Back to Journals » Infection and Drug Resistance » Volume 16
Diagnosis of Chest Wall Tuberculosis Using Fine Needle Aspiration: A Single-Center Experience
Received 15 January 2023
Accepted for publication 29 March 2023
Published 18 April 2023 Volume 2023:16 Pages 2281—2290
DOI https://doi.org/10.2147/IDR.S404804
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Wenting Li, Wei Sha
Department of Tuberculosis, Shanghai Pulmonary Hospital, Tongji University, Shanghai, People’s Republic of China
Correspondence: Wei Sha, Shanghai Pulmonary Hospital, Tongji University, Number 507 Zhengmin Road, Shanghai, 200433, People’s Republic of China, Tel +86 21 6511 5006 (ext 2013), Fax +86 2155662767, Email [email protected]
Introduction: Minimally invasive diagnosis of chest wall tuberculosis remains a challenge. Fine needle aspiration (FNA) is a simple and safe method of sampling. However, previous studies have shown that conventional tuberculosis tests had poor diagnostic performance in the needle aspirates. With the popularization of molecular detection application, the value of FNA in the diagnosis of chest wall tuberculosis needs to be reevaluated.
Methods: We retrospectively studied patients with suspected chest wall tuberculosis at admission who underwent FNA for diagnosis and reported the diagnostic efficacy of acid-fast bacilli smear, mycobacterial culture, cytology and Xpert MTB/RIF (GeneXpert) when testing FNA specimens. A composite reference standard (CRS) was used as the diagnostic gold standard for this study.
Results: Among 89 included FNA specimens, acid-fast bacilli smear, mycobacterial culture, and GeneXpert were positive in 15 (16.85%), 23 (25.8%), and 61 (68.5%), respectively. Thirty-nine (43.8%) had cytologic features suggestive of tuberculosis. According to CRS, 75 (84.3%) cases were categorized as chest wall tuberculosis, 14 (15.7%) were not diagnosed with tuberculosis. Using CRS as the gold standard, acid-fast bacilli smear, mycobacterial culture, cytology and GeneXpert exhibited sensitivity of 20%, 30.7%, 52% and 81.3%, respectively. Specificity in these four tests was found to be 100%. Sensitivity of GeneXpert was significantly higher than that of smear, culture and cytology, X2=66.3, p< 0.001.
Conclusion: GeneXpert achieved higher sensitivity as compared to cytology and conventional TB tests in the chest wall FNA specimens. The implementation of GeneXpert may increase the diagnostic efficacy of FNA in the diagnosis of chest wall TB.
Keywords: chest wall tuberculosis, fine needle aspiration, Xpert MTB/RIF, cytology, culture
Introduction
Globally, tuberculosis (TB) remains a significant public health concern.1 Mycobacterium tuberculosis (MTB) primarily infects the respiratory system but also affects extra-pulmonary organs via the blood or lymphatic system.2,3 Chest wall TB is a rare form of extra-pulmonary TB. It causes cheese-like necrosis, liquefaction, abscesses in the soft tissue of the chest wall, involving the ribs, costal cartilage, and sternum. Chest wall TB occurs by the following mechanisms: direct spread from pleural or pulmonary tuberculosis, haematogenous dissemination, extension from lymphangitis. Clinically, patients usually present with an enlarging, and occasionally painful mass on the chest wall.4–6 Chest wall TB has no specific clinical manifestations and is often misdiagnosed as malignant disease or other benign diseases. Incorrect diagnosis can lead to delayed treatment or unnecessary empirical treatment. Few studies have been investigated on the diagnostic method of chest wall TB.
With the development of imaging techniques, the location and extent of chest wall lesions can be more clearly understood. However, a definite diagnosis depends on clinical and imaging findings combined with pathological and bacteriological results. Surgical or core needle biopsy allows obtaining adequate tissue for histologic analysis, but requires high cost and complex technique.
Fine needle aspiration (FNA) is the most cost-effective and least invasive biopsy method. It enables to obtain a few cell clusters and tissue fragments for cytologic and bacteriological analysis. The outer diameter of a fine needle is less than 0.9mm, causing minor pain and trauma.
FNA is limited by a small sample volume. The paucibacillary nature leads to poor sensitivity of the conventional laboratory tests. Moreover, FNA does not allow histologic examination. Results of previous studies shown that conventional TB tests (acid-fast bacillus smear and culture) had low diagnostic sensitivity in the needle aspirates of chest wall lesion.7–9
In line with the limitations of FNA, more efficient detection methods are needed. With the development of molecular detection, such as Xpert MTB/RIF (GeneXpert), the detection rate of MTB in non-respiratory specimens has been improved.10 The value of FNA in the diagnosis of chest wall TB needs to be reevaluated with the popularization of molecular detection application.
The aim of this study was to report our experience of FNA in the diagnosis of chest wall TB and to evaluate the diagnostic efficacy of conventional TB tests (acid-fast bacillus smear and mycobacterial culture), cytologic examination and GeneXpert assay when testing FNA specimens.
Materials and Methods
Study Patients
This study was carried out at the Department of Tuberculosis in Shanghai Pulmonary Hospital. We reviewed the medical records of the patients clinically suspected of having chest wall TB at admission between December 2018 and June 2022. The main clinical presentations included mass or local swelling on the chest wall, with or without constitutional symptoms of fever, anorexia, and weight loss. Patients were included in this study if they underwent FNA for diagnosis, and the FNA specimens were sent for TB tests (acid-fast bacillus smear, mycobacterial culture and GeneXpert) and cytologic examination. The patients whose final diagnosis was not definite (cases who lacked specific evidence to support any diagnosis), those with FNA specimens less than 1mL, and those who were taking anti-tuberculosis treatment at the time of sampling were excluded from this study.
Sample Collection and Laboratory Methods
Prior to the FNA procedure, the patients underwent colour Doppler ultrasound (General Company, GE E9 colour Doppler ultrasound diagnostic instrument, Boston, Mass, USA) examination for detection of the chest wall lesion, with puncture point and puncture path initially determined. The puncture point was fixed with the left hand after local infiltration anesthesia with 2% lidocaine. The puncture needle in an outer diameter of 0.8mm with a 20-mL syringe was then inserted through the proposed puncture point and puncture path. Once the needle had penetrated into the ultrasound-guided depth, the assistant drew 20 mL of negative pressure from the syringe and maintained it. If the aspirate was thick, a 20-mL negative pressure was repeatedly aspirated for several times until there was enough specimen in the syringe. The sample volume was no less than 1mL. Specimen appearance was recorded as blood stained, caseous or purulent.
The first few drops of the aspirates were used for cytology smear and acid-fast bacillus (AFB) smear, with two glass slides each prepared. The smear on the glass slide was about 15mm in diameter.
Ziehl-Neelsen stain was used for AFB smear. The smears were stained with 3% carbol fuchsin for 15 minutes, heated for 5 minutes and then cooled in room temperature. The slides were then washed with tap water, decolorized with 0.5% acid alcohol and washed with tap water again. Slides were then stained with methylene blue dye for 5 minutes and dried at room temperature. The stained smears were examined for the presence of AFB using a light microscope and oil immersion.
Hematoxylin-eosin stain was used for cytologic analysis. Cell nucleus was stained with hematoxylin solution for 3–8 minutes. Then, cytoplasm was decolorized with 1% acid alcohol and cell nucleus was returned to blue with 0.6% ammonia water. After washing the alkaline solution with tap water, cytoplasm was stained with eosin solution for 1–3 minutes. The air-dried stained smears were analyzed by a pathologist. The cytologic criteria for diagnosis of possible TB was defined as epithelioid cell granulomas with or without caseous necrosis.11
The residue sample in the needle and syringe was rinsed into 1mL of normal saline and transferred to another sterile container. Half of this was sent for GeneXpert assay (Cepheid, Sunnyvale, CA, USA). The sample was mixed with the Xpert sample reagent in a 1:2 ratio. The mixture was vortexed for 15–30 seconds and incubated at room temperature for 15 minutes. Next, 2 mL of the reagent sample mix was transferred to an Xpert cartridge. The cartridge was loaded onto Xpert machine, and real-time polymerase-chain reaction processed. Results were reported as positive or negative for MTB. Rifampicin resistance results were reported as susceptible, resistant or indeterminate. The remaining sample in the container was sent for mycobacterial culture. It was decontaminated with the N-acetyl-L-cysteine-NaOH method for 15 minutes. After neutralization with phosphate buffer solution, the decontaminated specimen was centrifugated at 3000×g for 15 minutes. Next, 0.5 mL of suspension was inoculated into a Mycobacteria growth indicator tube (MGIT) for liquid cultivation. The growth of MTB was detected by a Bactec 960 instrument (Becton Dickinson, BACTEC MGIT, Cockeysville, MD, USA).
Operational Definition
A composite reference standard (CRS) based on WHO guidelines12 and Chinese TB diagnostic criteria13 was used as the diagnostic gold standard for this study. According to CRS, patients were diagnosed with chest wall TB if fulfilling one or combination of the following conditions: (1) patients with positive culture results for MTB from their chest wall specimens. (2) histology results confirmed the presence of epithelioid cell granulomas with caseous necrosis. (3) AFB smear and/or GeneXpert results from their chest wall specimens exhibited positive, or cytology results were suggestive of TB, or clinical and imaging findings were consistent with TB, and the patient responded well to anti-tuberculosis treatment. Effective anti-tuberculosis treatment was defined as the maximum diameter of chest wall lesion reduced by more than 1/3 after 1–3 months of treatment. Non-tuberculosis (Non-TB) was defined as not fulfilling the previous three criteria and some other diagnosis was established.
Statistical Method
Statistical analysis was conducted using the SPSS 17.0 software package. To evaluate the diagnostic performance of TB tests (AFB smear, mycobacterial culture and GeneXpert) and cytology against the CRS, the sensitivity, specificity, positive predictive values (PPV), negative predictive values (NPV), and the area under the Receiver Operator Characteristic (ROC) curve (AUC) were calculated. The frequency differences were compared using a chi-square test. The differences of AUC were compared using a z-test. In all analyses, a p-value <0.05 was considered statistically significant.
Results
Clinical Characteristics of the Patients
In total, 142 patients with clinical suspicion of chest wall tuberculosis were enrolled. Fifty-three patients were excluded based on the exclusion criteria. Finally, 89 FNA specimens from 89 patients were included in this retrospective analysis. The patients’ clinical characteristics are shown in Table 1. There were 52 men and 37 women. The patients ranged in age from 17 to 93 years (a mean of 43.8±1.9 years). All patients were HIV-negative. The main complaint was palpable mass in 84 (94.4%) patients and local swelling in 5 (5.6%) patients. The chest wall mass ruptured and formed sinus tract in 7 (7.9%) patients. Fifty (56.2%) patients complained of local chest pain and tenderness. The maximum diameter of the chest wall lesion ranged from 3 cm to 11 cm (a mean of 5.2 ± 0.2 cm). Chest computed tomography (CT) was performed before FNA in all 89 patients. On CT scan, the lesion formed a mass confined to the chest wall in 60 (67.4%) patients, breached through the intercostal muscle forming dumbbell-shaped lesion in 29 (32.6%) patients.
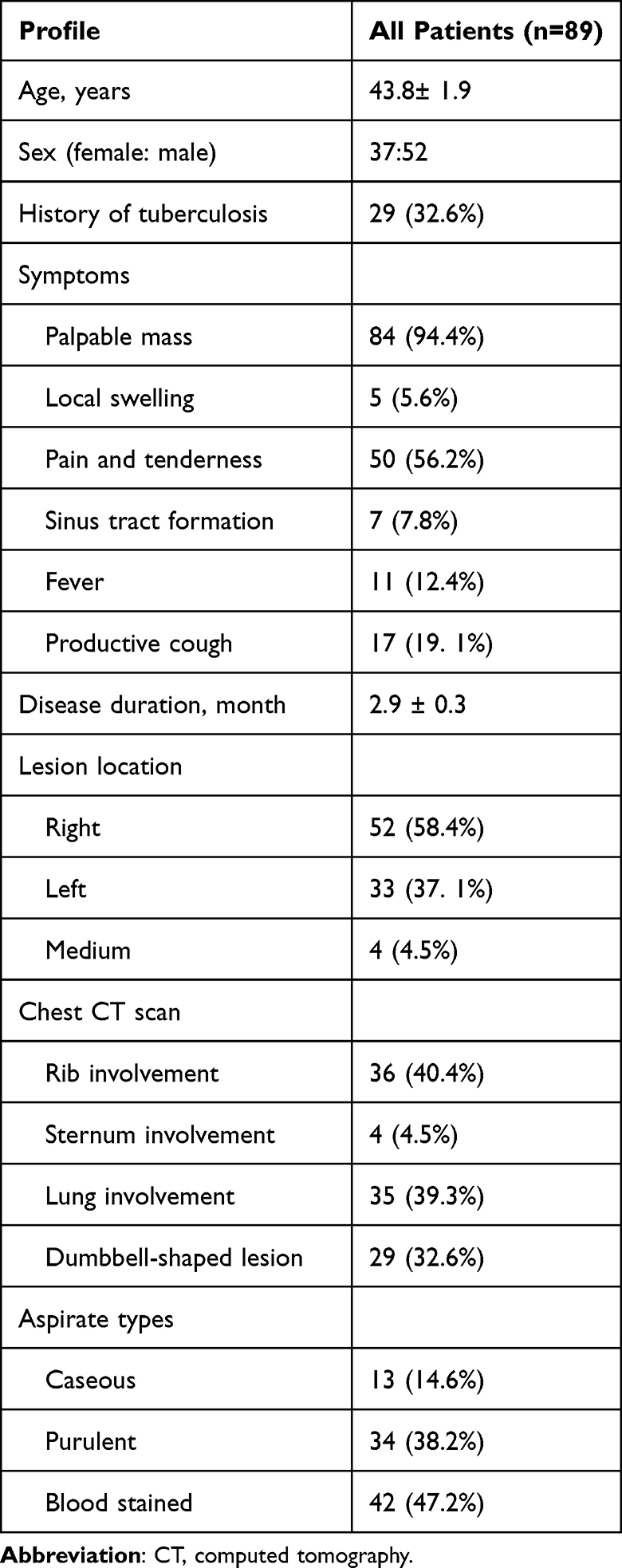 |
Table 1 Clinical Characteristics of the Included Patients |
Laboratory Findings of the FNA Specimens
Among the 89 FNA specimens, the appearance of aspirates was described as blood stained in 42 (47.2%), caseous in 13 (14.6%) and purulent in 34 (38.2%). AFB smear was positive in 15 (16.85%) specimens. Culture was positive for MTB in 23 (25.8%) specimens. On GeneXpert assay, 61 (68.5%) were positive for MTB (Table 2, Figure 1). GeneXpert positivity was reported as high for 3 specimens, medium for 13, low for 31, and very low for 14. Rifampicin resistance was detected in 2 specimens. On FNA cytologic analysis, thirty-nine (43.8%) had cytologic features suggestive of TB.
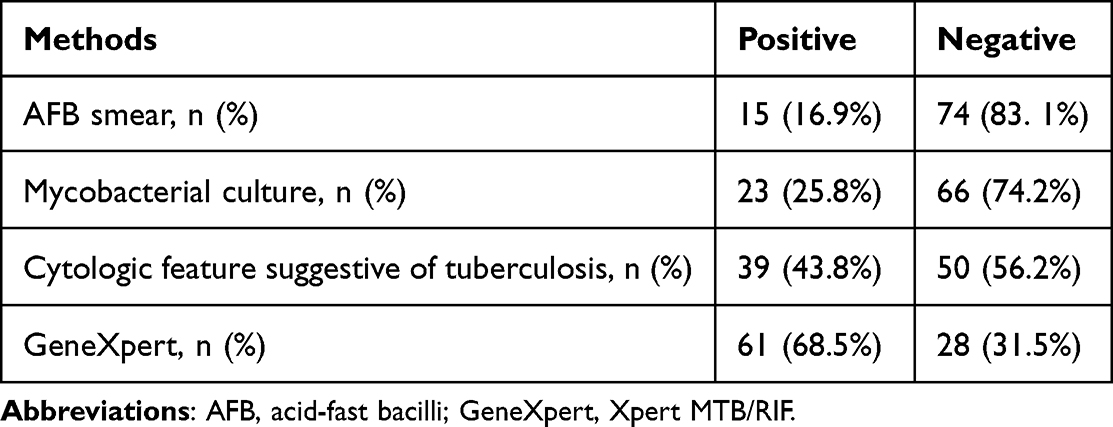 |
Table 2 The Positivity of Different Diagnostic Methods |
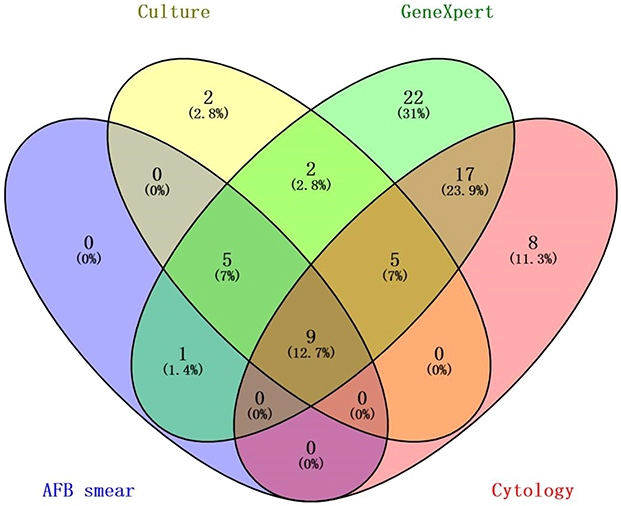 |
Figure 1 Wayne diagrams for the overlap of the positive results in AFB smear, mycobacterial culture, GeneXpert and cytology. |
Diagnostic Performance of AFB Smear, Mycobacterial Culture, Cytology and GeneXpert in the FNA Specimens
According to CRS, 75 cases were categorized as chest wall TB. Forty-one of them underwent chest wall lesion removal surgery 3 to 17 (a mean of 9.6±0.6) weeks after preoperative anti-tuberculosis treatment. Histologic examination of the surgical specimens all confirmed the diagnosis of TB.
Fourteen cases were categorized as non-TB. Nine of the non-TB cases were metastatic malignant tumor confirmed by FNA cytology. Five of the non-TB cases were cytologically suggestive of acute suppurative inflammation, which were eventually confirmed as other bacterial infection (pathogenic bacteria detected included Staphylococcus aureus, Streptococcus hemolyticus and Pseudomonas aeruginosa).
When compared to the CRS, AFB smear, mycobacterial culture, cytology and GeneXpert of the FNA specimens exhibited sensitivity of 20%, 30.7%, 52% and 81.3%, respectively (Table 3). The sensitivity of GeneXpert was significantly higher than that of cytology, culture and AFB smear (X2=66.3, p<0.001). We pairwise compared the sensitivity of these four methods: the cytology sensitivity was significantly higher than that of mycobacterial culture (X2=7.0, p=0.008) and AFB smear (X2 =16.7, p<0.001). The GeneXpert sensitivity was significantly higher than that of cytology (X2 =14.5, p<0.001), mycobacterial culture (X2 = 39.1, p<0.001) and AFB smear (X2 = 56.4, p<0.001). There was no statistical difference in sensitivity between AFB smear and mycobacterial culture. Specificity in these four tests was found to be 100%. AUC of AFB smear, mycobacterial culture, cytology and GeneXpert was 0.600, 0.653, 0.760 and 0.907, respectively (Figure 2). We pairwise compared the AUC of these four methods: the AUC of cytology was significantly higher than that of mycobacterial culture (z = 2.9, p=0.004) and AFB smear (z = 4.5, p<0.0001). The AUC of GeneXpert was significantly higher than that of cytology (z = 3.9, p=0.0001), mycobacterial culture (z = 7.9, p<0.0001) and AFB smear (z = 10.8, p<0.0001). There was no statistical difference in AUC between AFB smear and mycobacterial culture.
 |
Table 3 Diagnostic Accuracy of AFB Smear, Mycobacterial Culture, GeneXpert and Cytology in the FNA Specimens |
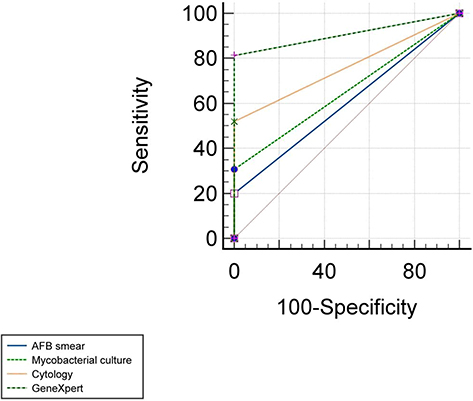 |
Figure 2 Receiver operator characteristic (ROC) curves of AFB smear, mycobacterial culture, GeneXpert and cytology in the diagnosis of chest wall tuberculosis. |
Combination of non-molecular methods (AFB smear+culture+cytology) detected 49 positive cases out of 75 TB cases, with a detection rate of 49/75 (65.3%). Non-molecular methods combined with GeneXpert (AFB smear+culture+cytology+ GeneXpert) detected 71 positive cases, the detection rate was 71/75 (94.6%), which was higher than that of the non-molecular methods combination (X2 = 20.2, p<0.001).
Detection Rate of AFB Smear, Mycobacterial Culture, Cytology and GeneXpert Among Different Types of Aspirates
Among the 75 TB cases, the appearance of FNA specimen was described as blood stained in 33 (44%), caseous in 13 (17.3%) and purulent in 29 (38.7%). The detection rate of AFB smear was 5/33 (15.15%) in the blood stained aspirates, 3/13 (23.1%) in the caseous aspirates and 7/29 (24.1%) in the purulent aspirates. The detection rate of mycobacterial culture was 8/33 (24.2%), 4/13 (30.8%) and 11/29 (37.9%) in the three types of specimens, respectively. The above difference was not statistically significant. The detection rate of GeneXpert was 23/33 (69.7%) in the blood stained aspirates, 10/13 (76.9%) in the caseous aspirates and 28/29 (96.5%) in the purulent aspirates, X2 =7.5, p=0.023. Typical cytologic feature suggestive of TB was observed in 21/33 (63.6%) of the blood stained aspirates, 10/13 (76.9%) of the caseous aspirates and 8/29 (27.6%) of the purulent aspirates, X2 =11.9, p=0.003.
Discussion
Patients with chest wall TB usually present with an enlarging mass on the chest wall. Similar clinical symptoms may also occur with tumors or other bacterial infections. Chest CT is the preferred method for detecting chest wall lesions, and it can specify the location and extent of the lesion. It can also reveal the presence of bone lysis, intrathoracic lymphadenopathy and pleuropulmonary lesions.6,14 However, imaging technique is difficult to establish differential diagnosis due to the lack of specificity. Microbiological and pathological findings remain the “golden standard” for diagnosis.
Surgery plays an important role in the diagnosis and treatment of chest wall TB.7–9,15,16 On one side, surgery can help to remove the chest wall lesion, eliminate the residual cavity and damaged bones. On the other side, intraoperative biopsy can achieve good tissue integrity, thus meeting the requirements of histologic examination.
However, surgical biopsy involves long time, large trauma, complex anesthesia and high cost. Moreover, surgical procedure can easily cause further aggravation of TB infection and even lead to systemic spread. The optimal timing of surgical treatment for chest wall TB is still controversial. At present, most of the data suggested that patients with confirmed or suspected chest wall TB should take 2–3 months of anti-tuberculosis drugs before surgery.7,17,18 In our study, the histology results of surgical specimens from 41 patients who underwent surgical treatment confirmed the diagnosis of TB, but all were obtained 3 to 17 weeks after preoperative anti-TB treatment. Surgical biopsy has the limitation in establishing early diagnosis.
Core needle biopsy (CNB) provides intact tissue fragments to meet the requirement of histologic analysis and is less invasive as compared to surgical biopsy.19 However, CNB requires the expertise of an interventionalist and expensive cost, meaning the method cannot be widely used. In addition, the CNB relies on spring-loaded physical cutting action which can form a temporary biopsy tract between the lesion and body surface. In infectious disease, the pathogenic microorganism in the lesion may be infected along the biopsy tract to form sinus tract.
In comparison with surgical biopsy and CNB, FNA has the advantages of simple technique, low cost and low complication risk. Results of a meta-analysis supported the expanded use of FNA for diagnosis of bone and soft tissue lesions, in light of a sensitivity and specificity comparable to CNB.20 Previous studies have mentioned needle aspiration as a preoperative diagnostic method for diagnosis of chest wall TB, but the diagnostic sensitivity was not ideal. Faure et al7 reported a diagnostic rate of 36.3% with needle aspiration. Sakuraba et al.8 Reported that the positive rate of AFB smear and mycobacterial culture was 62.29% and 42.86%, respectively, in the needle aspirates. Kim et al9 reported 16 cases with chest wall TB, of whom 7 underwent needle aspiration, and only 2 had positive results of AFB smear.
Before the widespread use of molecular detection technology, AFB smear and mycobacterial culture were crucial in diagnosing TB. The AFB smear method is simple, rapid and low cost, but with low sensitivity. The sample must contain between 5000 and 10,000 organisms per milliliter to be visible under a microscope.12,21 And AFB smear cannot distinguish between NTM and MTB. Culture is more sensitive, requiring approximately 100 organisms per milliliter.12,22 But it requires a well-equipped laboratory and several weeks. In our study, the sensitivity of AFB smear and culture in FNA specimens was only 20% and 30.7%, respectively. The small sample volume and the scanty bacilli could be the main factor for low sensitivity.
GeneXpert integrates real-time PCR and specimen processing into a self-contained test unit and detects MTB and rifampin resistance within two hours. After sample loading, the entire assay is fully automated and self-sufficient.23 It is applicable at every level of the healthcare system. A systematic review and meta-analysis by Kohli et al24 revealed that the pooled sensitivity of GeneXpert for tuberculosis varied depending on the type of specimen, ranging from 49.5% in the pleural fluid to 97.9% in bone or joint aspirate. The pooled specificity varied between 87% and 100%. Scott et al25 found that GeneXpert performed better in diagnosing purulent specimens when testing non-respiratory samples. Nowadays, GeneXpert has been recommended by WHO for testing non-respiratory specimens.10 In our study, GeneXpert exerted high sensitivity (81.3%) and specificity (100%) in the FNA specimens. More than 70% of the Xpert-positive samples were scored as “low” and “very low”, suggesting a limited number of bacilli in the FNA specimens.
In this study, the detection rate of non-molecular methods combined with GeneXpert was significantly higher than that of the non-molecular methods combined, which was 94.6% versus 65.3%. This finding demonstrated that integrated use of conventional methods and GeneXpert can improve the efficiency of FNA in diagnosing chest wall TB.
This study showed that GeneXpert performed the lowest detection rate in blood stained specimens. Several compounds in blood have been suggested to be PCR inhibitory.26 Blood stained sputum samples have been reported to reduce the sensitivity of GeneXpert.27 A study conducted by Aninagyei et al showed that the GeneXpert result was unreliable at more than 5% blood contamination of the sample, and absolute PCR inhibition occurred at 20% blood contamination.28 Local bleeding is an inevitable complication during needle puncture, which can interfere with GeneXpert detection.
Though the most reliable criteria for diagnosing TB is bacteriological findings, presence of epithelioid cell granuloma is considered as an evidence of TB in settings with high disease burden. The immune response pattern of MTB is mainly due to delayed type IV hypersensitivity. The macrophages aggregate around the lesions center to form a granuloma. Necrotic material in the central part is caseous necrosis. Previous studies emphasized the importance of intraoperative biopsy pathology, but rarely reported FNA cytology in the diagnosis of chest wall TB. In Faure’s study,7 the cytology’s diagnostic positivity in needle aspirates was only 1/11. In our study, the sensitivity of FNA cytology was 52%, higher than that of AFB smear and culture, lower than that of GeneXpert. The FNA specimens are mainly composed of cell cluster and broken tissues, which may result in the lack of characteristic cellular structures in some samples.
Our study further found that cytologic feature suggestive of TB was least present in the purulent specimens. Suppurative features, although non-specific, may occur in the later pathological process of TB.29 When the macrophage activation is weak, tissue destruction develops. The lesion enlarges further and the surrounding tissue is destroyed. If it continues to deteriorate, the caseous necrosis starts liquefying and contains high bacillary load. Therefore, typical epithelioid cell granuloma is less present in the lesions dominated by liquefaction. This could also explain the highest detection rate of GeneXpert in the purulent specimens.
Though granulomatous inflammation most supports a diagnosis of TB in endemic areas, it is also seen in diseases such as NTM infections, syphilis, leprosy, fungal infections and sarcoidosis. Cytology result alone cannot be used as a basis for definite diagnosis. In our study, the specificity of cytology was 100%. It was due to that the non-TB cases in this analysis only included metastatic tumors and bacterial suppurative inflammation, which generally do not share the similar pathological features with TB.
The main limitation of this study lies in the small number of cases and single-center retrospective study design. Chest wall TB is a rare form of extra-pulmonary TB. It is difficult to harvest large numbers of study cases in a single center. Extending the time of case inclusion or organizing multi-center studies may be a future work.
Conclusion
FNA is a minimally invasive and simple method of sampling for patients with suspected chest wall TB. GeneXpert had a good detection performance for MTB in the chest wall FNA specimens and achieved higher sensitivity as compared to cytology and conventional TB tests. The implementation of GeneXpert may increase the diagnostic efficacy of FNA in the diagnosis of chest wall TB and provide quicker results.
Ethics Approval and Informed Consent
We conducted the study in accordance with the amended Declaration of Helsinki. The study was approved by the Ethics Committee of Shanghai Pulmonary Hospital in China. The ethical approval No. was K18-156. Informed consent for inclusion was waived as this was a retrospective study and the medical records and patients’ information were anonymously collected. Privacy protection was guaranteed for each included participant.
Acknowledgment
We thank Qin Sun for his guidance on research and statistical methods.
Author Contributions
Wei SHA designed the research; Wen-ting LI and Wei SHA wrote the manuscript; Wen-ting LI collected the clinical data; Wen-ting LI and Wei SHA did the statistical work. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Shanghai Clinical Research Center of Infectious Diseases (Tuberculosis) [grant number 19MC1910800].
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Chakaya J, Khan M, Ntoumi F, et al. Global Tuberculosis Report 2020 - Reflections on the Global TB burden, treatment and prevention efforts. Int J Infect Dis. 2021;113(Suppl 1):S7–S12. doi:10.1016/j.ijid.2021.02.107
2. Pang Y, An J, Shu W, et al. Epidemiology of extrapulmonary tuberculosis among inpatients, China, 2008–2017. Emerg Infect Dis. 2019;25(3):457–464. doi:10.3201/eid2503.180572
3. Sandgren A, Hollo V, van der Werf MJ. Extrapulmonary tuberculosis in the European Union and European Economic Area, 2002 to 2011. Euro Surveill. 2013;18(12):20431. doi:10.2807/ese.18.12.20431-en
4. Tanaka S, Aoki M, Nakanishi T, et al. Retrospective case series analysing the clinical data and treatment options of patients with a tubercular abscess of the chest wall. Interact Cardiovasc Thorac Surg. 2012;14(3):249–252. doi:10.1093/icvts/ivr113
5. Kabiri EH, Alassane EA, Kamdem MK, et al. Tuberculosis cold abscess of the chest wall: a clinical and surgical experience. Report of 16 cases (Case series). Ann Med Surg. 2020;51:54–58. doi:10.1016/j.amsu.2020.02.001
6. Majeed FA, Ali A, Zafar U, Ahmed Taimure SZ, Mahmood U. Outcome analysis of primary chest wall tuberculosis: a series of 32 cases. J Ayub Med Coll Abbottabad. 2021;33(3):357–362.
7. Faure E, Souilamas R, Riquet M, et al. Cold abscess of the chest wall: a surgical entity? Ann Thorac Surg. 1998;66(4):1174–1178. doi:10.1016/S0003-4975(98)00770-X
8. Sakuraba M, Sagara Y, Komatsu H. Surgical treatment of tuberculous abscess in the chest wall. Ann Thorac Surg. 2005;79(3):964–967. doi:10.1016/j.athoracsur.2004.09.004
9. Kim YT, Han KN, Kang CH, Sung SW, Kim JH. Complete resection is mandatory for tubercular cold abscess of the chest wall. Ann Thorac Surg. 2008;85(1):273–277. doi:10.1016/j.athoracsur.2007.08.046
10. World Health Organization. Using the Xpert MTB/RIF Assay to Detect Pulmonary and Extrapulmonary Tuberculosis and Rifampicin Resistance in Adults and Children: Expertgroup Meeting Report. Geneva: World Health Organization; 2014. Available from: https://www.who.int/publications/i/item/WHO-HTM-TB-2013.14.
11. Narayana Reddy RA, Narayana SM, Shariff S. Role of fine-needle aspiration cytology and fluid cytology in extra-pulmonary tuberculosis. Diagn Cytopathol. 2013;41(5):392–398. doi:10.1002/dc.22827
12. World Health Organization. Implementing Tuberculosis Diagnostics: Policyframework. Geneva: World Health Organization; 2015. Available from: https://www.who.int/publications/i/item/9789241508612.
13. National Health and Family Planning Commission of the People’s Republic of China. Diagnosis for pulmonary tuberculosis (WS 288—2017); 2017. Available from: http://www.nhc.gov.cn/ewebeditor/uploadfile/2017/12/20171212154852389.pdf.
14. Boruah DK, Sanyal S, Sharma BK, Prakash A, Dhingani DD, Bora K. Role of cross sectional imaging in isolated chest wall tuberculosis. J Clin Diagn Res. 2017;11(1):TC01–TC06. doi:10.7860/JCDR/2017/23522.9185
15. Kuzucu A, Soysal O, Günen H. The role of surgery in chest wall tuberculosis. Interact Cardiovasc Thorac Surg. 2004;3(1):99–103. doi:10.1016/S1569-9293(03)00192-0
16. Keum DY, Kim JB, Park CK. Surgical treatment of a tuberculous abscess of the chest wall. Korean J Thorac Cardiovasc Surg. 2012;45(3):177–182. doi:10.5090/kjtcs.2012.45.3.177
17. Paik HC, Chung KY, Kang JH, Maeng DH. Surgical treatment of tuberculous cold abscess of the chest wall. Yonsei Med J. 2002;43(3):309–314. doi:10.3349/ymj.2002.43.3.309
18. Zhang W, Chen J, Wu X, et al. Preoperative ultra-short-course chemotherapy combined with surgery for the treatment of chest wall tuberculosis. Infect Drug Resist. 2020;13:2277–2284. doi:10.2147/IDR.S255740
19. VanderLaan PA. Fine-needle aspiration and core needle biopsy: an update on 2 common minimally invasive tissue sampling modalities. Cancer Cytopathol. 2016;124(12):862–870. doi:10.1002/cncy.21742
20. Chambers M, O’Hern K, Kerr DA. Fine-needle aspiration biopsy for the diagnosis of bone and soft tissue lesions: a systematic review and meta-analysis. J Am Soc Cytopathol. 2020;9(5):429–441. doi:10.1016/j.jasc.2020.05.012
21. Hobby GL, Holman AP, Iseman MD, Jones JM. Enumeration of tubercle bacilli in sputum of patients with pulmonary tuberculosis. Antimicrob Agents Chemother. 1973;4(2):94–104. doi:10.1128/AAC.4.2.94
22. H Y, Lacy J, Smith LR, LeMaistre CA. Quantitative studies of mycobacterial populations in sputum and saliva. Am Rev Respir Dis. 1967;95(6):998–1004. doi:10.1164/arrd.1967.95.6.998
23. Lawn SD, Nicol MP. Xpert® MTB/RIF assay: development, evaluation and implementation of a new rapid molecular diagnostic for tuberculosis and rifampicin resistance. Future Microbiol. 2011;6(9):1067–1082. doi:10.2217/fmb.11.84
24. Kohli M, Schiller I, Dendukuri N, et al. Xpert MTB/RIF Ultra and Xpert MTB/RIF assays for extrapulmonary tuberculosis and rifampicin resistance in adults. Cochrane Database Syst Rev. 2021;1(1):CD012768. doi:10.1002/14651858.CD012768.pub3
25. Scott LE, Beylis N, Nicol M, et al. Diagnostic accuracy of Xpert MTB/RIF for extrapulmonary tuberculosis specimens: establishing a laboratory testing algorithm for South Africa. J Clin Microbiol. 2014;52(6):1818–1823. doi:10.1128/JCM.03553-13
26. Al-Soud WA, Jönsson LJ, Râdström P. Identification and characterization of immunoglobulin G in blood as a major inhibitor of diagnostic PCR. J Clin Microbiol. 2000;38(1):345–350. doi:10.1128/JCM.38.1.345-350.2000
27. Katamba A, Sanyu I, Andama A, et al. Sputum quality and diagnostic performance of GeneXpert MTB/RIF among smear-negative adults with presumed tuberculosis in Uganda. PLoS One. 2017;12(7):e0180572. doi:10.1371/journal.pone.0180572
28. Aninagyei E, Ayivor-Djanie R, Attoh J, Dakorah MP, Ginko MN, Acheampong DO. Molecular detection of Mycobacterium tuberculosis in blood stained sputum samples using GeneXpert PCR assay. Diagn Microbiol Infect Dis. 2021;100(3):115363. doi:10.1016/j.diagmicrobio.2021.115363
29. Hemalatha A, Shruti P, Kumar MU, Bhaskaran A. Cytomorphological patterns of tubercular lymphadenitis revisited. Ann Med Health Sci Res. 2014;4(3):393–396. doi:10.4103/2141-9248.133466
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Patterns of Fine Needle Aspiration Cytology Diagnosed Thyroid Nodules Among Clinically Suspected Patients in Northeast Ethiopia
Ebrahim H, Tilahun M, Fiseha T, Debash H, Bisetegn H, Alemayehu E, Fiseha M, Ebrahim E, Shibabaw A, Seid A, Getacher Feleke D, Mohammed O
Pathology and Laboratory Medicine International 2023, 15:27-36
Published Date: 10 March 2023