath the skin to the surface.38 Compared with microdialysis, the technique for sampling tissue fluid not only overcomes the limitations imposed by the permeability of semi-permeable membranes but also more accurately reflects the microenvironmental characteristics of local tissues.39 Therefore, we propose that tissue fluid samples collected through the suction blister technique can effectively capture changes in the local microenvironment surrounding acupoints and serve as a reliable basis for assessing pain sensitization.
Current clinical studies have been able to observe a decrease in the pain threshold at the acupoints, but the reason for this change remains unclear. Mechanistic studies are mainly based on animal models or mainly focus on the changes of specific substances or related pain receptors within the acupoint area.13 Most of these investigations conduct meticulous mechanistic dissection analyses of only one or two types of pain-inducing substances or inflammatory mediators, resulting in a relatively narrow research perspective. This limitation hinders a comprehensive understanding of the complex mechanisms involved in the phenomenon.40 This study innovatively uses local tissue fluid collected from acupoints of clinical patients as the research sample. This methodology offers a more accurate reflection of the pathological and physiological characteristics associated with human acupoint pain sensitization. The study implements a multi-omics integrated analysis strategy, employing non-targeted proteomics41 and metabolomics42 techniques to perform a systematic and unbiased comprehensive profiling of the acupoint microenvironment, thereby overcoming the limitations of previous studies focusing on limited components. Furthermore, by integrating targeted verification techniques, quantitative analysis of key substances is conducted to clearly identify the changes in the concentrations of local related substances caused by the reduction of pain threshold at the acupoints. We will employ the Simple Western-Jess system during the protein quantification verification phase, which offers high-throughput and automated operation, reducing human error and providing precise quantification of target protein expression levels with enhanced sensitivity.43 By utilizing these accurate detection technologies, we aim to more objectively analyze the local microenvironment of acupuncture point sensitization, thereby achieving a more comprehensive biological understanding. Physiologically, we anticipate that sensitized acupoints will demonstrate altered profiles of pain-related mediators, such as HA, 5-HT, SP, and CGRP, consistent with neurogenic inflammation and mast cell activation. Our multi-omics analysis will allow us to assess these mediators within a broader network of metabolic and proteomic changes, potentially identifying novel biomarkers of sensitization.
This study is the first to combine blister fluid and multi-omics approaches to investigate the local microenvironment of acupoint sensitization, providing a more comprehensive and objective reflection of the sensitization phenomenon. However, there are some limitations. First, acupoint sensitization includes various types, such as pain sensitization, heat sensitization, and morphological changes. Our research focuses solely on pain sensitization in CAG patients, so the results are limited to explaining pain sensitization associated with this disease and cannot be applied to other forms of sensitization. Secondly, this study adopted a cross-sectional design, which only allowed for the analysis of the correlation between the microenvironment of the sensitized acupoints and the severity of the disease, but was unable to explore the dynamic changes of metabolites or assess their correlation with the therapeutic effect of acupuncture.
Acknowledgments
The authors would like to thank all the staff at the hospitals that recruited the participants.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study is supported by the National Key R&D Program of China (Project No. 2022YFC3500600) and by the “Jiebang Guashuai” Project of Beijing University of Chinese Medicine (Project No. 2022-JYB-JBZR-025).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Li Y, Yu Y, Liu Y, et al. Mast cells and acupuncture analgesia. Cells. 2022;11(5):860. doi:10.3390/cells11050860
2. Cui X, Zhang W, Sun JH, et al. Correlation between referred pain distribution and acupoint sensitization in patients with intestinal diseases. Zhongguo Zhen Jiu. 2019;39(11):1193–12. doi:10.13703/j.0255-2930.2019.11.016
3. Tan H, Tumilty S, Chapple C, et al. Acupoints sensitization in people with and without chronic low back pain:A matched-sample cross-sectional study. J Back Musculoskelet Rehabil. 2023;36(1):137–146. doi:10.3233/BMR-210297
4. Huang S, Li L, Liu J, et al. The preventive value of acupoint sensitization for patients with stable angina pectoris: a randomized, double-blind, positive-controlled, multicentre trial. Evid Based Complement Alternat Med. 2021;2021:7228033. doi:10.1155/2021/7228033
5. Tan H, Tumilty S, Chapple C, et al. Understanding acupoint sensitization: a narrative review on phenomena, potential mechanism, and clinical application. Evid Based Complement Alternat Med. 2019;2019:6064358. doi:10.1155/2019/6064358
6. Ben H, Li L, Rong PJ, et al. Observation of Pain-Sensitive points along the meridians in patients with gastric ulcer or gastritis. Evid Based Complement Alternat Med. 2012;2012:130802. doi:10.1155/2012/130802
7. Xu GX, Zhou YM, Sun MS, et al. Clinical observation on distribution characteristics and rules of pain sensitivity points on body surface in patients with knee osteoarthritis. Zhongguo Zhen Jiu. 2020;40(11):1198–1201. doi:10.13703/j.0255-2930.20190928-k0001
8. Lv Y, Jiang Z, Zhang J, et al. Research trends and hotspots of acupuncture therapy on allergic diseases from 2004 to 2024: a bibliometric analysis. J Multidiscip Healthc. 2025;18:4071–4087. doi:10.2147/JMDH.S528646
9. Ruyi Z. Clinical Study on Acupuncture Treatment of Chronic Non-Atrophic Gastritis Based on the Theory of Acupoint Sensitization. Kunming: Yunnan University of Traditional Chinese Medicine; 2021.
10. Jiang S, Zhao JS. The historical source of “Trigger points”: classical Ashi points. World J Acupunct Moxibustion. 2016;26(2):11–14. doi:10.1016/S1003-5257(17)30003-X
11. Siracusa R, Paola RD, Cuzzocrea S, et al. Fibromyalgia: pathogenesis, mechanisms, diagnosis and treatment options update. Int J Mol Sci. 2021;22(8):3891. doi:10.3390/ijms22083891
12. Wesselmann U, Lai J. Mechanisms of referred visceral pain: uterine inflammation in the adult virgin rat results in neurogenic plasma extravasation in the skin. Pain. 1997;73(3):309–317. doi:10.1016/S0304-3959(97)00112-7
13. Cui X, Liu K, Gao X, et al. Advancing the understanding of acupoint sensitization and plasticity through cutaneous C-Nociceptors. Front Neurosci. 2022;16:822436. doi:10.3389/fnins.2022.822436
14. Shi H, Cheng B, Li JH, et al. Involvement of mast cells and substance P in sensitization of acupoints in acute gastric mucosal injury rats. Zhen Ci Yan Jiu. 2010;35(5):323–329. doi:10.13702/j.1000-0607.2010.05.001
15. Xing B, Huang M, Zhang D, et al. Metabolite profile characteristics of acupoint sensitization induced by myocardial ischemia and acupuncture effect. Zhen Ci Yan Jiu. 2018;43(7):433–439. doi:10.13702/j.1000-0607.180066
16. Kuang W, Xu J, Xu F, et al. Current study of pathogenetic mechanisms and therapeutics of chronic atrophic gastritis: a comprehensive review. Front Cell Dev Biol. 2024;12:1513426. doi:10.3389/fcell.2024.1513426
17. Sikandar S, Dickenson AH. Visceral pain: the ins and outs, the ups and downs. Curr Opin Support Palliat Care. 2012;6(1):17–26. doi:10.1097/SPC.0b013e32834f6ec9
18. Fang Y, Han S, Li X, et al. Cutaneous hypersensitivity as an indicator of visceral inflammation via C-Nociceptor axon bifurcation. Neurosci Bull. 2021;37(1):45–54. doi:10.1007/s12264-020-00577-5
19. Peiming Z. Data Mining of Ancient Literature on Acupuncture for Chronic Gastritis and Observation of Distribution Patterns of Body Surface Sensitization Points/Areas. Changsha: Hunan University of Chinese Medicine; 2021. doi:10.27138/d.cnki.ghuzc.2020.000483
20. Merz B, Frommherz L, Rist MJ, et al. Dietary pattern and plasma BCAA-Variations in healthy men and women-results from the KarMeN study. Nutrients. 2018;10(5):623. doi:10.3390/nu10050623
21. Fetse J, Olawode EO, Deb S. Personalized medicine approach to proteomics and metabolomics of cytochrome P450 enzymes: a narrative review. Eur J Drug Metab Pharmacokinet. 2024;49(6):661–676. doi:10.1007/s13318-024-00912-5
22. Rosoff DB, Davey Smith G, Mehta N, et al. Evaluating the relationship between alcohol consumption, tobacco use, and cardiovascular disease: a multivariable Mendelian randomization study. PLoS Med. 2020;17(12):e1003410. doi:10.1371/journal.pmed.1003410
23. Thyfault JP, Bergouignan A. Exercise and metabolic health: beyond skeletal muscle. Diabetologia. 2020;63(8):1464–1474. doi:10.1007/s00125-020-05177-6
24. Bub A, Kriebel A, Dörr C, et al. The Karlsruhe Metabolomics and Nutrition (KarMeN) study: protocol and methods of a cross-sectional study to characterize the metabolome of healthy men and women. JMIR Res Protoc. 2016;5(3):e146. doi:10.2196/resprot.5792
25. Wallace M, Hashim YZ, Wingfield M, et al. Effects of menstrual cycle phase on metabolomic profiles in premenopausal women. Hum Reprod. 2010;25(4):949–956. doi:10.1093/humrep/deq011
26. STROBE statement--checklist of items that should be included in reports of observational studies (STROBE initiative). Int J Public Health. 2008;53(1):3–4. doi:10.1007/s00038-007-0239-9
27. Shah SC, Piazuelo MB, Kuipers EJ, et al. AGA clinical practice update on the diagnosis and management of atrophic gastritis: expert review. Gastroenterology. 2021;161(4):1325–1332.e7. doi:10.1053/j.gastro.2021.06.078
28. Chinese Society of Gastroenterology, Cancer Collaboration Group of Chinese Society of Gastroenterology, Chinese Medical Association. Guidelines for diagnosis and treatment of chronic gastritis in China (2022, Shanghai). J Dig Dis. 2023;24(3):150–180. doi:10.1111/1751-2980.13193
29. Wu XD, Huang LX, Zhao JS. Interpretation of China national standard nomenclature and location of meridian points (GB/T 12346-2021). Zhongguo Zhen Jiu. 2022;42(5):579–582. doi:10.13703/j.0255-2930.20220117-k0001
30. MacDonald EA, Katz EL, Pearson TF, Harris JE. Performing suction blister skin biopsies. Curr Protoc. 2024;4(6):e1073. doi:10.1002/cpz1.1073
31. Alseekh S, Aharoni A, Brotman Y, et al. Mass spectrometry-based metabolomics: a guide for annotation, quantification and best reporting practices. Nat Methods. 2021;18(7):747–756. doi:10.1038/s41592-021-01197-1
32. Gawor A, Bulska E. A standardized protocol for assuring the validity of proteomics results from liquid chromatography-high-resolution mass spectrometry. Int J Mol Sci. 2023;24(7):6129. doi:10.3390/ijms24076129
33. Yumei Z. Clinical Observation Study on Acupoint Sensitization Phenomenon in Knee Osteoarthritis. Chengdu: Chengdu University of Traditional Chinese Medicine; 2019.
34. Liu K, Lin Y, Rao T, et al. Acupressure attenuates fibromyalgia central sensitization via MAPK phosphorylation-mediated neuroinflammation regulation. J Orthop Surg Res. 2025;20(1):622. doi:10.1186/s13018-025-05986-8
35. Wiig H, Swartz MA. Interstitial fluid and lymph formation and transport: physiological regulation and roles in inflammation and cancer. Physiol Rev. 2012;92(3):1005–1060. doi:10.1152/physrev.00037.2011
36. Angeletti F, Kaufmann R. Suction blister epidermal graft (SBEG) - an easy way to apply this method. J Dtsch Dermatol Ges. 2019;17(4):468–471. doi:10.1111/ddg.13801
37. Zweiman B, Kaplan AP, Tong L, et al. Cytokine levels and inflammatory responses in developing late-phase allergic reactions in the skin. J Allergy Clin Immunol. 1997;100(1):104–109. doi:10.1016/s0091-6749(97)70201-x
38. Torres-Terán I, Venczel M, Stieler T, et al. Prediction of subcutaneous drug absorption - Characterization of subcutaneous interstitial fluids as a basis for developing biorelevant in vitro models. Int J Pharm. 2023;638:122906. doi:10.1016/j.ijpharm.2023.122906
39. Wang X, Li X, Gao Y, et al. Knowledge mapping of acupoint sensitization and acupoint specificity: a bibliometric analysis. Front Neurosci. 2023;17:1292478. doi:10.3389/fnins.2023.1292478
40. Samant PP, Niedzwiecki MM, Raviele N, et al. Sampling interstitial fluid from human skin using a microneedle patch. Sci Transl Med. 2020;12(571):eaaw0285. doi:10.1126/scitranslmed.aaw0285
41. Kool J, Reubsaet L, Wesseldijk F, et al. Suction blister fluid as potential body fluid for biomarker proteins. Proteomics. 2007;7(20):3638–3650. doi:10.1002/pmic.200600938
42. Wiig H, Luft FC, Titze JM. The interstitium conducts extrarenal storage of sodium and represents a third compartment essential for extracellular volume and blood pressure homeostasis. Acta Physiol. 2018;222(3). doi:10.1111/apha.13006
43. Liu Y, Beyer A, Aebersold R. On the dependency of cellular protein levels on mRNA abundance. Cell. 2016;165(3):535–550. doi:10.1016/j.cell.2016.03.014
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Transcutaneous Electrical Acupoint Stimulation for Moderate to Severe Pain in Hepatocellular Carcinoma: A Protocol for a Randomized Controlled Trial
Wu P, Zhu L, Zheng SY, Li JX, Wu MD, Wang WJ, Hou YC, Li J, Wu HG
Journal of Pain Research 2022, 15:1889-1896
Published Date: 6 July 2022
Vitamin B6 Metabolic Pathway is Involved in the Pathogenesis of Liver Diseases via Multi-Omics Analysis
Mei M, Liu D, Tang X, You Y, Peng B, He X, Huang J
Journal of Hepatocellular Carcinoma 2022, 9:729-750
Published Date: 11 August 2022
In vitro Activity of Cefepime/Avibactam Against Carbapenem Resistant Klebsiella pneumoniae and Integrative Metabolomics-Proteomics Approach for Resistance Mechanism: A Single-Center Study
Wen L, Luo C, Chen X, Liu T, Li X, Wang M
Infection and Drug Resistance 2023, 16:6061-6077
Published Date: 11 September 2023
The Impact of Immune Cells, Metabolites, Inflammatory Factors, and Circulating Proteins on Atopic Dermatitis: Insights from a Mendelian Randomization Study
Zhou D, Gan G, Song S, Zi C, Bao Y, Hao W, Chen Q
Clinical, Cosmetic and Investigational Dermatology 2024, 17:2999-3011
Published Date: 21 December 2024
Distinct and Shared Molecular Mechanisms in Pediatric Antrochoanal Polyps and Chronic Rhinosinusitis with Nasal Polyps: A Proteomic and Metabolomic Integrative Analysis
Chen YC, Wang X, Pan YW, Teng YS, Pan HG
Journal of Inflammation Research 2025, 18:4435-4447
Published Date: 26 March 2025