")
Back to Journals » International Journal of General Medicine » Volume 16
Prognostic Significance of Preoperative Lactate Dehydrogenase to Albumin Ratio in Breast Cancer: A Retrospective Study
Authors He J, Tong L, Wu P, Wu Y, Shi W, Chen L
Received 22 November 2022
Accepted for publication 31 January 2023
Published 8 February 2023 Volume 2023:16 Pages 507—514
DOI https://doi.org/10.2147/IJGM.S396871
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jing He,1,* Ling Tong,2,* Ping Wu,3 Yibo Wu,2 Weifeng Shi,1 Ling Chen1
1Department of Breast Surgery, Affiliated Hospital of Jiangnan University, Wuxi, Jiangsu, People’s Republic of China; 2Human Reproductive Medicine Center, Affiliated Hospital of Jiangnan University, Wuxi, Jiangsu, People’s Republic of China; 3Department of Clinical Nutrition, Affiliated Hospital of Jiangnan University, Wuxi, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ling Chen; Weifeng Shi, Email [email protected]; [email protected]
Purpose: We explored the relationship between platelet count to lymphocyte count ratio (PLR), monocyte count to lymphocyte count ratio (MLR), lactate dehydrogenase to albumin ratio (LAR), and long-term survival in patients with breast cancer.
Patients and Methods: We retrospectively analyzed the clinical and follow-up data of 134 patients with breast cancer. The receiver operating characteristic curve (ROC curve) was used to distinguish between the low and high ratio groups. The chi-square test or Fisher’s exact test was used to calculate the differences among the investigation factors. The Kaplan–Meier method was used to draw the survival curves. Log rank test was used for univariate analysis, and Cox proportional hazards regression model was used for multivariate analysis. A P value of < 0.05 was considered statistically significant.
Results: The median follow-up time was 45 months. The PFS rates in the low group (LAR≤ 3.4066) at 18 months, 24 months, and 36 months were 100%, 100%, and 97.6%, and those in the high group (LAR > 3.4066) were 97.7%, 94.3%, and 87.3%, respectively. LAR was associated with Age (P=0.002) and BMI (body mass index) (P=0.002). Univariate analysis showed that Tumor size (P=0.027), Node positivity (P< 0.001), TNM (tumor-node-metastasis) stage (P< 0.001), PLR (P=0.034), MLR (P=0.038), and LAR (P=0.035) were significantly associated with PFS (progression-free survival) in breast cancer patients. Multivariate analysis showed that Node positivity (P< 0.001) and LAR (P=0.035) were associated with PFS, while PLR and MLR were not independent prognostic indicators.
Conclusion: Preoperative high LAR will be an independent predictor of prognosis in patients with breast cancer.
Keywords: breast cancer, prognosis, lactate dehydrogenase, albumin, platelet count to lymphocyte count ratio, monocyte count to lymphocyte count ratio, lactate dehydrogenase to albumin ratio
A Letter to the Editor has been published for this article.
A Response to Letter by Miss Zehra has been published for this article.
Introduction
Breast cancer is the most common malignant tumor in women worldwide.1 Similarly, epidemiological data shows that it ranks first in the incidence of tumors among Chinese female population.2 With increasing rate of breast cancer incidence, mortality is also increasing year by year in China.3 Traditional prognostic variables including the age of the patients, TNM (tumor-node metastasis) staging, histological grade, estrogen receptor (ER), progesterone receptor (PR), human epidermal growth factor receptor 2 (c-erbB2 or HER2) status are essential means to determine the prognosis of breast cancer patients.4 In the last few years, tumor-based gene expression profiling provided great promise in predicting breast cancer outcome.5 However, it is well known that survival time differs even for patients with the same disease stage and the same pathogenic type at the time of diagnosis. The prognosis of breast cancer patients is not only related to the characteristics of tumor but also related to the body’s response. Individualized assessment is needed to improve the prediction of patient’s prognosis.
Presently, it is widely accepted that a patient’s immune status and inflammatory response are associated with their therapeutic reaction and tumor prognosis.6 Since blood is minimally invasive and easily accessible, inflammatory markers might have an impact on the prognosis of patients with operable breast cancer.7 Therefore, we consider it meaningful to identify biochemical indicators and combine them to analyze their effect on an individual’s clinical outcome.
In a wide variety of tumor prognosis studies, several systemic inflammatory biomarkers including platelet count to lymphocyte count ratio (PLR), monocyte count to lymphocyte ratio (MLR), lactate dehydrogenase (LDH) to albumin ratio (LAR) are commonly used to reflect inflammatory reaction and immune response.8–10 PLR and MLR have been proven to influence the prognosis and survival of breast cancer, but whether they can be independent prognostic factors remains controversial.11,12 In addition, LDH, which has been reported as an important prognostic indicator in different cancer species, is a noteworthy enzyme and has good predictive power for the prognosis of breast cancer.7 Albumin (ALB), which indicates nutritional status, also reflects a good prognosis.7 Previous research has shown that the value of LAR is associated with the prognosis of colon cancer.13 But until now, no studies have shown the prognosis value of LAR in breast cancer.
Therefore, we retrospectively analyzed the relationship between progression-free survival (PFS) and preoperative PLR, MLR, and LAR in 134 patients with breast cancer to find out the best independent prognostic factors.
Materials and Methods
Study Design
This study studied 134 Xanthous female breast cancer patients recently diagnosed with non-metastatic invasive mammary carcinoma. All of them were pathologically diagnosed with primary breast cancer and received their first surgical treatment at Affiliated Hospital of Jiangnan University between April 2017 and September 2018. Patients with known inflammation or infections prior to surgery were excluded from this study. No other factors such as age, pathological features, and follow-up treatments have these recruitment restrictions. This research complies with the Declaration of Helsinki and was approved by the Medical Ethics Committee of the Affiliated Hospital of Jiangnan University (JNMS01202100129). All data are anonymous and aggregated, so the requirements for informed consent are waived.
Data Acquisition
Clinical and pathological data were abstracted from the patients’ clinical data and pathological reports. Body mass index (BMI) was categorized into <18.5, 18.5, ~23.9, and >23.9.14 Cancer stage (including tumor size, axillary lymph node positivity, and TNM) was evaluated for each patient, according to the eighth edition of the American Joint Committee on Cancer (AJCC) staging manual.15 Serum biochemical examination including laboratory test data (lymphocytes, platelets, monocytes, lactic acid dehydrogenase, and albumin) was performed at the baseline follow-up before surgery. The follow-up information was derived from outpatient reviews and telephone interviews. The primary endpoint of this study was PFS, defined as the time from postoperative pathological diagnosis until medical imaging indicated distant metastasis or death.16
Statistical Analysis
The cutoff values of PLR, MLR, and LAR were calculated using R software. The Youden index was calculated using receiver operating characteristic (ROC) curve with disease progression or death as endpoint. SPSS 26.0 software was used for statistical analysis. Chi-square test or Fisher’s exact test was used to calculate the differences among the investigation factors. In survival analysis, Kaplan–Meier method was used to draw the survival curve. Log rank test was used for univariate analysis, and the Cox proportional hazards regression model was used for multivariate analysis. A P value of <0.05 was considered statistically significant.
Results
The Best Cutoff Determination of PLR, MLR, and LAR
The area under the curve (AUC) of PLR, MLR, and LAR were 0.573, 0.729, and 0.709, respectively. Their optimal cutoff values were 110.6667, 0.2632, and 3.4066, respectively. The optimal sensitivity and specificity were 94.1% and 38.5% for PLR, 80.7% and 54.3% for MLR, and 94.1% and 38.5% for LAR (Figure 1).
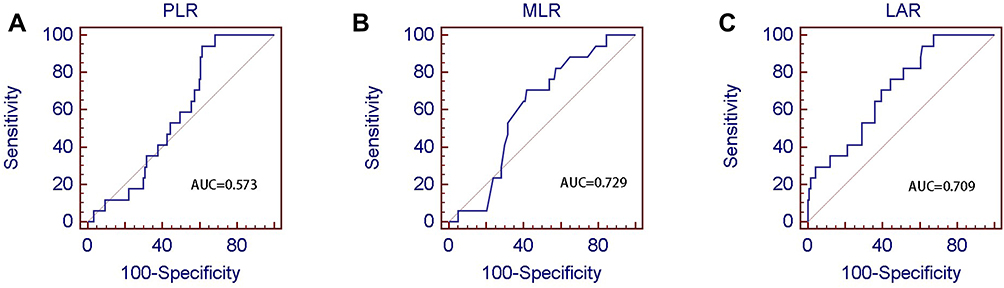 |
Figure 1 Best cutoff values of preoperative PLR, MLR, and LAR of 134 breast cancer patients. (A) Best cutoff of PLR; (B) Best cutoff of MLR; (C) Best cutoff of LAR. Abbreviation: AUC, area under the curve. |
Patient Characteristics
This study involved 134 Xanthous female patients newly diagnosed with non-metastatic invasive breast cancer, all of whom were admitted for surgical treatment initially. The median age of all patients was 51 years (range: 27–77 years). All primary tumor histological types were invasive ductal carcinoma. Two (1.5%) patients were underweight, 74 (55.2%) were in normal weight, and 58 (43.3%) were overweight, respectively. According to AJCC classification, 42 patients (31.3%) were diagnosed in stage I, 67 (50.0%) in stage II, and 25 (18.7%) in stage III, respectively. In terms of tumor size, 63 patients (47.0%) were T1, 67 patients (50.0%) were T2 and 4 patients (3.0%) were T3. Axillary lymph nodes were negative in 81 patients (60.5%), 1–3 positive in 28 patients (20.9%), 4–9 positive in 16 patients (11.9%), and ≥10 positive in 9 patients (6.7%), respectively. ER status was positive in 93 patients (69.4%) and negative in 41 patients (30.6%). About 73 patients (54.5%) had positive PR status and 61 patients (45.5%) had negative PR status. As for Her-2 status, 49 (36.6%) was positive and 85 (63.4%) negative. Table 1 shows the association of clinical pathological characteristics with LAR. LAR was associated with Age (P=0.002) and BMI (P=0.002). However, it was not statistically significant in correlation with other clinical pathological characteristics.
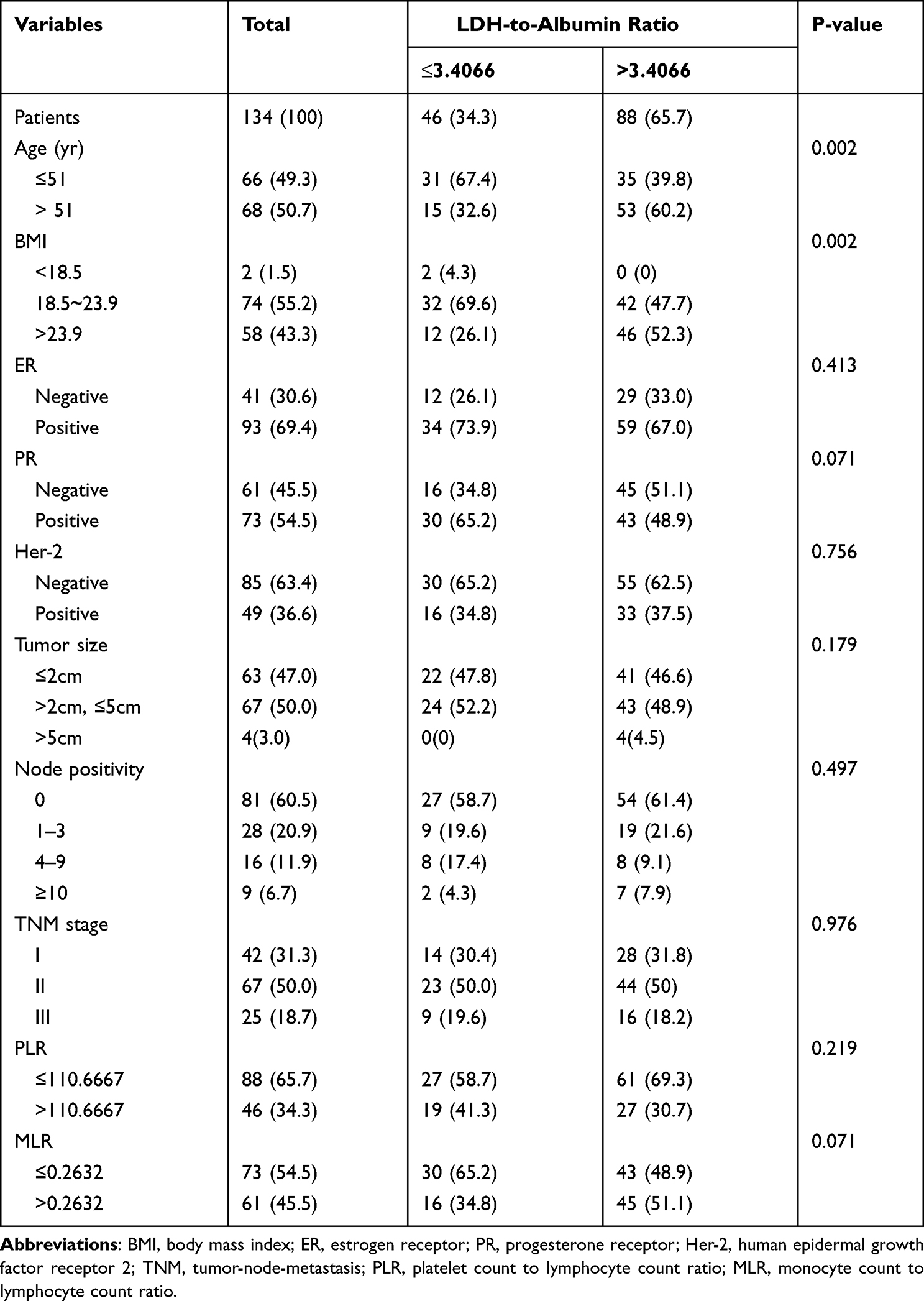 |
Table 1 Clinicopathological Characteristics of 134 Patients with Breast Cancer |
Survival Analysis and Prognosis of Breast Cancer Patients
The median follow-up period for the patients was 45 months. According to the best critical value, patients were divided into a high fraction group and a low fraction group. The PFS rates in the low group (LAR≤3.4066) at 18 months, 24 months, and 36 months were 100%, 100%, and 97.6%, and those in the high group (LAR > 3.4066) were 97.7%, 94.3%, and 87.3%, respectively.
Univariate analysis showed that Tumor size (P=0.027), Node positivity (P<0.001), TNM stage (P<0.001), PLR (P=0.034), MLR (P=0.038), and LAR (P=0.035) were significantly associated with PFS in patients with breast cancer (Table 2). There was a negative correlation between PFS and LAR, and PFS of high LAR group was lower than that of low LAR group. To better evaluate prognostic factors, Cox multiple regression model was used to analyze the relationship between PFS and Tumor size, Node positivity, TNM stage, PLR, MLR, LAR. The results showed that Node positivity (P<0.001) and LAR (P=0.035) in patients with breast cancer were associated with PFS (Table 2, Figure 2).
 |
Table 2 Analysis of Prognosis Factors in 134 Breast Cancer Patients by Univariate and Multivariate Analysis |
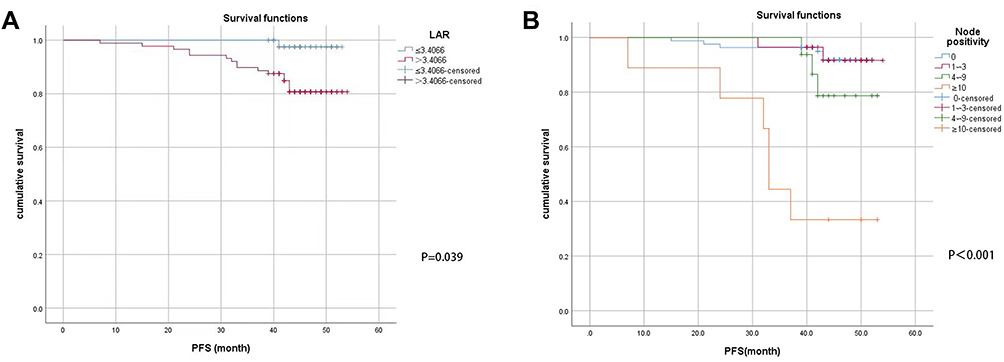 |
Figure 2 PFS curve of preoperative LAR and Node stage of 134 breast cancer patients. (A) LAR for PFS; (B) Node positivity for PFS. |
Discussion
In this study, PLR, MLR, and LAR values representing the immune status and inflammatory response were compared to determine the prognosis of patients with breast cancer. PFS of patients with high LAR was significantly lower than those with low LAR. In addition, LAR was negatively associated with PFS in patients with breast cancer according to a multivariate analysis. LAR is a repeatable, widely used, and inexpensive laboratory hematological index, which has become an important research object in cancer research.17,18 LAR is composed of two vital substances, LDH and albumin. LDH plays a pivotal role in converting pyruvate to lactate when oxygen is undersupplyed or deficient in the course of cell metabolism.19 Hypoxia in the tumor microenvironment results in high LDH levels.20 LDH is associated with a number of activities, including metabolic activity, tissue injury, inflammation, and neoplasm. Many studies have indicated that serum LDH is an effective index that could be used to evaluate tumor activity and forecast therapeutic effect and prognosis.21,22 It has been reported that high serum LDH levels are a prognostic indicator for poor survival in numerous tumor types.23 Xiaoan Liu et al7 found that higher LDH levels predict the higher risks of tumor metastasis in breast cancer. Serum albumin, a major protein in blood, is an efficient index for evaluating nutritional status.24 Due to mal-nutrition and systemic inflammatory response, serum albumin level fall drastically in advanced cancer patients.25 Pretreatment serum albumin has been utilized as a predictor to evaluate disease progression, the severity of disease and prognosis.26 It has been reported that lower blood serum albumin level is an independent affecting factor of worse survival in breast cancer regardless of stages.7 Therefore, LAR can be used as an indicator for the comprehensive assessment of tumor burden, nutritional status, and systemic inflammation in patients. Cumulative studies have shown that the value of LAR is associated with early diagnosis, prognosis evaluation, and recurrence prediction of tumors, which can be an independent poor-prognostic factor, including nasopharyngeal carcinoma, gastric carcinoma, colon carcinoma, and liver carcinoma.8,13,27,28 However, the prognostic value of LAR in breast cancer has not been reported yet so far. To our knowledge, the current study is the first to investigate the prognostic value of LAR in patients with breast cancer. The findings of this study suggest that preoperative LAR high values (LAR>3.4066) may be used as an independent indicator of poor prognosis in patients with breast cancer.
In this study, in univariate analysis, PLR and MLR values were associated with PFS in patients with breast cancer. However, in multivariate analysis, they were not correlated with PFS. Platelets play a major role in stimulating vasculogenic mimicry and metastasis of tumor cells.29 Lymphocytes, which can inhibit tumor cell proliferation and metastasis, have a major role in cancer immune surveillance.30 Azab et al31 showed that breast cancer patients with elevated lymphocyte counts had an improved survival than those with lower lymphocyte counts. Monocytes, as inflammatory biomarkers, have emerged as important regulators of cancer development and progression.32 PLR, the ratio of platelet count to lymphocyte count, has been investigated as a prognostic factor in several cancer entities. Jarroudi et al33 found that the elevated level of PLR was correlated with worse DFS (disease free survival) and OS (overall survival) in non-metastatic inflammatory breast cancer. Krenn-Pilko et al34 stated that an advanced preoperative PLR level appeared to have a significant effect on OS and Cancer-specific survival (CSS) in patients with non-metastatic breast cancer, whereas only univariable analysis presented a noticeable impact of increased PLR level on distant metastasis-free survival (DMFS). Azab et al31 stated that higher PLR indicated a trend of higher mortality only in patients with normal lymphocyte count. The findings of this study were in favor of the view of Krenn-Pilko et al34 partially, as the data suggested that PLR value was connected with PFS in patients with breast cancer in univariate analysis. The author speculated that this might be in connection with the small sample size selected by the single-center study. MLR, the ratio of monocytes to lymphocytes, is also regarded as a prognostic indicator in a variety of tumors. Li et al10 found that MLR was not only an independent prognostic factor but also a dangerous factor for recurrence in stage IIB cervical cancer. In breast cancer, Hua et al35 stated that MLR, combined with neutrophil–lymphocyte ratio (NLR), albumin-alkaline phosphatase ratio (AAPR), and prognostic nutritional index (PNI), which is called inflammatory nutritional prognostic score (INPS), is an independent prognostic factor of OS in women with early mammary cancer. Şahin et al36 found that in univariate analysis, MLR value was significantly associated with new accessorial chemotherapy response in breast cancer patients. However, multivariate analysis revealed an insignificant correlation. In this study, MLR can also be considered to be associated with tumor prognosis, but it is not an independent indicator.
In the survival analysis, data showed that Node positivity was significantly associated with PFS, while Tumor size and TNM were not directly associated with prognosis. In the eighth edition of the TNM classification published by the AJCC, tumor size, lymph node status, and distant metastasis are closely associated with survival.37 The author speculated that this outcome would be correlated with the small sample size, so stratified analysis cannot be performed. We investigated the correlation between clinical pathological characteristics and LAR value in breast cancer patients and found that BMI and age were associated with LAR. BMI is a nutrition monitoring index, while LAR itself can better represent the nutritional status of the whole body, so this is in line with forecast. Salive et al38 found that a 10-year age increment was associated with 0.8 g/l lower serum albumin and odds ratio of 1.56 for hypoalbuminemia after adjusting for demographic factors and health status. However, there were no reports which have shown that age is associated with LDH so far. Therefore, the results in our study that age were associated with LAR are consistent with previous report.
This study has several limitations. First of all, this study was only a single-center study, and the sample size (134 cases) may not be sufficient to fully reflect the status of breast cancer patients. Secondly, it is short of follow-up time and lacks OS. Median follow-up time was 45 months and most postoperative breast cancer patients often confront the first peak time of recurrence before 36 months.39 The OS rate continues to increase due to the diversification of treatment methods for advanced breast tumors. Meanwhile, due to the credible and complete quantitative data on PFS, the value of LAR for the prognosis of breast cancer patients is compelling and sufficient, especially for those who may suffer the first recurrent peak. Thirdly, this is a retrospective study and has some certain inherent limitations. Last but not least, LAR was only evaluated in time prior to surgery at a single point. However, dynamic changes in LAR may have a more significant effect on patients throughout their tumor treatment, which we did not evaluate.
Conclusion
In summary, the data from this study indicate that LAR will be used as an independent prognostic indicator to affect the prognosis of breast cancer patients. LAR may therefore be a useful biomarker in breast cancer evaluation to guide appropriate treatment, adjust follow-up intervals, and improve prognosis.
Acknowledgment
The authors wish to appreciate all the study participants and research staff who participated in this work.
Funding
The authors did not receive support from any organization for the submitted work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ferlay J, Soerjomataram I, Dikshit R, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015;136(5):E359–E386. doi:10.1002/ijc.29210
2. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
3. Lei S, Zheng R, Zhang S, et al. Global patterns of breast cancer incidence and mortality: a population-based cancer registry data analysis from 2000 to 2020. Cancer Commun. 2021;41(11):1183–1194. doi:10.1002/cac2.12207
4. D&apos G, Eredita M, Martellotta T, Natale F, Ferrarese A. Prognostic factors in breast cancer: the predictive value of the Nottingham Prognostic Index in patients with a long-term follow-up that were treated in a single institution. Eur J Cancer. 2001;37:591–596. doi:10.1016/S0959-8049(00)00435-4
5. Yersal O, Barutca S. Biological subtypes of breast cancer: prognostic and therapeutic implications. World J Clin Oncol. 2014;5(3):412–424. doi:10.5306/wjco.v5.i3.412
6. Elinav E, Nowarski R, Thaiss CA, Hu B, Jin C, Flavell RA. Inflammation-induced cancer: crosstalk between tumours, immune cells and microorganisms. Nat Rev Cancer. 2013;13(11):759–771. doi:10.1038/nrc3611
7. Liu X, Meng QH, Ye Y, Hildebrandt MA, Gu J, Wu X. Prognostic significance of pretreatment serum levels of albumin, LDH and total bilirubin in patients with non-metastatic breast cancer. Carcinogenesis. 2015;36(2):243–248. doi:10.1093/carcin/bgu247
8. Peng RR, Liang ZG, Chen KH, Li L, Qu S, Zhu XD. Nomogram based on Lactate Dehydrogenase-to-Albumin Ratio (LAR) and Platelet-to-Lymphocyte Ratio (PLR) for predicting survival in nasopharyngeal carcinoma. J Inflamm Res. 2021;14:4019–4033. doi:10.2147/JIR.S322475
9. Liang RF, Li JH, Li M, Yang Y, Liu YH. The prognostic role of controlling nutritional status scores in patients with solid tumors. Clin Chim Acta. 2017;474:155–158. doi:10.1016/j.cca.2017.09.021
10. Li YX, Chang JY, He MY, et al. Neutrophil-to-Lymphocyte Ratio (NLR) and Monocyte-to-Lymphocyte Ratio (MLR) predict clinical outcome in patients with stage IIB cervical cancer. J Oncol. 2021;2021:2939162. doi:10.1155/2021/2939162
11. Guo W, Lu X, Liu Q, et al. Prognostic value of neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio for breast cancer patients: an updated meta-analysis of 17079 individuals. Cancer Med. 2019;8(9):4135–4148. doi:10.1002/cam4.2281
12. Tiainen S, Rilla K, Hamalainen K, Oikari S, Auvinen P. The prognostic and predictive role of the neutrophil-to-lymphocyte ratio and the monocyte-to-lymphocyte ratio in early breast cancer, especially in the HER2+ subtype. Breast Cancer Res Treat. 2021;185(1):63–72. doi:10.1007/s10549-020-05925-7
13. Xie Z, Zhou H, Wang L, Wu Y. The Significance of the preoperative lactate dehydrogenase/albumin Ratio in the Prognosis of Colon Cancer: a retrospective study. PeerJ. 2022;10:e13091. doi:10.7717/peerj.13091
14. Zhou B-F. Effect of body mass index on all-cause mortality and incidence of cardiovascular diseases--report for meta-analysis of prospective studies open optimal cut-off points of body mass index in Chinese adults. Biomed Environ Sci. 2002;15(3):245–252.
15. Amin MB, Greene FL. AJCC Cancer Staging Manual.
16. Benjamin MAF, Fallara G, Ploussard G, Pradere B. Progression-free survival is an adequate endpoint for clinical trials of locally advanced and metastatic urothelial carcinoma. Curr Opin Urol. 2022;32(5):500–503. doi:10.1097/MOU.0000000000001012
17. Gao S, Wu M, Chen Y, et al. Lactic dehydrogenase to albumin ratio in prediction of unresectable pancreatic cancer with intervention chemotherapy. Future Oncol. 2018;14(14):1377–1386. doi:10.2217/fon-2017-0556
18. Feng JF, Wang L, Yang X, Jiang YH. Prognostic value of lactate dehydrogenase to albumin ratio (LAR) in patients with resectable esophageal squamous cell carcinoma. Cancer Manag Res. 2019;11:7243–7251. doi:10.2147/CMAR.S208320
19. Valvona CJ, Fillmore HL, Nunn PB, Pilkington GJ. The regulation and function of lactate dehydrogenase a: therapeutic potential in brain tumor. Brain Pathol. 2016;26(1):3–17. doi:10.1111/bpa.12299
20. Smith H, Board M, Pellagatti A, Turley H, Boultwood J, Callaghan R. The effects of severe hypoxia on glycolytic flux and enzyme activity in a model of solid tumors. J Cell Biochem. 2016;117(8):1890–1901. doi:10.1002/jcb.25488
21. Mishra D, Banerjee D. Lactate dehydrogenases as metabolic links between tumor and stroma in the tumor microenvironment. Cancers. 2019;11:6. doi:10.3390/cancers11060750
22. Feng Y, Xiong Y, Qiao T, Li X, Jia L, Han Y. Lactate dehydrogenase A: a key player in carcinogenesis and potential target in cancer therapy. Cancer Med. 2018;7(12):6124–6136. doi:10.1002/cam4.1820
23. Ding J, Karp JE, Emadi A. Elevated lactate dehydrogenase (LDH) can be a marker of immune suppression in cancer: interplay between hematologic and solid neoplastic clones and their microenvironments. Cancer Biomark. 2017;19(4):353–363. doi:10.3233/CBM-160336
24. Saito H, Kono Y, Murakami Y, et al. Postoperative serum albumin is a potential prognostic factor for older patients with gastric cancer. Yonago Acta Med. 2018;61(1):72–78. doi:10.33160/yam.2018.03.010
25. Yeun JY, Kaysen GA. Factors influencing serum albumin in dialysis patients. Am J Kidney Dis. 1998;32(6 Suppl 4):S118–S125. doi:10.1016/S0272-6386(98)70174-X
26. Gupta D, Lis CG. Pretreatment serum albumin as a predictor of cancer survival: a systematic review of the epidemiological literature. Nutr J. 2010;9:69. doi:10.1186/1475-2891-9-69
27. Gan W, Zhang MX, Wang JX, et al. Prognostic impact of lactic dehydrogenase to albumin ratio in hepatocellular carcinoma patients with Child-Pugh I who underwent curative resection: a prognostic nomogram study. Cancer Manag Res. 2018;10:5383–5394. doi:10.2147/CMAR.S176317
28. Nakazawa N, Sohda M, Yamaguchi A, et al. An elevated serum lactate dehydrogenase-to-albumin ratio is a useful poor prognostic predictor of nivolumab in patients with gastric cancer. Anticancer Res. 2021;41(8):3925–3931. doi:10.21873/anticanres.15188
29. Sabrkhany S, Griffioen AW, Oude Egbrink MG. The role of blood platelets in tumor angiogenesis. Biochim Biophys Acta. 2011;1815(2):189–196. doi:10.1016/j.bbcan.2010.12.001
30. Dunn GP, Old LJ, Schreiber RD. The immunobiology of cancer immunosurveillance and immunoediting. Immunity. 2004;21(2):137–148. doi:10.1016/j.immuni.2004.07.017
31. Azab B, Shah N, Radbel J, et al. Pretreatment neutrophil/lymphocyte ratio is superior to platelet/lymphocyte ratio as a predictor of long-term mortality in breast cancer patients. Med Oncol. 2013;30(1):432. doi:10.1007/s12032-012-0432-4
32. Olingy CE, Dinh HQ, Hedrick CC. Monocyte heterogeneity and functions in cancer. J Leukoc Biol. 2019;106(2):309–322. doi:10.1002/JLB.4RI0818-311R
33. Al Jarroudi O, El Bairi K, Abda N, et al. Neutrophil-to-lymphocyte and platelet-to-lymphocyte ratios as predictors of outcomes in inflammatory breast cancer. Biomark Med. 2021;15(14):1289–1298. doi:10.2217/bmm-2020-0717
34. Krenn-Pilko S, Langsenlehner U, Thurner EM, et al. The elevated preoperative platelet-to-lymphocyte ratio predicts poor prognosis in breast cancer patients. Br J Cancer. 2014;110(10):2524–2530. doi:10.1038/bjc.2014.163
35. Hua X, Duan F, Zhai W, et al. A novel inflammatory-nutritional prognostic scoring system for patients with early-stage breast cancer. J Inflamm Res. 2022;15:381–394. doi:10.2147/JIR.S338421
36. Sahin AB, Cubukcu E, Ocak B, et al. Low pan-immune-inflammation-value predicts better chemotherapy response and survival in breast cancer patients treated with neoadjuvant chemotherapy. Sci Rep. 2021;11(1):14662. doi:10.1038/s41598-021-94184-7
37. Amin MB, Greene FL, Edge SB, et al. The eighth edition AJCC cancer staging manual: continuing to build a bridge from a population-based to a more “personalized” approach to cancer staging. CA Cancer J Clin. 2017;67(2):93–99. doi:10.3322/caac.21388
38. Salive ME, Cornoni-Huntley J, Phillips,CL, et al. Serum albumin in older persons: relationship with age and health status. J Clin Epidemiol. 1992;45(3):213–221. doi:10.1016/0895-4356(92)90081-W
39. Ribelles N, Perez-Villa L, Jerez JM, et al. Pattern of recurrence of early breast cancer is different according to intrinsic subtype and proliferation index. Breast Cancer Res. 2013;15(5):R98. doi:10.1186/bcr3559
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.