Back to Journals » ImmunoTargets and Therapy » Volume 14
Prostate Cancer Immunotherapy: Time to Move Beyond Checkpoint Inhibitors
Authors Abel M, Warner AB ![]() , Karzai F, Madan RA
, Karzai F, Madan RA
Received 27 June 2025
Accepted for publication 9 September 2025
Published 13 September 2025 Volume 2025:14 Pages 1041—1052
DOI https://doi.org/10.2147/ITT.S549873
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Michael Shurin
Melissa Abel, Aanika Balaji Warner, Fatima Karzai, Ravi A Madan
Genitourinary Malignancies Branch, Center for Cancer Research, National Institutes of Health, Bethesda, MD, USA
Correspondence: Ravi A Madan, Email [email protected]
Abstract: Immune checkpoint inhibitors (ICIs) have led the advancement of cancer immunotherapy, with remarkable efficacy in many cancers. Prior to the advent of ICIs, prostate cancer had one of the first approvals for cancer immunotherapy with sipleucel-T, an anti-cancer vaccine. Despite this early success, ICIs have since failed to improve outcomes for most patients with prostate cancer, generating a narrative that prostate cancer is resistant immunotherapeutic approaches. Novel therapies like CAR T-cells, bispecific antibody therapies, anti-cancer vaccines and cytokine therapies are now generating early evidence for how the prostate cancer tumor immune microenvironment can be manipulated beyond checkpoint inhibition. Most notably, clinical trials with bispecific T-cell engagers (BiTEs) targeting tumor antigens like STEAP-1 and KLK2 have shown clinical promise. Moving beyond ICIs may lead to new approaches to alter the prostate cancer tumor immune microenvironment and improve clinical outcomes.
Keywords: prostate cancer, immunotherapy, immune checkpoint inhibitors
Introduction
Over the past 15 years, the development and expansion of immune checkpoint inhibitors (ICIs) across oncologic tumor types have been unprecedented. Rarely has a single therapeutic strategy led to so many regulatory approvals in varied cancers. Unfortunately, in prostate cancer immune checkpoint inhibitors have proved to be disappointing and rarely have clinical activity beyond a small subset of patients (microsatellite instability or high tumor mutational burden). These circumstances are not unique to prostate cancer, as not all tumors respond to ICIs. Undeterred by early data demonstrating a lack of single agent activity, multiple trials explored immune checkpoint-based combinations. Unfortunately, the results were unsuccessful and benefits from ICI could not be improved through combination therapy.
These results from ICI trials have painted a picture of a tumor that is not amenable to immunotherapy. Existing and emerging data, however, suggests that other immunotherapeutic approaches may be warranted in the treatment of prostate cancer (Figure 1). The first FDA approved immunotherapy in the modern era, sipuleucel-T, demonstrated clinical benefit in prostate cancer. More recently, other immune modalities have suggested the potential for clinical benefit in prostate cancer based on early clinical results. These data together suggest that there is a future for immunotherapeutic development with the field finally moving beyond ICIs.
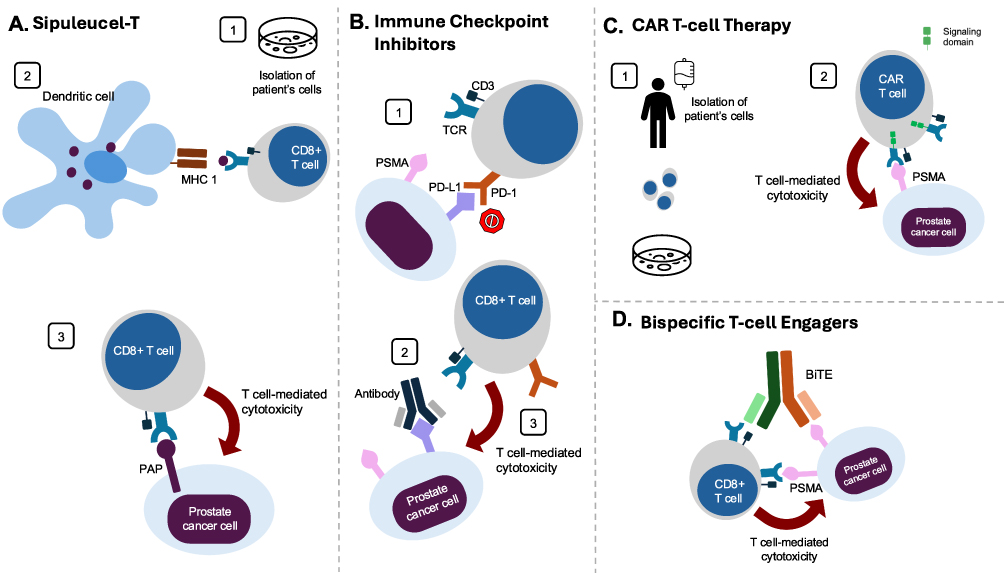 |
Figure 1 Mechanisms of action of immunotherapies. (A) Immune checkpoint inhibitors 1A) Multiple immune checkpoint inhibitor receptors exist; this example highlights the interaction between PD-1 found on the T-cell and PD-L1 found on the prostate cancer cell. PD(L)1 interaction acts as a “brake” on the immune system, halting further immune-mediated attack and is a key method by which tumor cells evade the immune system. 2A) ICIs block this interaction and allow for 3A) potentiation of the T-cell mediated cytotoxicity of the cancer cell. (B) Sipuleucel-T 1A) Via leukapheresis, the patient’s APCs are isolated and stimulated with antigen, in this example PAP-peptides, and GCSF. These activated APCs are then given back to the patient. 2B) Activated APCs present the PAP-peptides to a CD8+ T-cell. 3B) The CD8+ T cell now recognizes the foreign antigen on the cancer cell and induces apoptosis of the cancer cell. (C) CAR T-cell therapy. 1C) T-cells are removed from the patient via apheresis. These cells are then transfected with CAR which recognizes PSMA and expanded in the lab. 2C) The CAR T-cells are now re-infused into the patient. The CAR T-cell recognizes PSMA on the surface of the prostate cancer cell, binds to it, and the intracellular stimulatory domain allows for robust T-cell mediated apoptosis of the cancer cell. (D) BiTEs. The BiTE antibody contains two domains, one that recognizes CD3 on T-cells and the other that recognizes PSMA. When the antibody binds both the T-cell and prostate cancer cell, it brings these cells close together. The T-cell then recognizes the PSMA protein as foreign and induces apoptosis in the cancer cell. |
Sipuleucel-T
Antigen-directed immunotherapies (also called vaccines) have long been studied as a potential treatment for cancer.1 Harnessing the power of the immune system through “training” induced by cancer vaccines leads to a targeted, specific, and coordinated attack on cancer cells without the need for other systemic therapies. Prostate cancer has been an attractive target for cancer vaccines given its slow growing nature that allows time for the immune system to elicit a response and expression of unique proteins that reduce off-target immune effects.2 Additionally, the prostate is a non-essential organ and can be rendered non-functional due to immune cell killing without significant safety risk to the patient.3
The first and only FDA-approved cancer vaccine for prostate cancer, sipuleucel-T, is an active cellular immunotherapy consisting of the patient’s own antigen presenting cells obtained via leukapheresis and activated ex vivo with a fusion protein consisting of the antigen prostatic acid phosphatase and granulocyte-macrophage colony-stimulating factor (GM-CSF)4 (Figure 1A). The Phase III trial IMPACT (Immunotherapy Prostate Adenocarcinoma Treatment) led to the 2010 FDA approval of sipuleucel-T.5 IMPACT enrolled 512 total patients with mCRPC, of whom 341 received sipuleucel-T and 171 receive placebo. Compared to placebo, the sipuleucel-T group experienced a 22% reduction in the risk of death which translated to a 4.1-month improvement in median survival. Although PSA responses were rare, T-cell responses were seen in 73% of patients. Since sipuleucel-T was a novel immunotherapy, aspects of its mechanism of action (relative to chemotherapy) were poorly understood at the time. Thus, the lack of evidence of short-term changes in progression free survival, despite late improvements in survival, led to concern about the therapeutic efficacy of this agent. These seemingly paradoxical results are now much more accepted in the immune checkpoint inhibitor era of cancer therapeutics. Nonetheless, initial skepticism over this data and the concomitant emergence of next generation androgen receptor pathway inhibitors (ARPIs) in prostate cancer (abiraterone and enzalutamide) has minimized utilization of sipuleucel-T. Current ASCO and NCCN guidelines recommend sipuleucel-T to men with mCRPC who are minimally symptomatic without visceral metastases.6
Immune Checkpoint Inhibitors
ICIs bind to checkpoint molecules like PD-1/L1 and CTLA-4, which normally function to inhibit T-cell activation, generating a potential boost in immune-driven cancer cell death (Figure 1B). Despite significant clinical activity in many solid tumors, ICIs have failed to show clinical benefit in the treatment of unselected prostate cancer (Table 1). Anti-CTLA-4 has been evaluated in two Phase 3 trials in prostate cancer and neither study demonstrated an overall survival advantage.7,8 Monotherapy trials in mCRPC with the PD-1 inhibitors pembrolizumab and nivolumab have also yielded minimal evidence of clinical benefit.9–12 Dual-checkpoint inhibition with a combination of ipilimumab and nivolumab also failed to show benefit and led to high rates toxicity and treatment-related deaths.13 With the goal of enhancing the anti-tumor effects of ICIs in metastatic prostate cancer, numerous combination trials have been pursued, all without significant benefit to patients. In mCRPC, ICIs have been combined with docetaxel, ARPIs like enzalutamide, and with targeted therapies such as olaparib.11,14–18 All failed to meet survival endpoints.
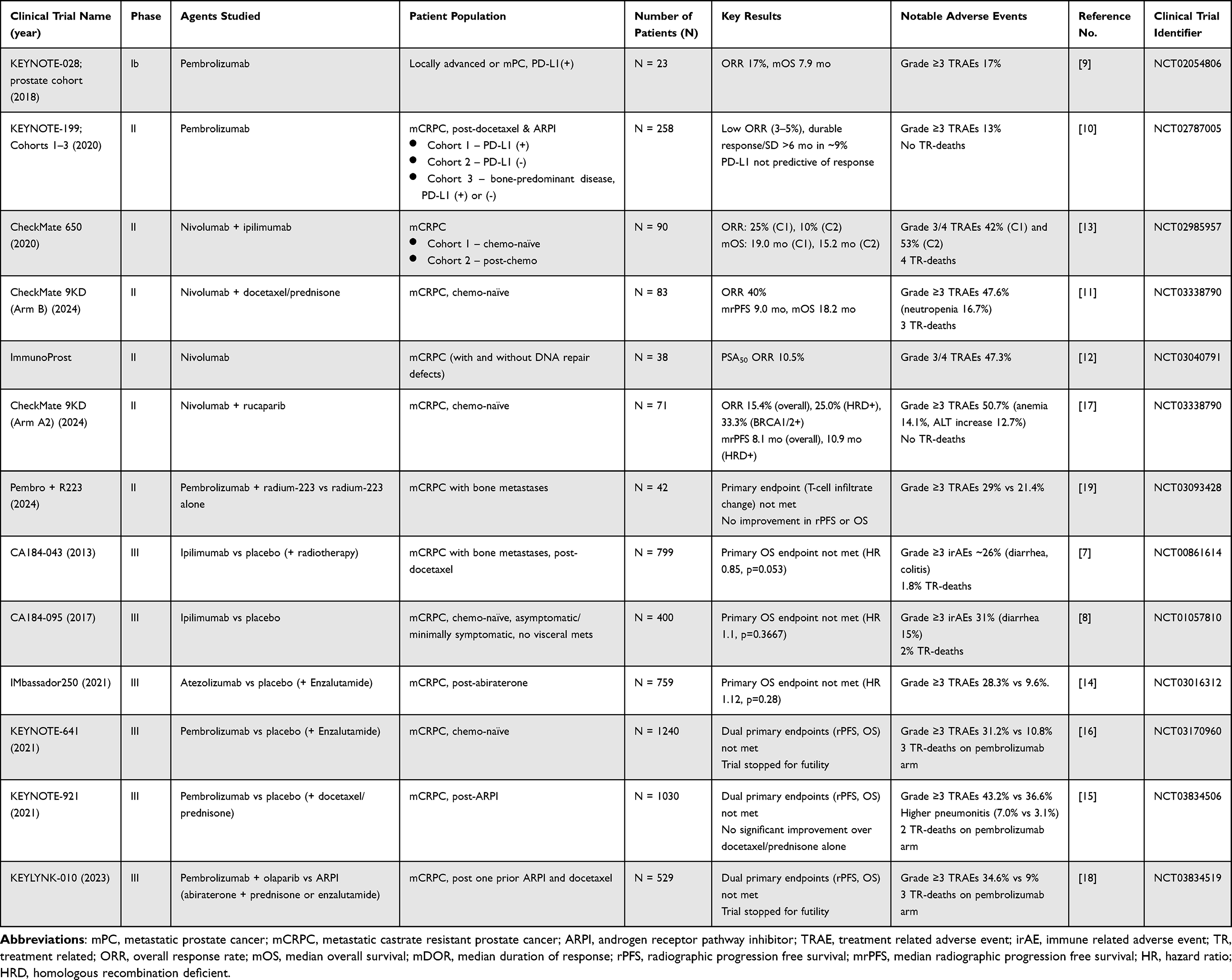 |
Table 1 Clinical Trials of Immune Checkpoint Inhibitors in Prostate Cancer |
The one notable exception in prostate cancer ICI responses is patients with germline or somatic DNA mismatch repair deficiency (dMMR) or high microsatellite instability (MSI-H).20 Tumors with dMMR/MSI-H features are particularly sensitive to ICI therapy across cancer types, which has led to the tumor-agnostic FDA approval of pembrolizumab monotherapy for these patients. While less than 5% of mCRPC tumors express these features, these patients have shown favorable responses to pembrolizumab, which is now a standard therapy recommendation for mCRPC patients in this subgroup.21 Recent results of a Phase II study of ipilimumab and nivolumab reported an average PFS of 32.7 months in patients with dMMR mCRPC, highlighting the susceptibility of these patients to ICIs.22 Optimal testing strategies for identifying dMMR/MSI-H patients are evolving, as further stratification of patients based on the number and types of positive dMMR/MSI-H tests may better identify ICI responsers.23
There is preclinical evidence that radiation therapy (RT) can boost T-cell based anti-tumor responses, which has led to many trials combining ICIs with radiation.19 In mCRPC, in patients previously treated with docetaxel, ipilimumab failed to show survival benefit over placebo immediately following bone-directed RT.7 Similarly, adding pembrolizumab to radium-223, an FDA-approved radiopharmaceutical used in mCRPC, did not lead to improved efficacy or an increase in T-cell infiltration into the tumor microenvironment.24
Additional novel ICI combination trials for prostate cancer are underway, including combinations with targeted therapies such as Pi3K/mTOR and CDK4/6 inhibitors and those with other immunotherapy approaches such as anti-cancer vaccines and cytokines.25,26 It is worth noting, however, that there has yet to be clinical success in any cancer for a Phase III ICI combination therapy when single-agent ICI did not show benefit in that tumor type. Novel immunotherapeutic targets in checkpoint inhibitory pathways are also being tested in prostate cancer. B7H3 is a protein that belongs to the B7 family and acts as an immune checkpoint. B7H3 inhibitors like enoblituzumab target a tumor-specific glycoprotein and may act as a checkpoint inhibitor.27 The B7H3 protein is highly expressed on prostate adenocarcinoma cells making it an attractive therapeutic target, and multiple studies are ongoing to assess activity.28–31 Ultimately, the field of prostate cancer therapy needs alternative approaches to leveraging anti-tumor immunity beyond standard ICI-based combinations.
CAR-T
Chimeric antigen receptor T-cell (CAR T-cell) therapy is generated by harvesting a patient’s own T-cells and genetically engineering them to express a CAR, typically accompanied by immune co-stimulatory molecules, that will bind to a known tumor antigen and home T-cells directly to tumor cells bearing the target (Figure 1C). Multiple CAR T-cell therapies have been approved for use in hematologic malignancies including ALL and B-cell lymphoma, where CD19 acts as a target, and multiple myeloma, which targets BCMA.32–34 While CAR T-cells have been investigated in multiple solid tumors, thus far there have been no approvals in this setting due to limited benefit. CAR T-cell therapy typically involves pre-treatment conditioning with lymphodepleting chemotherapy to maximize expansion of the CAR T-cells following infusion.35 A potentially dangerous side effect of CAR T-cell therapy is cytokine release syndrome (CRS), which can cause fevers and hypotension, and the related neurologic toxicity referred to as immune effector cell-associated neurotoxicity syndrome (ICANS).36 While both CRS and ICANS can be fatal, recent advances in management of these side effects using steroids and tocilizumab has reduced this risk.
CAR T-cell approaches are in the process of being explored for prostate cancer, engineered to target prostate-specific tumor antigen (PSMA) and a variety of other known tumor antigens. PSMA has become a practice-changing target used in molecular imaging of prostate cancer as well as a radiopharmaceutical target, with the approval of lutetium-177 in the mCRPC setting.37,38 PSMA is an attractive target due to high expression in prostate adenocarcinoma and low expression on healthy tissues.39 Outside of the prostate, PSMA is commonly expressed on salivary glands, and dry mouth was a notable side effect in patients receiving lutetium-177.40 Immunotherapy-based targeting of PSMA is an area of significant interest, with numerous recent Phase I trials investigating PSMA-targeted CAR-T cells.
PSMA-targeted CAR T-cells have been used in phase I clinical trials where safety and feasibility have been evaluated, resulting in toxicity like that of other established CAR T-cell therapies. However, in these small cohorts PSMA CAR T-cells have failed to show substantial anti-tumor responses in prostate cancer. One dose-escalating trial with a second-generation PSMA CAR had a best response of 2 of 7 patients with stable disease, while all patients at higher dose levels developed high fevers.41 Another Phase I dose-escalation study added IL-2 to a first-generation PSMA CAR, with the goal of boosting T-cell expansion.42 Two of five patients had PSA declines over 50%. An additional PSMA-targeted CAR called P-PSMA-101 was generated with a design meant to uniquely expand effector T-cells in the tumor microenvironment.43 While only 3/10 patients reached a PSA decline ≥50%, some radiographic responses were seen. One early treatment-related death was reported, with other toxicities at or below Grade 3. The study was terminated early due to strategic decisions by the pharmaceutical company. With the goal of overcoming an immunosuppressive tumor microenvironment to improve efficacy, PSMA CAR-Ts have been developed that block or subvert immune-inhibitory transforming growth factor (TGF)-β.44,45 This approach has shown some activity in Phase I mCRPC trials based on reduction in PSA along with expected adverse events. Multiple additional Phase I trials are ongoing with anti-PSMA CAR T-cells for metastatic prostate cancer (NCT05354375, NCT06228404, NCT06895811, NCT01140373, and NCT06046040). Larger Phase II trials will shed light on potential efficacy of additional PSMA CAR-T cell approaches.
Prostate stem cell antigen (PSCA) is a surface protein expressed on prostate tissue and up regulated in prostate cancer, making it another attractive therapeutic target.46 BPX-601, a PSCA-targeted CAR T-cell therapy, was investigated in a Phase I multi-center trial that was ultimately terminated early due to toxicity.47 Another Phase I study (NCT06193486) is evaluating safety and efficacy of delta gamma-enriched anti-PSCA CAR T-cells for the treatment of bone-metastatic CRPC. Preclinical data showed significant regression of prostate cancer bone tumors in mice when this CAR was used in with zoledronic acid pre-treatment, and clinical trial results are pending.48 An additional Phase I trial using a novel PSCA-targeted CAR led to PSA reductions of ≥30% in 4 of 14 patients with PSCA-expressing mCRPC (NCT03873805), with cases of significant radiographic improvements.49 Side effects were primarily Grade 1 or 2 cytokine release syndrome, with one dose-limiting toxicity of Grade 3 cystitis. A lack of durable remission was noted in the context of poor CAR T-cell persistence beyond 28 days. This therapy is now being combined with metastasis-directed radiotherapy in a Phase Ib trial (NCT05805371) in the hopes of improving responses.
Six-transmembrane epithelial antigen of prostate-1 (STEAP1) promotes prostate cancer growth and expressed in around 90% of prostate cancers, with low expression in normal tissues outside of the prostate. A STEAP1 CAR T-cell model had positive results in in-vitro and in-vivo preclinical studies, supporting an ongoing Phase I/II study combining anti-STEAP1 CAR T-cell therapy with enzalutamide (NCT06236139).50,51 Preclinical studies have also shown high STEAP2 expression at all stages of prostate cancer and STEAP2-targeted CAR T-cells have led to tumor responses in prostate cancer mouse models.51 AZD0754, a STEAP2-targeted CAR T-cell therapy, is being assessed in a Phase I/II multi-center study currently recruiting for patients with mCRPC (NCT06267729). STEAP1 and STEAP2 are promising emerging targets in prostate cancer, and clinical results of STEAP-targeted therapies are eagerly awaited.
Lastly, kallikrein-related peptidase 2 (KLK2) is a serine protease with expression associated with poor prognosis and a potential oncogenic role in prostate cancer and is also being investigated as a novel target for prostate cancer therapy.52 JNJ-7522941 is a KLK2 CAR undergoing Phase I dose-escalation in mCRPC patients (NCT05022849); results have not yet been reported.
Overall, CAR T-cells face similar obstacles in prostate cancer as in most solid tumors, including short duration of CAR T-cell survival and tumor microenvironment barriers. CAR T-cell therapy has yet to show the significant responses necessary to justify the toxicity of this approach in prostate cancer. Going forward, multi-pronged approaches and novel CAR designs may improve outcomes.
Bi-Specific T-Cell Engagers
Another strategy for targeted antigen-dependent T-cell activity is through bi-specific T-cell engagers (BiTEs), which are off-the-shelf therapies that combine antibodies to direct cytotoxic T-cells to tumors (Figure 1D). BiTEs have had great success in hematologic malignancies, leading to FDA approvals for acute lymphoblastic leukemia, large B-cell lymphoma, and multiple myeloma.53 Like with CAR T-cell therapy, BiTEs have faced more obstacles in treating solid tumors. However, in 2022 tebentafusp-tebn, a bispecific gp100 peptide and CD3 T-cell engager was approved for metastatic uveal melanoma.54 Subsequently, tarlatamab, a BiTE targeting CD3 and the delta-like ligand 3 (DLL3), was approved for relapsed small cell lung cancer in 2024 with a 40% response rate, generating hope for success in additional solid tumors.55
Numerous BiTEs have been designed that target similar prostate cancer tumor antigens used for CAR T-cells.56 Many different anti-PSMA/CD3 BiTEs have been designed, but despite evidence of anti-tumor activity, they have faced challenges of high toxicity and limited efficacy, with PSA drops ≥50% in only 5–31% of patients and rare radiographic responses. Early PSMA/CD3 BiTEs including pasotuxizumab (AMG212), acapatamab (AMG160), and JNJ-081, generated some PSA declines, but all studies were terminated or suspended before trial completion, in most cases due to high adverse events related to CRS.57–59 Many of these trials evaluated anti-drug antibody levels during treatment, which were frequently found in patients and hypothesized to play a role in limiting efficacy of these therapies.
There are multiple ongoing clinical trials with anti-PSMA BiTEs in prostate cancer, most of which are awaiting results. REGN5678 is a BiTE that combines an anti-PSMA domain with an anti-CD28 domain (NCT03972657). Like CD3, CD28 is a protein expressed on T-cells, but also serves as a co-stimulatory molecule driving T-cell activation.60 The trial combines this therapy with cemiplimab, an anti-PD1 immune checkpoint inhibitor, after three weeks of BiTE monotherapy. At the high dose level, three of four patients had PSA declines, all over 90%. Toxicity thus far has shown 54% of patients experiencing grade 3 or higher TRAEs, though CRS has rarely been reported and never beyond Grade 1. One patient death was considered treatment related. Another ongoing study of CC1, an anti-PSMA/CD3 BiTE that contains IgG scaffolding over the PSMA antibody, has shown rapid PSA reductions of up to 60% with an overall favorable toxicity profile.61 While CRS has been common, reported in 79% of patients thus far, all cases were Grade 1–2. This trial is ongoing (NCT04104607) and has led to development of a second trial in the biochemically recurrent prostate cancer setting (NCT05646550).
Beyond PSMA, BiTES targeting other tumor antigens, such as KLK2, STEAP1/2, HER-2, and DLL3 are being investigated in prostate cancer.62 Recent Phase I reports of pasritamig (JNJ-78278343), a first-in-class BiTE targeting KLK2 and CD3, showed a remarkably tolerable safety profile with only 9.8% of patients experiencing grade ≥3 adverse events and preliminary therapeutic activity with a 42.4% rate of PSA declines ≥50%.63,64 Perhaps the most promising results have come from xaluritamig (AMG509), a bispecific antibody with anti-CD3 and two anti-STEAP1 domains that has shown significant anti-tumor activity in mCRPC.65 Phase I data in 97 patients showed PSA declines in all dose levels, with drops ≥50% in 49% of patients and a radiographic overall response rate of 24% per RECIST.66 Of the 52 patients in highest dose level cohort, PSA responses ≥50% were seen in 59% with an overall response rate of 41%. CRS occurred in 72% of patients, but with only two Grade 3 cases. Dose-limiting toxicities occurred in 24% of patients with 19% discontinuing treatment due to toxicity. Patients in this trial were heavily pre-treated, with over half bearing visceral metastasis and 85% who had previously received chemotherapy. Anti-tumor activity was seen in both visceral and bone disease. Xaluritamig is now undergoing a Phase III clinical trial in patients with mCRPC67 as well as studies in the localized and biochemically recurrent settings, and the results are eagerly anticipated (NCT06613100, NCT06555796).
Cytokines
ICIs, bispecifics and CAR-T strategies are all based on the efficacy and therapeutic potential T-cells. It is well known that other immune cells play critical roles in the tumor microenvironment beyond T-cells, including myeloid derived suppressor cells (MDSCs) and tumor associated macrophages (TAMs). Furthermore, unlike T-cells, natural killer (NK) cells have been associated with better long-term outcomes when seen in prostatectomy samples.68 Cytokines present a unique opportunity to impact the broader immune microenvironment beyond T-cells and can activate NK cells, decrease MDSCs and convert pleiotropic TAMs to an anti-tumor phenotype.69
Cytokines are small paracrine and autocrine molecules that mediate essential immune cell functions, and there is substantial preclinical data showing their potential to enhance anti-tumor immunity.70 Historically, cytokines like IL-2 and TNF-a have had a significant impact on cancers such as kidney cancer and melanoma, respectively. Even though rare cures were seen, their utility was limited by the significant toxicity seen with these therapies. Novel cytokine therapies with lower toxicity are under development and may offer a means to overcome the resistance the tumor microenvironment imposes and recruit a broader range of immune responses beyond T-cells.
Interleukin-2 (IL)-2 plays a critical role in the recruitment of natural killer (NK) and CD8+ T cells.69,71 This cytokine has a duality in function: it also stimulates T regulatory cells (T-regs), an unwanted side effect. Multiple adjustments have been made to improve IL-2’s ability to activate the immune system and decrease the immunosuppressive effects, however, there have been severe dose-limiting toxicities of IL-2 in other solid tumors, which has limited this cytokine’s success is prostate cancer. IL-15 is similar in function to IL-2, except that it does not activate T-regs, making it an attractive alternative. In order to overcome IL-15’s short half-life and complicated attachment to its receptors, a superagonist, N-803, was designed to be co-administered. N-803 has recently been FDA approved when added to bacillus Calmette-Guerin (BCG) for the treatment of BCG-unresponsive non-muscle invasive bladder cancer.72 This combination resulted in 90–94% cystectomy-free survival at 2 years and a high proportion of complete responses, depending on staging. Currently, trials are in early stages to evaluate this drug’s effectiveness in prostate cancer.
IL-12 is a pro-inflammatory cytokine that mediates the transition from the innate to adaptive immune system, with the potential to enhance anti-tumor immune activity.73 Secretion of IL-12 from phagocytes and dendritic cells stimulates cytotoxic NK cells, NKT cells and CD8+ T-cells, and promotes the Th1 differentiation of CD4+ T-cells resulting in secretion of additional cytokines that promote cell-mediated immunity. There is evidence to suggest IL-12 plays a crucial role counteracting the immunosuppressive nature of the tumor microenvironment by inhibiting Tregs and attracting target cells into the heart of the tumor.74 Preliminary data has suggested that a tumor targeting IL-12 cytokine/fusion protein (PDS01ADC) monotherapy can impact NK cells, NK activity and potentially impact the tumor in some prostate cancer patients as measured by PSA.75 Current trials underway with this agent include NCT04633252, a phase I/II study in combination with docetaxel and abiraterone (mCSPC) or in combination with docetaxel (mCRPC). Another trial based on potential NK synergies is combining PDS01ADC with enzalutamide in biochemically recurrent prostate cancer (NCT06096870).
Certain cytokines can alternatively have an immunosuppressive effect in the tumor microenvironment, and in some cases promote tumor growth. Therapeutic strategies have been developed to deplete cytokine signaling that could be immune suppressive. Preclinical data suggests that castration increases Il-8, which may promote prostate cancer disease progression.76 Two early phase clinical trials are being conducted to evaluate the role of IL-8 blockade: the MAGIC-8 phase Ib/II trial combines ADT with nivolumab ± IL-8 blockade (NCT03689699) but thus far has not shown a therapeutic difference with IL-8 blockade.77 Another phase I trial has demonstrated safety of an anti-IL-8 monoclonal antibody (HuMax-IL8) in unresectable solid tumors, including prostate cancers (NCT02536469).78
MDSCs can be immune suppressive and promote tumor growth. CXCR2 has been implicated as a receptor on MDSCs that can be activated by chemokines (a subcategory of cytokines) which are produced by the prostate cancer tumor itself.79 As with IL-8, CXCR2 binding can allow MDSCs to promote tumor growth. A clinical trial has suggested that blocking CXCR2 in prostate cancer patients receiving enzalutamide could enhance responses as measured by PSA and imaging.80 Future studies with this strategy are under consideration.
Future Perspectives
Clinical development of prostate cancer immunotherapy thus far has been slow despite the initial approval of sipuleucel-T in 2010, predating the ICI era in oncology.5 The subsequent inability to demonstrate efficacy of ICIs beyond a very small subset led to several negative combination studies (Table 1). Such studies are not unique to prostate cancer. Indeed, no ICI has demonstrated efficacy in a combination approach in a tumor type where that ICI did not have proven independent activity already. This reality would suggest that ICI-based combinations are likely additive and not synergistic. If that is correct, the concept of turning a “cold tumor hot” (eg, making ICIs work in combination in a tumor type where they have no single agent activity) is likely not a realistic goal for future studies.
Finally, after nearly a decade of negative trials of ICIs in prostate cancer, there is new hope on the therapeutic horizon (Table 2). While CAR-Ts have demonstrated little promise, emerging data is much more promising with bispecific strategies. Bispecifics involving the targets KLK2 and STAEP2 have yielded promising clinical data, and more definitive trials are already underway.63,65 Additional strategies such as immunocytokines could enhance immune compartments beyond T-cells, impacting NKs while also potentially limiting the immune suppressive effects of MDSCs and TAMs.69,75,80 Expanding our knowledge of tumor surface targets and ideal antigen characteristics, well reviewed elsewhere, will be key in the development of novel therapies.81
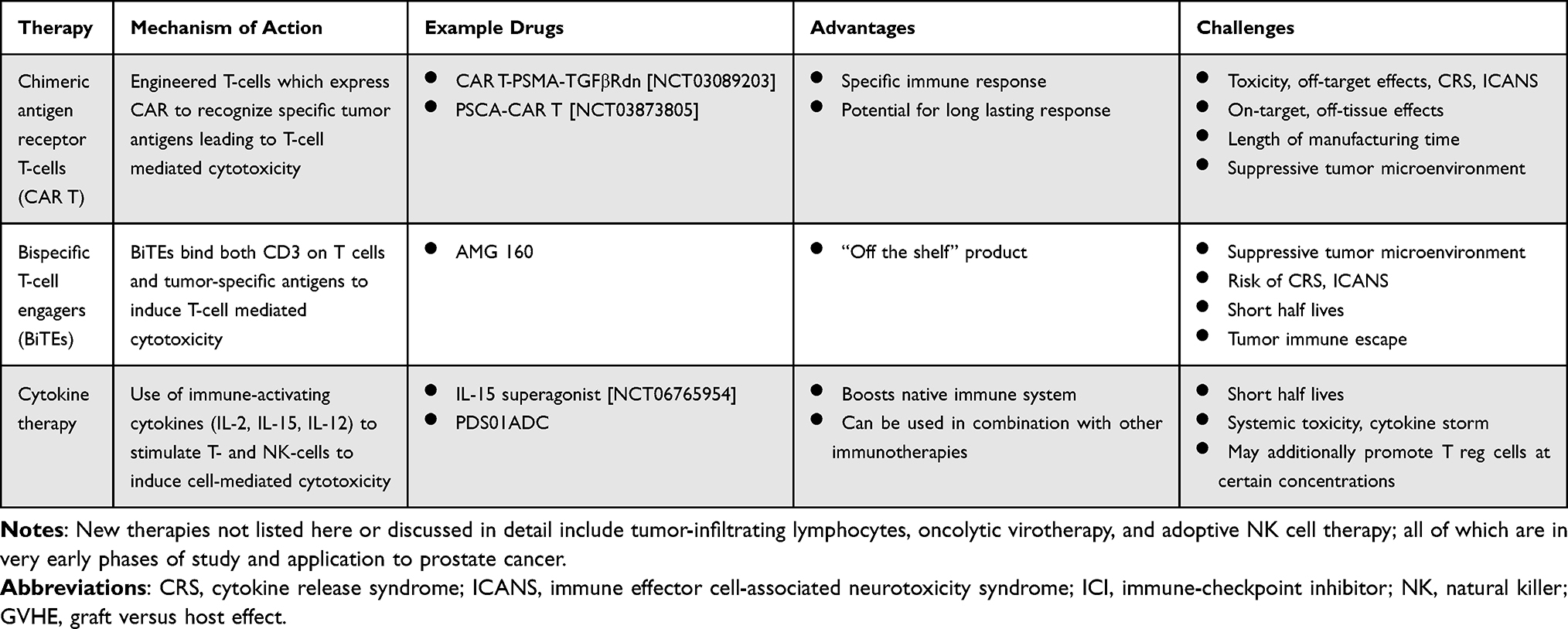 |
Table 2 Emerging Therapies for Prostate Cancer |
Combination strategies may remain an appropriate strategy beyond the concept of turning a cold tumor hot. NK cells may be important effectors within the immune microenvironment and have been associated with long term metastasis free survival.68 Emerging data suggest that standard therapies in prostate cancer such as enzalutamide and docetaxel are associated with increased NK cells and NK cell activation.82–84 It may be possible to further enhance these NK cell populations with immunotherapies to prolong the benefits of enzalutamide and docetaxel or perhaps delay therapeutic resistance. This strategy is being investigating in ongoing studies (eg NCT06096870).
It is also noteworthy that the research focus for phase 3 trials is shifting to earlier disease states. It is possible that patients in earlier stages of prostate cancer with less tumor volume and perhaps those who are less heavily pre-treated could have responses to immunotherapy that might otherwise be less effective when bulky tumors are entrenched in the dense bone microenvironment as is common with advanced metastatic prostate cancer.85 One stage of disease that is of growing interest is biochemically recurrent prostate cancer (BCR). This population of patients has residual disease after definitive surgery and/or radiation which was unfortunately not curative. Initially, these patients will only have disease detected by a rising serum tumor marker, PSA. Over time, it is likely that they will have disease seen on modern molecular imaging (eg prostate specific membrane antigen imaging or PSMA PET). Such patients have no proven therapy to extend their survival and have a long timeline (most times beyond 5 years) to benefit from immunotherapy before clinical progression.86
Indeed, there is data from an immunotherapy that shows potential differential outcomes in BCR compared to metastatic disease. PROSTVAC is a PSA targeting immunotherapy that had a negative phase 3 trial in advanced castration resistant prostate cancer.87,88 Although cross-trial comparisons are not ideal, it may be noteworthy that two Phase 2 studies in BCR with PROSTVAC showed PSA declines in about 1/3 of patients, something not reported in the phase 3 trial in metastatic disease.89,90 Such declines were often delayed showing the potential benefits using immunotherapy in an earlier stage of disease such as BCR where patients are asymptomatic for years. Interestingly, one of these trials associated PSA declines with changes on PSMA imaging as well.90
In addition to extended timelines to allow for an immune response, other key biologic factors differ when BCR is compared to mCRPC, the stage where most prostate cancer immunotherapies have been investigated. In BCR, tumor burden is very low as this is the minimal residual disease state. It appears at this stage that most of the disease is located in the lymph nodes; a location potentially more accessible to the immune cells than disease in late-stage patients which is predominantly harbored in the dense fibrous matrix of the bone. Furthermore, BCR patients need not have testosterone lowering therapy, so it may be possible to evaluate immunotherapy in the patients without testosterone suppression.85 It is not fully known what effects testosterone suppression may have on the immune system, but long-term castration may have negative impact over time that diminishes some of the immune capabilities within patients.
Conclusion
Prostate cancer immunotherapy is poised to emerge from a latent phase of clinical development, unfettered by the need to make ICIs therapeutically effective. The most promising current strategies include bispecifics targeting prostate specific antigens without ICIs. Despite limited benefit seen thus far, CAR-T remains an active area of research as well. Immunocytokines or cytokine blocking agents may further yield data from early studies by impacting immunotherapy effectors beyond the T-cells. While it is fair to say that prostate cancer not responsive to one type of immunotherapy (ICIs), it is likely premature for it to be labeled as non-responsive to immunotherapy. Modern immunotherapeutic strategies beyond ICIs are being investigated in all stages of prostate cancer. If these therapies can demonstrate clinical efficacy and minimal toxicity, they may dramatically change how we think about immunotherapy in prostate cancer as well as all other cancers that do not response to immune checkpoint inhibition.
Abbreviations
APC, antigen presenting cells; ICIs, immune checkpoint inhibitors; PAP, prostatic acid phosphatase; GCSF, granulocyte colony stimulating factor; BiTE, Bispecific T-cell engager; PSMA, prostate surface membrane antigen; CAR, chimeric antigen receptor.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sellars MC, Wu CJ, Fritsch EF. Cancer vaccines: building a bridge over troubled waters. Cell. 2022;185:2770–2788. doi:10.1016/j.cell.2022.06.035
2. Schlom J, Hodge JW, Palena C, et al. Therapeutic cancer vaccines. Adv Cancer Res. 2014;121:67–124. doi:10.1016/B978-0-12-800249-0.00002-0
3. Drake. Update on prostate cancer vaccines. Cancer J. 2011;17(5):294–299. doi:10.1097/PPO.0b013e3182325e78
4. Madan RA, Antonarakis ES, Drake CG, et al. Putting the pieces together: completing the mechanism of action jigsaw for sipuleucel-T. J Natl Cancer Inst. 2020;112(6):562–573. doi:10.1093/jnci/djaa021
5. Kantoff PW, Higano CS, Shore ND, et al. Sipuleucel-T immunotherapy for castration-resistant prostate cancer. N Engl J Med. 2010;363(5):411–422. doi:10.1056/NEJMoa1001294
6. Garje R, Riaz IB, Naqvi SA, et al. Systemic therapy in patients with metastatic castration-resistant prostate cancer: ASCO guideline update. J Clin Oncol.
7. Kwon ED, Drake CG, Scher HI, et al. Ipilimumab versus placebo after radiotherapy in patients with metastatic castration-resistant prostate cancer that had progressed after docetaxel chemotherapy (CA184-043): a multicentre, randomised, double-blind, phase 3 trial. Lancet Oncol. 2014;15(7):700–712. doi:10.1016/S1470-2045(14)70189-5
8. Beer TM, Kwon ED, Drake CG, et al. Randomized, double-blind, phase III trial of ipilimumab versus placebo in asymptomatic or minimally symptomatic patients with metastatic chemotherapy-naive castration-resistant prostate cancer. J Clin Oncol. 2017;35(1):40–47. doi:10.1200/JCO.2016.69.1584
9. Hansen AR, Massard C, Ott PA, et al. Pembrolizumab for advanced prostate adenocarcinoma: findings of the KEYNOTE-028 study. Ann Oncol. 2018;29(8):1807–1813. doi:10.1093/annonc/mdy232
10. Antonarakis ES, Piulats JM, Gross-Goupil M, et al. Pembrolizumab for treatment-refractory metastatic castration-resistant prostate cancer: multicohort, open-label phase II KEYNOTE-199 study. J Clin Oncol. 2020;38(5):395–405. doi:10.1200/JCO.19.01638
11. Fizazi K, González Mella P, Castellano D, et al. Nivolumab plus docetaxel in patients with chemotherapy-naive metastatic castration-resistant prostate cancer: results from the phase II CheckMate 9KD trial. Eur J Cancer. 2022;160:61–71. doi:10.1016/j.ejca.2021.09.043
12. Isaacsson Velho P, Bastos DA, Saint’ana PT, et al. Nivolumab in patients with metastatic castration-resistant prostate cancer with and without DNA repair defects. Clin Cancer Res. 2024;30(23):5342–5352. doi:10.1158/1078-0432.CCR-24-1595
13. Sharma P, Pachynski RK, Narayan V, et al. Nivolumab plus ipilimumab for metastatic castration-resistant prostate cancer: preliminary analysis of patients in the checkmate 650 trial. Cancer Cell. 2020;38(4):489–499e483. doi:10.1016/j.ccell.2020.08.007
14. Powles T, Yuen KC, Gillessen S, et al. Atezolizumab with enzalutamide versus enzalutamide alone in metastatic castration-resistant prostate cancer: a randomized phase 3 trial. Nat Med. 2022;28(1):144–153. doi:10.1038/s41591-021-01600-6
15. Petrylak DP, Ratta R, Matsubara N, et al. Pembrolizumab plus docetaxel versus docetaxel for previously treated metastatic castration-resistant prostate cancer: the randomized,double-blind,phase III keynote-921 trial. J Clin Oncol. 2025;43(14):1638–1649. doi:10.1200/JCO-24-01283
16. Graff JN, Burotto M, Fong PC, et al. Pembrolizumab plus enzalutamide versus placebo plus enzalutamide for chemotherapy-naive metastatic castration-resistant prostate cancer: the randomized, double-blind, phase III KEYNOTE-641 study. Ann Oncol. 2025;36(8):976–987. doi:10.1016/j.annonc.2025.05.007
17. Fizazi K, Retz M, Petrylak DP, et al. Nivolumab plus rucaparib for metastatic castration-resistant prostate cancer: results from the phase 2 checkmate 9KD trial. J Immunother Cancer. 2022;10(8):e004761. doi:10.1136/jitc-2022-004761
18. Antonarakis ES, Park SH, Goh JC, et al. Pembrolizumab plus olaparib for patients with previously treated and biomarker-unselected metastatic castration-resistant prostate cancer: the randomized, open-label, phase III KEYLYNK-010 trial. J Clin Oncol. 2023;41:3839–3850. doi:10.1200/JCO.23.00233
19. Wattenberg MM, Fahim A, Ahmed MM, Hodge JW. Unlocking the combination: potentiation of radiation-induced antitumor responses with immunotherapy. Radiat Res. 2014;182(2):126–138. doi:10.1667/RR13374.1
20. Klumper N, Grunwald V, Hartmann A, Holzel M, Eckstein M. The role of microsatellite instability/DNA mismatch repair deficiency and tumor mutational burden as biomarkers in predicting response to immunotherapy in castration-resistant prostate cancer. Eur Urol. 2024;86(5):388–390. doi:10.1016/j.eururo.2024.04.026
21. Abida W, Cheng ML, Armenia J, et al. Analysis of the prevalence of microsatellite instability in prostate cancer and response to immune checkpoint blockade. JAMA Oncol. 2019;5(4):471–478. doi:10.1001/jamaoncol.2018.5801
22. van Wilpe S, Kloots ISH, Slootbeek PHJ, et al. Ipilimumab with nivolumab in molecularly selected patients with castration-resistant prostate cancer: primary analysis of the phase II INSPIRE trial. Ann Oncol. 2024;35(12):1126–1137. doi:10.1016/j.annonc.2024.09.004
23. van Wilpe S, Taha T, Rothmann EC, et al. Efficacy of anti-PD-(L)1 immunotherapy in patients with DNA mismatch repair-deficient metastatic castration-resistant prostate cancer. Eur Urol Oncol. 2025. doi:10.1016/j.euo.2025.04.016
24. Choudhury AD, Kwak L, Cheung A, et al. Randomized phase II study evaluating the addition of pembrolizumab to radium-223 in metastatic castration-resistant prostate cancer. Cancer Immunol Res. 2024;12(6):704–718. doi:10.1158/2326-6066.CIR-22-0306
25. Eule CJ, Flaig TW, Wong K, Graf R, Lam ET. Effectiveness and durability of benefit of mTOR inhibitors in a real-world cohort of patients with metastatic prostate cancer and PI3K pathway alterations. Prostate Cancer Prostatic Dise. 2023;26(1):188–193. doi:10.1038/s41391-022-00612-8
26. Siskin M, Economides MP, Wise DR. Cyclin-dependent kinase inhibition in prostate cancer: past, present, and future. Cancers. 2025;17(5):774. doi:10.3390/cancers17050774
27. Feustel K, Martin J, Falchook GS. B7-H3 inhibitors in oncology clinical trials: a review. J Immunother Precis Oncol. 2024;7(1):53–66. doi:10.36401/JIPO-23-18
28. Benzon B, Zhao SG, Haffner MC, et al. Correlation of B7-H3 with androgen receptor, immune pathways and poor outcome in prostate cancer: an expression-based analysis. Prostate Cancer Prostatic Dis. 2017;20(1):28–35. doi:10.1038/pcan.2016.49
29. Shen Q, Zhou K, Lu H, et al. Immune checkpoint B7-H3 is a potential therapeutic target in prostate cancer. Discov Oncol. 2024;15(1):822. doi:10.1007/s12672-024-01674-x
30. Shi W, Wang Y, Zhao Y, et al. Immune checkpoint B7-H3 is a therapeutic vulnerability in prostate cancer harboring PTEN and TP53 deficiencies. Sci Transl Med. 2023;15(695):eadf6724. doi:10.1126/scitranslmed.adf6724
31. Shenderov E, De Marzo AM, Lotan TL, et al. Neoadjuvant enoblituzumab in localized prostate cancer: a single-arm, phase 2 trial. Nat Med. 2023;29(4):888–897. doi:10.1038/s41591-023-02284-w
32. Holstein SA, Lunning MA. CAR T-cell therapy in hematologic malignancies: a voyage in progress. Clin Pharmacol Ther. 2020;107(1):112–122. doi:10.1002/cpt.1674
33. Brudno JN, Kochenderfer JN. Chimeric antigen receptor T-cell therapies for lymphoma. Nat Rev Clin Oncol. 2018;15(1):31–46. doi:10.1038/nrclinonc.2017.128
34. Munshi NC, Sellars MC, Wu CJ, et al. Idecabtagene vicleucel in relapsed and refractory multiple myeloma. N Engl J Med. 2021;384(8):705–716. doi:10.1056/NEJMoa2024850
35. Canelo-Vilaseca M, Sabbah M, Di Blasi R, et al. Lymphodepletion chemotherapy in chimeric antigen receptor-engineered T (CAR-T) cell therapy in lymphoma. Bone Marrow Transplant. 2025;60(5):559–567. doi:10.1038/s41409-025-02539-9
36. Brudno JN, Kochenderfer JN. Current understanding and management of CAR T cell-associated toxicities. Nat Rev Clin Oncol. 2024;21(7):501–521. doi:10.1038/s41571-024-00903-0
37. Combes AD, Palma CA, Calopedos R, et al. PSMA PET-CT in the diagnosis and staging of prostate cancer. Diagnostics. 2022;12. doi:10.3390/diagnostics12112594
38. Sartor O, de Bono J, Chi KN, et al. Lutetium-177-PSMA-617 for Metastatic Castration-Resistant Prostate Cancer. N Engl J Med. 2021;385(12):1091–1103. doi:10.1056/NEJMoa2107322
39. Horoszewicz JS, Kawinski E, Murphy GP. Monoclonal antibodies to a new antigenic marker in epithelial prostatic cells and serum of prostatic cancer patients. Anticancer Res. 1987;7(5B):927–935.
40. Morris MJ, Castellano D, Herrmann K, et al. (177)Lu-PSMA-617 versus a change of androgen receptor pathway inhibitor therapy for taxane-naive patients with progressive metastatic castration-resistant prostate cancer (PSMAfore): a phase 3, randomised, controlled trial. Lancet. 2024;404(10459):1227–1239. doi:10.1016/S0140-6736(24)01653-2
41. Slovin SF, Wang X, Hullings M, et al. Chimeric antigen receptor (CAR +) modified T cells targeting prostate-specific membrane antigen (PSMA) in patients (pts) with castrate metastatic prostate cancer (CMPC). J Clin Oncol. 2013;31(6_suppl):72. doi:10.1200/jco.2013.31.6_suppl.72
42. Junghans RP, Ma Q, Rathore R, et al. Phase I trial of anti-PSMA designer CAR-T cells in prostate cancer: possible role for interacting interleukin 2-T cell pharmacodynamics as a determinant of clinical response. Prostate. 2016;76(14):1257–1270. doi:10.1002/pros.23214
43. Slovin SF, Dorff TB, Falchook GS, et al. Phase 1 study of P-PSMA-101 CAR-T cells in patients with metastatic castration-resistant prostate cancer (mCRPC). J Clin Oncol. 2022;40(6_suppl):98. doi:10.1200/JCO.2022.40.6_suppl.098
44. Narayan V, Barber-Rotenberg JS, Jung I-Y, et al. PSMA-targeting TGFbeta-insensitive armored CAR T cells in metastatic castration-resistant prostate cancer: a phase 1 trial. Nat Med. 2022;28(4):724–734. doi:10.1038/s41591-022-01726-1
45. Kloss CC, Lee J, Zhang A, et al. Dominant-negative TGF-beta receptor enhances PSMA-targeted human CAR T cell proliferation and augments prostate cancer eradication. Mol Ther. 2018;26(7):1855–1866. doi:10.1016/j.ymthe.2018.05.003
46. Reiter RE, Gu Z, Watabe T, et al. Prostate stem cell antigen: a cell surface marker overexpressed in prostate cancer. Proc Natl Acad Sci USA. 1998;95(4):1735–1740. doi:10.1073/pnas.95.4.1735
47. Stein MN, Dumbrava EE, Teply BA, et al. PSCA-targeted BPX-601 CAR T cells with pharmacological activation by rimiducid in metastatic pancreatic and prostate cancer: a phase 1 dose escalation trial. Nat Commun. 2024;15(1):10743. doi:10.1038/s41467-024-53220-6
48. Frieling JS, Tordesillas L, Bustos XE, et al. gammadelta-enriched CAR-T cell therapy for bone metastatic castrate-resistant prostate cancer. Sci Adv. 2023;9(18):eadf0108. doi:10.1126/sciadv.adf0108
49. Dorff TB, Blanchard MS, Adkins LN, et al. PSCA-CAR T cell therapy in metastatic castration-resistant prostate cancer: a phase 1 trial. Nat Med. 2024;30(6):1636–1644. doi:10.1038/s41591-024-02979-8
50. Jin Y, Lorvik KB, Jin Y, et al. Development of STEAP1 targeting chimeric antigen receptor for adoptive cell therapy against cancer. Mol Ther Oncolytics. 2022;26:189–206. doi:10.1016/j.omto.2022.06.007
51. Zanvit P, van Dyk D, Fazenbaker C, et al. Antitumor activity of AZD0754, a dnTGFbetaRII-armored, STEAP2-targeted CAR-T cell therapy, in prostate cancer. J Clin Invest. 2023;133(22). doi:10.1172/JCI169655
52. Shang Z, Niu Y, Cai Q, et al. Human kallikrein 2 (KLK2) promotes prostate cancer cell growth via function as a modulator to promote the ARA70-enhanced androgen receptor transactivation. Tumour Biol. 2014;35(3):1881–1890. doi:10.1007/s13277-013-1253-6
53. Amoozgar B, Bangolo A, Habibi M, Cho C, Goy A. From molecular precision to clinical practice: a comprehensive review of bispecific and trispecific antibodies in hematologic malignancies. Int J Mol Sci. 2025;26(11):5319. doi:10.3390/ijms26115319
54. Hassel JC, Piperno-Neumann S, Rutkowski P, et al. Three-year overall survival with tebentafusp in metastatic uveal melanoma. New England J Med. 2023;389(24):2256–2266. doi:10.1056/NEJMoa2304753
55. Ahn MJ, Cho BC, Felip E, et al. Tarlatamab for patients with previously treated small-cell lung cancer. N Engl J Med. 2023;389(22):2063–2075. doi:10.1056/NEJMoa2307980
56. Palecki J, Bhasin A, Bernstein A, et al. T-Cell redirecting bispecific antibodies: a review of a novel class of immuno-oncology for advanced prostate cancer. Cancer Biol Ther. 2024;25(1):2356820. doi:10.1080/15384047.2024.2356820
57. Hummel HD, Kufer P, Grüllich C, et al. Pasotuxizumab, a Bite ® immune therapy for castration-resistant prostate cancer: phase I, dose-escalation study findings. Immunotherapy. 2021;13(2):125–141. doi:10.2217/imt-2020-0256
58. Dorff T, Horvath LG, Autio K, et al. A phase I study of acapatamab, a half-life extended, PSMA-targeting bispecific T-cell engager for metastatic castration-resistant prostate cancer. Clin Cancer Res. 2024;30(8):1488–1500. doi:10.1158/1078-0432.CCR-23-2978
59. Lim EA, Schweizer MT, Chi KN, et al. Phase 1 study of safety and preliminary clinical activity of JNJ-63898081, a PSMA and CD3 bispecific antibody, for metastatic castration-resistant prostate cancer. Clin Genitourin Cancer. 2023;21(3):366–375. doi:10.1016/j.clgc.2023.02.010
60. Stein MN, Zhang J, Kelly WK, et al. Preliminary results from a phase 1/2 study of co-stimulatory bispecific PSMAxCD28 antibody REGN5678 in patients (pts) with metastatic castration-resistant prostate cancer (mCRPC). J Clin Oncol. 2023;41(6_suppl):154. doi:10.1200/JCO.2023.41.6_suppl.154
61. Heitmann JS, Walz JS, Pflügler M, et al. Abstract CT141: CC-1, a bispecific PSMAxCD3 antibody for treatment of prostate carcinoma: results of the ongoing phase I dose escalation trial. Cancer Res. 2022;82(12_Supplement):CT141. doi:10.1158/1538-7445.Am2022-ct141
62. Lampe H, Tam L, Hansen AR. Bi-specific T-cell engagers (BiTEs) in prostate cancer and strategies to enhance development: hope for a BiTE-r future. Front Pharmacol. 2024;15:1399802. doi:10.3389/fphar.2024.1399802
63. Stein MN, Vinceneux A, Robbrecht D, et al. Pasritamig, a first-in-class, bispecific T-cell engager targeting human kallikrein 2, in metastatic castration-resistant prostate cancer: a phase I study. J Clin Oncol.
64. Stein MN, Vinceneux A, Robbrecht D, et al. Pasritamig, a first-in-class, bispecific t-cell engager targeting human kallikrein 2, in metastatic castration-resistant prostate cancer: a phase I study. J Clin Oncol. 2025;43(22):2515–2526. doi:10.1200/jco-25-00678
65. Nolan-Stevaux O, Li C, Liang L, et al. AMG 509 (Xaluritamig), an anti-STEAP1 XmAb 2+1 T-cell redirecting immune therapy with avidity-dependent activity against prostate cancer. Cancer Discov. 2024;14(1):90–103. doi:10.1158/2159-8290.CD-23-0984
66. Kelly W, Danila D, Lin -C-C, et al. 1765O Interim results from a phase I study of AMG 509 (xaluritamig), a STEAP1 x CD3 XmAb 2+1 immune therapy, in patients with metastatic castration-resistant prostate cancer (mCRPC). Ann Oncol. 2023;34:S953–S954. doi:10.1016/j.annonc.2023.09.2715
67. Kelly WK, Morris MJ, Horvath L, et al. Trial in progress (XALute): phase 3 study of xaluritamig vs investigator’s choice of cabazitaxel or second androgen receptor directed therapy (ARDT) in post-taxane metastatic castration-resistant prostate cancer (mCRPC). J Clin Oncol. 2025;43(16_suppl):TPS5118–TPS5118. doi:10.1200/JCO.2025.43.16_suppl.TPS5118
68. Zhao SG, Lehrer J, Chang SL, et al. The immune landscape of prostate cancer and nomination of PD-L2 as a potential therapeutic target. J Natl Cancer Inst. 2019;111(3):301–310. doi:10.1093/jnci/djy141
69. Chandran E, Meininger L, Karzai F, Madan RA. Signaling new therapeutic opportunities: cytokines in prostate cancer. Expert Opin Biol Ther. 2022;22(10):1233–1243. doi:10.1080/14712598.2022.2108701
70. Maas RA, Dullens HF, Den Otter W. Interleukin-2 in cancer treatment: disappointing or (still) promising? A review. Cancer Immunol Immunother. 1993;36(3):141–148. doi:10.1007/BF01741084
71. Jiang T, Zhou C, Ren S. Role of IL-2 in cancer immunotherapy. Oncoimmunology. 2016;5(6):e1163462. doi:10.1080/2162402X.2016.1163462
72. Chamie K, Chang SS, Rosser CJ, et al. N-803 plus BCG treatment for BCG-naive or -unresponsive non-muscle invasive bladder cancer: a plain language review. Future Oncol. 2024;20(31):2307–2317. doi:10.1080/14796694.2024.2363744
73. Liu J, Cao S, Kim S, et al. Interleukin-12: an update on its immunological activities, signaling and regulation of gene expression. Curr Immunol Rev. 2005;1(2):119–137. doi:10.2174/1573395054065115
74. Minnar CM, Lui G, Gulley JL, Schlom J, Gameiro SR. Preclinical and clinical studies of a tumor targeting IL-12 immunocytokine. Front Oncol. 2023;13:1321318. doi:10.3389/fonc.2023.1321318
75. Meininger L, Madan RA, Toney N, et al. The immunocytokine M9241 in the treatment of prostate cancer (PCa): clinical and immune data from a phase 1 study. J Clin Oncol. 2022;40(6_suppl):127. doi:10.1200/JCO.2022.40.6_suppl.127
76. Lopez-Bujanda ZA, Haffne r MC, Chaimowitz MG, et al. Castration-mediated IL-8 promotes myeloid infiltration and prostate cancer progression. Nat Cancer. 2021;2(8):803–818. doi:10.1038/s43018-021-00227-3
77. Dallos M, Pan SM, Chaimowitz M, et al. A randomized phase Ib/II study of intermittent androgen deprivation therapy plus nivolumab with or without interleukin-8 blockade in men with hormone-sensitive prostate cancer (MAGIC-8). J Clin Oncol. 2022;40(16_suppl):5082. doi:10.1200/JCO.2022.40.16_suppl.5082
78. Bilusic M, Heery CR, Collins JM, et al. Phase I trial of HuMax-IL8 (BMS-986253), an anti-IL-8 monoclonal antibody, in patients with metastatic or unresectable solid tumors. J Immunother Cancer. 2019;7(1):240. doi:10.1186/s40425-019-0706-x
79. Highfill SL, Cui Y, Giles AJ, et al. Disruption of CXCR2-mediated MDSC tumor trafficking enhances anti-PD1 efficacy. Sci Transl Med. 2014;6(237):237ra267. doi:10.1126/scitranslmed.3007974
80. Guo C, Sharp A, Gurel B, et al. Targeting myeloid chemotaxis to reverse prostate cancer therapy resistance. Nature. 2023;623(7989):1053–1061. doi:10.1038/s41586-023-06696-z
81. Boixareu C, Taha T, Venkadakrishnan VB, de Bono J, Beltran H. Targeting the tumour cell surface in advanced prostate cancer. Nat Rev Urol. 2025;22(9):569–589. doi:10.1038/s41585-025-01014-w
82. Madan RA, Karzai F, Donahue RN, et al. Clinical and immunologic impact of short-course enzalutamide alone and with immunotherapy in non-metastatic castration sensitive prostate cancer. J Immunother Cancer. 2021;9(3):e001556. doi:10.1136/jitc-2020-001556
83. Madan RA, Donahue R, Tsai Y-T, et al. 1412P Immune changes after enzalutamide (Enza) is added to androgen-deprivation therapy (ADT) in first-line metastatic castration-resistant prostate cancer (mCRPC). Ann Oncol. 2022;33:S1191. doi:10.1016/j.annonc.2022.07.1898
84. Chandran EBA, Atiq MO, Donahue RN, et al. Evaluating the optimal sequence of immunotherapy and docetaxel in men with metastatic castration-sensitive prostate cancer. J Clin Oncol. 2022;40(6_suppl):130. doi:10.1200/JCO.2022.40.6_suppl.130
85. Bilusic M, Einstein DJ, Karzai FH, et al. The potential role for immunotherapy in biochemically recurrent prostate cancer. Urol Clin North Am. 2020;47(4):457–467. doi:10.1016/j.ucl.2020.07.004
86. Einstein DJ, Aragon-Ching JB, Karzai F, Madan RA. Biochemically recurrent prostate cancer in the era of EMBARK and PSMA PET imaging: everything has changed, except the patients. Curr Opin Oncol. 2024;36(3):164–168. doi:10.1097/CCO.0000000000001030
87. Madan RA, Heery CR, Gulley JL. Poxviral-based vaccine elicits immunologic responses in prostate cancer patients. Oncoimmunology. 2014;3:e28611. doi:10.4161/onci.28611
88. Gulley JL, Borre M, Vogelzang NJ, et al. Phase III trial of PROSTVAC in asymptomatic or minimally symptomatic metastatic castration-resistant prostate cancer. J Clin Oncol. 2019;37(13):1051–1061. doi:10.1200/JCO.18.02031
89. Madan RA, Karzai F, Bilusic M, et al. Immunotherapy for biochemically recurrent prostate cancer. J Clin Oncol. 2018;36(6_suppl):215. doi:10.1200/JCO.2018.36.6_suppl.215
90. Madan RA, Mena Gonzalez E, Chandran EBA, et al. 1614P PSA responses and PSMA scan changes after immunotherapy for biochemically recurrent prostate cancer (BCR) without androgen deprivation therapy (ADT). Ann Oncol. 2024;35:S974–S975. doi:10.1016/j.annonc.2024.08.1695
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Immunotherapy for Urothelial Carcinoma: Focus on Clinical Utility of Nivolumab
Chiang RS, Glover MJ, Khaki AR, Srinivas S
OncoTargets and Therapy 2022, 15:1259-1269
Published Date: 20 October 2022
The Extended Surgical Concepts for Hepatocellular Carcinoma in the Era of Immune Checkpoint Inhibitors
Hsu HM, Tsai HI, Lee WC, Wang CC, Yu MC, Lin SM, Lin CY, Wu CH, Lee CW
Journal of Hepatocellular Carcinoma 2023, 10:1873-1880
Published Date: 24 October 2023
Lethal Immune Myocarditis and Myasthenia Gravis Due to Anti-PD-1 Treatment for a Bladder Cancer Patient: A Case Report and Possible Treatment Inspiration
Gao P, Li X, He Z, Zhang H, Zhang Z, Liu Z
International Medical Case Reports Journal 2024, 17:359-365
Published Date: 18 April 2024
Recent Advances in Immunotherapy for Breast Cancer: A Review
Wen QE, Li L, Feng RQ, Li DH, Qiao C, Xu XS, Zhang YJ
Breast Cancer: Targets and Therapy 2024, 16:497-516
Published Date: 27 August 2024
Clinical Significance and Molecular Annotation for PD-L1 Negative Advanced Non-Small Cell Lung Cancer with Sensitivity to Responsive to Dual PD-1/CTLA-4 Blockade
Wang L, Liu L, Zhao J, Yu X, Su C
ImmunoTargets and Therapy 2024, 13:435-445
Published Date: 6 September 2024