Back to Journals » Integrated Pharmacy Research and Practice » Volume 11
Patient-Centered Communication Among Pharmacy Professionals Working in Hospitals and Drug Retail Outlets in Asmara, Eritrea: Knowledge, Attitude, Self-Efficacy and Barriers
Authors Michael E, Nurahmed A, Mihreteab H, Nurhussien M, Adem M, Goitom A ![]() , Mihreteab Siele S, Tesfamariam EH
, Mihreteab Siele S, Tesfamariam EH ![]() , Abdu N
, Abdu N ![]()
Received 15 March 2022
Accepted for publication 20 September 2022
Published 6 October 2022 Volume 2022:11 Pages 153—164
DOI https://doi.org/10.2147/IPRP.S363931
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Jonathan Ling
Ermias Michael,1 Abdulaziz Nurahmed,1 Haben Mihreteab,1 Mohammed Nurhussien,1 Mohammedali Adem,1 Alemseghed Goitom,1 Senai Mihreteab Siele,1 Eyasu H Tesfamariam,2 Nuru Abdu3
1Department of Medical Sciences, Pharmacy Unit, Orotta College of Medicine and Health Sciences, Asmara, Eritrea; 2Biostatistics and Epidemiology, Department of Statistics, College of Sciences, Mai-Nefhi, Eritrea; 3Department of Pharmacy, Adi-Tekelezan Community Hospital, Adi-Tekelezan, Eritrea
Correspondence: Nuru Abdu, Department of Pharmacy, Adi-Tekelezan Community Hospital, Adi-Tekelezan, Eritrea, Tel +291-7262928, Email [email protected]
Background: Globally, preventable medication-related problems are increasing constantly. Patient-centered communication (PCC) is essential to identify and reduce the occurrence of drug-related problems such as inappropriate use of medications, adverse drug reactions and non-adherence. In Eritrea, personal observations and anecdotal reports showed that pharmacy professionals’ practice towards PCC was unsatisfactory. This study was conducted to assess pharmacy professionals’ knowledge, attitude, self-efficacy and barriers towards the practice of PCC.
Methods: An analytical cross-sectional study design was employed among all pharmacy professionals who were employees of the drug retail outlets and hospital out-patient pharmacies of Asmara, Eritrea. A census approach was employed and data were collected from May to June 2021 using a face to face interview-based data collection tool. Descriptive and analytical statistics including independent samples t-test and multiple linear regression were employed using IBM SPSS (version-26).
Results: A total of 79 pharmacy professionals with a median age of 36 (IQR: 20) years were included in the study. The mean (SD) knowledge score of PCC was found to be 11.91 (2.0) out of 17. Moreover, the mean (SD) attitude score was 39.55 (4.0) out of 60 and the overall mean (SD) self-efficacy score was 52.51 (12.0) out of 96. Self-efficacy was significantly correlated with attitude (p=0.015). Work setting (p=0.002) and training (p=0.045) were predictors for the sub-scales of self-efficacy ‘exploring patient’s perspectives’ and ‘dealing with communicative challenges’, respectively. Workload/shortage of pharmacy professionals and time constraint were found to be the main barriers of the pharmacy professionals for not practicing PCC.
Conclusion: Generally the pharmacy professionals’ fairly encouraging knowledge and attitude score on PCC, it was not supported with their self-efficacy. This necessitates further attention from policy makers and health facility managers in creating an ideal working environment for the pharmacy professionals to practice PCC at their best.
Keywords: knowledge, attitude, self-efficacy, barriers, pharmacy professionals, hospitals, drug retail outlets, Eritrea
Erratum for this paper has been published.
Introduction
In pharmacy practice, effective communication with patients about their experiences, desires and worries about their health and medication is crucial to ensure adherence, detect drug-related problems such as inappropriate use of medications, adverse events and non-adherence.1,2 In addition, understanding patient needs and individualization of pharmaceutical care provided are important in order to deliver patient-specific services. Patient-centered communication (PCC) allows pharmacy professionals to address patient’s problems by considering the patient’s past familiarity of illness, the psychosocial perspective, and shared decision-making.3 PCC is defined as “Respecting and responding to patients wants, needs and preferences, so that patients can make choices in their care that best fit their individual circumstances.”4 Implementation of PCC in pharmacy practice involves creating a relationship between a pharmacy professional and a patient as a basis of faith.5,6 The implementation of PCC is done through the pharmacy professional-patient counseling process. Counseling, as a critical element of the dispensing process, provides a prospect for the pharmacy professionals to build a truthful liaison with patients and deliberate the use of medication to guarantee patients have a complete understanding of their treatment goal,7,8 strict adherence,9,10 and enhancement of their quality of life.7–9
Preventable medication-related problems in the world are increasing constantly.11 The most cited causes of these problems are non-adherence, adverse drug reactions and inappropriate prescribing and monitoring.11 Pharmacy professionals can take a leading role in preventing such problems by practicing patient-centered approach. The scale of these misadventures rise concerns about the cost of drug therapy and safety. This provides the opportunity for pharmacy professionals to play their role in providing assistance and assurance on the safety, cost effectiveness and prevention of ill health using the patient-centered practice. Moreover, this practice will help to empower pharmacy professionals and to take part in the leadership of providing improved quality of care. However, to deliver such practice requires more than scientific knowledge and expertise. In addition, pharmacy professionals could have barriers that limit them to practice PCC such as shortage of staff, lack of experience, time constraint, staff workload, environmental constraints, lack of legal regulation and lack of organizational facilities.12–14 Thus, it mandates a system that describes the role and responsibility of the pharmacy professionals and provides adequate infrastructure as well as clarity of processes for implementation.
In Eritrea, as in the rest of the developing countries, there is an evidence of irrational use of medicine.15–17 To tackle this problem, the Ministry of Health drafted a national drug policy to ensure rational use of medicine in the country. Despite this effort, irrational use of medicine is still a concern. Besides, there is no legal frame work for the job description of pharmacy professionals and the profession of pharmacy is not patient-oriented in the country.18 This issue further aggravates the existing irrational use of medicine. Although accurate data may not be available, personal observation and subjective reports showed that pharmacy professionals’ practice towards PCC was unsatisfactory. Understanding the current knowledge, attitude and self-efficacy of pharmacy professionals’ on PCC and their barriers to implementation is crucial in maneuvering future interventions. This study was therefore conducted to assess knowledge, attitude and self-efficacy of pharmacy professionals towards PCC as well as the barriers that hinder the practice of PCC in hospital pharmacies and pharmacy retail outlets located in Asmara, Eritrea.
Materials and Methods
Study Design and Setting
An analytical cross-sectional study was conducted in all drug retail outlets (both pharmacies and drug shops) and hospital pharmacies namely: Orotta National Referral Hospital, Halibet National Referral Hospital, Saint-Mary Neuro-Psychiatric National Referral Hospital, Brhan-Aini Ophthalmic National Referral Hospital and Hazhaz Community Hospital. All the study sites are located in Asmara, the capital city of Eritrea and data was collected between June and August, 2021.
In Asmara, there were a total of 44 drug retail outlets (26 community pharmacies, 6 governmentally-owned community chain pharmacies and 12 drug shops) during the study period. They cover more than 50% of all drug retail outlets in the country. In Eritrea, pharmacy professionals work in different areas such as community pharmacy, hospital pharmacy, administrative setting and pharmaceutical industry. Moreover, both pharmacy technicians and pharmacists are authorized to dispense medicines.
Source and Study Population
All pharmacy professionals who worked in the pharmacies were the source population for this study. Pharmacy professionals, regardless of their sex, who worked in the out-patient department of hospital pharmacy and drug retail outlets and were willing to deliver permission to be part of the study formed the study population. Pharmacy interns and non-pharmacy professionals were excluded from the study.
Sample Size and Sampling Technique
A total of 93 registered pharmacy professionals who worked in the respective drug retail outlets and out-patient hospital pharmacies were approached by the data collectors. However, 14 subjects were excluded from the study for different reasons (Figure 1). This study involved all pharmacy professionals (N = 79) that were eligible for study in all drug retail outlets and hospital pharmacies located in Asmara, Eritrea. Hence, there was no need of employing sampling technique in the study.
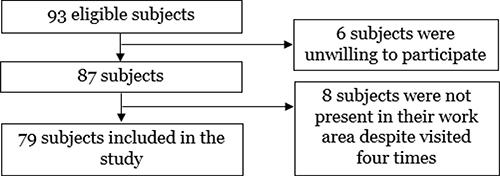 |
Figure 1 Eligibility and enrollment of study participants involved in a study that assessed patient-centered communication of pharmacy professionals in Asmara Eritrea, 2021 (N = 79). |
Data Collection Tool and Approach
A structured interview-based data collection tool upon appraisal of comparable published studies19–21 was used to collect data. The data collection tool consists of five sections. Section A includes socio-demographic and other background characteristics of the subjects such as age, sex and work experience. Section B intended to record information about the knowledge of the pharmacy professionals towards PCC using 17-items. Section C was aimed at recording information about the attitude of the pharmacy professionals using 12-items. Furthermore, section D assessed the current barriers and possible to the practice of PCC. Section E was used to assess the subject’s self-efficacy about patient-centered communication using 24-items. It was intended to assess the overall self-efficacy, using three sub-scales such as “exploring the patients” perspective’, “sharing information/power” and “dealing with communication challenges”. Moreover, section E was adopted from a standard questionnaire19 and slightly modified upon a consent from the original author.
All active pharmacy professional employees in the respective facilities were requested for consent to partake in this study. Once suitability and willingness were secured, data were collected by direct interview. To avoid confusion of the questions, any elaboration for the questions was provided by data collection team. In cases where pharmacy professionals were not present during data collection, efforts were made to reach them with all promising means and those who could not be reached after four attempts via physical visit or seems highly timid to participate in the study, were considered as non-respondents.
Outcome Variables and Variable Measurement
The primary outcome measures were knowledge, attitude, self-efficacy and barriers of PCC among the pharmacy professionals. The secondary outcome measure was the determinants of knowledge, attitude and self-efficacy of PCC.
Knowledge was measured using 17-items. A score of “1” was assigned to the correct answers and “0” to the wrong answers. Then, the assigned scores were added, divided by 17 and multiplied by 100 to get the overall knowledge scores.
Attitude was measured with 12-items in the form of 5-point Likert scale ranging from strongly agree to strongly disagree. Response for a negatively worded item was at first reverted to get a composite attitude score. Attitude score was computed from the initial responses of the respondents’, where the minimum and maximum ideal scores were 12 and 60, respectively.
Self-efficacy was also measured using a 5-point Likert scale. In order to make descriptive analysis, merging was done for “very high degree” and “high degree” as one category; and “Very low degree” and “low degree” as another; leaving “neutral” as third separate category. Moreover, the sub-scales of self-efficacy, “exploring patient’s perspectives’, “sharing information and power” and “dealing with communication challenges” were measured with 10, 8 and 6 items, respectively. The scores within the sub-scale of self-efficacy were computed from the original responses.
The overall self-efficacy score was computed from the original responses of the participants (using 24-items), where the minimum and maximum ideal scores were 0 and 96, respectively.
Data Quality Control
To confirm face and content validity, the data collection tool was peer-reviewed by various experts in the fields of pharmacy, medicine, pharmacoepidemiology, epidemiology and public health. The content validity index (CVI) was computed at item level, and all items rated as relevant were included to make the I-CVI of the final questionnaire one. The questionnaire was then modified and a pre-test was further conducted. A pre-test was conducted on 10 participants between 26th and 28th of May, 2021 at randomly selected community and hospital pharmacies. The pre-test was targeted at checking the questionnaire’s suitability or comprehensiveness, flow of question, skip patterns, familiarization of data to collectors, estimation of the time for completion of the questionnaire and to ascertain the feasibility of the study. Accordingly, some modifications were made to the questionnaire. Besides, the subjects which were included during the pre-test were excluded from the final analysis of the study.
Ethical Approval and Consent to Participate
Ethical approval to conduct the study was obtained from the Ministry of Health research ethics and protocol review committee. Permission was also obtained from the heads of the respective health facilities and drug retail outlets prior to the data collection. Written informed consent form was obtained from all the study participants and all personnel information were de-identified. All the information obtained was held confidential and used only for this study’s purpose.
Statistical Analysis
Data were entered and analyzed using Census and Survey Processing system (version 7.0) and IBM Statistical Package for Social Sciences (version 22), respectively. All descriptive statistics, mean, median, percentages and frequencies were computed as appropriate. Bivariate relationship between the dependent variables (knowledge, attitude, and self-efficacy) and socio-demographic and background characteristics was performed using independent samples t-test. Moreover, bivariate correlation with age and work experience was computed using Pearson’s correlation coefficient. Independent variables that were significantly correlated with the dependent variables were retained for multiple linear regressions. Linearity and multi-collinearity of the variables was assessed prior to the multiple linear regression. P-value less than 0.05 was considered as statistically significant.
Results
Socio-Demographic and Background Characteristics
A total of 79 subjects with a median age of 36 years (IQR: 20) were enrolled in the study. Most of the participants had never taken any training/course regarding PCC before (n = 54, 68.4%), had a bachelor degree and above in the field of pharmacy (n = 48, 60.8%) and employed in a drug retail outlet (n = 55, 69.6%). About 25.3% (n = 20) of them had a working experience of more than 20 years in the field of pharmacy. Detailed socio-demographic characteristics of the study population are provided in Table 1.
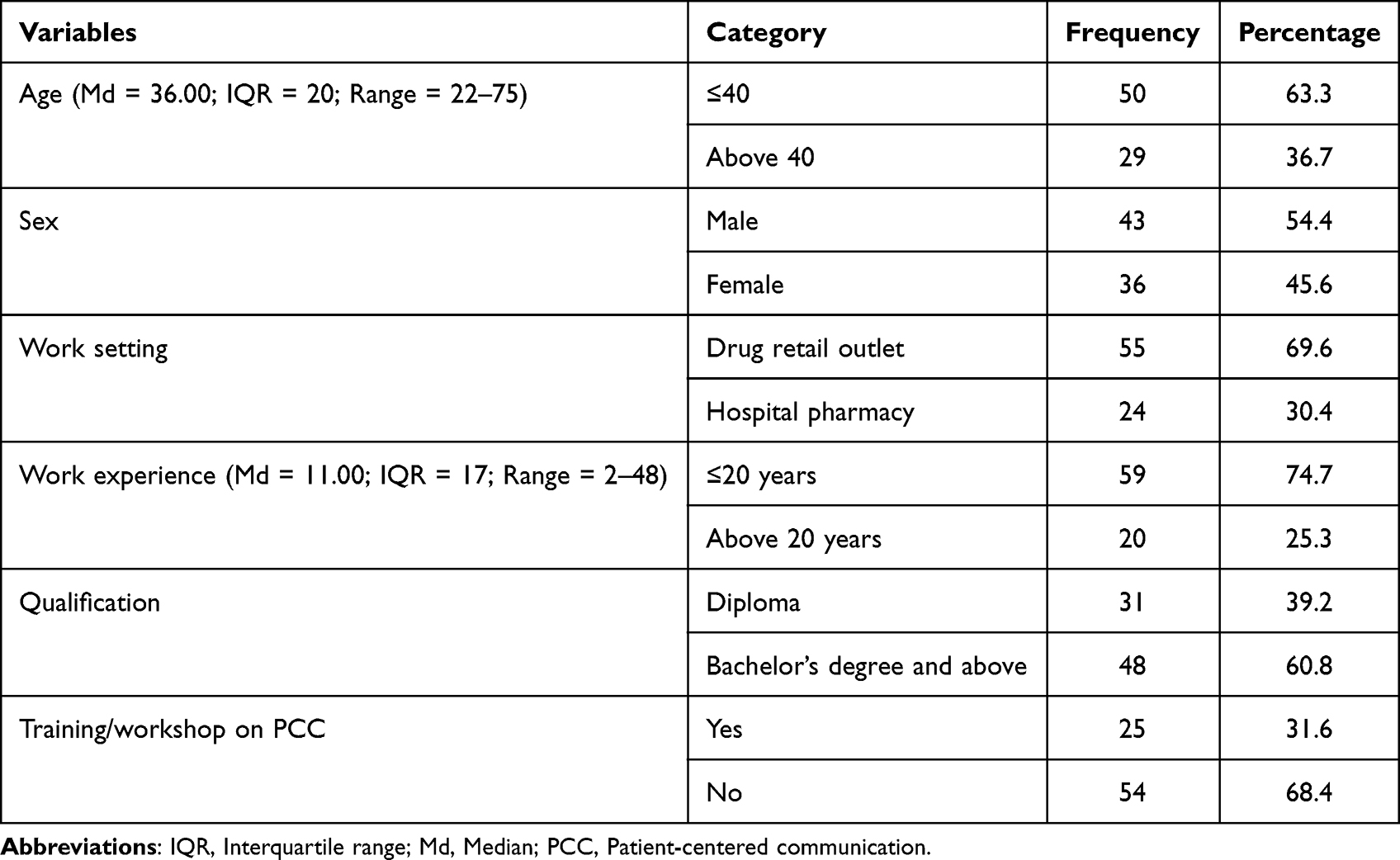 |
Table 1 Socio-Demographic Characteristics of the Respondents (N = 79) |
Knowledge of Pharmacy Professionals on Patient-Centered Communication and Its Associated Factors
Out of the total 79 participants, 22.8% (n = 18) have never heard and/or read the term PCC before. Of those who previously heard and/or read the term PCC (n = 61), 95.1% of them indicated that “The Pharmacy professional provides clear information about the treatment plan to patients” which made it the highest correctly responded item. Furthermore, the items “Providing PCC necessitates the Pharmacy professional to accept the legitimacy of patient’s views and feelings; and is not judgmental’ and “The Pharmacy professional has to offer the patient an opportunity to discuss and share decision making” were correctly responded by 91.8% (n=56/61) each. However, only 13.1% (n=8/61) of them correctly indicated that “Providing PCC requires the Pharmacy professional to not only fill the prescription and give direction on the medications” (Table 2).
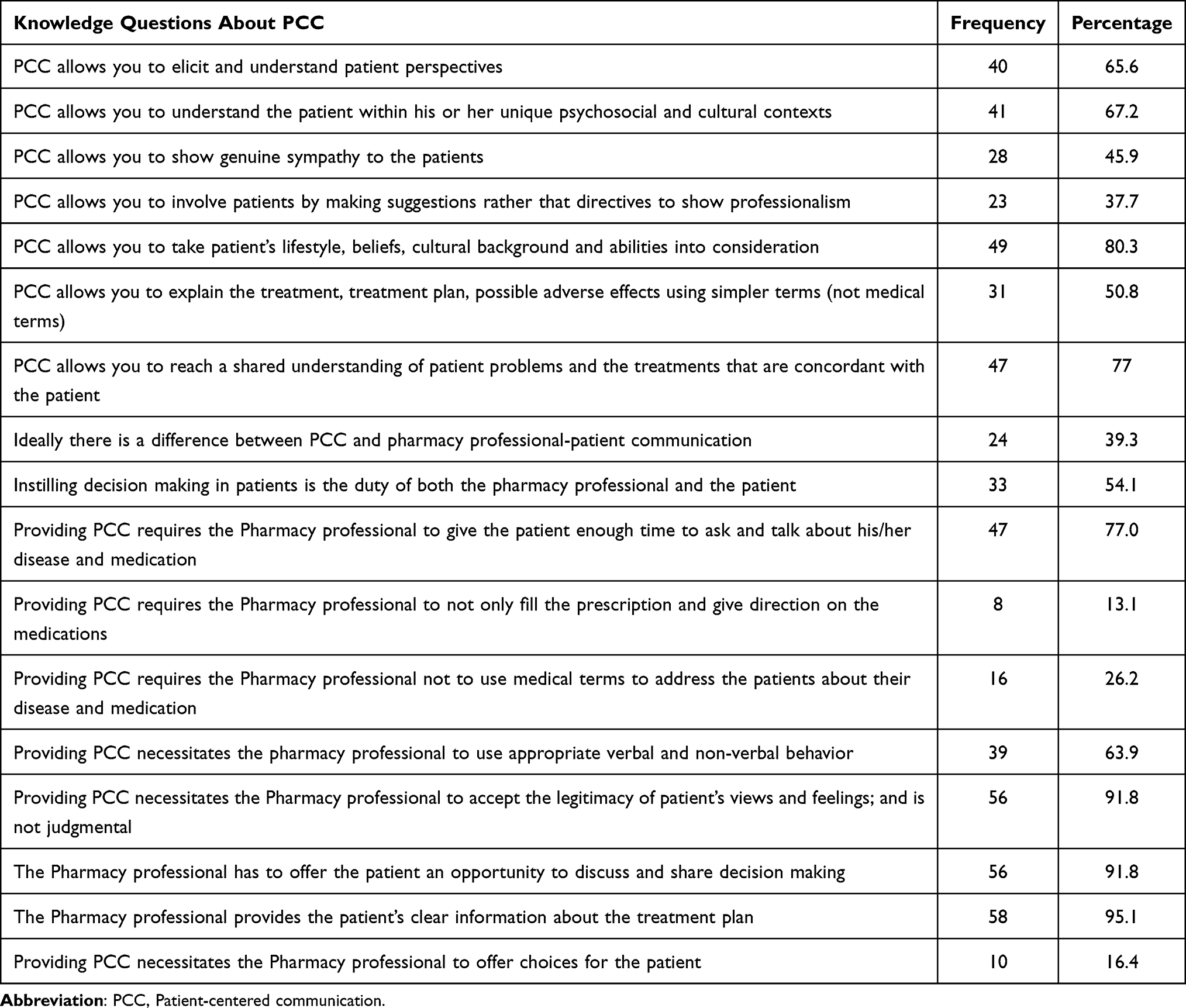 |
Table 2 Percentage Distribution of Correct Knowledge of PCC Among Pharmacy Professionals (N = 61) |
The mean (SD) knowledge score was 11.91 (2.0) out of 17. The knowledge score had no significant associations with age (rs=0.006, p=0.961), sex (p=0.423), qualification (p=0.05), training or workshop on PCC (p=0.716), work setting (p=0.346), work experience (rs= −0.052, p=0.691), attitude score (rs= −0.163, p=0.209) and self-efficacy score (rs=0.124, p=0.342) (Table S1).
Attitude of Pharmacy Professionals on Patient-Centered Communication and Its Associated Factors
The respondents showed their highest attitude by agreeing on “PCC is essential in the setting of pharmacy professional-patient Communication” (n=59/61, 96.7%) and “The level of communication in pharmacy patient communication could be improved” (n=59/61, 96.7%). Moreover, most of them (n=55/61, 90.2%) agreed that the “The Ministry of health should take initiative to encourage patient centered communication in all pharmacies in Eritrea”. However, only nine participants have agreed that PCC is currently practiced in all pharmacy setting in Eritrea (Table 3).
 |
Table 3 Percentage Distribution of Attitude of PCC Among Pharmacy Professionals (n = 61) |
The overall attitude mean (SD) value was 39.55 (4.0) out of 60. Only self-efficay score was significantly correlated with the overall attitude score (rs=0.311, p=0.015) (Table S2).
Self-Efficacy of Pharmacy Professionals on Patient-Centered Communication
In the sub-scale of “exploring patient’s perspectives’, the respondents showed their highest level of confidence in the item of “show a genuine interest in the patient and his/her situation” (n=55/79, 69.6%). On the other hand, only six of the total seventy nine respondents showed their high degree of confidence on “recognize the patient’s thoughts and feelings’. The mean (SD) score of the sub-scale was 22.78 (8.0) out of 40.
Furthermore, in the sub-scale of “sharing information and power”, the respondents showed their highest degree of confidence in the item of “inform the patient about the side effects, so the patient understands them” (n=51/79, 64.6%). However, only 6.3% (n=5/79) showed their high degree confidence on the item “advise and support the patient in making decision”. The mean (SD) score of the sub-scale “sharing information and power” was 16.48 (6.0) out of 32.
More than half (n=42/79, 53.2%) of respondents had a high degree confidence in “avoid letting myself be influenced by preconceptions about the patient” within the self-efficacy sub-scale of “dealing with communicative challenges”. Whereas, the lowest high degree level responded items were “to maintain the relationship with the patient when he/she is angry” and “to stay focused on what is best for the patient if there is a professional disagreement about the diagnosis and treatment” (each by 40.5%, n=32/79). The mean (SD) score of the sub-scale of “dealing with communicative challenges” was 13.69 (6.0) out of 24 (Table 4). Furthermore, the overall mean (SD) self-efficacy score was 52.51 (12.0) out of 96.
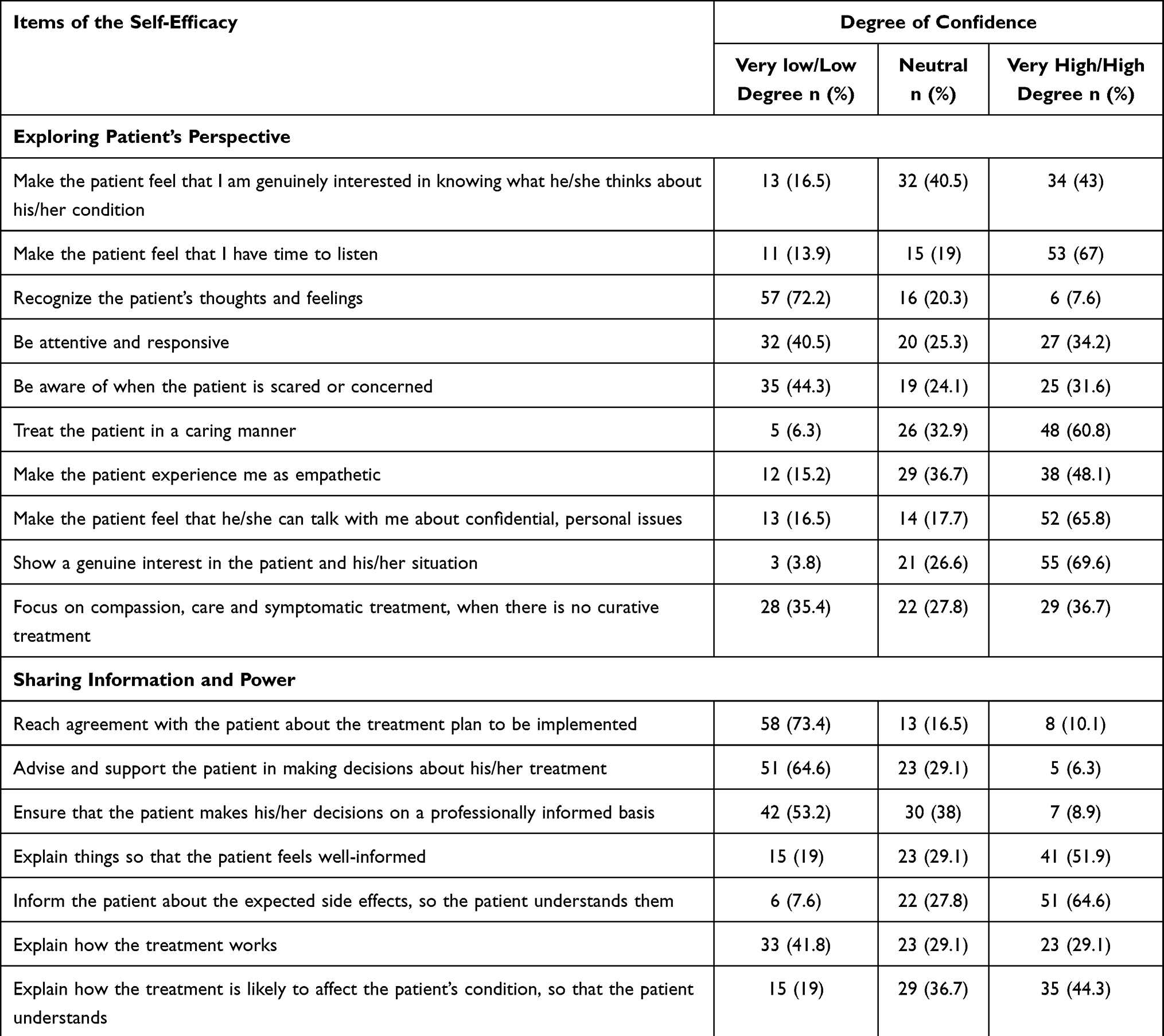 |
Table 4 Percentage Distribution of the Sub-Scales of Self-Efficacy (N = 79) |
Predictors of the Sub-Scales of Self-Efficacy
The mean score of the sub-scale of “exploring patient’s perspectives’, was not significantly associated with sex (p=0.134), qualification (p=0.074), training and/or workshop on PCC (p=0.169), heard or read the term PCC (p=0.55), age (rs=0.129, p=0.257), work experience (rs=0.161, p=0.157), knowledge score (rs=0.06, p=0.209) and attitude score (rs=0.185, p=0.154). However, it was significantly associated with work setting (p=0.002), where pharmacy professionals working in drug retail outlets (M = 23.9, SD = 4.8) scored higher than those working in hospital setting (M = 20.0, SD = 4.9) (Table S3).
Moreover, the mean score of the sub-scale of “sharing information and power” was not significantly associated with sex (p=0.532), qualification (p=0.422), training and/or workshop on PCC (p=0.417), work setting (p=0.067), age (rs=0.03, p=0.794), work experience (rs=0.034, p=0.767), knowledge score (rs=0.063, p=0.063) and attitude score (rs=0.250, p=0.052). On the other hand, it was found that, the pharmacy professionals who previously heard or read the term PCC (M = 16.4, SD = 4.35) had significantly (p<0.001) higher score that those who did not have (M = 13.3, SD = 2.46) (Table S4).
In the sub-scale of “dealing with communicative challenges”, no significant association was detected between the mean score of the sub-scale and the categories of sex (p=0.843), qualification (p=0.587), heard or read the term PCC (p=0.782), work setting (p=0.417), attitude score (rs=0.233, p=0.071) and knowledge score (rs=0.129, p=0.322). However, age (rs= −0.241, p=0.032), work experience (rs= −0.252, p = 0.025) and training and/or workshop on PCC (p=0.045) were significantly correlated with “dealing with communicative challenges” (Table S5).
Model diagnosis was performed after fitting the multiple linear regressions. The residual diagnosis showed homoscedasticity independent of errors, normality of errors and no multi-collinearity among the independent variables (after removing the variable age for its multi-collinearity with work experience as the initial model). Training and/or workshop on PCC (p=0.017) still retained its significance at a multivariate level (Table S5).
The overall mean self-efficacy score was not significantly associated with sex (p=0.301), qualification (p=0.177), training and/or workshop on PCC (p=0.802), heard or read the term PCC (p=0.166), age (rs= −0.021, p=0.855), work experience (rs= −0.007, p=0.953) and knowledge score (rs=0.124, p=0.342). Nevertheless, work setting of the pharmacy professionals (p=0.032) and attitude score (rs=0.311, p=0.015) was significantly associated with the overall self-efficacy score (Table S6).
To control confounding effect of the significantly associated variables (at bivariate level analysis), multiple regression was performed. The result showed that attitude score still retained its significance (p=0.022) at a multivariate level (Table 5).
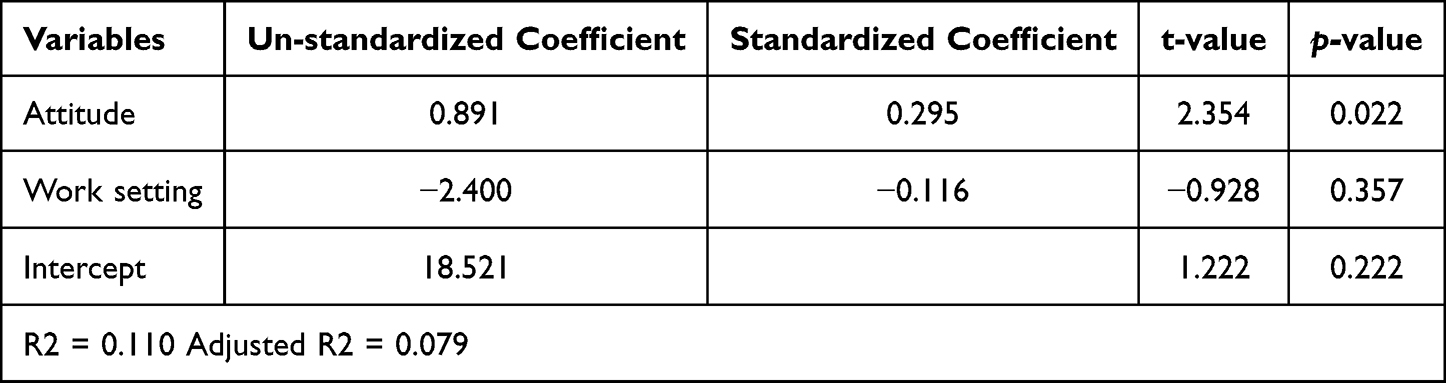 |
Table 5 Multivariate Analysis of the Predictors of Self-Efficacy of Pharmacy Professionals |
Correlation and Comparison Among the Sub-Scales of Self-Efficacy
A significantly positive correlation was observed between “exploring patient perspective” and “sharing information and power” (rp=0.317, p = 0.013). Moreover, a significant correlation was detected between “dealing with communicative challenges” and “sharing information and power” (rp = 0.262, p = 0.041). However, the relationship between “exploring patient perspective” and “dealing with communicative challenges” (rp = 0.161, p = 0.215) was not significant.
Upon comparison, “sharing information and power” was significantly lower (p<0.001) than “exploring patient perspective”. Whereas, “dealing with communicative challenges” score was significantly higher (p = 0.001) than that of “sharing information and power”.
Barriers to Practicing PCC
Majority of the respondents (n=70/79, 88.6%) had at least one barrier that hampered them for not practicing PCC. Workload and/or shortage of pharmacy staff, time constraint and discouraging working environment were found to be the main barriers (Figure 2). Improvement of working place (n=50/70, 71.4%), increasing the number of pharmacy staff (n=50/70, 71.4%) and a refresher training by the Ministry of Health (n=58/70, 82.9%) were the possible solutions suggested by the respondents to overcome the barriers for not practicing PCC.
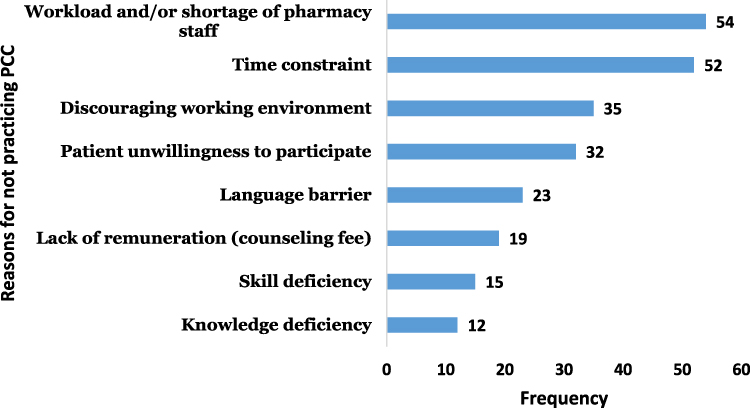 |
Figure 2 Barriers to practicing patient-centered communication (n = 70). |
Discussion
In the current study, the overall mean knowledge and attitude score was fairly encouraging. However, the overall mean self-efficacy score was not satisfactory. The respondents had a low degree confidence in recognizing the patient’s thoughts and feelings, providing advice and support to patients in decision-making and maintaining the relationship with the patient when they got angry. This reflects lack of awareness on PCC by the pharmacy professionals. Likewise, pharmacy professionals should play a key role in inspiring patients to actively participate in shared decision-making of their treatments, consider the patient’s thoughts and feelings and allow the patient in the treatment so as to increase treatment outcomes by the patients.
One in five of the respondents never heard and/or read the term PCC. This figure was not surprising as majority of them did not take any training and/or workshop on the subject matter. Furthermore, unlike the developed countries’ pharmaceutical care services (including PCC) are not yet standardized as a crucial role in developing countries.22 Majority of the respondents incorrectly responded that the concept of PCC requires to only fill prescriptions and provide direction on the medication. The current finding was in line with a study conducted in India where majority of the pharmacists (n=84/150) believed that they were only responsible to dispense and counsel patients on the prescribed medicines.23 This denotes that PCC was misunderstood by the respondents. Hence, continuous awareness raising programs should aim to correct such misconception and familiarize the pharmacy professionals with clear concepts of PCC as it aids in identifying or avoiding preventable medication-related problems such as non-adherence, inappropriate prescribing and adverse drug reactions at the earliest possible time.
Work setting of the respondents was a predictor for the sub-scale of “exploring patients” perspectives’ where pharmacy professionals who work in the drug retail outlets score higher than those who work in hospitals. It is unknown why the difference in work setting resulted in variation of score within the same sub-scale. This might be explained by the fact that respondents who work in the drug retail outlets can have sufficient time to discuss with the patients than those who work in the hospital setting. Moreover, it might also be due to convenience of setting for counseling, efforts to attract more clients as in the case of private drug retail outlets (DROs) and/or pharmacy professionals working in DROs might be much experienced compared to these in hospitals.
In the current study, training was a predictor variable for the sub-scale of “dealing with communicative challenges”. This was supported by a study conducted in South Korea as training increased the pharmacy students’ skills and attitudes and boosted their confidence in patient counseling.24
Workload and/or shortage of pharmacy staff, time constraint and discouraging working environment were found to be the main barriers identified for practicing PCC. Similar barriers were reported in studies conducted in Australia12 and Poland.25 The concerned body of the Ministry of Health should address the shortage of professionals and create a favorable working environment for a maximal PCC practice. In addition, training on the concepts of PCC, reported as a possible solution to overcome the barriers, is the simplest thing the Ministry of Health could offer to the pharmacy professionals.
Likewise, majority of the respondents showed a low knowledge on the items “Providing PCC requires the Pharmacy professional not to use medical terms to address the patients about their disease and medication” and “Providing PCC necessitates the Pharmacy professional to offer choices for the patient”. The respondents should be extra-cautious in avoiding medical terms as this is challenging in communicating with patients. Thus, efforts should be taken to clearly explain patients in simpler and easily understandable terms and should offer choices for the patient as it resulted in improved patient satisfaction and adherence.
In this study, the overall attitude mean value was encouraging. However, about one-third of the participants showed disagreement on the item “A patient should make a decision on his/her medication”. This might be due to the fact that the pharmacy professionals thought patients did not have sufficient knowledge to participate in the decision-making. However, patients are not blank sheets and they could have an expertise in their own and their children’s health. Hence, the pharmacy professionals should allow patients to make decision in their medications as this is important to reach in agreement about medications and thereby dictates the rationality of use by the patients. Majority of the respondents believed that PCC is not currently practiced in all pharmacy settings in Eritrea. Furthermore, the Spearman correlation revealed that with the increase in the mean attitude score the overall self-efficacy score increases.
This is the first study in Eritrea to investigate the knowledge, attitude, self-efficacy and barriers of patient-centered communication (PCC) in pharmacy professionals. The study engaged rigorous data quality and management approaches. Due to the cross-sectional nature of the study, cause-effect relationship did not be confirmed. Moreover, this study assessed self-efficacy of the pharmacy professionals, however this cannot be a valid measure to the current practice of PCC. The authors therefore recommended further studies that include a qualitative approach to measure the current practice of PCC and patients’ satisfaction to get the complete picture of the subject matter in Eritrea.
Conclusion
Though the pharmacy professionals’ overall understanding on PCC was fairly encouraging, it was not supported with their self-efficacy. Work setting and training were predictors for the sub-scales of self-efficacy “exploring patient’s perspectives’ and “dealing with communicative challenges”, respectively. The overall self-efficacy was significantly correlated with attitude score. Workload and/or shortage of pharmacy staff, time constraint and discouraging working environment were found to be the main barriers. To further promote the practice of PCC, a standard communication guideline and awareness raising programs targeting pharmacy professionals should be introduced.
Abbreviations
Df, Degree of freedom; IQR, Interquartile Range; MoH, Ministry of Health; PCC, Patient-centered communication; SD, Standard Deviation.
Data Sharing Statement
The data used in this study are available from the corresponding author and can be accessed upon reasonable request.
Ethical Approval and Consent to Participate
Ethical approval was obtained from Ministry of Health research ethics and protocol review Committee. Besides, permission was obtained beforehand from the medical director of the hospitals and owners of the drug retail outlets where the actual study and the pre-test survey were conducted. Study participants were informed about the aim of the study and written informed consent was provided from each subject. All the information obtained will be held confidential and was used only for this study’s purpose.
Acknowledgment
The authors would like to show gratitude to all participants of the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare no conflicts of interest in this work.
References
1. Gordon KSF, Dhillon S, Dhillon S. Effective chronic disease management: patients’ perspectives on medication-related problems. Patient Educ Couns. 2007;65(3):407–415. doi:10.1016/j.pec.2006.09.012
2. Wolters M, van Hulten R, Blom L, Bouvy ML. Exploring the concept of patient centred communication for the pharmacy practice. Int J Clin Pharm. 2017;39(6):1145–1156. doi:10.1007/s11096-017-0508-5
3. Stewart MBJ, Weston WW, McWhinney IR, McWilliam CL, Freeman TR. Patient-Centered Medicine: Transforming the Clinical Method. Thousand Oaks, Calif: Sage Publications; 1995.
4. Medicine I. Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001.
5. Schottenfeld L, Peikes D, Ricciardi R, Burak H, McNellis R, Genevro J. Creating Patient-Centered Team-Based Primary Care. Rockville, MD: Agency for Healthcare Research and Quality; 2016.
6. Barnett N. Patient-centered care in pharmacy practice; 2017.
7. Zhao PX, Wang C, Qin L, et al. Effect of clinical pharmacist’s pharmaceutical care intervention to control hypertensive outpatients in China. AJJP. 2012;6(1):48–56.
8. Okumura LM, Rotta I, Correr CJ. Assessment of pharmacist-led patient counseling in randomized controlled trials: a systematic review. Int J Clin Pharm. 2014;36:882–891. doi:10.1007/s11096-014-9982-1
9. Kaboli PJ, Hoth AB, McClimon BJ, Schnipper JL. Clinical pharmacists and inpatient medical care a systematic review. Arch Intern Med. 2006;166(9):955–964. doi:10.1001/archinte.166.9.955
10. Kuntz JL, Safford MM, Singh JA, et al. Patient-centered interventions to improve medication management and adherence: a qualitative review of research findings. Patient Educ Couns. 2014;97:310–326. doi:10.1016/j.pec.2014.08.021
11. Cresswell KM, Fernando B, McKinstry B, Sheikh A. Adverse drug events in the elderly. Br Med Bull. 2007;83(1):259–274. doi:10.1093/bmb/ldm016
12. Lloyd BEM, Innes L, Innes L. Barriers and enablers of patient and family centred care in an Australian acute care hospital: perspectives of health managers. Patient Exp J. 2018;5(3):55–64. doi:10.35680/2372-0247.1270
13. Esmaeili MCM, Salsali M, Salsali M. Barriers to patient-centred care: a thematic analysis study. Int J Nurs Knowl. 2014;25:2–8. doi:10.1111/2047-3095.12012
14. Luxford KSD, Delbanco T, Delbanco T. Promoting patient-centred care: a qualitative study of facilitators and barriers in healthcare organizations with a reputation for improving the patient experience. Int J Qual Health Care. 2011;23:510–515. doi:10.1093/intqhc/mzr024
15. Abdu N, Mosazghi A, Teweldemedhin S, et al. Non-Steroidal Anti-Inflammatory Drugs (NSAIDs): usage and co-prescription with other potentially interacting drugs in elderly: a cross-sectional study. PLoS One. 2020;15(10):e0238868. doi:10.1371/journal.pone.0238868
16. Tesfamariam S, Anand IS, Kaleab G, et al. Self-medication with over the counter drugs, prevalence of risky practice and its associated factors in pharmacy outlets of Asmara, Eritrea: a descriptive cross-sectional study. BMC Public Health. 2019;19:159. doi:10.1186/s12889-019-6470-5
17. Ateshim Y, Bereket B, Major F, et al. Prevalence of self-medication with antibiotics and associated factors in the community of Asmara, Eritrea: a descriptive cross sectional survey. BMC Public Health. 2019;19(1):726. doi:10.1186/s12889-019-7020-x
18. Awalom MT, Tesfa AF, Kidane ME, Ghebremedhin MR, Teklesenbet AH. Eritrean pharmacists’ job satisfaction and their attitude to re-professionalize pharmacy in to pharmaceutical care. Int J Clin Pharm. 2015;37:335–341. doi:10.1007/s11096-015-0064-9
19. Zachariae R, O’Connor M, Lassesen B, et al. The self-efficacy in patient-centeredness questionnaire–a new measure of medical student and physician confidence in exhibiting patient-centered behaviors. BMC Med Educ. 2015;15(1):1–13. doi:10.1186/s12909-014-0281-2
20. Stewart M, Brown JB, Weston W, McWhinney IR, McWilliam CL, Freeman T. Patient-Centered Medicine: Transforming the Clinical Method. CRC press; 2013.
21. Barnett NL. Developing a Person-Centred Approach to Pharmacy Practice. Kingston University; 2017.
22. Fang YYS, Feng B, Ni Y, Zhang K, Zhang K. Pharmacists’ perception of pharmaceutical care in community pharmacy: a questionnaire survey in Northwest China. Health Soc Care Community. 2011;19(2):189–197. doi:10.1111/j.1365-2524.2010.00959.x
23. Inamdar SZ, Apsy P, Rosy J, et al. Assessment of knowledge, attitude and practice of community pharmacist towards the provision of pharmaceutical care: a community based study. Int J Pharm Pract. 2018;11(3):158–163. doi:10.5530/ijopp.11.3.34
24. Jin HK, Park SH, Kang JE, et al. The influence of a patient counseling training session on pharmacy students’ self-perceived communication skills, confidence levels, and attitudes about communication skills training. BMC Med Educ. 2019;19(172):1–9. doi:10.1186/s12909-019-1607-x
25. Dorota Kopciuch AP, Zaprutko T, Ratajczak P, Nowakowska E, Kus K. A survey of pharmacists’ knowledge, attitudes and barriers in pharmaceutical care concept in Poland. BMC Med Educ. 2021;21(458):1–8. doi:10.1186/s12909-020-02436-3
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Knowledge and Perceptions of Nurse Practitioners on Adverse Events Following Immunization and Barriers to Reporting in the Central Region, Eritrea: A Cross-Sectional Study
Abdu N, Mosazghi A, Yehdego T, Tesfamariam EH, Russom M
Drug, Healthcare and Patient Safety 2022, 14:125-134
Published Date: 25 July 2022
COVID-19 and Saudi Arabia: Awareness, Attitude, and Practice
Fawzy MS, AlSadrah SA
Journal of Multidisciplinary Healthcare 2022, 15:1595-1618
Published Date: 26 July 2022
Knowledge, Attitude, Perceived Responsibilities, and Associated Factors Regarding Colostomy Care Among Nurses Working in Surgical Units at Amhara Region General and Referral Hospitals, Ethiopia: A Mixed Method Study
Tiruneh TE, Alem G, Taddele M, Tizazu ZM, Minale FK, Alemu KD
Nursing: Research and Reviews 2022, 12:191-206
Published Date: 13 October 2022
Prevalence and Predictors of Knowledge and Attitude on Optimal Nutrition and Health Among Pregnant Women in Their First Trimester of Pregnancy
Gebremichael MA, Lema TB
International Journal of Women's Health 2023, 15:1383-1395
Published Date: 4 September 2023
The Effect of Integrated Simulation Experiential Learning Disaster Nursing for Enhancing Learning Outcomes Among Undergraduate Nursing Students: A Quasi-Experimental Study
Emaliyawati E, Ibrahim K, Trisyani Y, Songwathana P
Advances in Medical Education and Practice 2025, 16:311-321
Published Date: 21 February 2025