Back to Journals » Cancer Management and Research » Volume 18

Prognostic Factors in Upper Gastrointestinal Neuroendocrine Carcinoma: A Retrospective Cohort Study of Clinicopathological Features and Survival Outcomes
Received 21 April 2026
Accepted for publication 10 July 2026
Published 17 July 2026 Volume 2026:18 618644
DOI https://doi.org/10.2147/CMAR.S618644
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Lu-Zhe Sun
Erdoğan Şeyran, Azer Gökmen
Department of Medical Oncology, Van Training and Research Hospital, Van, Turkey
Correspondence: Erdoğan Şeyran, Department of Medical Oncology, Van Training and Research Hospital, Van, Turkey, Email [email protected]
Background: Upper gastrointestinal neuroendocrine carcinoma (NEC) is a rare and highly aggressive malignancy with limited prognostic data. This study aimed to evaluate clinicopathological characteristics and to identify clinically relevant prognostic factors, with a particular focus on simple and readily available inflammatory and nutritional biomarkers that may support routine risk stratification.
Methods: In this retrospective cohort study, 54 patients with histologically confirmed esophageal or gastric NEC were analyzed. Clinical, pathological, laboratory, treatment, and survival data were collected. Overall survival (OS) was assessed using Kaplan–Meier analysis. Prognostic factors were evaluated using univariate and multivariate Cox proportional hazards models.
Results: The median OS was 17.9 months. On univariate analysis, metastatic disease, elevated LDH, elevated neutrophil-to-lymphocyte ratio (NLR), hypoalbuminemia, surgical resection, and adjuvant chemotherapy were significantly associated with OS. In multivariate analysis, hypoalbuminemia remained the only independent predictor of worse survival (HR 2.876, 95% CI 1.116– 7.414; p = 0.029).
Conclusion: Hypoalbuminemia emerged as a potential independent prognostic factor in this cohort and may serve as a simple and readily available marker of poor outcome. Albumin, LDH, and NLR may provide additional prognostic information in patients with upper gastrointestinal neuroendocrine carcinoma. However, these findings should be considered exploratory and require validation in larger prospective multicenter studies.
Keywords: albumin, inflammation, lactate dehydrogenase, neutrophil-to-lymphocyte ratio, nutritional status, overall survival, prognosis, upper gastrointestinal neuroendocrine carcinoma
Introduction
Neuroendocrine carcinomas (NECs) of the upper gastrointestinal tract are rare and highly aggressive malignancies characterized by poor differentiation, high proliferative activity, and unfavorable clinical outcomes.1–3 According to the World Health Organization (WHO) classification, NECs are defined by a Ki-67 index exceeding 20% and poorly differentiated morphology, reflecting their distinct biological behavior compared with well-differentiated neuroendocrine tumors.4 Although the overall incidence of neuroendocrine neoplasms has increased in recent decades, NECs of the esophagus and stomach remain uncommon but clinically significant due to their aggressive course and early metastatic potential.5–7
Upper gastrointestinal NECs pose substantial clinical challenges. Esophageal NEC accounts for approximately 1% of all esophageal malignancies but is associated with significantly worse survival compared with more common histological subtypes.8 Gastric NEC, although relatively more frequent within the gastrointestinal tract, is typically diagnosed at advanced stages and carries a similarly poor prognosis.9 Across published series, the median overall survival (OS) for patients with upper gastrointestinal NEC ranges between 11 and 20 months, underscoring the urgent need for improved prognostic stratification and optimized therapeutic strategies.10–12
Several clinicopathological factors, including disease stage, tumor burden, and treatment modality, have been associated with outcomes in NEC.13,14 However, these conventional parameters may not fully capture the complex interplay between tumor biology and host-related factors. In recent years, increasing attention has been directed toward systemic inflammatory and nutritional biomarkers as potential prognostic indicators in oncology.15,16 Among these, the neutrophil-to-lymphocyte ratio (NLR) has emerged as a readily accessible marker of systemic inflammation and has been associated with survival across a wide range of malignancies.17,18 Similarly, elevated lactate dehydrogenase (LDH), a surrogate of tumor burden and tumor hypoxia, has been linked to adverse outcomes in aggressive cancers, including neuroendocrine neoplasms.19
Serum albumin, a marker reflecting both nutritional status and systemic inflammatory response, has gained increasing recognition as a prognostic factor in gastrointestinal malignancies.20,21 Hypoalbuminemia reflects not only malnutrition but also cancer-related inflammation, which may contribute to tumor progression and impaired treatment tolerance.22,23 Despite accumulating evidence supporting the prognostic value of these biomarkers in various malignancies, data specifically focusing on upper gastrointestinal NEC remain limited. Most previous studies have evaluated heterogeneous populations of gastroenteropancreatic neuroendocrine neoplasms or focused on single primary sites, thereby limiting the generalizability of their findings to upper gastrointestinal NEC as a distinct clinical entity.
In this context, the present study aimed to evaluate clinicopathological characteristics, treatment patterns, and survival outcomes in patients with upper gastrointestinal NEC, including both esophageal and gastric primary tumors. We also sought to investigate the prognostic significance of readily available inflammatory and nutritional biomarkers—particularly NLR, LDH, and serum albumin—and to identify independent predictors of overall survival. By focusing on a relatively homogeneous cohort of upper gastrointestinal NEC, this study aims to clarify the clinical utility of simple biomarkers for routine prognostic stratification in this rare and aggressive malignancy.
Materials and Methods
Study Design and Patient Population
This retrospective cohort study included consecutive patients diagnosed with histologically confirmed neuroendocrine carcinoma (NEC) of the upper gastrointestinal tract (esophagus or stomach) between January 2012 and December 2024 at Van Training and Research Hospital, a tertiary referral center in Turkey.
The diagnosis of NEC was established according to the World Health Organization (WHO) classification criteria, requiring poorly differentiated morphology and a Ki-67 proliferation index >20%.
Eligible patients were required to meet the following inclusion criteria: (1) age ≥18 years, (2) histopathologically confirmed NEC originating from the esophagus or stomach, and (3) availability of adequate clinical and follow-up data for survival analysis. Patients with insufficient baseline clinical or pathological data were excluded.
A total of 54 consecutive patients with histologically confirmed upper gastrointestinal neuroendocrine carcinoma who met the study eligibility criteria during the study period were included in the final analysis. No eligible patients were excluded because of missing follow-up information. All available clinical, pathological, treatment, and laboratory data were retrieved retrospectively from institutional medical records.
As this was a retrospective study based on existing institutional medical records collected between January 2012 and December 2024, no prospective patient recruitment or additional data collection was performed after ethics approval. Before submission to the Ethics Committee, the study protocol, including the study objectives, eligibility criteria, variables to be collected, and the statistical analysis plan, had been prepared. Following ethics committee approval, anonymized data were extracted from the institutional database, analyzed according to the predefined study protocol, and the manuscript was prepared for submission.
Data Collection
Clinical, demographic, and pathological data were obtained from electronic medical records. Variables included age, sex, smoking history, comorbidities, presenting symptoms, primary tumor location (esophagus vs stomach), histological subtype, tumor stage (TNM), Ki-67 index, and PET SUVmax. Baseline laboratory parameters at diagnosis included complete blood count, neutrophil-to-lymphocyte ratio (NLR), serum albumin, lactate dehydrogenase (LDH), and tumor markers (CEA, CA19-9, CA15-3). CRP and fibrinogen were not included because these parameters were not routinely and consistently available in the institutional records during the study period. Treatment-related variables included neoadjuvant therapy, surgical resection, adjuvant treatment, and systemic chemotherapy regimens. Treatment decisions were made according to disease stage, patient performance status, multidisciplinary clinical evaluation, and the prevailing treatment standards during the study period.
Survival status and follow-up information were obtained through review of the hospital information system and institutional medical records. Overall survival (OS) was defined as the time from the date of diagnosis to the date of death from any cause or the last documented follow-up visit. Patients who were alive at the time of data collection were censored at their last recorded follow-up. The median follow-up duration for the entire cohort was 12.2 months, while the median follow-up among surviving patients was 13.9 months.
Definition of Variables
The neutrophil-to-lymphocyte ratio (NLR) was calculated as the ratio of absolute neutrophil count to absolute lymphocyte count. Hypoalbuminemia was defined as a serum albumin level <35 g/L. Elevated LDH was defined as >250 U/L. Elevated NLR was defined as >3.03, corresponding to the median value of the study cohort. This threshold is consistent with previously reported NLR cut-off values used in oncology studies, where median cut-off values around 3.0 have commonly been reported.24,25
Statistical Analysis
Statistical analyses were performed using IBM SPSS Statistics for Windows, Version 26.0 (IBM Corp., Armonk, NY, USA). Continuous variables were assessed for normality using the Kolmogorov–Smirnov test and presented as mean ± standard deviation (SD) or median (range), as appropriate. Categorical variables were expressed as frequencies and percentages. Overall survival (OS) was estimated using the Kaplan–Meier method and compared using the Log rank test. Univariate Cox proportional hazards regression analysis was performed to identify potential prognostic factors. Variables with p < 0.10 in univariate analysis were entered into the multivariate Cox regression model using a backward stepwise selection method. Hazard ratios (HRs) and 95% confidence intervals (CIs) were reported. A two-sided p-value < 0.05 was considered statistically significant. The proportional hazards assumption was assessed by reviewing survival patterns and model diagnostics during Cox model construction. Given the limited sample size, number of events, and sparse data, the multivariable estimates were interpreted cautiously.
Missing data were handled using a complete-case approach. Variables with unavailable laboratory or imaging data were analyzed using the available cases only. Baseline serum albumin levels were available for 49 patients (90.7%), LDH levels for 46 patients (85.2%), Ki-67 index for 38 patients (70.4%), and PET SUVmax values for 28 patients (51.9%). No imputation method was applied because of the retrospective design and the limited sample size. The number of available observations for each variable is reported in the corresponding tables.
Additional Survival Analyses
Additional survival analyses were conducted according to metastatic status, primary tumor location, and serum albumin level.
Ethical Considerations
The study was approved by the Non-Interventional Clinical Research Ethics Committee of Van Training and Research Hospital, Van, Turkey (Approval No: GOKAEK/2026-04/29; Approval Date: April 10, 2026). The requirement for informed consent was waived by the Ethics Committee due to the retrospective and non-interventional nature of the study, which involved review of existing medical records without direct patient contact or intervention. All patient data were anonymized prior to analysis, and confidentiality was strictly maintained throughout the study. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki.
Results
Patient and Tumor Characteristics
A total of 54 patients with upper gastrointestinal neuroendocrine carcinoma (NEC), including esophageal and gastric primary tumors, were included in the analysis. The mean age was 62.9 ± 10.4 years, and 59.3% of patients were male. The primary tumor was located in the stomach in 59.3% of patients and in the esophagus in 40.7%. At diagnosis, 59.3% of patients had distant metastases. Most tumors were poorly differentiated NEC with a high proliferative index (mean Ki-67: 86.6 ± 9.5%). Baseline laboratory evaluation showed that 38.8% of patients had hypoalbuminemia (<35 g/L), 50.9% had elevated NLR (>3.03), and 50.0% had elevated LDH (>250 U/L). Detailed baseline characteristics are presented in Table 1.
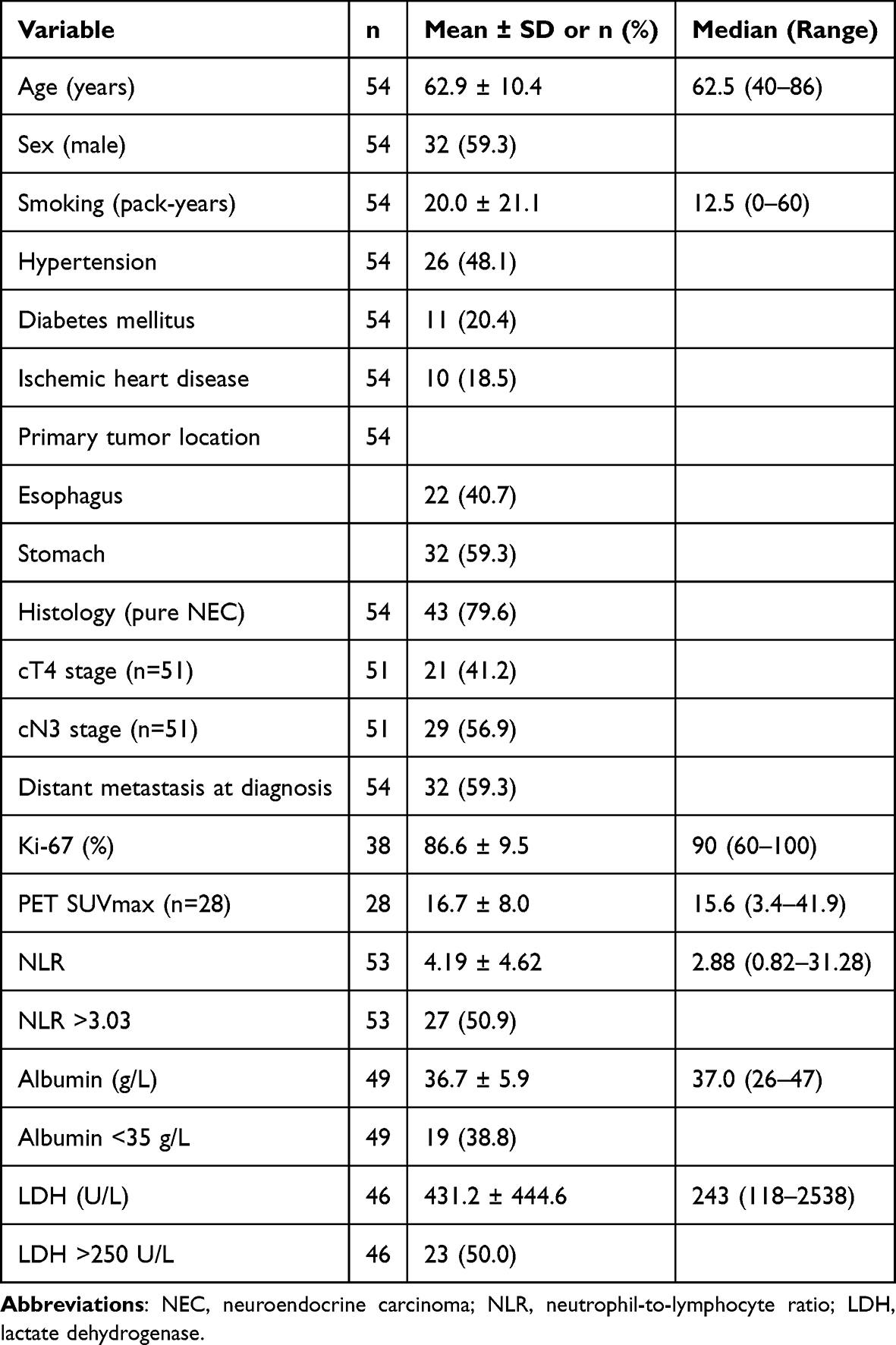 |
Table 1 Patient and Tumor Characteristics in Upper Gastrointestinal NEC |
Treatment Characteristics
Treatment strategies varied according to disease stage. Surgical resection was performed in 31.5% of patients, with an R0 resection rate of 86.7% among operated cases. Neoadjuvant therapy was administered in 14.8% of patients, while adjuvant chemotherapy and radiotherapy were given to 25.9% and 20.4% of patients, respectively. Platinum-based chemotherapy (cisplatin plus etoposide) was the most commonly used first-line regimen (61.2%), with an objective response rate of 51.1%. Second-line therapy was administered in 44.4% of patients. Detailed treatment characteristics are summarized in Table 2.
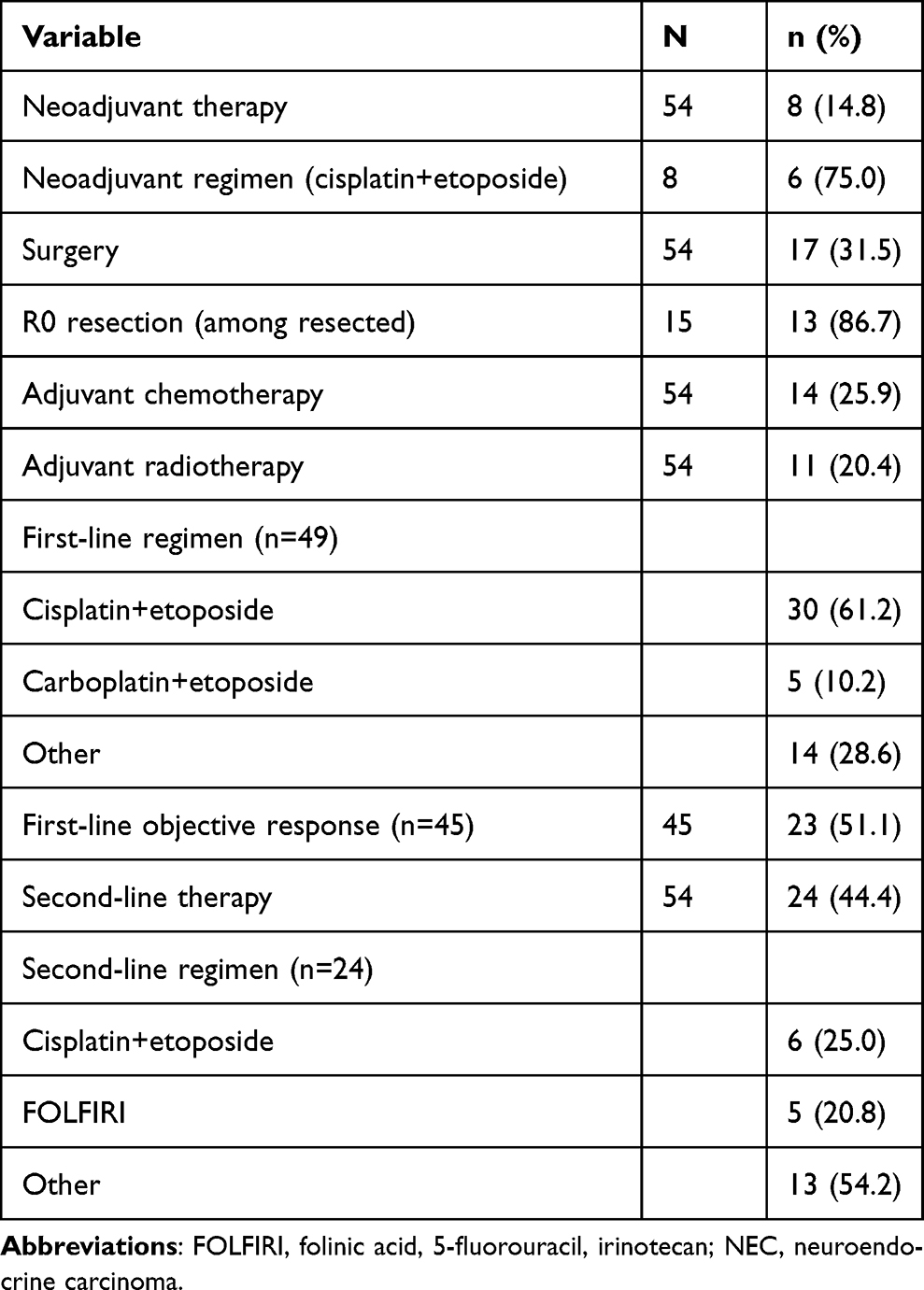 |
Table 2 Treatment Characteristics in Upper Gastrointestinal NEC |
Survival Outcomes
At the time of analysis, 72.2% of patients had died. The median overall survival (OS) for the entire cohort was 17.9 months. Kaplan–Meier survival analysis demonstrated that patients with metastatic disease had significantly shorter OS compared to those without metastasis (median OS: 12.1 vs 21.9 months; log-rank p < 0.001) (Figure 1). No statistically significant difference in OS was observed according to primary tumor location (median OS: 20.8 vs 14.3 months; log-rank p = 0.643).
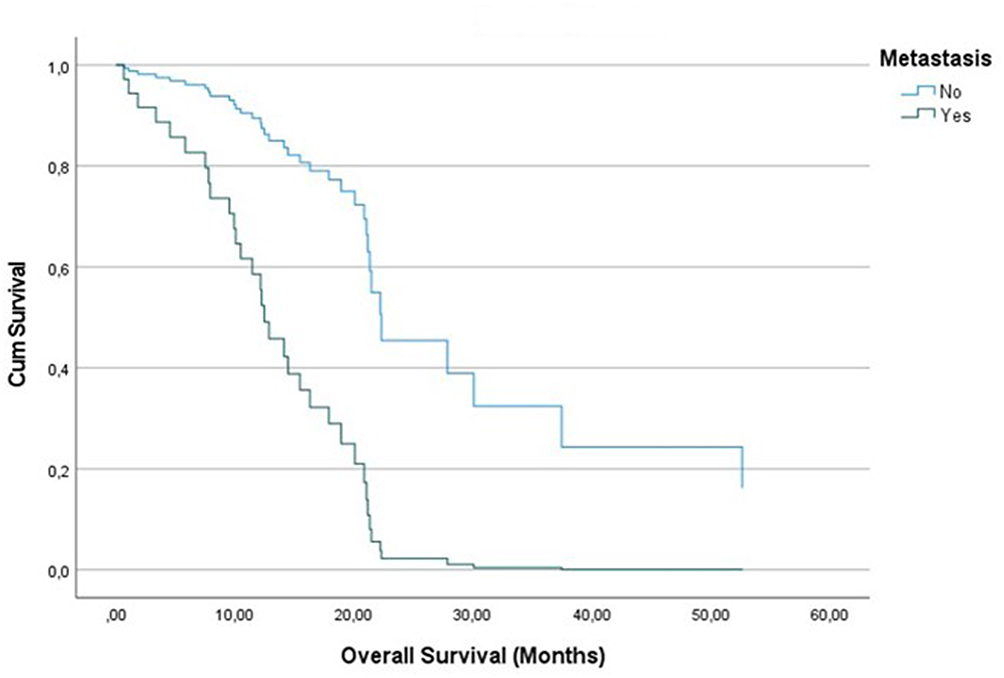 |
Figure 1 Kaplan–Meier survival curves according to metastatic status. Patients with metastatic disease had significantly shorter overall survival compared to those without metastasis (median OS: 12.1 vs 21.9 months; log-rank p < 0.001). |
Subgroup Analyses
Patients with hypoalbuminemia (serum albumin <35 g/L) had significantly worse overall survival compared with patients with normal albumin levels (median OS: 10.5 vs 21.1 months, respectively; log-rank p = 0.001) (Figure 2).
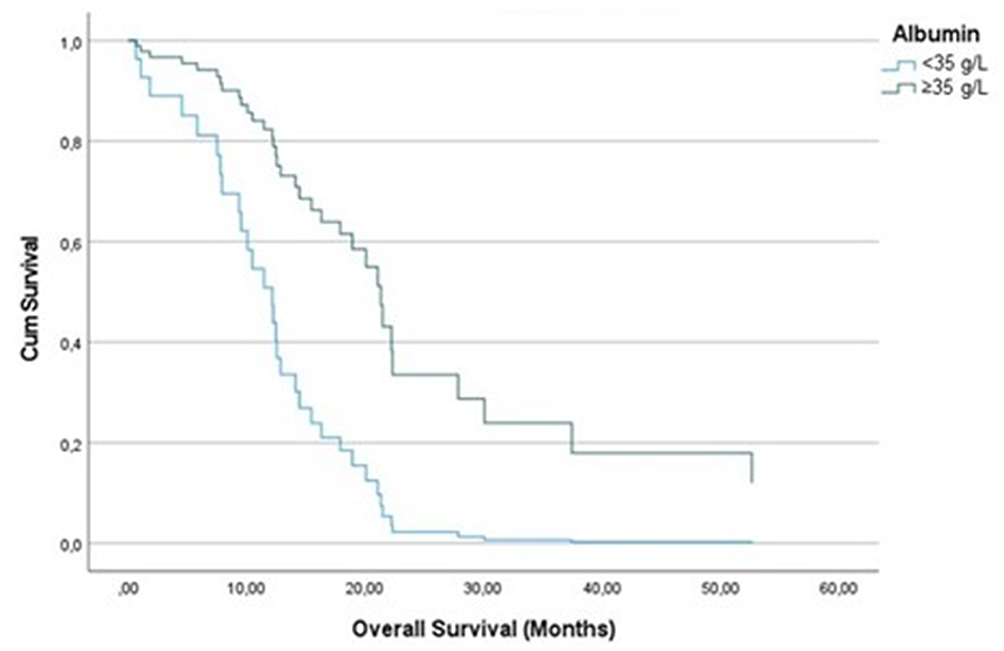 |
Figure 2 Kaplan–Meier curves for overall survival according to serum albumin level. Patients with hypoalbuminemia (<35 g/L) had significantly worse OS compared to those with normal albumin levels (median OS: 10.5 vs 21.1 months; log-rank p = 0.001). |
Univariate Cox Regression Analysis
Univariate Cox regression analysis identified several factors significantly associated with overall survival, including the presence of metastasis (HR = 4.816; p < 0.001), elevated LDH (HR = 3.867; p = 0.001), elevated NLR (HR = 3.278; p = 0.001), and hypoalbuminemia (HR = 3.484; p = 0.001). In addition, surgical resection (HR = 0.301; p = 0.002) and adjuvant chemotherapy (HR = 0.476; p = 0.044) were associated with improved survival. Detailed results are presented in Table 3.
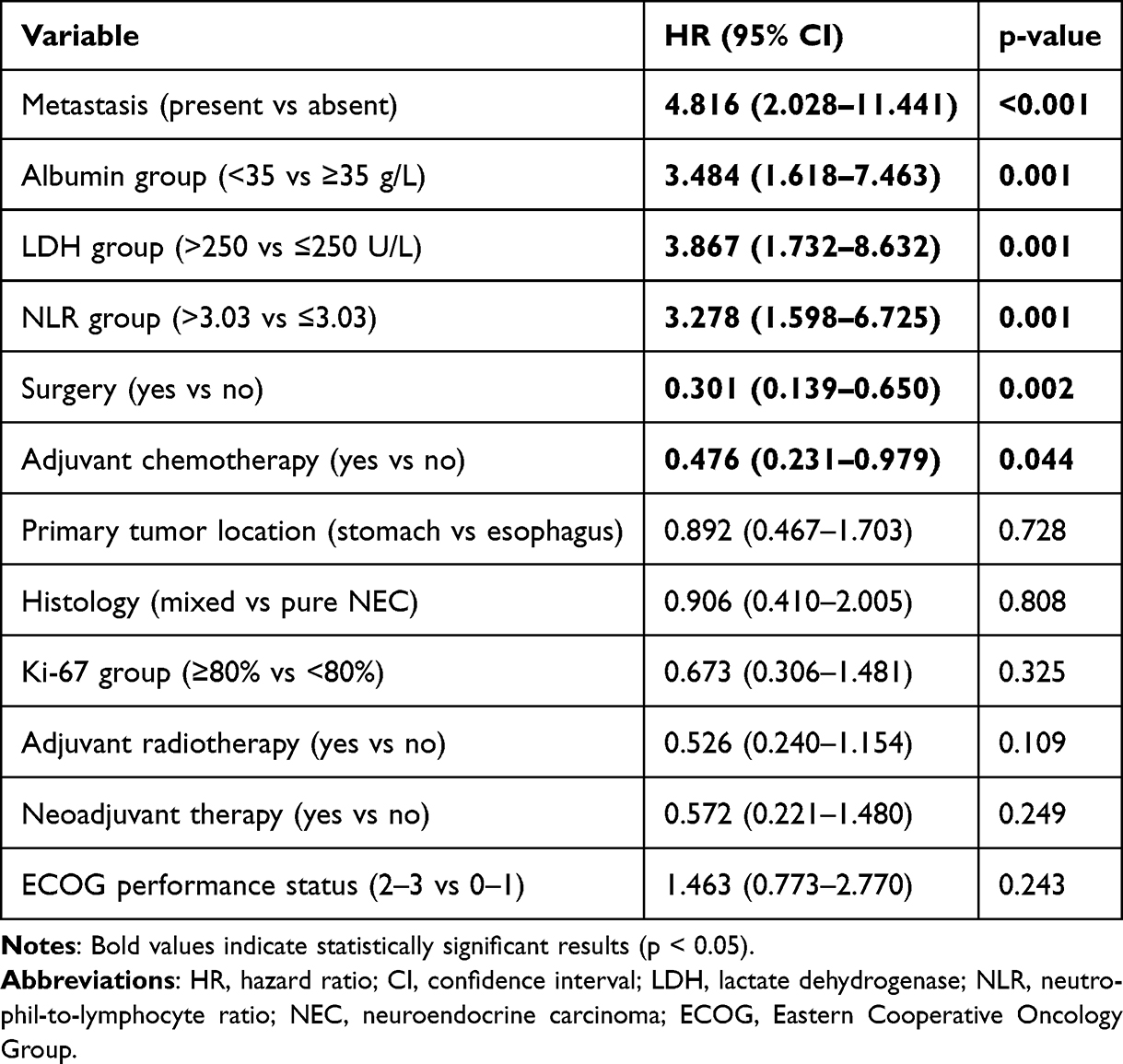 |
Table 3 Univariate Cox Regression Analysis for Overall Survival in Upper Gastrointestinal NEC |
Multivariate Cox Regression Analysis
Variables significant in univariate analysis were included in the multivariate Cox regression model. After adjustment, only hypoalbuminemia remained an independent predictor of worse overall survival (HR = 2.876; 95% CI: 1.116–7.414; p = 0.029). The attenuation of the hazard ratio for albumin in the multivariable model may reflect interactions and potential collinearity among clinical and laboratory variables included in the analysis. Despite this limitation, serum albumin remained the only variable independently associated with overall survival after multivariable adjustment. Detailed results are shown in Table 4.
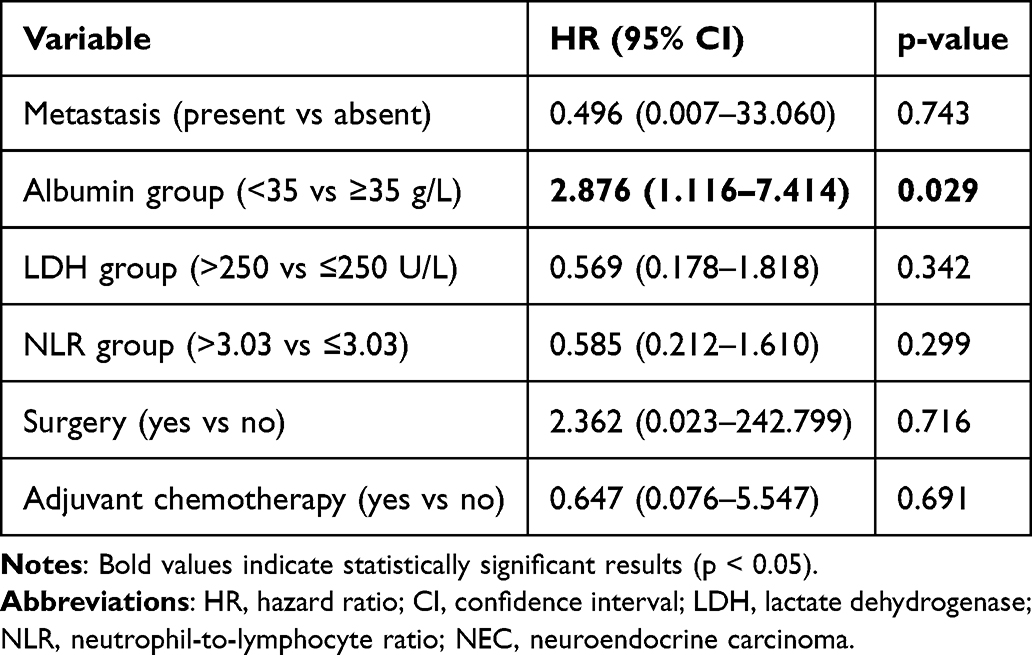 |
Table 4 Multivariate Cox Proportional Hazards Regression Analysis for Overall Survival in Upper Gastrointestinal NEC |
Discussion
In this retrospective cohort study of patients with upper gastrointestinal neuroendocrine carcinoma (NEC), we identified serum albumin as a potential independent prognostic factor for overall survival. While several clinical and laboratory variables—including metastatic disease, LDH, NLR, surgical resection, and adjuvant chemotherapy—were significantly associated with survival in univariate analyses, only hypoalbuminemia retained independent significance in multivariate modeling. These findings suggest that simple and widely available biomarkers may help refine routine prognostic stratification in this rare and aggressive malignancy.
Serum albumin is a well-established biomarker reflecting both nutritional status and systemic inflammatory response. In our cohort, hypoalbuminemia was associated with significantly worse overall survival and remained independently predictive after adjustment for multiple clinical factors. These findings are consistent with prior studies demonstrating the prognostic value of albumin across gastrointestinal malignancies.20–22 The underlying mechanisms are likely multifactorial. Cancer-related systemic inflammation, mediated by cytokines such as interleukin-6, suppresses hepatic albumin synthesis, while malnutrition may impair immune competence and reduce tolerance to systemic therapies.23 Malnutrition and inflammation are closely interconnected processes, with nutritional deterioration potentially amplifying systemic inflammatory responses and contributing to cancer progression. In upper gastrointestinal NEC, where patients frequently present with dysphagia, weight loss, and advanced disease, these mechanisms are particularly relevant. Importantly, hypoalbuminemia may reflect a combination of tumor-related and host-related factors, including systemic inflammation, nutritional decline, disease burden, and overall physiological reserve. Therefore, although albumin remained independently associated with survival in our study, its prognostic significance should be interpreted within this broader clinical context.
Systemic inflammatory biomarkers have increasingly been recognized as important determinants of cancer outcomes.15,16 In the present study, both NLR and LDH were significantly associated with survival in univariate analysis, consistent with previous reports in neuroendocrine and other solid tumors.17–19,24,25 Although these markers did not retain independent significance in multivariate analysis, their associations in univariate models support their potential role as indicators of systemic inflammation and tumor burden. Elevated LDH may reflect increased tumor metabolic activity and hypoxia, while an elevated NLR indicates a shift toward a pro-tumor inflammatory state. However, given the relatively small sample size and potential collinearity between inflammatory and nutritional variables, these findings should be interpreted with caution.
Interestingly, metastatic disease, which was strongly associated with survival in univariate analysis, did not retain significance in multivariate modeling. This finding may reflect the complex interaction between tumor burden and host-related factors such as systemic inflammation and nutritional status. In addition, the wide confidence intervals observed in the multivariate model suggest limited statistical precision, likely related to the relatively small sample size and number of events. Similarly, the apparent attenuation of the hazard ratio for albumin after multivariable adjustment may be explained by interactions and collinearity among covariates included in the model. Furthermore, residual confounding cannot be excluded, as factors potentially influencing albumin levels, such as comorbid conditions, liver involvement, chronic inflammatory states, and overall functional status, may not have been fully captured in the available retrospective data. These observations highlight the challenges of multivariable modeling in rare cancers with limited sample sizes.
Consistent with previous literature, the median overall survival observed in our cohort (17.9 months) falls within the range reported in prior studies of upper gastrointestinal and extrapulmonary NEC.10–12 Notably, no significant survival difference was observed between esophageal and gastric NEC, suggesting that these tumors may share similar biological behavior despite differences in anatomical origin. This finding supports the rationale for evaluating upper gastrointestinal NEC as a unified clinical entity. In addition, surgical resection and adjuvant chemotherapy were associated with improved survival in univariate analyses, highlighting the potential benefit of multimodal treatment in selected patients; however, these findings should be interpreted cautiously due to possible selection bias.
Our study adds to the existing literature by focusing specifically on upper gastrointestinal NEC and by integrating both inflammatory and nutritional biomarkers into prognostic assessment. Most previous studies have evaluated heterogeneous populations of gastroenteropancreatic neuroendocrine neoplasms, limiting the applicability of their findings to this distinct subgroup.11,12 To our knowledge, few studies have evaluated albumin, NLR, and LDH together in a relatively homogeneous cohort of upper gastrointestinal NEC.
From a clinical perspective, our findings suggest that serum albumin, a simple and widely available biomarker, may contribute to routine risk stratification in patients with upper gastrointestinal NEC. Early identification of patients with hypoalbuminemia may facilitate closer monitoring, timely supportive interventions, and nutritional optimization. However, given the retrospective design and potential residual confounding, albumin should not be interpreted as a standalone prognostic marker, and prospective validation is warranted. Given the rarity of this disease and the limited availability of specialized prognostic tools, such simple biomarkers may be particularly valuable in daily clinical practice.
This study has several limitations. First, its retrospective single-center design introduces the potential for selection bias. Second, the relatively small sample size limits statistical power, particularly in multivariate and subgroup analyses. Third, missing data for certain variables may have influenced the robustness of the findings. Fourth, the findings should be interpreted in the context of model instability reflected by the wide confidence intervals observed for some covariates in multivariable analysis. These limitations should be considered when interpreting the results.
In conclusion, hypoalbuminemia emerged as the only independent prognostic factor identified in the present cohort and may represent a useful prognostic marker for overall survival in patients with upper gastrointestinal neuroendocrine carcinoma. In addition, inflammatory biomarkers such as LDH and NLR were associated with survival in univariate analyses. These findings support the integration of simple host-related markers, particularly nutritional and inflammatory parameters, into routine prognostic assessment in this rare and aggressive malignancy. Further prospective, multicenter studies are needed to validate these findings.
Funding
The authors received no specific funding for this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Dasari A, Shen C, Halperin D, et al. Trends in the incidence, prevalence, and survival outcomes in patients with neuroendocrine tumors in the United States. JAMA Oncol. 2017;3(10):1335–10. doi:10.1001/jamaoncol.2017.0589
2. Yao JC, Hassan M, Phan A, et al. One hundred years after “carcinoid”: epidemiology of and prognostic factors for neuroendocrine tumors in 35,825 cases in the United States. J Clin Oncol. 2008;26(18):3063–3072. doi:10.1200/JCO.2007.15.4377
3. Sorbye H, Grande E, Pavel M, et al. European Neuroendocrine Tumor Society (ENETS) 2023 guidance paper for digestive neuroendocrine carcinoma. J Neuroendocrinol. 2023;35(8):e13311. doi:10.1111/jne.13249
4. WHO Classification of Tumours Editorial Board. Digestive System Tumours.
5. Hallet J, Law CH, Cukier M, et al. Exploring the rising incidence of neuroendocrine tumors: a population-based analysis. Cancer. 2015;121(4):589–597. doi:10.1002/cncr.29099
6. Ma Z, Cai H, Cui Y. Progress in the treatment of esophageal neuroendocrine carcinoma. Tumour Biol. 2017;39(6):1010428317711313. doi:10.1177/1010428317711313
7. Ishida M, Sekine S, Fukagawa T, et al. Neuroendocrine carcinoma of the stomach: morphologic and immunohistochemical characteristics and prognosis. Am J Surg Pathol. 2013;37(7):949–959. doi:10.1097/PAS.0b013e31828ff59d
8. Huang Q, Wu H, Nie L, et al. Primary high-grade neuroendocrine carcinoma of the esophagus: a clinicopathologic and immunohistochemical study of 42 resection cases. Am J Surg Pathol. 2013;37(4):467–483. doi:10.1097/PAS.0b013e31826d2639
9. Xie JW, Lu J, Wang JB, et al. Prognostic factors for survival after curative resection of gastric mixed adenoneuroendocrine carcinoma: a series of 80 patients. BMC Cancer. 2018;18(1):1021. doi:10.1186/s12885-018-4943-z
10. Sorbye H, Welin S, Langer SW, et al. Predictive and prognostic factors for treatment and survival in 305 patients with advanced gastrointestinal neuroendocrine carcinoma (WHO G3): the NORDIC NEC study. Ann Oncol. 2013;24(1):152–160. doi:10.1093/annonc/mds276
11. Dasari A, Mehta K, Byers LA, et al. Comparative study of lung and extrapulmonary poorly differentiated neuroendocrine carcinomas. Cancer. 2018;124(4):807–815. doi:10.1002/cncr.31124
12. Heetfeld M, Chougnet CN, Olsen IH, et al. Characteristics and treatment of patients with G3 gastroenteropancreatic neuroendocrine neoplasms. Endocr Relat Cancer. 2015;22(4):657–664. doi:10.1530/ERC-15-0119
13. Frizziero M, Spada F, Lamarca A, et al. Gastroenteropancreatic neuroendocrine neoplasms and inflammation. Crit Rev Oncol Hematol. 2020;146:102840. doi:10.1016/j.critrevonc.2019.102840
14. Wang W, Zhang Y, Peng Y, Jin KZ, Butler AE. A Ki-67 index to predict treatment response and prognosis in gastroenteropancreatic neuroendocrine neoplasms. J Transl Med. 2021;19(1):131. doi:10.1186/s12967-021-02797-3
15. Hanahan D, Weinberg RA. Hallmarks of cancer: the next generation. Cell. 2011;144(5):646–674. doi:10.1016/j.cell.2011.02.013
16. Mantovani A, Allavena P, Sica A, Balkwill F. Cancer-related inflammation. Nature. 2008;454(7203):436–444. doi:10.1038/nature07205
17. Templeton AJ, McNamara MG, Šeruga B, et al. Prognostic role of neutrophil-to-lymphocyte ratio in solid tumors: a systematic review and meta-analysis. J Natl Cancer Inst. 2014;106(6):dju124. doi:10.1093/jnci/dju124
18. Guthrie GJ, Charles KA, Roxburgh CS, et al. The systemic inflammation-based neutrophil-lymphocyte ratio. Crit Rev Oncol Hematol. 2013;88(1):218–230. doi:10.1016/j.critrevonc.2013.03.010
19. Zhang J, Yao YH, Li BG, et al. Prognostic value of pretreatment serum lactate dehydrogenase level in patients with solid tumors. Sci Rep. 2015;5:9800. doi:10.1038/srep09800
20. Gupta D, Lis CG. Pretreatment serum albumin as a predictor of cancer survival. Nutr J. 2010;9:69. doi:10.1186/1475-2891-9-69
21. McMillan DC. The systemic inflammation-based glasgow prognostic score. Cancer Treat Rev. 2013;39(5):534–540. doi:10.1016/j.ctrv.2012.08.003
22. Nazha B, Moussaly E, Zaarour M, et al. Hypoalbuminemia in colorectal cancer prognosis. World J Gastrointest Surg. 2015;7(12):370–377. doi:10.4240/wjgs.v7.i12.370
23. Don BR, Kaysen G. Serum albumin: relationship to inflammation and nutrition. Semin Dial. 2004;17(6):432–437. doi:10.1111/j.0894-0959.2004.17603.x
24. Bowen RC, Little NAB, Harmer JR, et al. Neutrophil-to-lymphocyte ratio as prognostic indicator in gastrointestinal cancers: a systematic review and meta-analysis. Oncotarget. 2017;8(19):32171–32189. doi:10.18632/oncotarget.16291
25. Ethier JL, Desautels D, Templeton AJ, Shah PS, Amir E. Prognostic role of neutrophil-to-lymphocyte ratio in breast cancer: a systematic review and meta-analysis. Breast Cancer Res. 2017;19(1):2. doi:10.1186/s13058-016-0794-1
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Prognostic Roles of Inflammation- and Nutrition-Based Indicators for Female Patients with Cancer
Yang M, Zhang Q, Ge Y, Tang M, Hu C, Wang Z, Zhang X, Song M, Ruan G, Zhang X, Liu T, Xie H, Zhang H, Zhang K, Li Q, Li X, Liu X, Lin S, Shi H
Journal of Inflammation Research 2022, 15:3573-3586
Published Date: 17 June 2022
Fashionable, but What is Their Real Clinical Usefulness? NLR, LMR, and PLR as a Promising Indicator in Colorectal Cancer Prognosis: A Systematic Review
Misiewicz A, Dymicka-Piekarska V
Journal of Inflammation Research 2023, 16:69-81
Published Date: 7 January 2023
Prognostic Significance of Preoperative Lactate Dehydrogenase to Albumin Ratio in Breast Cancer: A Retrospective Study
He J, Tong L, Wu P, Wu Y, Shi W, Chen L
International Journal of General Medicine 2023, 16:507-514
Published Date: 8 February 2023
Albumin Level is Associated with Short-Term and Long-Term Outcomes in Sepsis Patients Admitted in the ICU: A Large Public Database Retrospective Research
Cao Y, Su Y, Guo C, He L, Ding N
Clinical Epidemiology 2023, 15:263-273
Published Date: 3 March 2023
Utilizing the Lactate Dehydrogenase-to-Albumin Ratio for Survival Prediction in Patients with Bladder Cancer After Radical Cystectomy
Xu H, Lin T, Ai J, Zhang J, Zhang S, Li Y, Zheng X, Zhang P, Wei Q, Tan P, Yang L
Journal of Inflammation Research 2023, 16:1733-1744
Published Date: 18 April 2023