Back to Archived Journals » Pathology and Laboratory Medicine International » Volume 15
Patterns of Fine Needle Aspiration Cytology Diagnosed Thyroid Nodules Among Clinically Suspected Patients in Northeast Ethiopia
Authors Ebrahim H ![]() , Tilahun M
, Tilahun M ![]() , Fiseha T
, Fiseha T ![]() , Debash H, Bisetegn H
, Debash H, Bisetegn H ![]() , Alemayehu E
, Alemayehu E ![]() , Fiseha M
, Fiseha M ![]() , Ebrahim E
, Ebrahim E ![]() , Shibabaw A
, Shibabaw A ![]() , Seid A, Getacher Feleke D
, Seid A, Getacher Feleke D ![]() , Mohammed O
, Mohammed O ![]()
Received 30 November 2022
Accepted for publication 7 March 2023
Published 10 March 2023 Volume 2023:15 Pages 27—36
DOI https://doi.org/10.2147/PLMI.S399682
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Paul Zhang
Hussen Ebrahim,1 Mihret Tilahun,1 Temesgen Fiseha,1 Habtu Debash,1 Habtye Bisetegn,1 Ermiyas Alemayehu,1 Mesfin Fiseha,1 Endris Ebrahim,1 Agumas Shibabaw,1 Abdurahaman Seid,1 Daniel Getacher Feleke,2 Ousman Mohammed1
1Department of Medical Laboratory Sciences, College of Medicine and Health Sciences, Wollo University, Dessie, Ethiopia; 2Department of Microbiology, Immunology, and Parasitology, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Hussen Ebrahim, Po.Box:1145, Tel +251921332772, Email [email protected]
Background: Thyroid nodules are the most common thyroid disease and its incidence has been rising throughout the world. Thus, this study aimed to assess the patterns of fine needle aspiration cytology-diagnosed thyroid nodules among clinically suspected patients.
Methods: A prospective cross-sectional study was conducted from April 2021 to March 2022 using 424 study participants who were referred to undergo fine needle aspiration cytology examination and were consecutively included. Moreover, two FNAC smears were prepared and stained using Wright and Giemsa staining solutions and then examined by an experienced licensed pathologist. Multivariate logistic regression was used to determine the association of socio-demographic and clinical variables with nodules. P-value < 0.05 was considered to be statistically significant.
Results: The overall magnitude of benign and malignant nodules was 60.4% and 16.5% respectively. Moreover, the magnitude of atypical of undetermined significance or follicular lesion of undetermined significance (AUS/FLUS) and follicular neoplasm or suspicious of follicular neoplasm (FN/SFN) was 3.54% and 1.42% respectively. The magnitude of malignant thyroid nodules was 5.9% for malignant secondary adenocarcinoma, 3.5% for papillary thyroid carcinoma, 2.6% for Non-Hodgkin lymphoma, 2.4% for medullary thyroid carcinoma, 1.4% of an undifferentiated malignant thyroid tumor and 0.7% of Hodgkin lymphoma respectively. Multivariate logistic regression showed that age categories between 0 and 15 years and between 16 and 30 years, and nodule size > 2.5cm were significantly associated with malignant thyroid nodules.
Conclusion: The magnitude of benign and malignant tumors was 60.4% and 16.5% respectively. Being younger and having nodule size > 2.5cm were significantly associated with malignant thyroid nodules. Therefore, fine needle aspiration cytology examination has a crucial role in the diagnosis and management of benign and malignant thyroid nodules.
Keywords: benign, cytology, fine needle aspiration, malignant, thyroid tumors, thyroid gland, thyroid nodules, ultrasound, Ethiopia
Introduction
Thyroid gland is one of the largest endocrine glands comprised of two connected lobes in the human body weighing 20 to 30 grams in adults.1 The gland is histologically composed of two types of parenchymal cells. The follicular cell line of the colloid follicles has a significant role in iodine concentration and thyroid hormone production. The other is a Para-follicular cell that can involve in calcitonin hormone production.2 Thyroid lesions are occasionally found in the gland with a magnitude of 4% to 7%. In most cases, the lesions are asymptomatic, have normal thyroid hormone production, and are non-cancerous.1 Thyroid nodules are the most common thyroid disease and its incidence has been rising throughout the world. In recent years, data showed that the magnitude lies between 2 to 6% with physical examinations, 19 to 68% with sensitive imaging devices, and 8 to 65% with autopsy examinations.3 However, a recent investigation showed that around 90% of thyroid nodules were benign, and 7% to 15% of such cases have the risk of malignant transformation.4
Benign thyroid nodules are usually prevalent among the entire population. On many occasions, the cases are usually asymptomatic. However, the incidence has increased due to the increased application of ultrasound diagnostic procedures. Benign nodules are clinically monitored and managed as soon as the size increased enough causing compressive symptoms warranting surgery management.5 In most cases, surgical management of the nodules is well-tolerated and has low risk, but it may be related to a minor risk of complications including hypothyroidism, nerve injury, hematoma, injury to other structures, and wound infections.6 Nowadays, newer image-guided ablation techniques including radiofrequency ablation (RFA) have been introduced which have similar safety profiles as it is compared to surgery. It has been considered a promising result in a patient with a challenging surgical candidate.7
Multiple etiological factors have been considered to be the cause of thyroid cancer through a multi-step carcinogenesis process. Cancerous cells are originated from thyroid follicular cells under multiple exposures to the damaging agent to their genomic structure encompassing the oncogenes or anti-oncogenes counterpart. The overall mechanism results in accelerated proliferation or formation of malignant follicular cells infiltrating the nearby surrounding tissue or disseminating to distant organs.8 Evidence showed that the magnitude of clinically diagnosed thyroid cancer has been considered to be the first event of carcinogenesis. It has been thought to occur in middle age, but some cancer cells acquire a more aggressive phenotype after repeated proliferation, causing the accumulation of altered genetic compositions. Thyroid cancer is considered to be the most common endocrine malignant disorder representing 3.4% of all cancers. It is fifth-ranked cancer in women. It is common in women with a positive family history of thyroid disease.9
The transformation of thyroid follicular cells may lead to either differentiated or undifferentiated thyroid cancer through a multistep carcinogenesis process. The most widely accepted theory is follicular cell carcinogenesis suggesting that distinct molecular alterations have been associated with specific stages driving progression from well-differentiated to undifferentiated follicular-derived thyroid carcinomas.10 Recently, the cancer stem-like cells theory has proposed that phenotypically different cancer cells might be originated from a small subpopulation of stem cells after genetic and epigenetic transformations.3 Therefore, differentiated thyroid cancer accounts for more than 90% of malignant thyroid cancer mainly comprises papillary thyroid carcinoma and follicular thyroid carcinoma. However, poorly differentiated thyroid carcinoma and anaplastic thyroid carcinoma are rare thyroid tumors that accounted for 5% and 1% respectively which are associated with aggressive behavior and short median time of survival. Moreover, medullary thyroid carcinoma represents 5% of thyroid cancer which may arise from Para follicular cell lines.11
Physical, clinical, ultrasound (sensitive imaging examinations), and fine-needle aspiration cytology examinations (FNAC) are carefully investigated tremendously to differentiate benign from malignant thyroid nodules to facilitate the clinical decision-making process.12 Thyroid cancer is a common malignant disease in the endocrine system and its incidence increased rapidly throughout the world. Most thyroid cancers show biologically benign or indolent phenotypes and have excellent prognoses and survival rates. The incidence of thyroid cancer is about three to four times higher in females than males and is the most common malignant disease diagnosed in women worldwide.13 Ultrasonography and cytological testing of thyroid nodules utilizing fine-needle aspiration are the preferred tests for the diagnosis of benign and malignant thyroid tumors.14
The Bethesda system of reporting thyroid fine-needle aspiration specimens represents a major step toward standardization, reproducibility, and ultimately improved clinical significance, usefulness, and predictive value of thyroid fine-needle aspiration.15 Reporting FNAC results of thyroid lesions with the Bethesda system allows a more specific cytological diagnosis that helps to unify the terminology and morphologic criteria along with the corresponding risk of malignancy. So, there are six diagnostic categories of thyroid FNAC result reporting that include I (non-diagnostic or unsatisfactory), II (benign), III (atypical of undetermined significance ((AUS) or follicular lesion of undetermined significance (FLUS)), IV (follicular neoplasm (FN) or suspicious for follicular neoplasm (SFN)), V (suspicious of malignancy (SM) and V (malignant).16–18
Fine needle aspiration cytology combined with ultrasound imaging examination has wider application in clinical medicine for the diagnosis and monitoring of benign and malignant thyroid tumors. Few studies were conducted to assess the patterns of fine needle aspiration cytology-diagnosed thyroid nodules in resource-limited countries like Ethiopia. Still, there was a similar investigation yet conducted in the study area. Therefore, this study aims to assess the patterns of fine needle aspiration cytology-diagnosed thyroid nodules among clinically suspected patients in northeast Ethiopia.
Methods and Materials
Study Design, Period, and Area
A prospective cross-sectional study was conducted to assess the patterns of fine needle aspiration cytology-diagnosed thyroid nodules among clinically suspected patients in Dessie town, Northeast Ethiopia from April 2021 to March 2022. The study was conducted in the diagnostic laboratory which is found in Dessie town about 401 Km far from Addis Ababa, the capital city of Ethiopia. The clinical laboratory provides diagnostic services including routine and advanced laboratory investigations to the patients. It also serves as a diagnostics center for cancer patients who came from different health institutions.
Study Population, Participants, and Sampling Techniques
The study populations were all patients who were clinically suspected and referred to undergo fine needle aspiration cytology examination. Therefore, a total of 424 study participants who came to the diagnostic laboratory with a request form for fine needle aspiration cytology examination were consecutively included as the study participants during the study period.
Data Collection and Laboratory Analysis
The socio-demographic variables of study participants were collected using a structured questionnaire. The size, number, and characteristics of the nodules were assessed using an ultrasound imaging device by an experienced licensed radiologist. Fine-needle aspiration cytology specimen was collected from the most suspicious thyroid nodule area. Specimen for FNAC was collected using a 10 mL syringe with the 24-gauge needle. Moreover, two FNAC smears were prepared for each patient, and the preparation was stained using Wright and Giemsa staining solutions. Finally, the stained smears were examined by experienced and licensed general pathologists.
Data Quality Management
The specimen for fine needle aspiration cytology examination was collected and processed based on the standard operating procedures (SOPs). Smear preparations and examinations of fine needle aspiration cytology were strictly performed according to the standard operating procedures. Positive and negative smear preparations were used to monitor the quality of the stain and to check the quality of the smear preparations.
Data Management, Statistical Analysis, and Interpretation
After the data has been collected, it was coded and entered into Epi Data 3.1 version and then exported to statistical package for social sciences (SPSS) version 23.0 (IBM Corporation, Armonk, NY, USA). The result of this finding was expressed using mean and standard deviation and also texts and tables were used to present the necessary finding. The magnitudes of benign and malignant thyroid nodules were expressed using descriptive statistics including ratio, frequency, and percentage. Bivariate and multivariate logistic regressions were used to assess the association of socio-demographic and clinical variables with benign and malignant thyroid nodules among study participants. P-value < 0.05 was considered to be statistically significant.
Ethical Approval and Consent to Participate
Before the study started, ethical approval was obtained from the Research and Ethics Review Committee at the College of Medicine and Health Sciences, Wollo University. A support letter was obtained from Dessie zonal health office and a permission letter was obtained from the chief executive officer of the diagnostic medical laboratory plc. Furthermore, written informed consent was secured from each study participant before data collection.
Results
Patterns of Fine Needle Aspiration Cytology-Diagnosed Thyroid Nodules Among Study Participants
In this study, a total of 424 study participants who had abnormal neck swelling and were ordered by physicians to undergo fine needle aspiration cytology were included. The mean + SD of the age of the study participants was 37.74 (+17.78). Regarding the age of study participants, the minimum and maximum age was between 1 and 97 years. Out of 424 study participants, 269 (63.4%) were females. Furthermore, the majority of the study participants, 163 (38.4%) were grouped within the age categories between 15 and 30 years. The overall prevalence of benign nodules was 60.4% (256/424) in study participants. Moreover, the magnitude of atypical of undetermined significance or follicular lesion of undetermined significance ((AUS/FLUS); Bethesda category III)) was 3.54%, follicular neoplasm or suspicious of follicular neoplasm ((FN/SFN; Bethesda category IV)) were 1.42% and 16.5% cases were malignant nodules (Bethesda category VI) (Table 1).
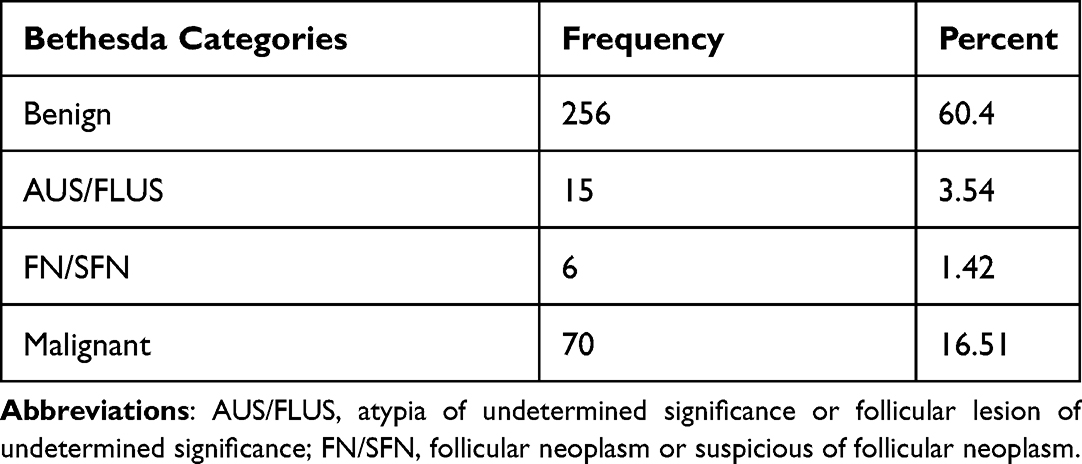 |
Table 1 Pattern of Thyroid Nodules Based on Bethesda Categories Among Study Participants in Northeast Ethiopia from April 2021 to March 2022 (n=424) |
The Magnitude of Benign Thyroid Nodules Among Study Participants
The prevalence of benign nodules (Bethesda category II) diagnosed was; 32.5% of benign adenomatoid goiter, 9.9% of chronic suppurative inflammation, 9.7% of TB lymphadenitis, 5.7% of reactive lymphoid hyperplasia, 1.9% of sub-acute granulomatous thyroiditis and 0.7% of Hashimoto’s thyroiditis respectively. In this study, a higher magnitude of benign nodules was found in female study participants accounting for 69.1% of cases. Furthermore, benign nodule cases were dominant within the age categories between 15 and 30 years which accounted for 44.9% of cases (Table 2).
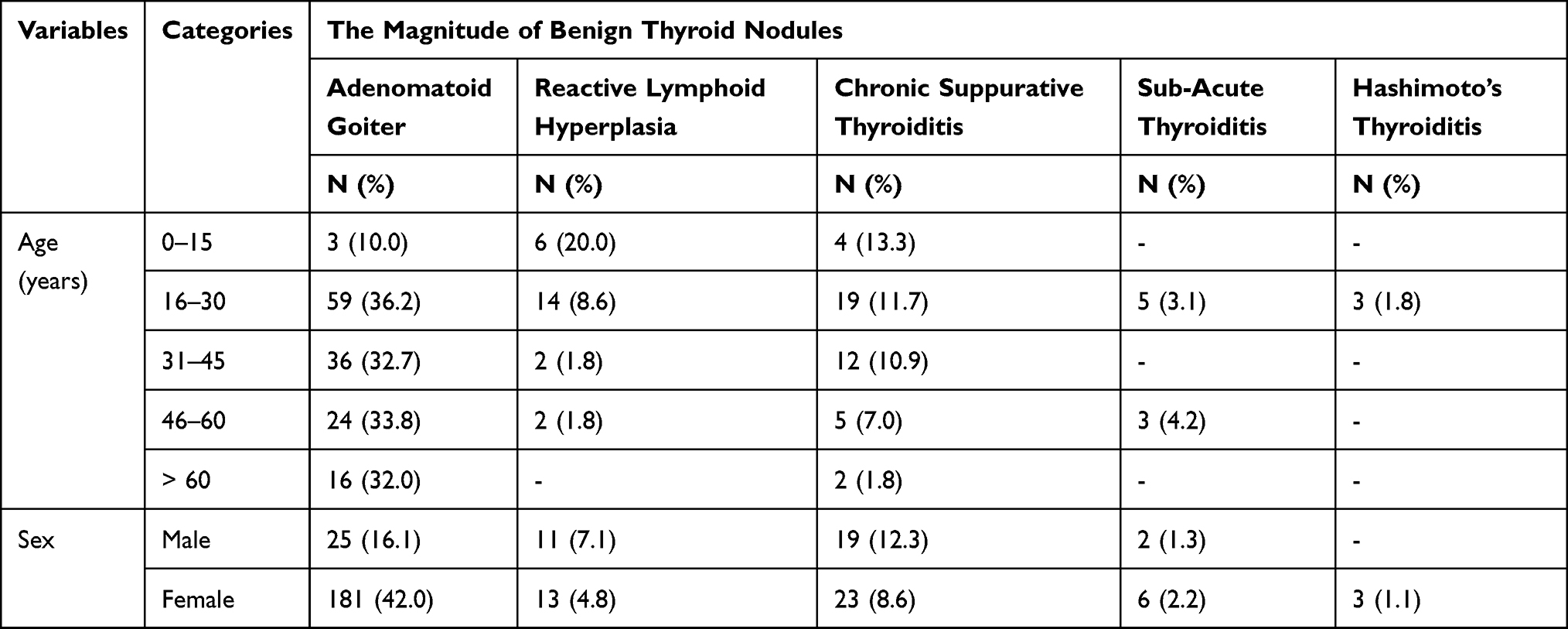 |
Table 2 Magnitude of Benign Thyroid Nodules Among Study Participants in Northeast Ethiopia from April 2021 to March 2022 (n=424) |
The Magnitude of Malignant Thyroid Nodules Among Study Participants
In this study, the overall magnitude of malignant thyroid nodule cases was 16.5% (70/424) among study participants. The magnitude of malignant thyroid nodules diagnosed was; 5.9% of malignant secondary adenocarcinoma, 3.5% of papillary thyroid carcinoma, 2.6% of Non-Hodgkin lymphoma, 2.4% of medullary thyroid carcinoma, 1.4% of high grade undifferentiated malignant thyroid tumor and 0.7% of Hodgkin lymphoma respectively. Furthermore, a higher prevalence of malignant thyroid nodules was found in females which accounted for 58.2% of malignant cases. Moreover, malignant thyroid nodule cases were dominant in the age categories between 15 and 30 years which accounted for 28.6% of cases (Table 3).
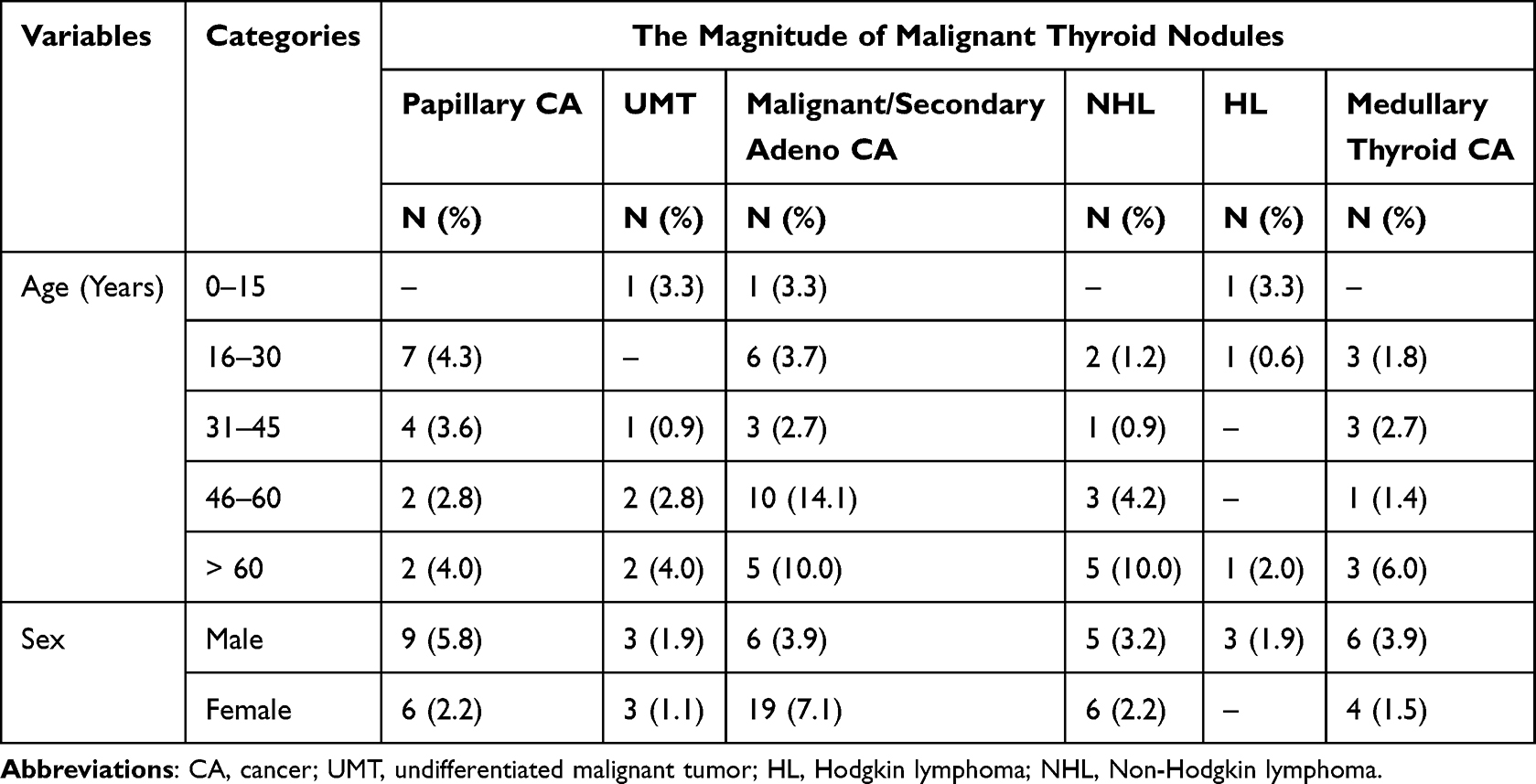 |
Table 3 Magnitude of Malignant Thyroid Nodules Among Study Participants in Northeast Ethiopia from April 2021 to March 2022 (n=424) |
Association of Socio-Demographic and Clinical Variables with Benign Thyroid Nodules Among Study Participants
In the current study, multivariate logistic regression showed that age categories between 16 and 30 years (AOR: 0.363, 95% CI, 0.183–0.717, P = 0.004), being male (AOR: 1.618, 95% CI, 1.053–2.486, P = 0.028), solitary types of the nodule (appearance of nodule) (AOR = 0.236, 95% CI, 0.134–0.418, P = 0.000) and multinodular types (AOR = 0.279, 95% CI, 0.144–0.540, P = 0.000) were significantly associated with benign thyroid tumor in study participants (Table 4).
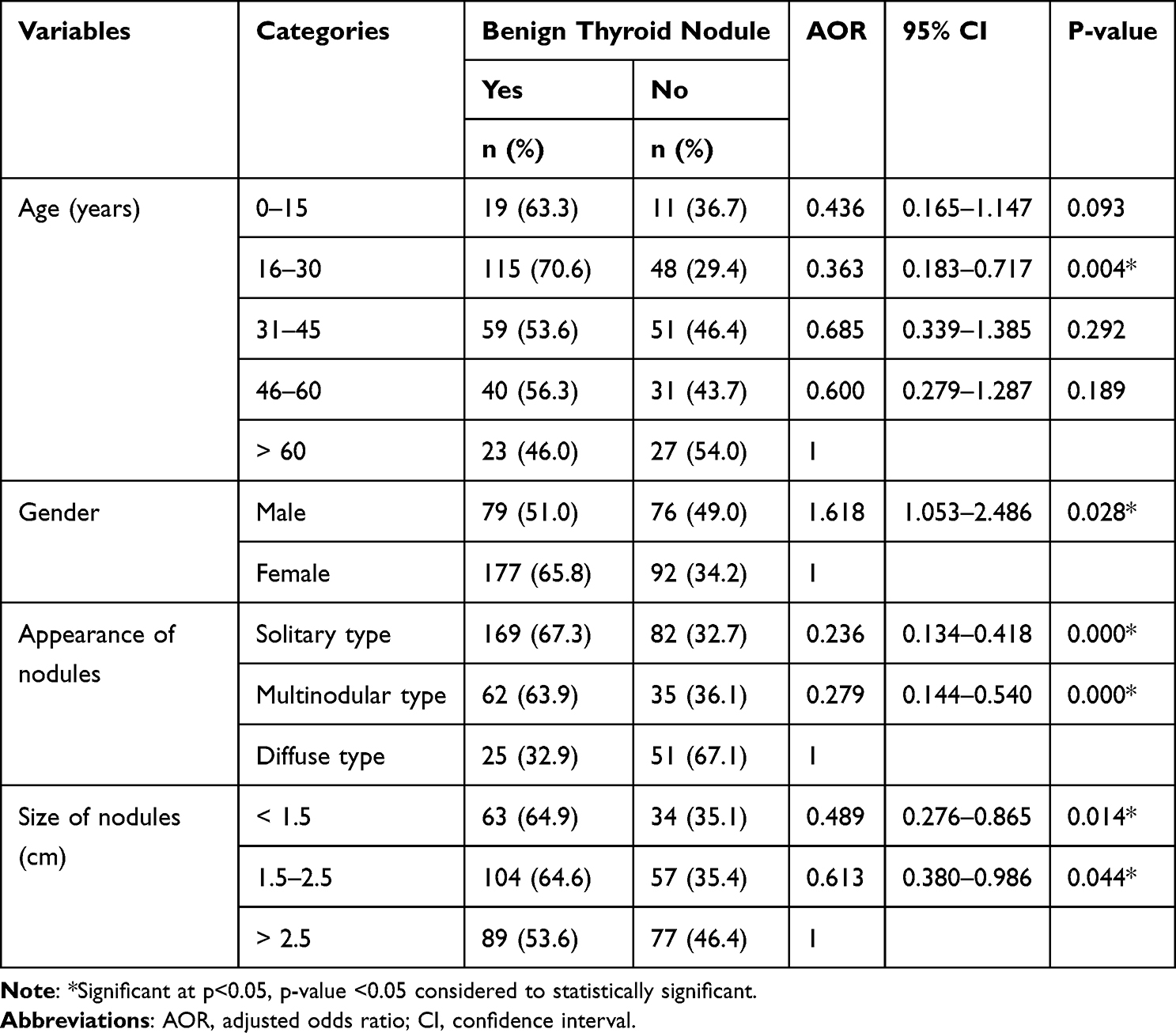 |
Table 4 Association of Socio-Demographic and Clinical Variables with Benign Thyroid Nodules Among Study Participants in Northeast Ethiopia from April 2021 to March 2022 (n=424) |
Association of Socio-Demographic and Clinical Variables with Malignant Thyroid Nodules Among Study Participants
In the current study, multivariate logistic regression showed that age categories between 0 and 15 years (AOR: 5.669, 95% CI, 1.460–22.010, P = 0.012), age categories between 16 and 30 years (AOR: 4.137, 95% CI, 1.909–8.965, P = 0.000), age categories between 31 and 60 (AOR: 4.892, 95% CI, 2.067–11.582, P = 0.000) and nodule size >2.5cm (AOR = 2.312, 95% CI, 1.038–5.151, P = 0.040) were significantly associated with malignant thyroid tumors (Table 5).
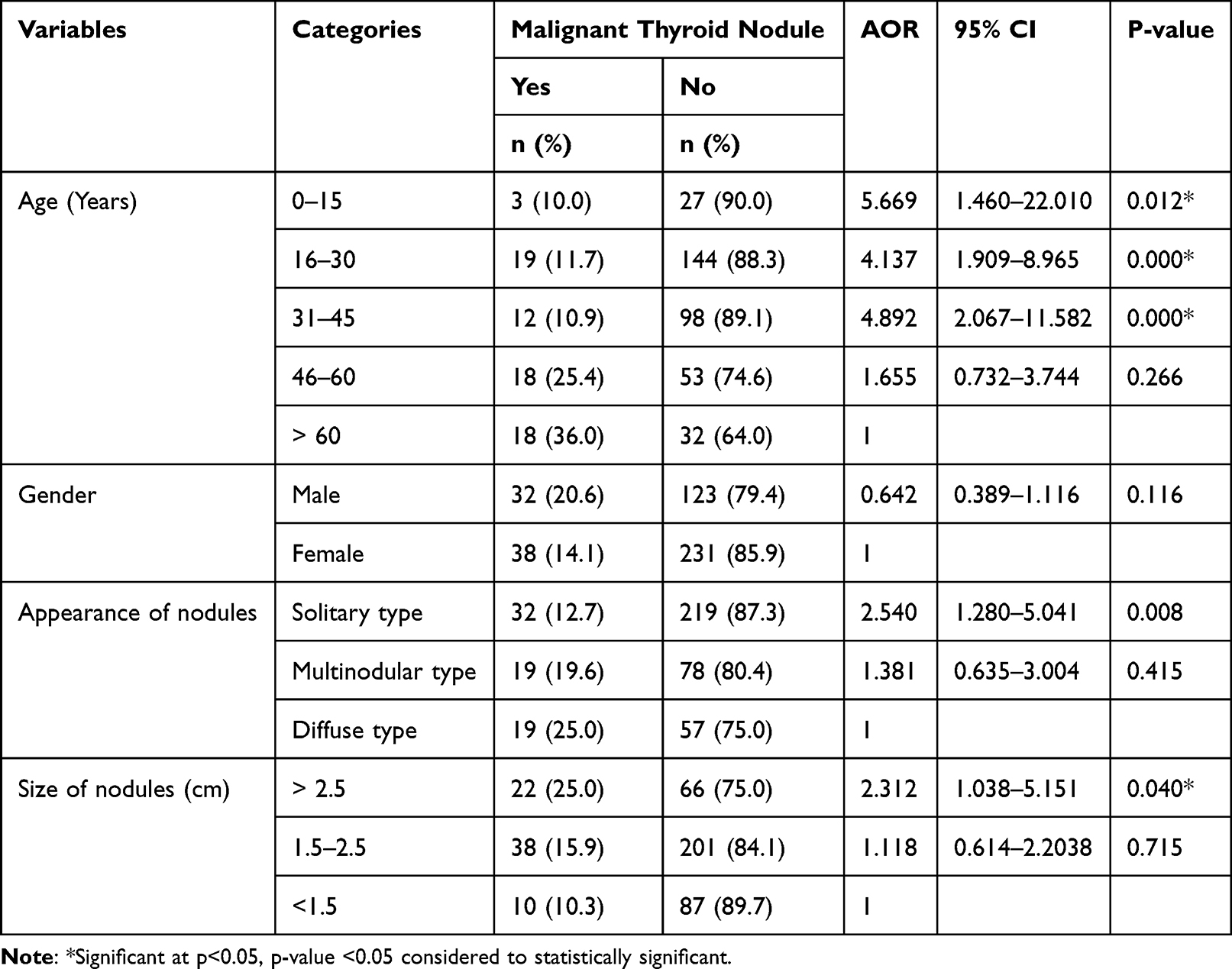 |
Table 5 Association of Socio-Demographic and Clinical Variables with Malignant Thyroid Nodules Among Study Participants in Northeast Ethiopia from April 2021 to March 2022 (n=424) |
Discussion
Recently, fine needle aspiration cytology has been supplemented with other tests for pre-operative evaluation of thyroid nodules. It has now routinely conducted procedures for increasing numbers of patients for the detection of thyroid cancers at earlier stages resulting in better outcomes for patients due to its simplicity, low cost, and absence of major complications led.19 Even though FNAC has its own limitations, the American thyroid association and national comprehensive cancer network recommended that FNAC should be used as the initial diagnostic test because of its superior diagnostic reliability and cost-effectiveness before both thyroid scintigraphy and ultrasonography.20
In the current study, the overall magnitude of benign thyroid nodules was 60.4% (256/424) in study participants. The prevalence of benign thyroid nodules diagnosed was; 32.5% of benign adenomatoid goiter, 9.9% of chronic suppurative lesion, 9.7% of TB lymphadenitis, 5.7% of reactive lymphoid hyperplasia, 1.9% of sub-acute granulomatous thyroiditis and 0.7% of Hashimoto’s thyroiditis respectively. In the current study, a higher magnitude of benign nodules was found in female study participants with a prevalence of 69.1% of the benign cases. Furthermore, benign thyroid nodule cases were dominant in the age categories between 15 and 30 years which accounted for 44.9% of cases. This finding was lower than the study done in Iran (90.3%),21 the United Kingdom (89.5%),22 and the USA (89.7%).23 On the other hand, the current finding was higher compared to the findings reported in China (52.05%) which showed about 32.1% of study participants were diagnosed with a nodular goiter, 13% had adenoma, and 4.5% had Hashimoto thyroiditis24 and (55.3%).25 The possible reasons for this difference might be the variations in sample size, study population, geographical location, and socio-demographic pattern.
In this study, the magnitude of AUS/FLUS (Bethesda category III) was 3.54%. The current finding was similar to the finding reported in Turkey (4.2%)26 and South Korea (5.2%)27 but lower than the finding reported in Greece (29.5%)18 and China (8.2%).28 On the other hand, the magnitude of FN/SFN (Bethesda category IV) was 1.42%. This finding was lower than the result found in Turkey 6.8% and 13.9% respectively.26,29 In this study, the overall magnitude of malignant thyroid nodule cases was 16.5% (70/424) among study participants. In the current study, a higher magnitude of malignant thyroid tumors was found in female study participants accounting for 54.3% of the cases. Moreover, malignant thyroid tumor cases were dominant in the age categories between 15 and 30 years which accounted for 27.1% of cases. This finding was higher than the studies done in Iran (9.7%),21 the United Kingdom (10.5%),22 and the USA (10.3%).30
The prevalence of malignant thyroid tumors diagnosed in the study was, about 5.9% of malignant secondary adenocarcinoma, 3.5% of papillary thyroid carcinoma cases, 2.6% of Non-Hodgkin lymphoma, 2.4% of medullary thyroid carcinoma, 1.4% of high grade undifferentiated malignant thyroid tumor and 0.7% of Hodgkin lymphoma respectively. The current finding was similar to the finding reported in the United Kingdom regarding papillary CA (5.2%)23 and the USA regarding papillary CA (5.8%)22 but higher than the magnitude of medullary CA (0.2%) found in the United Kingdom23 and USA of medullary CA (0.6%) but lower than follicular CA (2.9%).22 Furthermore, a similar finding was reported in China with 0.46% follicular carcinoma and a lower result was found including malignant lymphomas (0.09%) and medullary carcinoma (0.5%) as compared to the present finding.25
On the contrary, higher cases were reported in the USA in which about 86.36% of nodules were papillary thyroid carcinoma and 9.1% were metastatic papillary carcinoma30 and in South Korea, about 85.5% of cases were papillary thyroid carcinoma, and 10.6% cases were follicular thyroid carcinoma but lower finding were found regarding medullary carcinomas (1.5%) and lymphomas.31 Moreover, the current finding was low compared to the result reported in China (47.95%) in which papillary carcinoma accounted for 44.9% of cases, but higher findings were reported compared to medullary carcinoma (0.6%) and undifferentiated carcinoma (0.1%)24 and in South Korea (22.7%).31 On the other hand, the result showed in China also revealed a high prevalence (44.7%) of malignant tumors25 and in South Korea (22.7%).31
In the current study, multivariate logistic regression showed that age categories between 0 and 15 years (AOR: 5.669, 95% CI, 1.460–22.010, P = 0.012), age categories between 16 and 30 years (AOR: 4.137, 95% CI, 1.909–8.965, P = 0.000), age categories between 31 and 60 (AOR: 4.892, 95% CI, 2.067–11.582, P = 0.000) and nodule size >2.5cm (AOR = 2.312, 95% CI, 1.038–5.151, P = 0.040) were significantly associated with malignant thyroid tumors. The present finding was opposite to the finding reported from Italy indicating that being younger age (odds ratio (OR) =0.97, confidence interval (CI) 0.964–0.974; P< 0.0001) was significantly associated and independent risk predictor of malignant thyroid tumors.32 Moreover, although thyroid nodules in pediatric patients are less common than in adults and typically manifest as an asymptomatic neck mass, the identification of a nodule is clinically important due to its increased malignant potential in the pediatric population.33 Thyroid nodules are relatively common in the adult population occurring in 19–68% of the population but are rarely malignant.34,35 Thyroid nodules are less common in children and adolescents and occur in 1–3% of the population but more than a quarter of thyroid nodules that occurred in pediatric patients are malignant.34,36
Moreover, regarding the size of nodule discordant finding was obtained in the USA37 and India38 which showed that larger size nodules were less likely to be malignant tumors whereas concurrent result reported in the USA revealed that increasing nodule size could be highly associated with malignant tumors39 and another finding in USA also showed that nodule size >3.5 cm (odds ratio, 5.8 (95% CI, 1.5–22.5); P = 0.01) was associated with thyroid cancer.40 On the other hand, other findings showed that the magnitude of papillary thyroid carcinoma was nearly equal in the largest (>5cm) and the smallest (≤1 cm) thyroid nodules in white women.41
Limitations
This study did not include other laboratory tests such as thyroid function tests and the authors did not perform biopsy/cell block preparations for histological tests due to the absence of tissue sectioning materials.
Conclusion
The overall prevalence of benign (Bethesda category II) and malignant (Bethesda category VI) tumors was 60.4% and 16.5% respectively. The magnitude of AUS/FLUS (Bethesda category III) and FN/SFN (Bethesda category IV) were 3.54%, and 1.42% respectively. Generally, the magnitude of malignant thyroid tumors diagnosed was 5.9% of malignant secondary adenocarcinoma, 3.5% of papillary thyroid carcinoma cases, 2.6% of Non-Hodgkin lymphoma, 2.4% of medullary thyroid carcinoma, 1.4% of an undifferentiated malignant thyroid tumor and 0.7% of Hodgkin lymphoma respectively. The study found that the prevalence of benign tumors diagnosed was; 32.5% of benign adenomatoid goiter, 9.9% of a chronic suppurative lesion, 5.7% of reactive lymphoid hyperplasia, 1.9% of sub-acute granulomatous thyroiditis and 0.7% of Hashimoto’s thyroiditis respectively. Therefore, fine needle aspiration cytology examination combined with ultrasound imaging devices has a crucial role in the diagnosis and management of benign and malignant thyroid nodules.
Abbreviations
AOR, adjusted odds ratio; AUS, Atypia of Undetermined Significance; CA, cancer; CI, confidence interval; FNAC, fine-needle aspiration cytology examination; HL, Hodgkin lymphoma; NHL, Non-Hodgkin Lymphoma; SD, standard deviation; SOPs, standard operating procedures; TB, tuberculosis; TC, thyroid cancer; UMT, Undifferentiated Malignant Tumor.
Data Sharing Statement
The authors confirmed that all the data for this manuscript are available; if someone wants to request the data they can contact the corresponding author.
Ethics and Consent Statement
Before data collection started, ethical approval was obtained from the Research and Ethics Review Committee at the College of Medicine and Health Sciences, Wollo University. A support letter was secured from Dessie zonal health office and a permission letter was obtained from the diagnostic medical laboratory manager. Written informed consent was taken from each adult study participant. Additionally, written informed consents from guardians or parents of each study participant were obtained for those study participants whose ages were less than 18 years old in accordance with the Declaration of Helsinki. Moreover, the study was conducted in accordance with the declaration of Helsinki. Finally, all abnormal pathological findings were reported and linked to their respective physicians for better management options.
Acknowledgments
We authors like to give heartwarming thanks to those study participants and data collectors who participated during the study. Additionally, we would also give our heartfelt thanks to all who support and stood by our side during the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study did not receive any official funding.
Disclosure
We declare that we do not have any conflicts of interest related to this work or any activities about this research work.
References
1. Mulita F, Anjum F. Thyroid adenoma. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2022. Available from http://www.ncbi.nlm.nih.gov/books/NBK56225.
2. Carling T, Udelsman R. Thyroid cancer. Annu Rev Med. 2014;65(1):125–137. doi:10.1146/annurev-med-061512-105739
3. Bailey S, Wallwork B. Differentiating between benign and malignant thyroid nodules: an evidence-based approach in general practice. Aust J Gen Pract. 2018;47(11):770–774. doi:10.31128/AJGP-03-18-4518
4. Zhang Z, Reiding KR, Wu J, Li Z, Xu X. Distinguishing benign and malignant thyroid nodules and identifying lymph node metastasis in papillary thyroid cancer by plasma N-glycomics. Front Endocrinol. 2021;12:692910. doi:10.3389/fendo.2021.692910
5. Choi YJ, Jung I, Min SJ, et al. Thyroid nodule with benign cytology: is clinical follow-up enough? PLoS One. 2013;8(5):e63834. doi:10.1371/journal.pone.0063834
6. Kim M. Study of natural history of benign thyroid nodules shows only rare progression to cancer. Oncology Times. 2015;37(10):78–79. doi:10.1097/01.COT.0000466408.71686.15
7. Muhammad H, Santhanam P, Russell JO, Kuo JH. RFA and benign thyroid nodules: review of the current literature. Laryngosc Investig Otolaryngol. 2021;6(1):155–165. doi:10.1002/lio2.517
8. Takano T. Natural history of thyroid cancer. Endocr J. 2017;64(3):237–244. doi:10.1507/endocrj.EJ17-0026
9. Khosravi MH, Kouhi A, Saeedi M, Bagherihagh A, Amirzade-Iranaq MH. Thyroid cancers: considerations, classifications, and managements. In: Akarslan Z, editor. Diagnosis and Management of Head and Neck Cancer. InTech; 2017. doi:10.5772/intechopen.70128
10. Buffet C, Groussin L. Molecular perspectives in differentiated thyroid cancer. Annales D’ Endocrinologie. 2015;76(1):1S8–15. doi:10.1016/S0003-4266(16)30009-9
11. Prete A, Borges de Souza P, Censi S, Muzza M, Nucci N, Sponziello M. Update on fundamental mechanisms of thyroid cancer. Front Endocrinol. 2020;11:102. doi:10.3389/fendo.2020.00102
12. Sosa JA, Hanna JW, Robinson KA, Lanman RB. Increases in thyroid nodule fine-needle aspirations, operations, and diagnoses of thyroid cancer in the United States. Surgery. 2013;154(6):1420–1427. doi:10.1016/j.surg.2013.07.006
13. Katoh H, Yamashita K, Enomoto T, Watanabe M. Classification and general considerations of thyroid cancer. Ann Clin Pathol. 2015;3(1):1045.
14. Fagin JA, Wells SA. Biologic and clinical perspectives on thyroid cancer. N Engl J Med. 2016;375(11):1054–1067. doi:10.1056/NEJMra1501993
15. Crippa S, Cibas ES, Mazzucchelli L, Ali SZ. The Bethesda system for reporting thyroid fine-needle aspiration specimens. Am J Clin Pathol. 2010;134(2):343–345. doi:10.1309/AJCPXM9WIRQ8JZBJ
16. Cibas ES, Ali SZ. The Bethesda system for reporting thyroid cytopathology. Thyroid. 2009;19(11):1159–1165. doi:10.1089/thy.2009.0274
17. Kafle N, Koirala B, Kafle S, Singh M, Sinha A. Cytopathological evaluation of thyroid lesions based on Bethesda system in patients attending Birat Medical College and Teaching Hospital. Nep Med Coll J. 2020;22(4):260–265. doi:10.3126/nmcj.v22i4.34194
18. Mulita F, Plachouri MK, Liolis E, Vailas M, Panagopoulos K, Maroulis I. Patient outcomes following surgical management of thyroid nodules classified as Bethesda category III (AUS/FLUS). Endokrynol Pol. 2021;72(2):143–144. doi:10.5603/EP.a2021.0018
19. Masereka R, Okeny PK, Fualal JO, Wamala D. Diagnostic accuracy of fine needle aspiration cytology in patients undergoing thyroidectomy in Uganda: tertiary hospital experience. Afr Healt Sci. 2017;16(4):1143. doi:10.4314/ahs.v16i4.32
20. Bible KC, Kebebew E, Brierley J, et al. American Thyroid Association anaplastic thyroid cancer guidelines task force. Thyroid. 2021;31(3):337–386. doi:10.1089/thy.2020.0944
21. Rahimi M, Farshchian N, Rezaee E, Shahebrahimi K, Madani H. To differentiate benign from malignant thyroid nodule comparison of sonography with FNAC findings. Pak J Med Sci. 2013;29(1):77–80. doi:10.12669/pjms.291.2595
22. Lingam RK, Qarib MH, Tolley NS. Evaluating thyroid nodules: predicting and selecting malignant nodules for fine-needle aspiration (FNA) cytology. Insights Imaging. 2013;4(5)::617–24. doi:10.1007/s13244-013-0256-6
23. Middleton WD, Teefey SA, Tessler FN, et al. Analysis of malignant thyroid nodules that do not meet ACR TI-RADS criteria for fine-needle aspiration. Am J Roentgenol. 2021;216(2):471–478. doi:10.2214/AJR.20.23123
24. Shen Y, Liu M, He J, et al. Comparison of different risk-stratification systems for the diagnosis of benign and malignant thyroid nodules. Front Oncol. 2019;9:378. doi:10.3389/fonc.2019.00378
25. Yan H-X, Pang P, Wang F-L. Dynamic profile of differentiated thyroid cancer in male and female patients with thyroidectomy during 2000–2013 in China: a retrospective study. Sci Rep. 2017;7(1):15832. doi:10.1038/s41598-017-14963-z
26. Yaprak Bayrak B, Eruyar AT. Malignancy rates for Bethesda III and IV thyroid nodules: a retrospective study of the correlation between fine-needle aspiration cytology and histopathology. BMC Endocr Disord. 2020;20(1):48. doi:10.1186/s12902-020-0530-9
27. Yoo WS, Ahn HY, Ahn HS, et al. Malignancy rate of Bethesda category III thyroid nodules according to ultrasound risk stratification system and cytological subtype. Medicine. 2020;99(2):e18780. doi:10.1097/MD.0000000000018780
28. Zhao H, Guo H, Zhao L, et al. Subclassification of the Bethesda Category III (AUS/FLUS): a study of thyroid FNA cytology based on ThinPrep slides from the National Cancer Center in China. Cancer Cytopathol. 2021;129(8):642–648. doi:10.1002/cncy.22417
29. Ozdemi A, Uyan M, Kalcan S, Çolakoğlu MK, Pergel A. Malignancy rates and risk factors in Bethesda category IV thyroid nodules: is lobectomy enough in an endemic region? J Exp Clin Med. 2022;39(3):749–754. doi:10.52142/omujecm.39.3.30
30. Gregory A, Bayat M, Kumar V, et al. Differentiation of benign and malignant thyroid nodules by using comb-push ultrasound shear elastography. Acad Radiol. 2018;25(11):1388–1397. doi:10.1016/j.acra.2018.02.025
31. Hong MJ, Na DG, Baek JH, Sung JY, Kim JH. Impact of nodule size on malignancy risk differs according to the ultrasonography pattern of thyroid nodules. Korean J Radiol. 2018;19(3):534–541. doi:10.3348/kjr.2018.19.3.534
32. Rago T, Fiore E, Scutari M, et al. Male sex, single nodularity, and young age are associated with the risk of finding a papillary thyroid cancer on fine-needle aspiration cytology in a large series of patients with nodular thyroid disease. Eur J Endocrinol. 2010;162(4):763–770. doi:10.1530/EJE-09-0895
33. Paulson VA, Rudzinski ER, Hawkins DS. Thyroid cancer in the pediatric population. Genes. 2019;10(9):723. doi:10.3390/genes10090723
34. Lim-Dunham JE, Erdem Toslak I, Alsabban K, et al. Ultrasound risk stratification for malignancy using the 2015 American Thyroid Association Management guidelines for children with thyroid nodules and differentiated thyroid cancer. Pediatr Radiol. 2017;47(4):429–436. doi:10.1007/s00247-017-3780-6
35. Haugen BR, Alexander EK, Bible KC, et al. 2015 American Thyroid Association Management guidelines for adult patients with thyroid nodules and differentiated thyroid cancer: the American Thyroid Association Guidelines Task Force on thyroid nodules and differentiated thyroid cancer. Thyroid. 2016;26(1):1–133. doi:10.1089/thy.2015.0020
36. Creo A, Alahdab F, Al Nofal A, Thomas K, Kolbe A, Pittock ST. Ultrasonography and the American Thyroid Association ultrasound-based risk stratification tool: utility in pediatric and adolescent thyroid nodules. Horm Res Paediatr. 2018;90(2):93–101. doi:10.1159/000490468
37. Porterfield JR, Grant CS, Dean DS, et al. Reliability of benign fine needle aspiration cytology of large thyroid nodules. Surgery. 2008;144(6):963–969. doi:10.1016/j.surg.2008.09.006
38. Pinchot SN, Al-Wagih H, Schaefer S, Sippel R, Chen H. Accuracy of fine-needle aspiration biopsy for predicting neoplasm or carcinoma in thyroid nodules 4 cm or larger. Arch Surg. 2009;144(7):649–665. doi:10.1001/archsurg.2009.116
39. McCoy KL, Jabbour N, Ogilvie JB, Ohori NP, Carty SE, Yim JH. The incidence of cancer and rate of false-negative cytology in thyroid nodules greater than or equal to 4 cm in size. Surgery. 2007;142(6):837–844.e3. doi:10.1016/j.surg.2007.08.012
40. Fornwalt B, Melachuri M, Kubina M, McDaniel J, Jeyakumar A. Pediatric thyroid nodules: ultrasound characteristics as indicators of malignancy. OTO Open. 2022;6(1):24 739 74X 2110737. doi:10.1177/2473974X211073702
41. Lim H, Devesa SS, Sosa JA, Check D, Kitahara CM. Trends in thyroid cancer incidence and mortality in the United States, 1974–2013. JAMA. 2017;317(13):1338. doi:10.1001/jama.2017.2719
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Pathological Features of Ovarian Tumors, Diagnosed at a Tertiary Care Hospital in Afghanistan: A Cross-sectional Study
Ibrahimkhil AS, Malakzai HA, Haidary AM, Hussaini N, Abdul-Ghafar J
Cancer Management and Research 2022, 14:3325-3333
Published Date: 28 November 2022
Diagnosis of Chest Wall Tuberculosis Using Fine Needle Aspiration: A Single-Center Experience
Li W, Sha W
Infection and Drug Resistance 2023, 16:2281-2290
Published Date: 18 April 2023
Treatment of Cystic-Solid Thyroid Nodules with Ultrasound-Guided Radiofrequency Ablation and Enhancement of Thyroid Function
Lou Q, Zhu YF, Ye ML
Journal of Multidisciplinary Healthcare 2023, 16:2773-2779
Published Date: 20 September 2023
Diagnostic Values of Solid Features in Different Sizes Thyroid Nodules Based on C-TIRADS
Huang H, Li HJ, Gao Q, Zhu MJ, Li WM
Open Access Surgery 2024, 17:113-121
Published Date: 19 August 2024
Histopathological Analysis of Thyroid Nodules with Taller-Than-Wide Shape in Adults
Yang XY, Huang LF, Han YJ, Cen XX, Tao ZX
International Journal of General Medicine 2024, 17:5123-5131
Published Date: 7 November 2024